Embed Size (px)
Citation preview
U"lidaddelaColpasabilidaddelaVenaCavaInferioryelÍndicedelaVenayugularenlareanimación
Dra.OlgaGarcíaOropezaTerapiaIntensivaPediátrica

Técnicanoinvasiva
Segura
FácilejecuciónEstadodevolumenintravascular
Respuestaalaadministraciónde
líquidos
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112
VenaCavaInferiorARRIOJA A, ET AL
Avances Cardiol 121
región circundante es fundamental a la hora de la evaluación global de un individuo, por lo que el ��� ������������!�� ���#����!�� ������������������anatómicas se hacen cada vez más necesarios (1).
Anatomía de la vena cava inferior
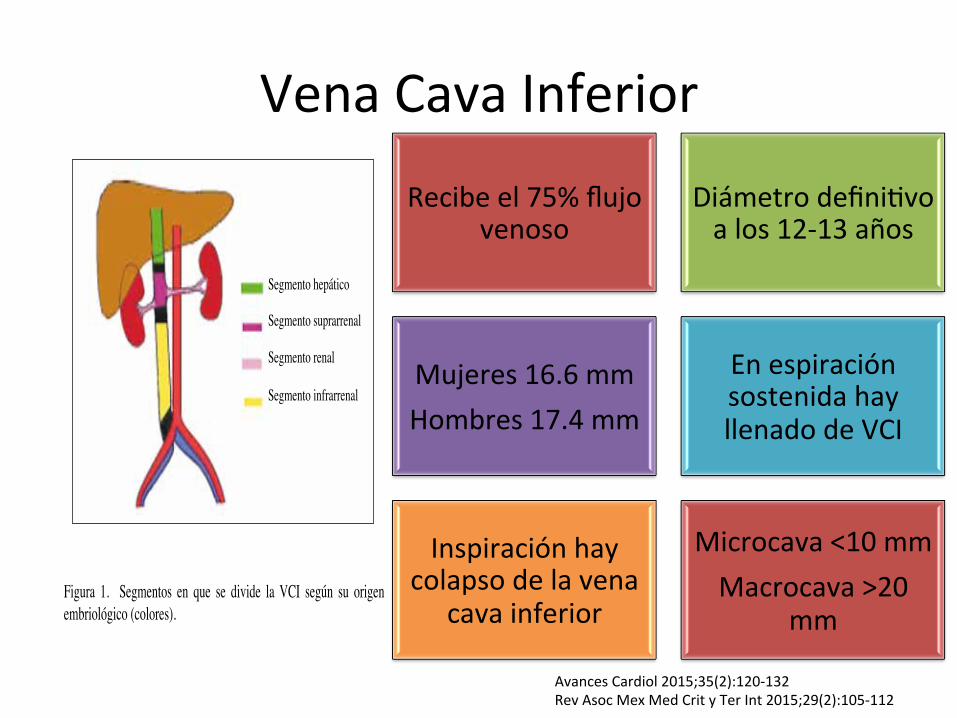
�� ���������������� ���������������� ��$��� ���de la vena ilíaca común derecha e izquierda que drenan la sangre de las extremidades inferiores y la pelvis. Asciende en el retroperitoneo a la derecha de la aorta abdominal, variando su forma desde redondeada hasta ovalada o similar a una hendidura dependiendo de la técnica de apnea y del equilibrio del líquido intravascular. Recibe tributarias mayores incluyendo las venas lumbares, vena renal derecha e izquierda, vena gonadal derecha y las venas hepáticas. El sistema venoso ácigos se conecta directamente a la VCI o a través de las venas renales (1). ���$���������������������������75.������$�����������������������������������������de los miembros inferiores, cavidad pélvica y ����������������������$��������������� �������������(VCS) representa el 24 % aproximadamente del retorno venoso correspondiente a cabeza, cuello, ��������� ����������� �� �!���� �� ��� $���� ���� ������������ �������������������������������$�����������cardíaco. De esta manera, de 80 cm3 de retorno venoso al corazón, 60 cm3 corresponden a la VCI y los otros 20 cm3 corresponden a la VCS y seno coronario (2). La VCI está formada por cuatro segmentos (Figura 1): hepático, suprarrenal, renal, e infrarrenal (1).
Anomalías de la cava inferior
La anomalía más frecuente de la VCI es la interrupción de su curso abdominal con drenaje cardíaco a través del sistema venoso de la ácigos o hemiácigos. De acuerdo con el nivel de desarrollo, las anomalías de la VCI pueden ser divididas en tres tipos (Tabla 1): del segmento infrarrenal, renal y suprarrenal. En un estudio prospectivo transversal y observacional de 12 000 estudios de tomografía computarizada multidetectores (TCMD), encontraron prevalencia de 0,15 % de
variantes anatómicas de las venas cavas, 68 % en el sexo femenino. La variante anatómica más común de la VCI resultó ser la duplicación de la VCI (33,3.%), seguida en orden de frecuencia por la duplicación de la VCI con continuación de la hemiácigos, VCI inferior izquierda, vena renal izquierda retroaórtica (que incluye VCI izquierda con vena renal retroaórtica), vena renal izquierda circumaórtica. Otras variedades incluyen la ausencia de VCI con preservación del segmento suprahepático, duplicación de la VCI con continuación de la ácigos, uréter retro o circumcava (1,3-5).
Métodos de exploración
La tomografía computarizada multidetectores (TCMD) combinada con técnicas de reconstrucción multiplanar y tridimensional han logrado que la angio-tomografía resulte un método atractivo que ofrece varias ventajas respecto a la angiografía convencional por cateterismo para evaluar anatomía vascular. Entre ellas resaltan el ser menos invasiva, menor costo, la posibilidad de obtenerse en período de tiempo breve y permitir mostrar alteraciones no vasculares no detectables en la angiografía
Figura 1. Segmentos en que se divide la VCI según su origen embriológico (colores).
Segmento hepático
Segmento suprarrenal
Segmento infrarrenal
Segmento renal
Recibeel75%flujovenoso
Diámetrodefini"voalos12-13años
Mujeres16.6mmHombres17.4mm
EnespiraciónsostenidahayllenadodeVCI
Inspiraciónhaycolapsodelavena
cavainferior
Microcava<10mmMacrocava>20
mm
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112
PRECARGA
Precarga Contrac"lidad
Distensibilidadeinterdependencia
ventricularPostcarga
Gastocardiaco
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112
RespuestaaLíquidos
350-500mlcristaloides
Ócoloide7ml/
kg
AumentaGastoCardiaco10-15%
Respondedoravolumen
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112
VCI
Indirecta
Noinvasiva
PADRelación
del80-90%
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112
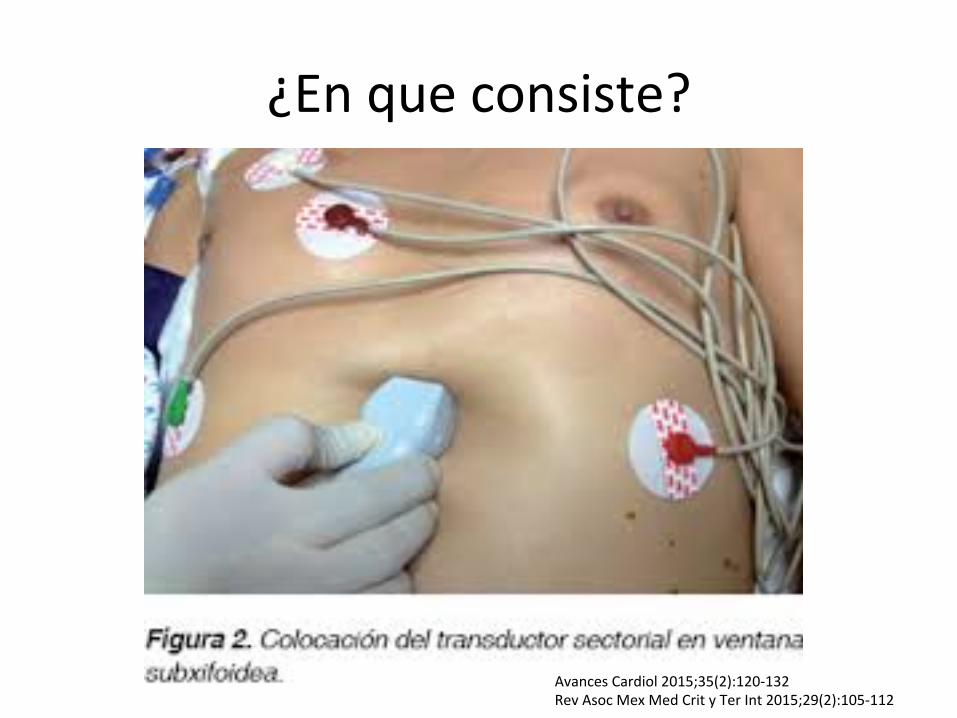
¿Enqueconsiste?
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112

A;00>##"%WX%=H%;#G%I'"9$'?$%C%'"*D6"*4$%$%(536#",%#"&)$,4"%634'$*5,5?'$7J$%&"%3$%(",$%9$($
JKP
!!!"#$%&'()*+&,"-('"#.
!"#$%&'()*$+#'%$"%$,-.'/-&'%0'/%1$&23/-042(
<=/=0`%0=;#>L;0I=%#;%+=<>:>O4%=4%+"<"%?%\+"4"1<>+=4I>"4;#]%;%,%:+%<>IH;#%<=%I3%34>O4%:"4%=#%;H0>"%<=0=:R"(%>4:#3I"%#;I%B3C;I%;+=0>:;4;I%<=%=:":;01<>"B0;DC;%0=:"+>=4<;4%I3%+=<>:>O4%8=08=4<>:3#;0%;#%=b=%#;0B"(%b3IH"%80"@>+;#%;%#;%34>O4%<=%#;%J=4;%R=8`H>:;(%a3=%=I%;80"@>+;<;+=4H=%<=%5$7%;%d%:+%<=%#;%;30C:3#;%<=0=:R;$%K=/=0`4%0=;#>L;0I=%+=<><;I%<=#%<>`+=H0"%+`@>+"%<=%34%:>:#"%0=I8>0;H"0>"%=4%>4I18>0;:>O4%^%=I8>0;:>O4%:K)?6'$%P>$66(6U
[;%=J;#3;:>O4%<=#%<>`+=H0"%+`@>+"%<=%#;%J=4;%:;J;%>4D=0>"0%^%I3%:"00=#;:>O4%:"4%#;%M!A%=4%8;:>=41H=I%/;b"%J=4H>#;:>O4%=I8"4H`4=;(%R;%I><"%0=8"0H;<;%8"0%43+=0"I"I%=IH3<>"I(%a3=<;4<"%0=I3+><"I%#"I%J;#"0=I%<=%M!A(%<>`+=H0"%^%I3%8"0:=4H;b=%<=%:"#;8I"%:"4%#;%0=I8>0;:>O4(%=4%=#%=Ia3=+;%=+>H><"%8"0%#;%.I"1:>;:>O4%.+=0>:;4;%<=%W:":;0<>"B0;DC;%:=6$&'5%;>$67
