Embed Size (px)
Citation preview

DOI:10.3966/207321472018061002004
通訊作者鄧景宜為長庚大學企業管理研究所教授、長庚紀念醫院林口總院復健科合聘研究員、明志科技大學經營管理系合聘教
授,地址:桃園市龜山區文化一路 259 號,電話:+886-3-2118800 ext. 5418,E-mail: [email protected]。作者張皓媛為國立
台灣大學醫學院護理系助理教授、臺大醫院護理部兼任督導,地址:100 台北市中正區仁愛路一段 1 號,電話:+886-2-23123456
ext. 88893,E-mail: [email protected]。作者徐亞瑛為長庚大學護理系教授,地址:桃園市龜山區文化一路 259 號,電話:
+886-3-2118800 ext. 5736,E-mail: [email protected]。作者黃美涓為長庚醫院桃園分院院長,地址:333 桃園市龜山區頂湖
路 123 號,電話:+886-3-3196200 ext. 2378,E-mail: [email protected]。作者朱宗藍為長庚醫院行政中心品管組組長,地
址:333 桃園市龜山區頂湖路 123 號,電話:+886-3-3196200 ext. 3385,E-mail: [email protected]。作者林思敏為衛生福利
部統計處研究助理。地址:11558 台北市南港區忠孝東路 6 段 488 號,電話:+886-2-85906666,E-mail: [email protected]。
商 略 學 報
151
護理人員的人力資源策略:嚴謹性與神經質人格特質
對病人安全的正面影響
張皓媛 國立臺灣大學
徐亞瑛 長庚大學
黃美涓 長庚醫院
朱宗藍 長庚醫院
林思敏 衛生福利部
鄧景宜 長庚大學
論文編號:IJCS2017028
收稿 2017 年 5 月 22 日→第一次修正 2017 年 11 月 12 日→正式接受 2017 年 12 月 21 日
過去研究已經發現嚴謹性對病人安全有正向的影響力,但尚未有研究探討是否神經質會調節這樣的影
響力。若有研究探討此不足之處將可提供提升病人安全的方式。因此,本研究的目的為探討護理人員人格
特質中的嚴謹性與神經質的交互作用對病人安全的影響力。本研究採用橫斷面的調查研究法,使用短題版
的人格特質量表 Mini-Markers,本研究的樣本為台灣的兩家醫學中心中的 313 位護理人員。病人安全採用
六種病人安全事件來衡量。採用迴歸分析來檢測研究假說。本研究發現護理人員的嚴謹性與神經質的交互
作用的確會對病人安全的結果有預測力(β = -.15, p = .01)。對於低神經質的護理人員,嚴謹性與病人安全
有正向關係(β = .30, p = .00)。對於高神經質的護理人員,嚴謹性與病人安全間的正向關係則不顯著 (β
= .11, p = .21)。管理者可以提供訓練課程、放鬆課程、或者營造支持團體來逐漸增進護理人員的嚴謹性與
降低神經質,或有助於病人安全。管理者可考慮採取漸進提升護理人員嚴謹性與降低神經質外顯行為的方
式,可能有助於提升病人安全。
關鍵字:病人安全、醫院護理人員、嚴謹性、神經質、交互作用。

DOI:10.3966/207321472018061002004
The Corresponding Author, Ching-I Teng, is a Professor in the Graduate Institute of Business and Management, Chang Gung University;
Adjunct Research Fellow, Department of Rehabilitation, Chang Gung Memorial Hospital, Linkou, Taiwan; Adjunct Professor, Department
of Business and Management, Ming Chi University of Technology, Address: No. 259, Wenhua 1st Rd, Gueishan, Taoyuan 333, Taiwan,
Tel: +886-3-2118800 ext. 5418, E-mail: [email protected] Hao-Yuan Chang, is an Assistant Professor in the School of Nursing,
College of Medicine, National Taiwan University; Adjunct Supervisor, Department of Nursing, National Taiwan University Hospital,
Address: No. 1, Sec. 1, Ren-Ai Rd, Taipei 100, Taiwan, Tel: +886-2-23123456 ext. 88893, E-mail: [email protected] Yea-Ing Lotus
Shyu, is a Professor in the School of Nursing, Chang Gung University, Address: No. 259, Wenhua 1st Rd, Gueishan, Taoyuan 333,
Taiwan, Tel: +886-3-2118800 ext. 5736, E-mail: [email protected] May-Kuen Wong, is the Chair of the Taoyuan Branch, Chang
Gung Memorial Hospital, Address: No. 123, Ding-Hu Rd, Taoyuan 333, Taiwan, Tel: +886-3-3196200 ext. 2378, E-mail:
[email protected] Tsung-Lan Chu, is the Chief Manager of the Quality Management Department, Administration Center, Chang
Gung Memorial Hospital, Address: No. 123, Ding-Hu Rd, Taoyuan 333, Taiwan, Tel: +886-3-3196200 ext. 3385, E-mail:
[email protected] Si Man Lam, is a research assistant of Ministry of Health and Welfare Department of Statistics, Taiwan,
Address: No. 488, Sec. 6, Zhongxiao East Rd., Taipei 11558, Taiwan, Tel: +886-2-33668000, E-mail: [email protected]
152
Human Resource Strategies for Nurses: The Positive Impact
of Conscientiousness and Neuroticism on Patient Safety
Hao-Yuan Chang National Taiwan University
Yea-Ing Lotus Shyu
Chang Gung University
May-Kuen Wong Chang Gung Memorial Hospital
Tsung-Lan Chu
Chang Gung Memorial Hospital
Si Man Lam
Ministry of Health and Welfare
Ching-I Teng
Chang Gung University
Paper No.:IJCS2017028
Received May 22, 2017→First Revised November 12, 2017→Accepted December 21, 2017
This study investigates the influence on patient safety of the interaction between nurse personality traits, i.e.,
conscientiousness and neuroticism. Previous studies have identified the positive impact of conscientiousness on
patient safety but little is known about how neuroticism moderates this impact. Research on this issue provides a
means for enhancing patient safety. This study is a cross-sectional survey in which personality traits, i.e.,
conscientiousness and neuroticism, are measured by items from Mini-Markers. The sample comprised 313 nurses
from two medical centers in Taiwan. Patient safety outcomes were measured using frequencies of six adverse events.
Regressions were used. Analytical results indicated that the effect of the interaction between nurse
conscientiousness and neuroticism significantly predicts a range of patient safety outcomes (β = -.15, p = .01). For
nurses with low neuroticism, conscientiousness was positively related to patient safety (β = .30, p = .00). For nurses
with high neuroticism, the correlation between conscientiousness and patient safety was not observed (β = .11, p
= .21). It is suggested that nursing managers increase nurse conscientiousness and decrease neuroticism to
potentially improve patient safety. Nursing managers may provide training courses, relaxation courses, and support
groups to gradually increase nurse conscientiousness and decrease nurse neuroticism to improve patient safety
outcomes.
Key Words: Patient Safety, Hospital Nurses, Conscientiousness, Neuroticism, Interaction.

