Embed Size (px)
Citation preview

The Neuromuscular Junc0on: Neurophysiology and Common
Disorders Nicholas J. Silvestri, M.D.
Assistant Professor of Neurology


Neuromuscular Transmission
• Presynap0c events • Events in the synap0c cleC • Post-‐synap0c events

Presynap0c Events
• Synthesis and degrada0on of ACh
Choline Acetyltransferase
Acetyl CoA + Choline à Acetylcholine

Presynap0c Events
• ACh packaged into vesicles in discrete units called quanta – Each quantum contains ~ 10,000 molecules of Ach
• Quanta are located in 3 separate stores – Primary store: ~1000 quanta available for immediate release
– Secondary store: ~10,000 quanta that can resupply primary store aCer several seconds
– Ter0ary store: ~100,000 quanta distant from NMJ

Presynap0c Events
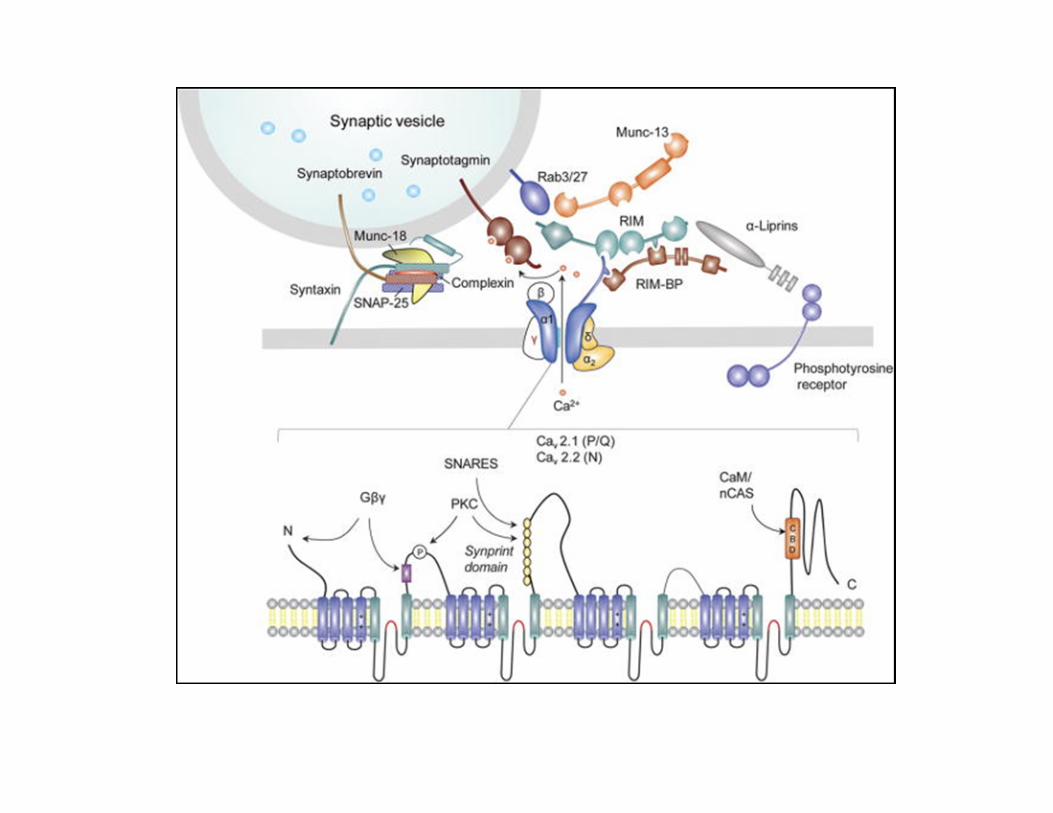
• Presynap0c nerve terminal lined with ac0ve zones which are specific sites on membrane where vesicles aQach and release ACh into synap0c cleC
Pre-‐Synap0c Events
• AP invades and depolarizes nerve terminal
• Voltage gated Ca++ channels open, allowing influx of Ca++
• Ca-‐dependent binding of vesicles to terminal membrane occurs – Rela0vely slow, lasts 0.5msec (of total 0.75msec for NMJ
transmission)
• Near-‐synchronous release of up to 200 quanta – Number of quanta released propor0onal to concentra0on of Ca
++

