Upload
cansu
View
238
Download
0
Embed Size (px)
Citation preview
8/14/2019 Toxicology (3) - Ullmann
1/22
2 01 2 Wi le y- VC H V er la g G mb H & C o. K Ga A, W ei nh ei m
Toxicology, 3. Evaluation of Toxic Effects
WOLFGANG DEKANT, Institute of Toxicology, University of Wuerzburg, Germany
SPIRIDONVAMVAKAS, Institute of Toxicology, University of Wuerzburg, Germany
1. Acceptable Risk, Comparison of Risks, and
Establishing Acceptable Levels of Risk . . . 256
2. The Risk Assessment Process. . . . . . . . . . . 258
2.1. Hazard Identification Techniques . . . . . . . 258
2.2. Determination of Exposure . . . . . . . . . . . . 260
2.3. Dose-Response Relationships. . . . . . . . . . . 261
2.4. Risk Characterization. . . . . . . . . . . . . . . . 262
2.4.1. The Safety-Factor Methodology . . . . . . . . . . 2622.4.2. Risk Estimation Techniques for Nonthreshold
Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . 264
2.4.3. Mathematical Models Used in High- to Low-
Dose Risk Extrapolation . . . . . . . . . . . . . . . 265
2.4.4. Interpretation of Data from Chronic Animal
Bioassays . . . . . . . . . . . . . . . . . . . . . . . . . . 266
2.4.5. Problems and Uncertainties in Risk
Assessment . . . . . . . . . . . . . . . . . . . . . . . . . 266
3. Future Contributions of Scientifically Based
Procedures to Risk Assessment and
Qualitative Risk Assessment for
Carcinogens . . . . . . . . . . . . . . . . . . . . . . . . 2704. Risk Assessment for Teratogens . . . . . . . . 274
References . . . . . . . . . . . . . . . . . . . . . . . . . 275
One of the major environmental and occupationalissues of concern to both scientists and adminis-trators is the control of potential health hazards tohumans due to the production, use, and disposal ofchemicals. Theconcern arises from the increasing
numbers of chemicals in production and use andthe increasing numbers of chemicals demonstrat-ed to exert toxic effects in one or several of thesensitive toxicity testing systems available. Thissituation has afforded growing legislative controlof the production and application of chemicals toensure adequate protection of human health. Con-trol measures based on the recognition of poten-tial adverse health effects may limit the presenceof hazardous chemicals in the environment orregulate the use of hazardous chemicals, thus
reducing the potential health risks to humans(Table 1).
Theassessment of potential human healthrisksresulting from the exposure to chemicals providesthe basis for appropriate regulatory and controlmeasures. The health risk assessment determineswhether a xenobiotic may cause adverse health
effects, at what level and frequency of exposure,and the probability that adverse health effects willoccur. The term risk assessment is increasinglyused in the context of potentially toxic chemicals.Scientific risk assessment considers the availabledata on the toxicologyof a specific chemical when
judging which agents potentially pose a signifi-cant risk to the human population. Toxicologyfocuses on the identification and quantitation ofpotential hazards by using animal studies assurrogates for humans. Permissible exposure
levels for humans are derived from the results ofthe animal studies by using margins of safety or
Abbreviations
AP: apurinic/apyrimidinic site
APS: adenosine 50-phosphosulfate
CoA: Coenzym A
ED: effective dose
LOAEL: lowest-observed-adverse-effect level
LOEL: lowest-observed-effect levelMTD: maximum tolerated dose
NOEL: no-observed-effect-level
DOI: 10.1002/14356007.o27_016
8/14/2019 Toxicology (3) - Ullmann
2/22
defining acceptable incidences of adversehealth effects in exposed humans [6].
Health risk assessment andits usein regulatorydecisions have recently generated intense contro-versy. The debate over risk assessment is politi-cally and emotionally charged, and creates anadverse atmosphere heightened by the extraordi-nary sums of money at stake. Industry complainsthat the costs of complying with possible over-regulation based on inappropriate risk assess-ments may be excessive; moreover, lawsuits on
potential environmentally caused diseases, espe-cially in the United States, involve huge sums ofmoney. On the other hand, environmentalistsclaim that risk assessment practices and policiesdo not adequately protect human health; more-over, health care costs for the treatment of en-vironmentally caused diseases may also be veryhigh. These considerations have led to an inten-sive rethinking of the health risk assessmentprocess and have increased the awareness that inmany cases, the scientific foundation for risk
assessment is weak. This rethinking led to theconclusion that resolution of the controversies bythe development of effective prevention strate-gies and rational priority setting may be achievedonly by strengthening the scientific backgroundand available data by research and by developingbetter methods to estimate risks due to chemicalexposures [68].
Before considering the practice of health riskassessment, several terms frequently used andmisused in risk assessment and its perception
should be clarified. In discussions on health ef-fects of potentially toxic chemicals, the termshazard and risk are often used with an
identical meaning, although they are clearly dif-ferent. Hazard defines the intrinsic toxicity of achemical and is not identical to risk. Risk is theestimated or measured probability of injury ordeath resulting from exposure to a specific chem-ical. Risk may be described either in semiquanti-
tative terms such as high or low risk or in quanti-tative terms such as one person experiencing anadverse effect per 10 000 persons exposed. Riskmay also be described in absolute terms (proba-bility of adverse effects due to a specific chemicalexposure) or in comparative terms by comparingthe probability of adverse effects between a pop-ulation exposed to an agent and an unexposedpopulation.
The health risks due to the contact with poten-tially toxic chemicals are dependent on the con-ditions of exposure, since not only the intrinsictoxicity of a chemical determines the magnitudeot the adverse effect but also the dose. As noted in! Toxicology, 1. Fundamentals, Chapter 1, themagnitude of the toxic effects is the product ofthe intrinsic toxicity of a chemical multiplied bythe dose taken up by exposed animals or humans;thus, all toxic effects are dose-dependent andevenvery toxic chemicals may not cause toxic effectswhen the dose is low. If the dose is zero, despite a
very high intrinsic toxicity of a specific chemical,the toxic effect and the risk of adverse healtheffects will be zero. On the other hand, chemicalswith low intrinsic toxicity may induce toxic ef-fects when the dose is high and may thus pose asignificant risk. In toxicological terms, risk istherefore the product of the intrinsic toxicity ofa chemical and the exposure characteristics.
1. Acceptable Risk, Comparison of
Risks, and Establishing AcceptableLevels of Risk
In earlier phases of risk assessment, the basicbelief was that few chemicals are toxic and all ofthese toxic chemicals are derived from syntheticprocesses. To achieve a zero risk, chemical ex-posure must be reduced below a threshold level,under which it causes absolutely no risk. How-ever, where such a threshold cannot be demon-strated, one must assume that a finite risk may
occur at any exposure level, consequently, abso-lute control of risk is possible only if the source ofexposure is eliminated altogether. These conside-
Table 1. Possible measures to reduce human exposure to hazardous
chemicals
Application or exposure
to chemical in question
Measures to reduce exposure
Industrial chemicals reduction or cessation of
application; protective
measures in the workplace;
alternative chemicals with
lower hazard
Pharmaceuticals cost benefit analysis
Alcohol, smoking,
drugs of abuse
education
Environmental chemicals quantitation of exposure,
strategies for avoidance
or reduction of environmental
pollution
256 Toxicology, 3. Evaluation of Toxic Effects Vol. 37
8/14/2019 Toxicology (3) - Ullmann
3/22
rations resulted in the zero-risk concept. TheDelaney Clause of the Federal Food and DrugAct in the United States is an example of a zero-risk approach in the regulation of food additives.This law states that no xenobiotic whose carcino-genic potency in animals has been demonstrated
may be used as a food additive.However, the more widespread testing of che-
micals for toxicity, the increased sensitivity ofanalytical instruments to determine chemicals inthe environment and at the workplace, and thedevelopments in the science of toxicology put thebasic assumption of the zero risk concept that is,only synthetic chemicals are toxic into question.
