Embed Size (px)
Citation preview
Stellenwert der endovaskulären TAAA-Chirurgie 2015
Dr. med. Michel Bosiers
Zentrum für Vaskuläre und Endovaskuläre Chirurgie Universitätsklinikum & St. Franziskus Hospital Münster
Direktor: Univ. Prof. Dr. med. G. Torsello
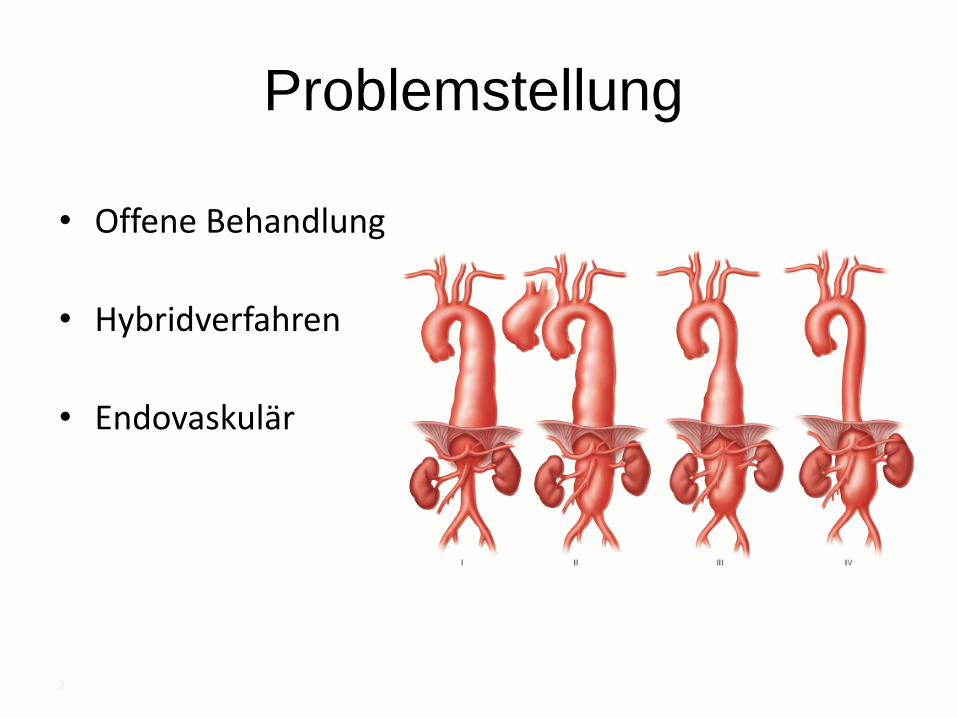
Problemstellung
• Offene Behandlung
• Hybridverfahren
• Endovaskulär
2
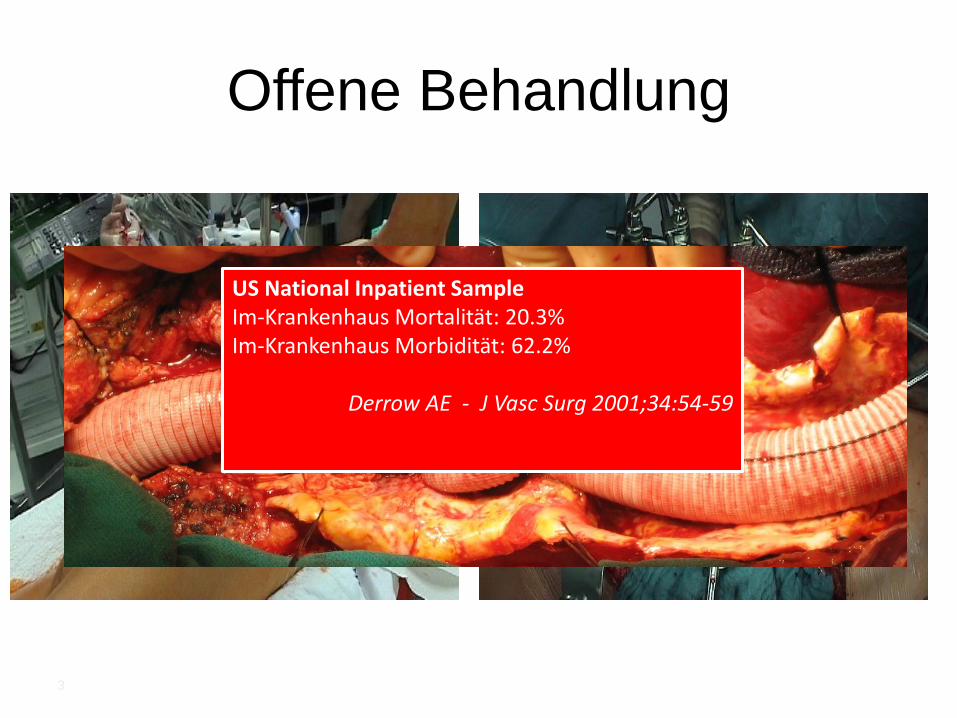
Offene Behandlung
US National Inpatient Sample Im-Krankenhaus Mortalität: 20.3% Im-Krankenhaus Morbidität: 62.2%
Derrow AE - J Vasc Surg 2001;34:54-59
3
Offene Behandlung
• US National Inpatient (Derrow AE - J Vasc Surg 2001;34:54-59)
- Im-Krankenhaus Mortalität: 20.3%
- Im-Krankenhaus Morbidität: 62.2% (pulmonal > kardial)
