Điều trị Tăng huyết áp
trên bệnh nhân Bệnh thận mạn
PGS. TS. BS. CHÂU NGỌC HOA
BỘ MÔN NỘI - ĐHYD

Hypertension remains the first cause of death
Série 1
High blood pressure
Smoking
High cholesterol
High BMI
Physical inactivity
Alcohol
0 3.25 6.5 9.75 13
Adapted from Ezzati et al. Lancet. 2002;360:1347-1360.
Attributable mortality (in percent) of 56 000 000 deaths in year 2000
7 million deaths
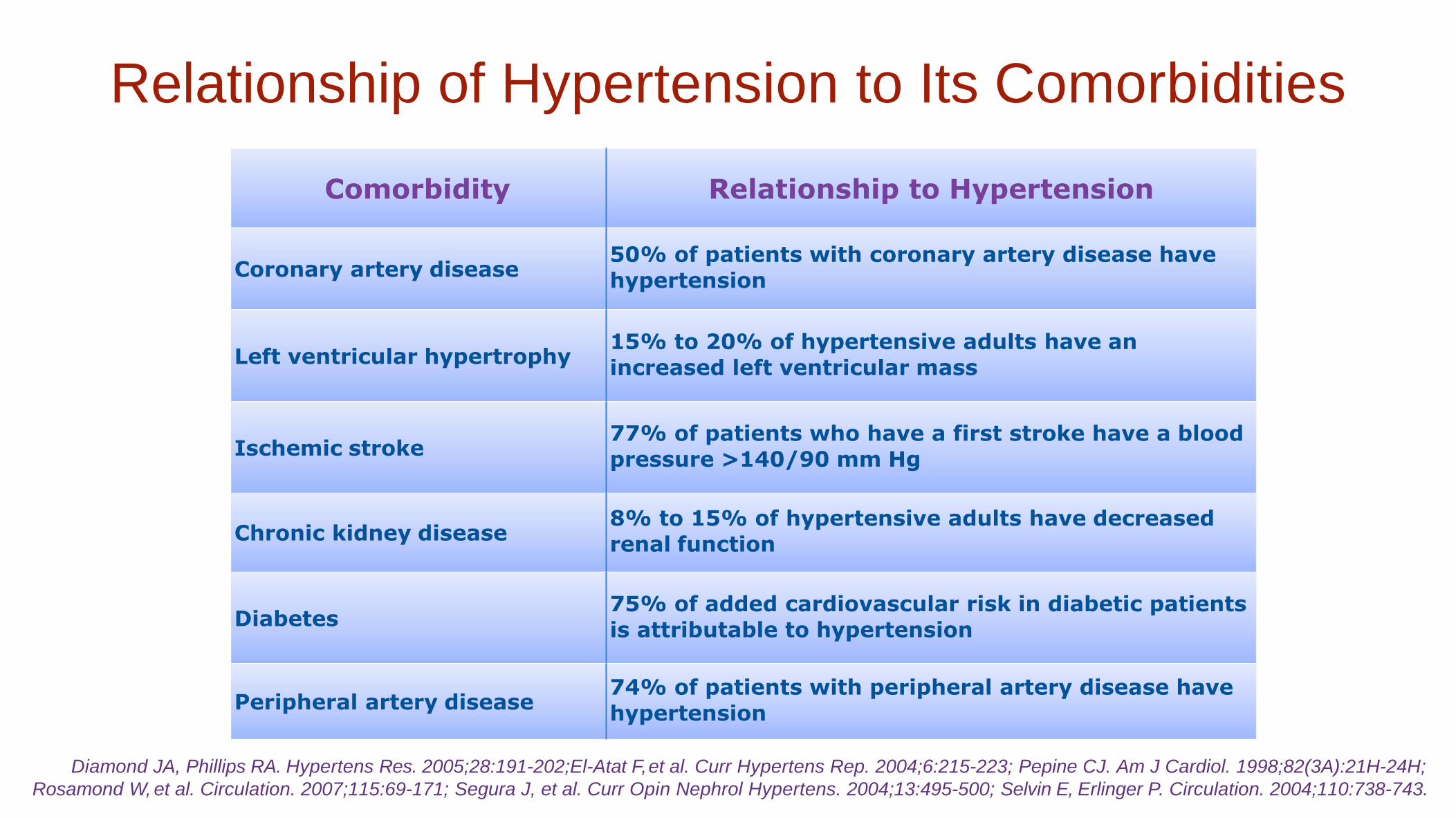
Relationship of Hypertension to Its Comorbidities
Comorbidity Relationship to Hypertension
Coronary artery disease 50% of patients with coronary artery disease have
hypertension
Left ventricular hypertrophy 15% to 20% of hypertensive adults have an
increased left ventricular mass
Ischemic stroke 77% of patients who have a first stroke have a blood
pressure >140/90 mm Hg
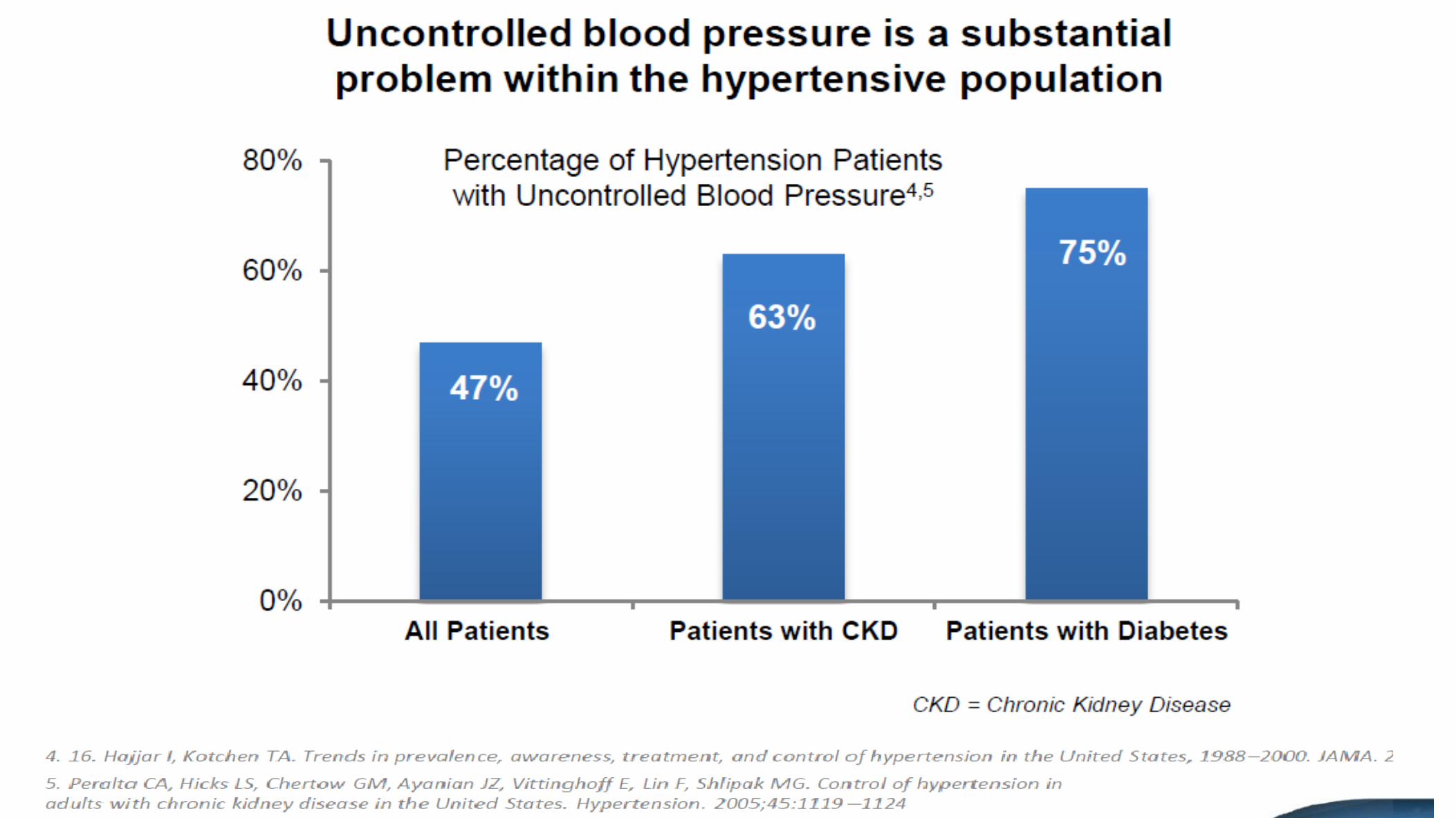
Chronic kidney disease 8% to 15% of hypertensive adults have decreased
renal function
Diabetes 75% of added cardiovascular risk in diabetic patients
is attributable to hypertension
Peripheral artery disease 74% of patients with peripheral artery disease have
hypertension
Diamond JA, Phillips RA. Hypertens Res. 2005;28:191-202;El-Atat F, et al. Curr Hypertens Rep. 2004;6:215-223; Pepine CJ. Am J Cardiol. 1998;82(3A):21H-24H;
Rosamond W, et al. Circulation. 2007;115:69-171; Segura J, et al. Curr Opin Nephrol Hypertens. 2004;13:495-500; Selvin E, Erlinger P. Circulation. 2004;110:738-743.