However, the more widespread testing of che-micals for toxicity, the increased sensitivity ofanalytical instruments to detect chemicals in theenvironment and the workplace, and developmentsin the science of toxicology put the basic assump-tion of the zero-risk concept that only syntheticchemicals are toxic in question. These develop-ments led to the recognition that zero risk wasunachievable and, perhaps, unnecessary for theregulation of chemicals. The observation wasbased mainly on a few facts: (1) all chemicals,both of synthetic and natural origin, are toxic underspecific exposure conditions; (2) most of the haz-
ardous chemicals routinely encountered by hu-mans are of natural rather than synthetic origin;(3) most of the exposure to hazardous syntheticchemicals cannot be avoided entirely or be elimi-nated from the environment without changingprofoundly the way of life in many countries; and(4) in the case of cancer risk assessment, DNAdamage and mutations, assumed to be of majorsignificance in the process of carcinogenesis, occurspontaneously, albeit at a low rate. Examples ofendogenously occurring DNA damage are hydro-
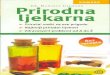
lytic deamination, depurination, oxidative modifi-cation, and endogenously formed DNA adducts.Well-known examples of hazardous synthetic che-micals are benzene, which is present in the envi-ronment as a result of its emission from motorvehicles, cigarette smoking, and other sources, or2,3,7,8-tetrachlorodibenzodioxin formed in forestfires. The effect of naturally occurring chemicalsand chemical exposure due to life-style factors isbest exemplified by the estimated contribution ofdifferent factors to the incidence of avoidable
cancers in humans (Fig. 1).According to the large epidemiological study
of DOLL and PETO (1981), natural chemicals in
diet and chemicals inhaled by cigarette smokingare the major causative agents in human cancer.Occupational and environmental exposure tosynthetic chemicals constitutes only a minor
causative factor.Given these facts, the acceptable risk conceptwas developed as an alternative. The acceptablerisk concept realizes that it is not possible toeliminate all potential health risks associatedwith chemical exposure due to the life style.According to the concept of acceptable risk,safety the reciprocal of risk is no longer anabsolute term but is redefined as a condition ofcertain, but very low and thus acceptable, risk.This conceptual change improves the ability to
deal with potentially very low risks identified bythe increased sensitivity of analytical instrumen-tation and with increasingly sensitive scientificmethods to detect potential adverse effects ofxenobiotics. The concept of acceptable risk alsopermits the definition of limits for the exposure totoxic chemicals that can be considered to have anegligible impact on the incidence of adverseeffects in an exposed population. Risk assess-ment is therefore unavoidable and must implic-itly or explicitly involve a balance of risk and
benefit [610]. Some of the main factors consid-ered in establishing acceptable risk levels forexposure to a chemical follow:
Figure 1. Contribution of chemical exposure and life-stylefactors to the incidence of avoidable cancer in human [21]
Vol. 37 Toxicology, 3. Evaluation of Toxic Effects 257
8/14/2019 Toxicology (3) - Ullmann
4/22
Beneficial aspects. Economic growth. Employment. Increased standard of living. Increased quality of life. Taxes generated
Detrimental aspects. Decreased quality of life. Health effects. Lawsuits. Loss of environmental resources. Loss of work. Medical expenses
2. The Risk Assessment Process
Several individual elements make up the riskassessment process. In the first step, the potentialadverse health effects of a chemical, a mixture ofchemicals or a specific technical process are eval-uated by the application of toxicity tests (for de-tails, see ! Toxicology, 2. Assessment Methods)and, if the chemical is already in widespread useand humans are exposed, by considering the datafrom epidemiological studies. The second step in
risk assessment determines the doseresponse forthe observed adverse effects. In parallel, the expo-sure of humans to this xenobiotic is quantitated byanalytical procedures or, if the chemical is not yetin widespread use, by the estimation of likelyexposure scenarios. In the third step, the resultsobtained in the toxicity studies are extrapolated.This involves an extrapolation both from adverseeffects seen in experimental animals to humans,and often an extrapolation from the effects seenafter high doses in animals to the much lower doses
humans usually encounter. The last step of riskassessment, risk characterization, involves thecombination of steps one to three to judge theexistence and magnitude of the public health prob-lem and characterizes the uncertainties inherent inthe risk assessment process
2.1. Hazard Identification Techniques
Hazard identification is the step in which the
adverse effects of the xenobiotic are determined.Evaluation of both acute and chronic toxicity isperformed by using animals as experimental
models for humans. The use of animals as surro-gate for humans is based on the following as-sumptions: (1) xenobiotics with a likely adverseeffect in humans will manifest some degree oftoxicity in other living systems when the dose issufficiently high; (2) if a sufficient number of
animal species are dosed with the xenobiotic, atleast one should exhibit a similar pattern ofbiotransformation and toxicokinetics to that seenin humans; and (3) if a sufficient number ofdifferent animal species are dosed with the xe-nobiotic, at least one is likely to exhibit the toxicresponses and clinical symptoms occurring inhumans.
Typical end points in studies aimed at hazardidentification in intact animals include mortality,reproductive and developmental effects, targetorgan toxicity, and cancer. Hazard identificationstudies at present also include the determinationof a range of biochemical end points related tospecific toxic effects such as toxicokinetics,routes and extent of biotransformation, structureof reactive intermediates, and binding of reactiveintermediates to cellular macromolecules. In ad-dition, many short-term tests for specific toxiceffects such as DNA damage, mutagenicity, orclastogenicity are increasingly included in haz-
ard identification procedures.The acute toxicity of xenobiotics is evaluatedby a number of procedures from which the LD50may be calculated. With the more recently re-commended fixed-dose method information ontarget organs affected and types of toxic effectsmay also be obtained. Repeated-dose toxicitystudies last between two weeks (subacute toxici-ty studies) and 624 months (chronic toxicitystudies), the lifespan of the animals, includingpost-mortem examination, histopathology, clini-
cal chemistry, and hematology at termination andat specified time points during the study. Fromthe chronic toxicity studies, the lowest observedeffect level (LOEL), also referred to as the lowestobserved adverse-effect level (LOAEL), and theno observed effect level (NOEL) are obtained fornoncancer endpoints. The NOEL is the highestdoes administered that does not induce observ-able toxic effects. The NOEL may not be identi-cal to the no-effect level if insensitive methodsare applied or the wrong end point is chosen.
Moreover, the value obtained for the NOEL willdepend on the number of animals used in thestudy and the spacing of the applied doses.
258 Toxicology, 3. Evaluation of Toxic Effects Vol. 37
8/14/2019 Toxicology (3) - Ullmann
5/22
Short-Term Tests for Specific Toxic Effects
In Vivo and In Vitro. A variety of short-termtests has been developed for the detection andquantification of toxic effects. Most of the moreestablished and well-evaluated test systems aredesigned to evaluate the genotoxic activities of
xenobiotics and employ well-defined geneticchanges (DNA damage, gene mutations, chro-mosome defects, cell transformation) in prokar-yotes, lower eukaryotes, and mammalian cells.Knowledge that a genotoxic chemical is active invivo in the target organ of carcinogenesis en-hances confidence that the genotoxicity of thechemical is important in the process of cancerinduction by that chemical. Before any short-term test can be used with confidence to assesspotential toxic effects, its validity should bethoroughly evaluated and its major drawbacksshould be explicitly noted. Moreover, it shouldbe kept in mind that most available short-termtests are well designed to give qualitative infor-mation and their major use for risk assessmentpurposes is therefore the confirmation or exclu-sion of a specific toxic response. The magnitudeof toxic response in intact animals or humansdepends on both toxicokinetics and toxicody-namics. The toxicokinetic phase of the toxic
response is not considered in most of the in vitroshort-term tests. Therefore, short-term tests invitro may be used for hazard identification onlyin combination with studies on adverse effects inanimals and studies on the toxicokinetics of axenobiotic.
Biotransformation and Toxicokinetics.
Studies on the extent of biotransformation in-cluding structural identification of the metabo-lites formed from the xenobiotic both in intact
animals and in appropriate in vitro systems suchas organ homogenates or fractions with enzymat-ic activity also contribute to hazard identification[11]. The structures of metabolites formed andthe presence and extent of covalent binding ofmetabolites to macromolecules such as proteinand DNA indicate the formation of electrophilicmetabolites and thus a potential hazard.
For example, the structure of excreted mer-capturic acids may give information on the struc-ture and reactivity of the electrophilic metabolite
and sites of cellular interactions [12]. Informa-tion on the rate of absorption and eliminationmay indicate a possible accumulation of the
xenobiotic in humans, with the consequence ofpotential adverse effects. These studies should beperformed on at least two animal species in vivo.For in vitro studies, human tissue samples shouldbe included to confirm that biotransformationreactions are identical to those, observed in ani-
mals occur in humans. Different mechanisms oftoxicity may operate at different dose levels; inthese instances, toxicokinetic data may help inunderstanding dose-dependent mechanistic dif-ferences. The toxicokinetics of a xenobiotic inhumans may be extrapolated by physiologicallybased pharmacokinetic models from the resultsobtained in experimental animals. Informationon potential pathways of biotransformation mayalso be made by computerized structure analysisof the xenobiotics with specific computer pro-grams [3, 13]. These are designed for predictingroutes and rates of biotransformation based onthe presence of functional groups in the mole-cule; however, at present, the available programsare far from perfect, and they should only be usedin conjunction with expertise and as a basis forexperimental planning.
StructureActivity Relationships and
Chemical Structure Analysis. Predictive data
on the potential of xenobiotics, mainly organicchemicals, to induce adverse effects may bederived from relationships between chemicalstructure (physicochemical properties, presenceof functional groups, atomic configuration) andbiological activity, termed structureactivityrelationships.
Two approaches to hazard prediction utilizestructureactivity relationships. The first is es-sentially a qualitative approach and involves thecomparison of the structure of the xenobiotic
with that of other compounds already known tocause specific toxic effects. The comparisonwith known structures and the knowledge ofbiotransformation reactions and mechanisms oftoxicity permits the identification of toxophoresin the structure of xenobiotics. Toxophores arefunctional groups present in the molecule whichare likely converted to toxic metabolites orposess chemical reactivity related to mechan-isms of toxicity. Examples of toxophores areolefinic moieties, which may be oxidized to
epoxides, and terminal carbon atoms in alipha-tics bearing two halogen atoms, which maybe oxidized to acyl halides. The scope and
Vol. 37 Toxicology, 3. Evaluation of Toxic Effects 259
8/14/2019 Toxicology (3) - Ullmann
6/22
usefulness of structureactivity relationshipsdepend on the availability of a sufficiently largedatabase on the toxic effects of chemicals withcommon subgroups and structures [3, 13]. Themain limitation of this approach is the qualita-tive nature of the resulting estimate of potential
toxicity. The second approach involves quanti-tative structureactivity relationships and relieson the computer-aided analysis of databases ontoxic effects of chemicals. A basic feature of theapplied techniques is the use of pattern-recog-nition schemes or substituent weighting factorscoupled with regression analysis. Some usefulpredictions have been made with these techni-ques, but due to the complex nature of toxiceffects and the multitude of factors governingthe toxic response, there are still severe limi-tations to the applicability of quantitativestructureactivity relationships for predictingtoxicity profiles.
