Embed Size (px)
Citation preview
PD Dr. Gian Marco De Marchis, MScStv. Leiter der Stroke Unit Universitätspital Basel
STROKE & STROKE MIMICS
TIA Abklärung – wann ambulant?
¨ 68-jähriger Patient¨ 4 Stunden vorher: plötzliche Armlähmung rechts
über 15 Sekunden, ohne Schmerzen, vollständig regredient
¨ Erstmalige Episode¨ Neurostatus: unauffällig. BD 150/75 mmHg¨ CVRF: Art. Hypertonie, Raucher¨ Medikamente: Olmesartan + Amlodipin à Ambulante Abklärung oder Zuweisung ins Spital?
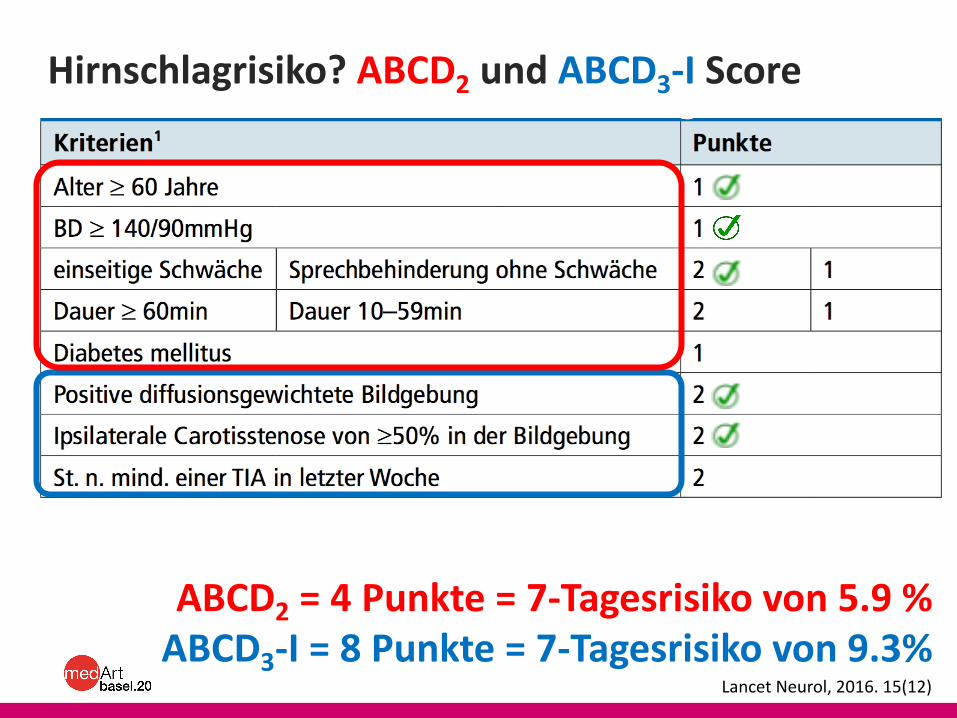
Hirnschlagrisiko? ABCD2 und ABCD3-I Score
Lancet Neurol, 2016. 15(12)
ABCD2 = 4 Punkte = 7-Tagesrisiko von 5.9 %ABCD3-I = 8 Punkte = 7-Tagesrisiko von 9.3%
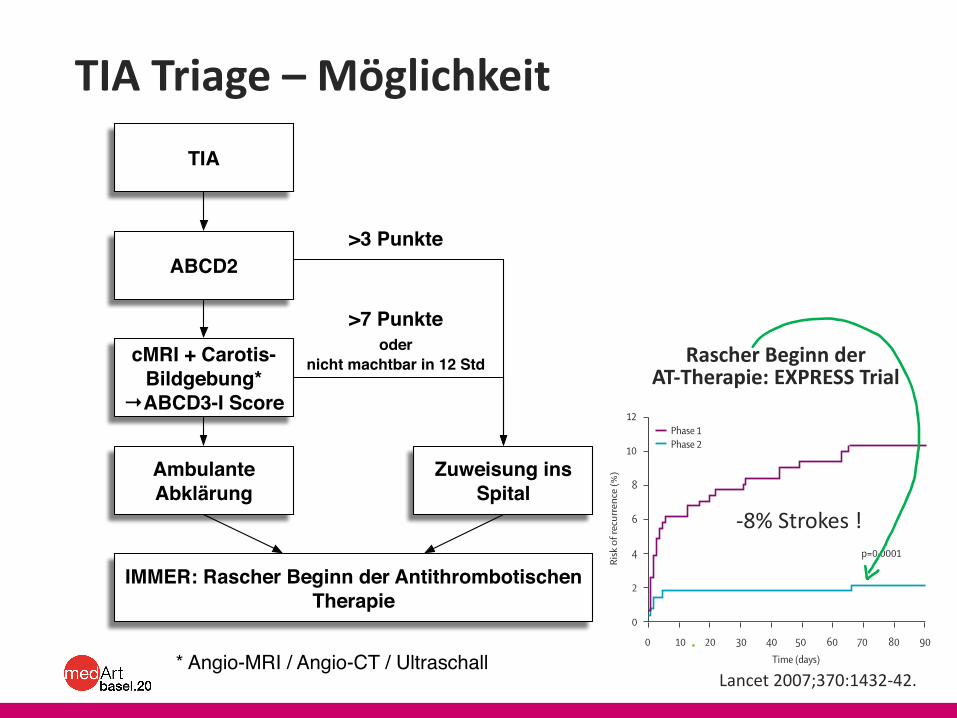
TIA Triage – Möglichkeit
Lancet 2007;370:1432-42.