• Hochspez. Zentren (Coselli JSet al. Ann Thorac Surg. 2007; Schepens MA et al. EJVES 2009)
- 30-d-mortality 5-14% - irreversible Paraplegie : 2,6 % - 8,3%
• Alle in California (elektiv) (Rigberg DA et al. JVS 2006)
- 30-d-mortality 19%
Hybrid
Tshomba Y et al. Clinical outcomes of hybrid repair for thoracoabdominal aortic aneurysms. Ann Cardiothorac
Surg. 2012 Sep;1(3):293-303. doi: 10.3978/j.issn.2225-319X.2012.07.15.
5
Im-Krankenhaus Mortalität: 12,8 %
Im- Krankenhaus Morbidität: 30,4 % - irreversible Paraplegie 4,5 %
- Paraparese 7,5 %
- Niereninsuffizienz 8,8 %
- Mesenterialischämie 5,2 %
- kardiale Problemen 3,7 %
- verlängerte Beatmung 8,2 %
Moulakakis KG et al. Circulation 2011;124:2670-2680
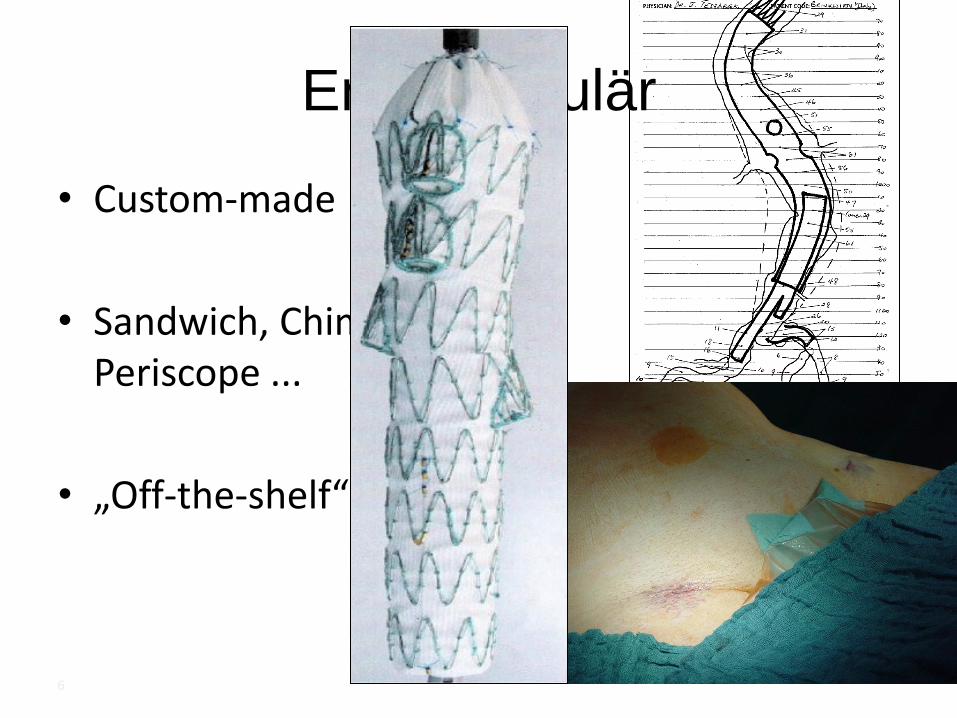
Endovaskulär
• Custom-made
• Sandwich, Chimney etc. Periscope ...