Synap0c Events
• Synap&c cle+ – Space between nerve terminal and depression in the postsynap0c membrane into which the terminal fits
– Site of hydrolysis of ACh by acetylcholinesterase (AChE)

Post-‐synap0c Events
• Post-‐synap&c membrane – Region of muscle fiber membrane across from the nerve
terminal, a.k.a. endplate • 1 endplate per fiber, number increases with reinnerva0on
– Contains mul0ple infoldings called secondary cleCs • Nico0nic ACh receptors concentrated on crests of folds • AChE concentrated in depths of cleCs
– ACh receptor is a transmembrane glycoprotein which binds 2 ACh molecules, opening a central channel in the receptor for a few msec, allowing Na+ to enter down its electrochemical gradient

NMJ Ultrastructure

Nico0nic ACh Receptor
Post-‐synap0c Events
• ACh diffuses across synap0c cleC and binds to ACh receptors, genera0ng an end plate poten0al (EPP)
• If the EPP > threshold for genera0ng an AP, all-‐or-‐none depolariza0on of the muscle membrane occurs – Threshold around 40-‐60 mV
Post-‐synap0c Events
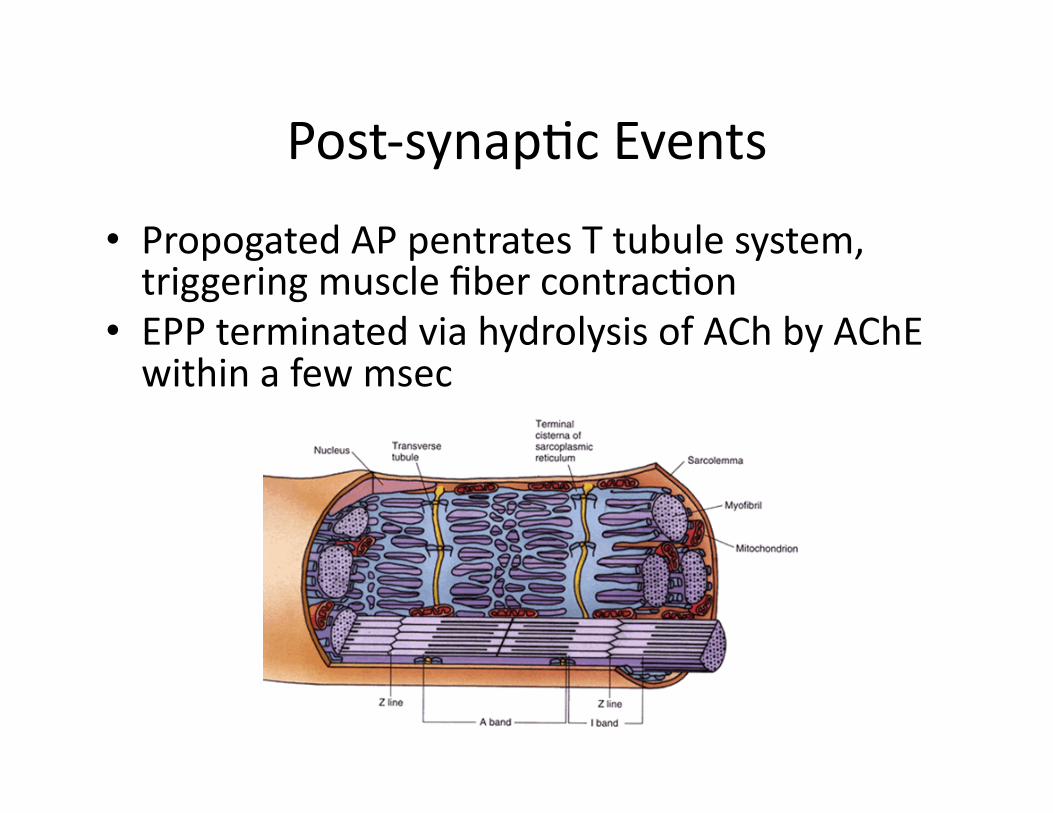
• Propogated AP pentrates T tubule system, triggering muscle fiber contrac0on
• EPP terminated via hydrolysis of ACh by AChE within a few msec

