Embed Size (px)
Citation preview

UN DECENNIO DI INNOVAZIONE
CON GLI ANTICOAGULANTI ORALI DIRETTI:
NUOVE PROSPETTIVE NELLE APPLICAZIONI CLINICHE
12° Meeting CardioLucca 2018
“IL labirinto cuore tra scienza e assistenza”
Lucca, 23 Febbraio 2018
Giuseppe Di Pasquale
Direttore Dipartimento Medico ASL Bologna
Direttore Unità Operativa Cardiologia
Ospedale Maggiore, Bologna
Giuseppe Di Pasquale Disclosures
• Member of the Steering Committee of the RELY, PALLAS, and
GLORIA AF
• Member of Advisory Board of Dabigatran,
Rivaroxaban, Apixaban, Dronedarone, Edoxaban
• Consulting fees / honoraria
Boehringer Ingelheim, Bayer AG, Sanofi Aventis
BMS / Pfizer, Daiichi Sankyo
FA valvolare

November 7, 2017
Breithardt G at al. Eur Heart J 2014
Avezum A et al. Abstract 4384, ESC Congress 2013
Ezekowitz et al. Circulation 2016;134:589-598
Renda G at al. Abstract ACC 2016
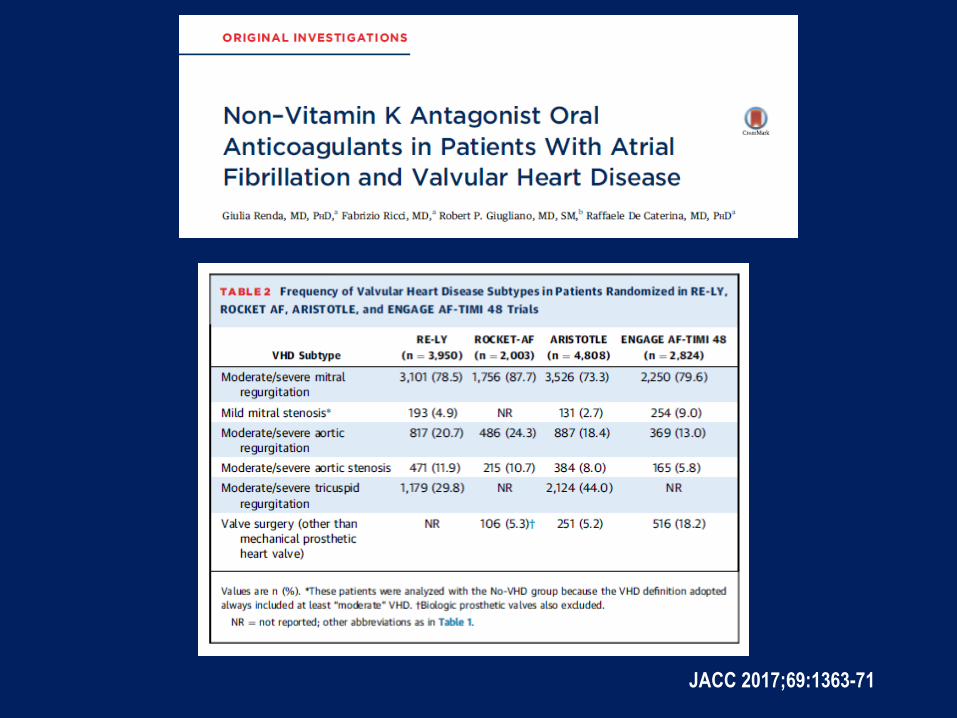
JACC 2017;69:1363-71
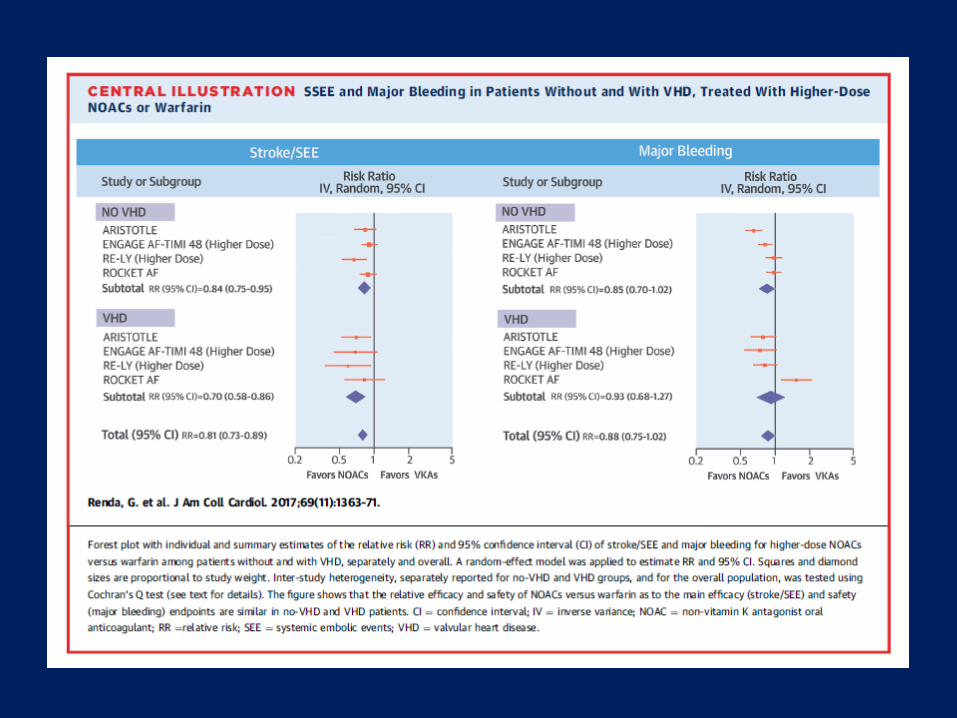
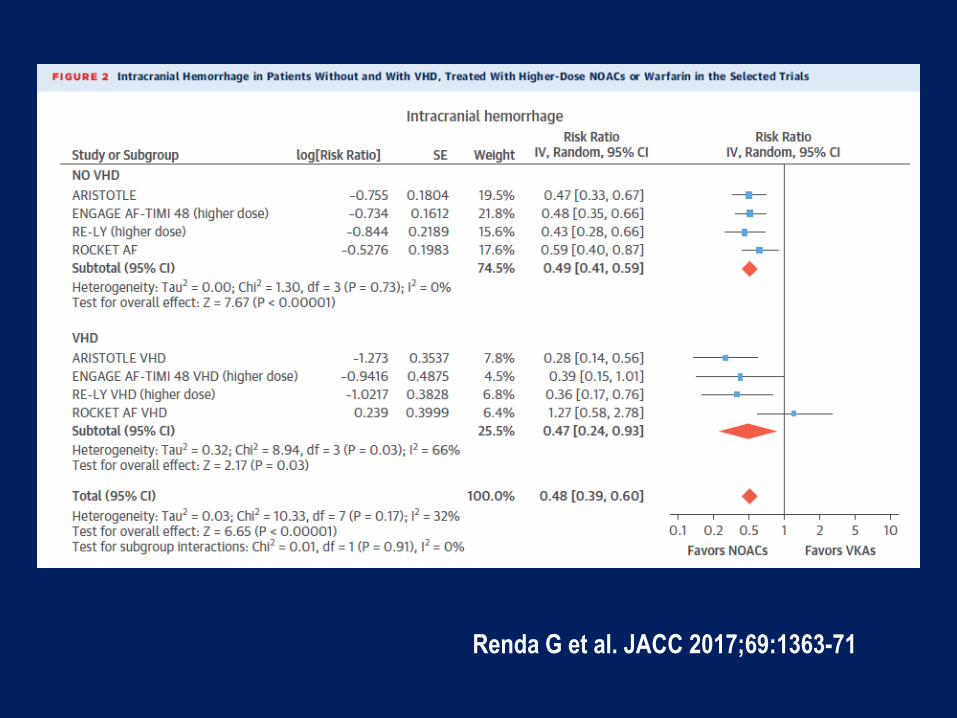
Renda G et al. JACC 2017;69:1363-71
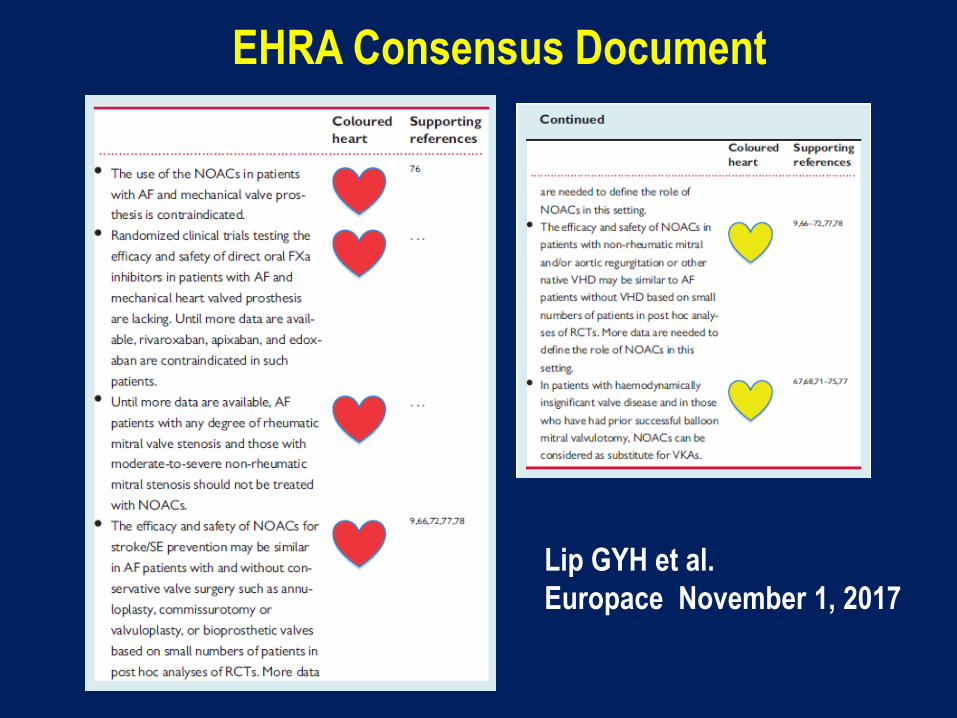
Lip GYH et al.
