Embed Size (px)
Citation preview

Vascular Anomalies Classification:Recommendations From theInternational Society for the Study ofVascular AnomaliesMichel Wassef, MDa, Francine Blei, MDb, Denise Adams, MDc, Ahmad Alomari, MDd, Eulalia Baselga, MDe,Alejandro Berenstein, MDf, Patricia Burrows, MDg, Ilona J. Frieden, MDh, Maria C. Garzon, MDi,Juan-Carlos Lopez-Gutierrez, MD, PhDj, David J.E. Lord, MDk, Sally Mitchel, MDl, Julie Powell, MDm, Julie Prendiville, MDn,Miikka Vikkula, MD, PhDo, on behalf of the ISSVA Board and Scientific Committee
abstractVascular anomalies represent a spectrum of disorders from a simple “birthmark”to life- threatening entities. Incorrect nomenclature and misdiagnoses arecommonly experienced by patients with these anomalies. Accurate diagnosis iscrucial for appropriate evaluation and management, often requiringmultidisciplinary specialists. Classification schemes provide a consistentterminology and serve as a guide for pathologists, clinicians, and researchers.One of the goals of the International Society for the Study of Vascular Anomalies(ISSVA) is to achieve a uniform classification. The last classification (1997)stratified vascular lesions into vascular malformations and proliferative vascularlesions (tumors). However, additional disease entities have since been identifiedthat are complex and less easily classified by generic headings, such as capillarymalformation, venous malformation, lymphatic malformation, etc. We herebypresent the updated official ISSVA classification of vascular anomalies. Thegeneral biological scheme of the classification is retained. The section on tumorshas been expanded and lists the main recognized vascular tumors, classified asbenign, locally aggressive or borderline, and malignant. A list of well-defineddiseases is included under each generic heading in the “Simple VascularMalformations” section. A short definition is added for eponyms. Two newsections were created: one dealing with the malformations of individually namedvessels (previously referred to as “truncular” malformations); the second groupslesions of uncertain or debated nature (tumor versus malformation). The knowngenetic defects underlying vascular anomalies are included in an appendix. Thisclassification is meant to be a framework, acknowledging that it will requiremodification as new scientific information becomes available.
Vascular anomalies (vascular tumors
and vascular malformations), often
named “angioma” or hemangioma, in
fact represent a broad spectrum of
disorders from a simple “birthmark” to
life-threatening entities, which affect
mainly infants, children, and young
adults. Certain vascular anomalies,
such as salmon patch (nevus simplex)
or infantile hemangioma, are very
common. Others such as port wine
stain are uncommon, and still others
are quite rare. Despite long-standing
efforts to promulgate standard
classification, nomenclature
terminology of vascular anomalies
continues to be confusing.1–4 The term
“hemangioma” is, for example,
commonly used to name different
types of vascular tumors as well as
aAssistance Publique–Hopitaux de Paris, LariboisièreHospital, Department of Pathology, Paris Diderot University,Paris, France; bVascular Birthmark Program, Lenox HillHospital of North Shore Long Island Jewish HealthcareSystem, New York, New York; cCincinnati Children’s HospitalMedical Center, Cancer and Blood Disease Institute, Universityof Cincinnati, Cincinnati, Ohio; dDepartment of Radiology,Boston Children’s Hospital and Harvard Medical School,Boston, Massachusetts; ePediatric Dermatology, Hospital dela Santa Creu i Sant Pau, Barcelona, Spain; fMt SinaiHealthcare System, Ichan School of Medicine, New York, NewYork; gDepartment of Radiology, Medical College of Wisconsin,Milwaukee, Wisconsin; hDepartment of Dermatology,University of California, San Francisco, San Francisco,California; iDepartment of Dermatology, Columbia University,New York, New York; jLa Paz Children´s Hospital, Madrid,Spain; kInterventional Radiology, Sydney Children’s HospitalsNetwork, Sydney, Australia; lDepartments of Radiology,Surgery, and Pediatrics, The Johns Hopkins Hospital,Baltimore, Maryland; mDivision of Dermatology (Pediatrics),Centre Hospithalier Universitaire Sainte-Justine, University ofMontreal, Montreal, Canada; nPediatric Dermatology,University of British Columbia, Vancouver, Canada; andoLaboratory of Human Molecular Genetics, Christian de DuveInstitute of Cellular Pathology, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain, Brussels, Belgium
Dr Wassef conceptualized and designed theclassification and drafted the initial manuscript; DrBlei, as chair of the scientific committee of theInternational Society for the Study of VascularAnomalies, led the initiative for the updatedclassification and spearheaded the project andcritically reviewed and revised the manuscript; DrsAdams, Baselga, Burrows, Frieden, Garzon, Lord, andPrendiville participated in the design of theclassification and critically reviewed and revised themanuscript; Dr Alomari participated in the design ofthe classification; Drs Berenstein, Lopez-Gutierrez,and Vikkula participated in the design of theclassification and critically reviewed themanuscript; Drs Mitchel and Powell criticallyreviewed and revised the manuscript; and allauthors approved the final manuscript assubmitted.
PEDIATRICS Volume 136, number 1, July 2015 SPECIAL ARTICLE by guest on April 12, 2020www.aappublications.org/newsDownloaded from

vascular malformations, despite thedifferent constitution, naturalevolution, and treatment of these 2groups of lesions. Incorrectnomenclature and misdiagnoses arecommonly experienced by patientswith vascular anomalies.2 Accuratediagnosis and common terminologyare crucial for appropriate evaluationand management, often requiringmultidisciplinary specialists.
