Embed Size (px)
Citation preview
Your Skin
J. C. DiGiacomo, M.D., FACS
Department of Surgery
CentraState Medical Center
Integumentary System
The Largest of Our 11 Organ Systems.
Consists of the skin (i.e., the cutaneous membrane) plus all the appendages (or accessory structures) of the skin including:– Sweat glands
(sudoriferous glands)– Sebaceous glands
(oil glands)– Hair
– Nails
General Functions of the Integumentary System
• Protection from Mechanical Injury• Physical Protection of Pathogen Entry• Chemical Prevention of Pathogen Entry• Sensation• Thermoregulation• Metabolic functions
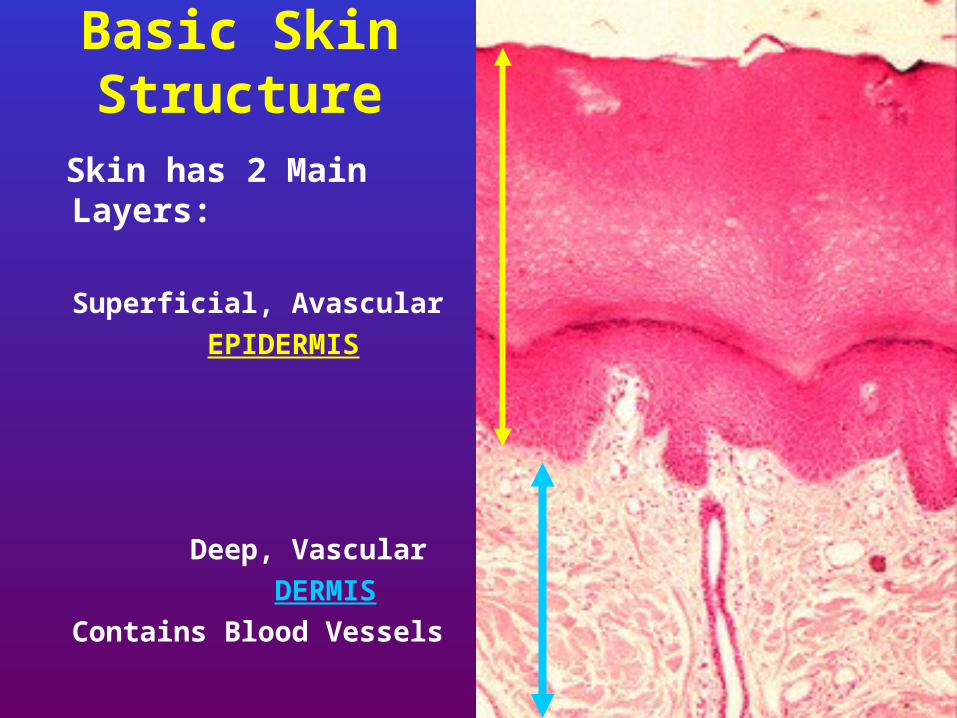
Basic Skin Structure
Skin has 2 Main Layers:
Superficial, Avascular
EPIDERMIS
Deep, Vascular
DERMIS
Contains Blood Vessels
The Epidermis
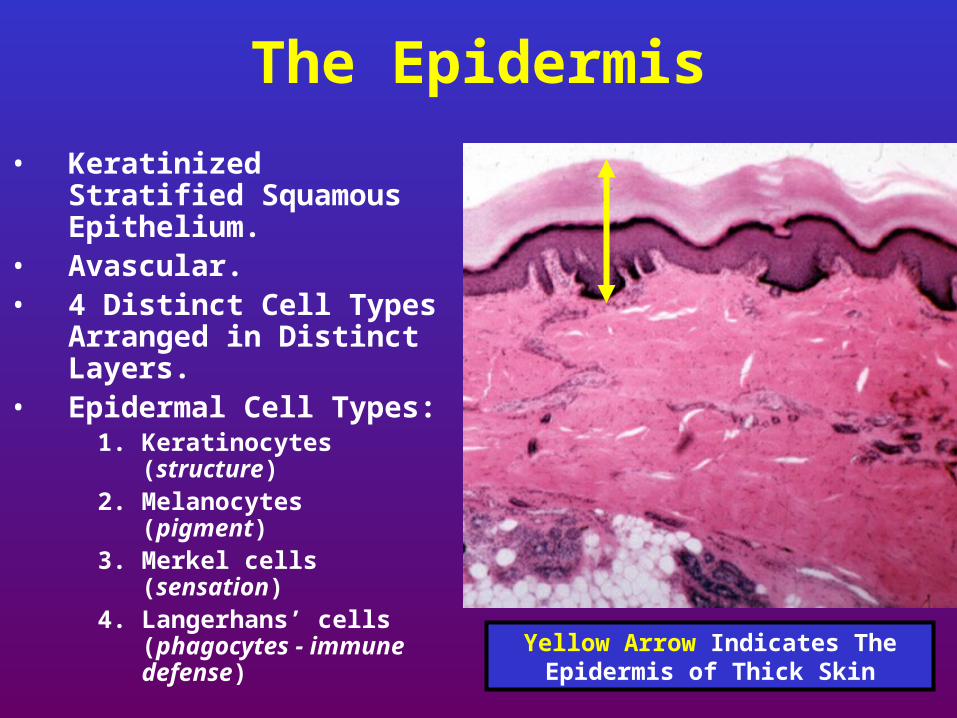
• Keratinized Stratified Squamous Epithelium.
• Avascular. • 4 Distinct Cell Types
Arranged in Distinct Layers.
• Epidermal Cell Types:1. Keratinocytes
(structure)2. Melanocytes
(pigment)3. Merkel cells
(sensation)4. Langerhans’ cells
(phagocytes - immune defense)
Yellow Arrow Indicates The Epidermis of Thick Skin
Keratinocytes
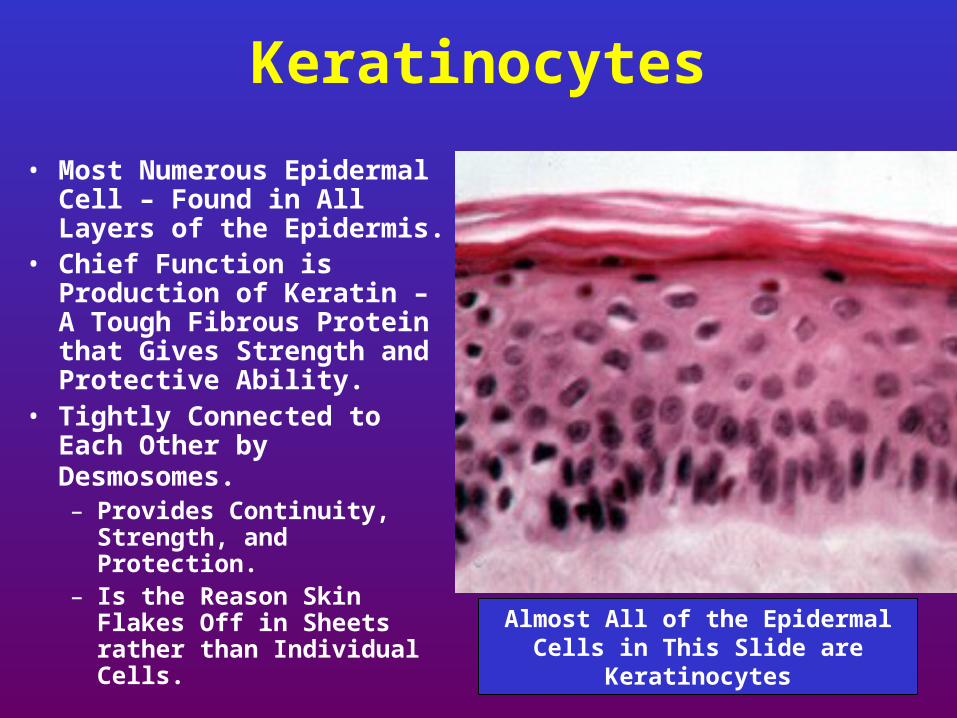
• Most Numerous Epidermal Cell – Found in All Layers of the Epidermis.