Disorders of the NMJ
• Myasthenia gravis • Congenital Myasthenic Syndromes
• Lambert-‐Eaton Myasthenic Syndrome
• Botulism
• Miscellaneous disorders of the neuromuscular junc0on

Myasthenia Gravis
n Incidence: 1-‐9 per million q F>M (7:3 in young age group, 1:1 in older)
q F peak at ages 20-‐24 and 70-‐74 years q M peak at ages 30-‐34 and 70-‐74 years
n Prevalence: 25-‐142 per million
n 10% cases present in childhood (juvenile myasthenia)

MG
• Pathophysiology – In 85% pa0ents with generalized MG and 50% pa0ents with ocular MG, an0bodies directed against ACh receptors • Binding an0bodies-‐ most common • Blocking an0bodies • Modula0ng an0bodies
– MuSK an0bodies – Other an0bodies

MG
• Pathophysiology – In the case of an0bodies to ACh receptors, damage to the NMJ occurs from: • Accelerated degrada0on of ACh receptors • Blocking ac0ve sites on ACh receptors • Damaging ACh receptors with the aid of complement

MG
• Thymic pathology – 40-‐70% of pa0ents with autoimmune MG have evidence of thymic hyperplasia
– 10-‐15% of pa0ents with autoimmune MG have underlying thymoma

MG
• Presen0ng Symptoms – Ocular: Ptosis, diplopia – Bulbar: Dysphagia, dysarthria, dysphonia, jaw fa0gue
– Respiratory: Dyspnea, orthopnea – Generalized: Neck, limb weakness – Dis0nc0ve feature is fluctua0ng nature of symptoms, producing a dynamic rather than sta0c disorder

MG
• In the vast majority of pa0ents (90%), ocular symptoms are first manifesta0on
• Generaliza0on ul0mately occurs in two-‐thirds of pa0ents with OMG, the majority within 2 years
• In most pa0ents, the severity of disease lessens with 0me and remissions are possible

MG
• Exam – Ocular signs
• Ptosis, diplopia on tes0ng of EOM, weakness of eye closure, over-‐contrac0on of frontalis
– Bulbar signs • Jaw weakness, facial diplegia, palatal weakness, tongue weakness
– Respiratory signs • Respiratory rate, use of accessory muscles, ease of speech
– Neck strength – Limb strength
• Examine for fa0gability

MG
• Diagnos0c Work-‐up – An0body tes0ng
• ACh receptor an0bodies in 85% GMG, 50% OMG • MuSK an0bodies in roughly 10% GMG, rare OMG
– Thyroid func0on studies – EMG and Nerve Conduc0on Studies – Evalua0on for thymic pathology
• CT or MRI of the chest – Edrophonium (Tensilon) test – Ice pack test

MG 3 Hz Repetitive Nerve Stimulation
Single Fiber EMG

MG
• Treatment – Ocular vs. Generalized – Acetylcholinesterase inhibitors – Prednisone – Steroid-‐sparing agents – IVIg – Plasmapheresis

MG
• Treatment of Ocular MG – Ini0ally, pyridos0gmine
– If symptoms refractory to pyridos0gmine and impac0ng quality of life, prednisone

MG
• An0-‐acetylcholinesterase medica0ons – Most commonly used is pyridos0gmine (Mes0non)
– Transiently inhibits AChE from metabolizing ACh
– Ini0ated at dose of 30-‐60mg q6h
– Gradually 0trated to effect, most adults requiring 60-‐120mg q4-‐6h
– Doses exceeding 600mg/day typically ineffec0ve and produce side effects