• „Off-the-shelf“
6
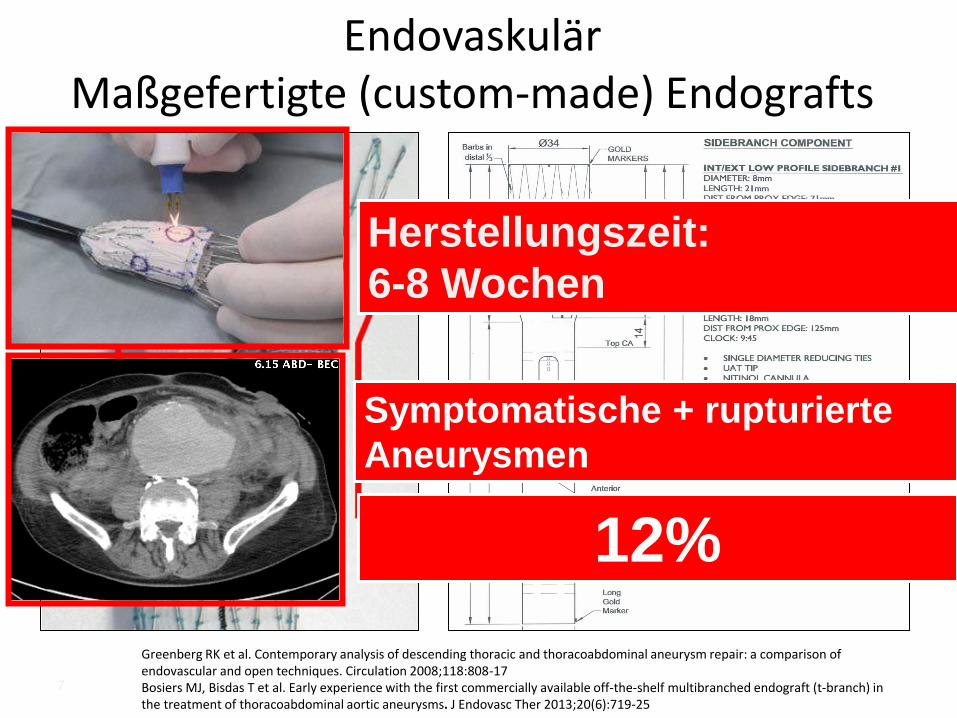
Greenberg RK et al. Contemporary analysis of descending thoracic and thoracoabdominal aneurysm repair: a comparison of endovascular and open techniques. Circulation 2008;118:808-17
Endovaskulär Maßgefertigte (custom-made) Endografts
Herstellungszeit:
6-8 Wochen
Symptomatische + rupturierte
Aneurysmen
12%
Bosiers MJ, Bisdas T et al. Early experience with the first commercially available off-the-shelf multibranched endograft (t-branch) in the treatment of thoracoabdominal aortic aneurysms. J Endovasc Ther 2013;20(6):719-25
7
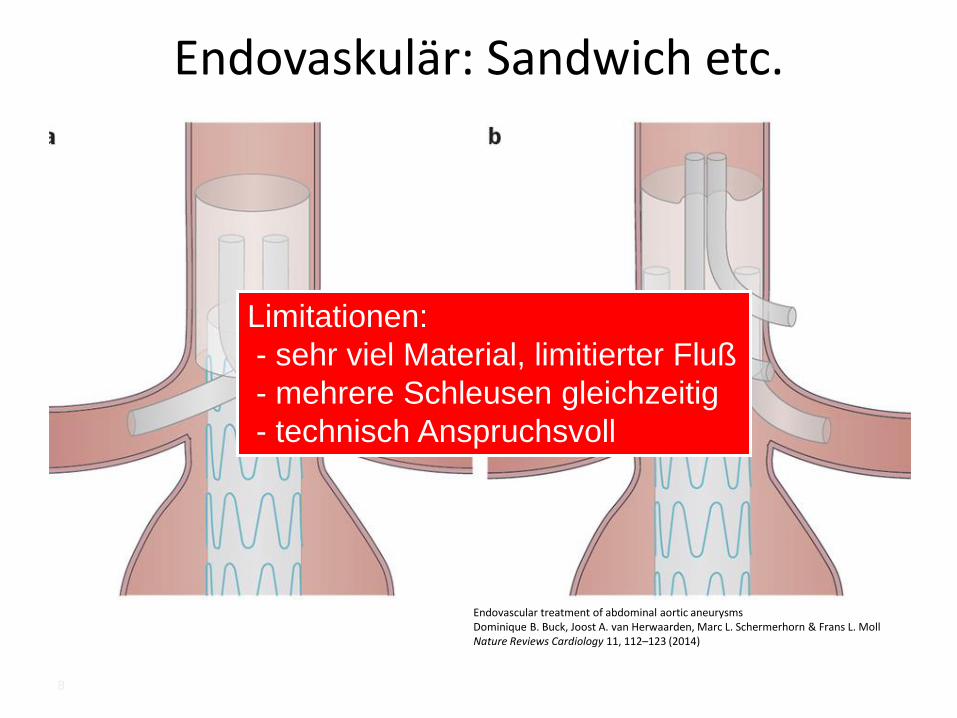
Endovaskulär: Sandwich etc.