2018
153 H.-Y. Chang, Y.-I. Shyu, M.-K. Wong, T.-L. Chu, S.-M. Lam and C.-I. Teng
Introduction
Patient safety—the degree to which patient
health is not threatened during care (Institute of
Medicine, 2003)—is essential to securing patient
health and continues to receive considerable attention
in the global health care sector (Aiken et al., 2003;
Rainer, 2015; Vogelsmeier et al., 2010). Frontline
clinicians, such as nurses, are at the coalface of patient
safety and are thus essential to any efforts to improve
it (Joyce et al., 2011). While robust hospital systems
may be in place to help ensure patient safety—i.e.,
fewer injuries due to care; fewer patient falls,
nosocomial infections, and medication administration
errors; less incomplete/incorrect documentation; and
fewer delays in patient care (Teng et al., 2012)—the
traits of individual hospital personnel may interact
with these to enhance or reduce patient safety. An
exploration of such traits can ensure that institutional
efforts work in concert with individual strengths to
increase patient safety.
Among frontline clinicians, nurses fulfill
multiple roles, which imposes intense time pressure on
them. In such a high-pressured situation, efficiency
can help individuals meet the demands of their work.
Moreover, healthcare settings require nurses to work
carefully. Working efficiency and carefulness are two
key elements of an influential personality
trait—conscientiousness (Saucier, 1994)—justifying
this study‟s adoption of conscientiousness.
Conscientiousness, the tendency to be efficient and
careful, may help improve care outcomes because it
improves job performance in multiple disciplines
(Barrick et al., 2001). Nursing workplaces are highly
stressful, sometimes resulting in individuals feeling
nervous and anxious. The tendency to be nervous and
anxious is at the core of another influential personality
trait (Saucier, 1994)—neuroticism—justifying its
adoption in this study. Neuroticism is related to
perceived stress (Luo and Roberts, 2015), indicating
its suitability in this research context. Moreover,
neuroticism is a personality trait that has been
frequently examined together with conscientiousness
(Buchanan, 2017; Chen et al., 2016; Cheng et al.,
2017), further supporting our inclusion of both traits.
A low level of neuroticism—the tendency to be
nervous, anxious, and temperamental (Saucier,
1994)—or a high level of emotional stability, may
improve patient safety outcomes, because emotional
stability enables nurses to make optimal decisions
without the interference of negative emotions.
Nevertheless, the interaction of
conscientiousness and neuroticism has not been
investigated, revealing a knowledge gap. Research
addressing this gap contributes to nursing literature by
providing a novel means for enhancing patient safety,
and thus is important to nursing managers. Therefore,
the purpose of this study is to investigate the effects of
the interaction between nurse conscientiousness and
neuroticism on patient safety.
This study is unique to nursing literature in
several aspects. First, where La Fuente et al. (2015)
examined the relation between neuroticism and
nursing burnout, this study examined the impact of
neuroticism in nursing contexts but explored whether
it contributes to patient safety, extending our
knowledge on the impact of neuroticism on nursing
outcomes.
Second, where Fornés-Vives et al. (2012)
indicated that stress increased neuroticism among
student nurses and that life events could modify
personality traits, the present study concurred that
personality traits can be modified, and thus be
managed. Moreover, the present study examined
neuroticism among nurses, broadening the application
of nursing neuroticism theories.
Third, where Yu and Perng (2014) found that the
number of reported adverse events among nurse aids
was related to years of work experience, and
concluded that on-the-job training focusing on care
delivery could be effective in maintaining care quality,
the present study examined the occurrence of adverse
events among nurses rather than nurse aids, and
included nurse neuroticism and conscientiousness to

154 International Journal of Commerce and Strategy June
provide further guidance for designing training
courses.
Literature Review
Patient Safety
Patient safety has been a recent focus of health
care studies and can be assessed using the actual rate
of adverse events and near misses. Adverse events are
patient injuries due to care and thus are generally the
focus of hospital administrators. However, near misses
are events that may have resulted in accident, disease
or injury, but did not ultimately prove harmful to
patients (Berntsen, 2004). Since near misses also
represent opportunities and valuable lessons for
improving patient safety, they have been deemed
relevant in previous studies (e.g., Berntsen, 2004).
Patient safety has been assessed by objective
measures (Aiken et al., 2003) and subjective measures
(Teng et al., 2009). Objective measures are helpful for
statistical purposes and cross-unit comparison but
mainly come from hospital records, which nurses or
health care professionals may regard as threatening to
their careers. Thus objective measures may not
include all adverse events and near misses. In a recent
cross-sectional survey study (Kim et al., 2011), only
28.3% of participants submitted an incident report of
adverse events. However, nurses‟ reports of quality are
related to patient safety. Subjective (or self-reported)
measures thus appear to be a useful means of
measuring patient safety (Spence Laschinger and
Leiter, 2006; Teng et al., 2009). Thus this study
utilized subjective measures for assessing error.
Incomplete or incorrect documentation, delayed
patient care, medication administration errors, patient
falls, injuries due to care, and nosocomial infection
(Cina-Tschumi et al., 2009; Teng et al., 2009) were
frequently measured.
The literature on patient safety has examined its
antecedents, including nurse emotions (Smith et al.,
2009), nurse emotional stability (Teng et al., 2009),
nurse interventions (Kelly et al., 2011), and
rechecking when preparing and administrating
medicine (Kim et al., 2011). Such findings indicate the
critical role of nurses in patient safety assurance.
To explain how nurses can ensure patient safety,
the signal detection theory (Wickens, 2001)—which
posits that the sensitivity of an individual can help
identify relevant signals amid irrelevant background
noise—may be appropriate. The theory also posits that
sensitivity to, and the ability to identify, relevant
signals depends on individual factors such as training
levels and degree of fatigue (Wickens, 2001) and can
thus be applied to this study. Nurses who are careful
and systematic in conducting care routines are more
likely to be sensitive in detecting risks to patient safety,
indicating the relevance of nurse conscientiousness.
Conscientiousness and Neuroticism
Conscientiousness and neuroticism are known as
influential personality traits. These two traits have
frequently been included in the Big Five personality
traits (Barrick et al., 2001; McCrae and Costa, 1985).
Highly conscientious individuals are careful,
responsible, efficient and systematic (Barrick et al.,
2001; McCrae and Costa, 1985) and are also highly
motivated to learn (Major et al., 2006). In health
contexts, nurses are at the frontline of patient care, and
thus are critical to patient safety. Nurses who are
highly careful, responsible and systematic are likely to
deliver high quality care and make few errors.
Moreover, a high level of conscientiousness predicts
nurses‟ intention to stay, i.e., to continue working as
nurses (Chen et al., 2016). Hence, nurse
conscientiousness should be considered in studies
addressing the relationship between the personality of
health professionals and patient safety.
In addition to conscientiousness, neuroticism is
also an influential personality trait. Neuroticism
indicates an individual‟s tendency to be nervous,
anxious and temperamental (Saucier, 1994). Previous
studies have used a high level of neuroticism and a
low level of emotional stability interchangeably (Teng
et al., 2009).