Clinical and Epidemiological Studies. Inprinciple, the best evidence for the toxic effectsof a chemical in humans is derived from clinicaland epidemiological studies. These studies as-sess effects in the species of interest for riskassessment and at relevant concentrations. Po-
tentially confounding extrapolations from highto low dose and from animals to humans are notrequired. However, several weaknesses limit theapplicability of these studies to hazard identifi-cation. In most cases, reliable exposure data arelacking, consequently, doseresponse relation-ships cannot be established. In addition, thesensitivity of epidemiological studies to detecthealth problems is comparatively low. Unless thetoxic effect of a particular xenobiotic is veryunusual in control (unexposed) groups, it may
pass unnoticed in a normal survey. Examples arethe identification of asbestos exposure as a causeof mesothelioma or vinyl chloride as a cause ofhemangiosarcoma, very rare forms of cancer inhumans not exposed to asbestos or vinyl chloride,respectively. Moreover, the results of epidemio-logical studies, especially on cancer risk, mayreflect the risk associated with exposure to che-micals decades ago because of the long latencyperiod. Other limitations are confounding vari-ables such as smoking and concomitant exposure
to other xenobiotics, which often impair theinterpretation of carcinogenicity data in humans.Thus, evidence based on epidemiological obser-
vations has identified only a limited number ofchemicals as human carcinogens; many of the
identified compounds are used in cancer chemo-therapy and have the intrinsic property of geno-toxicity (Table 2).
2.2. Determination of Exposure
The quantification of exposure, both in indivi-duals and in populations, is a prerequisite for thequantification of risk. Reliable data on exposureare needed to assess the adverse effects of the
xenobiotic and to recognize specific risk factorssuch as occupation, life style, and social status.The dimensions of exposure include intensity,frequency, route, and duration; in addition, thenature, size, and makeup of the exposed popula-tion should be characterized. The assessment ofexposure is a difficult and complex task, and isoften neglected. Typically, estimations and fieldmeasurements are required. The estimation ofhuman exposure to a particular xenobiotic in-volves an initial estimation of the possible
sources of the chemical and the possibilities forexposure. A good inventory of sources mayprovide important information on critical path-
Table 2. Examples of established human carcinogens based on
epidemiological observations
Chemical or agent Site of tumor formation
Aflatoxin liver
Alcoholic drinks mouth, esophagus
4-Aminobiphenyl bladder
Benzidine bladder
2-Naphthylamine bladder
Arsenic skin, lung
Asbestos lung, pleura, peritoneum
Azathioprine reticuloendothelial system
Benzene bone marrow
Bis(chloromethyl) ether lung
Cadmium prostate
Chlorambucil bone marrow
Chlornaphazine bladder
Chromium lung
Cyclophosphamide bladder
Bis(2-chloroethyl) sulfide larynx, lung
Nickel compounds nasal cavity, lungEstrogens endometrium, vagina
Phenacetin kidney and lower urinary tract
Polycyclic aromatic hydrocarbons skin, scrotum, lung
Steroid hormones liver
Tobacco mouth, pharynx, larynx,
esophagus, lung, bladder
Vinyl chloride liver
260 Toxicology, 3. Evaluation of Toxic Effects Vol. 37
8/14/2019 Toxicology (3) - Ullmann
7/22
ways of exposure, populations at particular risk,and the levels of exposure.
In many cases, the duration and level ofexposure, especially after chronic contact, mayonly be estimated from ambient levels of thexenobiotic in the environment, and estimations
may thus be crude; owing to the large numbers ofpotentially exposed persons, only in special si-tuations (e.g., occupational exposure, after dis-asters), will exposure data, including determina-tion of the internal dose, be available.
Specific procedures to detect exposure to acertain xenobiotic and procedures to estimateexposure by determining biological effects maybe used. These include:
. Direct measurement of the chemical in envi-ronmental samples such as water, air, and soil.
. Measurement of the chemical, its metabolitesor products of the interaction of the chemical orits biotransformation products with cellularmacromolecules (protein and/or DNA) in bodyfluids and tissues (biomonitoring).
Biological end points in exposure assessmentmay be:
.
Assessment of biochemical indicators for spe-cific adverse effects known to be caused by thexenobiotic, e.g., inhibition of specific enzymessuch as cholinesterase activity in persons ex-posed to organophosphate pesticides.
. Observation of pathological evidence of expo-sure such as cytogenetic changes in lympho-cytes from workers exposed to chromosome-damaging chemicals at the workplace. How-ever, the use of biological end points for expo-sure assessment lacks the resolving power to
discriminate between endogenous changes andthe effects of xenobiotics, and therefore chem-ical specific indices of exposure should befavored for quantitation of exposure [5, 14].
Due to the time-consuming and cost- andlabor-intensive procedures required, data on ex-posure to xenobiotics are usually limited. Diffi-culties in identifying concomitant exposures,interactions with other xenobiotics or activities,special risk groups such as the very old or very
young and pregnant women, and patterns ofexposure result in a high degree of uncertaintyin exposure assessment in human populations.
A stepwise approach to exposure assessmentusing the following hierarchy can be applied. Themost reliable exposure assessments are based onmeasured data, including the quantification ofkey exposure determinants. When these are notavailable, appropriate surrogate data may be
used. Modeling may also be used in the absenceof useful data, but the limitations of the modelingapproach should be clearly stated.
2.3. Dose-Response Relationships
The establishment of the doseresponse relation-ship for adverse effects in animals is the decisivestep in risk assessment. This step quantifies therelationship between received or administereddose and biological response and may be per-formed on an individual or population basis.Doseresponse assessment includes exposureintensity and duration and factors modifyingtoxic response such as sex, age, health status,and route of administration. Since the doseresponse assessment can only rarely be per-formed in humans, extrapolation from data ob-tained in animals to humans is usually required.Moreover, many animal experiments, particular-
ly carcinogenicity bioassays, are performed withhigh doses to increase the sensitivity of the assay.Therefore, besides species extrapolation, an ex-trapolation from effects seen after high doses inanimals to the low doses usually encountered byhumans is necessary. This extrapolation stepfrom high, sometimes toxic doses in animals tolow doses in humans is controversial.
The extrapolations form high to low dose areperformed differently depending on the type oftoxic response elicited by the xenobiotic. As
explained in ! Toxicology, 1. Fundamentals,Chapter 1, toxic effects of a chemical may becaused by both reversible and irreversible inter-actions of the xenobiotic or its metabolite(s) withmacromolecules in the organism. Many acutetoxic responses such as carbon monoxide poi-soning are based on reversible interactions andare associated with thresholds. Threshold dosesare doses below which the probability of a re-sponse is zero. The biological basis for thresholdsis well founded and may be demonstrated on a
mechanistic basis. On the other hand, manychronic toxic responses, particulary chemical car-cinogenesis, are often considered nonthreshold
Vol. 37 Toxicology, 3. Evaluation of Toxic Effects 261
8/14/2019 Toxicology (3) - Ullmann
8/22
effects. Since a negative can never be proven,the absence of thresholds cannot be demonstratedby experiments and is based on consideration ofthe mechanisms of chemical carcinogenesis.Different approaches have thus been developedin establishing acceptable levels of exposure to
threshold and nonthreshold responses (seebelow).
2.4. Risk Characterization
The hazard identification, the exposure assess-ment, and the doseresponse assessment mergeinto risk characterisation. Risk characterisationestimates the incidence of expected adversehealth effects in exposed populations. As notedin Section 2.1, risk characterization and theestablishment of acceptable exposure levels arehandled differently for carcinogenic and noncar-cinogenic xenobiotics. For chemicals that causeadverse effects by mechanisms with thresholds,the safety factor approach was developed. Fornonthreshold responses such as cancer, bothquantitative and qualitative risk assessment pro-cedures are used.
2.4.1. The Safety-Factor Methodology
When the safety assessment of a chemical isbased on animal toxicity testing, a differentevaluation of the data is required compared tosafety evaluations relying primarily on humanobservations. Since animal experiments to deter-mine health hazards of chemicals were widelyused in the 1940s and human health risks had tobe extrapolated from these data, the idea of a
safety factor, which was to be applied to theresults from animal studies, was developed. Thesafety factor approach was first proposed in the1950s by ARNOLD LEHMANN of the FDA as aprotective measure for human health and is in-tended to compensate for uncertainties in theextrapolations of animal data to humans. Thisconcept was applied to the determination ofacceptable daily intakes (ADIs) by the WorldHealth Organization from the 1960s onward. TheADI was defined as the daily intake of a chemi-
cal which, during an entire lifetime, appears to bewithout appreciable risk on the basis of all knownfacts at that time.
The safety factor, or as it is sometimes called,the uncertainty factor, has been introduced toconsider both interspecies and interindividualdifferences in response to potential toxic effectsof the chemical under consideration. The majorpurpose of the safety factor is the protection of
human health by establishing safe exposure le-vels; the exposure levels defined do not mean thatexposure above these levels will result in adverseeffects. Despite several limitations and criti-cisms, the safety factor approach has been usedfor many years in Western Europe and the UnitedStates, and has proven useful and reliable. It wasthus adopted internationally as the standard pro-cedure for assessing the ADI.