Europace November 1, 2017
EHRA Consensus Document
Circulation 2017;135:1273-75
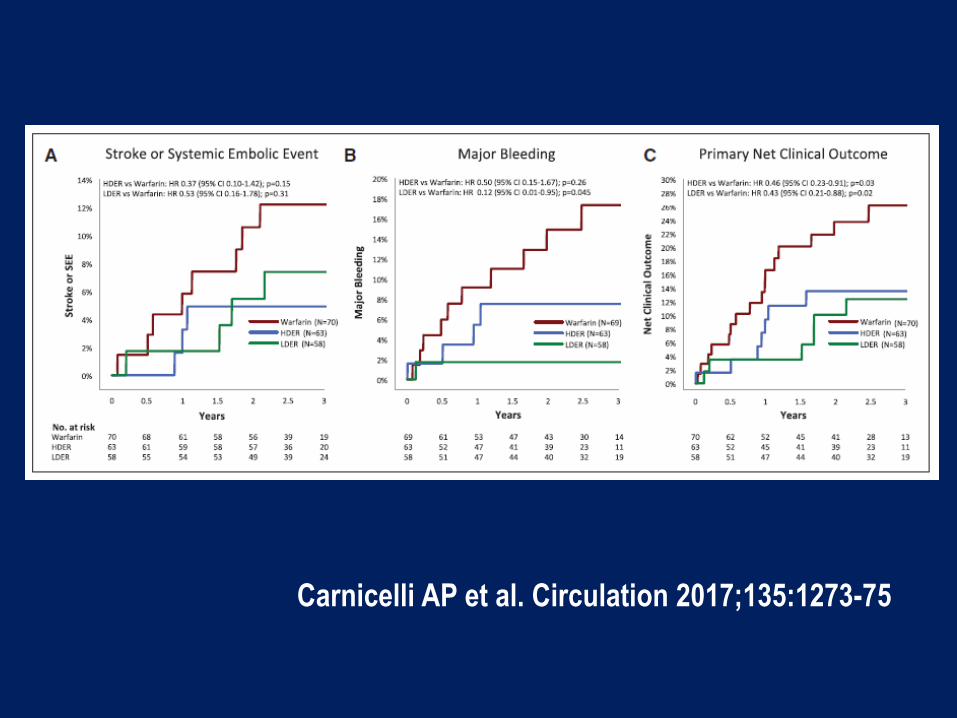
Carnicelli AP et al. Circulation 2017;135:1273-75
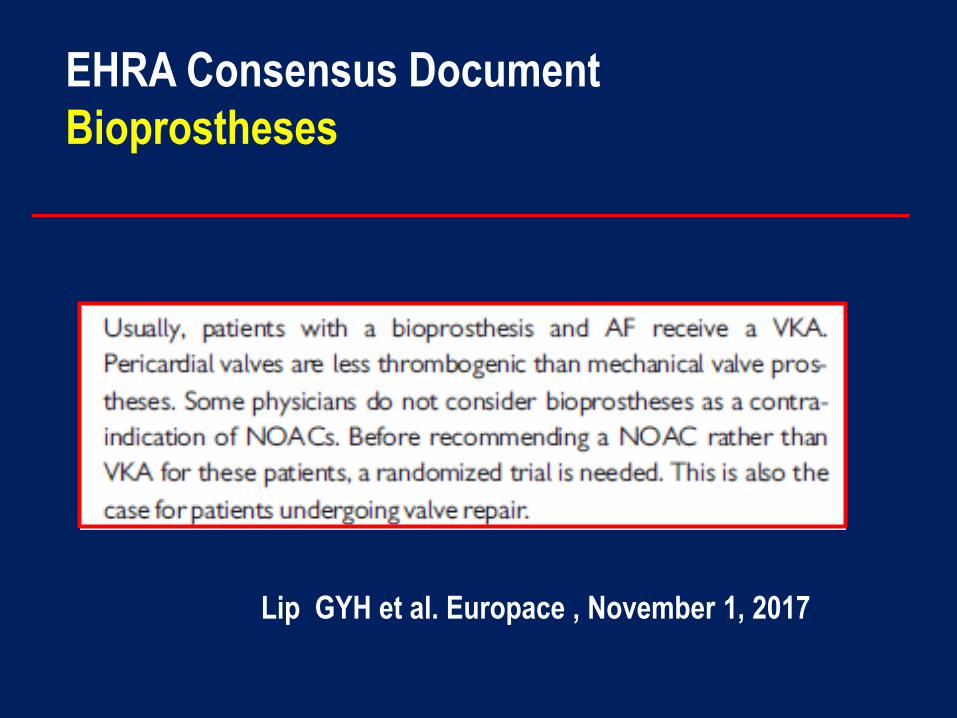
Lip GYH et al. Europace , November 1, 2017
EHRA Consensus Document
Bioprostheses
NAO: Quali spazi futuri?
NOACs : Future Perspectives
New Frontiers
NOACs vs LAAO▪
HF with SR▪
TAVI▪
ESUS▪
Cardiopatia ischemica cronica▪
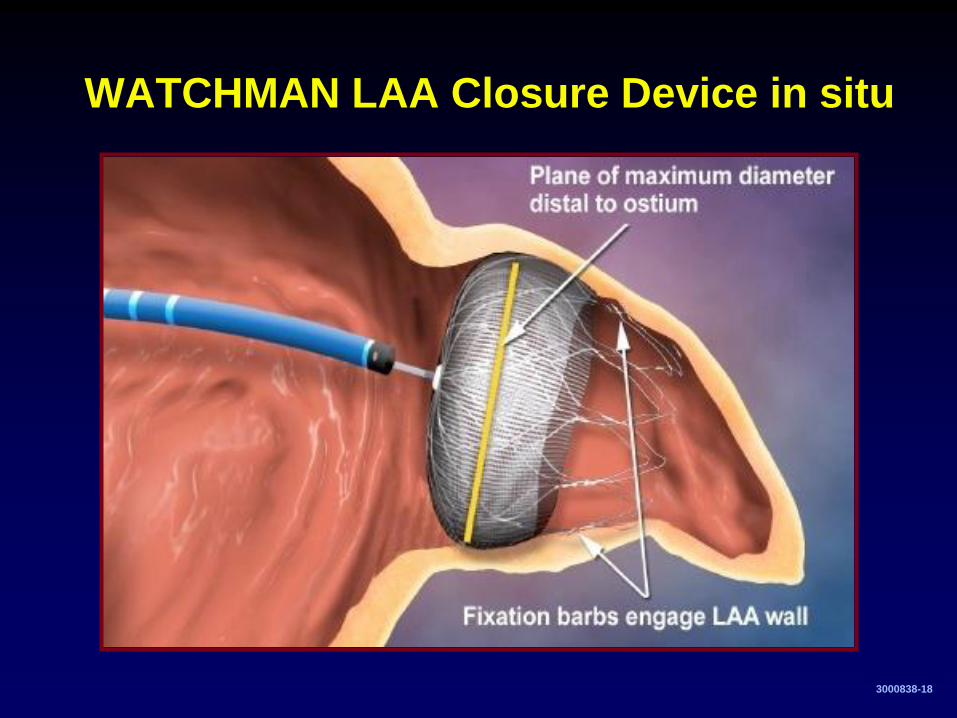
WATCHMAN LAA Closure Device in situ
3000838-18
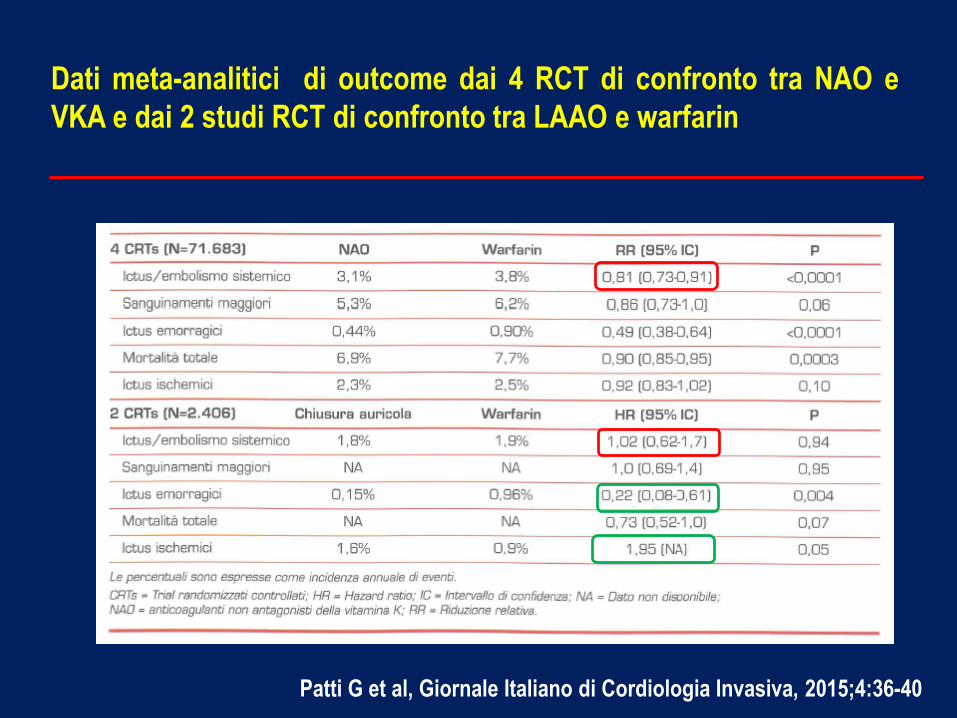
Dati meta-analitici di outcome dai 4 RCT di confronto tra NAO e
VKA e dai 2 studi RCT di confronto tra LAAO e warfarin
Patti G et al, Giornale Italiano di Cordiologia Invasiva, 2015;4:36-40
Left Atrial Appendage Occlusion vs NOACs
Ongoing Studies
▪ LAA Closure vs Novel Anticoagulation Agents in AF
(PRAGUE 17): apixaban vs Watchman; estimated enrollment 400 pts
▪ Evaluation of Watchman LAAO Device in Patients with
AF versus Rivaroxaban : estimated enrollment 200 pts
▪ Safety and Efficay of LAA Closure vs Antithrombotic
