Embed Size (px)
Citation preview

Lipid Lowering DrugsLipid Lowering Drugs
www.freelivedoctor.com

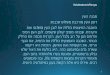
Pathways of Lipid Transport & Pathways of Lipid Transport & Inherited HyperlipidemiasInherited Hyperlipidemias
Familial HyperTriGlyceridemia Familial HyperTriGlyceridemia – LPL deficiency etc. RARE– LPL deficiency etc. RARE
Familial Combined Hypertriglyceridemia Familial Combined Hypertriglyceridemia – Polygenic. VERY COMMON – Polygenic. VERY COMMON
(ApoB) Remnant Removcal Disease – Remnant Removcal Disease – ApoE deficiency. UNCOMMON ApoE deficiency. UNCOMMON
Familial Hypoalphalipoproteinemia Familial Hypoalphalipoproteinemia (Tangier’s Disease) – HDL low. RARE(Tangier’s Disease) – HDL low. RARE
Familial Hyper- Familial Hyper- cholesterolemia – LDL cholesterolemia – LDL receptor deficiency. receptor deficiency. COMMON. COMMON. Heterozygotes ~1:500.Heterozygotes ~1:500.
X
X = HMG-coA Reductase step – blocked by Statins
www.freelivedoctor.com

Endemic Hyperlipidemias Endemic Hyperlipidemias
66% UK population have a Total cholesterol >5.2 mmol/L
Reflects high dietary fat, obesity and genotype
Secondary causes should be excluded* but explains only a minority of cases
* Liver or biliary disease, hypothyroidism, diabetes, nephrotic syndrome or drug-induced (etretinate, HAART, thiazides, OC, glucocorticoids, -blockade and ciclosporin)
www.freelivedoctor.com

Management StrategyManagement Strategy Who to treat?
Primary – 10 yr risk of event 30%
Secondary - Established IHD or CVD
What degree of hyperlipidemia should trigger intervention? Total cholesterol > 5mmol/L (or LDL >3)
What are the specific interventions Correct secondary causes – if possible
Dietary modification – in all subjects
Drug Rx – for vast majority a statin www.freelivedoctor.com

Dietary InterventionDietary Intervention
Step II diet has <30% of calories as fat, <7% as saturated fat and <200mg cholesterol/day.
Can achieve a fall in LDL-C of 8-15% … but long-term compliance a problem.
Has useful 2ary benefits Weight reduction BP reduction Reduced insulin resistance Improve intake vitamins & fresh fruit/vegetables
(folate and antioxidants)
www.freelivedoctor.com

General points about StatinsGeneral points about Statins
They competitively and potently inhibit HMG-CoA reductase (in nM range) leading to 2ary upregulation of surface LDL receptors
They have short half-lives (~2 hours except atorvastatin at 14h) but effective with once daily administration
All have slightly higher efficacy if given at night
All except pravastatin are metabolised through CYP enzymes in the liver (usually 3A4) which is the source of important interactions
Major side effects – hepatitis (stop if ALT rises > 3x ULN) and myositis
www.freelivedoctor.com

Clinical Trials in Primary and Secondary Clinical Trials in Primary and Secondary Prevention of IHDPrevention of IHD
Study
No. ofPatients
Follow-up(yrs) Drug
LDL/HDLChange (%)
Total Mortality(%)
CHD Death,Nonfatal MI (%)
PTCA, Bypass(%)
Primary prevention
LRC-CPPT[4] 3806 7.4 BAS -13/2 -7 -19 NR
AFCAPS/TexCAPS[14]
6605 4.8 Lovastatin -25/6 NR -40 -33
WOSCOPS[13] 6595 4.9 Pravastatin
-26/5 -22 -31 -37
HHS[8] 4081 5 Gemfibrozil
-10/10 0 -34 NR
Secondary prevention
CDP[7] 1119 15 Niacin -10/NA -11 NR NR
4S[12] 4444 5.4 Simvastatin
-35/8 -30 -34 -34
CARE[11] 4159 5 Pravastatin
-28/2 -9 -24 -27
LIPID[10] 9014 6 Pravastatin
-25/6 -22 -24 -20
PostCABG[16] 1351 4.3 + 3a Lovastatin -40/4 -35 -31 -30
VA-HIT[9] 2531 5.1 Gemfibrozil
0/6 -11 -22 -9
BIP[5] 3090 6.2 Bezafibrate
-7/18 +6 -11 -4
POSCH[6] 838 14.7 Surgery -38/4 -25 -40 -69
LRC-CPPT = Lipid Research Clinics-Coronary Primary Prevention Trial; BAS = bile acid sequestrant; NR = not reported; AFCAPS/TexCAPS = Air Force/Texas Coronary Atherosclerosis Prevention Study; WOSCOPS = West of Scotland Coronary Prevention Study; HHS = Helsinki Heart Study; CDP = Coronary Drug Project; NA = not applicable; 4S = Scandinavian Simvastatin Survival Study; CARE = Cholesterol and Recurrent Events; LIPID = Long-Term Intervention with Pravastatin in Ischaemic Disease; PostCABG = Post Coronary Artery Bypass Graft Trial; VA-HIT = Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial; BIP = Bezafibrate Infarction Prevention Study; POSCH = Program on the Surgical Control of Hyperlipidemias.www.freelivedoctor.com

