Embed Size (px)
Citation preview
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 1/31
Naeem Riaz
Pharmacology and Therapeutics-IVSemester VI
Poisoning and Overdose
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 2/31
Poisoning
• The adverse effects of plants, foods,
chemicals or pharmaceutical agents on
the body
Overdose
• Poisoning by excessive dose

7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 3/31
Accidental Deliberate
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 4/31
Two Peak Age Groups
• The first group,preschool age when
children are exploring there environment
• The second group is young adult age
group, when ingestion is a form or suicidal
behavior
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 5/31
General Assessment
• Management of poisoning is primarily supportive – Basic Life Support (BLS)
– Level Of Consciousness (LOC)
– Airway
– Breathing
– Circulation• Pulse
• Hemorrhage
• Skin color
• Skin temperature
• Skin Condition – Redness
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 6/31
History
• When, what, how much ?
• Why?
• Circumstances
• Drug history
• Psychiatric history
• Assess mental status and capacity
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 7/31
Specific Medical Questions
• Poisoning & Overdose History
– Substance – When exposed/ingested
– Amount
– Time Period
– Estimated weight
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 8/31
Obtains SAMPLE History
• S = Signs and symptoms
• A = Allergies
• M = Medication• P = Pertinent medical history
• L = Last oral intake
• E = Events
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 9/31
Initial Symptoms of Poisoning
• Pain
• Fluid imbalance
• Water and electrolyte imbalance• Acidosis
• Body temperature disregulation
• Malnutrition
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 10/31
Signs and Symptoms of Poisoning
• Central Nervous System Involvement
– Convulsion
– Coma
– Hyperactivity, Delirium, and Mania
• Hypoglycemia
• Hypoxia and depressed respiration
– Maintenance of Adequate Airway – Oxygen Administration
– Pulmonary Edema
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 11/31
Sign&Symptoms of Poisoning
• Circulatory System Involvement
– Circulatory failure or shock
– Congestive heart failure
– Cardiac arrest
• Genitourinary Tract Involvement
– Acute renal failure
– Urine retention
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 12/31
S&S of Poisoning
• Gastrointestinal Tract Involvement
– Vomiting
– Diarrhea
– Abdominal distention
• Blood and Hematopoietic System Involvement
– Methemoglobinemia
– Agranulocytosis and other blood dyscrasias
– Hemolytic reactions
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 13/31
General Comments
• Try and get as much history as possible including
witnesses
• People truly wanting to commit suicide often lie
• Remember the ABCs:
– Airway Clear mouth & throat, gag reflex
– Breathing O2 saturation, ABGs (Arterial BloodGas
– Circulation Venous access, IV fluids if shocked
• Examination
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 14/31
Investigations
• Always check blood glucose.
