8/20/2019 Acute Urticaria Infancy
http://slidepdf.com/reader/full/acute-urticaria-infancy 1/3
ACUTE URTICARIA IN INFANCY
Thato MosidiM edical student, U niversity of Cape Tow n, South Africa
Leanne WongM edical student, Vrye U niversiteit, Am sterdam , TheN etherlands
Sue J essop,M B C hB, FF Derm (SA )Consultant, D ivision of D erm atology, U niversity of Cape Tow n, South Africa
IntroductionU rticaria, or hives, is a com m on disorder in the youn gchild. The characteristic clinical finding in urticaria is aw ell-circum scribe d, raised, erythe m atou s plaque ,w hich is typically evanescent and freque ntly show scentral pallor. The lesions are usually very p ruritic. Them ast cell is the key cell in urticaria. Its activation caus-
es the release of vasoactive m ediators, predom inan tlyhistam ine, leading to oedem a in the superficial derm is.There are m any causes of urticaria. H ow ever, in m anycases the cause rem ains unknow n. The causes ofurticaria can be classified as IgE -m ediated hypersensi-tivity reactions, chem ically induced m ast-cell degranu-lation, physical urticaria, arachidonic acid m etabolismand com plem en t-m ediated reactions (Table I). It isim portant to differentiate urticaria from erythem a m ulti-form e, w hich show s epiderm al necrosis, w ith the char-acteristic target-like appearance. W hile urticaria andangio-oe dem a (in w hich the oedem a is large ly in thesubcutaneous tissue) are clinically distinct en tities,they m ay be seen in the sam e p atient, either concur-rently or at different tim es during the illness.1 U rticariais defined as ‘acute u rticaria’if it lasts for less than 6