ELIGIBILITY: MRC/BHF Heart Protection Study ELIGIBILITY: MRC/BHF Heart Protection Study (HPS)*(HPS)*
Increased risk of CHD death due to prior disease:
Myocardial infarction or other coronary heart disease;
Occlusive disease of non-coronary arteries; or
Diabetes mellitus or treated hypertension
Age 40-80 years
Total cholesterol 3.5 mmol/l ( 135mg/dl)
Statin or vitamins not considered clearly indicated or contraindicated by patient’s own doctors
* Lancet 2002;360:7-22
www.freelivedoctor.com

PRIOR DISEASE at BASELINEPRIOR DISEASE at BASELINE
Prior disease Number Percentage
Any MI 8510 41%Other CHD 4876 24%No CHD* 7150 35% Cerebrovascular 1820 Peripheral vascular 2701 Diabetes 3982
ALL PATIENTS 20,536 100%
* Overlap between categories within “No CHD” group
www.freelivedoctor.com

TOTAL & LDL CHOLESTEROLTOTAL & LDL CHOLESTEROLterciles at BASELINEterciles at BASELINE
Baseline lipids Number Percentage
LDL cholesterol (mmol/l)<3.0 (116 mg/dl) 6793 33%3.0 <3.5 5063 25%3.5 (135 mg/dl) 8680 42%
Total cholesterol (mmol/l)<5.0 (193 mg/dl) 4072 20%5.0 <6.0 7883 38%6.0 (232 mg/dl) 8581 42%
www.freelivedoctor.com

SIMVASTATIN 40mg daily:SIMVASTATIN 40mg daily: Muscle symptoms Muscle symptoms
Muscle pain orweakness
SIMVASTATIN(10,269)
PLACEBO(10,267)
P-value
Ever reported 3380 (33%) 3410 (33%) NS
Stopped tablets 49 (0.5%) 50 (0.5%) NS
www.freelivedoctor.com

SIMVASTATIN 40mg daily:SIMVASTATIN 40mg daily: Safety monitoring Safety monitoring
Blood enzymes (x upper limit of normal)
SIMVASTATIN (10,269)
PLACEBO (10,267)
Liver: ALT >4 x ULN 43 (0.42%) 32 (0.31%)
Muscle: CK 4 –10 x ULN 19 (0.09%) 13 (0.05%)
CK >10 x ULN 11 (0.11%) 6 (0.06%)
Myopathy* 10 (0.10%) 4 (0.04%)
*Muscle symptoms with CK >10 x ULN
www.freelivedoctor.com

Fatal Rhabdomyolysis with StatinsFatal Rhabdomyolysis with Statins• Rare – probably a class effect• Appears to be dose-dependent
– implications for superstatins• Risk increased by combination with fibrate
– Fibrates especially for gemfibrozil/cerivastatin– Nicotinic acid– Protease Inhibitors (HAART therapy)– Interacting drugs affecting metabolism through CYP pathway
FDA 2001 DataFDA 2001 Data Lova-Lova- Prava-Prava- Simva-Simva- Fluva-Fluva- Atorva-Atorva- Ceriva-Ceriva- AllAll
Cases 19 3 14 0 6 31 73
Total Scripts 99.2 81.4 116 37.4 140 9.8 484
Rate/million scripts 0.19 0.04 0.12 0 0.04 3.16 0.15
www.freelivedoctor.com

