Embed Size (px)
Citation preview

Torakoabdominal ve Hibrid Girişimler
Prof.Dr. Fürüzan NumanGirişimsel Radyoloji Bilim Dalı Bşk.
İstanbul ÜniversitesiCerrahpasa Tıp Fakültesi
2014 9.GİRİŞİMSEL RADYOLOJİ YILLIK TOPLANTISI ANTALYA

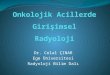
EVDOLOGIXVENTANA
fenestrated stent graft system

[J Endovasc Ther. 2013]PMID: 24325685 [PubMed - in process] J Endovasc Ther. 2012 Apr;19(2):173-8. doi: 10.1583/11-3706.1.Ventana fenestrated stent-graft system for endovascular repair of juxtarenal aortic aneurysms.Mertens R1, Bergoeing M, Mariné L, Valdés F, Krämer A, Vergara J.
The off-the-shelf Ventana fenestrated stent-graft system consists of a 25-mm IntuiTrak self-expanding bifurcated stent-graft implanted at the aortic bifurcation. A Ventana self-expanding fenestrated proximal extension stent-graft is overlapped with the bifurcated body distally and sealed proximally in the visceral segment with a 4-cm-long scallop below and around the SMA and celiac artery, obviating the need for an infrarenal neck. Movable, non-reinforced, 3-mm fenestrations for the renal arteries can be expanded to 10 mm.
The technique is illustrated in 2 patients (76 and 77 years of age) with significant comorbidities and juxtarenal aortic aneurysms measuring 5.9 and 7.4 mm,
Mean fluoroscopy times were 27 and 35 minutes, and the contrast volumes were 72 and 67 mL. Total procedure times were 84 and 71 minutes. The aneurysms were effectively excluded in uneventful procedures, with no migration, endoleak, or renal dysfunction at 6-month follow-up.

CUSTOM MADE ANACONDA

J Vasc Surg. 2012 Sep;56(3):601-7. doi: 10.1016/j.jvs.2012.02.011. Epub 2012 May 2.Physician-modified endovascular grafts for the treatment of elective, symptomatic, or ruptured juxtarenal aortic aneurysms.Starnes BW.
Food and Drug Administration-approved device (Zenith Flex; Cook Inc, Bloomington, Ind) to preserve branch vessels when used in the treatment of patients with elective, symptomatic, or ruptured juxtarenal aortic aneurysms.
Forty-seven consecutive patients underwent fenestrated endovascular repair using PMEG over a 3-year period
Technical success rate was 98%, and freedom from aneurysm-related death was 98%. There were six complications (13%). Three (6%) were access related, and three (6%) were procedure related and included one stroke, one case of renal failure, and one branch artery dissection. On follow-up, six patients (13%) had endoleak. There was one type 1 endoleak and five type 2 endoleaks. In-hospital and 30-day mortality was 2%,
PMEG is a safe and effective alternative for treating patients with juxtarenal aneurysms who have no other alternatives for repair


Robot –Assisted Antegrade In-Situ Fenestration
NickCheshire

F-EVAR BAŞARISIZLIĞI

Branched

Branched
COOK,Tim Chutter




Zentralbl Chir. 2011 Oct;136(5):451-7. doi: 10.1055/s-0031-1271550. Epub 2011 Jul 15.[Results of endovascular repair of TAAA in the first 50 patients].[Article in German]Verhoeven E1, Tielliu IF, Zeebregts CJ, Bekkema F, Vourliotakis G, Ritter W, Zipfel B, Renner H
,
METHODS:A literature review and results of first 50 patients treated with a custom-made Zenith device with fixed branches are presented. Most of the patients were refused open surgery mainly for the extent of the disease combined with co-morbidity, which included in most patients a combination of several risk factors. Extent of the aneurysm was type I (n = 9), type II (n = 13), type III (n = 19), and type IV (n = 9)
RESULTS:Primary and primary assisted technical successes in our series were 88 % (44 / 50) and 92 % (46 / 50), respectively. One patient died on day 1 from an intraoperative aneurysm rupture. In two patients a renal artery was lost, one due to rupture and one due to malpositioning of the bridging stent graft. In a fourth patient, a celiac artery could not be catheterised and was lost. Finally, in two more patients, catheterisation of in total three renal arteries proved impossible. This was solved by a retrograde approach for two renal arteries via laparotomy in one patient, and a spleno-renal bypass in the other patient. Thirty-day mortality was 8 %. Estimated survival at 6 months, 1 year, and 2 years was 91.2 %, 79.8 %, and 69.7 %, respectively. Freedom of reintervention of all kinds at 1 and 2 years was 81.9 % and 73.7 %, respectively