One of the goals of the InternationalSociety for the Study of VascularAnomalies (ISSVA) is to achievea uniform classification. The 1996ISSVA classification stratified vascularanomalies into vascularmalformations and proliferativevascular lesions (tumors) (Table 1).5,6
This classification was then“unofficially” updated on the basis ofevolving knowledge a decade later.7
However, since then, knowledgeabout these disorders has increasedconsiderably. The genetic basis ofmany types of vascularmalformations has been elucidatedand additional disease entities havebeen identified that need moreprecise classification rather thangeneric headings such as capillarymalformation (CM), venousmalformation (VM), lymphaticmalformation (LM), etc, which havebeen used previously. The ISSVAClassification of Vascular Anomalieswas recently updated by the Society’sScientific Committee and Board toincorporate these changes and wasadopted at the last workshop in
Melbourne, Australia (April 2014).The goal of this article is to brieflydiscuss some of the presentclassifications and to introduce the2014 updated ISSVA classification. Theinteractive document is available atwww.issva.org. This classification ismeant to represent the state-of-the-artin vascular anomalies classification,acknowledging that it will requiremodification as new scientificinformation becomes available.
Several classifications of vascularanomalies are available; some aregeneral classifications, and others dealwith specific organs or tissues or onlywith vascular tumors or vascularmalformations. The earliestclassification was that of Virchow,which was a pathologic classificationthat classified vascular anomalies as“angioma simplex, angiomacavernosum, angioma racemosum andlymphangioma.”8–10 This wasa primitive classification system butappropriate for the time. The WorldHealth Organization (WHO)classifications are generallyconsidered as the referenceclassification for tumors and tumorlikediseases. The WHO classification ofskin vascular “tumors”11 isa nonhierarchical list of a series ofdifferent diseases, irrespective of theirtumor, malformation, reactive, orinfectious nature. The WHOclassification of soft tissue tumors12
uses the word “hemangioma” todescribe a tumor or a malformation,further confusing the terminology.13
These inconsistencies in classificationand nomenclature make the WHO
classifications misleading andconfusing.8–10 It is then difficult forclinicians across specialties tocommunicate using a commonlanguage specific for each entity, andconfusion in the naming of lesionscreates inaccuracies in scientificadvances and the dissemination ofknowledge that may help patients. Italso makes coding and statistical dataabout the prevalence and incidence ofthese lesions inaccurate.
The 1996 ISSVA classificationscheme5 is based on the fundamentalseparation of vascular anomalies into
TABLE 1 1996 ISSVA Classification Scheme
Vascular Anomalies
Vascular tumors Vascular Malformations
Simple Combined
Hemangioma Capillary AVF, AVMOthers Lymphatic CVM, CLM
Venous LVM, CLVMArterial CAVM
CLAVM
AVF, arteriovenous fistula; AVM, arteriovenous malformation;CAVM, capillary-arteriovenous malformation; CLAVM, capillary-lymphatic-arteriovenous malformation; CLM, capillary-lymphatic malformation; CLVM, capillary-lymphatic-venousmalformation; CVM, capillary-venous malformation; LVM,lymphatic-venous malformation.
TABLE 2 2014 ISSVA Classification of Vascular Anomalies
Vascular Anomalies
Vascular Tumors Vascular Malformations
Simple Combined Of Major NamedVessels
Associated With OtherAnomalies
Benign CM See Table 5 See text See Table 6Locally aggressive or
borderlineLMVM
Malignant AVMArteriovenous
fistula
TABLE 3 Classification of Vascular Tumors
Benign vascular tumorsInfantile hemangioma/hemangioma of infancyCongenital hemangiomaRapidly involuting CH (RICH)a
Noninvoluting CH (NICH)Partially involuting CH (PICH)
Tufted angiomaa,b
Spindle cell hemangiomaEpithelioid hemangiomaPyogenic granuloma (or lobular capillary
hemangioma)Others
Locally aggressive or borderline vascular tumorsKaposiform hemangioendotheliomaa,b
Retiform hemangioendotheliomaPapillary intralymphatic angioendothelioma,
Dabska tumorComposite hemangioendotheliomaKaposi sarcomaOthers
Malignant vascular tumorsAngiosarcomaEpithelioid hemangioendotheliomaOthers
Reactive proliferative vascular lesions are listed withbenign tumors.a Some lesions may be associated with thrombocytopeniaand/or consumptive coagulopathy.b Many experts believe that these are part of a spectrumrather than distinct entities.
e204 WASSEF et al by guest on April 12, 2020www.aappublications.org/newsDownloaded from

those lesions with a proliferativecomponent (named “vascular tumors”)versus relatively static “vascularmalformations,” following Mulliken andGlowacki’s14 seminal work. Vascularmalformations, which are due toinborn errors in vascularmorphogenesis, are further classifiedon the basis of the main type of vesselthey are composed of: capillary,venous, lymphatic, arterial, andcombined malformations (Table 1).Another proposed classificationschema, the Hamburg classification,uses vessel type as the basis ofclassification of vascularmalformations. In each class, “truncularmalformations” affecting (individual)large vessels and “extratruncularmalformations” composed of smallervessels intimately embedded in thehost tissue are recognized. Thisdistinction is clinically relevant,because “truncular” malformationsseems to behave differently, and aremore often associated with pulmonaryembolism when affecting veins andwith chylous effusion when affectinglymphatic vessels.15 However, thisdistinction was not considered in the1996 ISSVA classification.
Beginning in 2013, a group of ISSVAleaders from both the scientificcommittee and board, with mindfulconsideration given to the variousexisting classifications, sought to updateand improve the classification ofvascular anomalies, both to make itmore clinically relevant and flexible andto acknowledge new knowledgeincluding new genetic and histologicinformation available since its 1996classification was approved. Thisupdated consensus classification isintended to be applicable and functionalfor all medical and surgical specialtiesand for every organ or tissue.
THE 2014 UPDATED ISSVACLASSIFICATION
Because the updated classificationlists a large number of differentdiseases, it is presented as a generaltable (Table 2) containing the main
classes of vascular anomalies andwith reference to other tables. Theonline version of the classification,which is available on the ISSVA Website (www.issva.org), containshypertext links that facilitate thenavigation in the classification and itsappendices.