Treatment in Patients with AF Undergoing DES
Implantation due to Complex CAD: dabigatran plus
aspirin/clopidogrel vs ACP; estimated enrollment 300 pts

NOACs : Future Perspectives
New Frontiers
NOACs vs LAAO▪
HF with SR▪
TAVI▪
ESUS▪
Cardiopatia ischemica cronica▪
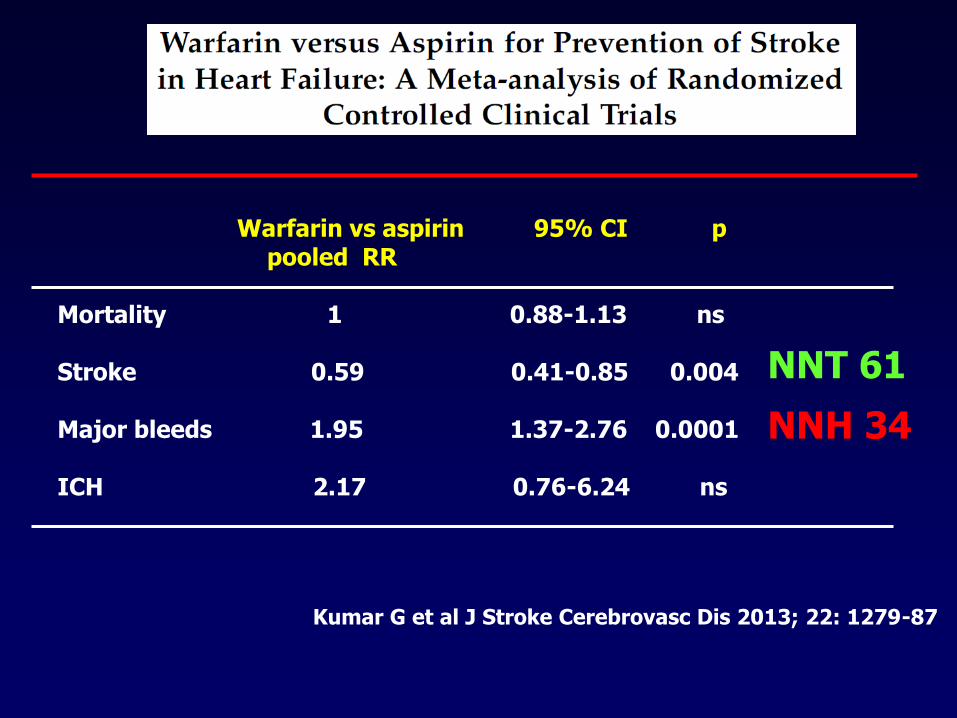
Kumar G et al J Stroke Cerebrovasc Dis 2013; 22: 1279-87
Warfarin vs aspirin 95% CI p pooled RR
Mortality 1 0.88-1.13 ns
Stroke 0.59 0.41-0.85 0.004
Major bleeds 1.95 1.37-2.76 0.0001
ICH 2.17 0.76-6.24 ns
NNT 61
NNH 34
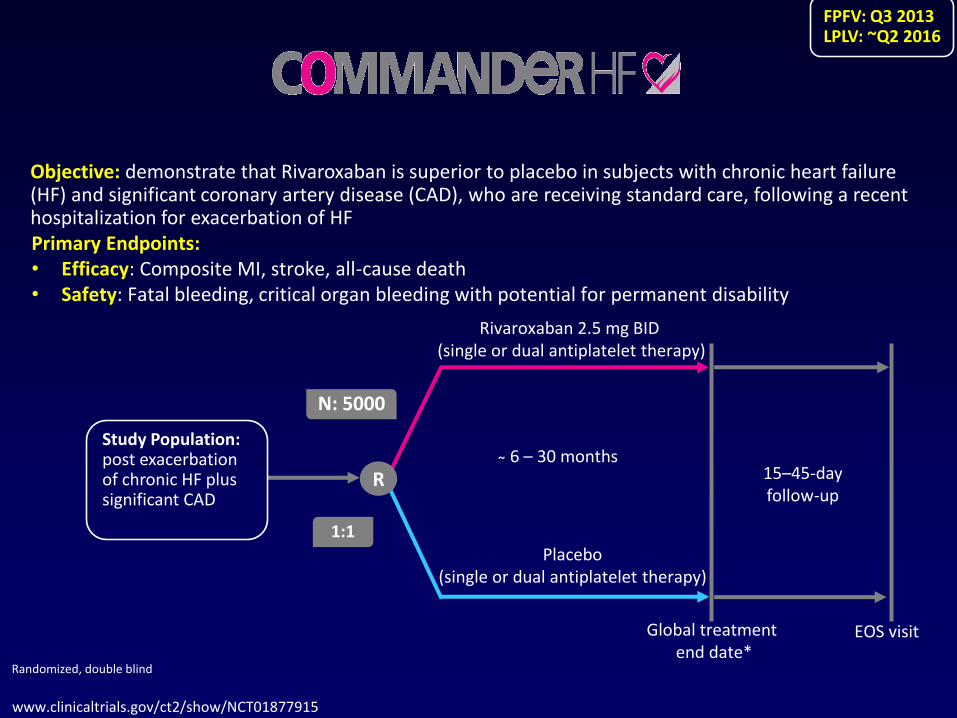
www.clinicaltrials.gov/ct2/show/NCT01877915
Objective: demonstrate that Rivaroxaban is superior to placebo in subjects with chronic heart failure (HF) and significant coronary artery disease (CAD), who are receiving standard care, following a recent hospitalization for exacerbation of HF
15–45-day follow-up
Rivaroxaban 2.5 mg BID(single or dual antiplatelet therapy)
Placebo (single or dual antiplatelet therapy)
N: 5000
R
Global treatment end date*
EOS visit
1:1
Randomized, double blind