Early experience with the first commercially available off-the-shelf multibranched endograft (t-branch) in the treatment of thoracoabdominal aortic aneurysms. Between November 2012 and May 2013, 15 patients (10 men; mean age 70 years) with TAAA underwent implantation of the Zenith t-Branch device, which received European marketing approval in late 2012.
Technical success was 100%, with all target vessels connected and patent. There was no renal function deterioration or organ ischemia. Paraplegia was observed in one patient despite cerebrospinal fluid drainage and monitoring. Four patients suffered from transient paraparesis, which was completely resolved before discharge. There was no in-hospital or 30-day mortality. After a mean follow-up of 5 months, no patient has died, and there has been no branch occlusion or type I/III endoleaks.
J Endovasc Ther. 2013 Dec;20(6):719-25. doi: 10.1583/13-4428R.1.Early experience with the first commercially available off-the-shelf multibranched endograft (t-branch) in the treatment of thoracoabdominal aortic aneurysms.Bosiers MJ1, Bisdas T, Donas KP, Torsello G, Austermann M.


Chimney Tekniği
Martin Malina

Periscope Tekniği(ters chimney)• Organlara gereken akımı endograftin distal landing
zone alanına yerleşerek tersten alıyor.• Elastikiyet nedeni ile tercihen Viabahn kullanılıyor.

J Vasc Surg. 2012 May;55(5):1497-503. doi: 10.1016/j.jvs.2011.10.009. Epub 2012 Jan 10.The chimney graft technique for preserving visceral vessels during endovascular treatment of aortic pathologies.Moulakakis KG1, Mylonas SN, Avgerinos E, Papapetrou A, Kakisis JD, Brountzos EN, Liapis CD.
CONCLUSIONS:The role of the chimney technique in the management of complex abdominal aortic aneurysms is still unclear. Thus, there is a reasonable hesitation to embrace the method for widespread use in the absence of long-term data.
The electronic literature search yielded 15 reports that fulfilled the inclusion criteria. Out of the 93 patients, 24.7% were operated on in an urgent setting (symptomatic or ruptured aneurysm). A total of 134 CGs were implanted: 108 to the renal arteries, 20 to the superior mesenteric artery, five to the celiac trunk, and one to the inferior mesenteric artery.
The 30-day in-hospital mortality was 4.3%. A total of 13 patients (14.0%) developed a type I endoleak. During a mean follow-up period of 9.0 ± 1.0 months, 131 of 134 (97.8%) CGs remained patent. Two CGs to the renal arteries and one to the superior mesenteric artery occluded. Postoperatively, 11.8% of patients suffered renal function impairment and 2.1% a myocardial infarction. Ischemic stroke pesented in 3.2% of patients.

Br J Surg. 2013 Nov;100(12):1557-64. doi: 10.1002/bjs.9274.Systematic review of chimney and periscope grafts for endovascular aneurysm repair.Wilson A1, Zhou S, Bachoo P, Tambyraja AL.
Twenty-four studies describing 234 patients who underwent EVAR with one or more chimney or periscope grafts for aortic branch vessels were identified. Most procedures were elective; only 62 (26.5 per cent) were performed urgently. There were 176 patients with an abdominal aortic aneurysm and 58 with a thoracic or thoracoabdominal aortic aneurysm. Three hundred and seventy-six branch vessels were perfused. Twelve patients (5.1 per cent) died within 30 days of aneurysm repair. Twenty-seven patients (11.5 per cent) developed a type I endoleak. After a mean(s.d.) follow-up of 12(5) months, seven branch vessels stents had occluded.

3D Multilayer stent!!!
Cardiatis spatial three dimensional stent design, by virtue of its geometry, slows and laminates
blood flow inside the aneurysm minimizing chances of aneurysm rupture and allowing an organized thrombus to form but with preservation of flow to the covered side branches

J Endovasc Ther. 2014 Feb;21(1):96-112. doi: 10.1583/13-4514MR.1.When not to implant the multilayer flow modulator: lessons learned from application outside the indications for use in patients with thoracoabdominal pathologies.Sultan S1, Hynes N, Sultan M; MFM Collaborators
Results : Although no death, paraplegia, stroke, or renovisceral compromise was documented during the initial hospital stay, technical success was zero. There were 31 (81.6%) cases in which there was failure to land the device in normal aorta. Other violations of the IFU included 12 with inadequate stent overlap and 11 cases involving a small MFM being deployed inside a larger one. Five of the 9 cases in which an undersized device was used resulted in a type I endoleak
During a mean follow-up of 10.0±6.9 months, all-cause mortality was 89.5% (34/38), of which 27 (71.1%) were aneurysm-related deaths. Overall survival, freedom from aneurysm-related death, and rupture-free survival estimates were 17.5%, 25.0%, 31.5%, respectively, at 18 months.
Conclusion : There are clinical scenarios in which the MFM does not perform well.