K30;4H=% #;% D;I=% >4I8>0;H"0>;%<=% #;%J=4H>#;:>O4%+=:`4>:;(%=#%>4:0=+=4H"%<=%#;%80=I>O4%8#=30;#%=I%H0;4I+>H><"%R;:>;%#;%;30C:3#;%<=0=:R;(%0=<3:>=4<"%=#%0=H"04"%J=4"I"%^%<>#;H;4<"%#;%!A'$%M"0%=#%:"4H0;0>"(%<30;4H=%#;%=I8>0;:>O4(%#;%0=<3::>O4%<=%#;%80=I>O4%>41H0;H"0`:>:;%D;J"0=:=%=#%0=H"04"%J=4"I"%^%<>I+>43^=%=#%<>`+=H0"%<=%#;%!A'$%WIH;I%J;0>;:>"4=I%=4%=#%<>`1+=H0"%<=%#;%!A'%I"4%+`I%=J><=4H=I%=4%8;:>=4H=I%R>8"J"#P+>:"I%^%8;0=:=4%=IH;0%<>I+>43><;I%=4%8;1:>=4H=I%R>8=0J"#P+>:"I%:3;4<"%#;%!A'%=I%+=4"I%<>I1H=4I>/#=$%WI%>+8"0H;4H=%0=:"0<;0%a3=%=4%8;:>=4H=I%/;b"%J=4H>#;:>O4%+=:`4>:;%8;0H>:3#;0+=4H=%;a3P##"I%:"4%80=I>"4=I%+=I=H;%<=%+`I%<=%,g%:+l,Y(%83=1<=4%<=I;00"##;0%95'%D63#5,$3"%;B3<"%^%<>"%:3#H;0%I3%=J;#3;:>O4%8;0;%<=H=0+>4;0%=4%a3P%8;0H=%<=%#;%:301J;%<=%N0;4i1QH;0#>4B%I=%=4:3=4H0;4%=%>4:#3I"%#"I%8;1:>=4H=I%:"4%D;##;%J=4H0>:3#;0%;B3<;%<=0=:R;%83=<=4%>+>H;0%;%34%8;:>=4H=%R>8"J"#P+>:"(%I>4%/=4="%:>;0I=%<=#%;8"0H=%<=%J"#3+=4%"%>4:#3I"%I3D0>0%<=H=0>"0"%:"4%=#%;8"0H=%<=%J"#3+=4(%;4H=%#"%:3;#%<=/=0`%3H>#>L;0I=%#;%+;^"0%:;4H><;<%<=%<;H"I%R=+"<>4`+>:"I%<>I8"14>/#=I%^%=+8#=;0%"H0"I%8;0`+=H0"I%<>4`+>:"I%;%"%4%
lCB;<"
!=4;%R=8`H>:;
!=4;%8"0H;
,%:+
!=4;%:;J;%>4D=0>"0
.30C:3#;%<=0=:R;
+,-.'/$;1$.34'$*5,)&5%",%#5&5%QR%",%&5,&"%*"%5@*"'($%3$%$,$45#J$%634'$*5,5?'M!%9$%&"%3$%(",$%9$($%),7"')5'%C%*6*%'"3$9)5,"*%$,$4+#)9$*G
?lL(%^%I=#=::>"4;4<"%=4%#;%+`a3>4;%<=%3#H0;I"14"B0;DC;%+"<"%/><>+=4I>"4;#%\,K](%^%=#%8=0D>#%<=%:;0<>"#"BC;(%I>%I=%:3=4H;%:"4%=#%+>I+"$%W#%8;:>=4H=%<=/=0`%=4:"4H0;0I=%><=;#+=4H=%=4%<=:*/>H"%<"0I;#%^%I=%#":;#>L;0`%#;%J=4H;4;%;:*IH>:;%I3/@>D"><=;%"%I3/:"IH;#(%:"#":;4<"%=#%H0;4I<3:H"0%>4+=<>;H;+=41H=%8"0%<=/;b"%^%#>B=0;+=4H=%R;:>;%#;%<=0=:R;%<=#%;8P4<>:=%@>D"><=I(%<>0>B>=4<"%=#%H0;4I<3:H"0%R;:>;%=#%R"+/0"%>La3>=0<"%<=#%8;:>=4H=%;80"@>+;<;+=4H=%;%67"(%:"4%#;%+;0:;%<=#%H0;4I<3:H"0%R;:>;%#;%>La3>=0<;%<=#%8;:>=4H=%=4%I=4H><"%R"0;0>"%;%#;I%<"I%"%H0=I(%^%:"4%34;%80"D34<><;<%<=%6f1,5%:+%"%+;^"0(%;%"%4%<=%#":;#>L;0%;#%:"0;LO4(%8;0;%8"IH=0>"0+=4H=%0=;#>L;0%34%B>0"%:"4H>43"%=4%I=4H><"%;4H>R"0;0>"%<=#%H0;4I<3:H"0%<=%#;I%d%;%#;I%6,%^%#>B=0"%<=I8#;L;+>=4H"%R;:>;%#;%>L1a3>=0<;%:K)?6'$*%Q%C%S>$%X=;#>L;4<"%#"I%+"J>+>=4H"I%<=#%H0;4I<3:H"0%<=I:0>H"I%I=%;80=:>;0`%#;%J=4;%:;J;%=4%I3%H0;^=:H"%8"0%=#%RCB;<"(%=4%I3%I>H>"%<=%34>O4%;#%;H0>"%<=0=:R"(%#;%B#`4<3#;%R=8`H>:;%^%#;%J=4;%R=18`H>:;%:K)?6'$%T>$%E4;%J=L%#":;#>L;<;%#;%J=4;%:;J;%
lCB;<"
!A'
m]
.%,$T6:+%%%%%m%,$5U%%
.] +,-.'/$<1$
;#$?",%634'$*5,5?'M7)9$%&"%3$%(",$%9$($%),7"')5'%",%&5,&"%*"%5@*"'($$8=%;#$?",%35,?)46&),$3%&"%(",$%9$($%),7"')5'%()*4$%*6@E95*4$3%",%#5&5%QRG%>=%/"&)9)+,%&"%3$%($')$9)+,%&"3%&)M#"4'5%&6E'$,4"%'"*D)'$9)+,%"*D5,4M,"$%",%#5&5%#5()#)",45B%:0>%A6"%'"D'"*",4$%"3%&)M#"4'5%#MO)#5%C%:U>%&)M#"4'5%#J,)#5G%V3%&)M#"E4'5%&"%3$%<=;%*"%5@4)","%95,%3$%*)E?6)",4"%7+'#63$W%:&<=;>%X%0EUYUG
\.]%%\m]%%
\m]%%\.]%%
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112

A;00>##"%WX%=H%;#G%I'"9$'?$%C%'"*D6"*4$%$%(536#",%#"&)$,4"%634'$*5,5?'$7J$%&"%3$%(",$%9$($
JKP
!!!"#$%&'()*+&,"-('"#.
!"#$%&'()*$+#'%$"%$,-.'/-&'%0'/%1$&23/-042(
<=/=0`%0=;#>L;0I=%#;%+=<>:>O4%=4%+"<"%?%\+"4"1<>+=4I>"4;#]%;%,%:+%<>IH;#%<=%I3%34>O4%:"4%=#%;H0>"%<=0=:R"(%>4:#3I"%#;I%B3C;I%;+=0>:;4;I%<=%=:":;01<>"B0;DC;%0=:"+>=4<;4%I3%+=<>:>O4%8=08=4<>:3#;0%;#%=b=%#;0B"(%b3IH"%80"@>+;#%;%#;%34>O4%<=%#;%J=4;%R=8`H>:;(%a3=%=I%;80"@>+;<;+=4H=%<=%5$7%;%d%:+%<=%#;%;30C:3#;%<=0=:R;$%K=/=0`4%0=;#>L;0I=%+=<><;I%<=#%<>`+=H0"%+`@>+"%<=%34%:>:#"%0=I8>0;H"0>"%=4%>4I18>0;:>O4%^%=I8>0;:>O4%:K)?6'$%P>$66(6U
[;%=J;#3;:>O4%<=#%<>`+=H0"%+`@>+"%<=%#;%J=4;%:;J;%>4D=0>"0%^%I3%:"00=#;:>O4%:"4%#;%M!A%=4%8;:>=41H=I%/;b"%J=4H>#;:>O4%=I8"4H`4=;(%R;%I><"%0=8"0H;<;%8"0%43+=0"I"I%=IH3<>"I(%a3=<;4<"%0=I3+><"I%#"I%J;#"0=I%<=%M!A(%<>`+=H0"%^%I3%8"0:=4H;b=%<=%:"#;8I"%:"4%#;%0=I8>0;:>O4(%=4%=#%=Ia3=+;%=+>H><"%8"0%#;%.I"1:>;:>O4%.+=0>:;4;%<=%W:":;0<>"B0;DC;%:=6$&'5%;>$67
K30;4H=% #;% D;I=% >4I8>0;H"0>;%<=% #;%J=4H>#;:>O4%+=:`4>:;(%=#%>4:0=+=4H"%<=%#;%80=I>O4%8#=30;#%=I%H0;4I+>H><"%R;:>;%#;%;30C:3#;%<=0=:R;(%0=<3:>=4<"%=#%0=H"04"%J=4"I"%^%<>#;H;4<"%#;%!A'$%M"0%=#%:"4H0;0>"(%<30;4H=%#;%=I8>0;:>O4(%#;%0=<3::>O4%<=%#;%80=I>O4%>41H0;H"0`:>:;%D;J"0=:=%=#%0=H"04"%J=4"I"%^%<>I+>43^=%=#%<>`+=H0"%<=%#;%!A'$%WIH;I%J;0>;:>"4=I%=4%=#%<>`1+=H0"%<=%#;%!A'%I"4%+`I%=J><=4H=I%=4%8;:>=4H=I%R>8"J"#P+>:"I%^%8;0=:=4%=IH;0%<>I+>43><;I%=4%8;1:>=4H=I%R>8=0J"#P+>:"I%:3;4<"%#;%!A'%=I%+=4"I%<>I1H=4I>/#=$%WI%>+8"0H;4H=%0=:"0<;0%a3=%=4%8;:>=4H=I%/;b"%J=4H>#;:>O4%+=:`4>:;%8;0H>:3#;0+=4H=%;a3P##"I%:"4%80=I>"4=I%+=I=H;%<=%+`I%<=%,g%:+l,Y(%83=1<=4%<=I;00"##;0%95'%D63#5,$3"%;B3<"%^%<>"%:3#H;0%I3%=J;#3;:>O4%8;0;%<=H=0+>4;0%=4%a3P%8;0H=%<=%#;%:301J;%<=%N0;4i1QH;0#>4B%I=%=4:3=4H0;4%=%>4:#3I"%#"I%8;1:>=4H=I%:"4%D;##;%J=4H0>:3#;0%;B3<;%<=0=:R;%83=<=4%>+>H;0%;%34%8;:>=4H=%R>8"J"#P+>:"(%I>4%/=4="%:>;0I=%<=#%;8"0H=%<=%J"#3+=4%"%>4:#3I"%I3D0>0%<=H=0>"0"%:"4%=#%;8"0H=%<=%J"#3+=4(%;4H=%#"%:3;#%<=/=0`%3H>#>L;0I=%#;%+;^"0%:;4H><;<%<=%<;H"I%R=+"<>4`+>:"I%<>I8"14>/#=I%^%=+8#=;0%"H0"I%8;0`+=H0"I%<>4`+>:"I%;%"%4%
lCB;<"
!=4;%R=8`H>:;
!=4;%8"0H;
,%:+
!=4;%:;J;%>4D=0>"0
.30C:3#;%<=0=:R;
+,-.'/$;1$.34'$*5,)&5%",%#5&5%QR%",%&5,&"%*"%5@*"'($%3$%$,$45#J$%634'$*5,5?'M!%9$%&"%3$%(",$%9$($%),7"')5'%C%*6*%'"3$9)5,"*%$,$4+#)9$*G
?lL(%^%I=#=::>"4;4<"%=4%#;%+`a3>4;%<=%3#H0;I"14"B0;DC;%+"<"%/><>+=4I>"4;#%\,K](%^%=#%8=0D>#%<=%:;0<>"#"BC;(%I>%I=%:3=4H;%:"4%=#%+>I+"$%W#%8;:>=4H=%<=/=0`%=4:"4H0;0I=%><=;#+=4H=%=4%<=:*/>H"%<"0I;#%^%I=%#":;#>L;0`%#;%J=4H;4;%;:*IH>:;%I3/@>D"><=;%"%I3/:"IH;#(%:"#":;4<"%=#%H0;4I<3:H"0%>4+=<>;H;+=41H=%8"0%<=/;b"%^%#>B=0;+=4H=%R;:>;%#;%<=0=:R;%<=#%;8P4<>:=%@>D"><=I(%<>0>B>=4<"%=#%H0;4I<3:H"0%R;:>;%=#%R"+/0"%>La3>=0<"%<=#%8;:>=4H=%;80"@>+;<;+=4H=%;%67"(%:"4%#;%+;0:;%<=#%H0;4I<3:H"0%R;:>;%#;%>La3>=0<;%<=#%8;:>=4H=%=4%I=4H><"%R"0;0>"%;%#;I%<"I%"%H0=I(%^%:"4%34;%80"D34<><;<%<=%6f1,5%:+%"%+;^"0(%;%"%4%<=%#":;#>L;0%;#%:"0;LO4(%8;0;%8"IH=0>"0+=4H=%0=;#>L;0%34%B>0"%:"4H>43"%=4%I=4H><"%;4H>R"0;0>"%<=#%H0;4I<3:H"0%<=%#;I%d%;%#;I%6,%^%#>B=0"%<=I8#;L;+>=4H"%R;:>;%#;%>L1a3>=0<;%:K)?6'$*%Q%C%S>$%X=;#>L;4<"%#"I%+"J>+>=4H"I%<=#%H0;4I<3:H"0%<=I:0>H"I%I=%;80=:>;0`%#;%J=4;%:;J;%=4%I3%H0;^=:H"%8"0%=#%RCB;<"(%=4%I3%I>H>"%<=%34>O4%;#%;H0>"%<=0=:R"(%#;%B#`4<3#;%R=8`H>:;%^%#;%J=4;%R=18`H>:;%:K)?6'$%T>$%E4;%J=L%#":;#>L;<;%#;%J=4;%:;J;%
lCB;<"
!A'
m]
.%,$T6:+%%%%%m%,$5U%%
.] +,-.'/$<1$