This risk assessement approach is based on theestablishment of a point of departure for therequired extrapolation, which may be an NOELor NOAEL or a benchmark dose (e.g. ED05) inanimal studies on chronic toxicity, and thendefining permissible human exposures by theapplication of a safety factor. In this context,the NOEL is defined as the lowest dose of thexenobiotic in an animal experiment which pro-duced no detectable effect in the most sensitiveanimal species treated. Once a NOEL has beendetermined, a safety factor for human exposure is
introduced and, often, a permissible level ofexposure of one hundredth of the NOEL inanimals is defined for humans. The 100-foldsafety factor is justified on the basis of a 10-folddifference to reflect an interspecies difference insusceptibility and a 10-fold difference to reflectpossible interindividual variations in susceptibil-ity in humans [9]. The acceptable daily intake isthen obtained by dividing the NOEL from thestudy by the safety factor.
The safety-factor approach assumes that toxic
effects exerted by the chemical exhibit a doseresponse curve with a threshold, that the resultsof the toxicity studies in animals are relevant tohumans, and that extrapolation of the dose isreliable.
A similar approach is the margin-of-safety(MOS) approach which determines by how muchthe derived NOAEL exceeds the determined orestimated exposure. The size of the MOS (< 100or > 100) determines the extent of concern of aspecific exposure.
As noted above, safety factors of 100 arefrequently applied. However, when reliable datafor adverse effects of the chemicals in humans
262 Toxicology, 3. Evaluation of Toxic Effects Vol. 37
8/14/2019 Toxicology (3) - Ullmann
9/22
are available, a safety factor of only 10 may beapplied. On the other hand, a safety factor ofmore than 100 is appropriate when no or onlylimited data on the toxicity of the chemical inanimals are available. Note that the safety factoris not based on scientific evidence. Additional
data on the mechanisms of toxic effects in ani-mals and on the toxicokinetics and biotransfor-mation of the xenobiotic in animals and humansare required and add scientific credibility to theproposed safety factors. Therefore, the choice ofa safety factor should consider, in addition to theNOEL, a series of further qualitative parameters:
Evaluation of animal toxicity studies. Number of studies and effects observed. Type of toxic effects. Time course for toxic effects. Tumorigenicity
Evaluation of biochemical end points. Biotransformation and toxicokinetics. Mechanism of action, covalent binding to
macromolecules. Short-term test for genotoxicity and other non-
threshold effects
Evaluation of species differences. Interspecies variations in biotransformation
and toxicokinetics. Influence on anatomical and physiological dif-
ferences of toxic effects between species
Application of the most appropiate safetyfactor requires careful analysis of the data avail-able on the toxic effects for every chemical, on acase-by-case basis. Consideration should be giv-en to the quality and completeness of the data and
the number and spread of the dose levels used.Besides the derived NOEL, all further informa-tion obtained in the long-term animal toxicitystudies is valuable for characterizing toxic effectsand determining safety factors. The type of toxiceffect and the shape of the doseresponse curveshould also be taken into account in setting thesize of the safety factor.
Also important are considerations of the abil-ity to extrapolate from toxic effects seen inanimals to human exposure scenarios and the
results of human epidemiology studies, whenavailable. Because of the complexity of informa-tion required, no universally accepted guidelines
can be developed for determination of the precisemagnitude of safety factors; therefore, expert
judgment on an individual basis is a major factorcontributing to the size of safety factors.
The safety factor approach has several pro-blems. In experiments to determine the NOEL in
animals, the experimental group size and thespacing of dose levels are major determinantsof the numerical value of the NOEL obtained; thesmaller the size of the individual dose groups andthe larger the spacing of doses, the less likely is itthat an effect will be observed. This phenomenonhas the effect of rewarding poor experimentaldesign because small group sizes in experimentswill tend to produce higher NOELs. Moreover,nonthreshold effects may not be detected due tothe low number of animals enrolled or the doselevels applied. In addition, the slope of the dose-response curve is often not considered or may notbe determined with sufficient accuracy, and che-micals with steep and shallow doseresponsecurves are treated alike. Advantages and disad-vantages of safety factors in the risk assessmentprocess follow:
Advantages. Simple application.
Ease of understanding. Flexibility of use. Use of expert judgment
Disadvantages. Uncertainties of threshold values and size of
safety factor. No risk comparison possible. Slope of doseresponse curve not adequately
considered. Experimental NOELs are dependent on group
size in the animal toxicity testing and end pointselected
One of the most promising alternatives to theuse of NOAELs or NOELs is the benchmarkconcept [15]. In the benchmark approach, adoseresponse curve is fitted to the completeexperimental data for each effect parameter. Onthe basis of the fitted curve, the lower confidencelimit of the dose at which a predefined criticaleffect size is observed (i.e., the dose at which
adverse effects start to arise or where 5% of theanimals are predicted to be affected, effectivedose, or ED05) is defined as the benchmark dose.
Vol. 37 Toxicology, 3. Evaluation of Toxic Effects 263
8/14/2019 Toxicology (3) - Ullmann
10/22
Advantages of this approach over the NOAELare:
. The benchmark dose is derived by using allexperimental data and gives a better reflectionof the doseresponse curve.
. The benchmark dose is independent of prede-fined dose levels and spacing of dose levels.
. The benchmark approach makes more reason-able use of sample size, and better study de-signs result in higher benchmark doses.
A disadvantage of this method is the uncer-tainty with respect to the reliability of the ap-proach when results are obtained from toxicitystudies performed according to the requirementsdefined in current guidelines. For the derivationof reliable doseresponse relationships, the clas-sical study design of three dose groups and avehicle control group is limited, since adverseeffects may only be observed at the highest doselevel. An improved benchmark model fit couldbe achieved by increasing the number of dosegroups without changing the total number ofanimals in the test.
At present, the determination of a NOAEL ismandatory for risk assessment in the EU. Never-
theless, the benchmark dose method can be usedin parallel when a NOAEL cannot be establishedfor the selected toxicological end point becauseonly a LOAEL is available. In this case, bench-mark modeling preferred over LOAELNOAELextrapolation, which uses more or less arbitraryassessment factors. Benchmark dose software(BMDS) is available from the US EPA internetsite (www.epa.gov).
2.4.2. Risk Estimation Techniques forNonthreshold Effects
The procedures outlined below are most oftenapplied to the low-dose risk estimation of humanor animal carcinogens. Since doseresponse dataare not available for effects in animals at dosesrelevant to human exposure, extrapolations arerequired for determining the potential humancancer risk. The methodology employs mathe-matical modeling to characterize the relationship
between exposure and response or to place anupper bound on the doseresponse relationship.Doseresponse data, available from specific
study situations (mainly animal bioassays usinghigh doses of the chemical and, sometimes,heavily exposed population groups), are extrap-olated to the often much lower exposures of thegeneral population in order to calculate the pos-sible risk. Therefore, cancer risk assessment
generally involves extrapolating risk from therelatively high exposure levels employed in ani-mal studies, or occupational studies where cancerresponses can be measured, to risks at the rela-tively low exposure levels that are of environ-mental concern. However, since the majority ofcarcinogenicity experiments use only two orthree doses, it is impossible to assess the shapeof the dose-response with a reasonable degree ofprecision. Risk assessment must therefore rely onsome arbitrary assumptions about the shape ofthe dose-response relationship at low doses. Riskestimates thus obtained are not true or actual riskbut values obtained by extrapolation well belowthe range of experimental observations. A sum-mary of the advantages and disadvantages ofquantitative risk assessment follows:
Advantages. Gives numerical values on risk that may be
used for setting exposure limits..
Permits the comparison of risks due to differentchemicals.. Provides a reasonable basis for setting expo-
sure limits by identifying compounds with highrisk.
Disadvantages. Extrapolation of data obtained at high doses to
low doses relevant for human exposure bymeans of mathematical models which are notbased on cancer biology and pathophysio-
logy.. Mechanistic and kinetic data are not used for
the risk estimation process.. Expensive and time- consuming lifelong
bioassays are required.
The risk extrapolation techniques used arebased on several conservative default assump-tions, some unsupported by any direct empiricalevidence. Conservatism is introduced to ensuremaximum protection for those exposed to pre-
sumed chemical carcinogens. These assumptionswere adopted to achieve some consistency in theapplication of risk-estimating techniques. The
264 Toxicology, 3. Evaluation of Toxic Effects Vol. 37
8/14/2019 Toxicology (3) - Ullmann
11/22
major assumptions are (1) carcinogenic risks areestimated from the data obtained in the mostsensitive animal model only using positive re-sponses (data from bioassays that do not show atreatment-related increase in cancer incidenceare ignored); (2) linear, nonthreshold dose-risk
models are applied; (3) statistical upper confi-dence limits are used rather than best estimates;and (4) a linear doseresponse curve is assumedat low doses.
2.4.3. Mathematical Models Used in High-
to Low-Dose Risk Extrapolation
Mathematical models for quantifying humancancer risk from exposure to carcinogens werefirst developed in the 1950s. These models werebased on the one-hit or the multistage model ofchemical carcinogenesis. A probit model wasproposed in 1961 for assessing low-dose risk byextrapolation. An improved probit model wasintroduced in the 1970s by the FDA for comput-ing the level of carcinogenic chemicals permis-sible in food. This procedure included the sug-gestion that the dose causing a very low risk (oneadditional cancer in 1 000 000 exposed people) to
be considered as a virtually safe dose. Intro-duction of this mathematical model into the riskassessment process stimulated the developmentof a variety of other mathematical models forcarcinogen risk assessment. The basis of all theabove methods is to apply a mathematical modelto the tumor incidence observed in a long-termanimal bioassay.