MG
• Side effects of an0-‐acetylcholinesterase medica0ons – Nausea, vomi0ng – Abdominal cramping – Diarrhea – Sialorrhea – Bradycardia – Encephalopathy (rare) – Cholinergic crisis (rare)

MG
• Treatment of Generalized MG – Ini0al treatment with pyridos0gmine and prednisone
– Subsequent treatment with steroid sparing agent • Azathioprine • Cyclosporine • Mycophenolate mofe0l • Tacrolimus • IVIg
– Thymectomy if thymoma present or in young pa0ents with thymic hyperplasia

Myasthenic Crisis
• Strictly defined as respiratory failure due to myasthenia gravis, though impending respiratory failure also qualifies
• Causes: infec0on, illness, surgery, trauma, stress, medica0ons
• More commonly occur within 3 years of ini0al diagnosis of MG
• Diagnosis – Largely based on history and exam – Assessment of pulmonary func0on (spirometry)

Myasthenic Crisis
• Treatment – Protec0on of airway
• Endotracheal intuba0on and ven0la0on versus non-‐invasive posi0ve pressure ven0la0on
• Signs of impending respiratory failure: – Rapid progression of weakness – Neck flexor weakness – Inability to converse in complete sentences – Use of accessory muscles – Tachypnea – Spirometry: NIF < -‐30cc, FVC < 15cc/kg or declining trend in these parameters

Myasthenic Crisis
• Treatment – Directed treatment toward inci0ng event if iden0fiable (e.g. infec0on)
– Prudent to hold an0-‐acetylcholinesterase drugs – Plasmapheresis

Medica0ons that can worsen MG • Anesthe0cs: Chloroprocaine, Diazepam, Ether, Halothane, Ketamine, Lidocaine • Neuromuscular blocking agents: Propanidid, Procaine, Botox, Magnesium • An0bio0cs: Aminoglycosides, Amikacin, Gentamicin, Kanamycin, Neomycin,
Ne0lmicin, Paromomycin, Spec0nomycin, Streptomycin, Tobramycin, Fluoroquinolones, Ampicillin, Clarithromycin, Clindamycin, Colis0n, Erythromycin, Lincomycin, Quinine, Telithromycin, Tetracyclines
• An0convulsants: Gabapen0n, Phenytoin, Trimethadione • An0psycho0cs: Chlorpromazine, Lithium ,Phenothiazines • An0rheuma0c drugs: Chloroquine, Penicillamine • Cardiovascular drugs: Beta blockers, Bretylium, Procainamide, Propafenone,
Quinidine, calcium channel blockers • Glucocor&coids • Ophthalmologic drugs: Betaxolol, Echothiophate, Timolol, Tropicamide,
Proparacaine • Other drugs: An0cholinergics, Carni0ne, Cholinesterase inhibitors, Deferoxamine,
Diure0cs, Eme0ne (Ipecac syrup), Interferon alpha, Iodinated contrast agents Oxytocin, An0retroviral protease inhibitors, Sta0ns,Thyroxine
• Narco0cs • Oral contracep0ves

Congenital Myasthenic Syndromes
• Presynap0c disorders – Choline acetyltransferase deficiency – Paucity of synap0c vesicles
• Synap0c disorders – End plate AChE deficiency
• Postsynap0c disorders – Primary kine0c defect +/-‐ AChR
deficiency – Primary AChR deficiency +/-‐ kine0c
defect – Rapsyn deficiency – Sodium channel myasthenia – Plec0n deficiency – Dok-‐7 myasthenia

Lambert-‐Eaton Myasthenic Syndrome
• Rare • Presenta0on
– Pa0ents typically complain of weakness and easy fa0gability, predominantly of proximal lower extremi0es
– Oculobulbar symptoms less common than in MG – Cholinergic dysautonomia

LEMS
• Exam – Signs of cholinergic dysautonomia
– Proximal muscle weakness, improved with repe00ve tes0ng (facilita0on)
– Hyporeflexia, improved with facilita0on