Vascular Tumors
A list of the main vascular tumorswas added in the section on tumors,divided into benign, locally aggressive
or borderline, and overtly malignant(Table 3). Reactive vascularproliferative lesions were groupedwith benign tumors. The distinctionbetween the reactive or tumor natureof a lesion is not alwaysstraightforward and is debated forseveral lesions (pyogenic granuloma/lobular capillary hemangioma,16
spindle cell hemangioma,17
epithelioid hemangioma18). Somerare vascular tumors are not includedin the table and are listed as “others,”
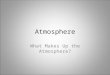
FIGURE 1Evolution scheme of untreated IH, RICH, and NICH. IH appears after birth, grows generally until theend of the first year of life, then stabilizes and gradually involutes most significantly during years 1to 2 and continues to improve over the ensuing years. CHs are fully grown at birth and rapidlyinvolute (RICH) or persist indefinitely (NICH). Reprinted with permission from Mulliken JB andEnjolras O.27 NICH, noninvoluting congenital hemangioma; RICH, rapidly involuting congenital hem-angioma. The Y axis show relative size.
FIGURE 2Infantile hemangioma. A, A large segmental lesion of the face in an infant. Such lesions may be part ofa PHACE syndrome. B, Involution of the lesion at age 24 months. C, Residual lesion at 10 years. D, IHendothelial cells express Glut-1, contrary to those of the normal artery (on the right side of the panel).
PEDIATRICS Volume 136, number 1, July 2015 e205 by guest on April 12, 2020www.aappublications.org/newsDownloaded from

because the number of such rarelesions is rapidly increasing andbecause they can be found in reviewarticles19–24 or in dermatology or softtissue textbooks.
Infantile hemangioma (IH; also namedhemangioma of infancy) is the mostcommon tumor of infancy with anincidence estimated between 4% and10% of all infants and children.25,26
IHs, which are more frequent infemales and in cervicofacial locations,appear within the first few weeks oflife as a solitary cutaneous lesion thatprogressively enlarges over monthsand then gradually regresses25–27
(Fig 1). IHs are subclassified as focal,multifocal, segmental, andindeterminate depending on theirmorphology, extent, or distribution(Fig 2)28 and as superficial, deep, andmixed depending on their location inthe skin and/or hypodermis.Segmental IHs may be associated withother vascular and nonvascularanomalies, especially in PHACE(posterior fossa anomaly,hemangioma, arterial anomalies,cardiovascular anomalies, eyeanomalies, sternal clefting and/orsupraumbilical raphe) and LUMBAR(lower body hemangioma, urogenitalanomalies, ulceration, myelopathy,bony deformities, anorectalmalformations, arterial anomalies, andrenal anomalies) syndromes.29–31 IHsare mainly composed of proliferatingendothelial cells and pericytes. Theseendothelial cells possess uniqueimmunohistochemical markers(glucose transporter 1 [Glut-1], LewisY antigen, FCg II receptor [FcgRII],and merosin),32,33 which are alsopresent on placental blood endothelialcells and other blood-tissue barriervessels (eg, brain, retina).
Congenital hemangiomas (CHs) areless common. They are present andare fully grown at birth. They oftenregress rapidly,27,34 before 1 year ofage, or can remain stable or partiallyinvolute (Fig 1). On the basis of thisnatural history, these 3 types arenamed, respectively, rapidly
FIGURE 3Rapidly involuting congenital hemangioma. A large bulky lesion on the scalp at birth (A) and at age 9months (B), without treatment.
FIGURE 4Noninvoluting congenital hemangioma. A, A plaque-like round lesion of the shoulder, with coarsecentral telangiectasia and blue peripheral halo. B, The tumor lobules are made of vessels of varioussize, with a virtual or an open lumen. Some lumina are large and stellate.
e206 WASSEF et al by guest on April 12, 2020www.aappublications.org/newsDownloaded from

involuting CH,27,35 noninvolutingCH,27,36 and partially involuting CH37
(Figs 3 and 4). They are composed ofcapillary lobules where endothelialcells do not express Glut-1 and areassociated with large extralobularveins, arteries, and lymphatics.Rapidly involuting CH may beassociated with transientthrombocytopenia and consumptioncoagulopathy.38 Other clinicallysignificant benign or locallyaggressive and borderline vasculartumors are tufted angiomas andkaposiform hemangioendotheliomas.
Tufted angiomas appear aserythematous or brown plaques or
macules (Fig 5) in children and youngadults.39 A few cases are present atbirth or are associated withhyperhidrosis or hypertrichosis.Some lesions regress spontaneously,especially in congenital cases. Tuftedangiomas are composed of small tuftsof capillaries, characteristicallysurrounded by a crescentic slitlikevessel, in the dermis and subcutis,with a cannon-ball distribution.Kaposiform hemangioendotheliomamay affect the skin and subcutis butoften involves the deep tissues,presenting as a locally aggressivetumor (Fig 6). It histologicallyresembles tufted angioma with larger
and confluent tumor lobules, witha more infiltrating pattern. Bothlesions focally express lymphaticendothelial markers (podoplanin,Prospero homeobox 1 [Prox-1])40 butdo not express Glut-1. Both tumorsmay be associated with the life-threatening Kasabach-Merrittphenomenon, characterized byprofound thrombocytopenia andconsumption of blood coagulationfactors.41–43 Many authors considertufted angioma and kaposiformhemangioendothelioma as part of
FIGURE 5Tufted angioma. A, Red vascular lesion with leathery quality on the arm of an infant. B, Histologically,the lesion is composed of small vascular tufts or lobules in a fibrous dermis.
FIGURE 6Kaposiform hemangioendothelioma in a child with Kasabach-Merritt phenomenon. A, Large, infiltrated,edematous and boggy lesion of the trunk, thighs, and labia major, associated with petechiae.B, Compared with tufted angioma, the lobules are larger and coalescent and infiltrate the hypodermisfat. C, a subset of tumor cells, often situated at the periphery of the lobules, express the lymphaticendothelial marker podoplanin (D2-40 antibody).