• Chief Function is Production of Keratin – A Tough Fibrous Protein that Gives Strength and Protective Ability.
• Tightly Connected to Each Other by Desmosomes. – Provides Continuity,
Strength, and Protection.– Is the Reason Skin Flakes
Off in Sheets rather than Individual Cells. Almost All of the Epidermal Cells in
This Slide are Keratinocytes
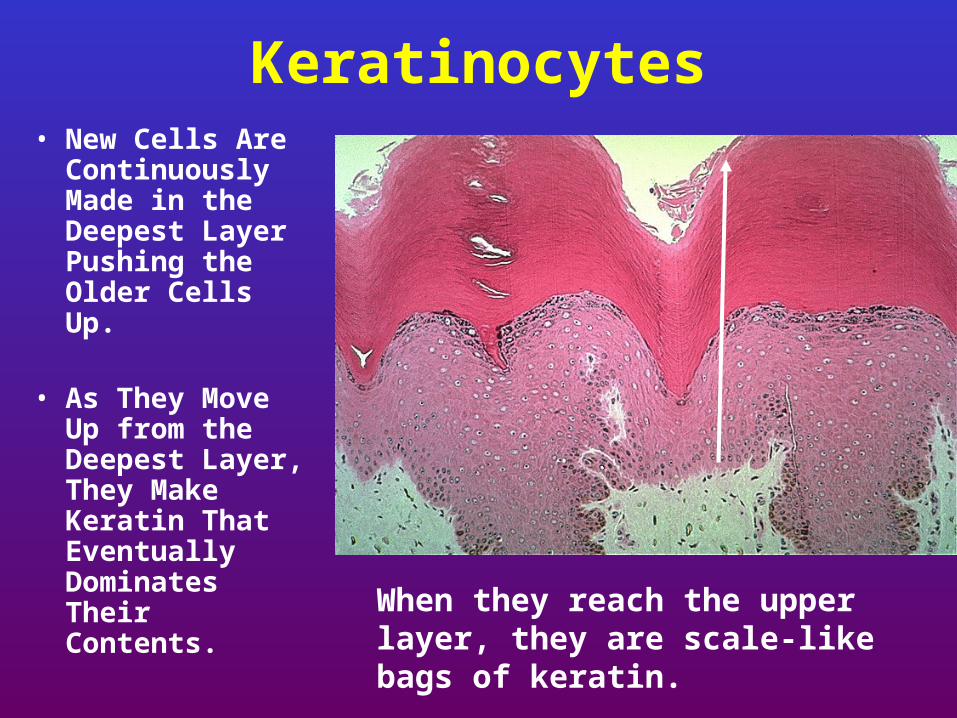
Keratinocytes• New Cells Are
Continuously Made in the Deepest Layer Pushing the Older Cells Up.
• As They Move Up from the Deepest Layer, They Make Keratin That Eventually Dominates Their Contents.
When they reach the upper layer, they are scale-like bags of keratin.
Melanocytes
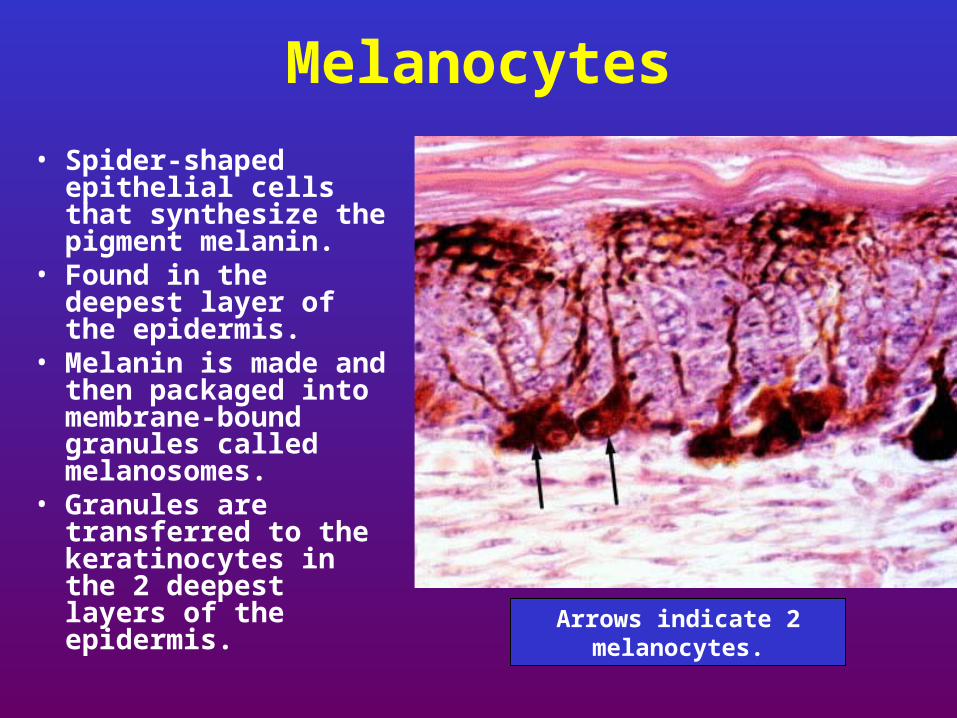
• Spider-shaped epithelial cells that synthesize the pigment melanin.
• Found in the deepest layer of the epidermis.
• Melanin is made and then packaged into membrane-bound granules called melanosomes.
• Granules are transferred to the keratinocytes in the 2 deepest layers of the epidermis.
Arrows indicate 2 melanocytes.