• Send blood & urine for toxicology screening.
• ALWAYS measure paracetamol & salicylate levels
– Failure to diagnose & treat is negligent.
• U&Es, LFTs, glucose, clotting, bicarbonate
• ECG, CXR (Chest X Ray)
• Specific blood levels
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 15/31
Management
• Supportive – Correct hypoxia, hypotension, dehydration, hypo-
hyperthermia, and acidosis
– Control seizures
• Monitor
– TPR, BP, ECG, Oxygenation,
• General
– Absorption
– Elimination
– Specific antidotes
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 16/31
Absorption
• Gastric lavage
– Only if within 1 hour & life-threatening
amount
– Never for corrosives
• Activated charcoal
– 50 g single or repeated dose (
elimination)
– Doesn’t bind heavy metals, ethanol, acids
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 17/31
Elimination
• Multiple dose activated charcoal
– Quinine, phenobarbitone
• Diuresis• Urinary alkalinization
– salicylates
• Dialysis
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 18/31
Drug Toxicology
• Paracetamol
• Salicylates
• CNS depressants• CNS stimulants
• Antidepressants
• Digitalis• Organophosphates
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 19/31
Paracetamol Overdose
• Acetaminophen
• Most common analgesic drug taken in overdose
• Often found in combination with antihistamines,
codeine Few symptoms or early signs
• As little as 12g can be fatal
• Hepatic and renal toxin
– Centrolobular necrosis, jaundice• More toxic if liver enzymes induced or reduced ability
to conjugate toxin
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 20/31
Pharmacokinetics
• Tablets dissolve rapidly
• Peak level 3-4 hours after ingestion
– May be delayed in the presence of other drugs(eg, antihistamines, anticholinergics, opiates)
• Volume of Distribution approx. 1L/kg
• Elimination half-life normally 1-3 hours
– Increased to 4-6 hours or more after overdose
Acetaminophen
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 21/31
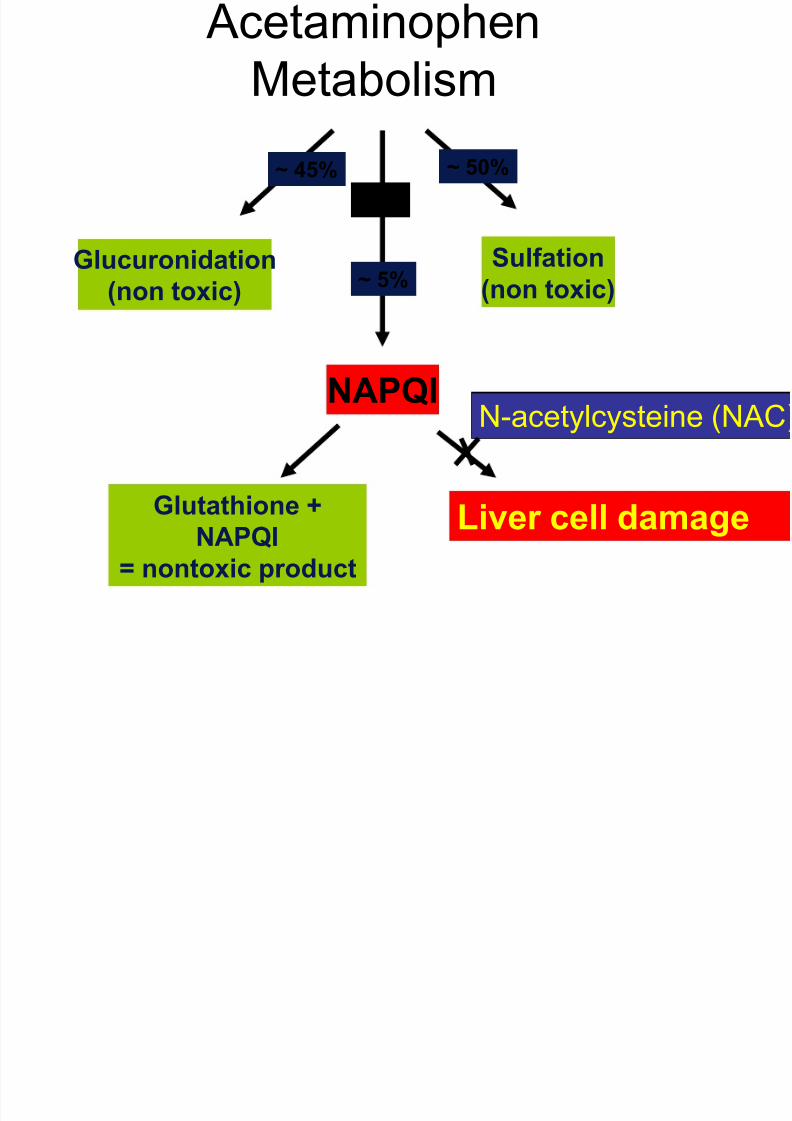
Acetaminophen
Metabolism
Glucuronidation
(non toxic)
Sulfation
(non toxic)
NAPQI
P450
~ 5%
Glutathione +
NAPQI
= nontoxic product
Liver cell damage
N-acetylcysteine (NAC
~ 45% ~ 50%
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 22/31
N-acetylcysteine
• Supplies glutathione
• Dosage for NAC infusion - ADULT – (1) 150mg/kg IV infusion in 200ml 5% dextrose over 15
minutes, then
– (2) 50mg/kg IV infusion in 500ml 5% dextrose over 4hours, then
– (3) 100mg/kg IV infusion in 1000ml 5% dextrose over 16hours
• Side-effects – Flushing, hypotension, wheezing, anaphylactoid reaction
• Alternative is methionine PO (<12 hours)
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 23/31
Management
• General measures including
– U&Es, LFTs, glucose, clotting, bicarbonate,paracetamol and salicylate levels
– Activated charcoal
• <8 hours – Start N-aceylcysteine if above treatment line
– Patients are usually declared fit for discharge frommedical care on completion of its administration.
However, check creatinine and ALT beforedischarge. Patients should be advised to return tohospital if vomiting or abdominal pain develop or recur.