A major problem in dose response and riskextrapolation is the determination of an appro-priate mathematical model to predict effects at
hypothetical low levels of exposure. Severalmodels have been developed, and most of themcontain analytical functions that appear to fitthe experimental dose range quite well and alsocontain a doseresponse functionality. Mostmodels differ in the functions used to estimateresponse in the very low dose range (i.e., asdose approaches zero). The mathematical mod-els in common use in carcinogen risk assess-ment are
. The linear model.
. Statistical or distribution models: logprobit,MantelBryan, logit, Weibull.
. Mechanistic models: one-hit (linear), multihit,multistage (ArmitageDoll), linearized multi-stage, Moolgavkar model.
. Other models: statisticopharmacokinetic,time-to-tumor.
Linear Model. Linear extrapolation involvesthe intersection of a straight line between theorigin (zero dose) and the upper confidence limitof the response at the single, lowest experimentaldose. This model is based on the assumption thatthe increase in tumor incidence by the appliedxenobiotic augments an already proceedingprocess.
Distribution Models are based on mathe-matical functions of presumed population char-acteristics i.e. on the assumption that everymember of a population has a critical dosage(threshold) below which the individual will notrespond to the exposure in question. The probitmodel assumes that log doseresponses have anormal distribution. This model serves as thebasis for the Mantel-Bryan risk extrapolationprocedure. Other distribution models on whichcarcinogenicity doseresponse models havebeen based include the logit and Weibull models.
Mechanistic Models are based on the cur-rently presumed mechanisms of chemical carci-nogenesis. Each model reflects the assumptionthat a tumor originates from a single cell. Theconcept underlying the one-hit model is that atumor can be induced by exposure of DNA to asingle molecule of a carcinogen. This model isessentially equivalent to assuming that the doseresponse is linear in the low-dose region and as aconsequence tends to produce very low calculat-
ed virtually safe doses compared with theother currently applied models. The multihitmodel is a generalized version of the one-hitmodel which assumes that more than one hit isrequired at the cellular level to initiatecarcinogenesis.
The biological justification for the multistage(ArmitageDoll) model is that cancer is assumedto be a multistage process that can be approxi-mated by a series of multiplicative linear func-tions. It assumes that the effect of a chemical
carcinogen occurs in multiple steps and that theeffect of each step is additive. The doseresponsepredicted by this model is approximately linear at
Vol. 37 Toxicology, 3. Evaluation of Toxic Effects 265
8/14/2019 Toxicology (3) - Ullmann
12/22
low doses and it results in estimates of potentialrisk that are similar to those of the one-hit model.
The MoolgavkarVensonKnudson modelattempts a more comprehensive consideration ofthe biologic processes of cancer formation thanthe other mechanistic models and may provide a
more accurate estimate of human risk by reduc-ing some of the interspecies uncertainty. It isbased on a two-stage growth model and considersthe birth and death of cells, the effect of cellproliferation on the number of available cells formalignant transformation, and assumes two spe-cific, irreversible, and rate-limiting mutationalevents to be necessary for cancer development.This model may quantitatively consider majorphenomena influencing cancer formation such ascell proliferation, initiation/promotion, geneticpredisposition, and synergism/antagonism.Moreover, model parameters may be obtainedexperimentally. At present, the major limitationfor the application of this model is the lack ofavailability of many of the important biologicalparameters.
Other Models. The carcinogenicity ofmany chemicals is based on their biotransforma-tion to reactive metabolites. The statisticophar-
macokinetic model arises from consideration ofcompeting metabolic activation and deactivationprocesses (e.g., detoxification and DNA repair)and estimates the effective dose, i.e., the levelof reactive metabolites formed and interactingwith critical macromeolecules, rather than theadministered dose.
A modification of the Probit model relates it tothe time at which a tumor is detected. For riskassessement, this time-to-tumor model uses thetime to observance (latency) in addition to the
proportion of animals bearing tumors at eachdose.
2.4.4. Interpretation of Data from Chronic
Animal Bioassays
The results of experimental animal studies mayprovide a variety of data in addition to the simpleindication of the presence or absence of cancer.This information may be useful for the evaluation
of potential human cancer risk and includes thenumber of neoplasms per animal, the number ofdifferent types of neoplasms observed, and the
number of species affected. The organ or targettissue in which the carcinogenic response occursis also important, as some rodents have extremelyhigh and variable spontaneous incidence of cer-tain tumor types. Where a chemical increases thenumber or accelerates the formation of neo-
plasms which spontaneously occur in high andvariable incidence, the response carries lessweight than the appearance of tumors with verylow spontaneous rates. The time to developmentof tumor will also give an indication of potency.Further considerations on the interpretation ofthe obtained data are given in ! Toxicology, 2.Assessment Methods, Chapter 8.
2.4.5. Problems and Uncertainties in Risk
Assessment
The practice of using tumor incidences obtainedin long-term animal experiments with high doses(MTD, maximum tolerated dose, see ! Toxi-cology, 2. Assessment Methods, Chapter 8) forhuman cancer risk assessment and several of theconservative default assumptions used in theextrapolation processes have become the subjectof major criticism. Some of the assumptions
made when using experimental animal data forhuman risk assessment are not directly testableexperimentally. Nevertheless, these assumptionsare widely used because risk assessment wouldbe difficult or impossible without them [9].
However, recent results on the mechanisms ofcarcinogenesis have revealed a complex biolog-ical process with many variables; a comprehen-sive consideration of all these parameters by asingle, generally applicable mathematical modelis not possible. Moreover, observations such as
nonlinear toxicokinetics and delineated mechan-isms of action for nongenotoxic carcinogenshave indicated that a more scientifically basedapproach to carcinogen risk assessment, likely ina case-by- case examination by expert panels,may be more appropriate for defining actual riskthan mathematical modeling. The major points ofcontroversy in risk extrapolation from animalexperiments and possible solutions to reduceuncertainties are described in Table 3.
Extrapolation between Species. In the ab-sence of information on the possible mechanismof carcinogenesis by a particular xenobiotic, the
266 Toxicology, 3. Evaluation of Toxic Effects Vol. 37
8/14/2019 Toxicology (3) - Ullmann
13/22
tumor incidences observed in an animal experi-ment are often assumed to be useful in assessinghuman risk. However, the differences in the
physiology and anatomy of laboratory animalsand humans are well recognized. For example,the life span of the laboratory rodent is approxi-mately two years whereas that of humans isapproximately seventy years. Cancer appears todevelop in rodents over a time scale that isproportional to the life span, and it is generallyassumed that this will apply to all chemicalsbeing assessed. The assumption that humans willrespond in a similar fashion to laboratory animals
is frequently shown to be inappropriate. Mecha-nistic studies demonstrate that qualitative andquantitative aspects of toxicokinetics and bio-transformation, DNA repair and tissue suscepti-bility, and immune and other defense mechan-isms may explain observed differences in theresponse of laboratory species and humans toexposure to carcinogens [16]. Expert judgementmay be required to assess the nature of the endpoint or the mechanisms of carcinogenic actionof the chemical in the experimental animal and to
decide whether they are relevant to man.
Extrapolation from High to Low Dose.
The use of very high doses in animal cancerbioassays and the required extrapolation formhigh to low dose are a major point of critisim.Most cancer bioassays are performed in relative-ly small groups of rodents (between 50 and 100)and with administration of high doses. The high-est dose selected is usually the maximum toler-ated dose (MTD) in order to have maximum
sensitivity and to ensure that the results obtaineddo not overlook a carcinogenic response simplybecause the dose was too low.
The following information that is obtained inbioassays with high doses in animals:
. Definite identification of compounds with car-cinogenic activity in the species.
. Information about relative potency of differentchemicals.
. Information about the carcinogenic activity ofthe test chemical, when administered alone.
. Characterization of tumor types, target organs,and presence or absence of doseresponserelationship, which permit comparison of dif-ferent chemicals and help in establishing struc-
tureactivity relationships to improve predic-tive capabilities.. Information on the lack of carcinogenicity of
many chemicals to assist priority setting inpublic health.
However, they also have the followinglimitations:
. No direct information about effects at doseslower than dose studied.
.
No information on the mechanism ofcarcinogenicity.
. No information on the effects of the test com-pound, when administered together with otherchemicals (synergistic/antagonistic effects).
. Use of high doses that may cause unspecifictoxic effects contributing to carcinogenicity.
. Acute toxic effects that may prohibit long-termadministration of specific chemicals in suffi-ciently high doses to cause tumors.