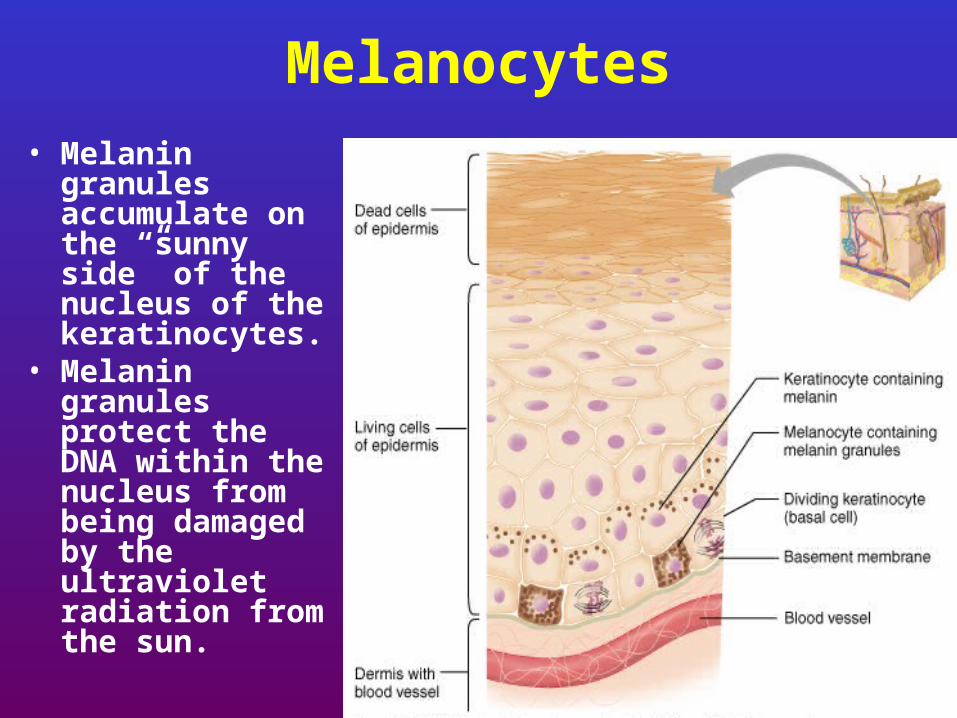
Melanocytes• Melanin granules
accumulate on the “sunny side” of the nucleus of the keratinocytes.
• Melanin granules protect the DNA within the nucleus from being damaged by the ultraviolet radiation from the sun.
Skin Color
• Due to 3 pigments: Melanin, Carotene, Hemoglobin
• Only melanin is made in the skin.
Polymer of tyrosine amino acids. Its synthesis is catalyzed by an enzyme called tyrosinase. Albinos lack this enzyme.
Color Ranges from yellow to reddish brown to black.All people have the same # of melanocytes,
individual variations in skin color are due to how much and what type of melanin is made.
Freckles and moles are local accumulations of melanin.
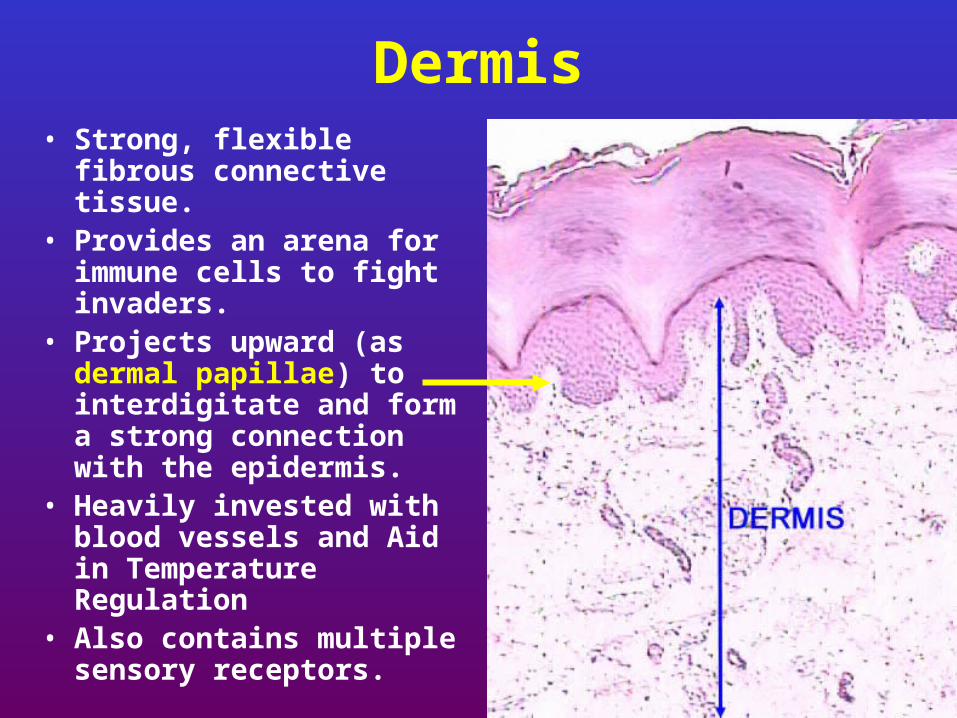
Dermis• Strong, flexible fibrous
connective tissue.• Provides an arena for
immune cells to fight invaders.
• Projects upward (as dermal papillae) to interdigitate and form a strong connection with the epidermis.
• Heavily invested with blood vessels and Aid in Temperature Regulation
• Also contains multiple sensory receptors.
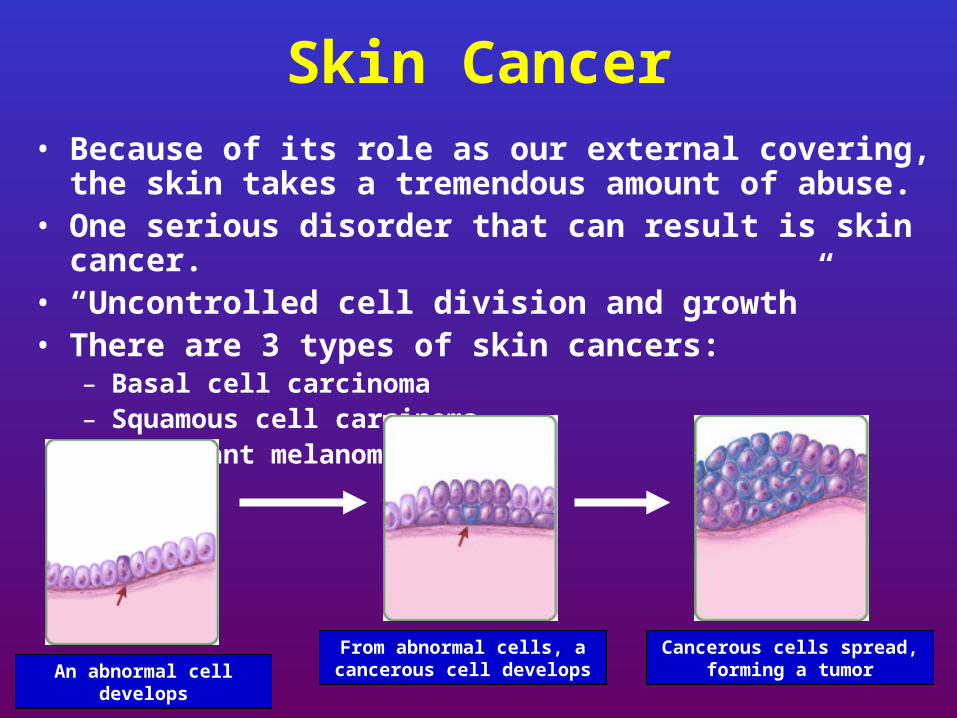
Skin Cancer• Because of its role as our external covering, the skin