2018
155 H.-Y. Chang, Y.-I. Shyu, M.-K. Wong, T.-L. Chu, S.-M. Lam and C.-I. Teng
Although neuroticism is generally regarded as a
deficiency, it can have positive results, e.g., increased
commitment to a goal (Bipp and Kleinbeck, 2011) and
improved training outcomes (Studer-Luethi et al.,
2012). These positive impacts of neuroticism indicate
that it is an influential trait, and not necessarily a
deficiency.
Neuroticism can be adjusted (Nelis et al., 2009;
Williams et al., 2006) and negative emotions
associated with neuroticism regulated or alleviated
(Johnson, 2009). In practice, training is one of the
most mentioned means for reducing neuroticism or
regulating negative emotions (Williams et al., 2006;
Yang & Wang, 2001).
In nursing contexts, neuroticism (or a low level
of emotional stability) was found to affect
patient-perceived care quality (Teng et al., 2007) and
patient safety measures (Teng et al., 2009), indicating
that neuroticism should be considered with regard to
patient outcomes. Moreover, a low level of
neuroticism predicts intention to stay, i.e., to continue
working as nurses (Chen et al., 2016), supporting its
influence in nursing contexts.
Yet, the interactive effect of conscientiousness
and neuroticism on patient safety outcomes has been
investigated neither in nursing nor in other disciplines,
revealing a knowledge gap. Research addressing this
gap thus contributes new knowledge to nursing
management by elucidating how the interaction of
personality traits impacts patient safety outcomes.
Knowledge of such an interaction may also provide
additional means for enhancing patient safety, and
thus is vital to nursing managers.
Hence, the purpose of this study is to investigate
the interactive effects of conscientiousness and
neuroticism on a range of patient safety outcomes.
Hypotheses Development
The signal detection theory indicates that
individual sensitivity can help an individual detect
relevant signals amid irrelevant noise (Wickens, 2001).
This theory can be applied to the present study since
nurses receive abundant patient information when
working and some of the information is critical for
patient safety. The signal detection performance (in
terms of perceptual sensitivity) is related to
conscientiousness (Rose et al., 2002). That is, the
signal detection theory could be used to build a
positive link between conscientiousness and
performance in signal detection.
Moreover, to explain the moderating influences
of neuroticism, the processing efficiency theory
(Eysenck and Calvo, 1992) is useful, since it posits
that individuals with strong emotions are hindered in
their efforts to complete tasks. This theory explains
how negative emotions may hamper an individual‟s
information processing, and thus may be applicable to
explaining the moderating role of neuroticism in
evoking negative emotions. As such, the processing
efficiency theory appears adequate for application to
this study.
Personality theory posits that conscientiousness
is characterized by carefulness (Rikoon et al., 2016),
and thus is widely recognized as contributing to job
performance (Barrick et al., 2001), including in
perceptual sensitivity (Rose et al., 2002). This is
reasonable, since conscientiousness boosts attention
(Huang and Bramble, 2016). According to the signal
detection theory (Wickens, 2001), perceptual
sensitivity can help individuals detect relevant signals.
Applied in nursing contexts, highly conscientious
nurses thus possess enhanced perceptual sensitivity to
detect relevant signals of potential threats to patients,
enabling them to improve patient safety outcomes, and
thus establishing a positive link between
conscientiousness and patient safety outcomes.
On the other hand, the influence of
conscientiousness on job performance may depend on
other factors such as neuroticism (as in Witt et al.,
2004). Thus the inclusion of neuroticism in the present
study is essential. Among personality traits,
neuroticism is widely used in psychological fields and
seen to be influential because it indicates an
individual‟s tendency to be nervous, anxious and

156 International Journal of Commerce and Strategy June
temperamental (Barrick et al., 2001; McCrae and
Costa, 1985) or to display a low level of emotional
stability (Williams et al., 2006). A low level of
emotional stability (or neuroticism) predicts
hypertension in adulthood (Cheng et al., 2017) and
failure in memory retrieval (Buchanan, 2017).
Neuropsychological studies have indicated that
negative emotions may hinder information-processing
capabilities (Conway and Giannopoulos, 1993),
suggesting that neuroticism may have such an effect.
Applying the processing efficiency theory (Eysenck
and Calvo, 1992)—which, as we have said, also
predicts that negative emotions are likely to hinder
individual decision-making capabilities—to health
care practice, nurses with low neuroticism rarely have
negative emotions that would affect their
information-processing capabilities (including the
ability to detect relevant signals on potential threats to
patients). In this case of minimum impact from
neuroticism, the positive link (as inferred by the signal
detection theory) between conscientiousness and
patient safety outcomes should be prominent.
Therefore, we hypothesize:
H1: For nurses with low levels of neuroticism,
conscientiousness is positively related to
patient safety outcomes.
However, nurses with high levels of neuroticism
frequently encounter negative emotions (Barrick et al.,
2001; McCrae and Costa, 1985), and, according to the
processing efficiency theory (Eysenck and Calvo,
1992), such emotions would restrain their ability to
process information (Conway and Giannopoulos,
1993), i.e., hindering their detection of signals on
potential threats to patients, even though
conscientiousness may provide them with perceptual
sensitivity. That is, the link between conscientiousness
and patient safety outcomes (as predicted above by the
signal detection theory) may not hold among nurses
with high levels of neuroticism. Therefore, we
hypothesize:
H2: For nurses with high levels of neuroticism,
conscientiousness is not related to patient
safety outcomes.
Methods
Sample and Data Collection Procedure
This study collected data in January 2008, using
questionnaires and a cross-sectional design. The issue
examined in this study remains relevant. The sample
comprised full-time registered nurses in 89 ward units
in two medical centers in northern Taiwan because
they had specialized departments and a large number
of nurses. The two medical centers had 90 ward units
in total. This study could not obtain access to one
ward unit and thus included all but that ward. That is,
this study included 89 out of 90 (98.9%). Such
inclusion of wards minimizes bias owing to sampling
wards.
The inclusion criteria for potential participants in
this study were: nurses who had licenses and worked
full-time. Most nurses in Taiwan work full-time, and
thus this criterion fits the population features. The
exclusion criteria were: head nurses, nursing
administrators and nursing students because their jobs
might have significantly differed from those of other
nurses. This study did not have access to the complete
list of the nurses in the two medical centers, and thus
the total number of nurses in the two medical centers
was not known. However, this study used
proportionate random sampling to ensure the sample‟s
representativeness in the sample distribution across
the units. Specifically, the randomization process was
conducted at the ward level, i.e., a third of nurses in
each ward were randomly sampled. For example, if
one ward unit had six nurses, two were randomly
sampled. Finally, 348 nurses in 89 wards were
recruited in this study. That is, the sample size was the
outcome of the entire data collection effort. No
previous similar studies could be used to infer the
sufficiency of the sample size. However, the sample
representativeness is warranted by the proportionate