Human exposure to carcinogens usually oc-curs at doses several orders of magnitude lowerthan those used in the experiment. Clearly, the
Table 3.Uncertainties in quantitative risk assessment and the application of scientifically based methods for reduction of these uncertainties
Uncertainty Reduction by
Extrapolation between species physiologically based toxicokinetic modeling, comparative studies on toxicokinetics
Extrapolation from high to low dose toxicokinetic modeling, quantitative determination of dose response
for biochemical effects of xenobiotics (e.g., DNA adducts, genetic changes),
mechanisms of carcinogenesis
Extrapolation from controlled experimental
conditions to variable human situations
none
Conservatism elucidation of mechanism of actions
Toxicity and increased cell proliferation dose response for cell proliferation and cytotoxic effects
Dosimetry toxicokinetic modeling and physiologically based toxicokinetic modeling
Mixtures research on mechanisms of interactions
Bioassay-inherent factors in risk assessment expert judgment
Vol. 37 Toxicology, 3. Evaluation of Toxic Effects 267
8/14/2019 Toxicology (3) - Ullmann
14/22
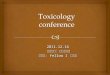
possible shape of the doseresponse relationshipis vitally important in establishing the likelyeffects at doses substantially below those in theobservable range. Mathematical models used forextrapolation only give the upper limits of risk,the real risk may be somewhere between zero andthe number calculated. Since the doseresponse
relationship can not be determined experimen-tally, application of different mathematical mod-els results in markedly different slopes of thecurves in the low-dose range (Fig. 2), and this hasmajor implications for risk assessment and theestablishment of ADI values.
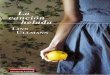
Only one study to determine the actual shapeof the doseresponse curve at low doses withgroup sizes large enough to constitute statisticalsignificance was performed, the so-called ED01study using the potent carcinogen 2-acetylami-
nofluoren as a model compound administered inthe diet to mice. Urinary bladder and liver neo-plasms were found to be related to 2-acetylami-nofluorene administration. The resulting tumorincidences showed that even within one speciesand with one specific carcinogen, there are majordifferences in the shape of the doseresponsecurve at low doses taht depend on the target organaffected. The incidence of bladder tumors at alltime points suggested the presence of a thresholdfor this end point, whereas the doseresponse
data for the liver tumors was nearly linear at alltime points and did not indicate a threshold(Fig. 3).
Extrapolation from Controlled Experi-mental Conditions to Variable Human Situa-
tions. In most animals studies, all critical fac-tors are carefully controlled to guarantee thereproducibility of experimental observations.This is in contrast to the sometimes very largedifferences and time-dependent changes in the
environmental exposure and other circumstancesof the human population, which cannot be simu-lated in animal experiments. The complexity ofthese circumstances (i.e., changing life-style fac-tors or workplaces) would necessitate an assess-ment of each human individually. Thus, riskassessment normally extrapolates directly fromthe animal data unless good evidence exists tosuggest that an important confounding factor hasbeen introduced. Besides the variable exposuresituations, the human populations exposed to
chemicals often differ in age, sex, and ethnicbackground and will certainly have a more het-erogeneous genetic makeup than experimentalanimals. For the majority of carcinogenic riskassessments, individual variability can be takeninto account only by the application of safetyfactors to compensate for these uncertainties.
Dosimetry. The problems of estimating en-vironmental and/or occupational exposure topotential carcinogens have been described
above. There are equally difficult problems inextrapolating the doses applied in animal experi-ments to those which might be encountered by
Figure 2. Possible slopes of dose response curves in thevery low dose range below the ability of experimental
determination in cancer bioassays. Experimental data point
Figure 3. Dose response data for the induction of liver
(D) and urinary bladder ( .
) tumors induced by 2-acetyla-minofluorene in mice after 24-month administration in diet
268 Toxicology, 3. Evaluation of Toxic Effects Vol. 37
8/14/2019 Toxicology (3) - Ullmann
15/22
humans due to environmental or occupationalexposure and to distinguish between adminis-tered dose and effective dose.
Doses can be extrapolated from animal ex-periments to humans by five methods:
1. Expression of dose as a function of bodyweight (mg/kg or mmol/kg).
2. Expression of dose as a concentration in foodor water (usually parts per million, i.e.,mg/gormL/L).
3. Expression of dose as a concentration ininhaled air (usually parts per million, i.e.,mL/L).
4. Correction of dose for surface area. This isachieved in a complicated process by firstraising the body weight of the laboratoryanimal to the power of 2/3 or 3/4. The correc-tion converts doses that are expressed asconcentrations in air or food to milligramsper kilogram of body weight in the laboratoryspecies. The dose is then corrected for bodysurface area and converted back to concen-trations in air or food by using appropriateconversion factors for humans. Correctionsusing surface area are based on the observa-tion that metabolic rate is proportional to body
surface area. For acute toxicity, this methodmay have some merit, but the rate of biotrans-formation may differently affect the potencyof a carcinogen, depending on the role ofbiotransformation in detoxification or activa-tion. Using correction factors for surface areaprovides data suggesting that humans may bemore susceptible to potential carcinogensthan laboratory animals compared to the dataobtained by extrapolation on the basis of bodyweight.
5. Extrapolation assuming that the tissue dose isthe primary determinant of carcinogenic re-sponse. This approach requires a study of thepathways of biotransformation and the kinet-ics of the pathway that generates the ultimateelectrophile. In vitro studies may be necessaryto obtain appropriate human data.
Further problems occur if the experiment iscarried out by a protocol that is completelydissimilar from the human experience, for exam-
ple, if animal exposure is carried out for a lifetimeand human exposure is for a shorter period or ifthe animal experiment uses an exposure route
that is not relevant for humans. As a general rulefor chemical carcinogens, where the target tissuedose is presumably the most important determi-nant of the carcinogenic potency, the total bodyburden must be computed from the various routesof exposure to assess overall dose.
Mixtures. Cancer bioassays in animals aremost often performed with a single chemical ofdefinite high purity; exposure of experimentalanimals to other chemicals or other confoundingfactors such as vector-based disease is carefullyavoided. In contrast, humans are continuouslyexposed to mixtures of chemicals and otheragents. Thus, even when animals or humans areexposed to two or more chemicals, further com-plications of data interpretation are introduced.In general, the response of the animal and thehuman will depend on whether the chemicalsactivities are interactive or not and whether theeffects of the chemicals are similar or not. If thechemicals are not interactive and the response issimilar, an additive effect may be assumed tooccur. If they are not interactive, the overallresponse may be less than additive. In addition,a variety of metabolic or infectious diseases inthe course of a humans life may have major
impact on the development of a certain tumor dueto exposure to the chemical under question. It isnot feasible to simulate these real-life factors inthe experimental situation [17].
Bioassay-Inherent Factors in Risk Assess-
ment. A variety of biological factors exist thatinfluence the assessment of carcinogenic hazard.Among these are the quality of the experiment,including the quality of the pathology, environ-mental control of animal facilities, estimation
and standardization of chemical administration,purity of the chemical administered, and manyother factors that together make up compliancewith good laboratory practice. A further problemmay be encountered if differences occur in out-come from different experiments. In the majorityof cases, some aspect of an exceptional experi-ment may explain why the response was different(e.g., use of a different strain of animal). Sinceonly positive data are used and negative data areignored for carcinogenic risk assessment purpose
to provide a conservative estimate of risk, thisfactor may also contribute to an overestimationof risk.
Vol. 37 Toxicology, 3. Evaluation of Toxic Effects 269
8/14/2019 Toxicology (3) - Ullmann
16/22
Conservatism and the Mechanisms of
Chemical Carcinogenesis. To provide maxi-mum protection, a conservative approach to riskassessment is preferred. This approach assumesthat a single molecule of a carcinogen can inter-act with DNA and produce cancer; therefore,
there can be no threshold for chemical carcino-genesis. Moreover, selection of the most sensi-tive response, irrespective of mechanism of ac-tion, and the assumption that the doseresponseis linear at low doses may overestimate risk. Thisoverestimation may be due to the unknown de-gree of conservatism at each step and to theamplification of previous bias in the assumptionby the next step. The magnitude of overstatementof risk by these conservative assumptions isunknown, but is claimed to amount to severalorders of magnitude.
Role of Toxicity and Increased Cell Prolif-
eration. Critics point out that the high doses usedin rodent carcinogenicity studies may have non-specific effects such as an increase in the rate of cellproliferation due to cytotoxic effects [18]. Theseeffects can be unique to high doses, and mitogen-esis may itself be mutagenic in numerous ways,either by errors in replication or by conversion of
endogenous DNA damage (e.g., by oxidative pro-cesses) and exogenous DNA damage to mutationsbefore repair can occur. Moreover, sustained in-creases in the rate of cell proliferation may alsoyield secondary mutational events and could beimportant in the promotional phase of carcinoge-nicity by increasing the clonal expansion of initi-ated cells and thus increasing the chance thatmultiple critical mutational events will occur[19]. Thus, cell division will increase the chanceof tumor formation. In this case, the tumor inci-
dence for the same chemical applied at much lowerdoses is likely to be much lower than a linear modelwould predict and may even be zero [4, 20, 21].Therefore, it would be important to add methodsfor determining cell division to animal cancerbioassaysandapply theobtained results to estimatelow-dose risks more adequately. Cell proliferationhas been implicated as a major contributor to thecancerogenicity of several chemicals such as phe-nobarbital, 1,4-dichlorobenzene,d-limonene, andperoxisome proliferators.
Selection of Mathematical Model. Thevarious models used in risk extrapolation fit the
experimentally observed data well; however,they predict widely differing potential risks atlow doses. Depending on the data used in thecalculation, the predicted risks may differ byseveral orders of magnitude. These differencesare inherent in the application of mathematical
models, since only two or three doses are used inthe experimental dose groups.