TABLE 4 Simple Vascular Malformations
CMsCutaneous and/or mucosal CM (“port wine”
stain)CM with bone and/or soft tissue overgrowthCM with CNS and/or ocular anomalies
(Sturge-Weber syndrome)CM of CM-AVMCM of microcephaly-CM (MICCAP)CM of megalencephaly-CM-polymicrogyria
(MCAP)TelangiectasiaHereditary hemorrhagic telangiectasia (HHT;
different types)Others
Cutis marmorata telangiectatica congenita(CMTC)
Nevus simplex/salmon patch/ “angel kiss,”“stork bite”
OthersLMsCommon (cystic) LMsMacrocystic LMMicrocystic LMMixed cystic LM
Generalized lymphatic anomaly (GLA)LM in Gorham-Stout diseaseChannel-type LMPrimary lymphedemaOthers
VMsCommon VMFamilial VM cutaneo-mucosal (VMCM)Blue rubber bleb nevus (Bean) syndrome VMGlomuvenous malformation (GVM)Cerebral cavernous malformation (CCM;
different types)Others
AVMsSporadicIn HHTIn CM-AVM
AVFsSporadicIn HHTIn CM-AVMOthers
PEDIATRICS Volume 136, number 1, July 2015 e207 by guest on April 12, 2020www.aappublications.org/newsDownloaded from

a spectrum rather than distinctdiseases.42 The description of themany other types of even rarervascular tumors is beyond the focusof this article.
Vascular Malformations
Vascular malformations are dividedinto 4 groups: simple malformations,combined malformations,malformations of major namedvessels, and malformations associatedwith other anomalies. “Malformationsof major named vessels” was thename chosen for those malformationsnamed “truncular” in the Hamburgclassification.
Simple Vascular Malformations
Most simple malformations arecomposed mainly of only 1 type ofvessel (capillaries, lymphatics, orveins), with the exception ofarteriovenous malformation, whichcontains arteries, veins, andcapillaries (ie, not a combined venousmalformation with an arterialmalformation but rather a separatedisease composed of several types ofvessels). Similarly, nonacquiredarteriovenous fistula is notconsidered a combined malformation.For each type of simple malformation,a list of the well-defined diseases isproposed (Table 4).
Capillary malformations (CMs;Table 4) mainly affect the skin andmucosa, appearing as pink to redmacules (often referred to as “portwine” stains) (Fig 7). They arepresent at birth and generally persistthroughout life. These lesions maythicken and darken with time andmay be associated with soft tissue orbone overgrowth. Some variants,which affect the midline of the head,in the forehead, eyelids, glabella, ornape (named nevus simplex orsalmon patch, or so-called angel kissor stork bite) may lighten anddisappear with time, generally before5 years of age. CMs consist of dilatedcapillaries and/or postcapillaryvenules. Lesions associated with softtissue or bone overgrowth may
contain deep lobular aggregates ofvenous-like vessels. CMs may beassociated with other vascular andnonvascular anomalies andsyndromes (see below).
Lymphatic malformations (LMs;Table 4) are made up of variously
dilated lymphatic channels or cysts,lined by endothelial cells witha lymphatic phenotype. They areclassified as microcystic, macrocystic,and mixed subtypes. There is nouniform consensus regarding thedefinition of macrocystic and
FIGURE 7Capillary malformation: macular vascular lesion that blanches upon pressure.
FIGURE 8Lymphatic malformation. A, Large macrocytic LM of the axillary region. B, MRI of a macrocystic LM ofthe neck after contrast injection. Thin septae are visible between the large cysts. C, The endothelialcells of LM present a lymphatic phenotype (anti-podoplanin D2-40 antibody).
e208 WASSEF et al by guest on April 12, 2020www.aappublications.org/newsDownloaded from

microcystic LMs. A useful distinctionis whether the cysts can besuccessfully aspirated/sclerosed,resulting in a decrease in LM size,44
with the smaller cysts being morechallenging. Radiographic featuresalso can help to define the differencebecause macrocystic LMs are oftenevident as discernible fluid-filledareas. Common LM develops mainlyin the cervicofacial and axillaryregion, generally under normal-colored skin (Fig 8), except whenintralesional hemorrhage occurs.Generalized lymphatic anomaly isdefined as a multifocal LM that mayaffect the skin and superficial softtissue and abdominal and thoracicviscera, and often involve bone, withbone disease that is generallynonprogressive and spares the bonecortical boundaries. Chylous effusions(pericardial, pleural, or peritoneal)can be present. In contrast, Gorham-Stout disease, also nameddisappearing or vanishing bonedisease, is characterized by LMaffecting a single or multiple bonesand often neighboring soft tissue,with a progressive osteolysis alsoaffecting the cortical bone. Patientswith Gorham-Stout disease can alsohave abdominal and thoracic visceralinvolvement as well as effusions.Pathologic fractures may occur inboth entities. Primary lymphedemasare considered a subtype of LM dueto a primary dysgenesis of thelymphatic network. The causalmutations underlying many types ofprimary lymphedemas are nowelucidated (list available on the ISSVAWeb site, www.issva.org). LMs maybe associated with other vascular andnonvascular anomalies (see below).
Venous malformations (VMs)(Table 4) generally manifest as a blueskin discoloration when superficial(Fig 9) or as a soft subcutaneous massand may affect every tissue or viscera.Common VMs are soft andcompressible and tend to increase involume with an increase in venouspressure (eg, Valsalva maneuver orstraining) when the affected segment
is dependent or with exercise. Becauseof sluggish flow of blood through themalformed vessels, thrombosis mayoccur, resulting in pain and theformation of rounded hyalineorganized thrombi (phleboliths) thatmay be palpable or visible on imagingwhen calcified. Morphologically, VMsmay be focal, multifocal, or diffuse, the
latter typically involving an entiremuscle or limb. Common VMs aregenerally sporadic. They may beevident at birth, but many cases,particularly those with predominantlyintramuscular disease, often presentlater in life with pain provoked byvigorous physical activity.45 FamilialVMs present generally as small
FIGURE 9Venous malformation. A, Blue, soft, ill-defined mass involving the lips, nose, and cheek. B, MRI of the samechild showing a hyperintense lobulated lesion, extending to the pharynx, on T2-weighted images. C, Histo-logically, VMs are made up of thin-walled stellate, generally empty vessels, dissecting the host tissue.