;#$?",%634'$*5,5?'M7)9$%&"%3$%(",$%9$($%),7"')5'%",%&5,&"%*"%5@*"'($$8=%;#$?",%35,?)46&),$3%&"%(",$%9$($%),7"')5'%()*4$%*6@E95*4$3%",%#5&5%QRG%>=%/"&)9)+,%&"%3$%($')$9)+,%&"3%&)M#"4'5%&6E'$,4"%'"*D)'$9)+,%"*D5,4M,"$%",%#5&5%#5()#)",45B%:0>%A6"%'"D'"*",4$%"3%&)M#"4'5%#MO)#5%C%:U>%&)M#"4'5%#J,)#5G%V3%&)M#"E4'5%&"%3$%<=;%*"%5@4)","%95,%3$%*)E?6)",4"%7+'#63$W%:&<=;>%X%0EUYUG
\.]%%\m]%%
\m]%%\.]%%
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112
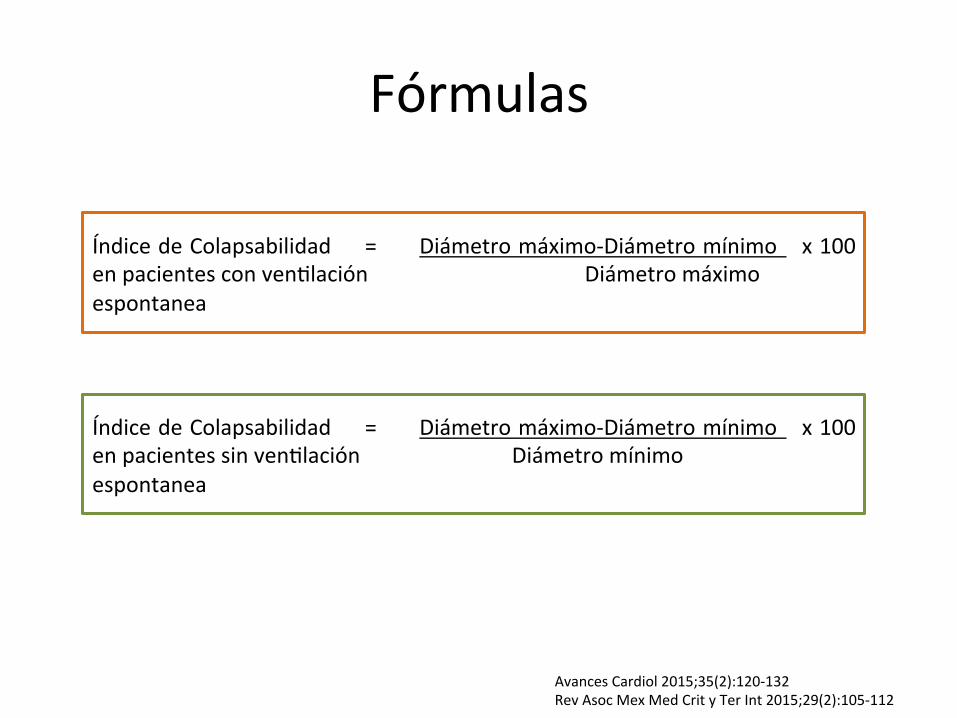
Fórmulas
ÍndicedeColapsabilidad = Diámetromáximo-Diámetromínimo x100enpacientesconven"laciónDiámetromáximoespontanea
ÍndicedeColapsabilidad = Diámetromáximo-Diámetromínimo x100enpacientessinven"laciónDiámetromínimoespontanea
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112
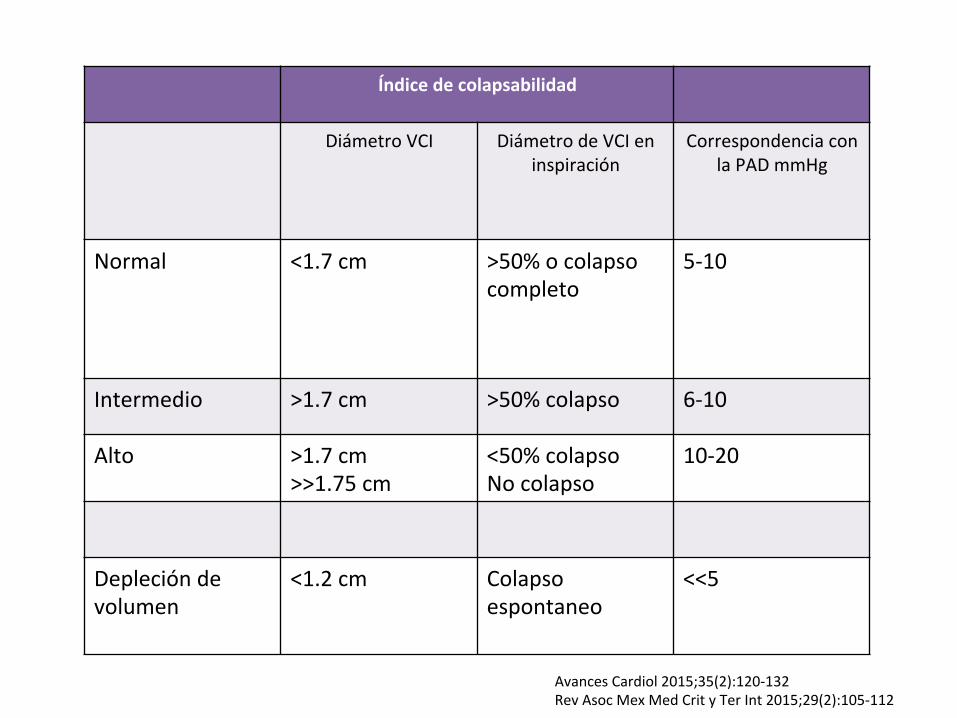
Índicedecolapsabilidad
DiámetroVCI DiámetrodeVCIeninspiración
CorrespondenciaconlaPADmmHg
Normal <1.7cm >50%ocolapsocompleto
5-10
Intermedio >1.7cm >50%colapso 6-10
Alto >1.7cm>>1.75cm
<50%colapsoNocolapso
10-20
Deplecióndevolumen
<1.2cm
Colapsoespontaneo
<<5
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112
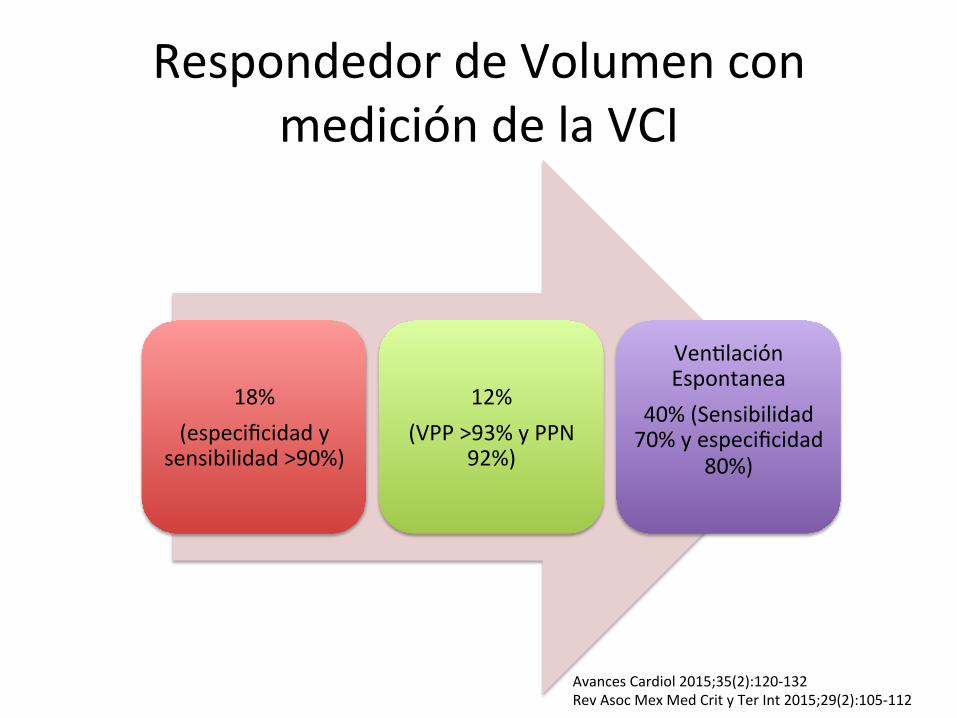
RespondedordeVolumenconmedicióndelaVCI
18%(especificidady
sensibilidad>90%)
12%(VPP>93%yPPN
92%)
Ven"laciónEspontanea
40%(Sensibilidad70%yespecificidad
80%)
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112

d Review
ULTRASONOGRAPHIC MEASUREMENT OF THE RESPIRATORY VARIATION INTHE INFERIOR VENA CAVA DIAMETER IS PREDICTIVE OF FLUID
RESPONSIVENESS IN CRITICALLY ILL PATIENTS: SYSTEMATIC REVIEWANDMETA-ANALYSIS
ZHONGHENG ZHANG,* XIAO XU,* SHENG YE,y and LEI XUz
*Department of Critical Care Medicine, Jinhua Municipal Central Hospital, Jinhua Hospital of Zhejiang University, Zhejiang,People’s Republic of China; yDepartment of Pediatric ICU, Children’s Hospital of Zhejiang University School of Medicine,Hangzhou, People’s Republic of China; and zDepartment of Ultrasonography, Jinhua Municipal Central Hospital, Jinhua
Hospital of Zhejiang University, Zhejiang, People’s Republic of China
(Received 14 July 2013; revised 4 December 2013; in final form 6 December 2013)
Abstract—Respiratory variation in the inferior vena cava (DIVC) has been extensively studied with respect to itsvalue in predicting fluid responsiveness, but the results are conflicting. This systematic review was aimed at inves-tigating the diagnostic accuracy ofDIVC in predicting fluid responsiveness. Databases includingMedline, Embase,Scopus and Web of Knowledge were searched from inception to May 2013. Studies exploring the diagnostic per-formance of DIVC in predicting fluid responsiveness were included. To allow for more between- and within-studyvariance, a hierarchical summary receiver operating characteristic model was used to pool the results. Subgroupanalyses were performed for patients on mechanical ventilation, spontaneously breathing patients and those chal-lenged with colloids and crystalloids. A total of 8 studies involving 235 patients were eligible for analysis. Cutoffvalues ofDIVC varied across studies, ranging from 12% to 40%. The pooled sensitivity and specificity in the over-all population were 0.76 (95% confidence interval [CI]: 0.61–0.86) and 0.86 (95% CI: 0.69–0.95), respectively. Thepooled diagnostic odds ratio (DOR)was 20.2 (95%CI: 6.1–67.1). The diagnostic performance ofDIVC appeared tobe better in patients on mechanical ventilation than in spontaneously breathing patients (DOR: 30.8 vs. 13.2). Thepooled area under the receiver operating characteristic curve was 0.84 (95% CI: 0.79–0.89). Our study indicatesthat DIVC measured with point-of-care ultrasonography is of great value in predicting fluid responsiveness,particularly in patients on controlled mechanical ventilation and those resuscitated with colloids. (E-mail:[email protected]) ! 2014 World Federation for Ultrasound in Medicine & Biology.
Key Words: Fluid responsiveness, Ultrasonography, Variation in inferior vena cava, Critical illness, Mechanicalventilation, Meta-analysis.
INTRODUCTION
Fluid management is crucial in the treatment of criticallyill patients, particularly for those with acute circulatoryfailure. Accumulating evidence suggests that either hypo-volemia or fluid overload can lead to poor clinical out-comes, including prolonged mechanical ventilation,higher mortality, renal dysfunction and impairment inoxygenation (Alsous et al. 2000; Boyd et al. 2011;Correa et al. 2012; Murphy et al. 2009). Therefore,
many investigators have explored reliable techniquesor biomarkers in the goal of predicting fluidresponsiveness in critically ill patients. The goal of fluidresuscitation is to maintain sufficient tissue perfusionwhile avoiding significant interstitial edema. TheFrank-Starling principle states that the greater the volumeof blood entering the heart during diastole, the greater isthe volume of blood ejected during systole (Saks et al.2006). This phenomenon, termed fluid responsiveness,is one of the most reliable parameters in the decision onwhether additional fluid can be given. Many parameters,for example, central venous pressure, pulse pressure vari-ation and stroke volume variation, have been evaluatedwith respect to their utility in fluid management, usingfluid responsiveness as the reference standard (Saugelet al. 2013; Suehiro et al. 2012; Yang et al. 2013).
Address correspondence to: Zhongheng Zhang, 351#, MingyueRoad, Jinhua, Zhejiang Province, China 321000. E-mail:[email protected]
Conflicts of Interest: The authors have indicated that they have noconflicts of interest regarding the content of this article.
845
Ultrasound in Med. & Biol., Vol. 40, No. 5, pp. 845–853, 2014Copyright ! 2014 World Federation for Ultrasound in Medicine & Biology
Printed in the USA.0301-5629
http://dx.doi.org/10.1016/j.ultrasmedbio.2013.12.010
Open access under CC BY-NC-ND license.
Open access under CC BY-NC-ND license.