Primary Endpoints:Efficacy• : Composite MI, stroke, all-cause deathSafety• : Fatal bleeding, critical organ bleeding with potential for permanent disability
Study Population:post exacerbation of chronic HF plus significant CAD
6 – 30 months
FPFV: Q3 2013LPLV: ~Q2 2016
NOACs : Future Perspectives
New Frontiers
▪ NOACs vs LAAO
▪ HF with SR
▪ TAVI
▪ ESUS
▪ Cardiopatia ischemica cronica
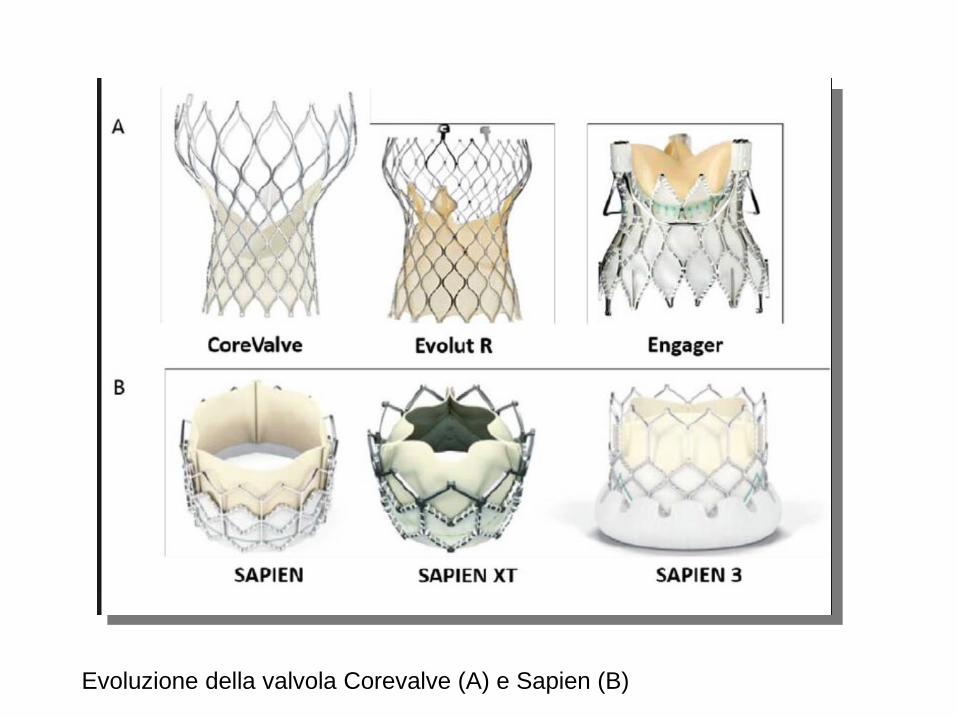
Evoluzione della valvola Corevalve (A) e Sapien (B)
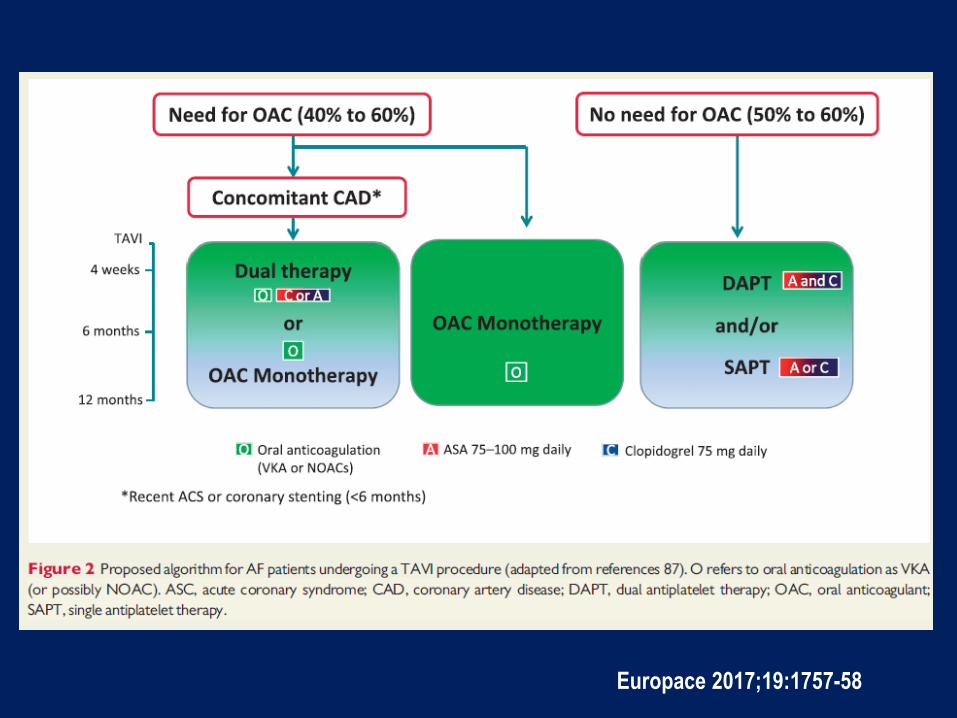
Europace 2017;19:1757-58
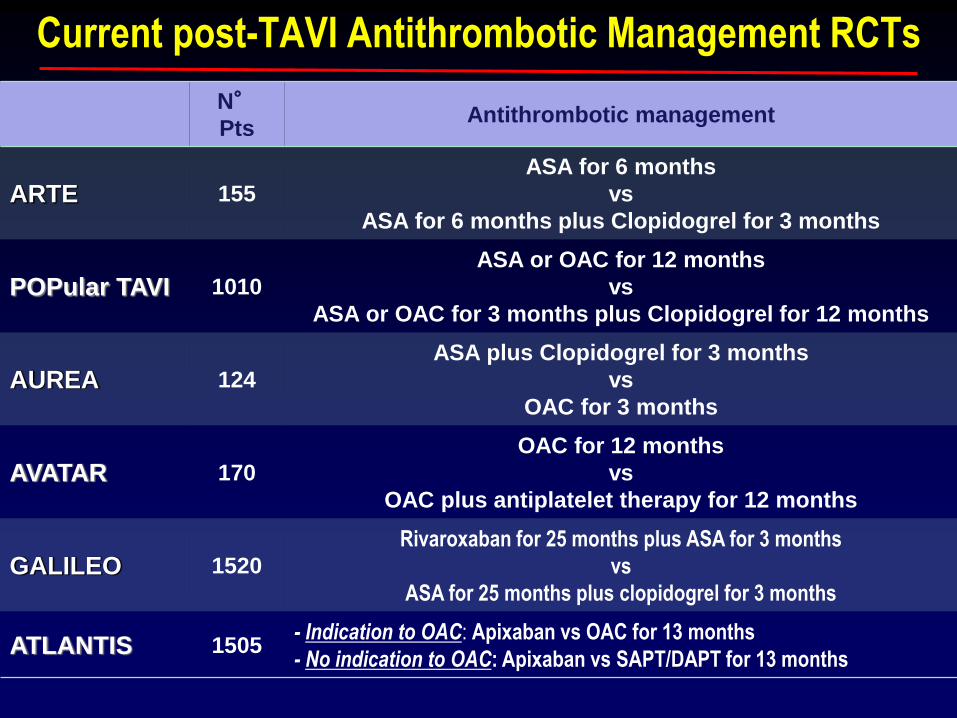
Current post-TAVI Antithrombotic Management RCTs
N°Pts
Antithrombotic management
ARTE 155
ASA for 6 months
vs
ASA for 6 months plus Clopidogrel for 3 months
POPular TAVI 1010
ASA or OAC for 12 months
vs
ASA or OAC for 3 months plus Clopidogrel for 12 months
AUREA 124
ASA plus Clopidogrel for 3 months
vs
OAC for 3 months
AVATAR 170
OAC for 12 months
vs
OAC plus antiplatelet therapy for 12 months
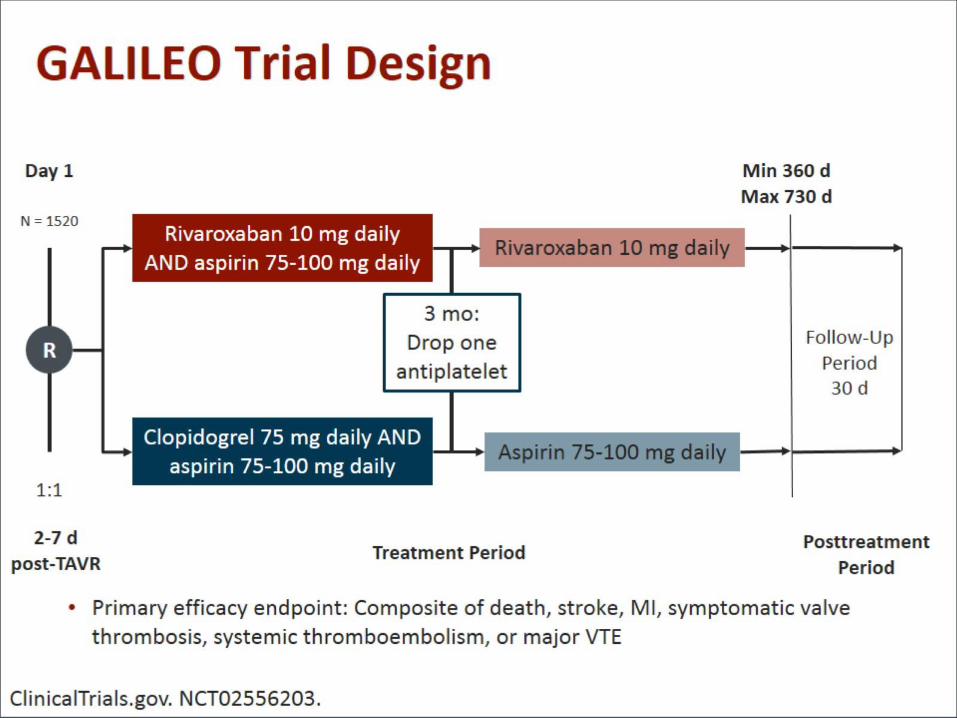
GALILEO 1520