FIGURE 10Glomuvenous malformation. A, Multifocal dilated veins in checkerboard pattern with blue-colored skin.B, Vessel walls of glomuvenous malformation contain distinctive round or cuboidal glomus cells.
PEDIATRICS Volume 136, number 1, July 2015 e209 by guest on April 12, 2020www.aappublications.org/newsDownloaded from

multiple lesions affecting the skin andmucosa. These familial cutaneo-mucosal VMs are caused by germ-lineautosomal dominant mutations in thetyrosine kinase with immunoglobulin-like and EGF-like domain 2 (Tie2)gene.46 A proportion of sporadicVMs also are caused by somaticmutations in the same Tie2 gene.47
Both common and familial VMs arecomposed of a network of veins withthin walls, defective in smooth musclecell media, dissecting the host tissue.Patients affected by the blue rubberbleb syndrome (Bean syndrome)present with multiple VMs affectingthe skin, soft tissue, andgastrointestinal tract, the latterresponsible for chronic bleeding andanemia. Some of the skin VMs,especially on the soles and palms,present as small, round, darkhyperkeratotic bleblike or nipple-likelesions. Glomuvenous malformations,formerly known as glomangioma orglomangiomatosis, form nodular orplaque-like lesions, sometimes witha cobblestone appearance, affectingthe skin (Fig 10), with rare mucosallocalization. They are generally ofdarker blue to purple color and lesscompressible compared with bluishsoft common VMs and are usuallypainful to palpation. Their histologicappearance is similar to common VMsexcept for the presence, at least focally,in the vein walls of rounded “glomus”cells corresponding to modifiedsmooth muscle cells. Glomuvenousmalformations are related to aninactivating mutation in the glomulingene.48 Cerebral cavernousmalformations (CCMs) are solitary ormultiple nodular aggregates of thin-walled, round, closely packed veins,progressively appearing in the brain ofaffected patients. Contrary to otherVMs, no normal tissue structures areenclosed in the lesion between theabnormal veins. CCMs are related tomutations in several different genes:KRIT1 (Krev interaction trapped 1;CCM1), malcavernin (CCM2), andPDCD10 (programmed cell death 10;CCM3).49 VMs may be associated with
other vascular and nonvascularanomalies (see below).
Arteriovenous malformations (AVMs)are potentially the more aggressivetype of vascular malformation. Theyare composed of malformed arteries,veins, and capillaries, with directarteriovenous communicationsresulting in arteriovenous shunting.They may present as a pseudo-CM
with pulsation at palpation or a bruit;as an enlarging red, warm, painfullesion (Fig 11); as an ulcerated andbleeding lesion due to trophic skinlesions; or rarely, with a shunt-relatedcardiac overload. Individual lesionsmay progress from a quiescent toa more aggressive lesion, followingthe 4 stages defined by Schobinger.50
AVMs and congenital arteriovenous
FIGURE 11Arteriovenous malformation. A, Bright-red enlarged hand and distorted fingers in a patient with AVM ofthe arm treated with multiple embolizations. The patient was born with cardiomegaly, a high-flowcardiac state, and bruit in the affected arm. B, AVMs are made of round or oval thick-walled vessels ofvarious size, evenly distributed in the tissue, along with various amounts of small capillary vessels.
TABLE 5 Combined Vascular Malformations
Combined Vascular Malformations
CM + VM Capillary-venous malformationCM + LM Capillary-lymphatic malformationCM + AVM Capillary-arteriovenous malformationLM + VM Lymphatic-venous malformationCM + LM + VM Capillary-lymphatic-venous malformationCM + LM + AVM Capillary-lymphatic-arteriovenous malformationCM + VM + AVM Capillary-venous-arteriovenous malformationCM + LM + VM + AVM Capillary-lymphatic-venous-arteriovenous malformation
e210 WASSEF et al by guest on April 12, 2020www.aappublications.org/newsDownloaded from

fistulas may be sporadic or observedin patients presenting with hereditaryhemorrhagic telangiectasia51 or CM-AVM RASA1 (RAS p21 proteinactivator [GTPase activatingprotein])–related disease.52 AVMsand arteriovenous fistulas may beassociated with other vascular andnonvascular anomalies (see below).
Combined Vascular Malformations
Combined vascular malformationsassociate $2 vascular malformationsin 1 lesion. These may be simplemalformations, malformations ofmajor named vessels, ora combination of both types. Somecombined malformations associatea cutaneous CM and an underlyingVM, LM, or AVM, or a VM with an LM.Others are also associated withnonvascular anomalies (see below).A list of the different existingcombinations is presented in Table 5.
Malformations of Major Named Vessels
These malformations affect veins,arteries, or lymphatics of generallylarge caliber, often axial or conductingvessels. They consist of anomalies inthe origin, course, number, length,
diameter (aplasia, hypoplasia,ectasia/aneurysm) or valves.Congenital arteriovenous fistulas andthe persistence of embryonic vesselsare also included in this group ofmalformations.
Vascular Malformations AssociatedWith Other Anomalies
Vascular malformations (simple and/or of major named vessels) may beassociated with anomalies of bone,soft tissue, or viscera. Thesenonvascular anomalies are oftenovergrowth of soft tissue and/or boneor, rarely, undergrowth. Most of theseassociations are eponymoussyndromes. Most of these syndromesor diseases are listed in Table 6 alongwith their most common associations
Provisionally Unclassified VascularAnomalies
A small number of vascular anomaliesremain unclassified, because it is stillunclear whether they are tumors ormalformations or because theirdefinition and clinicopathologiccharacteristics are still incompletelyunderstood. The main unclassifiedlesions are verrucous hemangioma andangiokeratoma,53,54 multifocallymphangioendotheliomatosis withthrombocytopenia/cutaneovisceralangiomatosis with thrombocytopenia,kaposiform lymphangiomatosis,55,56
phosphatase and tensin homolog(PTEN) (type) hamartoma of softtissue, and “angiomatosis” of softtissue.57,58
GENETIC CAUSES OF VASCULARANOMALIES AND OTHER APPENDICES
In recent years, our knowledge of thegenetic causes of vascular anomalieshas increased considerably. Many ofthe identified genes cause inheriteddiseases, but the genetic anomaliesunderlying some sporadicmalformations with postzygoticsomatic mutations have also beenunraveled. Because the list ofcausative genetic anomalies is rapidlylengthening, it has not been includedin the body of the classification but is
presented in an appendix. Otherappendices include a list ofabbreviations used in theclassification or recommended, a listof vascular anomalies possiblyassociated with thrombocytopenia orcoagulation disorders, and someadditional information on IH, themost common vascular tumor. Theseappendices as well as the completeclassification are freely available onthe ISSVA Web site (www.issva.org).It is anticipated that thiscomprehensive updated classificationwill provide a consistent framework,encourage common terminology, andaid in both management of affectedpatients and research.