TĂNG HUYẾT ÁP- BỆNH THẬN MẠN
Chronic Kidney Disease in the US
Over 20 Million Americans have some degree of renal
insufficiency….1 in 8 people.
20 million others are at risk
Hypertension & Diabetes are the leading causes of kidney failure
• 23% of all Americans have hypertension
• 16 million Americans have diabetes
Both are independent risk factors for cardiovascular disease

Incidence by Race
2008
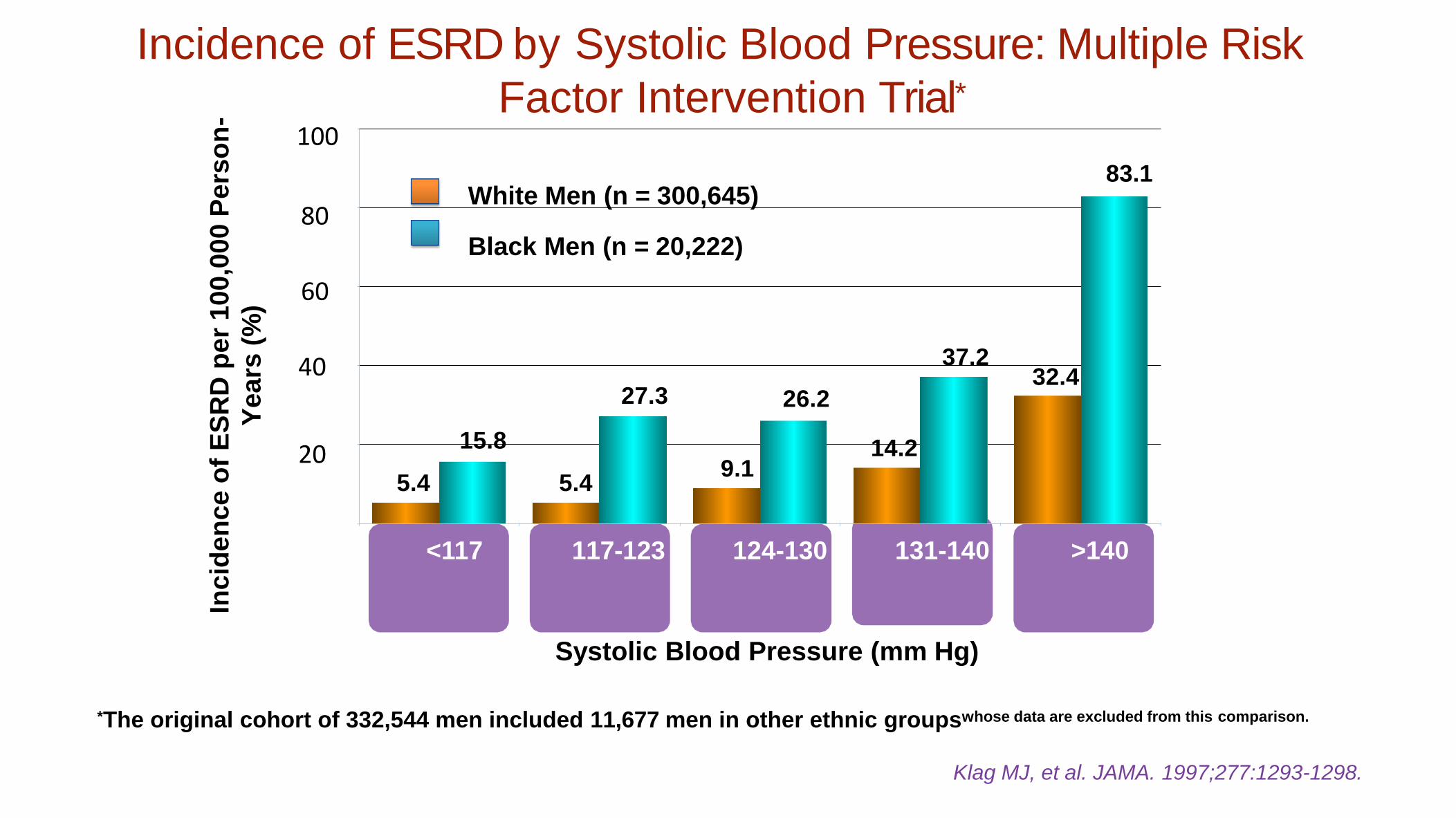
Incidence of ESRD by Systolic Blood Pressure: Multiple Risk
Factor Intervention Trial*
Systolic Blood Pressure (mm Hg)
*The original cohort of 332,544 men included 11,677 men in other ethnic groupswhose data are excluded from this comparison.
Klag MJ, et al. JAMA. 1997;277:1293-1298.