Rivaroxaban for 25 months plus ASA for 3 months
vs
ASA for 25 months plus clopidogrel for 3 months
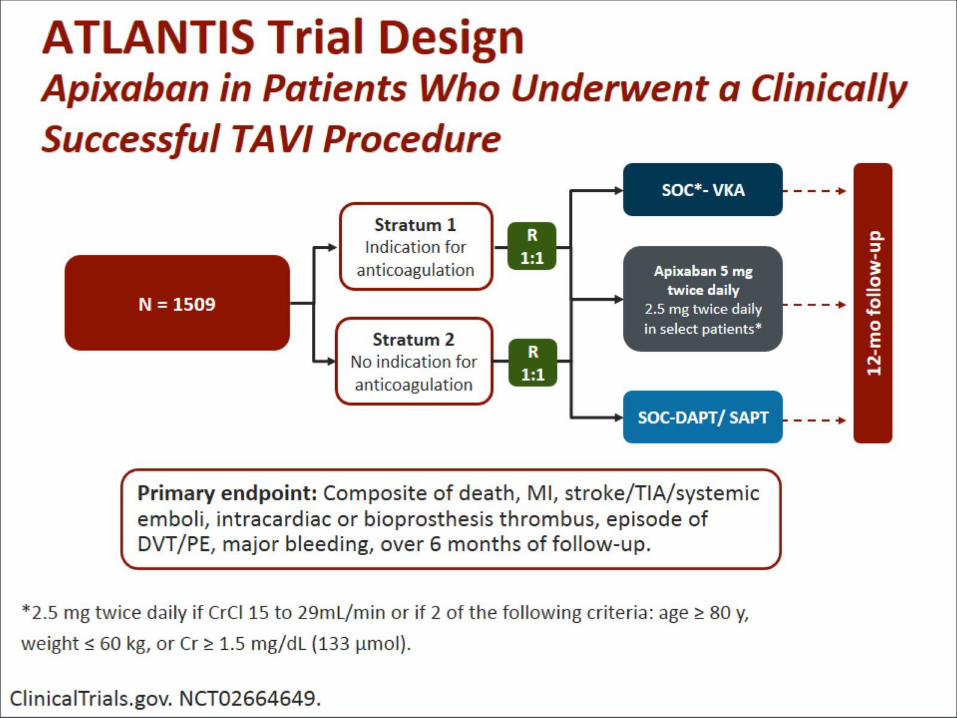
ATLANTIS 1505- Indication to OAC: Apixaban vs OAC for 13 months
- No indication to OAC: Apixaban vs SAPT/DAPT for 13 months
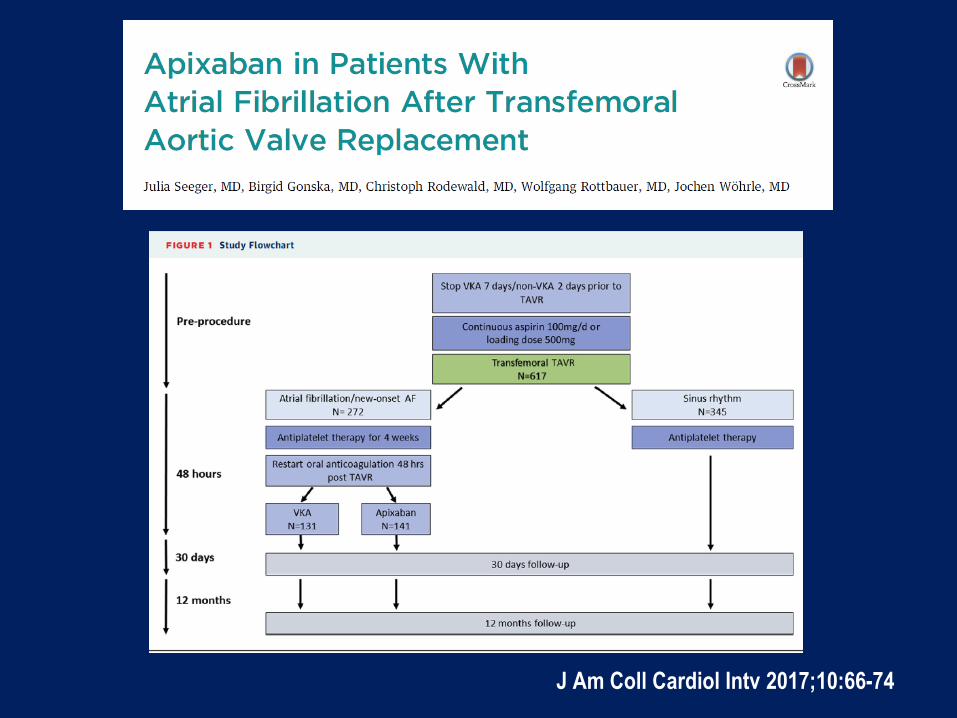
J Am Coll Cardiol Intv 2017;10:66-74
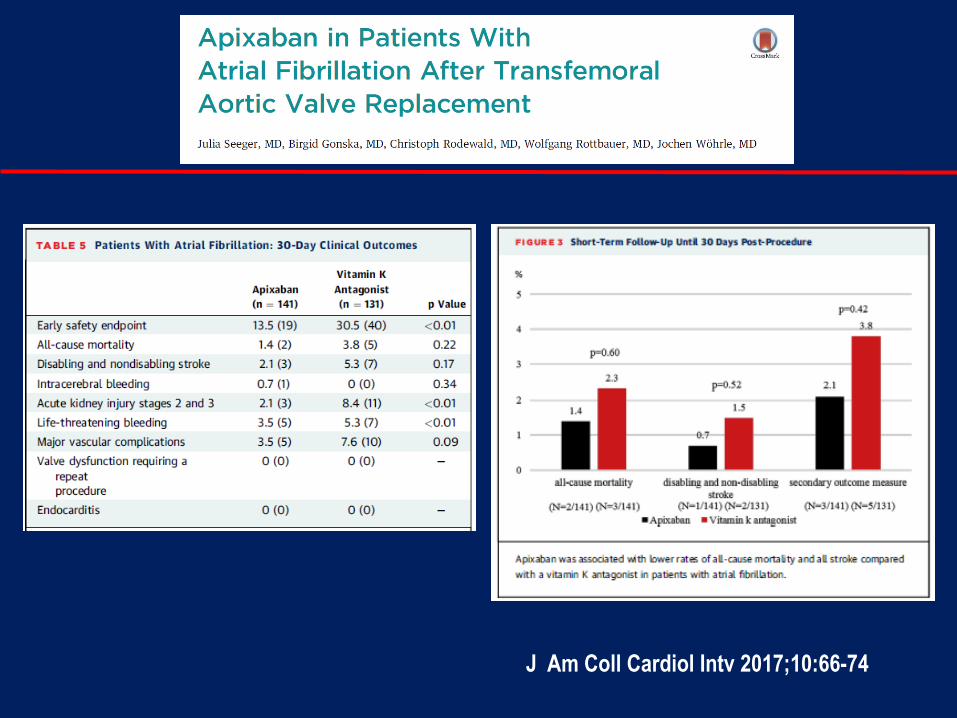
J Am Coll Cardiol Intv 2017;10:66-74
Windecker S. et al. Am Heart J 2017;184:81-7
NOACs : Future Perspectives
New Frontiers
▪ NOACs vs LAAO
▪ HF with SR
▪ TAVI
▪ ESUS
▪ Cardiopatia ischemica cronica
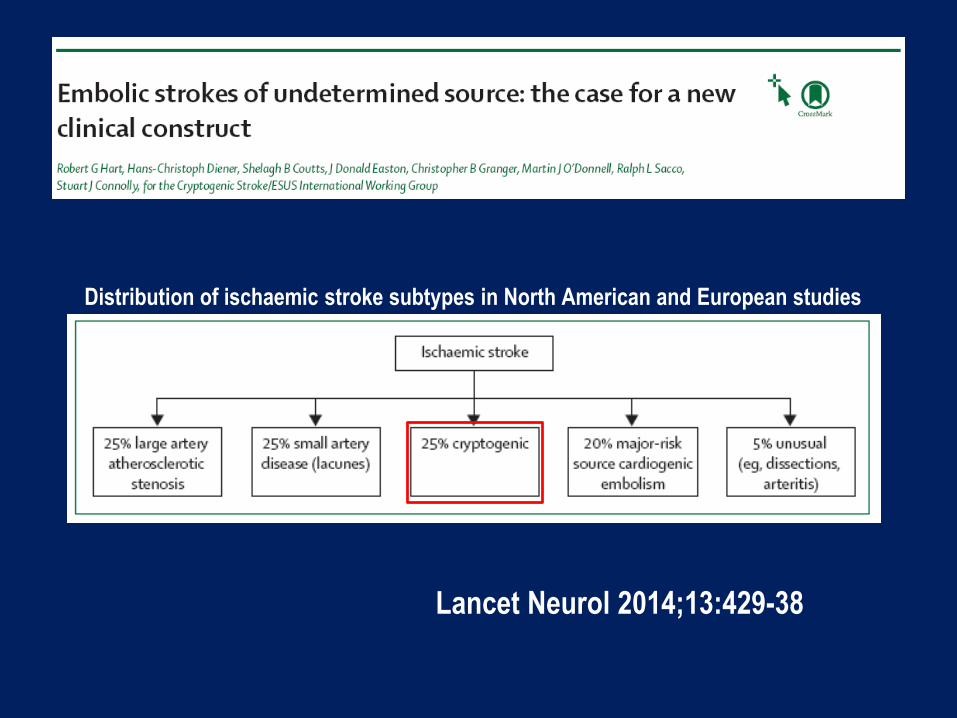
Lancet Neurol 2014;13:429-38
Distribution of ischaemic stroke subtypes in North American and European studies
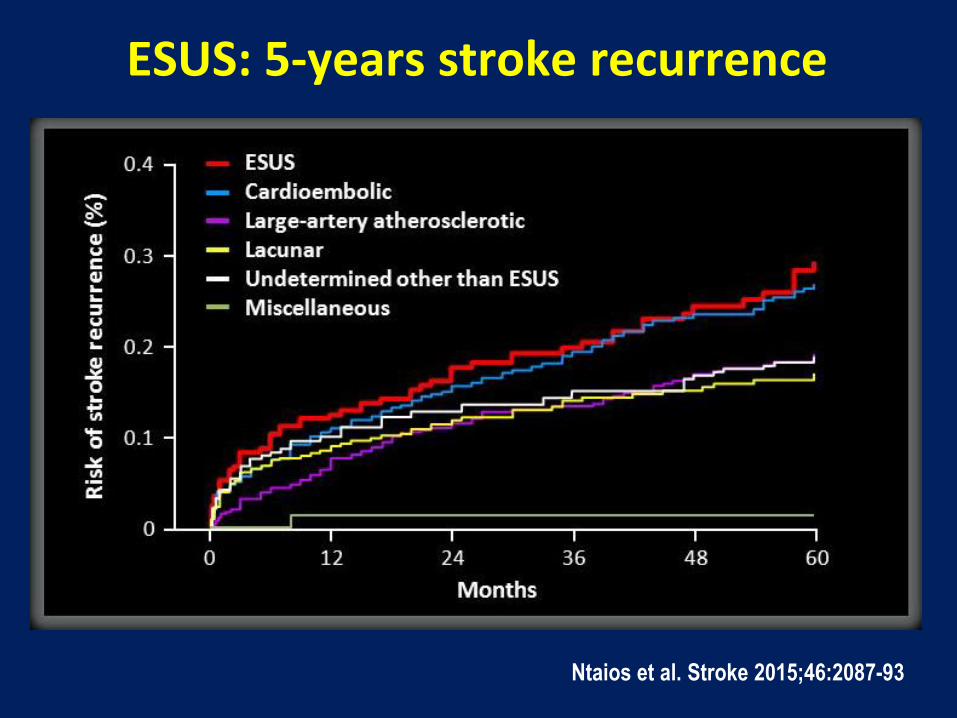
Ntaios et al. Stroke 2015;46:2087-93
ESUS: 5-years stroke recurrence
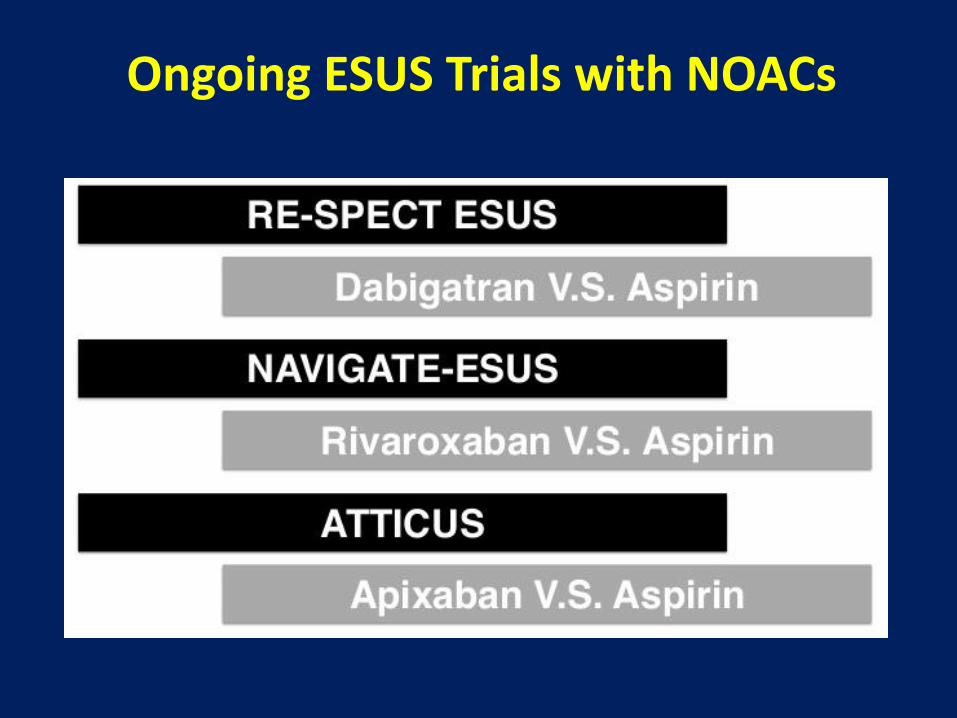
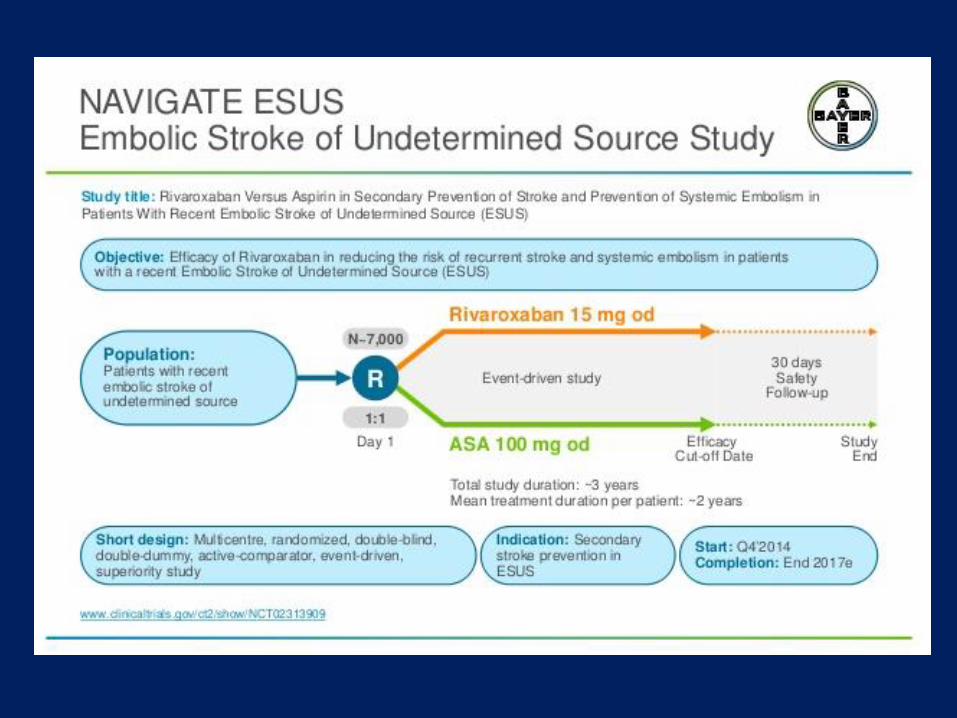
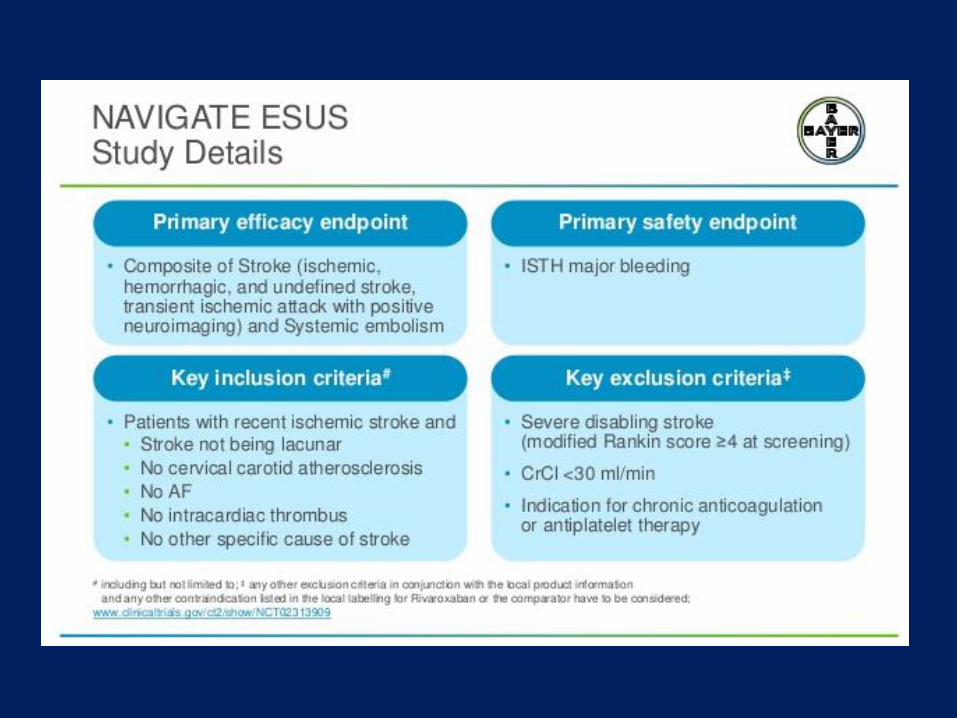
Ongoing ESUS Trials with NOACs
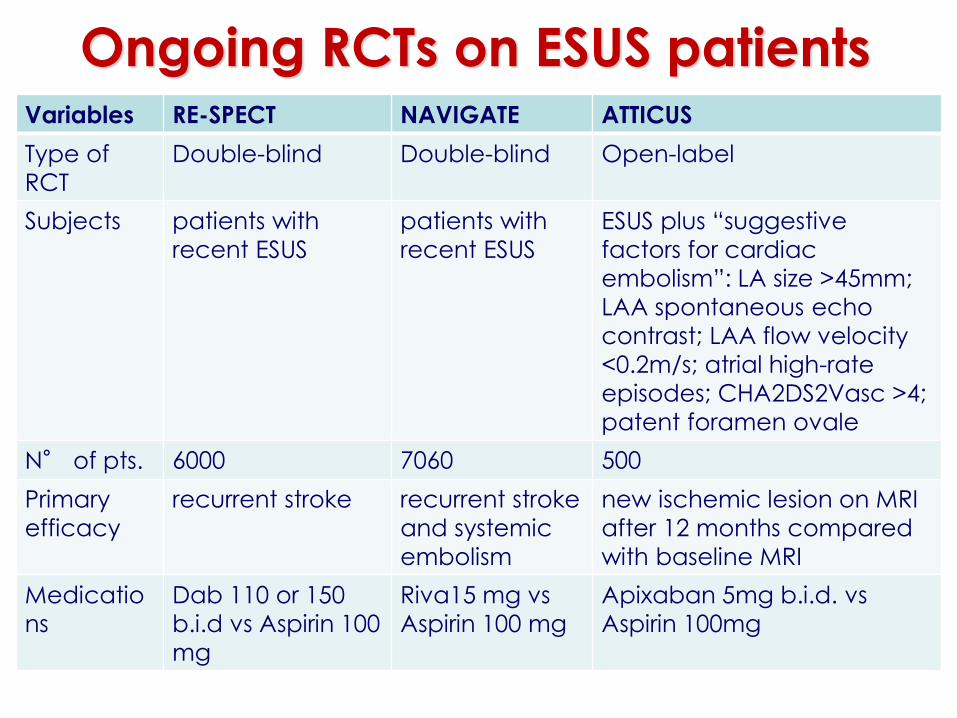
Ongoing RCTs on ESUS patients Variables RE-SPECT NAVIGATE ATTICUS
Type of
RCT
Double-blind Double-blind Open-label
Subjects patients with
recent ESUS
patients with
recent ESUS
ESUS plus “suggestive
factors for cardiac
embolism”: LA size >45mm;
LAA spontaneous echo
contrast; LAA flow velocity
<0.2m/s; atrial high-rate
episodes; CHA2DS2Vasc >4;
patent foramen ovale
N° of pts. 6000 7060 500
Primary
efficacy
recurrent stroke recurrent stroke
and systemic
embolism
new ischemic lesion on MRI
after 12 months compared
with baseline MRI
Medicatio
ns
Dab 110 or 150
b.i.d vs Aspirin 100
mg
Riva15 mg vs
Aspirin 100 mg
Apixaban 5mg b.i.d. vs
Aspirin 100mg
This decision is based on the recommendation of the study’s
Independent Data Monitoring Committee (IDMC) as the trial
showed comparable efficacy between rivaroxaban and the
standard of care, aspirin, and little chance of rivaroxaban
showing an overall benefit versus aspirin if the study were to
be completed. While bleeding rates were very low overall and
within the expected range, an increase in bleeding was
observed in the rivaroxaban arm compared to aspirin.
