Embed Size (px)
Citation preview

RESEARCH ARTICLE
Tumor necrosis factor-α 238 G/A polymorphism and gastriccancer risk: a meta-analysis
Jian-yong Yu & Li Li &HengMa &Kai Liu &Xurui Cheng &
Yan-liang Li & Xi-lin Song
Received: 26 May 2013 /Accepted: 24 June 2013 /Published online: 31 July 2013# International Society of Oncology and BioMarkers (ISOBM) 2013
Abstract Though many studies were performed to assess theassociation between tumor necrosis factor-α (TNF-α) 238G/Apolymorphism and gastric cancer risk, there were no conclu-sive findings. A meta-analysis of previous published stud-ies was performed to get a comprehensive assessment ofthe association between TNF-α 238 G/A polymorphismsand gastric cancer. The pooled odds ratios (ORs) and 95 %confidence intervals (95 % CIs) were calculated to assess theassociation. Fifteen studies with a total of 7,795 participantswere finally included into this meta-analysis. Overall, there wasan obvious association between TNF-α 238 G/A polymorphismand increased risk of gastric cancer (Avs. G: OR=1.32, 95%CI1.02–1.72, P=0.036; GA vs. GG: OR=1.32, 95 % CI 1.01–1.72, P=0.042; and AA/GAvs. GG: OR=1.34, 95 % CI 1.02–1.76, P=0.036). Subgroup analysis by ethnicity showed thestatistically significant association between TNF-α 238 G/Apolymorphism and gastric cancer was limited to Asian popula-tions (Avs. G: OR=1.59, 95 % CI 1.29–1.97, P<0.001; GAvs.GG: OR=1.63, 95 % CI 1.29–2.04, P<0.001; and AA/GA vs.GG: OR=1.64, 95 %CI 1.31–2.05, P<0.001), and there wasno obvious association in Caucasians. In conclusion, TNF-α238 G/A polymorphism is significantly associated with in-creased risk of gastric cancer, especially in Asians.
Keywords TNF-α 238 G/A a . Gastric cancer .
Polymorphism .Meta-analysis
Introduction
Gastric cancer is one of the most common cancers and causesserious damage to human health in the world [1]. Previousstudies have suggested that gastric cancer is a multifactorialdisease, and both environmental and genetic factors playimportant roles in the development of gastric cancer [2, 3].Tobacco smoking and Helicobacter pylori infection havebeen identified as major risk factors of gastric cancer [2, 3].H. pylori infection can cause chronic inflammation in thestomach, which may further result in the development ofgastric cancer [4, 5]. Tumor necrosis factor-α (TNF-α) isan inflammatory cytokine which may play important roles onthe immune response and the progression of gastric cancer[6–8]. Genetic variants of inflammation-related cytokinesare a potential risk factor because H. pylori infection caninduce chronic inflammation in gastric mucosa which is acritical step in gastric carcinogenesis. Therefore, geneticpolymorphisms in the TNF-α gene have been supposed ascandidate risk factors of gastric cancer [7]. Currently, thereare several common single-nucleotide polymorphisms iden-tified in the TNF-α gene which can regulate TNF-α expres-sion, TNF-α 308G/A and 238 G/A [7, 9]. There are a largenumber of studies on the association between TNF-α308G/A and gastric cancer; TNF-α 308G/A has been suc-cessfully identified as one risk factor of gastric cancer [10,11]. Though many studies were also performed to assess theassociation between TNF-α 238 G/A polymorphism andgastric cancer risk, there were no conclusive findings. Ameta-analysis of previous published studies was performed
Jian-yong Yu and Li Li contributed equally to the study.