SIMVASTATIN: CORONARY EVENTSSIMVASTATIN: CORONARY EVENTS & REVASCULARISATION& REVASCULARISATION
(10269) (10267)
SIMVASTATIN PLACEBO Rate ratio & 95% CI
STATIN better PLACEBO better
Major coronary event
357 574Non-fatal MI587 707Coronary death
(8.7%) (11.8%)27% SE 4reduction
898 1212
(2P<0.00001)
CORONARY EVENTS
Revascularisation
513 725Coronary450 532Non-coronary
(9.1%) (11.7%)24% SE 4reduction
939 1205
(2P<0.00001)
REVASCULARISATIONS
0.4 0.6 0.8 1.0 1.2 1.4
www.freelivedoctor.com

SIMVASTATIN: MAJOR VASCULAR EVENTSSIMVASTATIN: MAJOR VASCULAR EVENTS
(10269) (10267)
SIMVASTATIN PLACEBO Rate ratio & 95% CI
STATIN better PLACEBO better
Vascularevent
898 1212Major coronary
444 585Any stroke
939 1205Revascularisation
(19.8%) (25.2%)24% SE 3reduction
2033 2585
(2P<0.00001)
ANY OF ABOVE
0.4 0.6 0.8 1.0 1.2 1.4
www.freelivedoctor.com

SIMVASTATIN:SIMVASTATIN:MAJOR VASCULAR EVENT by YEARMAJOR VASCULAR EVENT by YEAR
0 1 2 3 4 5 60
5
10
15
20
25
30
Years of follow-up
5(3) 20(4) 35(5)
SIMVASTATIN
PLACEBO
46(5) 54(7) 60(18)Benefit/1000 (SE):
Pe
op
le s
uff
eri
ng
eve
nts
(%
)
www.freelivedoctor.com

SIMVASTATIN: MAJOR VASCULAR EVENTSIMVASTATIN: MAJOR VASCULAR EVENTby LDL & TOTAL CHOLESTEROLby LDL & TOTAL CHOLESTEROL
(10269) (10267)SIMVASTATIN PLACEBO Rate ratio & 95% CI
STATIN better PLACEBO betterLipid levelsat entry
LDL cholesterol (mmol/l)
598 756(17.6%) (22.2%)< 3.0 (116 mg/dl)
484 646(19.0%) (25.7%) 3.0 < 3.5
951 1183(22.0%) (27.2%) 3.5 (135 mg/dl)
Total cholesterol (mmol/l)
360 472(17.7%) (23.1%)< 5.0 (193 mg/dl)
744 964(18.9%) (24.5%) 5.0 < 6.0
929 1149(21.6%) (26.8%)> 6.0 (323 mg/dl)
24% SE 3reduction(2P<0.00001)
2033 2585(19.8%) (25.2%)ALL PATIENTS
0.4 0.6 0.8 1.0 1.2 1.4
www.freelivedoctor.com

SIMVASTATIN: Main conclusionsSIMVASTATIN: Main conclusions
After allowance for non-compliance, 40mg daily simvastatin safely reduces the risk of heart attack, of stroke, and of revascularisation by about one-third
5 years of statin treatment typically prevents these “major vascular events” in about:
100 of every 1000 people with previous MI 80 " " " other CHD 70 " " " cerebrovascular disease 70 " " " other arterial disease 70 " " " diabetes (age 40+)
irrespective of cholesterol level (or age, or sex, or other treatments)
www.freelivedoctor.com

05
10152025303540
Cor o
nary
Even
t R
ate
(%
)
Sacks FM et al. Sacks FM et al. CirculationCirculation 2002;105:1424-1428. 2002;105:1424-1428.
Prospective Pravastatin Pooling Project: Prospective Pravastatin Pooling Project: Coronary Event Rates in CARE and LIPID Coronary Event Rates in CARE and LIPID Patients with Baseline LDL-C <3.3mmol/LPatients with Baseline LDL-C <3.3mmol/L
<60 F M + — + — + — >27
<27
<40
>40
>150
<150
Age Sex HTN Smoking DM BMI HDL-C TG
*****PravastatinPravastatin
PlaceboPlacebo
*p=.004*p=.004**p (interaction) =.005**p (interaction) =.005
>60