NOACs : Future Perspectives
New Frontiers
▪ NOACs vs LAAO
▪ HF with SR
▪ TAVI
▪ ESUS
▪ Cardiopatia ischemica cronica
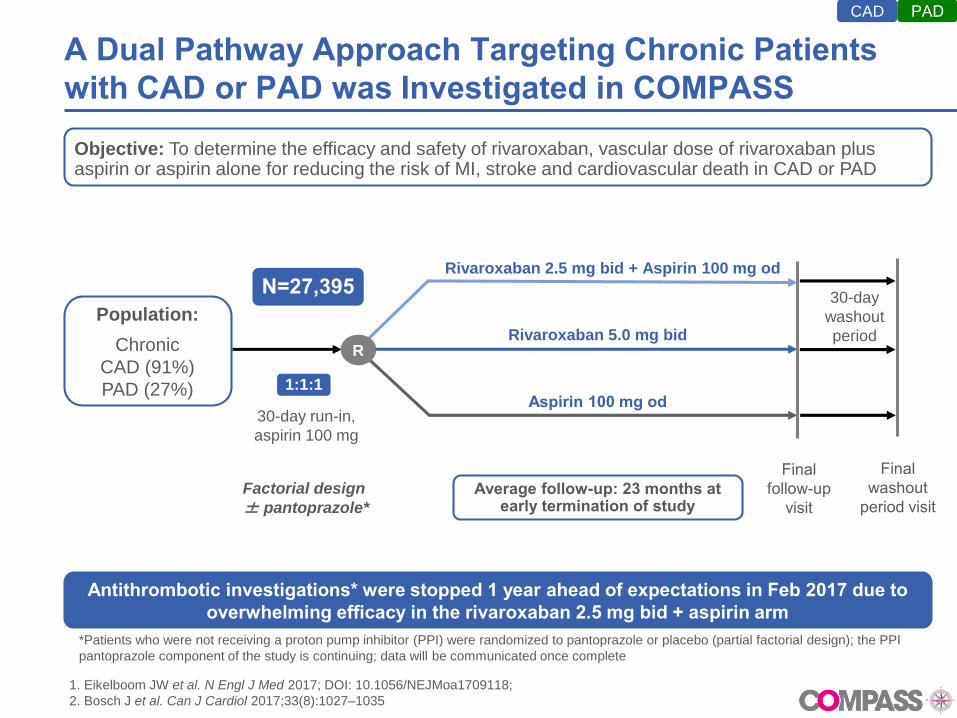
A Dual Pathway Approach Targeting Chronic Patients
with CAD or PAD was Investigated in COMPASS
Objective: To determine the efficacy and safety of rivaroxaban, vascular dose of rivaroxaban plus aspirin or aspirin alone for reducing the risk of MI, stroke and cardiovascular death in CAD or PAD
Antithrombotic investigations* were stopped 1 year ahead of expectations in Feb 2017 due to
overwhelming efficacy in the rivaroxaban 2.5 mg bid + aspirin arm
Rivaroxaban 5.0 mg bid
Aspirin 100 mg od
Rivaroxaban 2.5 mg bid + Aspirin 100 mg od
30-day
washout
period
30-day run-in,
aspirin 100 mg
Final
follow-up
visit
R
Final
washout
period visit
1:1:1
N=27,395
Population:
Chronic
CAD (91%)
PAD (27%)
*Patients who were not receiving a proton pump inhibitor (PPI) were randomized to pantoprazole or placebo (partial factorial design); the PPI
pantoprazole component of the study is continuing; data will be communicated once complete
1. Eikelboom JW et al. N Engl J Med 2017; DOI: 10.1056/NEJMoa1709118;
2. Bosch J et al. Can J Cardiol 2017;33(8):1027–1035
Average follow-up: 23 months at early termination of study
Factorial design
± pantoprazole*
PADCAD
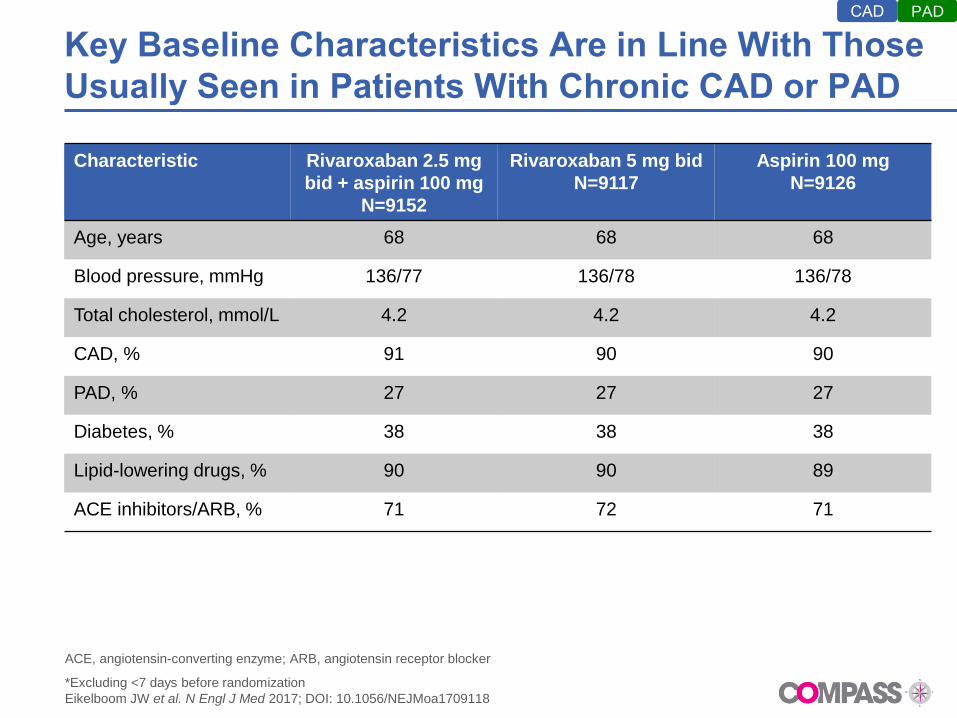
Key Baseline Characteristics Are in Line With Those
Usually Seen in Patients With Chronic CAD or PAD
Characteristic Rivaroxaban 2.5 mg
bid + aspirin 100 mg
N=9152
Rivaroxaban 5 mg bid
N=9117
Aspirin 100 mg
N=9126
Age, years 68 68 68
Blood pressure, mmHg 136/77 136/78 136/78
Total cholesterol, mmol/L 4.2 4.2 4.2
CAD, % 91 90 90
PAD, % 27 27 27
Diabetes, % 38 38 38
Lipid-lowering drugs, % 90 90 89
ACE inhibitors/ARB, % 71 72 71
ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker
*Excluding <7 days before randomization
Eikelboom JW et al. N Engl J Med 2017; DOI: 10.1056/NEJMoa1709118
PADCAD
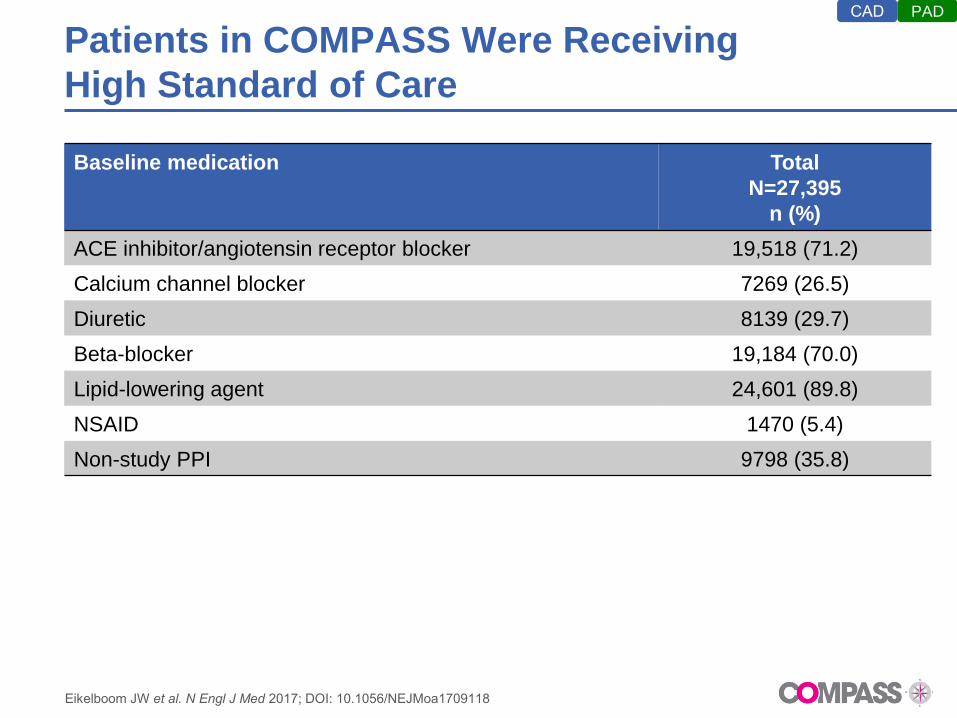
Patients in COMPASS Were Receiving
High Standard of Care
Baseline medication Total
N=27,395
n (%)
ACE inhibitor/angiotensin receptor blocker 19,518 (71.2)
Calcium channel blocker 7269 (26.5)
Diuretic 8139 (29.7)
Beta-blocker 19,184 (70.0)
Lipid-lowering agent 24,601 (89.8)
NSAID 1470 (5.4)
Non-study PPI 9798 (35.8)
Eikelboom JW et al. N Engl J Med 2017; DOI: 10.1056/NEJMoa1709118
PADCAD
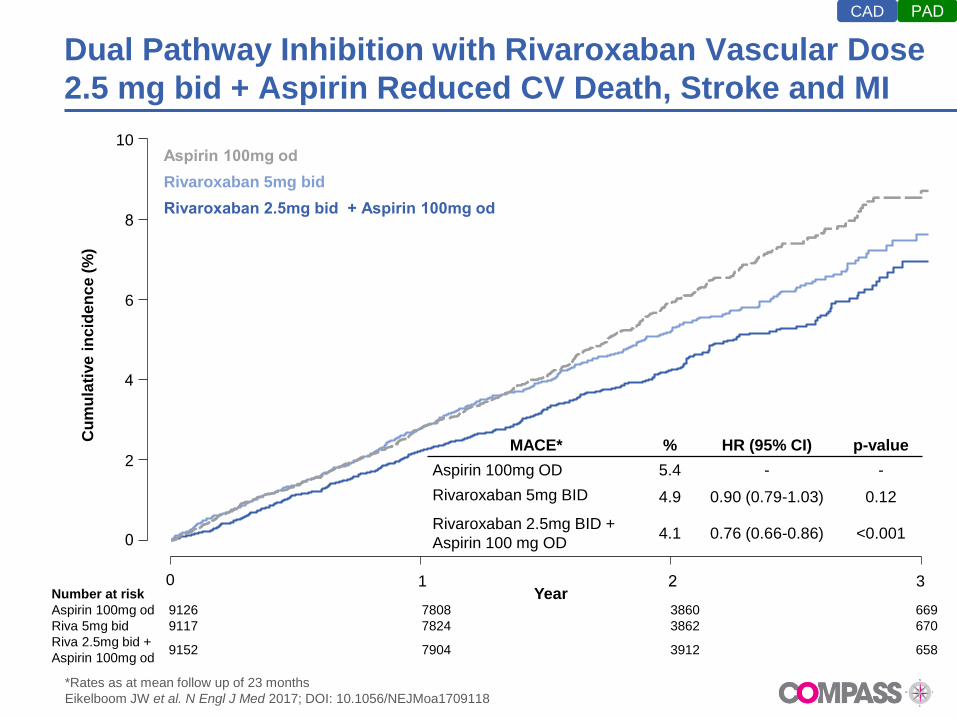
Dual Pathway Inhibition with Rivaroxaban Vascular Dose
2.5 mg bid + Aspirin Reduced CV Death, Stroke and MI
*Rates as at mean follow up of 23 months
Eikelboom JW et al. N Engl J Med 2017; DOI: 10.1056/NEJMoa1709118
MACE* % HR (95% CI) p-value
Aspirin 100mg OD 5.4 - -
Rivaroxaban 5mg BID 4.9 0.90 (0.79-1.03) 0.12
Rivaroxaban 2.5mg BID +