8
Endovascular treatment of abdominal aortic aneurysms Dominique B. Buck, Joost A. van Herwaarden, Marc L. Schermerhorn & Frans L. Moll Nature Reviews Cardiology 11, 112–123 (2014)
Limitationen:
- sehr viel Material, limitierter Fluß
- mehrere Schleusen gleichzeitig
- technisch Anspruchsvoll
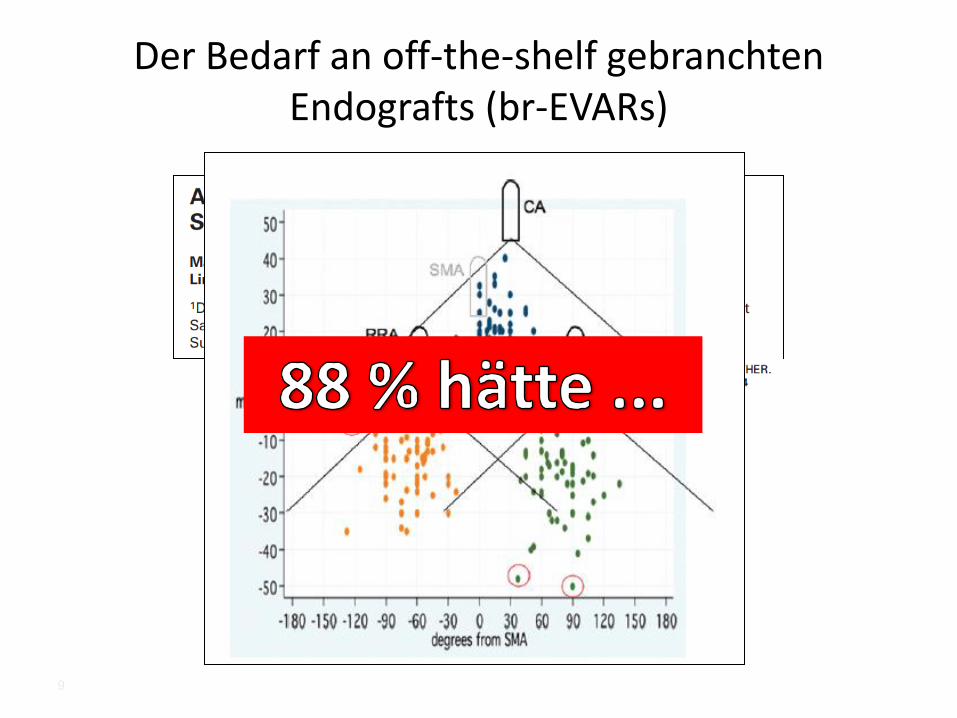
Der Bedarf an off-the-shelf gebranchten Endografts (br-EVARs)
9
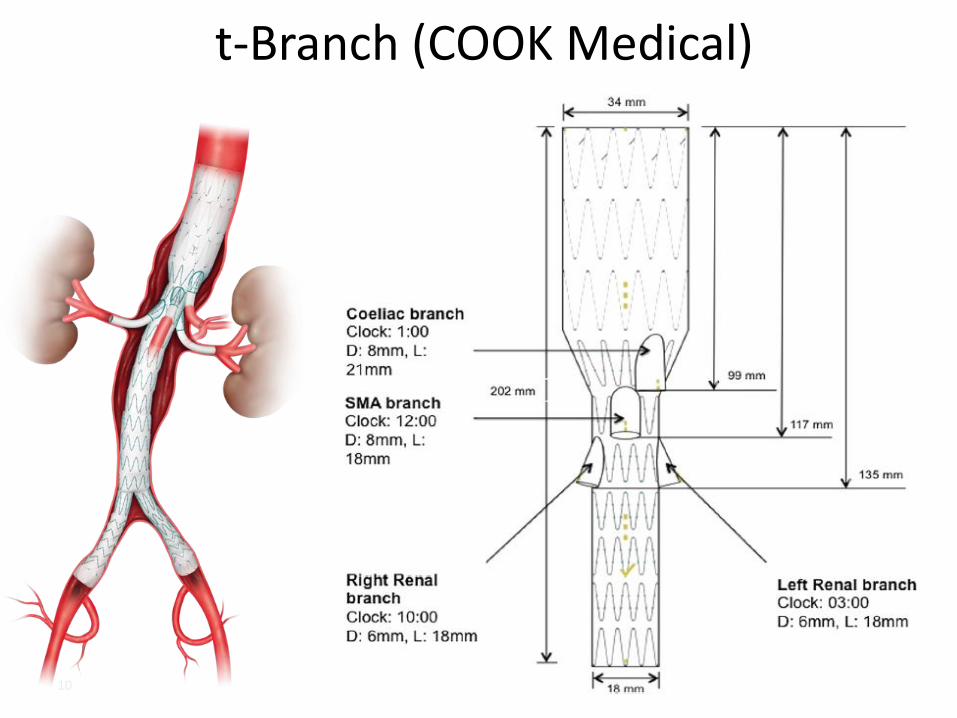