3. Future Contributions of
Scientifically Based Procedures to
Risk Assessment and Qualitative Risk
Assessment for Carcinogens
Since quantitative cancer risk assessment canneither claim to be a scientific basis for develop-ment of historical models nor attempt to incor-porate the large amount of scientific data on themechanism of carcinogenesis into the assessmentof risk, qualitative approaches considering allrelevant data may be the best available solutionfor risk assessment. This approach, referred to aweight-of-evidence determination of risk isincreasingly emphasized by regulatory authori-ties. The weight-of-evidence approach includes
critical evaluation of the animal bioassay and allother available information on adverse effects ofthe chemical together with biotransformation,toxicokinetics, and expert judgment [22].
The criticims outlined above have demon-strated the need for further refinement of theextrapolation procedures by toxicokinetics andstudies on the mechanisms of tumor formation.The role of animal experiments in predicting thepotential risk of human carcinogen exposure willlikely remain an important step of the risk asses-
sement process despite the obvious limitations ofthis approach [18, 23]. However, the data ob-tained with animals must be interpreted withcaution and in light of other data, both quantita-tive and qualitative, on the adverse effects of thecompound (Table 4).
Application of Toxicokinetic Models in Risk
Assessment. Information on the way in which achemical is absorbed, biotransformed, and ex-creted may be critical in extrapolating the rele-
vance of the results obtained in experimentalanimals to humans [1, 24]. For the purposes ofrisk extrapolation, it is generally assumed that the
270 Toxicology, 3. Evaluation of Toxic Effects Vol. 37
8/14/2019 Toxicology (3) - Ullmann
17/22
administered dose is proportional to the effectivedose. However, many chemicals are known to becarcinogenic only after they have been activatedto reactive electrophiles by enzymatic reactions.The amount of reactive metabolite formed mightnot be directly related to dose because saturableenzymatic processes are involved in both bioac-tivation and detoxication. The extent of bioacti-vation and detoxication may therefore be highlydose dependent, and the relationship betweenadministered dose and target dose may not belinear at all administered doses. For example,
when high-affinity, low-capacity enzymes cata-lyze the detoxication of a xenobiotic and low-affinity, high-capacity enzyme catalyze its bioac-tivation, the amount of reactive metaboliteformed is likely highly dependent on the admin-istered dose (i.e., a tenfold higher administereddose may result in a 100-fold higher effectivetarget dose). Moreover, there may be depletion ofcosubstrates required by the enzymes catalyzingbioactivation or detoxication. After the reactivemetabolite is formed, it is often deactivated by a
second enzyme, such as epoxide hydrolase orglutathione S-transferase. These enzymes canalso be saturated. The reactive metabolites thatare not destroyed by these detoxication pathwaysmay bind to DNA. The metabolites bound toDNA can be removed by saturable DNA repairsystems. These effects are referred to as nonlin-ear toxicokinetics. Nonlinear kinetics are alsoseen with chemicals inhibiting or inducing drug-metabolizing enzymes. Application of a carcin-ogen at high doses may result in the induction of
enzymes catalyzing its bioactivation and mayleave detoxifying enzymes unaffected. Thus, theexpected steady-state concentrations of reactive
intermediates present in the cell and capable ofbinding to DNA are expected to be dispropor-tionately higher after application of high doseswhich induce biotransformation enzymes thanafter low doses which leave the levels of bio-transformation enzymes unaffected. Moreover,
the metabolism of a xenobiotic may be changedas a consequence of the effects of long-termadministration of the chemical [25].
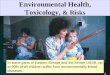
To estimate the dose-dependent relationshipbetween administered dose and the effectivedose, toxicokinetic models incorporating satura-ble processes have been applied. The examples inFigure 4 show the theoretically derived relation-ships between administered dose and effectivedose for the same chemical in animals by varyingthe kinetic parameters for bioactivation, detoxi-cation, and DNA repair [26]: saturation ofenzymatic bioactivation (A), saturation of detox-ication and activation (B), and saturation ofactivation, detoxication, and DNA repair (C).
The hockey-stick shape of the dose-responsecurve may remain unnoticed in animal experi-ments with high dose. The nonlinear correlationbetween effective dose and administered dose inthe low, relevant dose region for human exposuremay result in a decrease in the potential risk of
exposure when compared to risk estimationbased on experiments with high doses. Effectivedoses may be determined by measuring theamount of DNA adducts formed after adminis-tration of a carcinogen based on the assumptionthat for genotoxic agents the carcinogenic re-sponse is related to the extent of DNA adductformation in target tissues. Unfortunately, non-linear doseresponse curves for effective doseshave not yet been observed experimentally; allattempts to determine the dose-dependent forma-
tion of DNA adducts of potent carcinogens haveshown linear relationships between administereddose and effect [27]. However, the increasedsensitivity of analytical instruments currentlyavailable offers the opportunity to study thedoseeffect curve for a wide range of carcino-gens transformed to intermediates with differentelectrophilic reactivity in the low-dose range byquantifying the dose-dependent concentrationsof DNA lesions. Quantitation of xenobiotichemoglobin adducts and chromosomal abnor-
malities in lymphocytes (e.g., siste-chromatidexchange frequency) offers other examples ofbiological markers that may prove useful in the
Table 4. Descriptive dimensions proposed as a framework to facilitate
the use of mechanistic data in evaluation of carcinogenic risk to
humans
Data set Example of information
required
Evidence of genotoxicity DNA adduct formation,
mutagenicity, bioactivation
Evidence of effects on the
expression of genes relevant to the
process of carcinogenesis
alterations of the structure
or quantity of product of
a proto-oncogene or
suppressor gene
Evidence for effects on cell behavior mitogenesis, cell
proliferation, hyperplasia
Evidence of time and dose
response relationships and interactions
initiation, promotion,
progression
Vol. 37 Toxicology, 3. Evaluation of Toxic Effects 271
8/14/2019 Toxicology (3) - Ullmann
18/22
definition of doseresponse curves. The applica-tion of these procedures offers the advantage ofobtaining quantitative information on a nonsto-
chastic effect thought to be relevant in the me-chanisms of carcinogenesis and thus in riskassessment.
As noted in Section 2.4.5, dosimetry may be amajor cause of uncertainties in risk extrapolationform animals to humans. Besides saturable en-zymatic reactions, the effective dose of a carci-nogenic chemical may also be influenced byspecies differences in absorption, distribution
and elimination, which may also be influencedby the dose administered.
To account for such factors, physiologicallybased pharmacokinetic models are increasinglyused in the process of risk assessment. Theprincipal purpose of the application of physio-logically based pharmacokinetic models is topredict the concentration of carcinogen at thetarget site and describe the relationship betweenadministered dose and target dose over a range ofconcentrations. By application of these models, amore accurate dose extrapolation is possible overbroad ranges and may also incorporate nonlinea-rities in bioactivation and detoxification. Sincethe principles employed in the development ofthese models apply across species, the definitionof the relationship between administered doseand effective dose and the important rate pro-cesses that cause a deviation from linearity per-mits a more accurate species extrapolation. Theapplication of known physiological parameters
may also enable the prediction of target organconcentrations in humans when direct measure-ments are not possible and may permit the com-parison of different routes of application foreffective dose. Physiologically based pharmaco-kinetic models are increasingly used to supportquantitative risk assessments. Due to the riskestimates based on effective dose rather thanexternal dose levels and the consideration ofpotential nonlinear relationships, an overestima-tion of risk obtained by linear extrapolations may
be overcome and result in more scientificallyfounded risk assessments.
Mechanisms of Carcinogenicity and the
Risk Assessment Process. Research on themolecular effects of particular agents has in-creased our understanding of the mechanisms ofcarcinogenicity. A range of biological processeshas been implicated in carcinogenesis. Some ofthese mechanisms may be common to mostcarcinogens, others may be restricted to particu-
lar classes of chemicals or specific circum-stances. In spite of the incomplete knowledgeon carcinogenesis and a limited understanding of
Figure 4. Possible relationships between administered doseand effective dose for the same data set including correctionfor nonlinear toxicokineticsA) Saturation of enzymatic bioactivation; B) Saturation ofdetoxification and activation; C) Saturation of activation,detoxification, and DNA repairThe shapes of the curves in the low-dose range are shown indetail in the small sections
272 Toxicology, 3. Evaluation of Toxic Effects Vol. 37
8/14/2019 Toxicology (3) - Ullmann
19/22
many processes, mechanism.based decisions areincreasingly being introduced into risk assess-ment [28].
The emerging field of molecular toxicologymay hold promise for the future of human riskassessment, and the application of methods de-
veloped for molecular biology may also offermore accurate ways of assessing human risk. Themost promising application of mechanistic resultsfor risk assessment are non-genotoxic carcino-gens [29]. A number of xenobiotics are carcino-genic in animals but do not cause any detectablemutagenicity in in vitro studies. In contrast toother chemical carcinogens, which affect multi-ple organs or both sexes of both rat and mouse,many nongenotoxic carcinogens affect only asingle organ in a single sex of a single species[2]. There are numerous examples of xenobioticsor treatment regimens in which production oftumors in animal experiments unlikely involvesinteraction of the xenobiotic or its metabolite withDNA. Examples include the induction of subcu-taneous sarcomas by the repeated injection ofglucose or saline solutions, the induction of skincancer after chronic skin damage, and the induc-tion of bladder cancer by the implantation of solidmaterials [30]. Recent experimental evidence
also suggests that a number of xenobiotics thatdo not damage DNA may induce cancer in spe-cific organs after systemic administration. Exam-ples include chemicals binding to the circulatingproteina2u-globulin [31], peroxisome prolifera-tors, and several structurally unrelated com-pounds interacting with receptors [32] (Table 5).