TIA
ABCD2
Zuweisung ins Spital
cMRI + Carotis-Bildgebung*
→ABCD3-I Score
Ambulante Abklärung
>7 Punkteoder
nicht machtbar in 12 Std
>3 Punkte
* Angio-MRI / Angio-CT / Ultraschall
IMMER: Rascher Beginn der Antithrombotischen Therapie
Articles
1436 www.thelancet.com Vol 370 October 20, 2007
ResultsTable 1 shows the number of patients seeking medical attention after a fi rst event, stratifi ed by place of presentation and by type of fi rst event (probable or defi nite TIA or stroke). 51 patients sought medical attention after an event in both phases. 40 OXVASC patients presenting with subarachnoid haemorrhage and ten patients with stroke who died in the community before reaching medical attention were excluded; 23 patients who fi rst sought medical attention outside Oxfordshire were included.
For all patients seeking medical attention with TIA or stroke in the study population, and for all patients referred to the study clinic, baseline characteristics were much the same in the two phases of the study, except for a small increase in the proportion of patients using statins at presentation in phase 2 compared with in phase 1 (p=0·002 for both comparisons; table 2). There were no signifi cant diff erences between the phases in the numbers of patients not referred to secondary care, or in the proportion of patients who were referred or who self-referred to acute hospital services versus those referred to outpatient services (table 1). In patients presenting with TIA, there were also no signifi cant
diff erences in any of the components of the ABCD² score (data not shown).3
90-day follow-up data were available for all patients who presented with TIA or stroke in the study population, irrespective of where they initially sought medical
p=0·0001
Risk
of r
ecur
renc
e (%
)0
2
4
6
8
10
12
Time (days)0 10 20 30 40 50 60 70 80 90
Phase 1Phase 2
Figure 2: Risk of recurrent stroke after fi rst seeking medical attention in all patients with TIA or stroke who were referred to the study clinic
Phase 1 (n=310) Phase 2 (n=281) p
First call for medical attention*
≤12 h 128 (41·3%) 105 (37·5%) 0·35
≤24 h 184 (59·4%) 160 (57·1%) 0·62
First call for attention to assessment in study clinic†
≤6 h 5 (1·7%) 80 (29·0%) <0·0001
≤24 h 70 (23·4%) 163 (59·1%) <0·0001
*Data unavailable for one patient in phase 2. †Data unavailable for two patients in phase 2, and not applicable in a further 11 patients in phase 1 and three patients in phase 2 who were referred to the EXPRESS clinic but had a stroke and were admitted to hospital before the clinic assessment.
Table 4: Delay to seeking medical attention and subsequent delay in being seen in the clinic for all patients who were referred to the study clinic
Cum
ulat
ive
prop
ortio
n (%
)Cu
mul
ativ
e pr
opor
tion
(%)
Cum
ulat
ive
prop
ortio
n (%
)Cu
mul
ativ
e pr
opor
tion
(%)
Time from seeking medical attention (days)
00
10
10
20
20
30
30
40
40
50
50
60
60
70
70
80
80
90
90100
0102030405060708090
100
0102030405060708090
100
0102030405060708090
100Phase 1Phase 2
A
B
C
D
Figure 3: Cumulative proportions of patients prescribed new medication since fi rst seeking medical attention(A) Any statin drug (in patients not already on a statin); (B) clopidogrel (usually in addition to aspirin); (C) initiation of a fi rst blood-pressure-lowering drug (in patients not already on such medication); (D) initiation of two blood-pressure-lowering drugs (in patients previously on none or only one drug). Clopidogrel was given for 4 weeks only.