<117
White Men (n = 300,645)
Black Men (n = 20,222)
117-123 124-130 131-140 >140
5.4
15.8
5.4 9.1
14.2
32.4 27.3 26.2
37.2
83.1
20
40
60
80
100
Inc
ide
nc
e o
f E
SR
D p
er
10
0,0
00
Pe
rso
n-
Ye
ars
(%
)
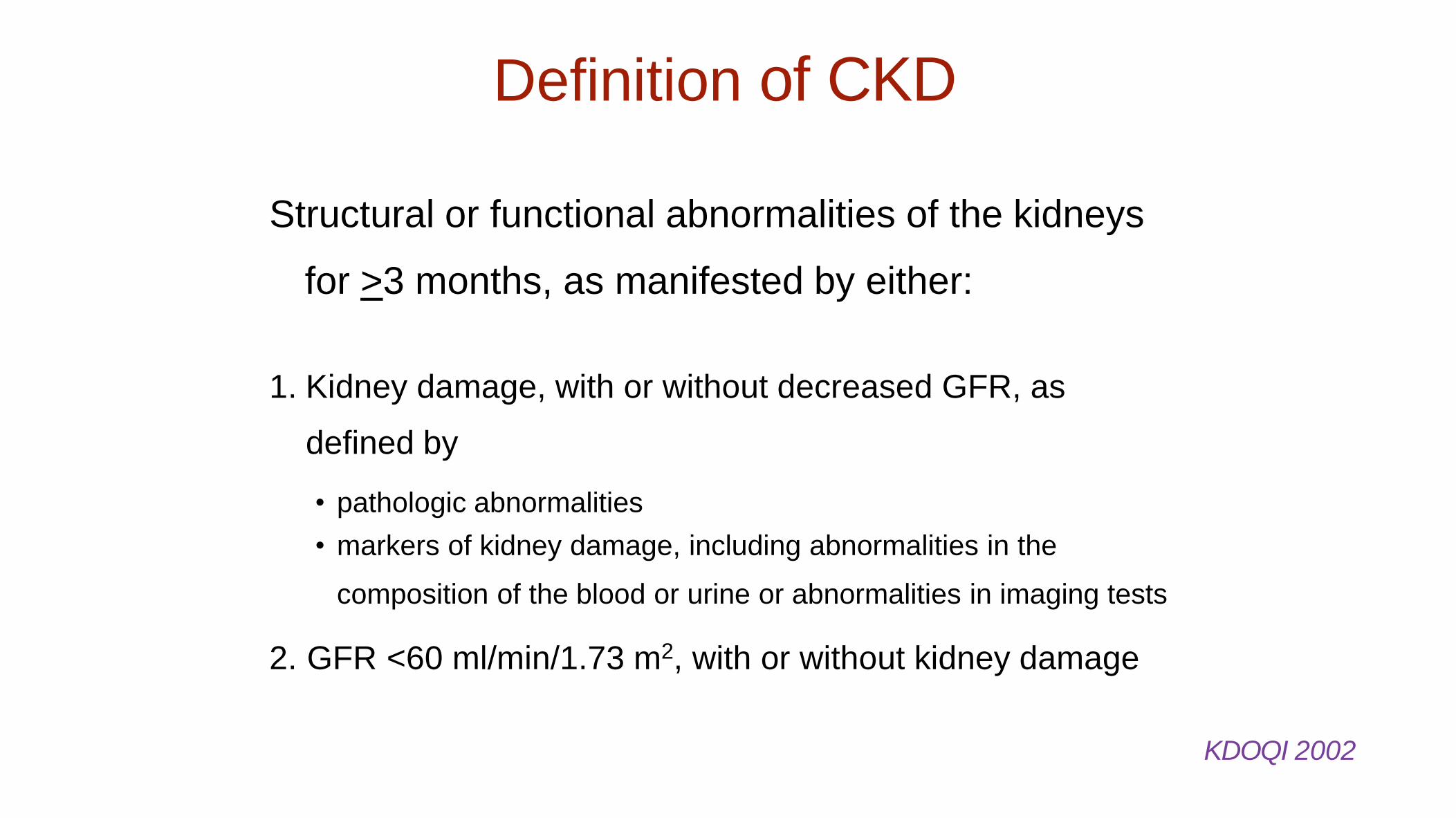
Definition of CKD
Structural or functional abnormalities of the kidneys
for >3 months, as manifested by either:
1. Kidney damage, with or without decreased GFR, as
defined by
• pathologic abnormalities
• markers of kidney damage, including abnormalities in the
composition of the blood or urine or abnormalities in imaging tests
2. GFR <60 ml/min/1.73 m2, with or without kidney damage