The terms genotoxic and nongenotoxicwere defined by Butterworth [2]: A genotoxicagent is one for which a primary biologicalactivity of the chemical or a metabolite is alter-
ation of the information encoded in the DNA.These can be point mutations, insertions, dele-tions or changes in chromosome structure ornumber. Chemicals exhibiting such activity canusually be identified by assays that measure
reactivity with the DNA, induction of mutations,induction of DNA repair or cytogenetic effects.Nongenotoxic chemicals are those that lack gen-otoxicity as a primary biological activity. Whilethese agents may yield genotoxic events as asecondary result of other induced toxicity, such
as forced cellular growth, their primary actiondoes not involve reactivity with the DNA.
Xenobiotics such as unleaded gasoline, limo-nene, and 1,4-dichlorobenzene induce renal can-cer in male rats, but not in female rats or in eithersex of mice [33]. Metabolites of these xenobio-tics bind to the circulating proteina2u-globulin,whose synthesis in the rat is under the control ofandrogens. The modified a2u-globulin is concen-trated in the kidney proximal tubules and is notdegradable by the processes responsible for deg-radation of unmodified a2u-globulin. Thus, ac-cumulation of the modified protein causes cyto-toxicity and regenerative cell proliferation,which has been implicated as the cause of tumorformation in the kidney.
Tumors in organs whose function is regulatedby the endocrine system are often observed afterhormonal therapies in humans and hormonetreatment in animals and, due to the absence ofgenotoxicity of most hormones, nongenotoxic
processes involving receptor-mediated transcrip-tion and activation or repression of specific geneshave been implicated in hormonal carcinogene-sis [34].
For both of the above cited examples, thresh-old mechanisms may be postulated. Kidney can-cer induced by a2u-globulin-binding agents re-quires cytotoxicity and cell death. Nontoxic lowconcentrations of these xenobiotics applied maynot be tumorigenic. For receptor-mediated pro-cesses, a disproportional relationship between
receptor occupancy and hormonally mediatedcancer is also considered likely [3537]. Hence,any assessment of carcinogenic risk of thesechemicals must take into account the mechan-isms by which they produce their effects.
Table 5.Examples of nongenotoxic carcinogens and Their presumed mechanisms of action
Class of nongenotoxic carcinogen Typical examples Presumed mechanism of action
Peroxisome proliferators diethylhexylphthalate receptor-mediated increase in gene transcription, oxidative stress
a2u-Globulin-binding agents unleaded gasoline, limonene, decalin regenerative cell proliferation due to cytotoxicity
Phenobarbital mitogenic activityChlorinated dioxins 2,3,7,8-tetrachlorodibenzodioxin receptor-mediated increase in gene transcription
Hormones 17-a-ethynylestradiol receptor-mediated increase in gene transcription
Vol. 37 Toxicology, 3. Evaluation of Toxic Effects 273
8/14/2019 Toxicology (3) - Ullmann
20/22
The use of molecular toxicology in risk as-sessment is also advocated by the InternationalAgency for Research on Cancer [28]. A mono-graph on the identification of cancer risks bymechanistic investigations suggested that can-cer risks by mechanistic investigations suggests
that when available data on mechanisms arethought to be relevant to evaluation of thecarcinogenic risk of an agent to humans, theyshould be used in making the overall evaluation,together with the combined evidence for animaland/or human carcinogenicity. The consensusreport further states that no definite guidelinesfor the inclusion of mechanistic data in theevaluation of carcinogens can be elaborated.However, a range of options are available:First, information concerning mechanisms ofaction may confirm a particular level of carcin-ogen classification as indicated on the basis ofepidemiological and/or animal carcinogenicitydata. Second, for a particular agent, strong evi-dence for a mechanism of action that is relevantto carcinogenicity in humans could justifyupgrading its overall evaluation. Third, anoverall evaluation of human cancer hazard onthe basis of animal carcinogenicity data couldbe downgraded by strong evidence that the
mechanism responsible for tumor growth inexperimental animals is not relevant to humans.In keeping with the goal of public health, prior-ity must be given to the demonstration that themechanism is irrelevant to humans.
4. Risk Assessment for Teratogens
The timing of exposure and patterns of doseresponse from animal studies have important
implications for extrapolating animal data tohumans. A wide spectrum of end points can beproduced, even under the controlled conditionsof timing and exposure that can be achieved inanimal studies. In some cases, the spectrumincludes a continuum of responses, with de-pressed birth weight or functional impairmentoccurring at low doses, birth defects at interme-diate doses, and lethality at high doses. Lesscommonly, birth defects alone or lethality aloneare produced. Therefore, in estimating human
risk, all exposure-specific adverse outcomesmust be taken into consideration, and not justbirth defects.
A similar response pattern is observed in hu-mans exposed to developmental toxicants. Thespectrum of responses is determined by the timeand duration of exposure, magnitude of expo-sure, and interindividual differences in sensitivi-ty. Hence, manifestations of developmental toxi-
city can not be expected to be identical acrossspecies; that is, an animal model can not beexpected to forecast exactly the human responseto a given exposure. For instance, an agent thatinduces cleft palate in the mouse may elevate thefrequency of spontaneous abortion or retardgrowth in humans. However, any manifestationof exposure-related developmental toxicity inanimal studies can be regarded as indicative ofa spectrum of response in humans.
Epidemiological data suggest that the majo-rity of human embryos with chromosomal and/ormorphologic abnormalities are lost through earlymiscarriage and that relatively few survive toterm. Consequently, determination of malforma-tions or growth retardation at the time of birthalone (malformations, stillbirths, low birthweight) is likely to result in a substantial under-estimate of the true risk, since the onset ofembryolethality would be missed.
The sensitivity (ability to detect a true positive
response in humans) and specificity (ability todetect a true negative response in humans) oflaboratory animal studies have been evaluated[38]. Of 38 compounds with demonstrated orsuspected teratogenic activity in humans, all butone (tobramycin, which causes otological defi-cits in humans) tested positive in at least oneanimal species. Approximately 80% of the com-pounds were positive in multiple species. Apositive response was elicited to 85% in themouse, 80% in the rat, 60% in the rabbit, 45%
in the hamster, and 30% in the monkey. Thesefindings indicate that the usual laboratory animalspecies are highly sensitive for detecting humanteratogens.
In contrast to the high sensitivity, laboratoryanimals show low specificity for predicting hu-man teratogenesis; of 165 test compounds withno evidence of teratogenic activity in humans 65(41%) were positive in more than one animalspecies. The high percentage of false positiveresults (i.e., compounds with no evidence for
human teratogenicity inducing malformations inanimals may be in part accounted for by the highdoses usually applied in the animal tests. Also,
274 Toxicology, 3. Evaluation of Toxic Effects Vol. 37
8/14/2019 Toxicology (3) - Ullmann
21/22
human studies determine effects from the time ofbirth onward, which may result in underestima-tion of the true risk.
References
1 M. E. Andersen, D. Krewski, J. R. Withey, Cancer Lett. 69
(1993) 1 14.
2 B. Butterworth,Mutation Res. 239 (1990) 117 132.
3 J. Ashby,R. W. Tennant,Mutation Res. 257 (1991) 229
306.
4 B. N. Ames, L. S. Gold in T. Slaga, B. Butterworth (eds.):
Chemically Induced Cell Proliferation: Implications for
Risk Assessment, Wiley-Liss, New York 1991, pp. 1
20.
5 P. B. Farmer, H.-G. Neumann, D. Henschler,Arch. Tox-
icol.60 (1987) 251 260.6 D. M. Maloney, Environ. Health Perspect. 101 (1993)
396 401.
7 C. C. Harris, Science 262 (1993) 1980 1981.
8 J. V. Rodricks, Environ. Health Perspect. 102 (1994)
258 264.
9 F. R. Johannsen, CRC Crit. Rev. Toxicol.20 (1990) 341
367.
10 A. M. Jarabek, W. H. Farland,Toxicol. Ind. Health 6
(1990) 199.
11 D. W. Nebert, Mutat. Res. 247 (1991) 267 281.
12 R. T. H. van Welie, R. G. J. M. van Dijck, N. P. E.
Vermeulen, N. J. van Sittert, CRC Crit. Rev. Toxicol. 22
(1992) 271 306.
13 R. W. Tennant, J. Ashby,Mutat. Res.257 (1991) 209
227.
14 A. C. Beach, R. C. Gupta, Carcinogenesis 13 (1992)
1053 1074.
15 K. Crump,CRC Crit. Rev. Toxicol. 32 (2002) 133 53.
16 C. C. Travis, Toxicology 47 (1987) 3 13.
17 H. Vainio, M. Sorsa, A. J. McMichael: Complex Mixtures
and Cancer Risk, International Agency for Research on
Cancer (WHO), Lyon 1990.
18 J. A. Swenberg, R. R. Maronpot in (ed.): Chemically
Induced Cell Proliferation: Implications for Risk Assess-
ment, Wiley-Liss, New York 1991, pp. 245 251.
19 S. M. Cohen, L. B. Ellwein, Cancer Res. 51 (1991)
6493 6505.
20 B. N. Ames, L. S. Gold, Science 249 (1990) 970 1.
21 B. N. Ames, L. S. Gold,Mutat. Res. 250 (1991) 3 16.
22 G. M. Gray, J. T. Cohen, J. D. Graham,Environ. Health
Perspect.101(1993) 203 208.
23 J. C. Barrett, Environ. Health Perspect. 100 (1993) 9
20.