takes a tremendous amount of abuse.• One serious disorder that can result is skin cancer.• “Uncontrolled cell division and growth” • There are 3 types of skin cancers:
– Basal cell carcinoma– Squamous cell carcinoma– Malignant melanoma
An abnormal cell developsFrom abnormal cells, a
cancerous cell developsCancerous cells spread,
forming a tumor
Skin Cancer
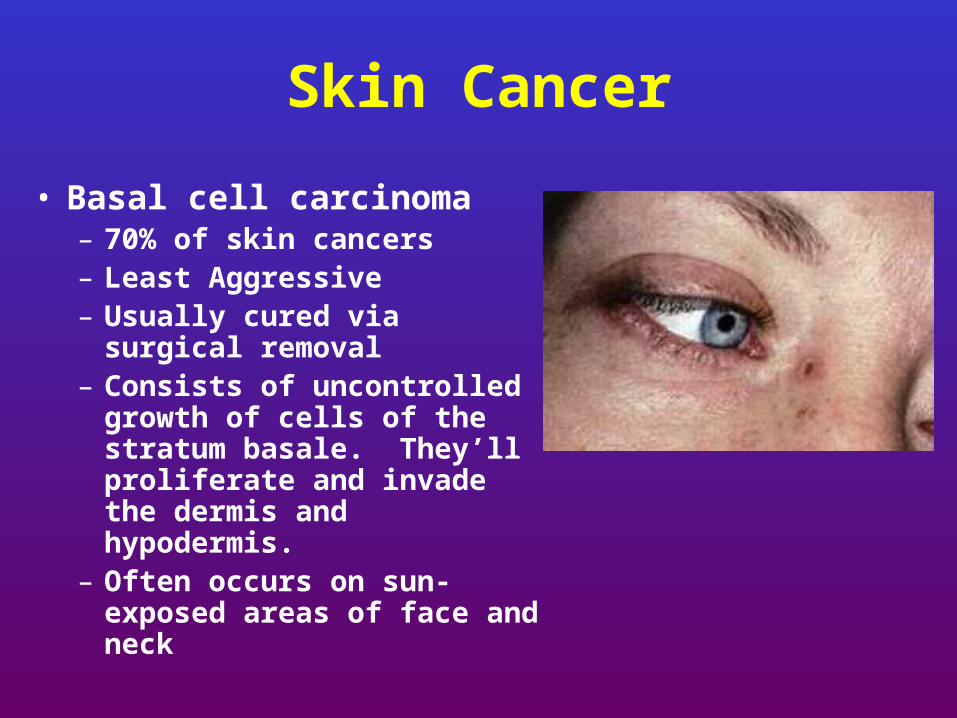
• Basal cell carcinoma– 70% of skin cancers– Least Aggressive– Usually cured via surgical
removal – Consists of uncontrolled
growth of cells of the stratum basale. They’ll proliferate and invade the dermis and hypodermis.
– Often occurs on sun-exposed areas of face and neck
Skin Cancer
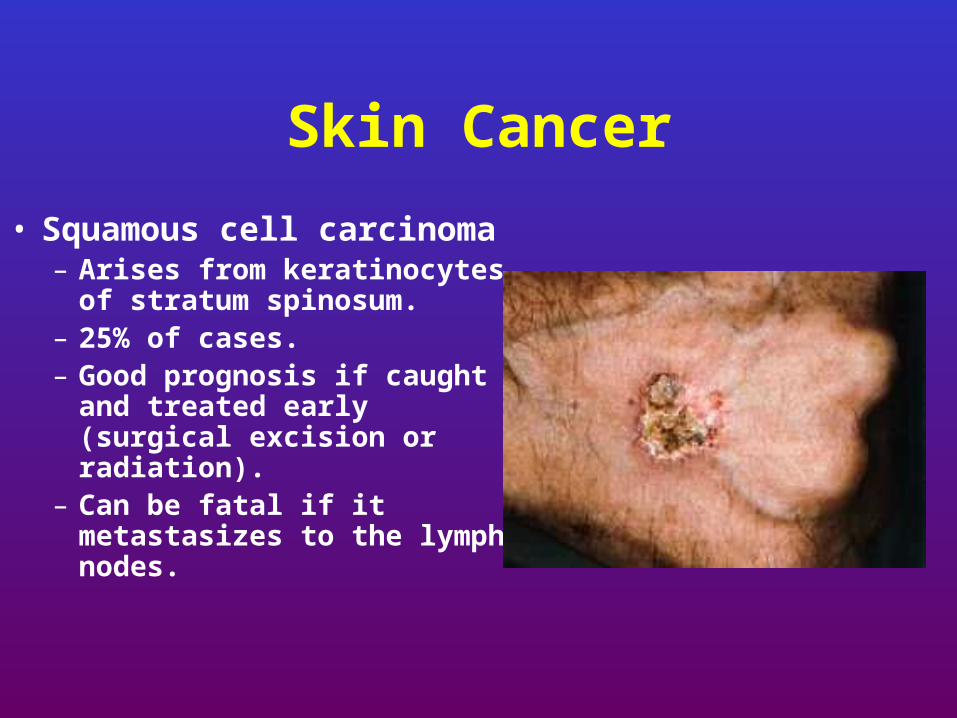
• Squamous cell carcinoma– Arises from keratinocytes
of stratum spinosum.– 25% of cases.– Good prognosis if caught
and treated early (surgical excision or radiation).
– Can be fatal if it metastasizes to the lymph nodes.

Skin Cancer
• Malignant melanoma– Least common and most
dangerous.– Cancer of melanocytes.– Often arises from a pre-existing
mole.– ABCD rule for early detection:
Asymmetry (2 sides do not match)Border irregularityColor (multiple)Diameter (>6mm is bad!)