18 mm
t-Branch (COOK Medical)
10
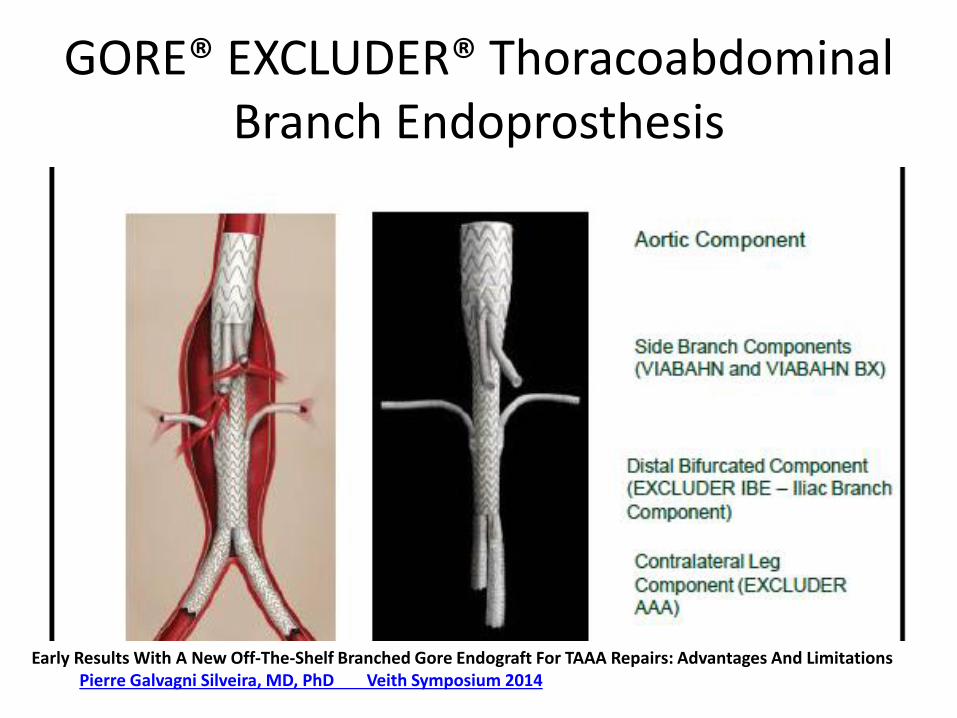
GORE® EXCLUDER® Thoracoabdominal Branch Endoprosthesis
Early Results With A New Off-The-Shelf Branched Gore Endograft For TAAA Repairs: Advantages And Limitations Pierre Galvagni Silveira, MD, PhD Veith Symposium 2014

Assessing the anatomic applicability of the
multibranched endovascular repair of thoracoabdominal aortic aneurysm technique.