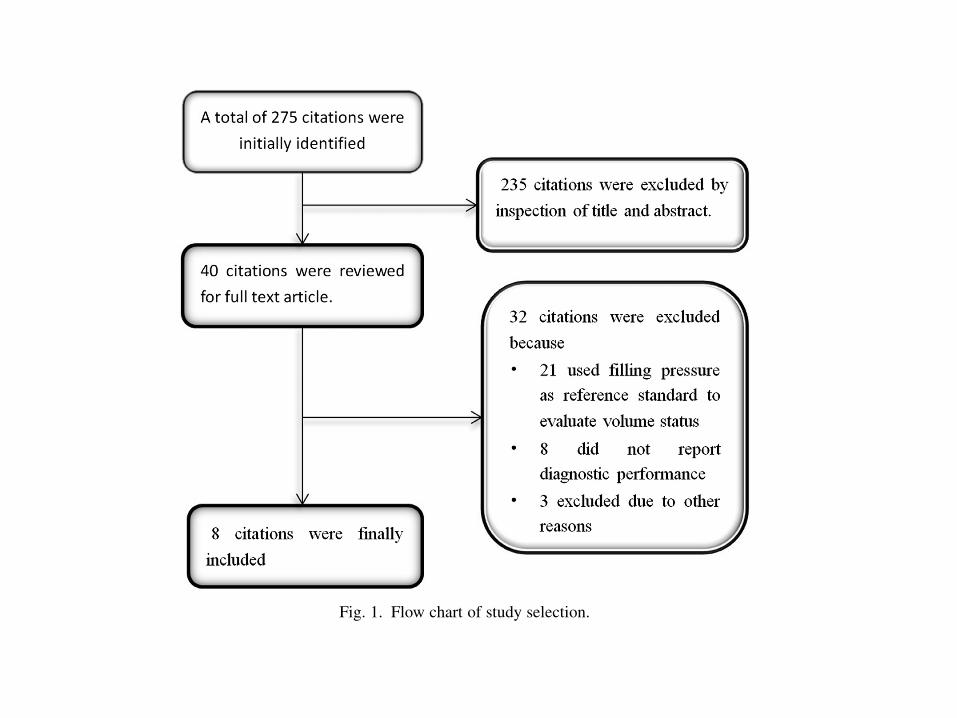
abstract because they were reviews, animal studies andother irrelevant articles. The full texts of the remaining40 studies were reviewed to identify potentially relevantstudies. Another 32 studies were excluded: 21 for usingfilling pressures as the reference standard to evaluate vol-ume status, 8 for not reporting diagnostic performanceand 3 for other reasons (Fig. 1). Finally, a total of 8 studies(Barbier et al. 2004; Brun et al. 2013; Byon et al. 2013;Corl et al. 2012; Feissel et al. 2004; Machare-Delgadoet al. 2011; Moretti and Pizzi 2010; Muller et al. 2012)were included in our analysis. Agreement between theresults obtained by independent reviewers was good,with a k of 0.91.
Characteristics of the included studies are listed inTable 1. All studies included critically ill patients; onestudy (Byon et al. 2013) focused on pediatric patients.Sample sizes were generally small, ranging from 20to 40 patients. The total number of patients included was235. Five studies (Barbier et al. 2004; Byon et al. 2013,Feissel et al. 2004; Machare-Delgado et al. 2011;Moretti and Pizzi 2010) enrolled patients on mechanicalventilation, and two (Corl et al. 2012; Muller et al.2012) enrolled spontaneously breathing patients; theremaining one (Brun et al. 2013) did not report the respi-ratory pattern. With respect to the site of IVC measure-ment, six studies (Brun et al. 2013; Byon et al. 2013;Corl et al. 2012; Feissel et al. 2004; Machare-Delgadoet al. 2011; Muller and Pizzi 2012) used the right atrium
as the reference, and the remaining two (Barbier et al.2004; Moretti and Pizzi 2010) used the suprahepaticvein as the reference. Variations in IVC during therespiratory cycle were calculated as the differencebetween maximum IVC diameter (Dmax) and minimumIVC diameter (Dmin), normalized by Dmin in threestudies (Barbier et al. 2004; Machare-Delgado et al.2011; Moretti and Pizzi 2010), by Dmax in two studies(Corl et al. 2012; Muller et al. 2012) and by(Dmax 1 Dmin)/2 in three studies (Brun et al. 2013; Byonet al. 2013; Feissel et al. 2004). Fluid responsivenesswas defined as an increase in cardiac index in threestudies (Barbier et al. 2004; Corl et al. 2012; Morettiand Pizzi 2010), stroke volume index in three studies(Brun et al. 2013; Byon et al. 2013; Machare-Delgadoet al. 2011), cardiac output and velocity-time index inthe remaining two studies (Feissel et al. 2004; Mulleret al. 2012). Six studies (Barbier et al. 2004; Brun et al.2013; Byon et al. 2013; Corl et al. 2012; Feissel et al.2004; Muller et al. 2012) used ultrasound to assess fluidresponsiveness, one study (Moretti and Pizzi 2010) usedthe transpulmonary thermodilution technique to measurecardiac index and another study (Machare-Delgado et al.2011) used theVigileomonitor (Edwards LifeSciences, Ir-vine, CA, USA) to record stroke volume index. Fluid chal-lenge was performed using plasma in one study (Barbieret al. 2004), normal saline in two studies (Brun et al.2013; Machare-Delgado et al. 2011), hydroxyethyl
Fig. 1. Flow chart of study selection.
Respiratory variation in IVC and fluid responsiveness d Z. ZHANG et al. 847
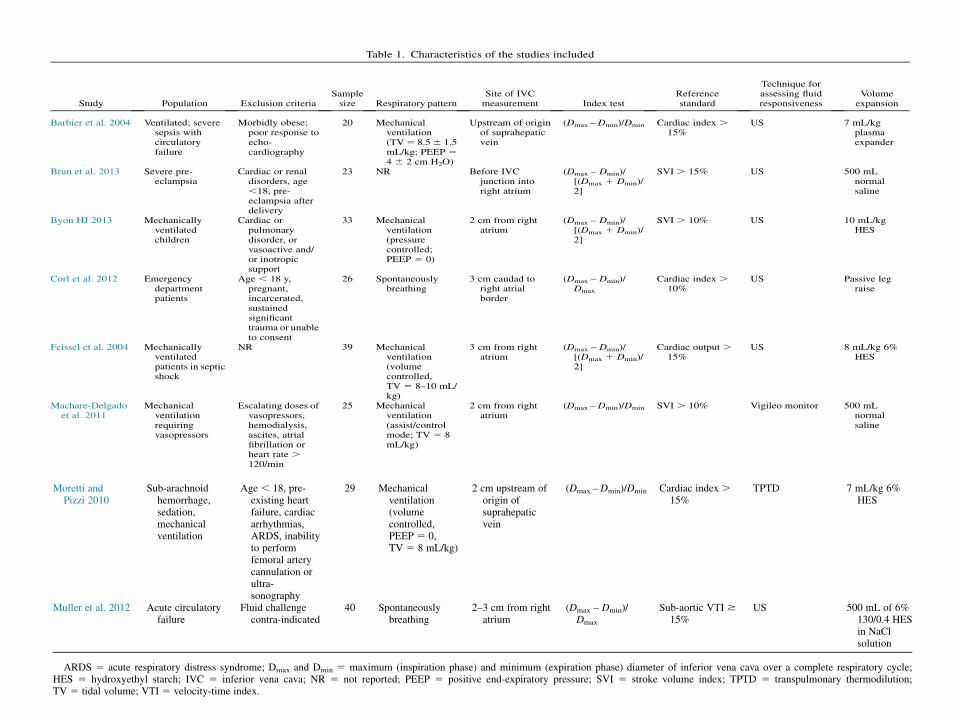
Table 1. Characteristics of the studies included
Study Population Exclusion criteriaSamplesize Respiratory pattern
Site of IVCmeasurement Index test
Referencestandard
Technique forassessing fluidresponsiveness
Volumeexpansion
Barbier et al. 2004 Ventilated; severesepsis withcirculatoryfailure
Morbidly obese;poor response toecho-cardiography
20 Mechanicalventilation(TV5 8.56 1.5mL/kg; PEEP 54 6 2 cm H2O)
Upstream of originof suprahepaticvein
(Dmax –Dmin)/Dmin Cardiac index .15%
US 7 mL/kgplasmaexpander
Brun et al. 2013 Severe pre-eclampsia
Cardiac or renaldisorders, age,18, pre-eclampsia afterdelivery
23 NR Before IVCjunction intoright atrium
(Dmax – Dmin)/[(Dmax 1 Dmin)/2]
SVI . 15% US 500 mLnormalsaline
Byon HJ 2013 Mechanicallyventilatedchildren
Cardiac orpulmonarydisorder, orvasoactive and/or inotropicsupport
33 Mechanicalventilation(pressurecontrolled;PEEP 5 0)
2 cm from rightatrium
(Dmax – Dmin)/[(Dmax 1 Dmin)/2]
SVI . 10% US 10 mL/kgHES
Corl et al. 2012 Emergencydepartmentpatients
Age , 18 y,pregnant,incarcerated,sustainedsignificanttrauma or unableto consent
26 Spontaneouslybreathing
3 cm caudad toright atrialborder
(Dmax – Dmin)/Dmax
Cardiac index .10%
US Passive legraise
Feissel et al. 2004 Mechanicallyventilatedpatients in septicshock
NR 39 Mechanicalventilation(volumecontrolled,TV 5 8–10 mL/kg)
3 cm from rightatrium
(Dmax – Dmin)/[(Dmax 1 Dmin)/2]
Cardiac output .15%
US 8 mL/kg 6%HES
Machare-Delgadoet al. 2011
Mechanicalventilationrequiringvasopressors
Escalating doses ofvasopressors,hemodialysis,ascites, atrialfibrillation orheart rate .120/min
25 Mechanicalventilation(assist/controlmode; TV 5 8mL/kg)
2 cm from rightatrium
(Dmax –Dmin)/Dmin SVI . 10% Vigileo monitor 500 mLnormalsaline
848Ultrasound
inMedicine
andBiology
Volume40,N
umber5,2014
starchinfourstudies
(Byon
etal.2013;Feisseletal.2004;
Morettiand
Pizzi2010;M
ulleretal.2012)and
passiveleg
raisein
onestudy
(Corl
etal.
2012).Table
2sum
marizes
thedifferent
echocardiographicparam
etersused
inthe
differentstudies.
Quality
assessment
accordingto
QUA-
DAScriteria
isoutlined
inTable
3.Spectrum
biaswas
pre-sent
inthree
studies(Corl
etal.2012;
Feissel
etal.2004;
Muller
etal.
2012).Allexcept
onestudy
(Feissel
etal.
2004)explicitly
describedselection
criteria.Allstudies
correctlydefi
nedthe
measurem
entoffluid
responsiveness.Nostudy
hadpartial
ordifferential
verification
bias.All
studieshad
adetailed
descriptionof
theindex
testand
referencestandard.
Three
studies(Corl
etal.
2012;Feissel
etal.
2004;Muller
etal.
2012)reported
poor-quality
ultrasoundim
ages,and
theseun-interpretable
re-sults
were
excludedfrom
analysis.The
diagnosticperform
anceof
DIV
Cin
eachstudy
isprovided
inTable
4.Six
studies(B
arbieret
al.2004;
Brun
etal.
2013;Feissel
etal.
2004;Machare-D
elgadoet
al.2011;
Moretti
andPizzi
2010;Muller
etal.
2012)reported
complete
datafor
meta-analysis.
Cutoff
valuesfor
DIV
Cvaried
acrossstudies,
rangingfrom
12%to
40%.T
hepooled
sensitivityand
specificity
forthe
overallpopulation
were
0.76(95%
confidence
interval[CI]:
0.61–0.86)and
0.86(95%
CI:0.69–0.95),
respectively.The
diagnosticodds
ratio(D
OR)was
20.2(95%
CI:
6.1–67.1)(Fig.
2).Diagnostically,
DIV
Cperform
edbet-
terinpatients
onmechanicalventilation
thaninspontane-
ouslybreathing
patients(D
OR:30.8
vs.13.2).
With
respectto
thetype
offluid
usedfor
fluid
challenge,DIV
Cappeared
toperform
betterin
patientswho
receivedcolloids
thanin
thosewho
receivednorm
alsaline
(DOR:32.1
vs.4.9)
(Table
5).AUROCswere
re-ported
inseven
studies(Barbier
etal.
2004;Brun
etal.
Moretti andPizzi 2010
Sub-arachnoidhemorrhage,sedation,mechanicalventilation
Age , 18, pre-existing heartfailure, cardiacarrhythmias,ARDS, inabilityto performfemoral arterycannulation orultra-sonography
29 Mechanicalventilation(volumecontrolled,PEEP 5 0,TV 5 8 mL/kg)
2 cm upstream oforigin ofsuprahepaticvein
(Dmax –Dmin)/Dmin Cardiac index .15%
TPTD 7 mL/kg 6%HES
Muller et al. 2012 Acute circulatoryfailure
Fluid challengecontra-indicated
40 Spontaneouslybreathing
2–3 cm from rightatrium
(Dmax – Dmin)/Dmax
Sub-aortic VTI $15%
US 500 mL of 6%130/0.4 HESin NaClsolution
ARDS 5 acute respiratory distress syndrome; Dmax and Dmin 5 maximum (inspiration phase) and minimum (expiration phase) diameter of inferior vena cava over a complete respiratory cycle;HES 5 hydroxyethyl starch; IVC 5 inferior vena cava; NR 5 not reported; PEEP 5 positive end-expiratory pressure; SVI 5 stroke volume index; TPTD 5 transpulmonary thermodilution;TV 5 tidal volume; VTI 5 velocity-time index.