Precancerous skin lesions
•Actinic keratoses
•Dysplastic melanocytic nevi

Actinic keratoses
10% risk of malignant transformation

Hypertrophic AK’s
• Liquid nitrogen cryotherapy
• Topical therapies
– 5-FU (Efudex)
– Imiquimod (Aldara)
• Curettage for hypertrophic lesions
Treatment of AK’s
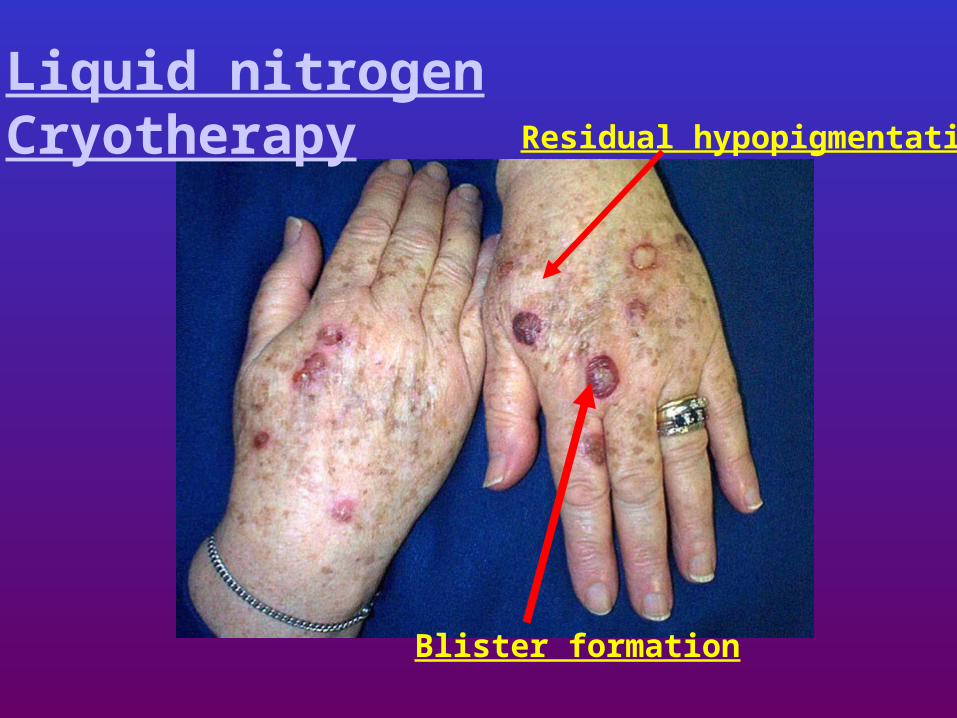
Residual hypopigmentation
Blister formation
Liquid nitrogenCryotherapy
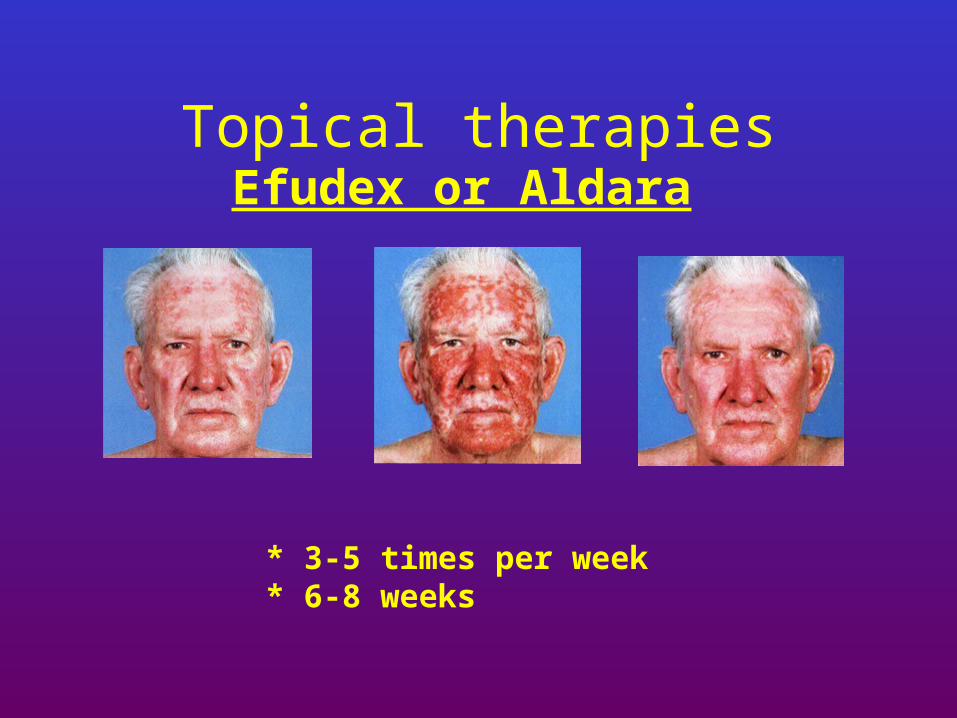
Topical therapiesEfudex or Aldara
* 3-5 times per week* 6-8 weeks

Dysplastic nevi
•Precursors for melanoma
•Markers for melanoma
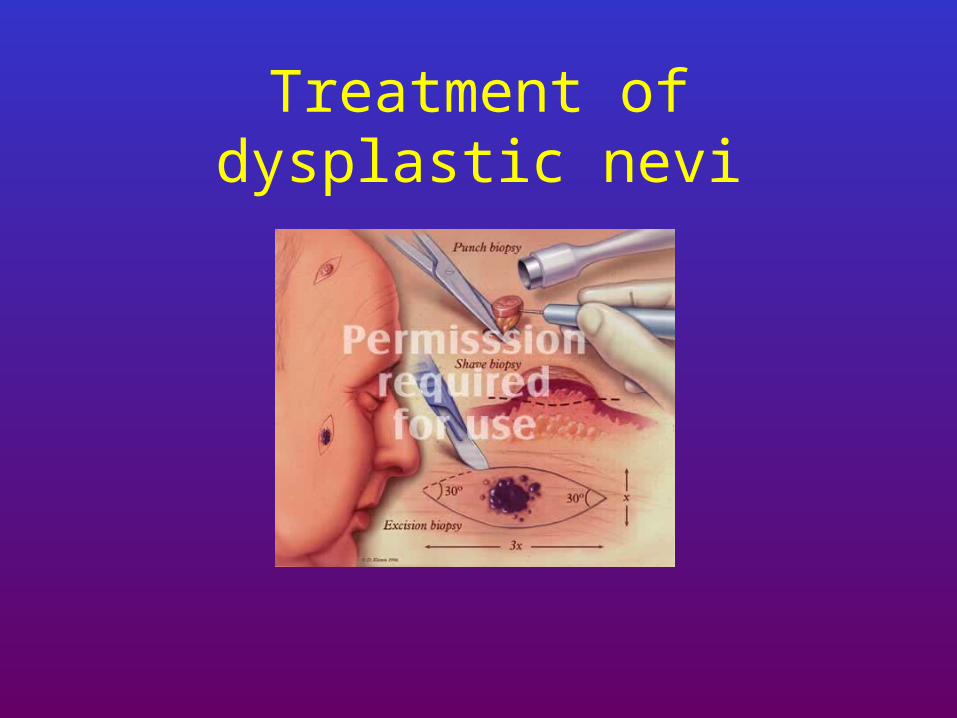
Treatment of dysplastic nevi
• Non-melanoma skin cancers (NMSC)
– Basal cell carcinoma
– Squamous cell carcinoma
– Keratoacanthoma
Risk factors for development of BCC and SCC
• Fair skin (Fitzpatrick’s types I-III)– Blue eyes– Red hair