KDOQI 2002

Định nghĩa bệnh thận mạn theo KDIGO 2012
Bệnh thận mạn là những bất thường về cấu trúc và chức năng thận kéo dài trên 3 tháng, ảnh hưởng lên sức khỏe của bn
Bệnh thận mạn được phân lọai theo CGA
Nguyên nhân (Cause)
Độ lọc cầu thận (GFR) Albumine
niệu (Albuminuria)
Ví dụ: C(THA) G3a A Kidney Disease Improving Global Outcome 2012
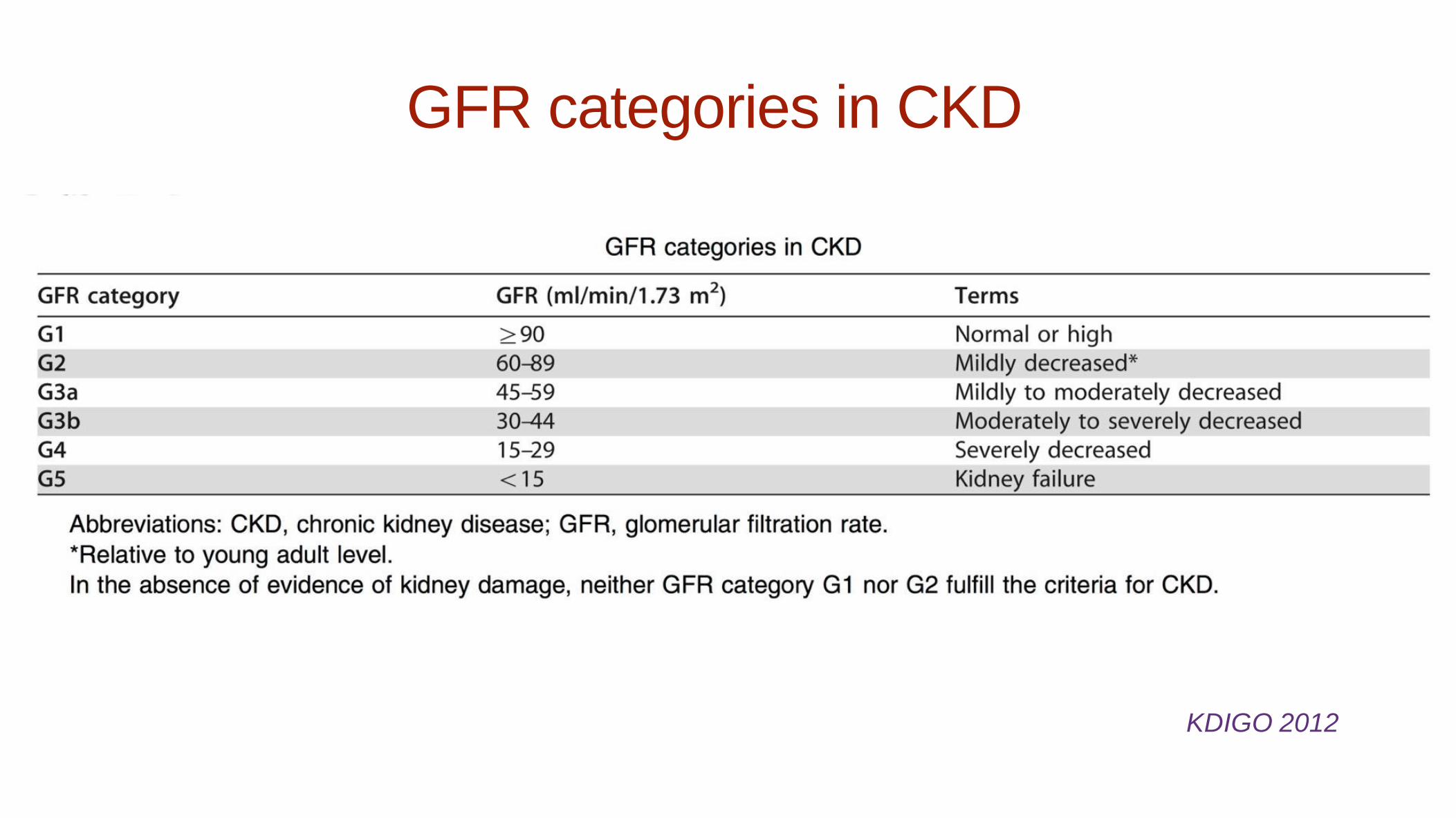
GFR categories in CKD
KDIGO 2012
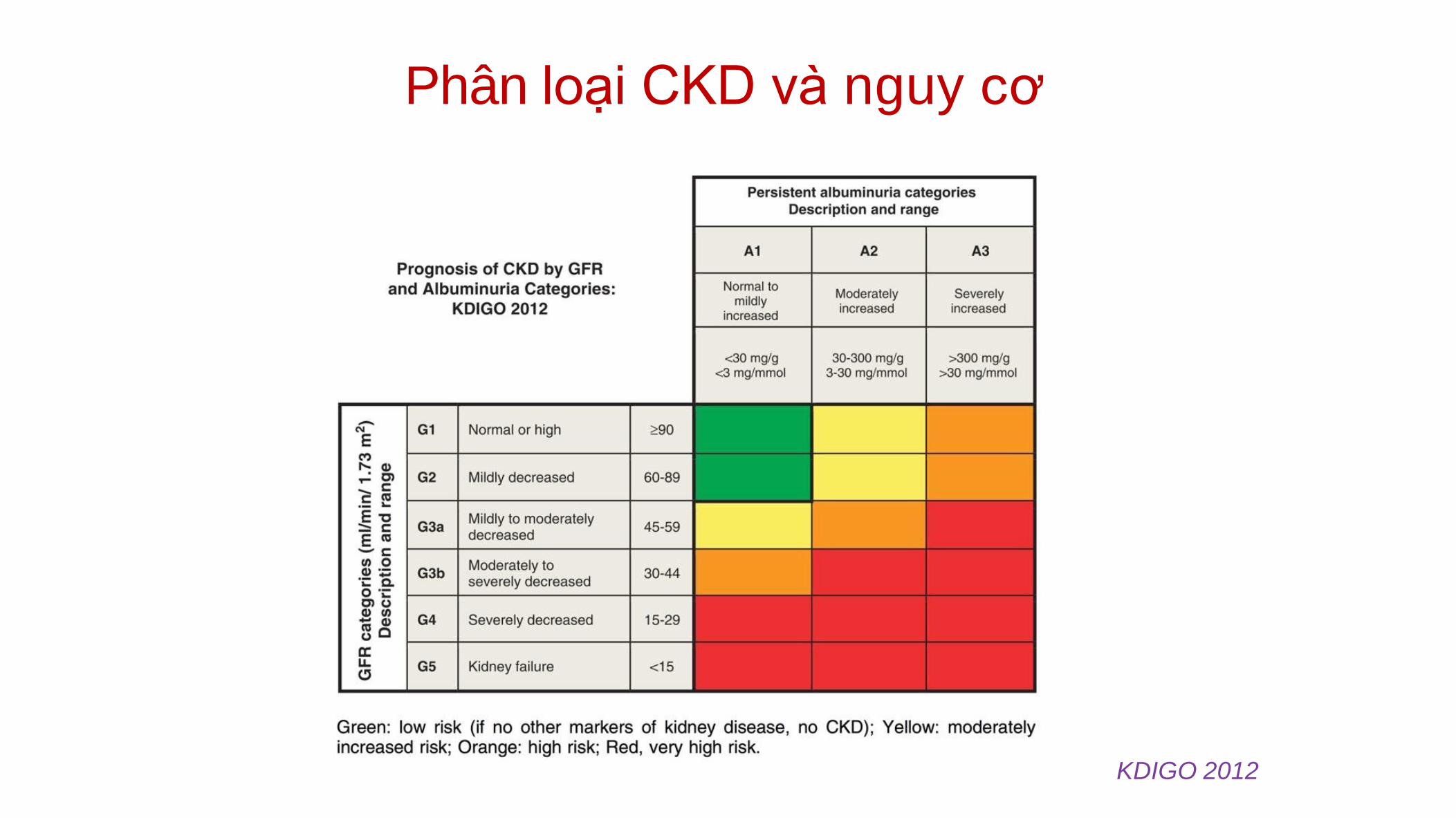
Phân loại CKD và nguy cơ
KDIGO 2012
2 screening tests
• eGFR
• ACR Albumin/
Creatinine ratio
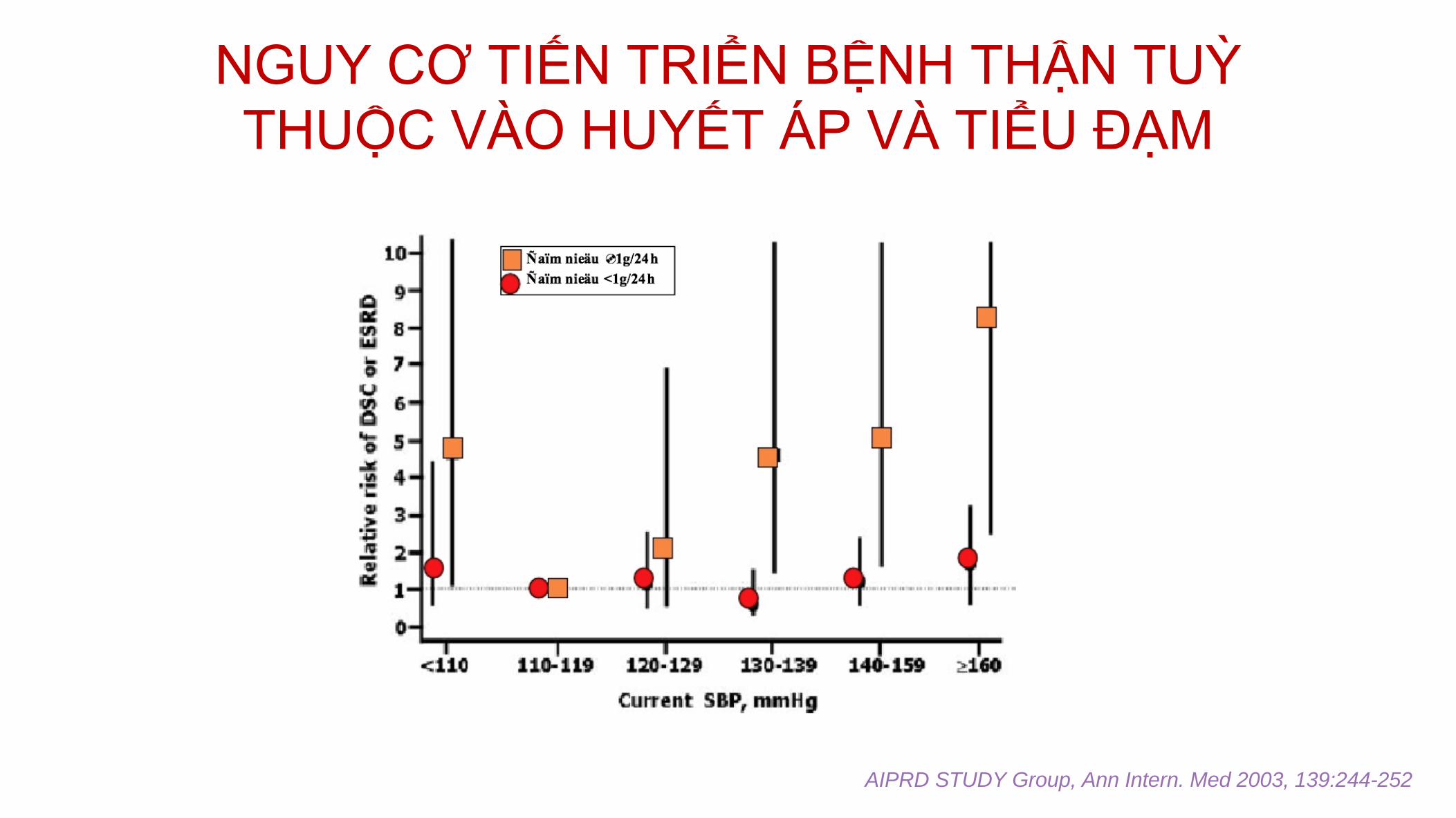