J.<y. Yu :H. Ma :K. Liu :X. Cheng :Y.<l. Li :X.<l. Song (*)Department of Gastrointestinal Surgery, Shandong Cancer Hospital,Jinan 250117, Chinae-mail: [email protected]
L. LiDepartment of Trauma Surgery, Wendeng Osteopathic Hospital,Wendeng, Shandong Province, China
Tumor Biol. (2013) 34:3859–3863DOI 10.1007/s13277-013-0972-z

NOTE: Weights are from random effects analysis
Overall (I-squared = 59.8%, p = 0.002)
Crusius JB 2008
Wu MS 2004
Bai JP 2010
Zambon CF 2005
Jang WH 2001
Study
Zeng QD 2007
Hou L 2007
ID
Xing P 2006
Kamangar F 2006
Lee SG 2004
Yi D 2011
Wu MS 2003
Lu W 2005
Yang JJ 2009
Garcia-Gonzqlez 2007
1.32 (1.02, 1.72)
0.68 (0.41, 1.13)
1.03 (0.36, 2.96)
2.85 (1.29, 6.31)
1.27 (0.75, 2.14)
0.26 (0.06, 1.17)
2.13 (1.28, 3.57)
1.23 (0.70, 2.16)
OR (95% CI)
2.13 (1.28, 3.57)
2.26 (0.68, 7.50)
0.88 (0.51, 1.53)
2.39 (1.06, 5.37)
1.31 (0.51, 3.36)
1.54 (0.88, 2.71)
1.57 (0.74, 3.32)
0.80 (0.57, 1.12)
100.00
8.48
4.11
5.80
8.30
2.43
%
8.38
7.90
Weight
8.38
3.45
8.03
5.66
4.78
7.90
6.14
10.27
1.32 (1.02, 1.72)
0.68 (0.41, 1.13)
1.03 (0.36, 2.96)
2.85 (1.29, 6.31)
1.27 (0.75, 2.14)
0.26 (0.06, 1.17)
2.13 (1.28, 3.57)
1.23 (0.70, 2.16)
OR (95% CI)
2.13 (1.28, 3.57)
2.26 (0.68, 7.50)
0.88 (0.51, 1.53)
2.39 (1.06, 5.37)
1.31 (0.51, 3.36)
1.54 (0.88, 2.71)
1.57 (0.74, 3.32)
0.80 (0.57, 1.12)
100.00
8.48
4.11
5.80
8.30
2.43
%
8.38
7.90
Weight
8.38
3.45
8.03
5.66
4.78
7.90
6.14
10.27
1.057 1 17.5
NOTE: Weights are from random effects analysis
Overall (I-squared = 53.9%, p = 0.007)
Zeng QD 2007
Wu MS 2003
Jang WH 2001
Bai JP 2010
Xing P 2006
Zambon CF 2005
Lee SG 2004
Study
ID
Yi D 2011
Lu W 2005
Kamangar F 2006
Crusius JB 2008
Wu MS 2004
Hou L 2007
Yang JJ 2009
Garcia-Gonzqlez 2007
1.32 (1.01, 1.72)
2.44 (1.40, 4.26)
1.05 (0.26, 4.26)
0.29 (0.06, 1.37)
2.21 (0.94, 5.19)
2.44 (1.40, 4.26)
0.88 (0.47, 1.65)
0.88 (0.50, 1.54)
OR (95% CI)
2.45 (1.08, 5.57)
1.46 (0.82, 2.63)
2.30 (0.69, 7.71)
0.65 (0.38, 1.11)
1.03 (0.21, 5.16)
1.24 (0.70, 2.20)
1.61 (0.74, 3.48)
0.99 (0.68, 1.45)
100.00
8.67
2.90
2.46
5.76
8.67
7.92
8.62
%
Weight
6.02
8.36
3.62
8.83
2.30
8.51
6.44
10.91
1.32 (1.01, 1.72)
2.44 (1.40, 4.26)
1.05 (0.26, 4.26)
0.29 (0.06, 1.37)
2.21 (0.94, 5.19)
2.44 (1.40, 4.26)
0.88 (0.47, 1.65)
0.88 (0.50, 1.54)
OR (95% CI)
2.45 (1.08, 5.57)
1.46 (0.82, 2.63)
2.30 (0.69, 7.71)
0.65 (0.38, 1.11)
1.03 (0.21, 5.16)
1.24 (0.70, 2.20)
1.61 (0.74, 3.48)
0.99 (0.68, 1.45)
100.00
8.67
2.90
2.46
5.76
8.67
7.92
8.62
%
Weight
6.02
8.36
3.62
8.83
2.30
8.51
6.44
10.91
1.0619 1 16.2
NOTE: Weights are from random effects analysis
Overall (I-squared = 58.0%, p = 0.003)
ID
Zambon CF 2005
Yang JJ 2009
Yi D 2011
Garcia-Gonzqlez 2007
Crusius JB 2008
Study
Lu W 2005
Kamangar F 2006
Wu MS 2004
Wu MS 2003
Lee SG 2004
Hou L 2007
Bai JP 2010