Table
2.Echocardiographic
parameters
usedin
thedifferent
studies
Study
Equipm
entProbe
Frequency(M
Hz)
Barbier
etal.
2004HDI3500
CVsystem
,Philips/
ATL,Atlanta,G
A,USA
Phasedarray
1.67–3.2
Brun
etal.
2013HD11
XE,P
hilips/ATL
——
Byon
etal.2013
Vivid
7Pro,
GEVingm
edUltrasound,H
orten,Norw
ay
——
Corl
etal.2012
M-Turbo,S
onosite,Bothell,
WA,USA
Phasedarray
—
Feissel
etal.
2004—
——
Machare-D
elgadoet
al.2011
M-Turbo,S
onoSite
—5
Moretti
andPizzi
2010Esaote
MyL
ab30
CV,
Biosound
Esaote,
Genoa,
Italy
—3.5
Muller
etal.2012
Vivid
S6machine,G
eneralElectric,C
leveland,OH,
USA
——
Respiratory
variationin
IVCand
fluid
responsivenessd
Z.Z
HANGet
al.849
2013; Byon et al. 2013; Corl et al. 2012; Machare-Delgado et al. 2011; Moretti and Pizzi 2010; Mulleret al. 2012). In four studies (Barbier et al. 2004;Machare-Delgado et al. 2011; Moretti and Pizzi 2010;Muller et al. 2012), the AUROC was significantlygreater than 0.5, and in the remaining three (Brun et al.2013; Byon et al. 2013; Corl et al. 2012), DIVC had nodiagnostic value. Overall, the pooled AUROC was 0.84(95% CI: 0.79–0.89) (Fig. 3).
DISCUSSION
Our study indicates that DIVC is of great value indistinguishing patients who are fluid responsive fromthose who are not. In particular, its ability to distinguishappears to be better in patients on mechanical ventilation(vs. spontaneously breathing patients) and in thosereceiving colloid fluid loading (vs. normal saline). These
findings are clinically relevant because point-of-care ul-trasonography is becoming increasingly popular, andDIVC values can be obtained immediately in the emer-gency or critical care setting. Our study confirms thatfluid resuscitation based on DIVC is feasible and reliable.
To the best of our knowledge, two systematic re-views (Dipti et al. 2012; Mandeville and Colebourn2012) have investigated the diagnostic performance ofultrasonography in predicting fluid responsiveness. Thestudy by Mandeville and Colebourn (2012) includedtwo of our eight studies. That study is different fromours in that the techniques employed to predict fluidresponsiveness differed across component studies, lead-ing the authors to conclude that meta-analysis was im-possible because of such significant heterogeneity. Inour study, we selected only studies using DIVC to predictfluid responsiveness, which significantly reduced hetero-geneity. The analysis by Dipti et al. (2012) compared
Table 3. Quality assessment of the studies included
Barbier et al.2004
Brun et al.2013
Byon et al.2013
Corl et al.2012
Feissel et al.2004
Machare-Delgadoet al. 2011
Moretti andPizzi 2010
Muller et al.2012
Spectrum bias Yes Yes Yes No No Yes Yes NoSelection criteria clearlydescribed
Yes Yes Yes Yes No Yes Yes Yes
Correct reference standard Yes Yes Yes Yes Yes Yes Yes YesDisease progression bias No No No No No No No NoPartial verification bias* No No No No No No No NoDifferential verificationbiasy
No No No No No No No No
Detailed description ofindex test
Yes Yes Yes Yes Yes Yes Yes Yes
Detailed description ofreference standard
Yes Yes Yes Yes Yes Yes Yes Yes
Un-interpretable/intermediate test resultsreportedz
Yes Yes Yes No No Yes Yes No
Participants withdrawnexplained
Yes Yes Yes Yes No Yes Yes No
* Some study participants did not receive confirmation of the diagnosis by the reference standard.y Not all index test results were verified by the same reference standard.z Low-quality ultrasound images; exclusion of these cases may potentially distort the final results.
Table 4. Sensitivity and specificity of DIVC in predicting fluid responsiveness
Study
Number of patientsCutoff value
(increase in percentage) Sensitivity (%) Specificity (%) AUROC (95% CI)TP FP FN TN
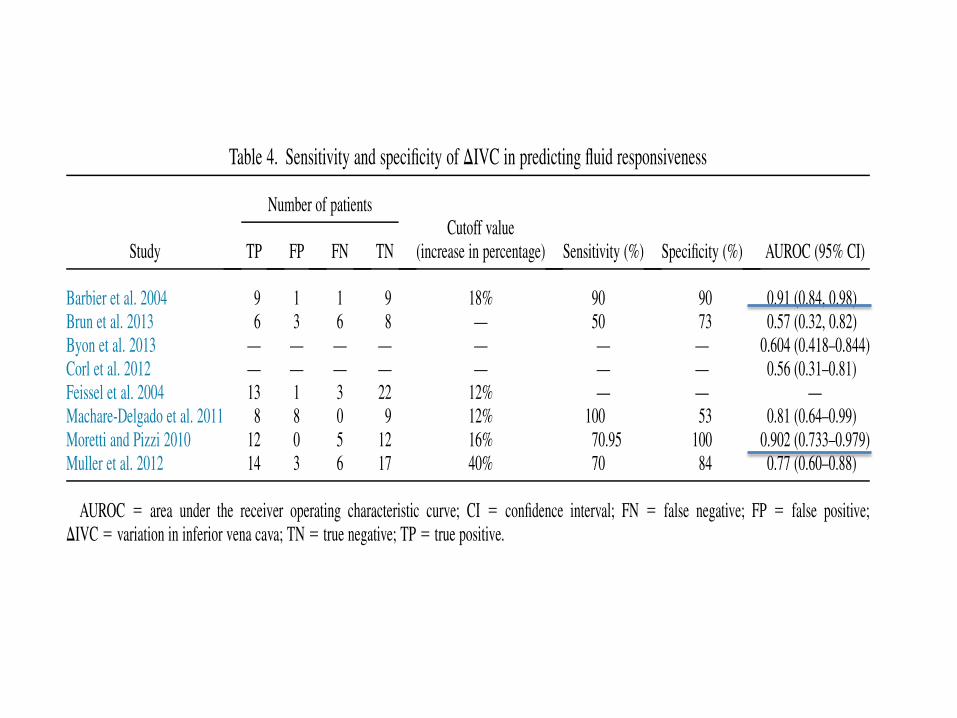
Barbier et al. 2004 9 1 1 9 18% 90 90 0.91 (0.84, 0.98)Brun et al. 2013 6 3 6 8 — 50 73 0.57 (0.32, 0.82)Byon et al. 2013 — — — — — — — 0.604 (0.418–0.844)Corl et al. 2012 — — — — — — — 0.56 (0.31–0.81)Feissel et al. 2004 13 1 3 22 12% — — —Machare-Delgado et al. 2011 8 8 0 9 12% 100 53 0.81 (0.64–0.99)Moretti and Pizzi 2010 12 0 5 12 16% 70.95 100 0.902 (0.733–0.979)Muller et al. 2012 14 3 6 17 40% 70 84 0.77 (0.60–0.88)
AUROC 5 area under the receiver operating characteristic curve; CI 5 confidence interval; FN 5 false negative; FP 5 false positive;DIVC 5 variation in inferior vena cava; TN 5 true negative; TP 5 true positive.
850 Ultrasound in Medicine and Biology Volume 40, Number 5, 2014
Conclusióndelarnculo
• ElíndicedecolapsabilidaddelaVCI"eneungranvalorparadis"nguiralrespondedordevolumenyalnorespondedor.
• Predicemejorenpacientesven"lados(volumen"dalpredecible)
• Pacientesreanimadosconcoloides


IJV
Alterna"vamedirPVC
Noinvasivo
Alterna"vacuandonosepuedemedir
IVC
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112
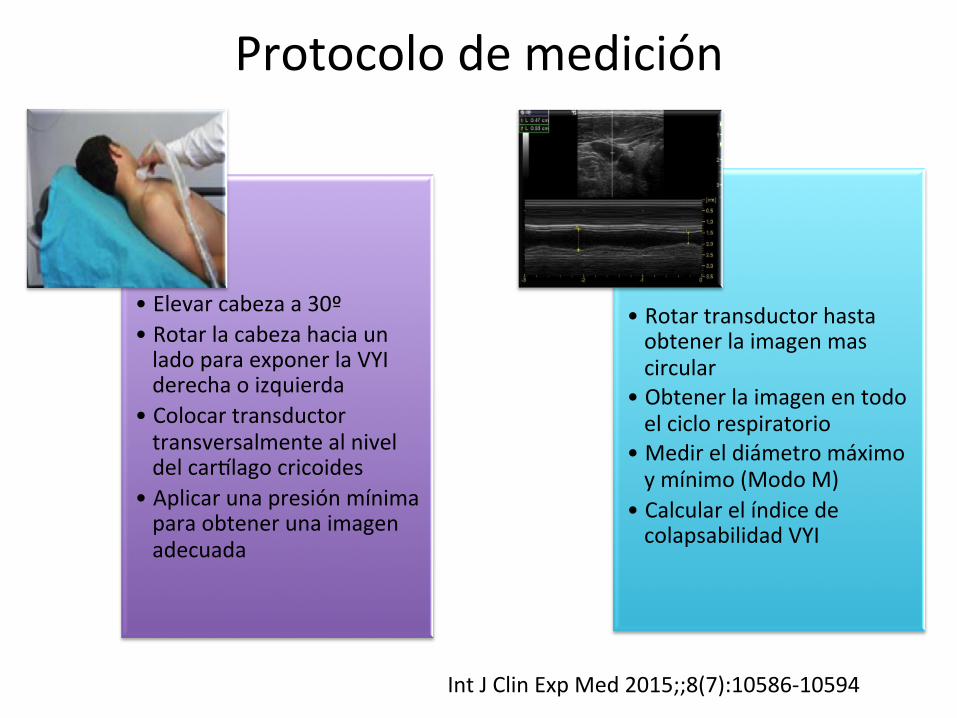
Protocolodemedición
• Elevarcabezaa30º• RotarlacabezahaciaunladoparaexponerlaVYIderechaoizquierda
• Colocartransductortransversalmentealniveldelcarnlagocricoides
• Aplicarunapresiónmínimaparaobtenerunaimagenadecuada
• Rotartransductorhastaobtenerlaimagenmascircular
• Obtenerlaimagenentodoelciclorespiratorio
• Medireldiámetromáximoymínimo(ModoM)
• CalcularelíndicedecolapsabilidadVYI
IntJClinExpMed2015;;8(7):10586-10594
to maximal diameter with insufflation, and the inferior venacava (IVC) distensibility index, calculated as the differencein maximal diameter at inflation and minimal diameter atexpiration predict volume responsiveness [6]. IVC imagingcan be problematic in the obese and those with ascites, andSVC imaging, though more accurate requires transesopha-geal echocardiography, limiting its application.Many clinical examples, from tricuspid regurgitation
to heart failure, from right heart failure to both hypo-and hypervolemia illustrate that any time pressure andvolume change within the intrathoracic systemic venouscompartment a change also occurs in extrathoracicveins, such as in the intra-abdominal IVC or extra-thoracic internal jugular vein (IJV) [7-10]. Based on thislinkage of intrathoracic venous pressure and volume toextrathoracic venous pressure we hypothesized thatright heart functional status relative to its volume re-sponsiveness should be reflected by changes in IJV pres-sures as assessed by IJV diameter changes.Since IJV imaging does not require transesophageal
echocardiography and is technically easier to performthan IVC visualization, we tested the hypothesis that re-spiratory changes in IJV diameter in mechanically venti-lated patients would also predict fluid responsiveness.