2018
157 H.-Y. Chang, Y.-I. Shyu, M.-K. Wong, T.-L. Chu, S.-M. Lam and C.-I. Teng
random sampling process. Moreover, such a sample
size is consistent with the sample sizes in the recent
nursing studies using similar methods on related
topics (i.e., 362 in Cho et al., 2017; 323 in Johnson et
al., 2017).
The research assistants recruited for this study
did not work for either of the two medical centers.
Hence, nurses would be unlikely to be afraid of any
professional repercussions owing to their honest
responses to the study, reducing the intention of the
nurses to distort their responses. The research
assistants visited the ward units and sampled and
approached nurses who were eligible for participation.
The assistants then informed them of the study and
solicited their participation. Each participant spent
about 10 minutes filling in the questionnaire, and
received an envelope in which to enclose the
completed questionnaire, thus ensuring that
supervising nurses could not learn the responses,
helping reduce bias owing to participants‟ intention to
distort their responses. In total, 348 nurses were
approached, and 313 usable responses were gathered,
yielding an effective response ratio of 89.9%.
Ethical Considerations
The Institutional Review Boards (IRB) of the two
medical centers reviewed and approved the ethical
aspects of this study (96-0562B, 200706017R).
Participants were informed of the aim of this study
and agreed to participate.
Instruments
The six items measuring patient safety came
from Teng et al. (2009), who selected the items
applicable to multiple hospitalization units. Items
measuring patient safety were introduced by the
following: “In the past year, what was the frequency
of the following incidents that involved your clients or
yourself?” to enable the nurses to self-evaluate the
frequency of incidents involving patient safety. Items
measuring patient safety were adapted from previous
studies (Cina-Tschumi et al., 2009; Spence Laschinger
and Leiter, 2006). The six items measuring patient
safety were as follows: patient injury due to care,
patient falls, nosocomial infection, medication-related
administrative errors, incomplete or incorrect
documentation, and delayed care. The six items are
applicable across ward units and were used with
response options ranging from 1 (twice daily) to 9
(never). High scores represent high levels of patient
safety. These items have been applied to nursing and
had a Cronbach‟s α of .76 (Teng et al., 2009) or .79
(Teng et al., 2010). Moreover, these items have
exhibited sufficient convergent (λ .65) and
discriminant validity in the literature (Teng et al.,
2009). Responses to the six items were averaged for
subsequent analyses. Such an approach is consistent
with patient safety literature (e.g., Spence Laschinger
and Leiter, 2006; Teng et al., 2009).
Items measuring conscientiousness and
neuroticism came from the Mini-Markers of Saucier
(1994). The items measuring conscientiousness had a
Cronbach‟s α of .83 and the items measuring
neuroticism had a Cronbach‟s α of .78, indicating that
they had sufficient internal consistency. Since
questionnaire length may reduce response validity,
using a reduced scale is reasonable. Thus, this study
used the scale of Teng et al. (2007), which is a reduced
version of Saucier‟s (1994) Mini-Markers, for
measuring conscientiousness and neuroticism. The
items measuring conscientiousness (α = .82) and
neuroticism (α = .78) had an acceptable reliability.
Moreover, the scale exhibited sufficient reliability and
validity among nurse participants (as in Teng et al.,
2007), indicating adequate external validity. Five
items were used to measure conscientiousness and
neuroticism, respectively, as in Teng et al. (2007) and
in the present study. All items involved a response
option ranging from 1 (very disagreeable) to 7 (very
agreeable).

158 International Journal of Commerce and Strategy June
The study also collected information on nurse
gender, age, educational level, years of nursing
experience, and number patients cared for per day
shift. This study used SPSS17 and LISREL Version
8.54 as the analytical tools. The former was used to
compute the demographic distributions and conduct
the regression analyses. The latter was used for
conducting confirmatory factory analysis (CFA), an
analytical technique for effectively and thoroughly
examining measurement reliability and validity.
Psychometric Properties
This study conducted CFA to directly assess
measurement reliability and validity, consistent with
recent nursing studies (Chang et al., 2012). Results of
CFA are reported in this section to support the quality
of measurement. Table 1 summarizes the results. Items
measuring each construct had a Cronbach‟s α
exceeding .85. The minimum lower bound of 95%
confidence intervals for Cronbach‟s α exceeded .81.
Moreover, items measuring each construct had a
composite reliability (CR) exceeding .88 and average
variance extracted (AVE) exceeding .56, suggesting
that measures in this study had sufficient reliability. It
may be noted that the scores for patient safety were
high. The reason may be that the two medical centers
in this study are well established, with strong expertise,
sound management and continual improvement efforts.
Moreover, we were restrained from confirming the
absence of under-reporting.
Indicator loadings all exceeded .61 and had t
statistics exceeding 2 (the minimum t value was 9.90),
indicating satisfactory convergent validity. The
squared correlation for each pair of constructs was
below the AVE for each pair of constructs, indicating
Table 1 Summary of Confirmatory Factor Analysis
Construct Item Mean SD λ α C.I. of α CR AVE
Patient safety .85 [.81, .86] .88 .56
Injury due to care 8.41 1.37 .64
Patient falls 8.12 1.22 .67
Nosocomial infection 7.79 1.59 .76
Medication administration errors 7.93 1.48 .90
Incomplete/incorrect documentation 7.03 2.10 .74
Delayed patient care 7.13 2.39 .73
Conscientiousness .95 [.94, .96] .96 .81
I am efficient 4.64 1.25 .92
I am systematic 4.69 1.19 .99
I am organized 4.69 1.20 .97
I am careful 4.90 1.15 .82
I am conscientious 4.81 1.20 .79
Neuroticism .89 [.87, .91] .91 .68
I am high-strung 3.86 1.31 .61
I am nervous 4.19 1.53 .65
I am temperamental 3.59 1.43 .92
I am touchy 3.68 1.41 .96
I am moody 3.59 1.37 .91
Note: λ denotes indicator loading. CR denotes composite reliability, and AVE denotes average variance extracted.

2018
159 H.-Y. Chang, Y.-I. Shyu, M.-K. Wong, T.-L. Chu, S.-M. Lam and C.-I. Teng
discriminant validity for items measuring distinct
constructs.
Using confirmatory factor analysis, this study
had χ2 = 3020.48 and df = 566. If having a construct
representing the common method variance (CMV) and
assigning all items explained the CMV construct, the
model fit significantly degraded (χ2 = 8865.11 and df
= 594, Δχ2 = 5844.63, Δdf = 28, 5844.63 > χ2(df = 28,
α = 5%) = 41.34), indicating that the CMV model is
significantly worse than the original model. Such
analytical results support the minimum common
method bias of the measures in this study. Table 2 lists
the correlations between study constructs.
Analytical Processes
This study utilized hierarchical regression
analyses for testing the hypothesis on the interaction
of conscientiousness and neuroticism (results listed in
Table 4). Since the interaction term of
conscientiousness and neuroticism may be highly
correlated with either conscientiousness or
neuroticism, we adopted the suggestion of Neter et al.
(1996) by moving the means of conscientiousness and
neuroticism to zero to minimize such correlations and
the associated multicollinearity problem.
Additionally, we used the median split method to
separate the sample into two groups (median score =
3.80), namely for high neuroticism (scores ≥ 3.80, n =
152) and low neuroticism (scores < 3.80, n = 161).
Median split is a common means for analyzing
interaction effect, supporting our adoption of the
method. For each group, we tested the impact of
conscientiousness on patient safety using regression
analyses. The two groups did not differ markedly in
gender, age, educational level, years of experience in
nursing, or number of patients cared for (p > .29).
Nearly all respondents were female (98.1%).
Moreover, age, working experience in nursing, and
working experience in the current hospital were highly
correlated (r ranging from .74 to .95), inhibiting us
from entering all of them into regressions, which may
cause a serious multicollinearity problem. We chose
nurse age as the control variable in the regressions;
replacing it with working experience in nursing or in
the same hospital did not change the analytical results.
Results
Characteristics of the Sample
Table 3 describes the sample demographic profile.
Among the sample, 98.1% were female, 95.5% were
under 40 years of age, 96.8% had attended universities or
colleges, 77.9% had less than 10 years of experience in
nursing, and 81.8% cared for five to nine patients per day
shift. To retain the sample representativeness, the
responses that contained missing values on demographics
were still included in the analyses. Missing values were
6.8% of any item. Hence, we conducted pairwise
analyses.
Hypotheses Testing
Table 4 lists the analytical results. The interaction of
conscientiousness and neuroticism was significantly
related to patient safety (β = -.13, p < .05; ΔR2 = .02, p
< .05), supporting the study hypotheses and necessitating
further analyses on how the interaction term impacts
patient safety.
Table 2 Correlations between Study Constructs
Conscientiousness Neuroticism Patient safety
Conscientiousness ---
Neuroticism -.30** ---
Patient safety .24** -.04 ---
Note. ** denotes p < .01.