Gasper WJ et al.
Division of Vascular and Endovascular Surgery, University of California San Francisco
J Vasc Surg. 2013 Jun;57(6):1553-8
N=43 pts
mit maßgefertigten gebranchten
Endografts
Anatomische Einsetzbarkeit t-Branch
Dissertation | Michel Bosiers | Münster, 19.12.2014
12

Implantationstechnik
T-branch
AMS
PRÄOPERATIV NACH T-BRANCH
Dissertation | Michel Bosiers | Münster, 19.12.2014
13
Aber ...
• Branch-Verschlüsse / Reintervention
• Zugangsgefäße
• Paraparese/ Paraplegie
• Kontrastmittel/ OP-Zeit...
Branch Verschluss/ Re-Intervention
• Panuccio G et al. EJVES 2015
150 Patienten, 523 bridging Stents
13 Okklusionen (2%) 19 Re-Intervention (4%)
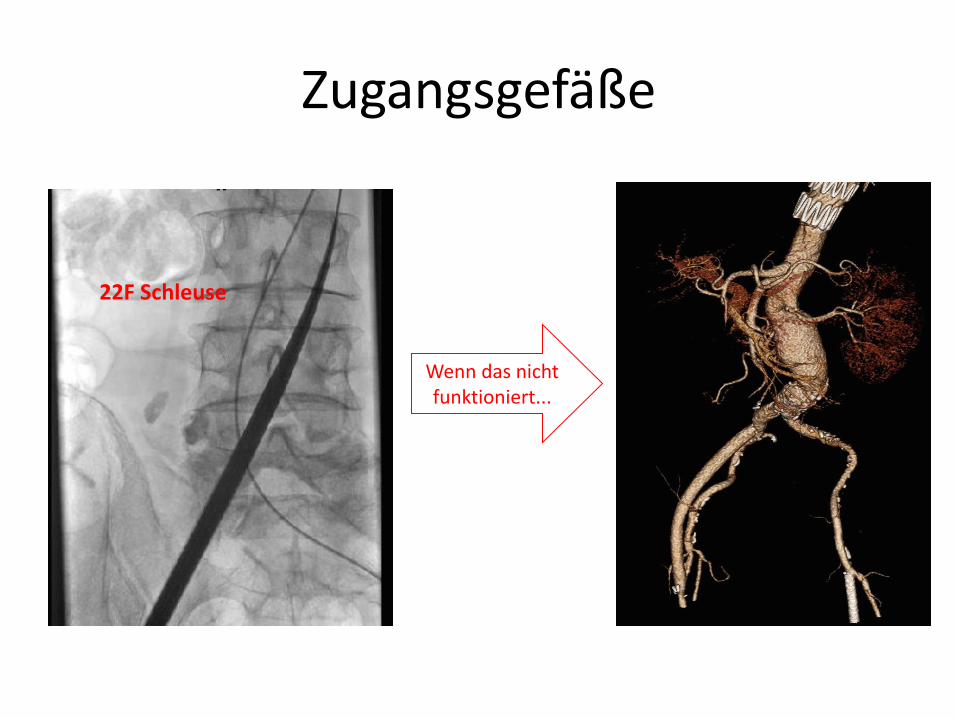
Zugangsgefäße
22F Schleuse
Wenn das nicht funktioniert...