Rascher Beginn der AT-Therapie: EXPRESS Trial
-8% Strokes !
STROKE MIMICS
Raupe Mango Baron (Euthalia Aconthea)
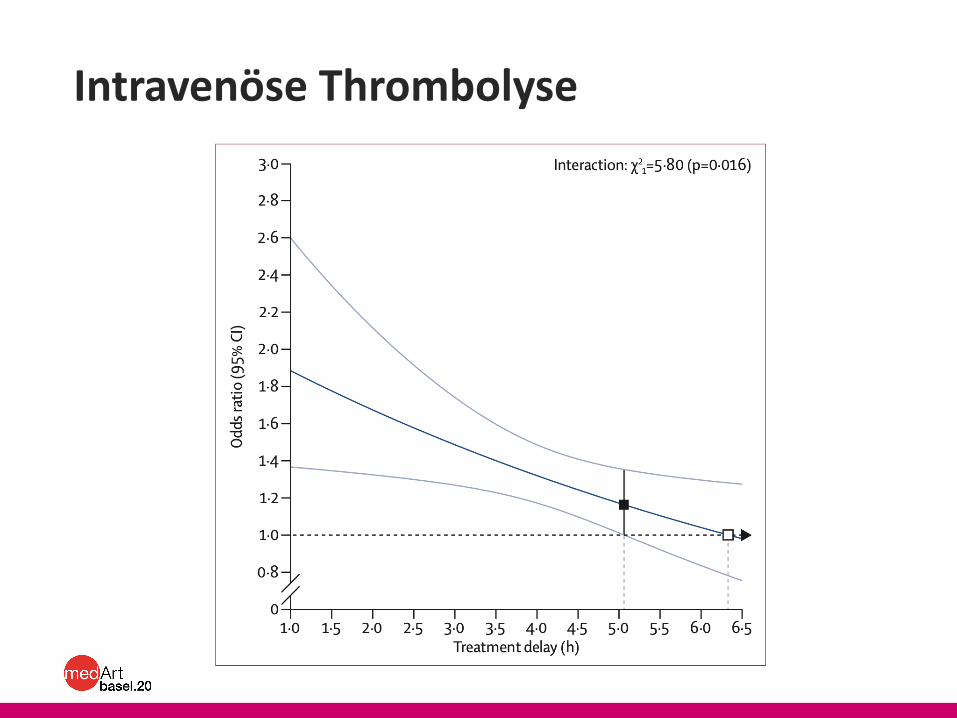
Intravenöse Thrombolyse
Stroke Mimics (SM)
¨ Bis 10% aller Patienten, die eine i.v. Thrombolyse erhalten, erweisen sich – im Nachhinein – als SM.
¨ 3 häufigste SMs:1. Migräne mit Aura (cMRI / Triptane)2. Epileptischer Anfall / Todd‘sche Parese (EEG / Anti-
ep.)3. Psychogene Symptomen (Psychiatrische
Konsultation)¨ SM: Intrakranielle Blutungsrate = 0.3%
¤ Beim „echten“ Hirnschlag 3-5%
Stroke, 2015. 46(5)Annals of Neurology, 2019

STROKE CHAMÄLEONS
STROKE CHAMÄLEONS
¨ 2% aller akuten Hirnschlagfälle: initial fehldiagnostiziert
¨ 1 aus 4 der Stroke Chamäleons: hätte für die i.v. Thrombolyse qualifiziert
¨ Stroke Chamäleon = ungünstige Prognosen
Neurology, 2015. 85(6)
TAKE-HOME MESSAGES
¨ TIA können auch Sekunden andauern¨ Stationär wenn ABCD2 > 3 Pkt. oder ABCD3-I > 7
Pkt. ¨ Antithrombotische Therapie: Beginn am gleichen
Tag (NNT = 12)¨ Outlook: NT-pro-BNP1 / MR-pro-ANP2 / Copeptin3:
¤ Individualisierung der Dauer vom Herzrhythmus-Monitoring
¤ Prognoseeinschätzung1 Int J Cardiol, 2020
2 Neurology, 20183 Stroke, 2014





