NGUY CƠ TIẾN TRIỂN BỆNH THẬN TUỲ
THUỘC VÀO HUYẾT ÁP VÀ TIỂU ĐẠM
AIPRD STUDY Group, Ann Intern. Med 2003, 139:244-252
Management of Hypertension in
Chronic Kidney Disease
• Non-pharmacological treatment
• Blood pressure goal
• Pharmacological treatment
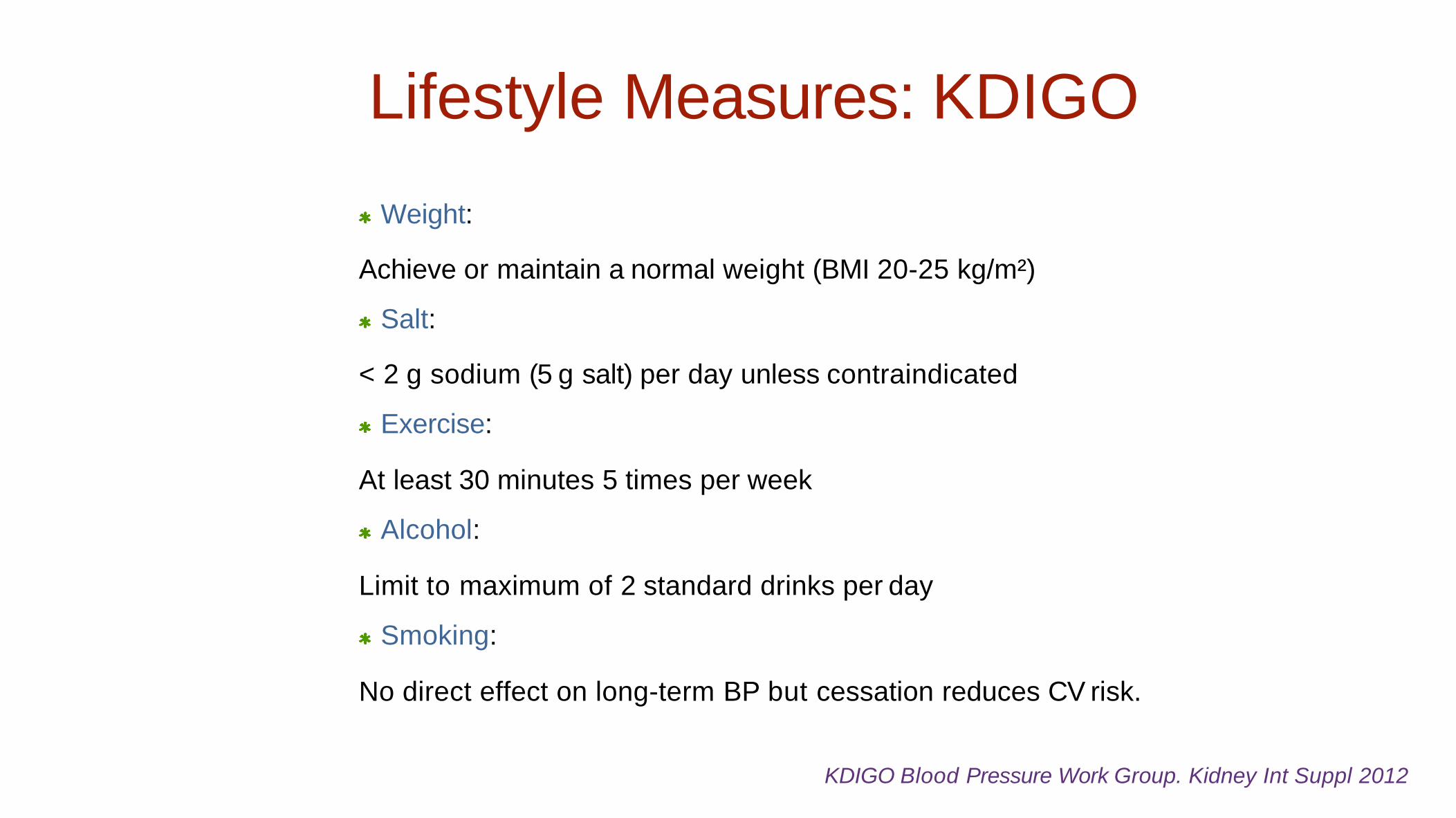
KDIGO Blood Pressure Work Group. Kidney Int Suppl 2012
Lifestyle Measures: KDIGO
Weight:
Achieve or maintain a normal weight (BMI 20-25 kg/m²)
Salt:
< 2 g sodium (5 g salt) per day unless contraindicated
Exercise:
At least 30 minutes 5 times per week
Alcohol:
Limit to maximum of 2 standard drinks per day
Smoking:
No direct effect on long-term BP but cessation reduces CV risk.
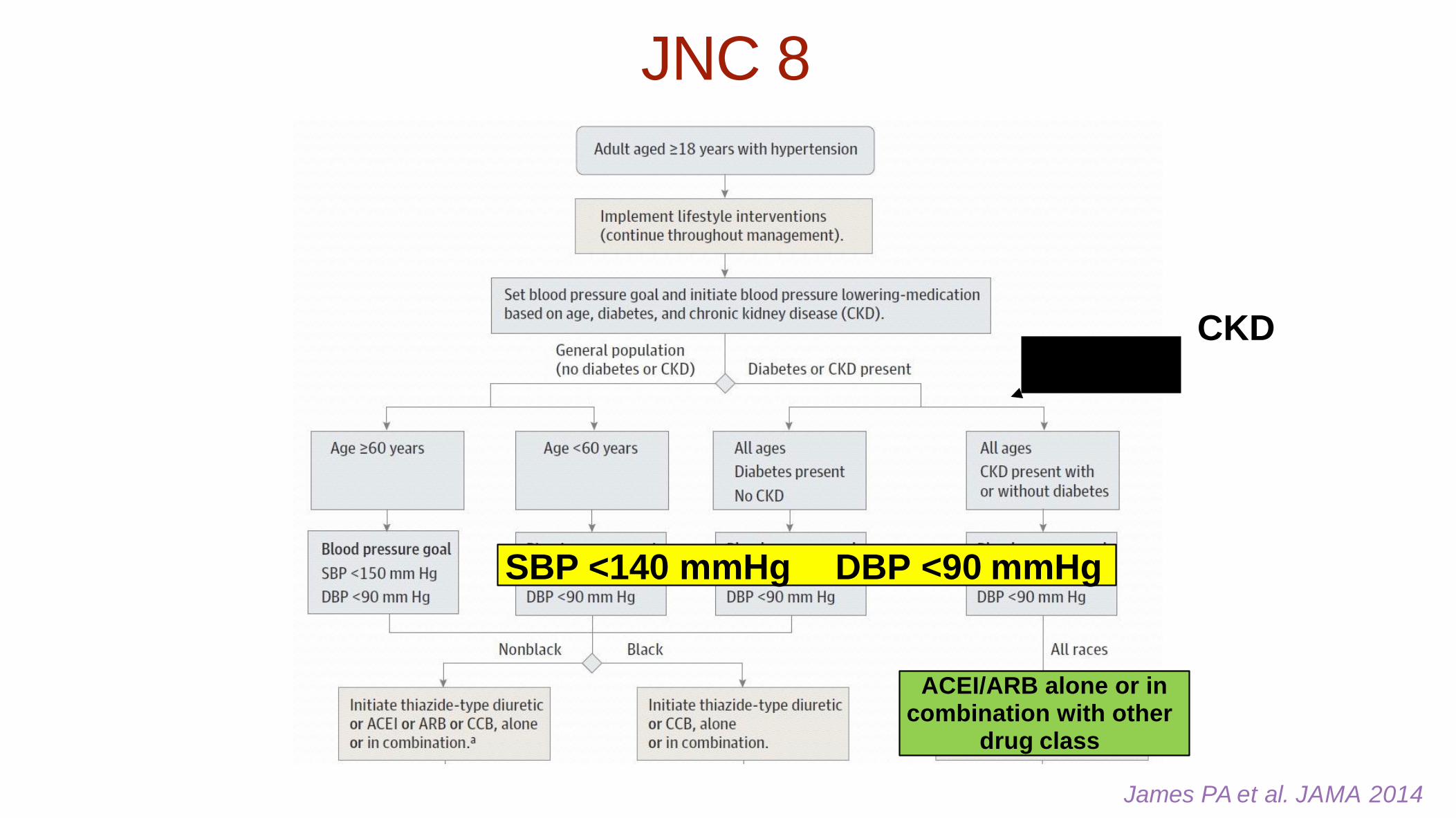
James PA et al. JAMA 2014
KD C
SBP <140 mmHg DBP <90 mmHg
ACEI/ARB alone or in combination with other
drug class
JNC 8
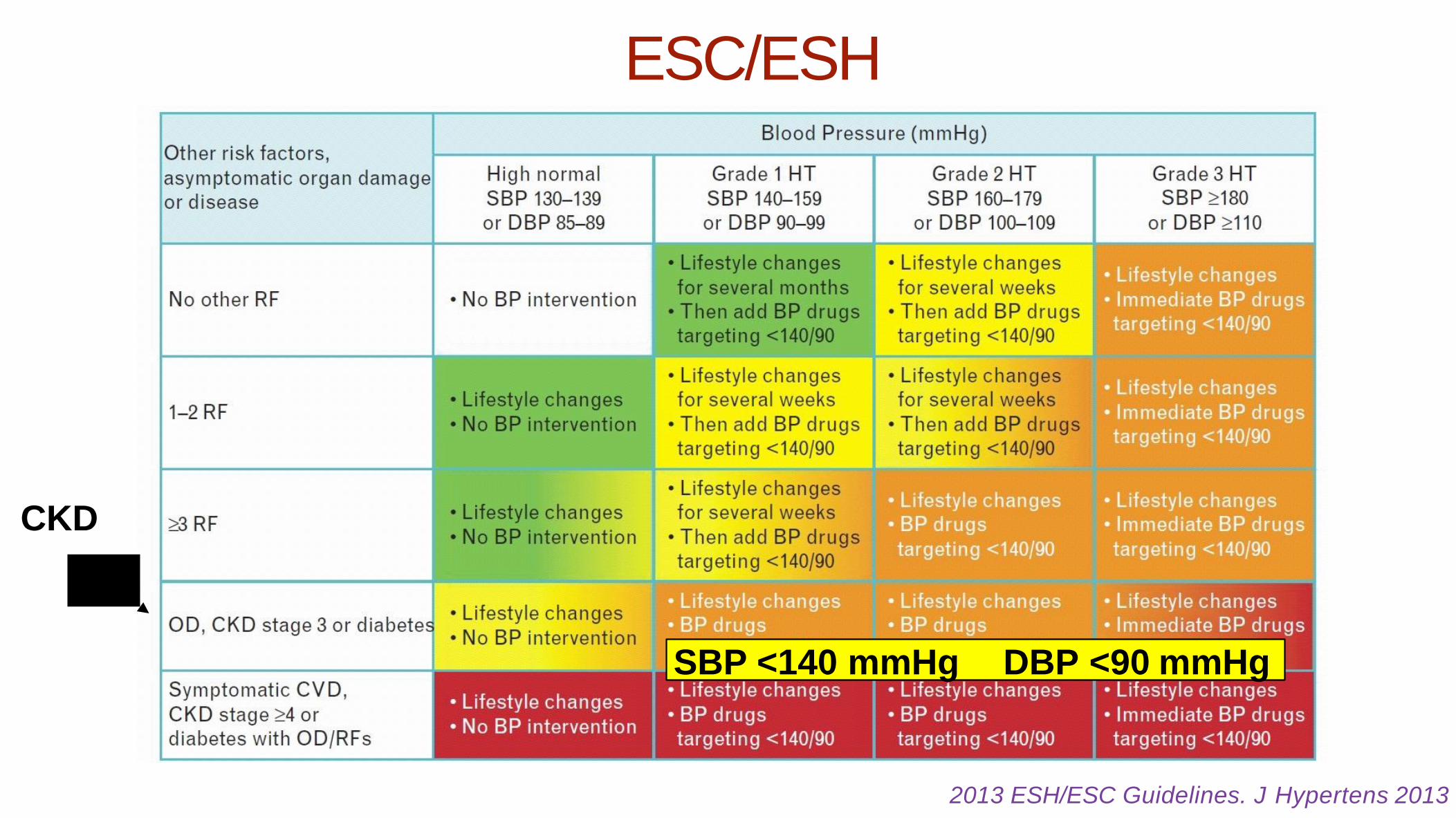
2013 ESH/ESC Guidelines. J Hypertens 2013
SBP <140 mmHg DBP <90 mmHg
CKD
ESC/ESH
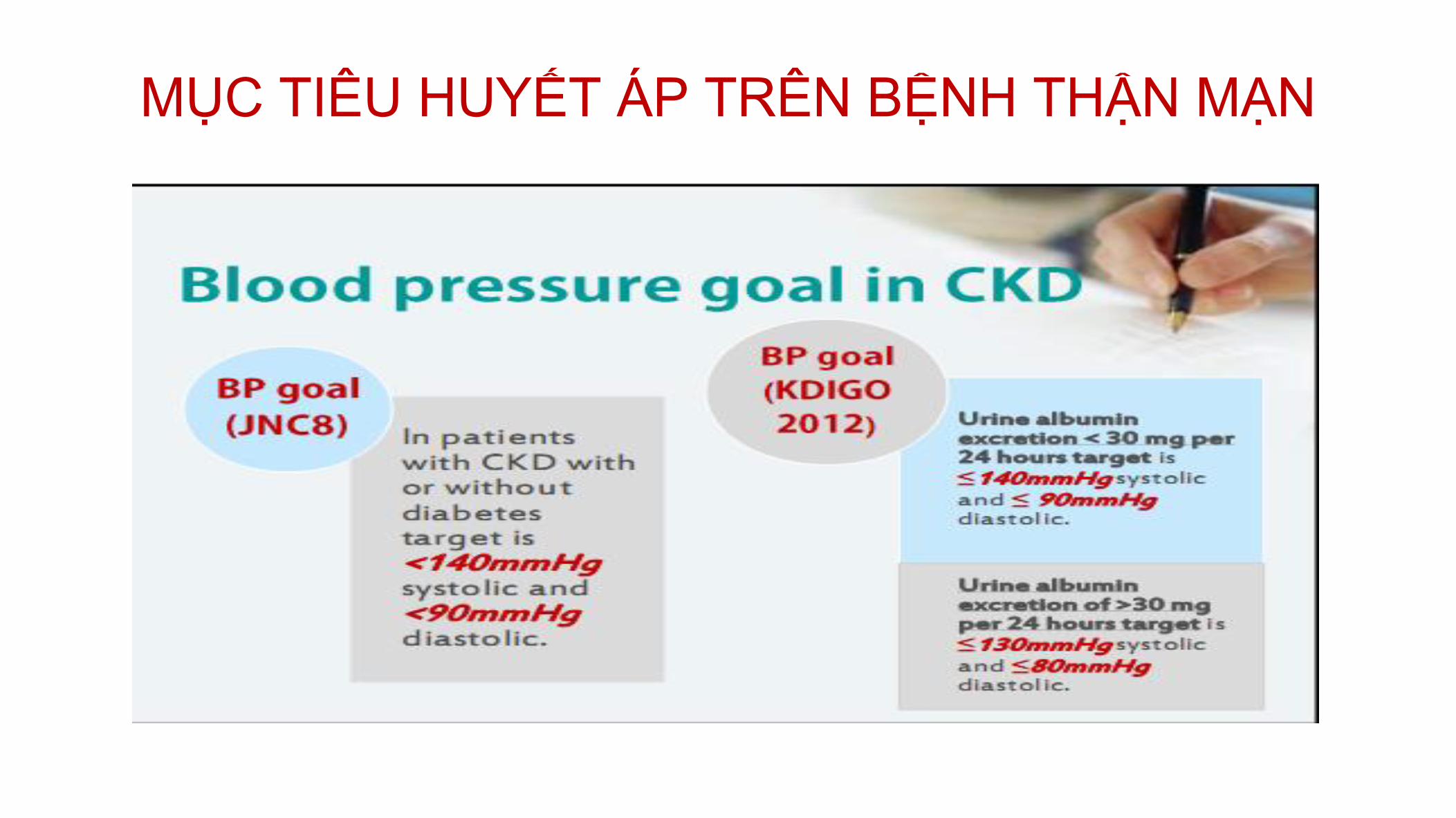
MỤC TIÊU HUYẾT ÁP TRÊN BỆNH THẬN MẠN

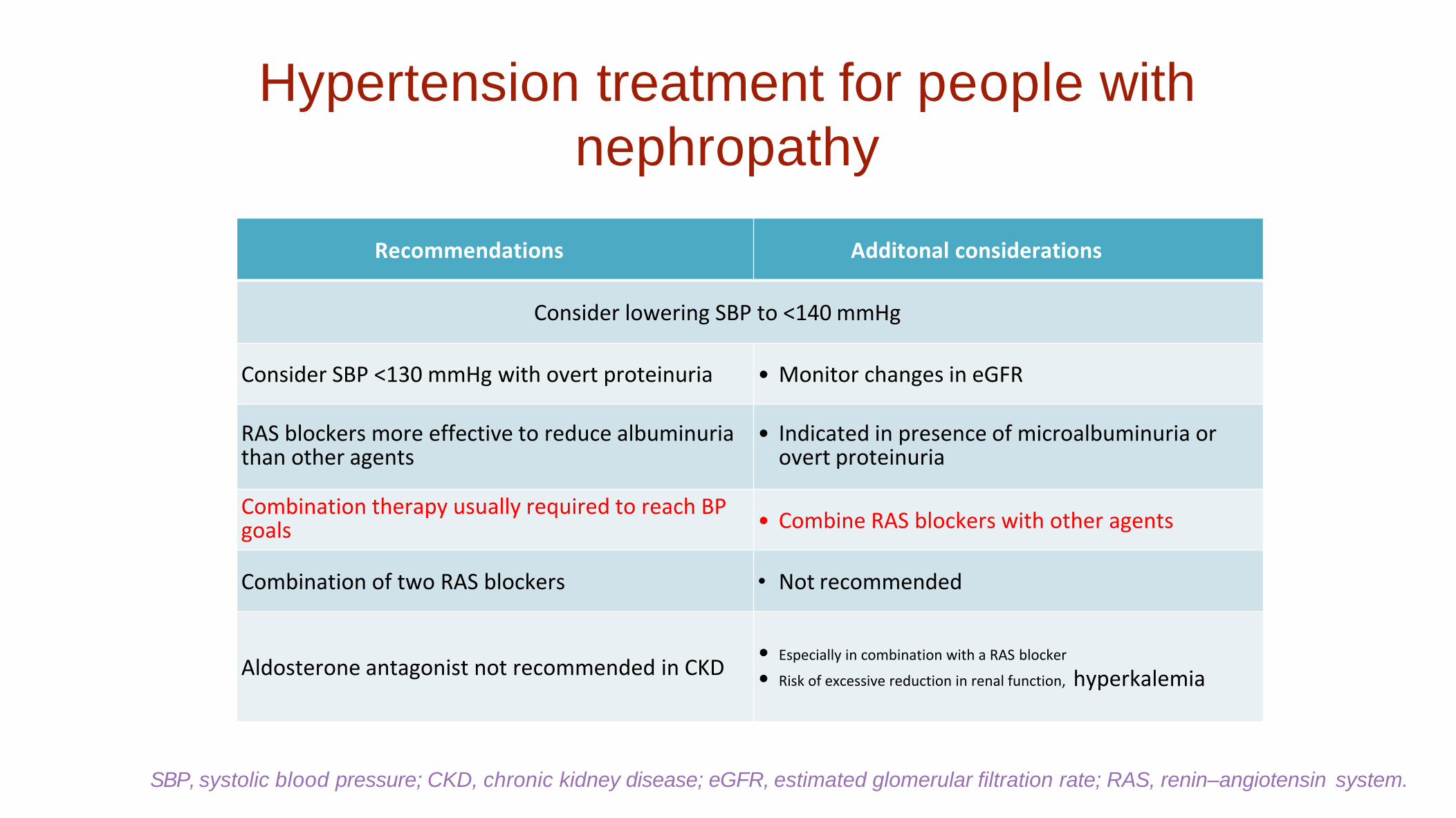
Hypertension treatment for people with
nephropathy
Recommendations Additonal considerations
Consider lowering SBP to <140 mmHg
Consider SBP <130 mmHg with overt proteinuria • Monitor changes in eGFR
RAS blockers more effective to reduce albuminuria than other agents
• Indicated in presence of microalbuminuria or overt proteinuria
Combination therapy usually required to reach BP goals
• Combine RAS blockers with other agents
Combination of two RAS blockers • Not recommended
Aldosterone antagonist not recommended in CKD • Especially in combination with a RAS blocker
• Risk of excessive reduction in renal function, hyperkalemia
SBP, systolic blood pressure; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; RAS, renin–angiotensin system.