160 International Journal of Commerce and Strategy June
Table 5 lists the additional analytical results. For
nurses with low neuroticism, conscientiousness was
positively related to patient safety (β = .39, t = 3.42, p
= .00), supporting H1. However, for nurses with high
neuroticism, we did not observe any correlation
between conscientiousness and patient safety (β = .10,
t = 0.95, p = .34), supporting H2. The R2 value of the
regressions are .12 and .02, respectively. Cohen (1988)
indicated that R2 of .05 and .13 should be interpreted
as low and moderate effect size, respectively. That is,
the regression for nurses with low neuroticism had a
moderate effect size, while the regression for nurses
with high neuroticism had a low effect size. Moreover,
the variances explained by the model are consistent
with those in literature on personality, i.e., .07 in
Błachnio and Przepiorka (2016), .05 in Teng and Liu
(2014), and .08 in Matz et al. (2016). That is, the R2
values reported herein should be comparable to the
psychological literature, indicating a degree of clinical
relevance.
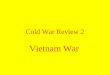
The alternative means to interpret the interaction
term in regression analysis is to plot the means for
groups at -1 and +1 standard deviation below and above
the mean. Figure 1 illustrates how the interaction term
impacts patient safety. Consistently, this study observed
that for nurses with low neuroticism, conscientiousness
Table 3 Demographic Characteristics of the Sample
Variable Category Frequency Percent (%)
Gender Female 307 98.1
Male 1 0.3
Missing 5 1.6
Age < 30 years old 228 72.8
≥ 30 but < 40 years old 71 22.7
≥ 40 but < 50 years old 6 2.0
≥ 50 but < 60 years old 1 0.3
Missing 7 2.2
Educational level University or college 303 96.8
Graduate institute 4 1.3
Missing 6 1.9
Years of experience in
nursing
< 1 year 62 19.8
≥ 1 but < 5 years 105 33.5
≥ 5 but < 10 years 77 24.6
≥ 10 but < 15 years 45 14.4
≥ 15 but < 20 years 14 4.5
≥ 20 years 3 1.0
Missing 7 2.2
Averaged number of
patients cared for
< 5 patients 8 2.6
≥ 5 but < 10 patients 256 81.8
≥ 10 but < 15 patients 33 10.5
≥ 15 patients 5 1.6
Missing 11 3.5

2018
161 H.-Y. Chang, Y.-I. Shyu, M.-K. Wong, T.-L. Chu, S.-M. Lam and C.-I. Teng
was positively related to patient safety scores. However,
for nurses with high neuroticism, conscientiousness was
not significantly related to patient safety scores. Such
analytical results also supported the study hypothesis.
Moreover, we did not observe any effects on
patient safety (p ≥ .13) of nurse educational level,
years of experience in nursing, and average number of
patients cared for. The Durbin-Watson statistics
ranged from 1.79 to 2.03, supporting the absence of
autocorrelations. Moreover, the variance inflation
factors were all below 10, indicating the absence of
multicollinearity, thus supporting the adequacy of
using regressions for analyses.
Discussion
Main Findings
This study found that for nurses with low
neuroticism, conscientiousness was positively
associated with improved patient safety outcomes, but
for nurses with high neuroticism, such a positive
association vanished. The reason may be that nurses
with low neuroticism are usually calm and thus their
conscientiousness yields carefulness (Barrick et al.,
2001; McCrae and Costa, 1985), which reduces errors.
Moreover, conscientiousness is positively related to
the use of a problem-focused coping strategy (Bartley
and Roesch, 2011). Hence, nurses with low
neuroticism who are highly conscientious likely
focused on solving problems so as to ensure patient
safety, increasing their performance in patient safety
outcomes. Moreover, according to the processing
efficiency theory (Eysenck and Calvo, 1992), nurses
Table 4 Interactive Influence of Conscientiousness and Neuroticism on Patient Safety
M1 M2 M3
Nurse Gender -.01 .00 .00
Nurse Age .14* .06 .04
Nurse Educational Level -.12* -.10 -.09
Medical Center .08 .12 .11
Conscientiousness .24* .23
Neuroticism .02 .03
Conscientiousness Neuroticism -.13*
R2 .19* .29* .31*
Adjusted R2 .04* .08* .10*
ΔR2 .04* .04* .02*
Note. Numbers are standardized beta coefficients. * denotes p < .05.
Table 5 Influence of Conscientiousness on Patient Safety among Nurses with Low or High Neuroticism
Nurses with Low Neuroticism Nurses with High Neuroticism
β C.I. of β t p β C.I. of β t p
Conscientiousness 0.39 [0.16, 0.61] 3.42 .00* 0.10 [-0.11, 0.32] 0.95 .34
Educational level -1.17 [-2.67, 0.33] -1.54 .13 -0.31 [-2.78, 2.16] -0.25 .80
Years of experience in
nursing -0.08 [-0.28, 0.12] -0.80 .43 0.06 [-0.16, 0.27] 0.53 .60
Number of patients
cared for 0.01 [-0.06, 0.07] 0.23 .82 0.04 [-0.06, 0.14] 0.74 .46
Note. * denotes p < .05.

162 International Journal of Commerce and Strategy June
with high neuroticism easily engage in negative
emotions that may block rational and optimal
decision-making, and thus restrain the influence of
their conscientiousness. Such an observation supports
the contention that the interaction of nurse
conscientiousness and neuroticism impacts patient
safety outcomes. It is suggested that this finding may
prove useful in enabling health service providers to
better understand the potential relationship between
the individual nurse‟s personality and patient safety
outcomes. Such an understanding could provide
insights that assist healthcare managers to better
design their systems to ensure patient safety.
Theoretical Implications
This study found that neuroticism (associated
with negative emotions) may block the positive
influence of conscientiousness on several patient
safety outcomes. In nursing management literature,
Smith et al. (2009) observed that emotional
intelligence influences patient safety, showing that the
negative emotions of nurses can hinder patient safety.
This study complements those findings in addressing
the influence of nurses‟ negative emotions on a range
of patient safety outcomes. As such, this study breaks
new ground for subsequent studies to investigate how
social psychological variables may impact on a range
of medical and health care outcomes.
An additional result of this study was that
education level was found to be unrelated to patient
safety outcomes. Aiken et al. (2003) identified nurse
education as a possible predictor for patient safety.
This study is in concordance with theirs in attempting
to replicate their findings at the individual level, but
did not observe a positive link between individual
nurse education and patient safety, showing that nurse
education may impact patient safety only at an
aggregated level, which requires further study to
verify.
Witt et al. (2002) investigated the interactive
effects of conscientiousness and extraversion, and
those of conscientiousness and agreeableness. The
present study followed theirs by investigating how
conscientiousness interacts with neuroticism.
This study found that neuroticism is pivotal in
the relationship between conscientiousness and patient
safety outcomes. Teng and colleagues found that
neuroticism has a direct relationship with care quality
(Teng et al., 2007) and patient safety (Teng et al.,
2009). Compared with those studies, the present study
is new in identifying neuroticism as a moderator,
rather than as a direct predictor, of health service
outcomes (i.e., patient safety outcomes).
This study found that the influence of
conscientiousness has a boundary condition (i.e.,
when the influence does not exist), that is, only when
nurses have low levels of neuroticism. Barrick et al.
(2001) found that conscientiousness had a
Figure 1 Interactive Effect of Nurse Conscientiousness and Neuroticism on Patient Safety
7.0
7.2
7.4
7.6
7.8
8.0
8.2
8.4
-1SD
Conscientiousness
+1SD
Pati
ent
safe
ty 8.6
(7.6)
(7.4) (7.8)
(8.2
)
High neuroticism
Low neuroticism