• Family history– Genetic syndromes
• Chronic sun exposure
• Old age
• Arsenic, tar
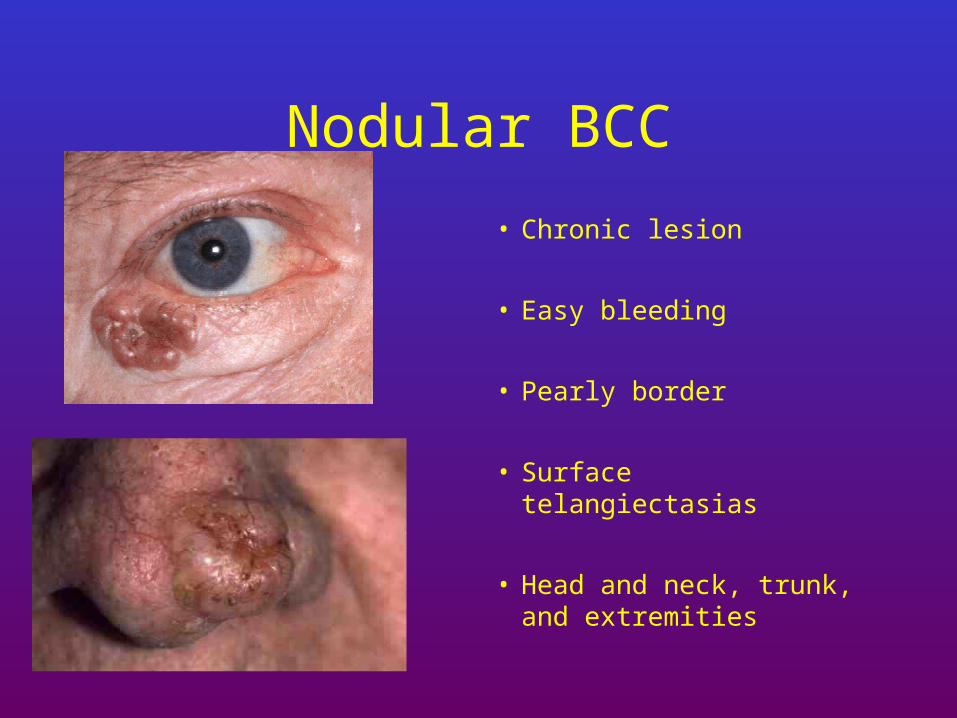
Nodular BCC
• Chronic lesion
• Easy bleeding
• Pearly border
• Surface telangiectasias
• Head and neck, trunk, and extremities

Pigmented BCC
• Similar to nodular but with black discoloration
– Melanin deposits
• Pigmented races
• Face, trunk, and scalp
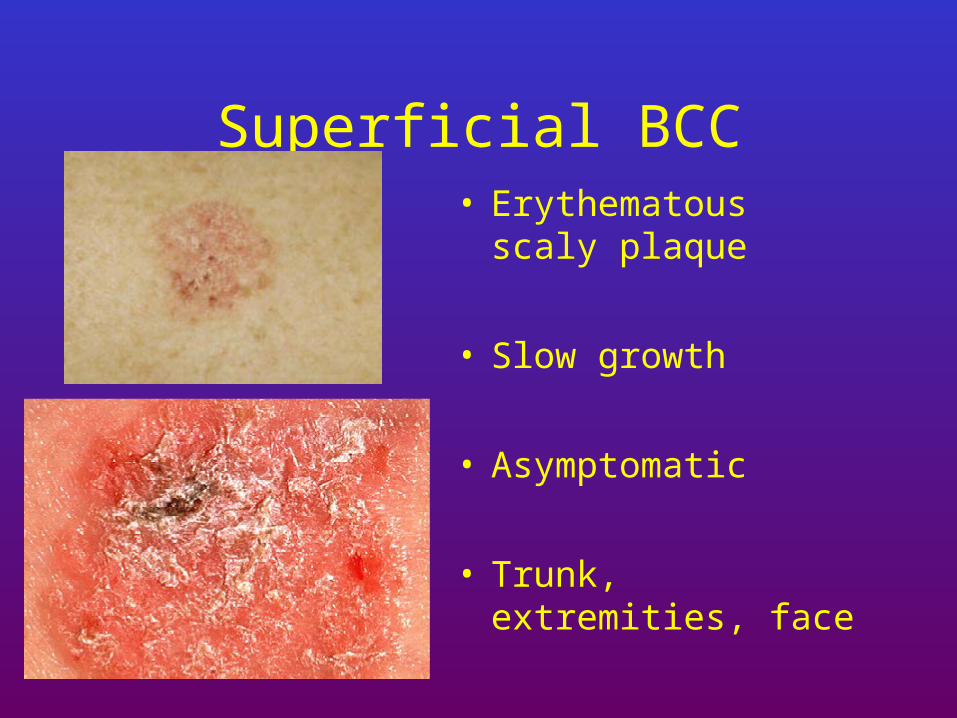
Superficial BCC• Erythematous scaly
plaque
• Slow growth
• Asymptomatic
• Trunk, extremities, face
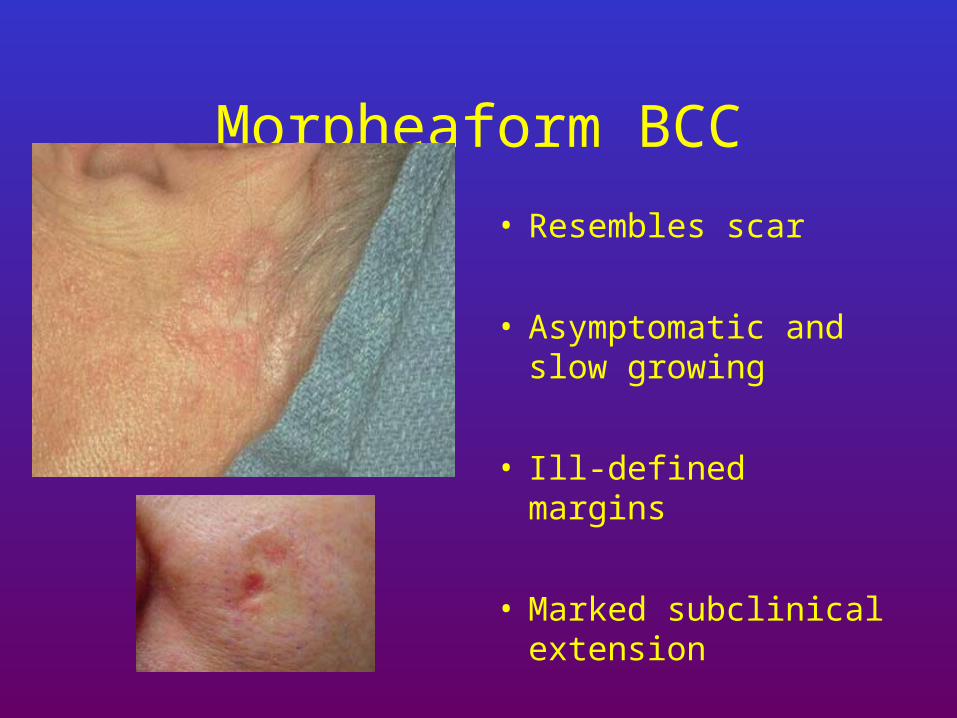
Morpheaform BCC
• Resembles scar
• Asymptomatic and slow growing
• Ill-defined margins
• Marked subclinical extension
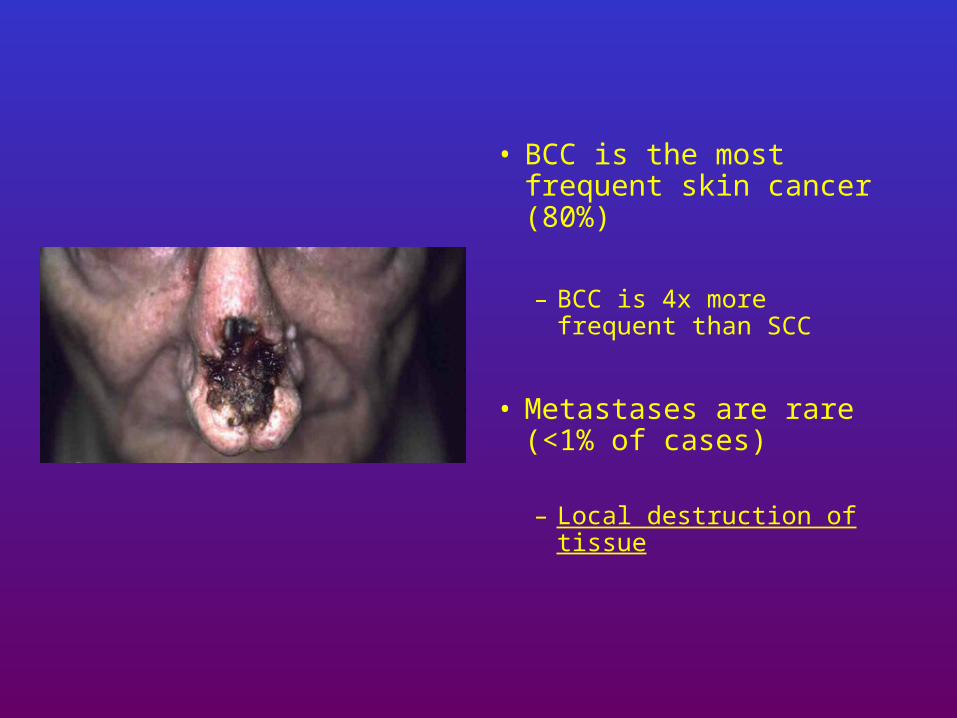
• BCC is the most frequent skin cancer (80%)
– BCC is 4x more frequent than SCC