Xing P 2006
Zeng QD 2007
Jang WH 2001
1.34 (1.02, 1.76)
OR (95% CI)
1.07 (0.60, 1.91)
1.61 (0.74, 3.48)
2.45 (1.08, 5.57)
0.89 (0.62, 1.28)
0.66 (0.39, 1.12)
1.52 (0.85, 2.71)
2.30 (0.69, 7.71)
1.03 (0.29, 3.61)
1.23 (0.41, 3.71)
0.88 (0.50, 1.54)
1.24 (0.70, 2.20)
2.60 (1.13, 5.98)
2.44 (1.40, 4.26)
2.44 (1.40, 4.26)
0.27 (0.06, 1.24)
100.00
Weight
8.12
6.29
5.90
10.40
8.61
%
8.09
3.63
3.44
4.11
8.28
8.17
5.81
8.32
8.32
2.52
1.34 (1.02, 1.76)
OR (95% CI)
1.07 (0.60, 1.91)
1.61 (0.74, 3.48)
2.45 (1.08, 5.57)
0.89 (0.62, 1.28)
0.66 (0.39, 1.12)
1.52 (0.85, 2.71)
2.30 (0.69, 7.71)
1.03 (0.29, 3.61)
1.23 (0.41, 3.71)
0.88 (0.50, 1.54)
1.24 (0.70, 2.20)
2.60 (1.13, 5.98)
2.44 (1.40, 4.26)
2.44 (1.40, 4.26)
0.27 (0.06, 1.24)
100.00
Weight
8.12
6.29
5.90
10.40
8.61
%
8.09
3.63
3.44
4.11
8.28
8.17
5.81
8.32
8.32
2.52
1.0573 1 17.5
a
b
c
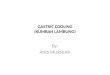
Fig. 1 Forest plot describing theassociation between TNF-α238G/A polymorphism andgastric cancer risk (each study isshown by the point estimate ofthe OR and 95 % CI and the sizeof the square is proportional tothe weight of each study)
3860 Tumor Biol. (2013) 34:3859–3863

to get a comprehensive assessment of the association be-tween TNF-α 238 G/A polymorphism and gastric cancer.
Methods
Literature search and inclusion criteria
A literature search was performed in the PubMed andWanfangdatabases to identify those studies assessing the associationbetween TNF-α 238 G/A polymorphism and gastric cancerrisk. There were no language restrictions and the last searchtime was 18 March 2013. We used the keywords and subjectterms: (“gastric carcinoma”, “gastric cancer”, or “stomach can-cer”) and (“tumor necrosis factor”, or “TNF”, or “TNF-α”, or“238 G/A”) and (“polymorphism” or “variant” or “genotype”or “mutation”). All eligible studies were retrieved and theirbibliographies were checked for other relevant publications.
The following inclusion criteria were used in the meta-analysis: (1) case–control studies comparing gastric cancercases with healthy or noncancer controls; (2) studies evalu-ating the association between TNF-α 238 G/A polymor-phism and gastric cancer risk; (3) sufficient genotype dataof TNF-α 238 G/A polymorphism were reported. Case-onlystudies, case reports, reviews, or studies without useable datawere all excluded.
Data extraction
The following data were extracted: first author, year of publi-cation, country, ethnicity, study design, diagnostic criteria,source of cases and controls, number of cases and controls,genotyping method, and frequencies of TNF-α 238 G/A geno-types in both cases and controls. Two investigators performedthe data extraction independently and the conflicting data weresettled by discussion among all investigators.