2018
163 H.-Y. Chang, Y.-I. Shyu, M.-K. Wong, T.-L. Chu, S.-M. Lam and C.-I. Teng
predominant influence on various job performance
measures in various occupations. Compared with
theirs, this study uniquely identified a boundary
condition for the influence of conscientiousness.
Implications for Managers
By conducting a short survey using the ten items
reported in this study, nursing managers could
measure the levels of nurses‟ conscientiousness and
neuroticism, as a base for further managing nurses and
patient safety. This study posits that negative emotions
originate from individual neuroticism. However, as
negative emotions can also originate from workplace
factors—such as lack of effective teamwork, working
in a blame culture, and hierarchical relationships
between professional groups—nursing managers
cannot look at the relationship between
conscientiousness and neuroticism in isolation; they
should take a holistic approach that considers both
nurse personality and the work environment. For
example, based on the findings of Chang et al. (2012),
nursing managers could learn how to manage their
mood to facilitate effective teamwork among nurses.
Nelis et al. (2009) noted that training could improve
emotional intelligence, which could help manage
moods.
The current study showed that the interaction
between conscientiousness and neuroticism could
affect patient safety. Specifically, the
conscientiousness of nurses with low neuroticism was
positively associated with patient safety, indicating the
relevance of reducing neuroticism. It may be
questioned whether a personality can be stabilized.
However, recent personality theories suggest that
personality can be markedly changed (Terracciano et
al., 2010). Emotional management programs have
been found effective in reducing neuroticism (Yang
and Wang, 2001). Thus these means for reducing
neuroticism or its impact may amplify the positive
influence of conscientiousness on patient safety.
Furthermore, support groups can help manage
negative emotions. Hence, it is suggested that nursing
managers encourage nurses to participate in such
groups.
Limitations and Future Research
Directions
Nursing personality includes a wide spectrum of
personality traits, revealing fertile research ground.
For example, nurse hardiness was found to be
negatively related to nursing burnout (Rich and Rich,
1987). Future studies are encouraged to explore the
impact of further personality traits among nurses or
explore the mechanism underlying the impact of
nursing personality on nursing job outcomes and
patient safety outcomes.
This study collected data from nurses in all
available units in the two chosen hospitals, thereby
maximizing the sample representativeness. One of the
two hospitals is public and the other privately owned,
increasing the generality of the study findings to both
public and private hospitals.
Although the data were collected almost a decade
ago, patient safety remains a critical issue, both in
clinical practice and in academics. Moreover, the
influence of personality traits is ongoing and unlikely
to dramatically change over time. Therefore, the use
of such data remains relevant.
Taiwanese nurses are required by law to have
licenses (equivalent to registered nurses) for working
in hospitals. Thus the participants in this study were
all registered nurses, restraining this study from
examining whether the proportion of registered nurses
to all staffed nurses impacted the study findings.
Future studies may replicate this study and explore
whether these findings might be moderated by the
proportion of registered nurses.
This study adopted a correlational design suitable
to its requirements. However, such a design is limited
in its ability to examine causality among the study
constructs. Therefore, future studies could examine
whether the current study‟s findings originate from
causality using longitudinal or experimental designs.
This study followed nursing literature (i.e.,

164 International Journal of Commerce and Strategy June
Cina-Tschumi et al., 2009; Spence Laschinger and
Leiter, 2006; Teng et al., 2009) in its use of subjective
measures, which avoided the problem of
underestimation of hospital-recorded adverse events
(as in Kim et al., 2011). Therefore, using subjective
measures for patient safety should be acceptable.
Moreover, this study had attempted to reduce
self-reported bias. However, using hospital-recorded
data can provide an alternative measurement approach.
Self-reported rates and hospital-recorded rates may
have large differences. Hence, future studies may
include objective measures as well as subjective
measures.
This study has attempted to reduce the response
bias on the reporting of patient safety. However, it was
still restrained from evaluating any potential
under-reporting of the adverse events. Future studies
may explore the possibility of using advanced
technologies to help detect the degree of correct
reporting.
This study did not intend to blame adverse events
on individuals. The literature on patient safety has
verified that systematic factors, rather than individual
ones, are usually at the root of failure in patient safety.
Therefore, future studies could further examine how
personality traits interact with systematic factors to
enhance or hinder patient safety. Such efforts could
contribute to the building of well-designed processes
of care to prevent, recognize, and quickly recover
from errors so that patients are not harmed.
Although this study examined individual
personality traits, its findings should not be used to
reduce the responsibility of health service
organizations to provide effective systems to ensure
patient safety. Moreover, the findings regarding
individual factors reflect the challenges encountered
by healthcare professionals, i.e., “to error is human”,
and thus should not be taken as any basis for blame.
This study found that personality traits are related
to patient safety. However, the explained variance of
patient safety was limited. Such a finding is
reasonable, since nursing personality traits may
impact patient safety via nurses‟ psychology and
behavior. Therefore, future studies aiming to fully
predict or ensure patient safety should include how
nursing personality traits impact nurses‟ psychology
and behavior, and subsequently patient safety.
This study follows the relevant literature (i.e., Teng
et al., 2009; Teng et al., 2010) to combine the scores
on the six adverse events. This means has been
acceptable for representing the patient safety concept
in the literature. However, it may be noted that the
six adverse events included in this study may have
widespread scores and thus may not be appropriate to
be used in combination. To check the potential
problem, we observed that the scores for the six
items ranged from 7.03 to 8.41 in a nine-point
response scale (from 1 to 9), thus the responses were
within a limited range. Nevertheless, future works
could explore problems associated widespread scores
on such items.
Conclusion
Using the processing efficiency theory and the
signal detection theory, this study developed a
hypothesis on the interactive effect of nurse
neuroticism and conscientiousness on patient safety,
and provided evidence supporting this hypothesis.
Conscientiousness increased the safety of patients
cared for by nurses with a low level of neuroticism,
but not for those cared for by nurses with a high level
of neuroticism. Further evidence is warranted to
confirm the causal relations between nursing
neuroticism, conscientiousness and patient safety. The
results of this study provide an additional means for
enhancing patient safety, and thus are important to
nursing managers. According to our findings, we
suggest hospital administrators provide emotional
management programs, relaxation courses and support
groups for nurses with high neuroticism to help
elevate patient safety.