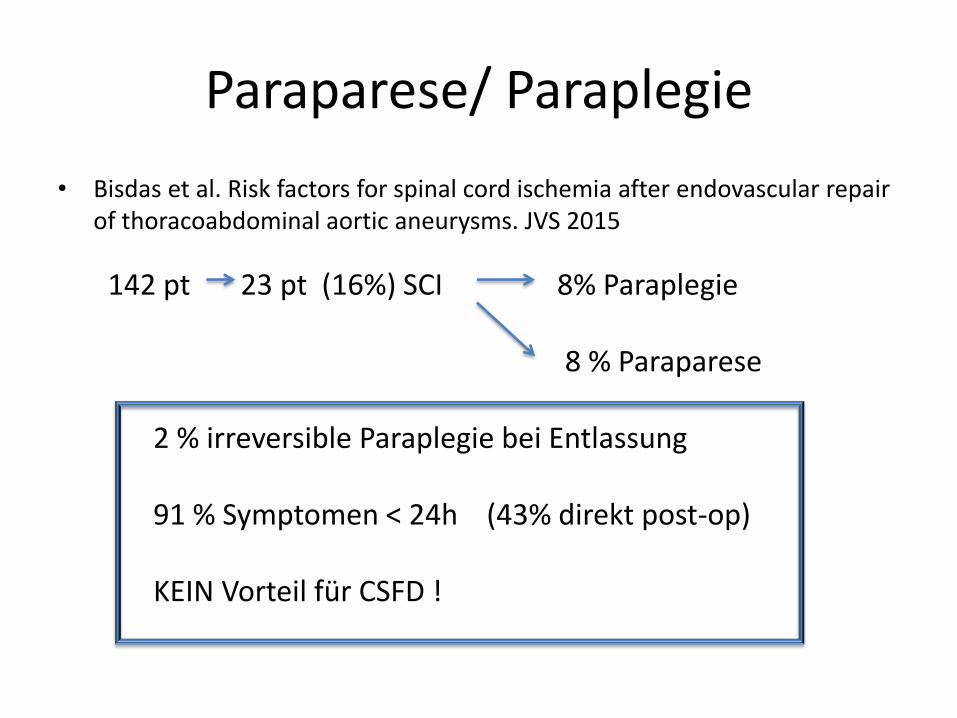
Paraparese/ Paraplegie
• Bisdas et al. Risk factors for spinal cord ischemia after endovascular repair of thoracoabdominal aortic aneurysms. JVS 2015
142 pt 23 pt (16%) SCI 8% Paraplegie 8 % Paraparese 2 % irreversible Paraplegie bei Entlassung 91 % Symptomen < 24h (43% direkt post-op) KEIN Vorteil für CSFD !
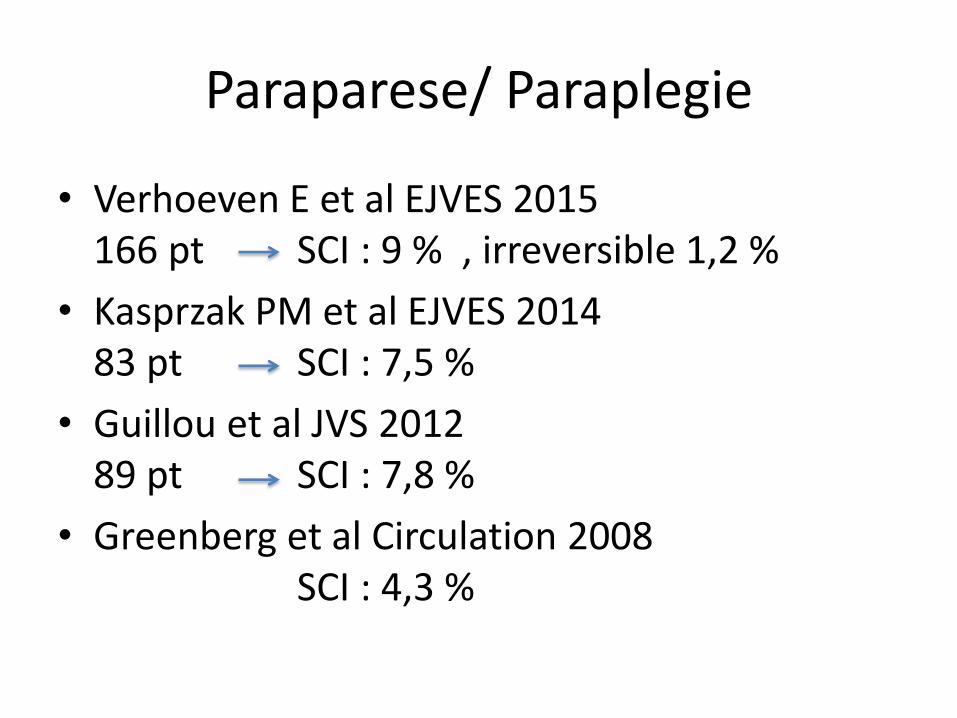
Paraparese/ Paraplegie
• Verhoeven E et al EJVES 2015 166 pt SCI : 9 % , irreversible 1,2 %
• Kasprzak PM et al EJVES 2014 83 pt SCI : 7,5 %
• Guillou et al JVS 2012 89 pt SCI : 7,8 %
• Greenberg et al Circulation 2008 SCI : 4,3 %
Paraparese/ Paraplegie
• Staged Procedure
• Vor Anschluss der Zielgefäße : „unten zu machen“
• Evt. Branch offen lassen
• Post-Op mindestens 24 h intensive Überwachung ( auch Pt wach machen nachts)
• Bei SCI -> CSFD, RR anheben, ggf. EK´s

Kontrastmittel/ OP-Zeit
• Fusion-Technik (z.B. Siemens) 2D/3D oder 3D/3D
Cost effectiveness?