Statistical analysis
The strength of the associations between TNF-α 238 G/Apolymorphism and gastric cancer risk was estimated usingodds ratios (ORs) and their 95 % confidence interval (95 %CIs). The following contrasts for the associations betweenTNF-α 238 G/A polymorphism and gastric cancer risk wereevaluated: the allele model (Avs. G), the heterozygote model(GAvs. GG), and the dominant model (AA/GAvs. GG). TheI2 statistic to quantify the proportion of the total variation dueto heterogeneity were calculated and an I2 value of more than50 % was interpreted as significant heterogeneity amongstudies [12]. When the effects were assumed to be homoge-nous, the fixed-effects model was used (Mantel–Haenszelmethod) [13]. If obvious heterogeneity was present, therandom-effects model was used (DerSimonian–Laird meth-od) [14]. Subgroup analysis based on ethnicity was alsoperformed. Potential publication bias was assessed by visualinspection of the funnel plot, in which the standard error of
Table 1 Meta-analysis of theassociation between TNF-α238G/A polymorphism andgastric cancer risk
OR odds ratio, 95 % CI 95 %confidence interval
Groups Studies (subjects) OR (95 % CI) P value I2 value (%)
Total studies
A vs. G 15 (7,795) 1.32 (1.02–1.72) 0.036 59.8
GA vs. GG 15 (7,795) 1.32 (1.01–1.72) 0.042 53.9
AA/GA vs. GG 15 (7,795) 1.34 (1.02–1.76) 0.036 58.0
Caucasians
A vs. G 5 (3,970) 0.93 (0.74–1.15) 0.488 39.9
GA vs. GG 5 (3,970) 0.95 (0.75–1.21) 0.696 19.0
AA/GA vs. GG 5 (3,970) 0.94 (0.74–1.19) 0.593 21.3
Asians
A vs. G 10 (3,825) 1.59 (1.29–1.97) <0.001 45.1
GA vs. GG 10 (3,825) 1.63 (1.29–2.04) <0.001 42.9
AA/GA vs. GG 10 (3,825) 1.64 (1.31–2.05) <0.001 47.1
0.2
.4.6
.8
-2 -1 0 1 2logor
Funnel plot with pseudo 95% confidence limits
Fig. 2 Funnel plot for the detection of the publication bias in themeta-analysis
Tumor Biol. (2013) 34:3859–3863 3861

logOR of each study was plotted against its logOR, and anasymmetric plot suggested possible publication bias. All anal-yses were conducted using STATA (Version 11.0, StataCorp,College Station, TX, USA). All P values were two-sided inthe meta-analysis.
Results
Study characteristics
Fifteen studies with a total of 7,795 participants were finallyincluded into this meta-analysis [15–29]. Among those 15studies, 10 studies were from Asian populations [15–19, 22,25, 27–29] while five studies were from Caucasians [20, 21,23, 24, 26]. The sample size of cases ranged from 52 to 404,while the sample size of the controls ranged from 92 to 1123in the controls [15–29].
Meta-analysis
Overall, there was an obvious association between TNF-α238 G/A polymorphism and increased risk of gastric cancer(A vs. G: OR=1.32, 95 % CI 1.02–1.72, P=0.036; GA vs.GG: OR=1.32, 95 % CI 1.01–1.72, P=0.042; AA/GA vs.GG: OR=1.34, 95 % CI 1.02–1.76, P=0.036; Fig. 1,Table 1). Subgroup analysis by ethnicity showed the statis-tically significant association between TNF-α 238 G/A poly-morphism and gastric cancer was limited to Asian popula-tions (A vs. G: OR=1.59, 95 % CI 1.29–1.97, P<0.001; GAvs. GG: OR=1.63, 95 % CI 1.29–2.04, P<0.001; AA/GAvs.GG: OR=1.64, 95 % CI 1.31–2.05, P<0.001), and there wasno obvious association in Caucasians (Table 1).
Publication bias was investigated by Begg’s funnel plotand the funnel plots showed there was low possibility ofasymmetry (Fig. 2). Therefore, there was no obvious risk ofpublication bias in the meta-analysis.
Discussion
Gastric cancer is a multifactorial disease, and both environ-mental and genetic factors play important roles in the devel-opment of gastric cancer [2, 3]. H. pylori infection has beenidentified as the major risk factor of gastric cancer [2, 3]. H.pylori infection can cause chronic inflammation in the stom-ach, which may further result in the development of gastriccancer [4, 5]. Genetic variants of inflammation-related cyto-kines are a potential risk factor because H. pylori infectioncan induce chronic inflammation in gastric mucosa which isa critical step in gastric carcinogenesis.
TNF-α is an inflammatory cytokine which may playimportant roles on the immune response and the progression
of many cancers including gastric cancer [6–8]. Therefore,genetic polymorphisms in the TNF-α gene have been sup-posed as candidate risk factors of cancer [7]. Currently, thereare several common single nucleotide polymorphisms identi-fied in the TNF-α gene which can regulate the TNF-α expres-sion, and TNF-α 308G/A and 238 G/A [7, 9]. There are alarge number of studies on the association between TNF-α308G/A polymorphism and gastric cancer, and TNF-α308G/A has been successfully identified as one risk factor ofgastric cancer [10, 11]. In addition, TNF-α 308G/A polymor-phism has also been identified as risk factors of other cancers,such as cervical cancer and breast cancer [30, 31]. Thosepositive associations above suggest that TNF-α plays impor-tant roles in the carcinogenesis of common cancers.