Materials and methodsAfter approval from the ethical committee for humanbiomedical of Azienda Ospedaliero Universitaria Pisanaand the University of Pittsburgh, a prospective study wasestablished elaborating hemodynamic data obtainedfrom patients presenting sepsis, according to the defin-ition of, and treated following the indications of the Sur-viving Sepsis Campaign [11]. Patients with history of anycardiac disease, evidence of jugular vein thrombosis oratrial fibrillation were excluded. Informed consent wasobtained from all patients.All enrolled patients older than 18 years were mechan-
ically ventilated in mandatory minute ventilation(MMV) modality in supine position with the head ele-vated to 30°, and with ventilatory parameters adjusted tomaintain Pplat <30 cmH2O (median 20 cmH2O, IQR 18to 22), PCO2 <40 mmHg (respiratory rate median 16breaths per minute, IQR 12 to 17), SaO2 >96%, with atidal volume of 6 to 8 ml/kg, positive end-expiratorypressure (PEEP) of 6 cmH2O (median 6 cmH2O, IQR 5to 7) and inspired oxygen fraction (FiO2) of 0.4.We analyzed a series of measured hemodynamic vari-
ables from an indwelling radial arterial catheter in septicpatients. These data included cardiac index (CI) (L/min/M2), heart rate (beats/minute), mean arterial pres-sure (MAP) (mmHg), CVP (mmHg) and pulse pressurevariation (PPV) using the the Most Care® (Vytech Health,Padova, Italy) continuous hemodynamic monitoring systembased on the pressure recording analytical method (PRAM)
algorithm [12]. PPV is defined as the ratio of the maximumdifference in PP observed over three respiratory cycles andthe average of these two PPs as follows:
PPmax−PPminð Þ= PPmax þ PPminð Þ=2ð Þ:
A PPV >13% was presumed to identify those patientswho would increase their cardiac output by >15% inresponse to a 500-ml colloid fluid bolus, as previouslyvalidated [4].We simultaneously collected the hemodynamic data and
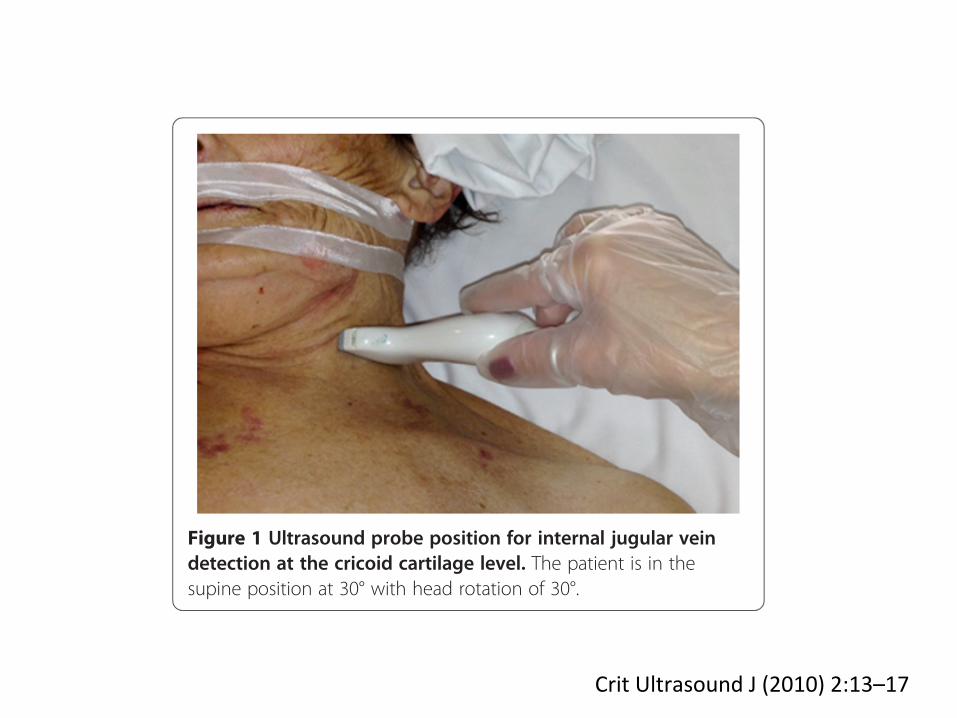
an ultrasound (US) examination of the IJV by the same op-erator. The ultrasound examination was performed with a12-MHz linear transducer (Esaote, Milan, Italy) and ultra-sound system (MyLab™ 50 XVision). The IJV was visualizedwith two-dimensional echo at the level of the cricoid cartil-age and recognized by compression, color Doppler andpulse wave Doppler sampling. As the patient position caninfluence IJV, all measurements were performed in thesemi-recumbent position (head elevated 30°).The antero-posterior (AP) IJV diameter was measured
using M-mode during a respiratory cycle. In order to avoidchanges in vein diameter unrelated to respiratory variation,gentle pressure by the US probe was used to collapse theIJV in order to distinguish it from the carotid artery, thenthe pressure was relieved to the US probe-skin interfaceand attention was given to avoid influence of probe com-pression on IJV dimensions [13] during the US examin-ation. Moreover, in order to avoid interference of probe-to-vein angle, the JV evaluation was performed by posi-tioning the probe perpendicular to the skin and orientedorthogonally to the JV short-axis diameter (Figure 1). TheIJV distensibility index (%) was calculated as the ratio ofthe difference in the maximal IJV AP diameter during in-spiration and minimum IJV expiratory diameter to theminimum IJV expiratory diameter × 100.
Figure 1 Ultrasound probe position for internal jugular veindetection at the cricoid cartilage level. The patient is in thesupine position at 30° with head rotation of 30°.
Guarracino et al. Critical Care (2014) 18:647 Page 2 of 8
CritUltrasoundJ(2010)2:13–17
patients or 13% of patients were on vasopressor support
(two for each group). Sixteen patients (52%) were hypo-
volemic patients with a mean age of 63 (±19) years andweight of 77.7 (±17.5) kg. Fifteen patients or 48% were
euvolemic patients, with a mean age of 59 years (±13) and
weight of 82.1 kg (±21.8).The hypovolemic patients were 50% male and 75%
white. The baseline physiologic variables of the hypovo-
lemic group were as follows: mean blood pressure 77(±32) mmHg, heart rate 99 (±19) beats per minute, and
respiratory rate 23 (±7) breaths per minute, and tempera-
ture 37.3!C (±0.8). Significant variables between thehypovolemic and euvolemic patients were the mean arterial
pressure, heart rate, respiratory rate, CVP, and IJV col-
lapsibility index (Table 2).The logistic regression model for variables associated
with hypovolemia showed that the following variables:
heart rate, respiratory rate, systolic blood pressure, meanarterial pressure, CVP, and IJV collapsibility index were all
significant (p\ 0.05) (Table 3). The diagnosis of hypo-
volemia was established by the treating ICU physician andthe logistic regression model was used to correlate the
results. The ROC curve analysis found the best sensitivity
of 87.5% and specificity of 100%, when IJV collapsibility
index was C39%. In comparing the area under the ROCcurve (AUC) for the IJV collapsibility index was 0.938
with no significant difference to the CVP AUC of 0.87
(p = 0.467) (Fig. 2).Subset analysis of the five mechanically ventilated
hypovolemic patients showed a mean IJV collapsibility
index of 52.9% compared to the one euvolemic mechani-cally ventilated patient with an IJV collapsibility index of
21% (p = 0.31). All mechanically ventilated patients were
on PEEP.
Discussion
Point-of-care ultrasound can identify the IJV collapsibility
index, which can aid in determining the volume status inICU patients. The IJV collapsibility index can be applied to
most ICU patients including those with mechanical venti-
lation on PEEP or vasopressor support, which were notincluded in previous studies [1, 2].
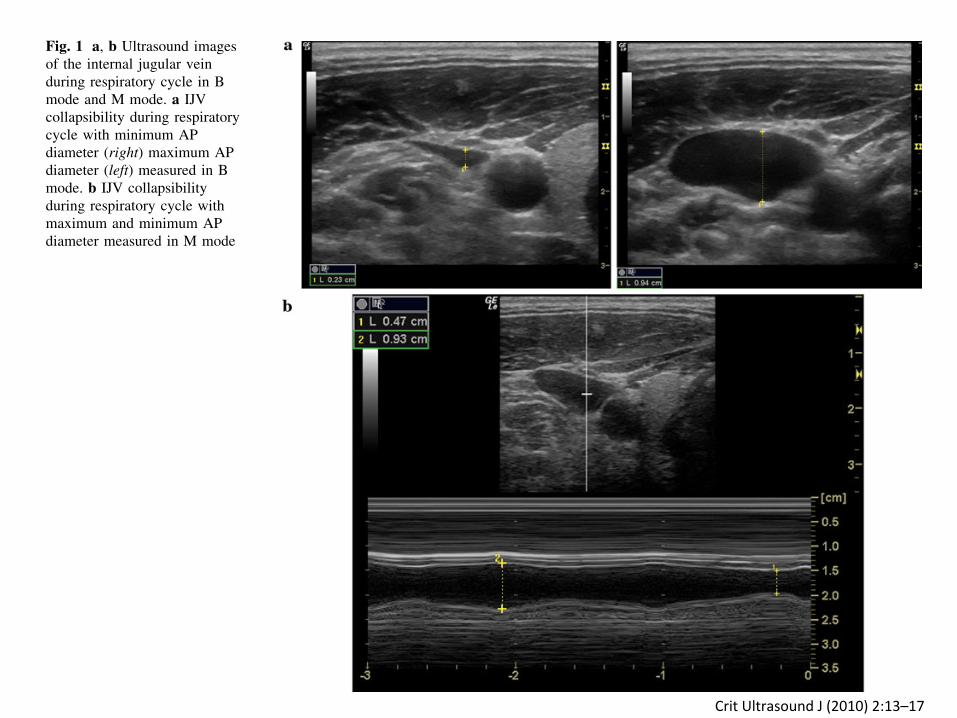
Fig. 1 a, b Ultrasound imagesof the internal jugular veinduring respiratory cycle in Bmode and M mode. a IJVcollapsibility during respiratorycycle with minimum APdiameter (right) maximum APdiameter (left) measured in Bmode. b IJV collapsibilityduring respiratory cycle withmaximum and minimum APdiameter measured in M mode
Crit Ultrasound J (2010) 2:13–17 15
123
CritUltrasoundJ(2010)2:13–17
ÍndicedeColapsabilidad = Diámetromáximo-Diámetromínimo x100enpacientesconven"laciónDiámetromáximoespontanea
AvancesCardiol2015;35(2):120-132RevAsocMexMedCrityTerInt2015;29(2):105-112
2.4. Primary data analysis
The mean (±SD) was reported for all normally distributeddata. To assess differences between continuous variables, ttests were used. The correlation between 2 variables wasassessed using interclass correlation coefficients.
3. Results
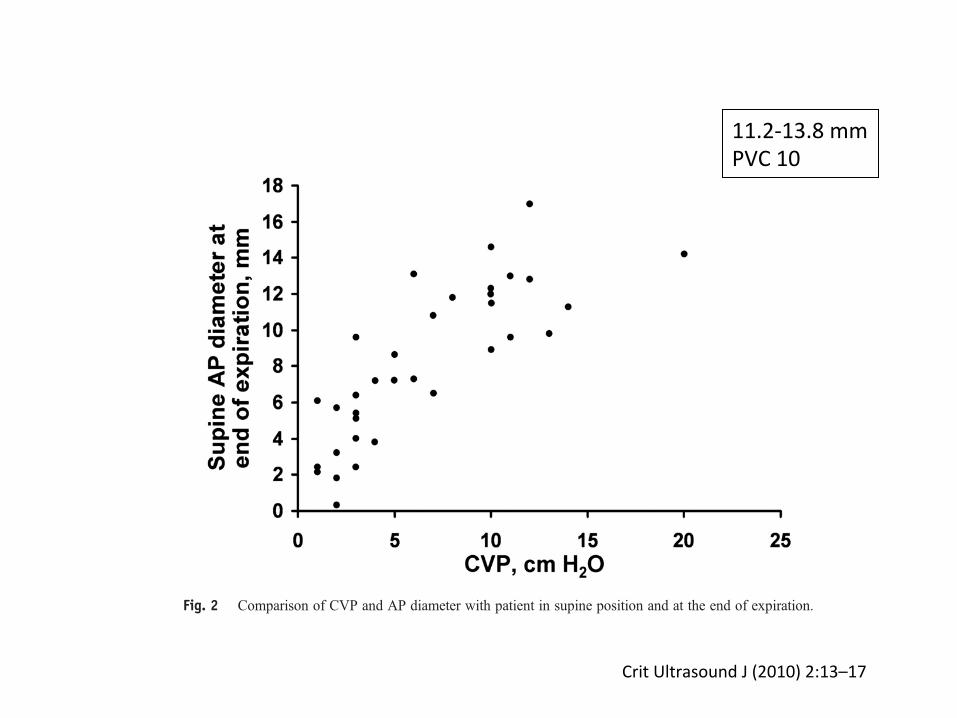
In total, 34 patients were evaluated by the primaryinvestigator over a 4-month period. The characteristics of thepatients are summarized in Table 1. As shown in Fig. 1, mostpatients (27 patients) had a CVP less than or equal to 10 cmH2O. Seven patients had a CVP greater than 10 cm H2O.Because open-ended PICCs were used to measure thepatients' CVPs, 1 cm H2O was subtracted from the actualCVP reading; this factor was reflected in the data of patientswho had CVPs of “0” cm H2O.
For statistical analysis, CVP values were divided into 2categories: “low” (b10 cm H2O) and “high” (≥10 cmH2O). These categories were formed after enrollment andafter the distribution of CVPs within the patient group was
analyzed. The interclass correlation coefficient was highestwith the patient in a supine position and at the end ofexpiration (0.82 [95% confidence interval [CI]). Within thisgroup, the standard t test of AP diameter was 7.0 mm (95%CI, 3.5-7.3) for a low CVP and 12.5 mm (95% CI, 10.9-13.5) for a high CVP. Table 2 summarizes the correlationcoefficients overall; Fig. 2 compares the CVP with the APdiameter of the patient in a supine position and at the endof expiration.
To evaluate whether the patient's neck circumference orBMI would affect the correlation coefficients, indices werecreated using AP diameter or area vs BMI and neckcircumference. These indices and subsequent correlationcoefficients are shown in Table 3. The use of neckcircumference or BMI did not positively affect the correla-tion between IJV measurements and CVP.