2018
165 H.-Y. Chang, Y.-I. Shyu, M.-K. Wong, T.-L. Chu, S.-M. Lam and C.-I. Teng
References
Aiken, L. H., Clarke, S. P., Cheung, R. B., Sloane, D. M.
and Silber, J. H., 2003. Educational levels of
hospital nurses and surgical patient mortality.
Journal of the American Medical Association,
290(12), 1617-1623.
Barrick, M. R., Mount, M. K. and Judge, T. A., 2001.
Personality and performance at the beginning of
the new millennium: What do we know and where
do we go next? International Journal of Selection
and Assessment, 9(1,2), 9-30.
Bartley, C. E. and Roesch, S. C., 2011. Coping with daily
stress: The role of conscientiousness. Personality
and Individual Differences, 50(1), 79-83.
Berntsen, K. J., 2004. Valuable lessons in patient safety:
Reporting near misses in healthcare. Journal of
Nursing Care Quality, 19(3), 177-179.
Bipp, T. and Kleinbeck, U., 2011. The effect of
neuroticism in the process of goal pursuit.
Personality and Individual Differences, 51(4),
454-459.
Błachnio, A. and Przepiorka, A., 2016. Personality and
positive orientation in Internet and Facebook
addiction. An empirical report from Poland.
Computers in Human Behavior, 59, 230-236.
Buchanan, T., 2017. Self-assessments of memory
correlate with neuroticism and conscientiousness,
not memory span performance. Personality and
Individual Differences, 105, 19-23.
Chang, H.-Y., Teng, C.-I., Chu, T.-L., Chang, H.-T. and
Hsu, W.-H., 2012. Impact of nurse agreeableness
and negative mood of nursing supervisors on
intention to help colleagues. Journal of Advanced
Nursing, 68(3), 636-646.
Chen, L.-C., Perng, S.-J., Chang, F.-M. and Lai, H.-L.,
2016. Influence of work values and personality
traits on intent to stay among nurses at various
types of hospital in Taiwan. Journal of Nursing
Management, 24(1), 30-38.
Cheng, H., Montgomery, S., Treglown, L. and Furnham,
A., 2017. Emotional stability, conscientiousness,
and self-reported hypertension in adulthood.
Personality and Individual Differences, 115,
159-163.
Cho, S.-H., Mark, B. A., Knafl, G., Chang, H. E. and
Yoon, H.-J., 2017. Relationships between nurse
staffing and patients‟ experiences and the mediating
effects of missed nursing care. Journal of Nursing
Scholarship, 49(3), 347-355.
Cina-Tschumi, B., Schubert, M., Kressig, R. W., De
Geest, S. and Schwendimann, R., 2009.
Frequencies of falls in Swiss hospitals:
Concordance between nurses‟ estimates and fall
incident reports. International Journal of Nursing
Studies, 46(2), 164-171.
Cohen, J., 1988. Statistical power analysis for the
behavioral sciences, 2nd ed. Hillsdale, NJ:
Lawrence Erlbaum Associates.
Conway, M. and Giannopoulos, C., 1993. Dysphoria and
decision making: Limited information use for
evaluations of multiattribute targets. Journal of
Personality and Social Psychology, 64(4), 613-623.
Eysenck, M. W. and Calvo, M. G., 1992. Anxiety and
performance: The processing efficiency theory.
Cognition & Emotion, 6(6), 409-434.
Fornés-Vives, J., García-Banda, G., Frías-Navarro, D.,
Hermoso-Rodríguez, E. and Santos-Abaunza, P.,
2012. Stress and neuroticism in Spanish nursing
students: A two-wave longitudinal study. Research
in Nursing & Health, 35(6), 589-597.
Huang, J. L. and Bramble, R. J., 2016. Trait, state, and
task-contingent conscientiousness: Influence on
learning and transfer. Personality and Individual
Differences, 92, 180-185.
Institute of Medicine, 2003. Patient safety: Achieving a
new standard for care. Institute of Medicine,
Washington.
Johnson, D. R., 2009. Goal-directed attentional
deployment to emotional faces and individual
differences in emotional regulation. Journal of
Research in Personality, 43(1), 8-13.
Johnson, J., Louch, G., Dunning, A., Johnson, O., Grange,
A., Reynolds, C., Hall, L. and O‟Hara, J., 2017.
Burnout mediates the association between
depression and patient safety perceptions: A
cross-sectional study in hospital nurses. Journal of
Advanced Nursing, 73(7), 1667-1680.
Joyce, J. S., Cioffi, G. A., Petriwsky, J. G. and Robinson,
J. S., 2011. Legacy health‟s „big aims‟ initiative to

166 International Journal of Commerce and Strategy June
improve patient safety reduced rates of infection
and mortality among patients. Health Affairs, 30(4),
619-627.
Kelly, J., Wright, D. and Wood, J., 2011. Medicine
administration errors in patients with dysphagia in
secondary care: A multi-centre observational study.
Journal of Advanced Nursing, 67(12), 2615-2627.
Kim, K. S., Kwon, S.-H., Kim, J.-A. and Cho, S., 2011.
Nurses‟ perceptions of medication errors and their
contributing factors in South Korea. Journal of
Nursing Management, 19(3), 346-353.
La Fuente, G. A. C.-D., Vargas, C., San Luis, C., García,
I., Cañadas, G. R. and La Fuente, E. I. D., 2015.
Risk factors and prevalence of burnout syndrome
in the nursing profession. International Journal of
Nursing Studies, 52(1), 240-249.
Luo, J. and Roberts, B. W., 2015. Concurrent and
longitudinal relations among conscientiousness,
stress, and self-perceived physical health. Journal
of Research in Personality, 59, 93-103.
Major, D. A., Turner, J. E. and Fletcher, T. D., 2006.
Linking proactive personality and the Big Five to
motivation to learn and development activity.
Journal of Applied Psychology, 91(4), 927-935.
Matz, S. C., Gladstone, J. J. and Stillwell, D., 2016.
Money buys happiness when spending fits our
personality. Psychological Science, 27(5), 715-725.
McCrae, R. R. and Costa, P. T. Jr., 1985. Updating
Norman‟s “adequate taxonomy”: Intelligence and
personality dimensions in natural language and in
questionnaires. Journal of Personality and Social
Psychology, 49(3), 710-721.
Nelis, D., Quoidbach, J., Mikolajczak, M. and Hansenne,
M., 2009. Increasing emotional intelligence: (How)
is it possible? Personality and Individual
Differences, 47(1), 36-41.
Neter, J., Kutner, M., Nachtsheim, C. and Wasserman, W.,
1996. Applied linear statistical models, 4th ed.
Chicago, IL: Irwin.
Rainer, J., 2015. Speaking up: Factors and issues in
nurses advocating for patients when patients are in
jeopardy. Journal of Nursing Care Quality, 30(1),
53-62.
Rich, V. L. and Rich, A. R., 1987. Personality hardiness
and burnout in female staff nurses. Journal of
Nursing Scholarship, 19(2), 63-66.
Rikoon, S. H., Brenneman, M., Kim, L. E., Khorramdel,
L., MacCann, C., Burrus, J. and Roberts, R. D.,
2016. Facets of conscientiousness and their
differential relationships with cognitive ability
factors. Journal of Research in Personality, 61,
22-34.
Rose, C. L., Murphy, L. B., Byard, L. and Nikzad, K.,
2002. The role of the Big Five personality factors
in vigilance performance and workload. European
Journal of Personality, 16(3), 185-200.
Saucier, G., 1994. Mini-Marker: A brief version of
Goldberg‟s unipolar Big-Five marker. Journal of
Personality Assessment, 63(3), 506-516.
Smith, P., Pearson, P. H. and Ross, F., 2009. Emotions at
work: What is the link to patient and staff safety?
Implications for nurse managers in the NHS.
Journal of Nursing Management, 17(2), 230-237.
Spence Laschinger, H. K. and Leiter, M. P., 2006. The
impact of nursing work environments on patient
safety outcomes: The moderating role of
burnout/engagement. Journal of Nursing
Administration, 36(5), 259-267.
Studer-Luethi, B., Jaeggi, S. M., Buschkuehl, M. and
Perrig, W. J., 2012. Influence of neuroticism and
conscientiousness on working memory training
outcome. Personality and Individual Differences,
53(1), 44-49.
Teng, C.-I., Chang, S.-S. and Hsu, K.-H., 2009.
Emotional stability of nurses: Impact on patient
safety. Journal of Advanced Nursing, 65(10),
2088-2096.
Teng, C.-I., Hsu, K.-H., Chien, R.-C. and Chang, H.-Y.,
2007. Influence of personality on care quality of
hospital nurses. Journal of Nursing Care Quality,
22(4), 358-364.
Teng, C.-I. and Liu, T.-W., 2014. How do personality
interactions affect service quality? The perspective
of processing efficiency theory. Service Business,
8(2), 375-397.
Teng, C.-I., Shyu, Y.-I. L., Chiou, W.-K., Fan, H.-C. and
Lam, S. M., 2010. Interactive effects of
nurse-perceived time pressure and burnout on