w eeks and ‘chronic urticaria’if it lasts for m ore than 6w eeks.
Case report A 6-m onth-old boy presented to the pae diatric derm a-tology clinic w ith a 3-day h istory of a generalised bodyrash. Prior to this presentation, he had a 4-day historyof sym ptom s suggestive o f an u pper resp iratory tractinfection for w hich he w as given am oxycillin and adecongestant con taining p seudoephedrine. Tw enty-four ho urs later the rash appeared. H e w as also fever-ish and irritable. This w as the first episode of such areaction and he had p reviously used the m ed icationw ithout any adverse effects.
The child further developed conjunctivitis 1 d ay afterthe rash appeared. H e had no o ther m edical or derm a-
tological history of note and had no know n allergies.H is m other is asthm atic.
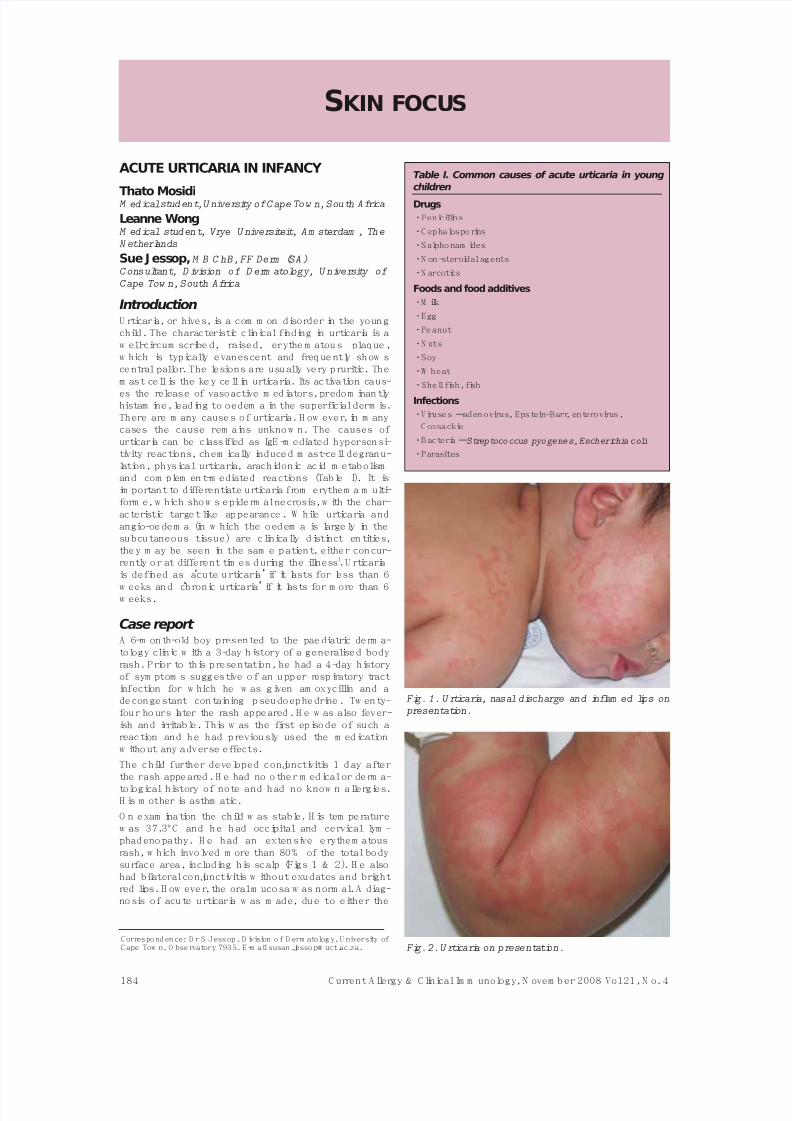
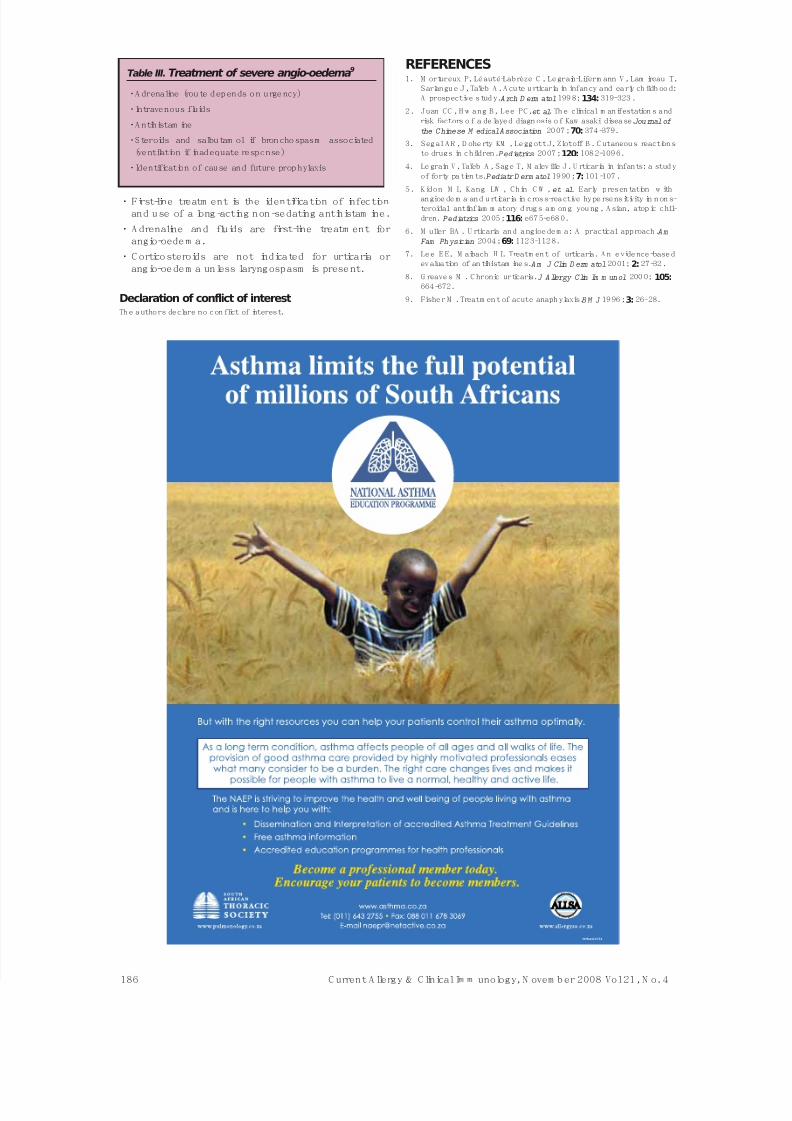
O n exam ination the child w as stable. H is tem peraturew as 37.3°C and he h ad occipital and cervical lym -phadeno pathy. H e had an extensive erythem atousrash, w hich involved m ore than 80% of the total bodysurface area, including his scalp (Figs 1 & 2). H e alsohad bilateral conjunctivitis w ithout exudates and brightred lips. H ow ever, the oral m ucosa w as norm al. A diag-no sis of acute u rticaria w as m ade, du e to either the
184 C urrent A llergy & Clinical Im m unology, N ovem b er 2008 Vol 21, N o. 4
SKIN FOCUS
C orrespondence: D r S Jessop, D ivision o f D erm atology, U niversity ofC ape Tow n, O bservatory 7935. E-m ail susan.jessop@ uct.ac.za.