A separate study group of 10 volunteers also had IJVmeasurements, to assess interobserver variation. Interob-server variation between the principal investigator and theexpert ultrasonographer remained small: interclass correla-tion coefficient between the 2 observers was 0.92(95% CI).
4. Discussion
In this pilot study, we found that a rapid ultrasoundtechnique, regardless of the operator's prior ultrasonographicskills, has the potential to rapidly and accurately determinethe CVP and to be used to assess volume status. This findingmay have tremendous application in the care of the acutelyill patient.
Table 3 Indices and interclass correlation coefficients
Index of measurements with patient insupine position during expiration
Correlationcoefficient
AP diameter and BMI 0.71AP diameter and neck circumference 0.72Area and BMI 0.60Area and neck circumference 0.63
Fig. 2 Comparison of CVP and AP diameter with patient in supine position and at the end of expiration.
854 S.P. Donahue et al.
CritUltrasoundJ(2010)2:13–17
11.2-13.8mmPVC10

RESEARCH Open Access
Jugular vein distensibility predicts fluidresponsiveness in septic patientsFabio Guarracino1*, Baldassarre Ferro1, Francesco Forfori2, Pietro Bertini1, Luana Magliacano2 and Michael R Pinsky3
Abstract
Introduction: The purpose of the study was to verify the efficacy of using internal jugular vein (IJV) size anddistensibility as a reliable index of fluid responsiveness in mechanically ventilated patients with sepsis.
Methods: Hemodynamic data of mechanically ventilated patients with sepsis were collected through a radialarterial indwelling catheter connected to continuous hemodynamic monitoring system (Most Care®, Vytech Health,Padova, Italy), including cardiac index (CI) (L/min/M2), heart rate (beats/min), mean arterial pressure (MAP) (mmHg),central venous pressure (CVP) (mmHg) and arterial pulse pressure variation (PPV), coupled with ultrasoundevaluation of IJV distensibility (%), defined as a ratio of the difference between IJV maximal antero-posteriordiameter during inspiration and minimum expiratory diameter to minimum expiratory diameter x100. Patients wereretrospectively divided into two groups; fluid responders (R), if CI increase of more than or equal to 15% after a 7ml/kg crystalloid infusion, and non-responders (NR) if CI increased more than 15%. We compared differences inmeasured variables between R and NR groups and calculated receiver-operator-characteristic (ROC) curves ofoptimal IJV distensibility and PPV sensitivity and specificity to predicting R. We also calculated a combined inferiorvena cava distensibility-PPV ROC curve to predict R.
Results: We enrolled 50 patients, of these, 30 were R. Responders presented higher IJV distensibility and PPV beforefluid challenge than NR (P <0.05). An IJV distensibility more than 18% prior to volume challenge had an 80%sensitivity and 85% specificity to predict R. Pairwise comparison between IJV distensibility and PPV ROC curvesrevealed similar ROC area under the curve results. Interestingly, combining IJV distensibility more than 9.7% and PPVmore than 12% predicted fluid responsiveness with a sensitivity of 100% and specificity of 95%.
Conclusion: IJV distensibility is an accurate, easily acquired non-invasive parameter of fluid responsiveness inmechanically ventilated septic patients with performance similar to PPV. The combined use of IJV distensibilitywith left-sided indexes of fluid responsiveness improves their predictive value.
IntroductionIncreasing cardiac output by volume expansion is acornerstone treatment of critically ill patients with sepsispresumed to have tissue hypoperfusion. Fluid resuscitationis performed because it is assumed that the heart is oper-ating of the steep ascending portion of the Frank-Starlingcurve (preload-responsive). However, fluid resuscitation inthe non-preload-responsive patient may be deleterious if itpromotes cor pulmonale, pulmonary edema, or peripheral
edema [1]. It is therefore useful to have reliable predictorsof volume responsiveness.Several studies have emphasized the reduced clinical
value of static hemodynamic parameters, such as centralvenous pressure (CVP) and pulmonary artery occludingpressure, as compared with dynamic parameters in pre-dicting fluid responsiveness [2,3]. Such dynamic indicatorsinclude positive-pressure ventilation-induced changes inleft ventricular stroke volume and arterial pulse pressure(PP) [4]. Similarly, ultrasound evaluation of respiratoryvariations of both superior and inferior vena cava diameteraccurately reflects volume responsiveness [5,6]. Specific-ally, both the superior vena cava (SVC) collapsibility index,calculated as the ratio of the difference in maximal diam-eter at expiration and the minimal diameter at inspiration
* Correspondence: [email protected] of Anesthesia and Critical Care Medicine, CardiothoracicAnesthesia and Intensive Care Medicine, Azienda Ospedaliero UniversitariaPisana, Via Paradisa, 2 56123 Pisa, ItalyFull list of author information is available at the end of the article
© 2014 Guarracino et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly credited. The Creative Commons Public DomainDedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article,unless otherwise stated.
Guarracino et al. Critical Care (2014) 18:647 DOI 10.1186/s13054-014-0647-1

50pacientes(3
0respon
dedo
res,
20re
spon
dedo
res)
IC,FC,TAM,PVC,VPP,IJV
>18%IJV
Sensibilidad80%Especifidad95%
Conclusión
IJV(simple,fácil,accesible)
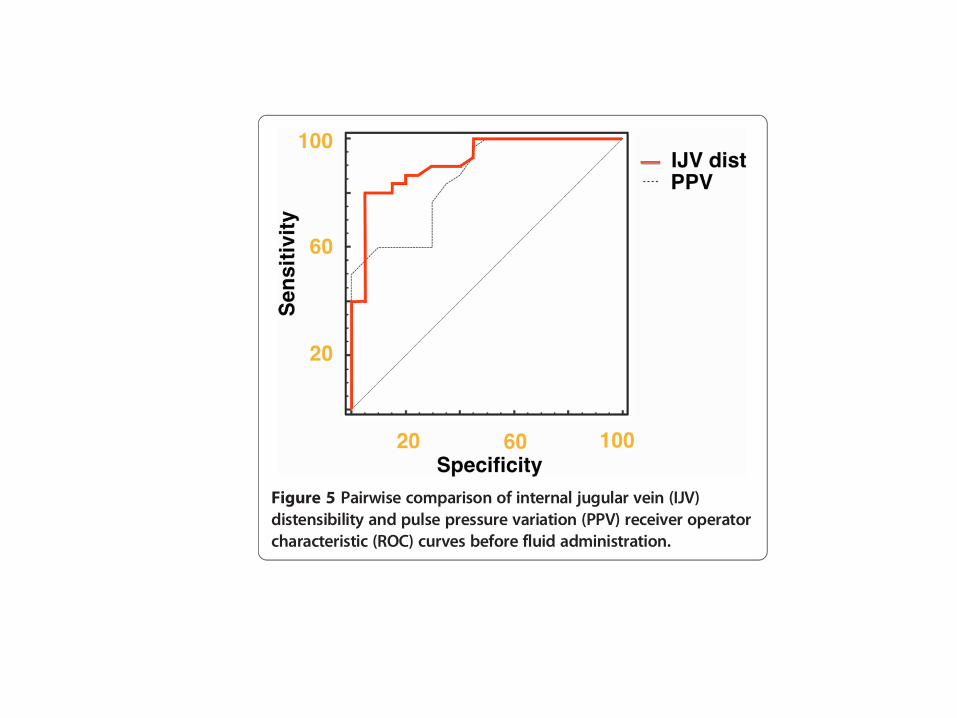
Cannesson et al. used a gray-zone approach evidencingthat when PPV decreases into a gray zone between 9 and13%, uncertainty exists and clinicians should attempt todefine volume responsiveness using additional measures[16]. By combining IJV distensibility with PPV, we demon-strate that such gray-zone conditions can be minimized.Our new measure of IJV diameter change is easily seen
with US with minimal training, as this approach is fre-quently used for US-guided central vein catheterization.We demonstrated the reliability of IJV distensibility ondetecting fluid responsiveness of ventilated patients with avalue of 16.4% IJV distensibility having a sensitivity of 80%and a specificity of 85% in mechanically ventilated septicpatients. Similarly, PPV threshold values of 12.5% havebeen reported in the literature to discriminate between Rand NR with similar sensitivity and specificity. Thus, bothPPV and IJV distensibility can be used to assess fluid re-sponsiveness. Perhaps more interesting, the combinationof both PPV and IJV distensibility improves the sensitivityand specificity of fluid responsiveness prediction with bestresults for values of IJV >9.9% and PPV of >12%. Thesedata suggest that combining right- and left-sided dynamicparameters should improve their predictive values.Our study has several limitations. First, all subjects
were on mechanical ventilation and fully adapted to theventilator. However, IVC collapse analysis remains pre-dictive of fluid responsiveness in spontaneously breath-ing subjects, suggesting that the IJV distensibility indexmay remain valid as well. Still, the IJV distensibilityindex needs to be studied in spontaneously breathingsubjects. Second, we did not also measure IVC collapseor stroke-volume variation, both measures of volume re-sponsiveness similar in quality to our IJV distensibilityand PPV measures, respectively. Still, PPV should be anacceptable surrogate for stroke-volume variation in this
type of comparison. Third, changes in CVP influencethe IJV pressure and diameter and may decrease relativedistensibility. Conditions associated with increased intra-abdominal or intrathoracic pressure may potentially in-crease CVP and can lead to a reduced IJV distensibilityindex independent of preload responsiveness. We didnot study the effect of high CVP on IJV distensibility.However, this process would have similar effects on bothSVC and IVC collapse parameters. Accordingly, right-sided US indices, using large-vein collapsibility to predictvolume responsiveness, require careful awareness ofthese potential limitations. Again, these specific clinicalconditions may also minimize the predictive values ofPPV as well. Fourth, patients’ position can influence IJVsize. The supine position leads to increased IJV diameter,which is further increased in the Trendelenburg position,whereas sitting or standing can reduce the IJV filling andIJV diameter. Therefore, we made all our measurementsfrom a standard 30° head of the bed elevated semi-recumbent position. However, since this is the recom-mended position for supine ventilated patients, tominimize aspiration, this limitation needs to be under-stood and positioning standardized in clinical practice ifIJV distensibility index is used for clinical decision-making. Fifth, we did not include patients with cardiacdisease, who would particularly benefit from functionalhemodynamic monitoring. However, in this initial clin-ical study we did not aim to evaluate the effectiveness ofsuch methods in those patients, because of the potentialconfounding effect that right heart failure would imposeon venous pressures. As cor pulmonale markedly altersother dynamic indices, often making them appear positivewhen not, we chose to also exclude these patients fromour study. However, this patient cohort had a wide rangeof baseline cardiac reserve, as manifested by having only30 of 50 patients being volume responsive. Therefore, inthis initial validation study, any confounding condition,such as cardiac disease, jugular vein thrombosis or atrialfibrillation was excluded. Sixth, our only cardiovascularchallenge was fluid loading. It is not clear if the use ofvasoactive drugs, which may independently alter bothCVP and the effective circulating blood volume, would in-dependently affect the IJV distensibility index. This inter-action and its interpretation remain to be assessed. Finally,as all measurements were performed by a single operator,inter-observer variability in IJV diameter measurement re-mains to be assessed in future studies.
ConclusionsUltrasound evaluation of IJV distensibility is a simple,easy, and readily accessible bedside measure that predictsvolume responsiveness in critically ill ventilator-dependentseptic patients. Importantly, the combined use of IJV dis-tensibility with PPV increases the predictive value of these
Figure 5 Pairwise comparison of internal jugular vein (IJV)distensibility and pulse pressure variation (PPV) receiver operatorcharacteristic (ROC) curves before fluid administration.
Guarracino et al. Critical Care (2014) 18:647 Page 6 of 8

Rev Bras Ter Intensiva. 2015;27(3):205-211
Right internal jugular vein distensibility appears to be a surrogate marker for inferior vena cava vein distensibility for evaluating fluid responsiveness
ORIGINAL ARTICLE
INTRODUCTION
Circulatory failure is often the result of hypovolemia, which therefore must be corrected. Volume expansion improves the prognosis,(1,2) whereas inappropriate use of vasoconstrictors leads to harmful tissue hypoperfusion.(3,4) However, volume expansion may prove ineffective or even deleterious, by worsening pre-existing heart failure or by degrading gas exchange in a mechanically ventilated patient.(5) Reliable tools for predicting the efficacy of volume expansion are therefore essential in critically ill patients. Several tools have proven sufficiently reliable, including minimally invasive measurements, such as variation in pulse pressure.(6,7) The inferior vena cava (IVC) can be visualized by a subcostal
Fabiano Broilo1, Andre Meregalli1, Gilberto Friedman2
1. Central Intensive Care Unit, Complexo Hospitalar Santa Casa - Porto Alegre (RS), Brazil.2. Postgraduate Program in Pneumological Sciences, Faculdade de Medicina, Universidade Federal do Rio Grande do Sul - Porto Alegre (RS), Brazil.
Objective: To investigate whether the respiratory variation of the inferior vena cava diameter (∆DIVC) and right internal jugular vein diameter (∆DRIJ) are correlated in mechanically ventilated patients.