LEMS
• Pathophysiology – An0bodies directed against P/Q voltage-‐gated calcium channels on presynap0c membrane at both NMJ and preganglionic parasympatheic nerve terminals

LEMS
• Roughly two-‐thirds of cases associated with underlying malignancy – Most common underlying malignancy is SCLC (90%, others include lymphoprolifera0ve disorders, breast, ovarian, and pancrea0c ca)
• Diagnosis typically precedes that of malignancy by ~10 months

LEMS
• Diagnos0c work-‐up – An0body tes0ng
• 85-‐90% of pts have an0-‐P/Q voltage-‐gated Ca channel an0bodies (both paraneoplas0c and non-‐paraneoplas0c)
• ~10% of pts also have an0-‐ACh R an0bodies – Electrodiagnos0c studies – Evalua0on for malignancy
• CT torso

LEMS
50 Hz RNS
Pre- and post-tetanic stimulation (10 seconds of maximal voluntary contraction)

LEMS
• Treatment – Of malignancy-‐ pa0ents may improve
– An0-‐acetylcholinesterase drugs may produce a modest effect (variable)
– 3,4 diaminopyridine – ?Immunosuppression (steroids, IVIg, plasmapheresis)

Botulism
• Caused by toxin of Clostridium botulinum – Gram posi0ve, rod-‐shaped, obligate anaerobe – A, B, E strains of toxin most common
• Can be acquired via several routes: – Wound – Food borne – Infan0le – Hidden (suspected gastrointes0nal) – Inhala0onal

Botulism
• Pathophysiology – Neurotoxins produced by C. botulinum degrade proteins necessary for docking and fusion of ACh vesicles to the synap0c membrane, thereby preven0ng release into the synap0c cleC

Botulism
• Presenta0on – Neurologic: Dysphagia, xerostomia, diplopia, dysarthria begin acutely and progress over 12-‐36 hours with rostral to caudal progression of weakness eventually involving limbs and/or respiratory muscles
– Gastrointes0nal: Nausea, vomi0ng, diarrhea followed by cons0pa0on, abdominal cramps
– Anxiety

Botulism
• Exam – Ptosis, ophthalmoplegia, facial diplegia, palatal and tongue weakness
– Limb weakness and hypo-‐ to areflexia
– Evalua0on of respiratory func0on – Signs of dysautonomia: e.g. poorly reac0ve pupillary light response, bradycardia

Botulism
• Differen0al Diagnosis – Myasthenia gravis
– Guillain-‐Barre syndrome – Tick paralysis – Poliomyeli0s
– LEMS – Heavy metal intoxica0on – Brainstem stroke

Botulism
• Diagnos0c work-‐up – Toxin
• Serum in foodborne • Stool in infan0le • Wound scrapings in wound
– EMG/NCS

Botulism
• Treatment – Suppor0ve care
• Respiratory monitoring, intuba0on as necessary • Gastrointes0nal symptoms
– An0-‐toxin • Equine serum trivalent botulism an0toxin (A, B, E) is available in the United States through State Health Departments or the CDC
• Early treatment – An0bio0cs
• Unproven but oCen given for wound botulism

Botulism
• Most pa0ents require hospitaliza0on for 1 to 3 months for suppor0ve care
• Mortality rate ~5%

Other Causes of Neuromuscular Junc0on Dysfunc0on
• Drug-‐induced MG (penicillamine, amiodarone) • Aminoglycoside an0boi0cs
• Hypermagnesemia • Envenoma0ons (various snakes, scorpions, spiders,
cobras, kraits) • Certain forms of 0ck paralysis • Agents designed for chemical warfare
• Prolonged neuromuscular blockade (curare-‐like agents in the cri0cally ill)













![Lipocalin-type prostaglandin D synthase protects against ... · dysautonomia, Alzheimer’s disease and Parkinson’s disease [3,4]. A number of studies have suggested that the excessive](https://img.pdfslide.tips/doc/110x75/5e42a83ed84fab24ed3c5530/lipocalin-type-prostaglandin-d-synthase-protects-against-dysautonomia-alzheimeras.jpg)