• Metastases are rare (<1% of cases)
– Local destruction of tissue
Treatment of BCC
• Curettage electrodessication (ED/C)
• Surgical excision• Traditional
• Mohs surgery
• Radiation therapy
• Topical therapy– imiquimod
95% Cure Rate
50-75% Cure Rate
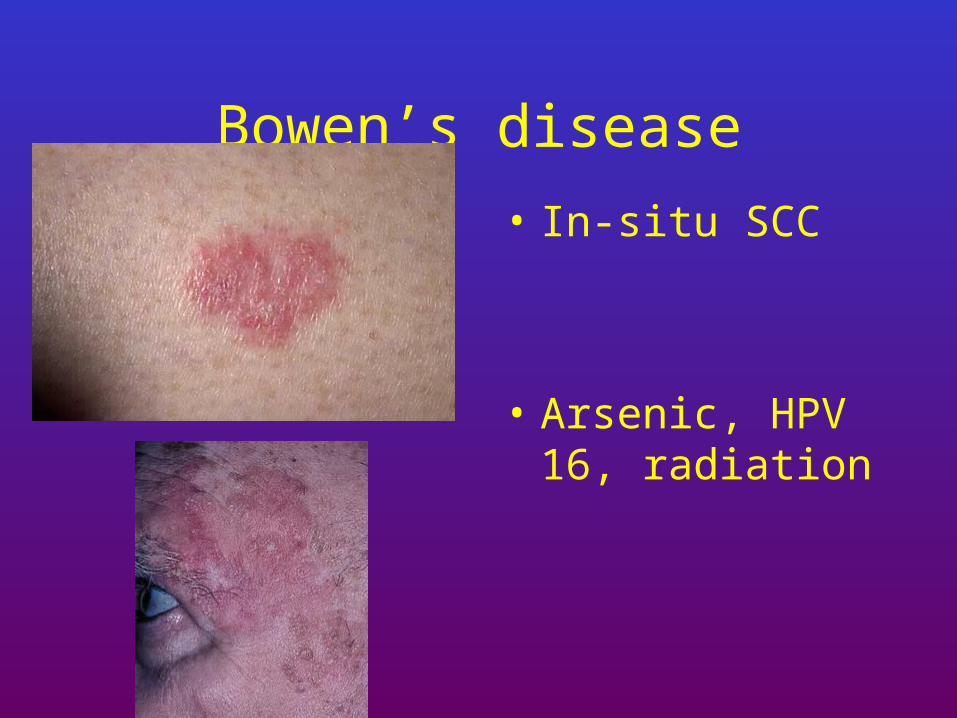
Bowen’s disease• In-situ SCC
• Arsenic, HPV 16, radiation

Invasive SCC
• Erythematous nodule
• Indurated lesion
• Sun-exposed skin– Men > women
• Slow growth

Invasive SCC
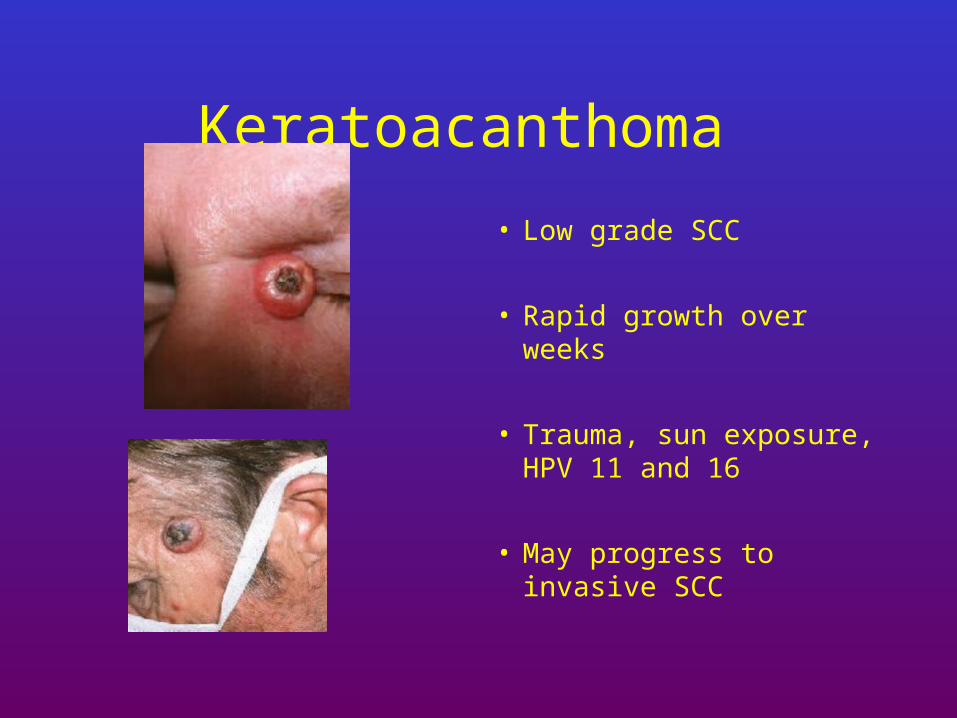
Keratoacanthoma
• Low grade SCC
• Rapid growth over weeks
• Trauma, sun exposure, HPV 11 and 16
• May progress to invasive SCC
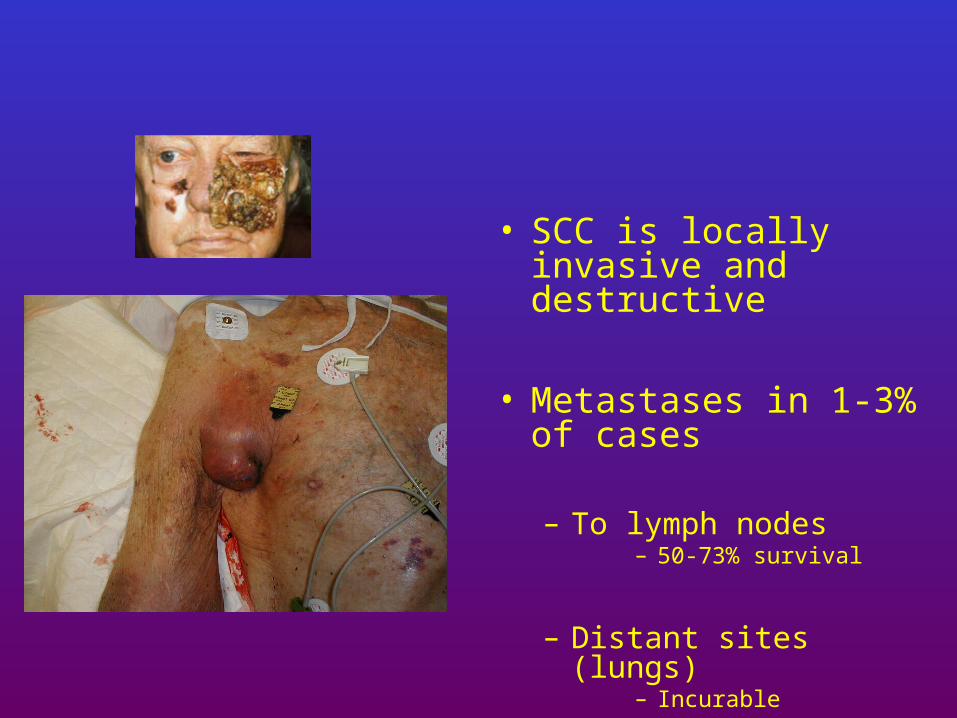
• SCC is locally invasive and destructive
• Metastases in 1-3% of cases
– To lymph nodes– 50-73% survival
– Distant sites (lungs)– Incurable