Methods: This study was a prospective clinical analysis in an intensive care unit at a university hospital. Thirty-nine mechanically ventilated patients with hemodynamic instability were included. ∆DIVC and ∆DRIJ were assessed by echography. Vein distensibility was calculated as the ratio of (A) Dmax - Dmin/Dmin and (B) Dmax - Dmin/mean of Dmax - Dmin and expressed as a percentage.
Results: ∆DIVC and ∆DRIJ were correlated by both methods: (A) r = 0.34, p = 0.04 and (B) r = 0.51, p = 0.001. Using 18% for ∆DIVC, indicating fluid responsiveness by method (A), 16 patients
Conflicts of interest: None.
Submitted on March 21, 2015Accepted on June 30, 2015
Corresponding author:Gilberto FriedmanHospital de Clínicas de Porto AlegreRua Ramiro Barcelos, 2.350 - Santa CecíliaZip code: 90035-903 - Porto Alegre (RS), BrazilE-mail: [email protected]
Responsible editor: Luciano César Pontes de Azevedo
A distensibilidade da veia jugular interna parece ser uma alternativa à distensibilidade da veia cava inferior para avaliar a responsividade a fluidos
ABSTRACT
Keywords: Vena cava, inferior/ultrasonography; Jugular veins/ultrasonography; Fluid therapy; Respiration, artificial; Hemodynamics
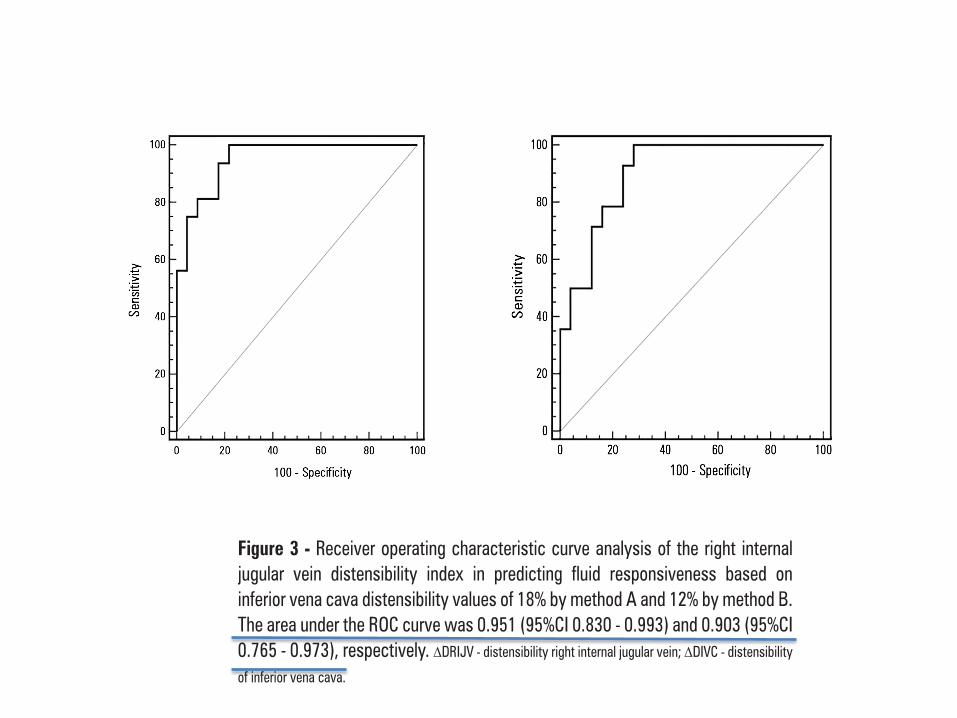
were responders and 35 measurements showed agreement (weighted Kappa = 0.80). The area under the ROC curve was 0.951 (95%CI 0.830 - 0.993; cut-off = 18.92). Using 12% for ∆DIVC, indicating fluid responsiveness by method (B), 14 patients were responders and 32 measurements showed agreement (weighted Kappa = 0.65). The area under the ROC curve was 0.903 (95%CI 0.765 - 0.973; cut-off value = 11.86).
Conclusion: The respiratory variation of the inferior vena cava and the right internal jugular veins are correlated and showed significant agreement. Evaluation of right internal jugular vein distensibility appears to be a surrogate marker for inferior vena cava vein distensibility for evaluating fluid responsiveness.
DOI: 10.5935/0103-507X.20150042
RevBrasTerIntensiva.2015;27(3):205-211
46pacientesVen"ladosChoque
IVC-ICIJV-IC
a.D.Máximo-D.Mínimo/D.Mínimoenespiración(18%)b.D.Máximo-D.Mínimo/D.Máximo+D.Mínimo(12%)
Right internal jugular vein distensibility 209
Rev Bras Ter Intensiva. 2015;27(3):205-211
Figure 3 - Receiver operating characteristic curve analysis of the right internal jugular vein distensibility index in predicting fluid responsiveness based on inferior vena cava distensibility values of 18% by method A and 12% by method B. The area under the ROC curve was 0.951 (95%CI 0.830 - 0.993) and 0.903 (95%CI 0.765 - 0.973), respectively. �DRIJV - distensibility right internal jugular vein; �DIVC - distensibility
of inferior vena cava.
DISCUSSION
Our findings demonstrate that ultrasound evaluation of RIJV respiratory diameter changes can serve as a simple alternative or surrogate marker for IVC distensibility
indexes in the evaluation of the appropriateness of volume expansion in mechanically ventilated patients.
Correcting hypovolemia is of paramount importance,(1,2) but in mechanically ventilated patients, its correction should be guided to avoid ineffective or even deleterious volume expansion and worsening of the respiratory function.(5) Mechanical ventilation induces cyclic variations in vena cava diameter that have been shown to be accurate predictors of fluid responsiveness.(8,9,19) However, IVC measurements are often not possible.(13)
There are few studies investigating respiratory variations in RIJV diameter in the evaluation of hypovolemia or hemodynamic response to a fluid challenge, and these were conducted mainly in spontaneously breathing patients.(14,15,17) During inspiration, the pressure inside the thorax increases more than the pressure outside the thorax. Therefore, the pressure gradient for venous return is reduced, the systemic venous return decreases, the volume of extrathoracic venous blood decreases, and hence the endoluminal diameter of distensible veins, such as the jugular vein increases.(8,10,11) A greater decrease in venous return during insufflation may occur in a hypovolemic patient.
Our study demonstrated that the changes in IJV diameter during inspiration and expiration were significant. Similar findings were observed in several studies designed to evaluate IJV changes before and after blood donation(14,15) or fluid challenge.(17) However, in patients who are breathing spontaneously, the IJV collapse may be inexact.
In critically ill, mechanically ventilated patients, the subject is even less well studied. Recently, Guarracino et al. showed that IJV distensibility accurately predicts volume responsiveness.(17) They measured cardiac output to calculate a cut-off of 18% with an 80% sensitivity and 85% specificity for predicting response. Thus, we compared the RIJV with IVC distensibility to predict fluid responsiveness, to explore the hypothesis that cyclic respiratory changes in both veins could be similar. In our population of mechanically ventilated patients with hemodynamic instability, we have shown that the IVC distensibility indexes and RIJV distensibility indexes agree and are well correlated. Taken together, despite the differences in study design, our findings agree with those of Guarracino et al.(17) Although we have not evaluated volume expansion, the ∆IVC has been shown to be a good method for assessing fluid responsiveness in mechanically ventilated patients(8,9) and our results show that ∆IVC and ∆RIJV correlate well.
Right internal jugular vein distensibility 209
Rev Bras Ter Intensiva. 2015;27(3):205-211
Figure 3 - Receiver operating characteristic curve analysis of the right internal jugular vein distensibility index in predicting fluid responsiveness based on inferior vena cava distensibility values of 18% by method A and 12% by method B. The area under the ROC curve was 0.951 (95%CI 0.830 - 0.993) and 0.903 (95%CI 0.765 - 0.973), respectively. �DRIJV - distensibility right internal jugular vein; �DIVC - distensibility
of inferior vena cava.
DISCUSSION
Our findings demonstrate that ultrasound evaluation of RIJV respiratory diameter changes can serve as a simple alternative or surrogate marker for IVC distensibility
indexes in the evaluation of the appropriateness of volume expansion in mechanically ventilated patients.
Correcting hypovolemia is of paramount importance,(1,2) but in mechanically ventilated patients, its correction should be guided to avoid ineffective or even deleterious volume expansion and worsening of the respiratory function.(5) Mechanical ventilation induces cyclic variations in vena cava diameter that have been shown to be accurate predictors of fluid responsiveness.(8,9,19) However, IVC measurements are often not possible.(13)
There are few studies investigating respiratory variations in RIJV diameter in the evaluation of hypovolemia or hemodynamic response to a fluid challenge, and these were conducted mainly in spontaneously breathing patients.(14,15,17) During inspiration, the pressure inside the thorax increases more than the pressure outside the thorax. Therefore, the pressure gradient for venous return is reduced, the systemic venous return decreases, the volume of extrathoracic venous blood decreases, and hence the endoluminal diameter of distensible veins, such as the jugular vein increases.(8,10,11) A greater decrease in venous return during insufflation may occur in a hypovolemic patient.
Our study demonstrated that the changes in IJV diameter during inspiration and expiration were significant. Similar findings were observed in several studies designed to evaluate IJV changes before and after blood donation(14,15) or fluid challenge.(17) However, in patients who are breathing spontaneously, the IJV collapse may be inexact.
In critically ill, mechanically ventilated patients, the subject is even less well studied. Recently, Guarracino et al. showed that IJV distensibility accurately predicts volume responsiveness.(17) They measured cardiac output to calculate a cut-off of 18% with an 80% sensitivity and 85% specificity for predicting response. Thus, we compared the RIJV with IVC distensibility to predict fluid responsiveness, to explore the hypothesis that cyclic respiratory changes in both veins could be similar. In our population of mechanically ventilated patients with hemodynamic instability, we have shown that the IVC distensibility indexes and RIJV distensibility indexes agree and are well correlated. Taken together, despite the differences in study design, our findings agree with those of Guarracino et al.(17) Although we have not evaluated volume expansion, the ∆IVC has been shown to be a good method for assessing fluid responsiveness in mechanically ventilated patients(8,9) and our results show that ∆IVC and ∆RIJV correlate well.
Right internal jugular vein distensibility 209
Rev Bras Ter Intensiva. 2015;27(3):205-211
Figure 3 - Receiver operating characteristic curve analysis of the right internal jugular vein distensibility index in predicting fluid responsiveness based on inferior vena cava distensibility values of 18% by method A and 12% by method B. The area under the ROC curve was 0.951 (95%CI 0.830 - 0.993) and 0.903 (95%CI 0.765 - 0.973), respectively. �DRIJV - distensibility right internal jugular vein; �DIVC - distensibility
of inferior vena cava.
DISCUSSION
Our findings demonstrate that ultrasound evaluation of RIJV respiratory diameter changes can serve as a simple alternative or surrogate marker for IVC distensibility
indexes in the evaluation of the appropriateness of volume expansion in mechanically ventilated patients.
Correcting hypovolemia is of paramount importance,(1,2) but in mechanically ventilated patients, its correction should be guided to avoid ineffective or even deleterious volume expansion and worsening of the respiratory function.(5) Mechanical ventilation induces cyclic variations in vena cava diameter that have been shown to be accurate predictors of fluid responsiveness.(8,9,19) However, IVC measurements are often not possible.(13)
There are few studies investigating respiratory variations in RIJV diameter in the evaluation of hypovolemia or hemodynamic response to a fluid challenge, and these were conducted mainly in spontaneously breathing patients.(14,15,17) During inspiration, the pressure inside the thorax increases more than the pressure outside the thorax. Therefore, the pressure gradient for venous return is reduced, the systemic venous return decreases, the volume of extrathoracic venous blood decreases, and hence the endoluminal diameter of distensible veins, such as the jugular vein increases.(8,10,11) A greater decrease in venous return during insufflation may occur in a hypovolemic patient.
Our study demonstrated that the changes in IJV diameter during inspiration and expiration were significant. Similar findings were observed in several studies designed to evaluate IJV changes before and after blood donation(14,15) or fluid challenge.(17) However, in patients who are breathing spontaneously, the IJV collapse may be inexact.
In critically ill, mechanically ventilated patients, the subject is even less well studied. Recently, Guarracino et al. showed that IJV distensibility accurately predicts volume responsiveness.(17) They measured cardiac output to calculate a cut-off of 18% with an 80% sensitivity and 85% specificity for predicting response. Thus, we compared the RIJV with IVC distensibility to predict fluid responsiveness, to explore the hypothesis that cyclic respiratory changes in both veins could be similar. In our population of mechanically ventilated patients with hemodynamic instability, we have shown that the IVC distensibility indexes and RIJV distensibility indexes agree and are well correlated. Taken together, despite the differences in study design, our findings agree with those of Guarracino et al.(17) Although we have not evaluated volume expansion, the ∆IVC has been shown to be a good method for assessing fluid responsiveness in mechanically ventilated patients(8,9) and our results show that ∆IVC and ∆RIJV correlate well.
Conclusiónes
Las imágenesultrasonográficasde la vena cavainferior y vena yugular interna es segura, noinvasivaparadeterminarlarespuestaalíquidosenunpacientegrave.