Table I. Common causes of acute urticaria in young
children
Drugs
•Penicillins
•Cephalosporins
•Sulphonam ides
•N on-steroidal agents
•N arcotics
Foods and food additives
•M ilk
•Egg
•Peanut
•N uts
•Soy
•W heat
•Shell fish, fish
Infections
•Viruses –adenovirus, Epstein-Barr, enterovirus,
C oxsackie
•Bacteria –Streptococcus pyogenes, Escherichia coli
•Parasites
Fig. 1. U rticaria, nasal discharge and inflam ed lips on presentation.
Fig. 2. U rticaria on presentation.

8/20/2019 Acute Urticaria Infancy
http://slidepdf.com/reader/full/acute-urticaria-infancy 2/3
infection or the am oxycillin or both, and all m edicationw as stop pe d. In view of the brigh t red lips, extensiverash, conjun ctivitis, fever and aden opathy, Kaw asakisyndrom e w as also conside red in the differen tial diag-nosis; how ever the lack of hand oed em a or desquam a-tion, the short duration of fever and rapid clearing of theother clinical signs w ere thought to be against thisdiagno sis.2 The child w as adm itted and treated w ithtw o antihistam ine drugs (containing ch lorph en iram inem aleate and cetirizine dihydrochloride), erythrom ycin,paracetam ol and oxym etazoline h ydrochloride n asal
drops.W ithin the follow ing 4 days the child’s skin problemresolved alm ost com pletely, leaving a reticular appear-ance. (Fig. 3).
DiscussionIn our case, a 6-m onth-old infant de veloped extensiveurticaria 24 hours after starting treatm en t w ith am oxy-cillin for a resp iratory tract infection. Possible cause sfor this skin eruption w ou ld includ e bo th the und erlyinginfection and the therapy.
In a prospective hospital-based study of 56 children (0
to 36 m onths) w ith urticaria, M ortureuxet al.1
reportedthe com m on est association s to be viral infection (18cases) and m edication (12 cases).
1O ur patient patient
probably developed urticaria as a result of the respira-tory infection , althou gh the drug m ay have played a roleitself. It m ay have be en due to a com bination of infec-tion and therapy, as infection and drug e xposu re m ayact synergistically in som e cases.
Pure drug allergy is relatively uncom m on in you ng chil-dren, but m ay be com m oner in older children.3,4 In 6children, foo d allergy w as suspected and in othersthere w ere m ultiple possible causes, includ ing thecom bination of presum ed viral infection and drug ther-apy. Fo od allergy is relatively co m m on in babies, butviral infection m ay again be a co factor.1,4 M ortureux etal.1 found that the children w ith drug-induced urticarias
develope d the rash 6 to 10 days after starting w ith thetherapy. Som e of the children had used the drug previ-ously yet this w as their first skin reaction.
The drugs that m ost com m only cause an urticarial reac-tion in infants have bee n show n to be beta-lactam andsulphur-containing antibiotics and non-steroidal anti-inflam m atory drugs (N SA ID s). N SA ID s m ay causeurticaria by altering the m etabolism of arachidonic acid,w hich results in increased prod uction an d release ofleukotrienes. N SA ID s are also im plicated in causingangio-oedem a.5 U rticaria w ith angio-oedem a is also rel-atively com m on in children w ith food allergy.
Treatment of urticariaM edical m anage m en t is required in the early stages, toalleviate sym ptom s, although the aim should be toidentify and disco ntinue the o ffending agent in thecase of foo d or drug allergy. A ntihistam ines are them ainstay of therapy and should be given in adequatedoses to control the sym ptom s. The m ain groups ofantihistam ines com m on ly used in u rticaria are sh ow n inTable II. D uring the acute p hase o f the illness, oneshou ld g ive the antihistam ine s on a reg ular basis,according to half-life, rather than in response to the
severity of sym ptom s.
First-line therapy should be a non-sedating long-actingH 1 receptor blocker6 (see Table II). The approach tourticaria in general is dictated by clinical se ve rity andresp onse but one should add further agents until con-trol is achieved, w hile continuing to try to identify theun derlying cause. If a single agent does not control thesym ptom s, a second an tihistam ine such as one of theolder sedating group m ay be added at night. There isno evidence to show that one antihistam ine is superiorto any other in this condition.