• Invasive squamous cell carcinoma
• Surgical excision– Traditional
– Mohs surgery
• Radiation therapy
Risk factors- MM• Fair skin, red hair, and blue eyes
• Intermittent sun exposure– Sunburns– Tanning beds
• Freckles and melanocytic nevi
• Family history of melanoma

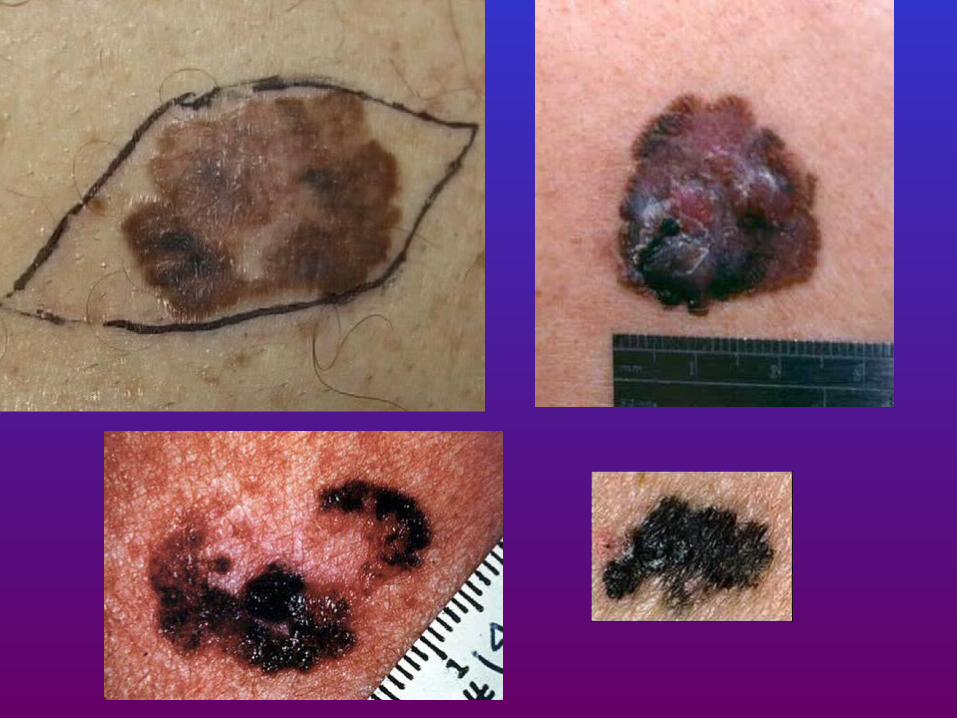
Clinical types- MM
Superficial spreading melanoma
Lentigo maligna melanoma
Acral lentiginous melanoma Nodular melanoma

ABCD of Melanoma
• Asymmetry
• Border irregularity
• Color variegation
• Diameter >6mm
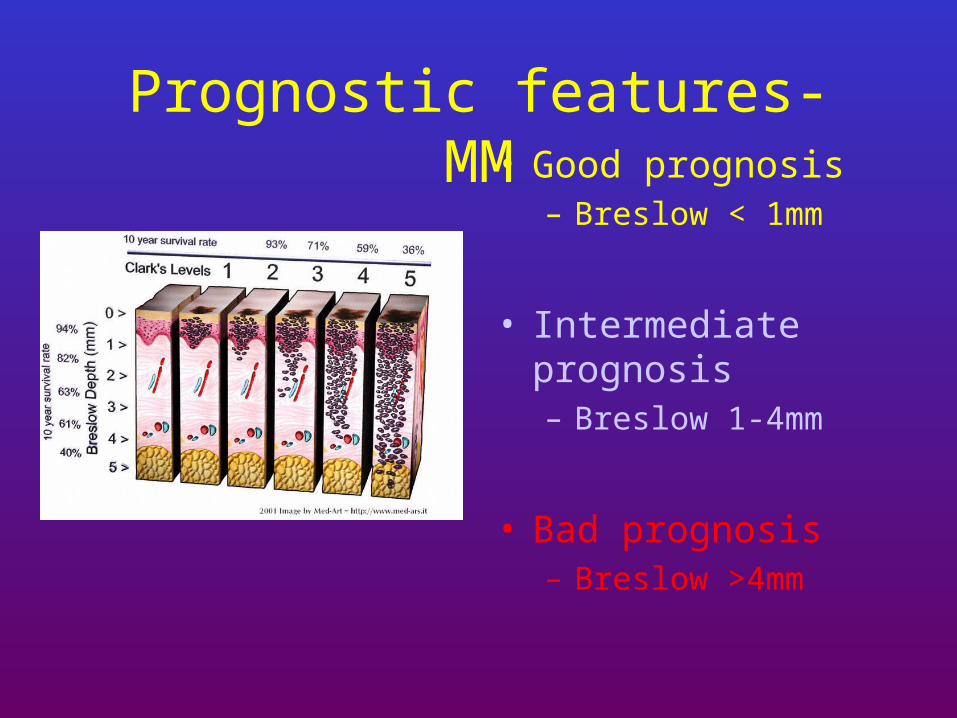
Prognostic features- MM• Good prognosis
– Breslow < 1mm
• Intermediate prognosis– Breslow 1-4mm
• Bad prognosis– Breslow >4mm
Treatment of MM
• Surgical excision
– In situ = 5 mm margin
– Invasive= 1-3 cm depending on Breslow’s depth





