• Armstrond N. et al. The use of fenestrated and branched endovascular aneurysm repair for juxtarenal and thoracoabdominal aneurysms: a systematic review and cost-effectiveness analysis. Health Technol Assess. 2014 Dec;18(70)
Conclusion : Despite a thorough search, no studies could be found that met the inclusion criteria. All studies that compared either fEVAR or bEVAR with either OSR or no surgery explicitly selected patients based on prognosis, i.e. essentially the populations for each comparator were not the same.
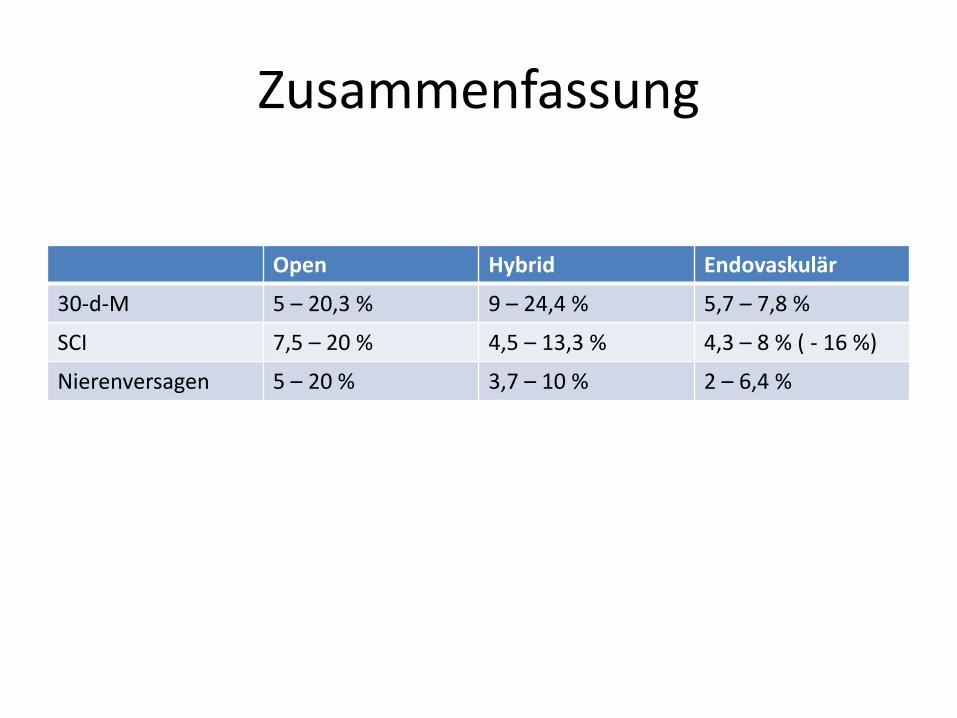
Zusammenfassung
Open Hybrid Endovaskulär
30-d-M 5 – 20,3 % 9 – 24,4 % 5,7 – 7,8 %
SCI 7,5 – 20 % 4,5 – 13,3 % 4,3 – 8 % ( - 16 %)
Nierenversagen 5 – 20 % 3,7 – 10 % 2 – 6,4 %
Zusammenfassung
• Endovaskuläre TAAA Chirurgie wird mehr und mehr zugepasst
• „off-the-shelf“ Endoprothese -> endo noch zugänglicher
• Deutliche Reduktion in Mortalität und Morbidität
• TAAA sollte weiterhin in hochspez. Zentren versorgt werden
• Nachkontrollen extrem wichtig (weiterhin viele Re-Interventionen)