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 24/31
Management
• >8 hours – Urgent action required because the efficacy of
NAC declines progressively from 8 hours after the overdose
– Therefore, if > 150mg/kg or > 12g (whichever isthe smaller) has been ingested, start NACimmediately, without waiting for the result of theplasma paracetamol concentration
• >24 hours
– Still benefit from starting NAC
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 25/31
Aspirin
• Aspirin is a widely prescribedantiplatelet therapy for cardiovascular andcerebrovascular disease
• When combined with the factthat aspirin is readilyavailable, aspirin toxicityremains an important clinicalproblem
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 26/31
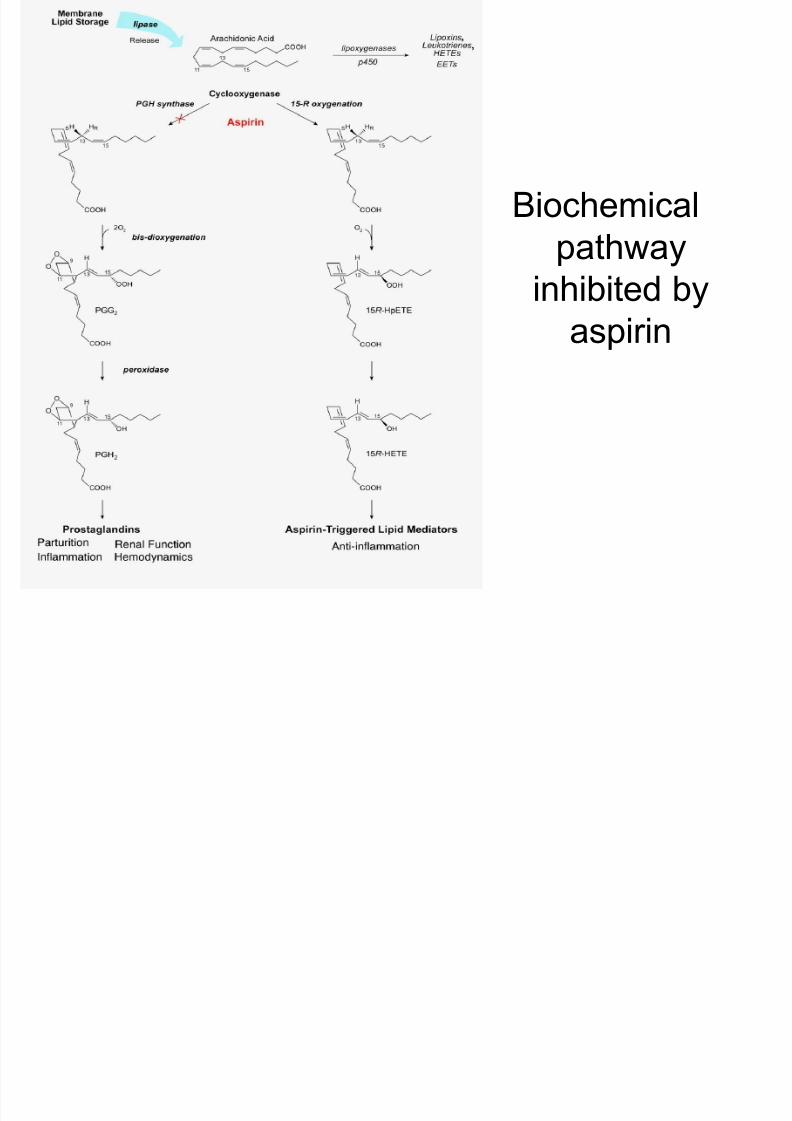
Biochemical
pathway
inhibited byaspirin
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 27/31
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 28/31
Pharmacokinetics
• Rapidly absorbed in the stomach
– Reach peak levels in 15-60 minutes
• 90% bound to albumin in the blood at a dose
of 10 mg/dL
• 90% metabolized in the liver, 10% unchanged
• T1/2 = 15-20 minutes• Metabolites and unchanged drug are filtered
and secreted by the kidneys
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 29/31
Toxicokinetics
– Peak blood concentrations may be delayed 2-4 hours
• 76% bound to albumin at a dose of 40mg/dL
– increased free drug in the blood
• Hepatic enzymes become saturated andelimination follows zero-order kinetics
– Functional half-life can be over 20 hours
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 30/31
Diagnosis
• Serum salicylate concentrations andconcomitant arterial blood pH values can
definitively confirm or exclude toxic salicylate
levels
7/29/2019 Toxicology Lect 2
http://slidepdf.com/reader/full/toxicology-lect-2 31/31
Management• General measures
• Blood – Salicylate level >2 hours, and after 2hrs
– >700mg/L potentially lethal
– >500mg/L moderate-severe poisoning
– U&Es, glucose, ABG, bicarbonate
• Activated charcoal
• Rehydrate, monitor glucose, correct acidosis and K+
• If levels >500mg/L alkalinize urine (HCO3-
)• Levels > 700 mg/L before rehydration, renal failure
or pulmonary oedema consider haemodialysis