ACKNOWLEDGMENTS
ISSVA 2013 Board: Hans-Peter Berlien(President), Laurence M. Boon, PatriciaBurrows, Steven Fishman, Ilona J.Frieden, and Raul Mattassi. ISSVA 2013Scientific Committee: Francine Blei(Head), Denise Adams, Ahmad Alomari,Eulalia Baselga, Alejandro Berenstein,Maria C. Garzon, Rainer Grantzow,Juan-Carlos Lopez-Gutierrez, David J.E.Lord, Sally Mitchel, John Stuart Nelson,Julie Powell, Julie Prendiville, andMichel Wassef.
We thank Dr John B. Mulliken for hisinsight and diligent review of ourupdated classification, as well as ourcolleagues, support staff, and patientswho provide our inspiration.
ABBREVIATIONS
AVM: arteriovenous malformationCH: congenital hemangiomaCCM: cerebral cavernous
malformationCM: capillary malformationGlut-1: glucose transporter 1IH: infantile hemangiomaISSVA: International Society for
the Study of VascularAnomalies
LM: lymphatic malformationVM: venous malformationWHO: World Health Organization
TABLE 6 Vascular Malformations AssociatedWith Other Anomalies
Klippel-Trenaunay syndrome: CM + VM +/2 LM +limb overgrowth
Parkes-Weber syndrome: CM + AVF + limbovergrowth
Servelle-Martorell syndrome: limb VM + boneundergrowth
Sturge-Weber syndrome: facial + leptomeningealCM + ocular anomalies +/2 bone and/or softtissue overgrowth
Limb CM + congenital nonprogressive limbhypertrophy
Maffucci syndrome: VM +/2 spindle cellhemangioma + enchondroma
Macrocephaly-CM (M-CM)/megalencephaly-CM-polymicrogyria (MCAP)
Microcephaly-CM (MICCAP)CLOVES syndrome: LM + VM + CM +/2 AVM +
lipomatous overgrowthProteus syndrome: CM, VM and/or LM +
asymmetric somatic overgrowthBannayan-Riley-Ruvalcaba syndrome: AVM + VM +
macrocephaly, lipomatous overgrowth
CLOVES, congenital, lipomatous, overgrowth, vascularmalformations, epidermal nevi and spinal/skeletal anomaliesand/or scoliosis.
PEDIATRICS Volume 136, number 1, July 2015 e211 by guest on April 12, 2020www.aappublications.org/newsDownloaded from

www.pediatrics.org/cgi/doi/10.1542/peds.2014-3673
DOI: 10.1542/peds.2014-3673
Accepted for publication Mar 27, 2015
Address correspondence to Michel Wassef, MD, Department of Pathology, Lariboisière Hospital, 2 rue Ambroise Paré, 75010 Paris, France. E-mail: michel.wassef@lrb.
aphp.fr
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
COMPANION PAPER: A companion to this article can be found on page e225, online at www.pediatrics.org/cgi/doi/10.1542/peds.2015-0688.
REFERENCES
1. Hand JL, Frieden IJ. Vascularbirthmarks of infancy: resolvingnosologic confusion. Am J Med Genet.2002;108(4):257–264
2. Hassanein AH, Mulliken JB, Fishman SJ,Greene AK. Evaluation of terminology forvascular anomalies in current literature.Plast Reconstr Surg. 2011;127(1):347–351
3. Kollipara R, Dinneen L, Rentas KE, et al.Current classification and terminologyof pediatric vascular anomalies. AJRAm J Roentgenol. 2013;201(5):1124–1135
4. Mulligan PR, Prajapati HJ, Martin LG,Patel TH. Vascular anomalies:classification, imaging characteristicsand implications for interventionalradiology treatment approaches.Br J Radiol. 2014;87(1035):20130392
5. Enjolras O, Mulliken JB. Vascular tumorsand vascular malformations (newissues). Adv Dermatol. 1997;13:375–423
6. Enjolras O. Classification andmanagement of the various superficialvascular anomalies: hemangiomas andvascular malformations. J Dermatol.1997;24(11):701–710
7. Enjolras O, Wassef M, Chapot R. ColorAtlas of Vascular Tumors and VascularMalformations. Cambridge, UnitedKingdom: Cambridge University Press;2007
8. Virchow R. Angioma in die KrankhaftenGeschwülste. Berlin, Germany:Hirshwald; 1863:306–425
9. Wegener G. Ueber Lynmphangiome. ArchKlin Chir. 1877;20:641–707
10. Mulliken JB, Young AE. VascularBirthmarks: Hemangiomas andMalformations. Philadelphia, PA:Saunders; 1988
11. Sangueza OP, Kasper RC, LeBoit P, et al.Vascular tumors. In: LeBoit PE, Burg G,Weedon D, Sarasain A, eds. Pathologyand Genetics of Skin Tumors: WorldHealth Organization Classification ofTumours. Lyon, France: IARC Press; 2006:233–246
12. Fletcher CDM, Bridge JA, HogendoornPCW, Mertens F, eds. WHO Classificationof Tumors of Soft Tissue and Bone. Lyon,France: IARC Press; 2013
13. Calonje JE. Hemangiomas. In:Fletcher CDM, Bridge JA, HogendoornPCW, Mertens F, eds. WHOClassification of Tumors of Soft Tissueand Bone. Lyon, France: IARC Press;2013:138–140
14. Mulliken JB, Glowacki J. Hemangiomasand vascular malformations ininfants and children: a classificationbased on endothelial characteristics.Plast Reconstr Surg. 1982;69(3):412–422
15. Lee BB, Baumgartner I, Berlien P, et al.Diagnosis and treatment of venousmalformations consensus document ofthe International Union of Phlebology(IUP): updated 2013. Int Angiol. 2015;34(2):97–144
16. Godfraind C, Calicchio ML, Kozakewich H.Pyogenic granuloma, an impaired woundhealing process, linked to vasculargrowth driven by FLT4 and the nitricoxide pathway. Mod Pathol. 2013;26(2):247–255