Though many studies were also performed to assess theassociation between TNF-α 238 G/A polymorphism and gas-tric cancer risk, there were no conclusive findings. Therefore,we performed a meta-analysis of previous published studies toget a comprehensive assessment of the association betweenTNF-α 238 G/A polymorphism and gastric cancer. Finally, 15studies with a total of 7,795 participants were finally includedinto this meta-analysis. Overall, there was an obvious associ-ation between TNF-α 238 G/A polymorphism and increasedrisk of gastric cancer (Avs. G: OR=1.32, 95 % CI 1.02–1.72,P=0.036; GA vs. GG: OR=1.32, 95 % CI 1.01–1.72,P=0.042; AA/GA vs. GG: OR=1.34, 95 % CI 1.02–1.76,P=0.036; Table 1). Subgroup analysis by ethnicity showed thestatistically significant association between TNF-α 238 G/Apolymorphism and gastric cancer was limited to Asian popu-lations and there was no obvious association in Caucasians(Table 1). In conclusion, TNF-α 238 G/A polymorphism issignificantly associated with increased risk of gastric cancer,especially in Asians.
Conflicts of interest None
References
1. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Globalcancer statistics. CA Cancer J Clin. 2011;61:69–90.
2. Houghton J, Wang TC. Helicobacter pylori and gastric cancer: anew paradigm for inflammation-associated epithelial cancers.Gastroenterology. 2005;128:1567–78.
3. Polk DB, Peek Jr RM. Helicobacter pylori: gastric cancer andbeyond. Nat Rev Cancer. 2010;10:403–14.
4. Wroblewski LE, Peek Jr RM. Helicobacter pylori in gastric carcino-genesis: mechanisms. Gastroenterol Clin North Am. 2013;42:285–98.
5. Lamb A, Chen LF. Role of the Helicobacter pylori-induced inflam-matory response in the development of gastric cancer. J Cell Biochem.2013;114:491–7.
6. Vendramini-Costa DB, Carvalho JE. Molecular link mechanisms be-tween inflammation and cancer. Curr Pharm Des. 2012;18:3831–52.
7. Chu WM. Tumor necrosis factor. Cancer Lett. 2013;328:222–5.
3862 Tumor Biol. (2013) 34:3859–3863

8. Lippitz BE. Cytokine patterns in patients with cancer: a systematicreview. Lancet Oncol. 2013;14:e218–228.
9. Watts TH. TNF/TNFR family members in costimulation of T cellresponses. Annu Rev Immunol. 2005;23:23–68.
10. Gorouhi F, Islami F, Bahrami H, Kamangar F. Tumour-necrosisfactor-α polymorphisms and gastric cancer risk: a meta-analysis. BrJ Cancer. 2008;98:1443–51.
11. Persson C, Canedo P, Machado JC, El-Omar EM, Forman D.Polymorphisms in inflammatory response genes and their associationwith gastric cancer: a huge systematic review and meta-analyses. AmJ Epidemiol. 2011;173:259–70.
12. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuringinconsistency in meta-analyses. BMJ. 2003;327:557–60.
13. Mantel N, Haenszel W. Statistical aspects of the analysis of data fromretrospective studies of disease. J Natl Cancer Inst. 1959;22:719–48.
14. DerSimonian R, Laird N. Meta-analysis in clinical trials. ControlClin Trials. 1986;7:177–88.
15. Jang WH, Yang YI, Yea SS, Lee YJ, Chun JH, Kim HI, et al. The -238 tumor necrosis factor-alpha promoter polymorphism is associ-ated with decreased susceptibility to cancers. Cancer Lett.2001;166:41–6.
16. WuMS,Wu CY, Chen CJ, LinMT, Shun CT, Lin JT. Interleukin-10genotypes associate with the risk of gastric carcinoma in TaiwaneseChinese. Int J Cancer. 2003;104:617–23.
17. Lee SG, Kim B, Yook JH, Oh ST, Lee I, Song K. TNF/LTA poly-morphisms and risk for gastric cancer/duodenal ulcer in the Koreanpopulation. Cytokine. 2004;28:75–82.