Aspirin 100 mg OD4.1 0.76 (0.66-0.86) <0.001
Cu
mu
lati
ve
in
cid
en
ce
(%
)
0
2
4
6
8
10
0 1 2 3
Rivaroxaban 2.5mg bid + Aspirin 100mg od
Rivaroxaban 5mg bid
Aspirin 100mg od
Number at risk
Aspirin 100mg od 9126 7808 3860 669
Riva 5mg bid 9117 7824 3862 670
Riva 2.5mg bid +
Aspirin 100mg od9152 7904 3912 658
Year
PADCAD
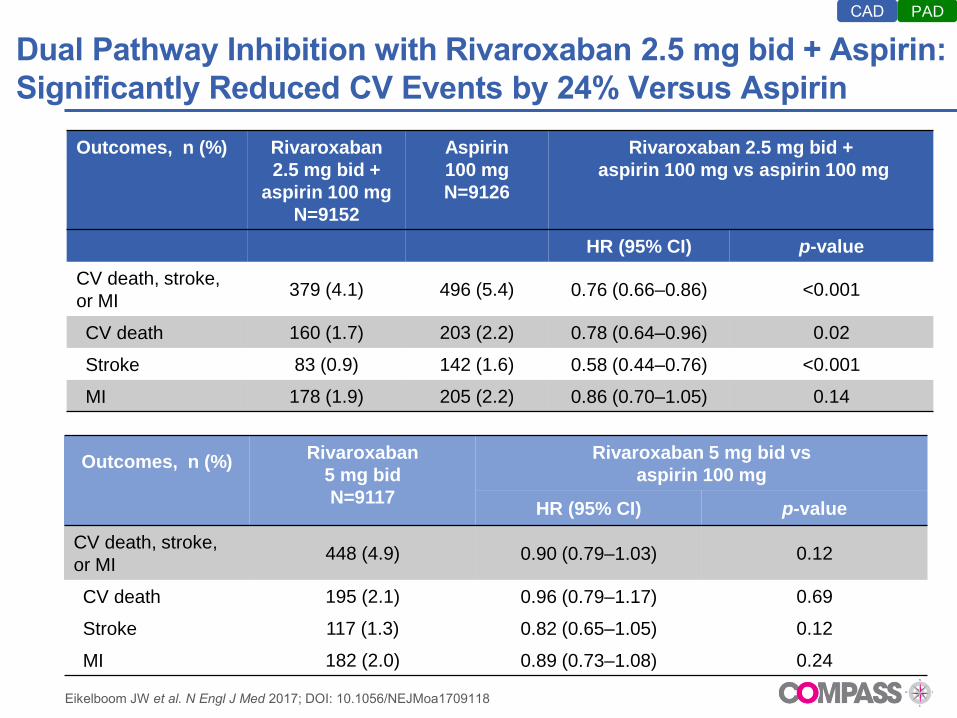
Dual Pathway Inhibition with Rivaroxaban 2.5 mg bid + Aspirin:
Significantly Reduced CV Events by 24% Versus Aspirin
Outcomes, n (%) Rivaroxaban
2.5 mg bid +
aspirin 100 mg
N=9152
Aspirin
100 mg
N=9126
Rivaroxaban 2.5 mg bid +
aspirin 100 mg vs aspirin 100 mg
HR (95% CI) p-value
CV death, stroke,
or MI379 (4.1) 496 (5.4) 0.76 (0.66–0.86) <0.001
CV death 160 (1.7) 203 (2.2) 0.78 (0.64–0.96) 0.02
Stroke 83 (0.9) 142 (1.6) 0.58 (0.44–0.76) <0.001
MI 178 (1.9) 205 (2.2) 0.86 (0.70–1.05) 0.14
Outcomes, n (%)Rivaroxaban
5 mg bid
N=9117
Rivaroxaban 5 mg bid vs
aspirin 100 mg
HR (95% CI) p-value
CV death, stroke,
or MI448 (4.9) 0.90 (0.79–1.03) 0.12
CV death 195 (2.1) 0.96 (0.79–1.17) 0.69
Stroke 117 (1.3) 0.82 (0.65–1.05) 0.12
MI 182 (2.0) 0.89 (0.73–1.08) 0.24
Eikelboom JW et al. N Engl J Med 2017; DOI: 10.1056/NEJMoa1709118
PADCAD
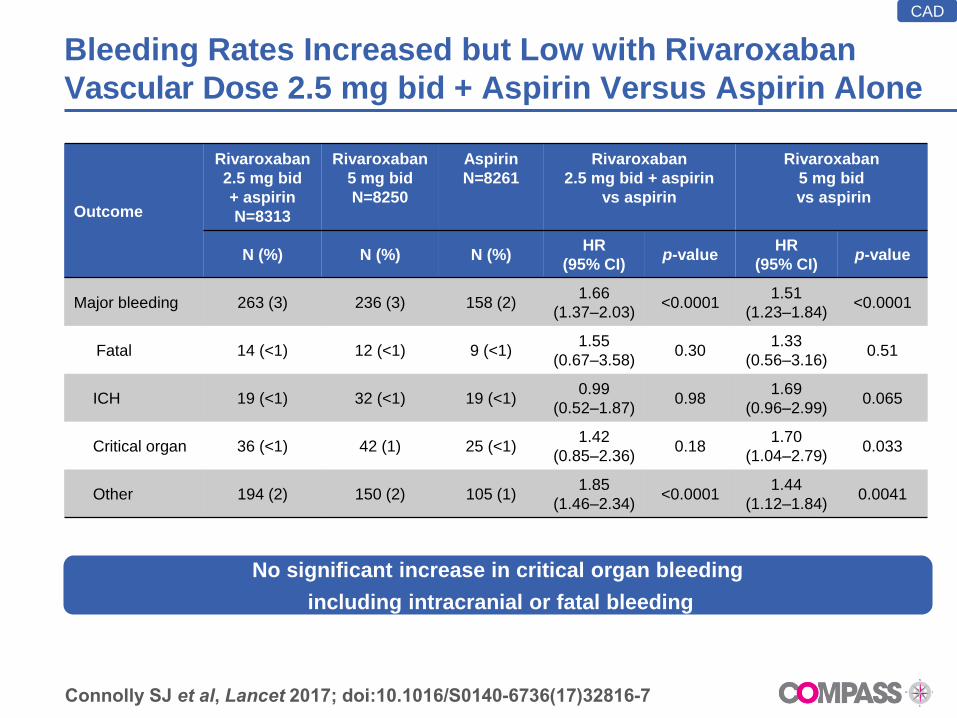
Bleeding Rates Increased but Low with Rivaroxaban
Vascular Dose 2.5 mg bid + Aspirin Versus Aspirin Alone
Outcome
Rivaroxaban
2.5 mg bid
+ aspirin
N=8313
Rivaroxaban
5 mg bid
N=8250
Aspirin
N=8261
Rivaroxaban
2.5 mg bid + aspirin
vs aspirin
Rivaroxaban
5 mg bid
vs aspirin
N (%) N (%) N (%)HR
(95% CI)p-value
HR
(95% CI)p-value
Major bleeding 263 (3) 236 (3) 158 (2)1.66
(1.37–2.03)<0.0001
1.51
(1.23–1.84)<0.0001
Fatal 14 (<1) 12 (<1) 9 (<1)1.55
(0.67–3.58)0.30
1.33
(0.56–3.16)0.51
ICH 19 (<1) 32 (<1) 19 (<1)0.99
(0.52–1.87)0.98
1.69
(0.96–2.99)0.065
Critical organ 36 (<1) 42 (1) 25 (<1)1.42
(0.85–2.36)0.18
1.70
(1.04–2.79)0.033
Other 194 (2) 150 (2) 105 (1)1.85
(1.46–2.34)<0.0001
1.44
(1.12–1.84)0.0041
Connolly SJ et al, Lancet 2017; doi:10.1016/S0140-6736(17)32816-7
CAD
No significant increase in critical organ bleeding
including intracranial or fatal bleeding
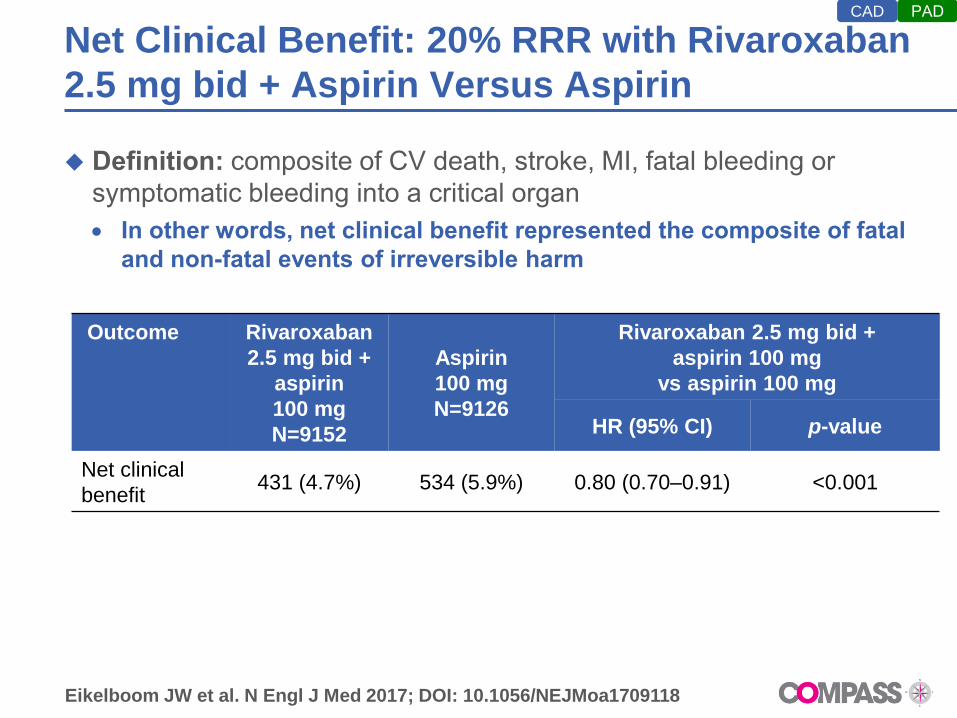
Net Clinical Benefit: 20% RRR with Rivaroxaban
2.5 mg bid + Aspirin Versus Aspirin
Definition: composite of CV death, stroke, MI, fatal bleeding or
symptomatic bleeding into a critical organ
In other words, net clinical benefit represented the composite of fatal •
and non-fatal events of irreversible harm
Outcome Rivaroxaban
2.5 mg bid +
aspirin
100 mg
N=9152
Aspirin
100 mg
N=9126
Rivaroxaban 2.5 mg bid +
aspirin 100 mg
vs aspirin 100 mg
HR (95% CI) p-value
Net clinical
benefit431 (4.7%) 534 (5.9%) 0.80 (0.70–0.91) <0.001
Eikelboom JW et al. N Engl J Med 2017; DOI: 10.1056/NEJMoa1709118
PADCAD