17. Battocchio S, Facchetti F, Brisigotti M.Spindle cell haemangioendothelioma:further evidence against its proposedneoplastic nature. Histopathology. 1993;22(3):296–298
18. Sun ZJ, Zhang L, Zhang WF, Liu B, Li ZB,Zhao YF. A possible hypoxia-inducedendothelial proliferation in thepathogenesis of epithelioid hemangioma.Med Hypotheses. 2006;67(5):1133–1135
19. Requena L, Sangueza OP. Cutaneousvascular anomalies. Part I. Hamartomas,malformations, and dilation ofpreexisting vessels. J Am Acad Dermatol.1997;37(4):523–549; quiz 549–552
20. Requena L, Sangueza OP. Cutaneousvascular proliferation. Part II.Hyperplasias and benign neoplasms.J Am Acad Dermatol. 1997;37(6):887–919;quiz 920-882
21. Requena L, Sangueza OP. Cutaneousvascular proliferations. Part III.Malignant neoplasms, other cutaneousneoplasms with significant vascularcomponent, and disorders erroneouslyconsidered as vascular neoplasms.J Am Acad Dermatol. 1998;38(2 pt 1):143–175; quiz 176–148
22. North PE, Waner M, Buckmiller L, JamesCA, Mihm MC Jr. Vascular tumors ofinfancy and childhood: beyond capillaryhemangioma. Cardiovasc Pathol. 2006;15(6):303–317
23. Wassef M, Hunt SJ, Santa Cruz DJ,Barnhill RL. Vascular tumors andvascular malformations. In: Barnhill RL,Crowson AN, Magro CM, Piepkorn MW,eds. Dermatopathology. 3rd ed. NewYork, NY: McGraw-Hill; 2010:802–856
e212 WASSEF et al by guest on April 12, 2020www.aappublications.org/newsDownloaded from

24. Kozakewich HPW, Mulliken JB.Histopathology of vascularmalformations. In: Mulliken JB, BurrowsPE, Fishman SJ, eds. Mulliken & Young’sVascular Anomalies, Hemangiomasand Malformations. 2nd ed. New York,NY: Oxford University Press; 2013:480–507
25. Kilcline C, Frieden IJ. Infantilehemangiomas: how common are they?A systematic review of the medicalliterature. Pediatr Dermatol. 2008;25(2):168–173
26. Kanada KN, Merin MR, Munden A,Friedlander SF. A prospective study ofcutaneous findings in newborns in theUnited States: correlation with race,ethnicity, and gestational statususing updated classification andnomenclature. J Pediatr. 2012;161(2):240–245
27. Mulliken JB, Enjolras O. Congenitalhemangiomas and infantilehemangioma: missing links. J Am AcadDermatol. 2004;50(6):875–882
28. Waner M, North PE, Scherer KA, FriedenIJ, Waner A, Mihm MC Jr. The nonrandomdistribution of facial hemangiomas. ArchDermatol. 2003;139(7):869–875
29. Frieden IJ, Reese V, Cohen D. PHACEsyndrome: the association of posteriorfossa brain malformations,hemangiomas, arterial anomalies,coarctation of the aorta and cardiacdefects, and eye abnormalities. ArchDermatol. 1996;132(3):307–311
30. Metry D, Heyer G, Hess C, et al; PHACESyndrome Research Conference.Consensus statement on diagnosticcriteria for PHACE syndrome. Pediatrics.2009;124(5):1447–1456
31. Iacobas I, Burrows PE, Frieden IJ, et al.LUMBAR: association between cutaneousinfantile hemangiomas of the lowerbody and regional congenitalanomalies. J Pediatr. 2010;157(5):795–801, e791
32. North PE, Waner M, Mizeracki A, MihmMC Jr. GLUT1: a newly discoveredimmunohistochemical marker forjuvenile hemangiomas. Hum Pathol.2000;31(1):11–22
33. North PE, Waner M, Mizeracki A, et al.A unique microvascular phenotypeshared by juvenile hemangiomas andhuman placenta. Arch Dermatol. 2001;137(5):559–570
34. Boon LM, Enjolras O, Mulliken JB.Congenital hemangioma: evidence ofaccelerated involution. J Pediatr. 1996;128(3):329–335
35. Berenguer B, Mulliken JB, Enjolras O,et al. Rapidly involuting congenitalhemangioma: clinical andhistopathologic features. Pediatr DevPathol. 2003;6(6):495–510
36. Enjolras O, Mulliken JB, Boon LM, WassefM, Kozakewich HP, Burrows PE.Noninvoluting congenital hemangioma:a rare cutaneous vascular anomaly.Plast Reconstr Surg. 2001;107(7):1647–1654
37. Nasseri E, Piram M, McCuaig CC, Kokta V,Dubois J, Powell J. Partially involutingcongenital hemangiomas: a report of 8cases and review of the literature. J AmAcad Dermatol. 2014;70(1):75–79
38. Baselga E, Cordisco MR, Garzon M,Lee MT, Alomar A, Blei F. Rapidlyinvoluting congenital haemangiomaassociated with transientthrombocytopenia and coagulopathy:a case series. Br J Dermatol. 2008;158(6):1363–1370
39. Osio A, Fraitag S, Hadj-Rabia S, BodemerC, de Prost Y, Hamel-Teillac D. Clinicalspectrum of tufted angiomas inchildhood: a report of 13 cases anda review of the literature. Arch Dermatol.2010;146(7):758–763
40. Le Huu AR, Jokinen CH, Rubin BP, et al.Expression of prox1, lymphaticendothelial nuclear transcription factor,in Kaposiform hemangioendotheliomaand tufted angioma. Am J Surg Pathol.2010;34(11):1563–1573
41. Zukerberg LR, Nickoloff BJ, Weiss SW.Kaposiform hemangioendothelioma ofinfancy and childhood: an aggressiveneoplasm associated with Kasabach-Merritt syndrome andlymphangiomatosis. Am J Surg Pathol.1993;17(4):321–328