18. Wu MS, Chen LT, Shun CT, Huang SP, Chiu HM, Wang HP, et al.Promoter polymorphisms of tumor necrosis factor-alpha are asso-ciated with risk of gastric mucosa-associated lymphoid tissue lym-phoma. Int J Cancer. 2004;110:695–700.
19. Lu W, Pan K, Zhang L, Lin D, Miao X, You W. Genetic poly-morphisms of interleukin (IL)-1B, IL-1RN, IL-8, IL-10 and tumornecrosis factor alpha and risk of gastric cancer in a Chinese popu-lation. Carcinogenesis. 2005;26:631–6.
20. Zambon CF, Basso D, Navaglia F, Belluco C, Falda A, Fogar P,et al. Pro- and anti-inflammatory cytokines gene polymorphismsand Helicobacter pylori infection: interactions influence outcome.Cytokine. 2005;29:141–52.
21. Kamangar F, Abnet CC, Hutchinson AA, Newschaffer CJ,Helzlsouer K, Shugart YY, et al. Polymorphisms in inflammation-related genes and risk of gastric cancer (Finland). Canc CausesContr. 2006;17:117–25.
22. Xing P, Xiao D, Zeng Q, Gao W. Relationship between cytokinegene polymorphisms on development and clinical characteristics ofgastric adenocarcinoma. Chin J Gen Surg. 2006;15:659–63.
23. Garcia-Gonzalez MA, Lanas A, Quintero E, Nicolas D, Parra-BlancoA, StrunkM, et al. Gastric cancer susceptibility is not linked to pro-andanti-inflammatory cytokine gene polymorphisms in whites: a nation-wide multicenter study in Spain. Am J Gastroenterol. 2007;102:1878–92.
24. Hou L, El-Omar EM, Chen J, Grillo P, Rabkin CS, Baccarelli A,et al. Polymorphisms in Th1-type cell-mediated response genes andrisk of gastric cancer. Carcinogenesis. 2007;28:118–23.
25. Zeng QD, Lu LH, Xing PX, Lu B, Wang YS. Relationship betweencytokine gene polymorphism and development of gastric adeno-carcinoma. Zhonghua Yi Xue Za Zhi. 2007;87:1037–9.
26. Crusius JB, Canzian F, Capella G, Pena AS, Pera G, Sala N, et al.Cytokine gene polymorphisms and the risk of adenocarcinoma ofthe stomach in the European Prospective Investigation into Cancerand Nutrition (EPIC-EURGAST). Ann Oncol. 2008;19:1894–902.
27. Yang JJ, Ko KP, Cho LY, Shin A, Gwack J, Chang SH, et al. Therole of TNF genetic variants and the interaction with cigarettesmoking for gastric cancer risk: a nested case–control study.BMC Cancer. 2009;9:238.
28. Bai JP, Guo Y, Chen R, Shen Y, Zhang P. Study on gastric cancersusceptibility genes in ethnic Hani and Yi populations withHelicobacter pylori infection in Yunnun Province. Chin Eur JGastroenterol Hepatol. 2010;14:669–73.
29. Yi D, Wang Q, Wang F, Meng T, Ge L. Relationship betweentagSNPs and haplotype of TNF-α gene and gastric cancer inUygur and Han ethnic groups in Xinjiang. Carcinog TeratogMutagen. 2012;24:261–5.
30. Shen C, Sun H, Sun D, Xu L, Zhang X, Liu A, et al. Polymorphismsof tumor necrosis factor-alpha and breast cancer risk: a meta-analysis.Breast Cancer Res Treat. 2011;126:763–70.
31. Zhang HL, Zhang YJ. A systemic assessment of the associationbetween tumor necrosis factor alpha 308 G/A polymorphism andrisk of cervical cancer. Tumour Biol. 2013;34:1659–65.
Tumor Biol. (2013) 34:3859–3863 3863





![java1-lecture6.ppt [호환 모드]dis.dankook.ac.kr/lectures/java20/wp-content/... · Polymorphism 다형성(Polymorphism) 다형성(polymorphism)이란객체들의타입이다르면똑같은](https://img.pdfslide.tips/doc/110x75/5fcfbaad9d9260016a636609/java1-eeoedisdankookackrlecturesjava20wp-content-polymorphism.jpg)