2018
167 H.-Y. Chang, Y.-I. Shyu, M.-K. Wong, T.-L. Chu, S.-M. Lam and C.-I. Teng
patient safety: A cross-sectional survey.
International Journal of Nursing Studies, 47(11),
1442-1450.
Teng, C.-I., Shyu, Y.-I. L., Dai, Y.-T., Wong, M.-K., Chu,
T.-L. and Chou, T.-A., 2012. Nursing accreditation
system and patient safety. Journal of Nursing
Management, 20(3), 311-318.
Terracciano, A., McCrae, R. R. and Costa, P. T. Jr., 2010.
Intra-individual change in personality stability and
age. Journal of Research in Personality, 44(1),
31-37.
Vogelsmeier, A., Scott-Cawiezell, J., Miller, B. and
Griffith, S., 2010. Influencing leadership
perceptions of patient safety through just culture
training. Journal of Nursing Care Quality, 25(4),
288-294.
Wickens, T. D., 2001. Elementary signal detection theory.
New York, NY: Oxford University Press.
Williams, L. M., Brown, K. J., Palmer, D., Liddell, B. J.,
Kemp, A. H., Olivieri, G., et al., 2006. The mellow
years? Neural basis of improving emotional
stability over age. Journal of Neuroscience, 26(24),
6422-6430.
Witt, L. A., Burke, L. A., Barrick, M. A. and Mount, M.
K., 2002. The interactive effects of
conscientiousness and agreeableness on job
performance. Journal of Applied Psychology, 87(1),
164-169.
Witt, L. A., Andrews, M. C. and Carlson, D. S., 2004.
When conscientiousness isn‟t enough: Emotional
exhaustion and performance among call center
customer service representatives. Journal of
Management, 30(1), 149-160.
Yang, M. K. and Wang, G. S., 2001. The effects of an
emotional management programme on the work
emotional stability and interpersonal relationships
of vocational school students. Global Journal of
Engineering Education, 5(2), 175-184.
Yu, M.-L. and Perng, S.-J., 2014. Adverse events among
nurse aids in long-term care facilities in Taiwan.
Journal of Nursing Care Quality, 29(3), E7-E14.

168 International Journal of Commerce and Strategy June
張皓媛為國立台灣大學醫學院護理學系助理教授、臺大醫院護理部兼任督導。國立台灣大學護理學博士。主要研究領域為懷
孕婦女下背痛、偏頭痛、產後婦女泌乳諮詢、護理人力管理。學術論文曾發表於 Journal of Nursing Scholarship、Journal of
Advanced Nursing、Journal of Nursing Management、Scandinavian Journal of Caring Science 等期刊。
Hao-Yuan Chang, is an Assistant Professor in the School of Nursing, College of Medicine, National Taiwan University; Adjunct
Supervisor, Department of Nursing, National Taiwan University Hospital. She received her Doctoral degree in School of Nursing from
National Taiwan University, Taiwan. Her main research areas include low back pain and migraine among pregnant women and
lactation consulting among postpartum women. Her research papers have been published at Journal of Nursing Scholarship, Journal of
Advanced Nursing, Journal of Nursing Management, Scandinavian Journal of Caring Science, and others.
徐亞瑛為長庚大學護理學系教授。美國奧勒岡健康科學大學博士。主要研究領域為失能老人及其家庭照顧者之照護以及質性
研究。學術論文曾發表於 International Journal of Nursing Studies、Journal of Nursing Scholarship、Journal of Advanced Nursing、
Scandinavian Journal of Caring Science 等期刊。
Yea-Ing Lotus Shyu, is a Professor in the School of Nursing, Chang Gung University. She received her Doctoral degree from Oregon
Health & Science University, USA. Her main research areas include the care on disabled elders and their family and qualitative
research. Her research papers have been published at International Journal of Nursing Studies, Journal of Nursing Scholarship, Journal
of Advanced Nursing, Scandinavian Journal of Caring Science, and others.
黃美涓為長庚紀念醫院桃園分院院長。台灣大學醫學士。主要研究領域為兒童復健。學術論文曾發表於 Pain、American Journal
of Physical Medicine and Rehabilitation、Journal of Nursing Scholarship、Journal of Nursing Management 等期刊。
May-Kuen Wong, is the Chair of the Taoyuan Branch, Chang Gung Memorial Hospital. She received her Medical Doctoral degree
from National Taiwan University, Taiwan. Her main research areas include pediatric rehabilitation. Her research papers have been
published at Pain, American Journal of Physical Medicine and Rehabilitation, Journal of Nursing Scholarship, Journal of Nursing
Management, and others.
朱宗藍為長庚紀念醫院行政中心品管組組長。長庚大學護理學碩士。主要研究領域為護理人員管理。學術論文曾發表於 Journal
of Nursing Scholarship、Journal of Nursing Management、Scandinavian Journal of Caring Science 等期刊。
Tsung-Lan Chu, is the Chief Manager of the Quality Management Department, Administration Center, Chang Gung Memorial
Hospital. She received her Master degree from Chang Gung University, Taiwan. Her main research areas include nursing management.
Her research papers have been published at Journal of Nursing Scholarship, Journal of Nursing Management, Scandinavian Journal of
Caring Science, and others.
林思敏為衛生福利部統計處研究助理。主要研究領域為護理人管理。學術論文曾發表於 International Journal of Nursing Studies。
Si Man Lam, is a research assistant of Ministry of Health and Welfare Department of Statistics, Taiwan. She received her Master
degree from National Taiwan University, Taiwan. Her main research areas include nursing management. Her research papers have
been published at International Journal of Nursing Studies.
鄧景宜為長庚大學企業管理研究所教授、長庚紀念醫院林口總院復健科合聘研究員、明志科技大學經營管理系合聘教授。國
立臺灣大學商學研究所博士。主要研究領域為護理人員管理、電子商務。學術論文曾發表於 Journal of Service Research、Journal
of Computer-Mediated Communication、International Journal of Electronic Commerce、International Journal of Nursing Studies 等期
刊。
Ching-I Teng, is a Professor in the Graduate Institute of Business and Management, Chang Gung University; Adjunct Research
Fellow, Department of Rehabilitation, Chang Gung Memorial Hospital; Adjunct Professor, Department of Business and Management,
Ming Chi University of Technology. He received his Doctoral degree from National Taiwan University, Taiwan. His main research
areas include nursing management and electronic commerce. His research papers have been published at Journal of Service Research,
Journal of Computer-Mediated Communication, International Journal of Electronic Commerce, International Journal of Nursing
Studies, and others.