Cumulative Coronary Event Rates in Cumulative Coronary Event Rates in Diabetic and Nondiabetic Patients with Diabetic and Nondiabetic Patients with
Baseline LDL-C <3.3mmol/LBaseline LDL-C <3.3mmol/L
0
5
10
15
20
25
30
35
40
Cu
mu
lati
ve R
isk
of
Coro
nary
E
ven
t or
Pro
ced
ure
(%
)
Years Follow-up
Sacks FM et al. Sacks FM et al. CirculationCirculation 2002;105:1424-1428. 2002;105:1424-1428.
0 1 2 3 4 6 75
Placebo DiabeticPravastatin NondiabeticPravastatin DiabeticPlacebo Nondiabetic

Are the effects of Statins solely Are the effects of Statins solely explained by reduction in explained by reduction in
cholesterol ?cholesterol ?
Atherosclerosis can be viewed as an inflammatory process
Statins could affect inflammatory process by 2ary effect on LDL uptake by macrophages (as
source of CRP) 1ary effect on the acute phase-response
Both scenarios suggest an exclusive focus on cholesterol reduction may be misplaced

Cardiovascular Risk Prediction:Cardiovascular Risk Prediction: the role of hs-CRP (1) the role of hs-CRP (1)
Women’s Health Survey – Women’s Health Survey – long term effects of ASA & long term effects of ASA & vit Evit E
Baseline samples from Baseline samples from 27,939 patients27,939 patients
Mean age 55. 25% had HT, Mean age 55. 25% had HT, 12% smoked, 45% on HRT & 12% smoked, 45% on HRT & 2.5% had DM2.5% had DM
Followed for mean of 8 yearsFollowed for mean of 8 years
Endpoint of MI, stroke, Endpoint of MI, stroke, revascularization of CV revascularization of CV deathdeath
Ridker et al, NEJM 2002;347:1557

Cardiovascular Risk Cardiovascular Risk Prediction:Prediction:
the role of hs-CRP (2) the role of hs-CRP (2)
CRP provides additional risk prediction to that provided CRP provides additional risk prediction to that provided by Framingham risk assessor across all LDL-C groups.by Framingham risk assessor across all LDL-C groups.

Statins have an Effect on Statins have an Effect on Inflammatory Markers such as CRPInflammatory Markers such as CRP
CHEST study (Heart 2003;5:2-7) – in 80 dyslipidaemic patients statins (atorva, simva and pravastatin) reduced CRP at 1 week with further falls up to 12 weeks. Fall in CRP correlated closely with the fall in LDL-cholesterol
PRINCE study (JAMA 2001;286:9) – primary prevention study of 1702 subjects randomised to placebo or 40mg prava and CRP followed to 24 weeks. Prava reduced CRP by 17%
Atheroscleosis 2003;166:129 – 186 Type2 DM patients randomised to placebo or 10/80mg atorvastatin. Atorva reduced CRP by 15 & 47% without significant effect on plasma IL-6

Platelet Receptor Inhibition in Platelet Receptor Inhibition in Ischemic Syndrome Management Ischemic Syndrome Management (PRISM): Statin Therapy Reduced (PRISM): Statin Therapy Reduced
Event RateEvent Rate
02468
1012141618
Event
Rate
s [M
ort
alit
y, M
I] (
%)
30-day Follow-up Period0 1 2 3 4 75
Heeschen C et al. Heeschen C et al. CirculationCirculation 2002;105:1446-1452. 2002;105:1446-1452.
Statins discontinuedStatins discontinued
No statinsNo statins
Statin continuedStatin continued

Current Unresolved Issues on the Current Unresolved Issues on the Use of StatinsUse of Statins
For For secondary preventionsecondary prevention we should treat all patients with we should treat all patients with established IHD but …established IHD but …
How soon after an event should they be started?How soon after an event should they be started?
Is dose-titration versus LDL-chol still appropriate?Is dose-titration versus LDL-chol still appropriate?
Should we simply put all patients on a high dose of a statin Should we simply put all patients on a high dose of a statin without titration in keeping with HPS?without titration in keeping with HPS?
For For primary preventionprimary prevention is the current threshold of 30% risk is the current threshold of 30% risk over 10 years too stringent? over 10 years too stringent?