7Th e addition of an H2
receptor blocker such as cim etidine or ranitidine iscom m on practice in chronic urticaria and is suppo rtedby a co ntrolled trial.8 Topical antihistam ines andsteroids have n o role in the treatm ent of urticaria. O ralsteroids are gene rally undesirable, except in the m an-
agem ent of severe angio-oedem a, as rebound urticarialw eals tend to be a problem w hen the m edication isw ithdraw n.
A dverse effects such as drow siness, dry m outh andurinary retention are frequent w ith the older sedatingantihistam ine s, altho ugh less prom inent in children,w ho m ay even show paradoxical restlessness and
excitem ent w ith som e antihistam ines.A ngio-oedem a in children w ith urticaria w ill usuallyrespond to the sam e m easures. H ow ever w hen angio-oedem a affects the airw ay or is associated w ith shock,urgent em ergency treatm ent is required , w ith adrena-line and intravenous fluids
9(Table III).
Key points• Infection is the com m one st cause of acute urticaria
in you ng children .
• D rug and food allergy m ay also occur or m ay have asynergistic effect.
C urrent A llergy & Clinical Im m unology, N ovem ber 2008 Vol 21, N o. 4 185
Fig. 3. Clearing of urticaria on day 4.Table II. Antihistamine therapy for acute urticaria
(A dd from each g rou p increm en tally if req uired )
N on-sedating H 1 recep tor blocker
•Cetirizine
•Levocetirizine
•Loratadine
•D esloratidine
•Fexofenadine
Sedating H 1 receptor blocker
•Alkylam ine, e.g. m ep yram ine , chlorphen iram ine
•Phenothiazine , e.g. prom ethazine
•Piperazine, e.g. hydroxyzine
•Cyproheptadine
H 2 receptor blocker
•Cim etidine
•Ranitidine
8/20/2019 Acute Urticaria Infancy
http://slidepdf.com/reader/full/acute-urticaria-infancy 3/3
• First-line treatm ent is the identification of infectionand use of a long -acting non -sedating antihistam ine.
• A drenaline and fluids are first-line treatm ent forangio-oede m a.
• C orticosteroids are not indicated for urticaria orangio-oedem a unless laryngospasm is present.
Declaration of conflict of interestTh e authors declare no con flict of interest.
REFERENCES1. M ortureux P, Léauté-Labrèze C , Legrain-Liferm ann V, Lam ireau T,
Sarlangu e J, Taïeb A . A cute urticaria in infancy and early childh ood:A prospective study.Arch D erm atol199 8;134: 319-323.
2. Juan CC , H w ang B, Lee PC,et al. Th e clinical m anifestation s andrisk factors o f a delayed diagn osis of Kaw asaki disease. Journal of the Chinese M edical Association 2007;70: 374-379.
3. Segal A R , D ohe rty KM , Leggott J, Zlotoff B . C utaneous reactionsto drugs in children.Pediatrics 2007;120: 1082-1096.
4. Le grain V, Taïeb A , Sage T, M aleville J. U rticaria in infants: a studyof forty patien ts.Pediatr D erm atol1990;7: 101-107.
5. Kidon M I, Kang LW , Chin C W , et al. Early presen tation w ith
angioe de m a and urticaria in cross-reactive hype rsensitivity in non s-teroidal antiinflam m atory d rugs am ong you ng, A sian, atopic chil-dren. Pediatrics 2005;116: e675-e680.
6. M uller BA . U rticaria and angioedem a: A practical approach. AmFam Physician 2004;69: 1123-1128.
7. Lee E E, M aibach H I. Treatm ent of urticaria. A n evidence-basedevaluation of an tihistam ine s.Am J Clin D erm atol2001;2: 27-32.
8. G reaves M . C hronic urticaria. J Allergy Clin Im m unol 200 0; 105:664-672.
9. Fisher M . Treatm ent of acute anaphylaxis.BM J 1996;3: 26-28.
186 C urrent A llergy & Clinical Im m unology, N ovem b er 2008 Vol 21, N o. 4
Table III.Treatment of severe angio-oedema9
•Adrenaline (route depends o n urgency)
•Intravenous fluids
•Antihistam ine
•Steroids and salbutam ol if bronchospasm associated
(ventilation if inadequate response)
•Identification of cause and future prophylaxis
Recommended

