42. Enjolras O, Wassef M, Mazoyer E, et al.Infants with Kasabach-Merritt syndromedo not have “true” hemangiomas.J Pediatr. 1997;130(4):631–640
43. Sarkar M, Mulliken JB, Kozakewich HP,Robertson RL, Burrows PE.Thrombocytopenic coagulopathy(Kasabach-Merritt phenomenon) isassociated with kaposiformhemangioendothelioma and not with
common infantile hemangioma. PlastReconstr Surg. 1997;100(6):1377–1386
44. Fishman SJ, Young AE. Slow-flowvascular malformations. In: Mulliken JB,Burrows PE, Fishman SJ, eds. Mulliken &Young’s Vascular Anomalies,Hemangiomas and Malformations. 2nded. New York, NY: Oxford UniversityPress; 2013:562–594
45. Vogel SA, Hess CP, Dowd CF, et al.Early versus later presentations ofvenous malformations: where andwhy? Pediatr Dermatol. 2013;30(5):534–540
46. Vikkula M, Boon LM, Carraway KL III, et al.Vascular dysmorphogenesis caused byan activating mutation in the receptortyrosine kinase TIE2. Cell. 1996;87(7):1181–1190
47. Soblet J, Limaye N, Uebelhoer M, BoonLM, Vikkula M. Variable somatic TIE2mutations in half of sporadic venousmalformations. Mol Syndromol. 2013;4(4):179–183
48. Brouillard P, Boon LM, Mulliken JB, et al.Mutations in a novel factor, glomulin, areresponsible for glomuvenousmalformations (“glomangiomas”). Am JHum Genet. 2002;70(4):866–874
49. Fischer A, Zalvide J, Faurobert E,Albiges-Rizo C, Tournier-Lasserve E.Cerebral cavernous malformations:from CCM genes to endothelial cellhomeostasis. Trends Mol Med. 2013;19(5):302–308
50. Kohout MP, Hansen M, Pribaz JJ, MullikenJB. Arteriovenous malformations of thehead and neck: natural history andmanagement. Plast Reconstr Surg. 1998;102(3):643–654
51. McDonald J, Bayrak-Toydemir P, PyeritzRE. Hereditary hemorrhagictelangiectasia: an overview of diagnosis,management, and pathogenesis. GenetMed. 2011;13(7):607–616
52. Revencu N, Boon LM, Mendola A, et al.RASA1 mutations and associatedphenotypes in 68 families with capillarymalformation-arteriovenousmalformation. Hum Mutat. 2013;34(12):1632–1641
53. Tennant LB, Mulliken JB, Perez-Atayde AR,Kozakewich HP. Verrucous hemangiomarevisited. Pediatr Dermatol. 2006;23(3):208–215
PEDIATRICS Volume 136, number 1, July 2015 e213 by guest on April 12, 2020www.aappublications.org/newsDownloaded from

54. Mankani MH, Dufresne CR. Verrucousmalformations: their presentation andmanagement. Ann Plast Surg. 2000;45(1):31–36
55. North PE, Kahn T, Cordisco MR, DadrasSS, Detmar M, Frieden IJ. Multifocallymphangioendotheliomatosis withthrombocytopenia: a newly recognized
clinicopathological entity. Arch Dermatol.2004;140(5):599–606
56. Prasad V, Fishman SJ, Mulliken JB, et al.Cutaneovisceral angiomatosis withthrombocytopenia. Pediatr Dev Pathol.2005;8(4):407–419
57. Rao VK, Weiss SW. Angiomatosis of softtissue: an analysis of the histologic
features and clinical outcome in 51cases. Am J Surg Pathol. 1992;16(8):764–771
58. Kurek KC, Howard E, Tennant LB,et al. PTEN hamartoma of soft tissue:a distinctive lesion in PTENsyndromes. Am J Surg Pathol. 2012;36(5):671–687
e214 WASSEF et al by guest on April 12, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2014-3673 originally published online June 8, 2015; 2015;136;e203Pediatrics
Prendiville and Miikka VikkulaJuan-Carlos Lopez-Gutierrez, David J.E. Lord, Sally Mitchel, Julie Powell, Julie
Alejandro Berenstein, Patricia Burrows, Ilona J. Frieden, Maria C. Garzon, Michel Wassef, Francine Blei, Denise Adams, Ahmad Alomari, Eulalia Baselga,
Society for the Study of Vascular AnomaliesVascular Anomalies Classification: Recommendations From the International
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/136/1/e203including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/136/1/e203#BIBLThis article cites 42 articles, 1 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/birth_defects_subBirth Defectssubhttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_Fetus/Newborn Infanthttp://www.aappublications.org/cgi/collection/dermatology_subDermatologyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on April 12, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2014-3673 originally published online June 8, 2015; 2015;136;e203Pediatrics
Prendiville and Miikka VikkulaJuan-Carlos Lopez-Gutierrez, David J.E. Lord, Sally Mitchel, Julie Powell, Julie
Alejandro Berenstein, Patricia Burrows, Ilona J. Frieden, Maria C. Garzon, Michel Wassef, Francine Blei, Denise Adams, Ahmad Alomari, Eulalia Baselga,
Society for the Study of Vascular AnomaliesVascular Anomalies Classification: Recommendations From the International
http://pediatrics.aappublications.org/content/136/1/e203located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on April 12, 2020www.aappublications.org/newsDownloaded from