FibratesFibrates FA oxidation in muscle and
liver and lipogenesis in the liver
Most effective at reducing VLDL (TG); smaller in LDL-chol but useful in HDL-chol
Act as PPAR ligands (cf glitazones) - reduced expression of Apo C11 is key to VLDL catabolism
Main side effects
GI intolerance
1-2% increase in the incidence of gallstones
Important interactions
increased risk of myositis on a statin
reduction in dose requirements (~30%) for patients on warfarin

Nicotinic AcidNicotinic Acid 1ary effect is reduced FA mobilization from the periphery
hepatic VLDL synthesis
Is the agent with largest impact on HDL, and the only agent that lowers Lp(a) (by ~ 30%)
Usually employed in combination with fibrate, resin or statin – this avoids side effects of higher doses
Major side effectsFlushing – prostaglandin mediatedSkin drying & GI intolerance

Anion-Exchange ResinsAnion-Exchange Resins Sequester bile acids (BA) in the
gut hence blocking enterohepatic cycling of BA e.g. cholestyramine and colestipol
2ary effect on cholesterol synthesis actually VLDL and hyperTG may limit use
Usually used in combination with a statin
Major side effect – not palatable and constipate
Important interactions – bind polar drugs such as warfarin, digoxin, thyroxine and statins give 1 hr before resin

‘‘Super’ StatinsSuper’ Statins New ‘Superstatins’
Rosuvastatin launched 2003, Pitavastatin expected 2005
‘Super’ is an exaggeration
Do we really need them?
No doubt that reduction in ischaemic end-points is a class-effect
Proven safety should probably be the major concern following cerivastatin withdrawal
Older statins going generic i.e. costs likely to fall

Does the intensity of Lipid reduction Does the intensity of Lipid reduction matter?matter?
PROVE IT-TIMI 22 Trial (NEJM 2004; 350:1495)
designed as a non-inferiority study of the two agents
4162 patients within 10 days of an ACS were randomized to pravastatin 40mg/d or atorvastatin 80mg/d
followed up for mean of 24 months
Atorvastatin limb produced a 16% reduction in primary end point events
LDL-cholesterol was 1.6 mmol/l vs 2.46 in pravastatin limb
Note early separation of event curves vs. 12-18 m delay in 2ary prevention trials – does this still reflect differences in the pleiotropic actions of the 2 statins?

The Z phase of the A to Z Trial: intense The Z phase of the A to Z Trial: intense vs leisurely simvastatin, SS vs leisurely simvastatin, SS
• Patients with ACS randomised to either SS 40mg/d for 1/12 then 80mg/d OR placebo for 4/12 then SS 20mg/d
• No difference in 1ary end point (composite CV death, non-fatal MI, ACS or need for revasc) in first 4/12
• Differences only obvious after 6-8/12
• Only 10 episodes of myopathy (9 in intense limb)
0
0.5
1
1.5
2
2.5
3
3.5
0m 1m 4m 8m 24m
LDL-C levels
Intense
Leisurely

Newer Therapies - EzetimibeNewer Therapies - Ezetimibe Novel inhibitor of intestinal cholesterol
transporter (? SR-B1)
Rapidly metabolised to glucuronide (EZEG) – which has 400x the potency of EZE and prolongs action by enterohepatic cycling
No important adverse effects OR significant drug interactions
Effective in mild/moderate HC as monotherapy or in combination with statins for moderate/severe HC where it acts synergistically
Unlike resins does not raise TG - actually falls and again synergism with a statin
www.freelivedoctor.com

Emerging Therapy - TorcetrapibEmerging Therapy - Torcetrapib
Novel inhibitor of cholesteryl ester transfer protein, (CETP), that is normally responsible for transfer of these esters from HDL to Apo-B1 => fall in HDL-cholesterol content and particle size.
NEJM 2004;350:1505NEJM 2004;350:1505
• small rise in HDL with atorvastatin 20mg/d• much larger and dose-dependent rise with Torcetrapib
www.freelivedoctor.com

Important pointsImportant points Hyperlipidemia is common and a major risk factor for
IHD and stroke
Intervention with a statin is highly effective and can reduce risk by ~ 1/3rd
Statins are safe but still under prescribed even to high risk groups (e.g. diabetics)
HPS has still to impact on guidelines and clarification needed on the dogma of dose-titration
Prescription of statins is likely to expand substantially driven by appearance of generics and OTC sales?
www.freelivedoctor.com