Xơ hoá cầu
thận
Tăng huyết áp mao
mạch cầu thận
Tổn thương cầu thận do áp lực lọc
Stress oxy hoá
Bệnh thận mạn
Gây tăng trưởng tế bào
Gây viêm
Angiotensin II
Brewster, Perazella. Am J Med 2004;116:263–272
Giảm nephron
Vai trò trung tâm của Angiotensin II trong bệnh thận
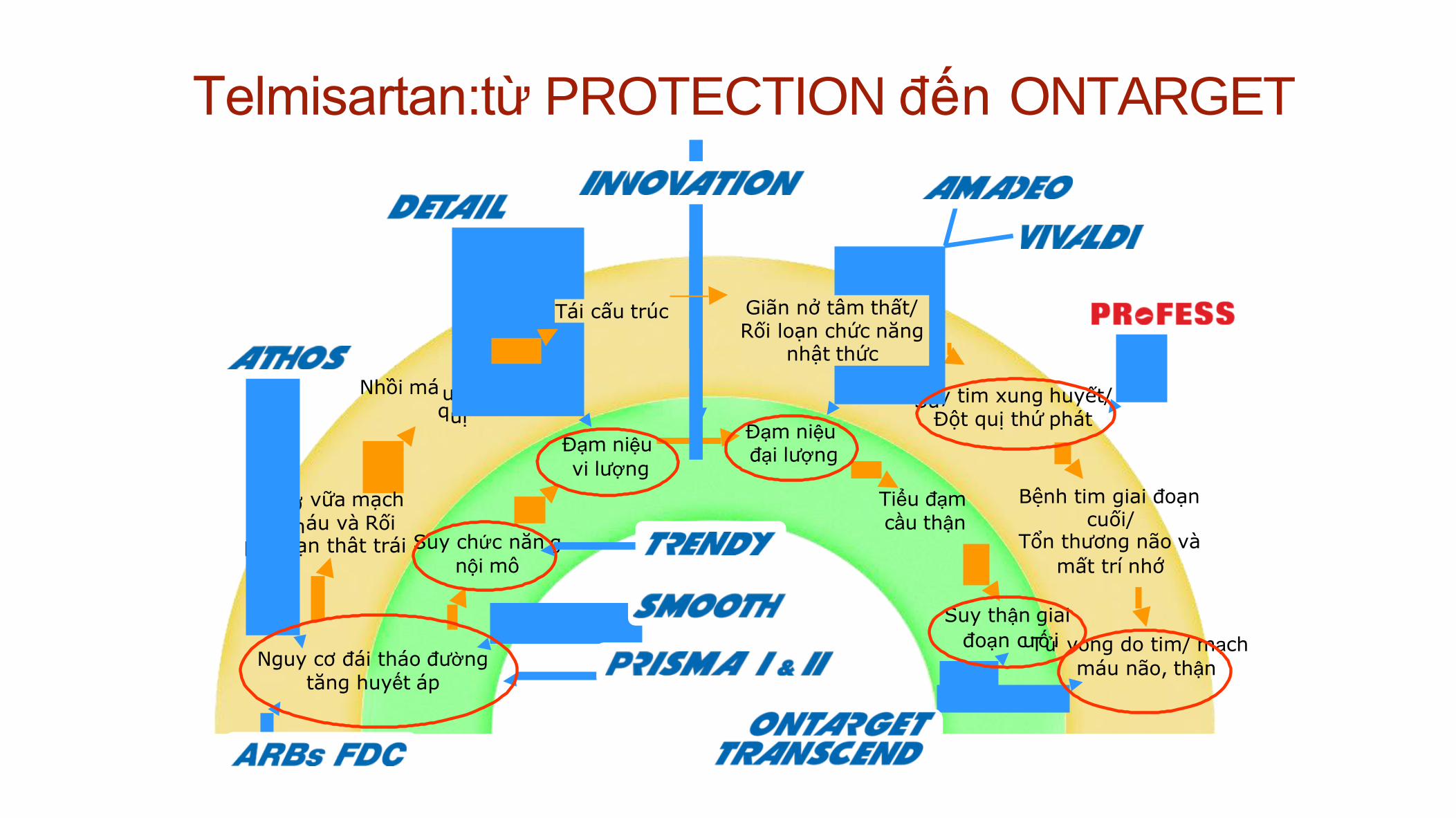
Telmisartan:từ PROTECTION đến ONTARGET
máu não, thận
Bệnh tim giai đoạn cuối/
Tổn thương não và
mất trí nhớ
Suy thận giai
đoạn cuTốửi vong do tim/ mạch
g nội mô
Đạm niệu
vi lượng
Su y tim xung huyết/
Đột quị thứ phát
Tiểu đạm
cầu thận
Đạm niệu đại lượng
Nhồi má
q
u cơ & Đột uị
vữa mạch
áu và Rối
Xơ m
lo ạn thât trái Suy chức năn
Giãn nở tâm thất/ Rối loạn chức năng
nhật thức
Tái cấu trúc
Nguy cơ đái tháo đường
tăng huyết áp
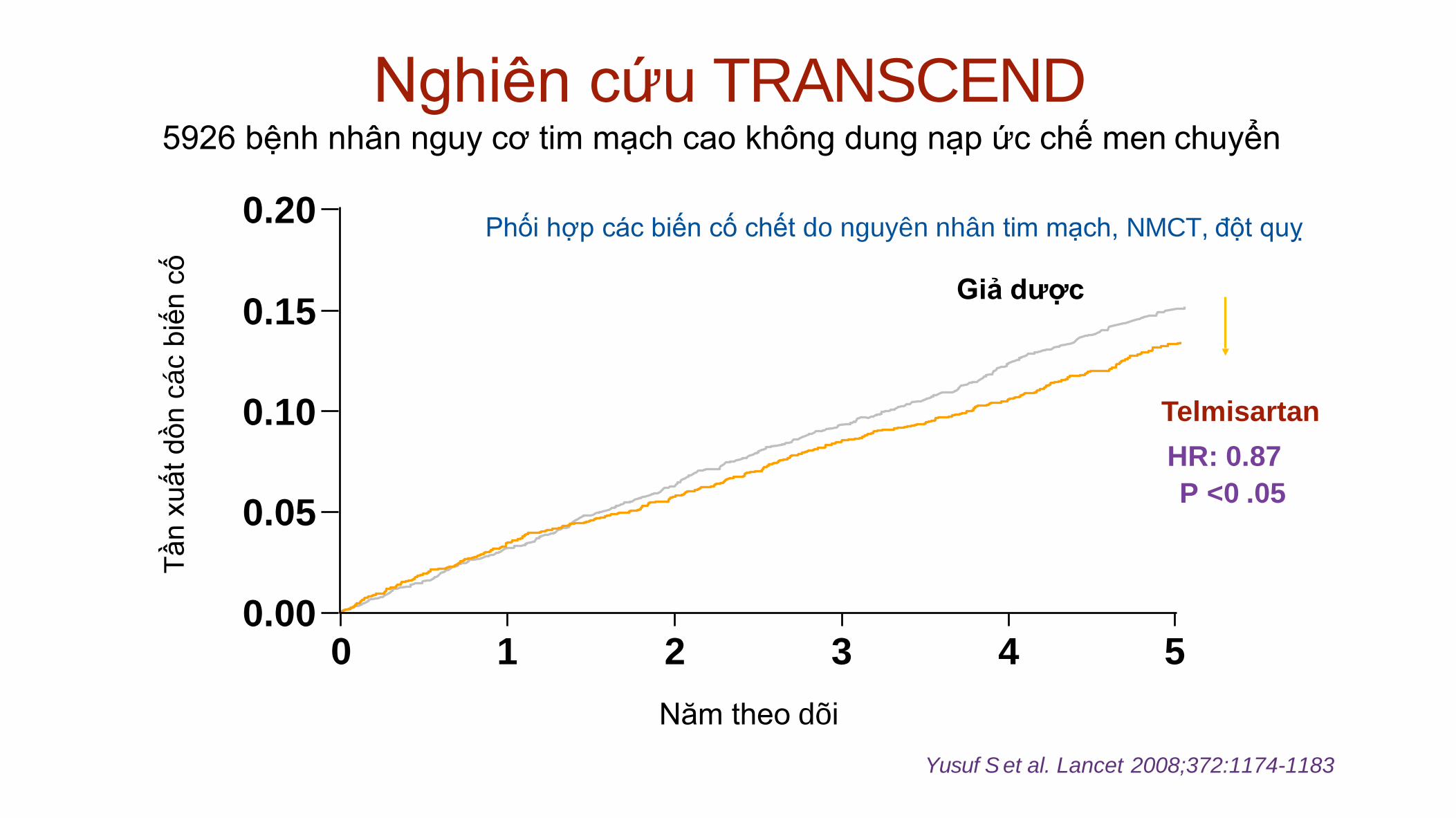
Nghiên cứu TRANSCEND 5926 bệnh nhân nguy cơ tim mạch cao không dung nạp ức chế men chuyển
0.20
0.15
0.10
0.05
0.00 0 1 4 5
Tần x
uất
dồn c
ác b
iến c
ố
Giả dược
Telmisartan
HR: 0.87
P <0 .05
2 3
Năm theo dõi
Yusuf S et al. Lancet 2008;372:1174-1183
Phối hợp các biến cố chết do nguyên nhân tim mạch, NMCT, đột quỵ
0
18
35
53
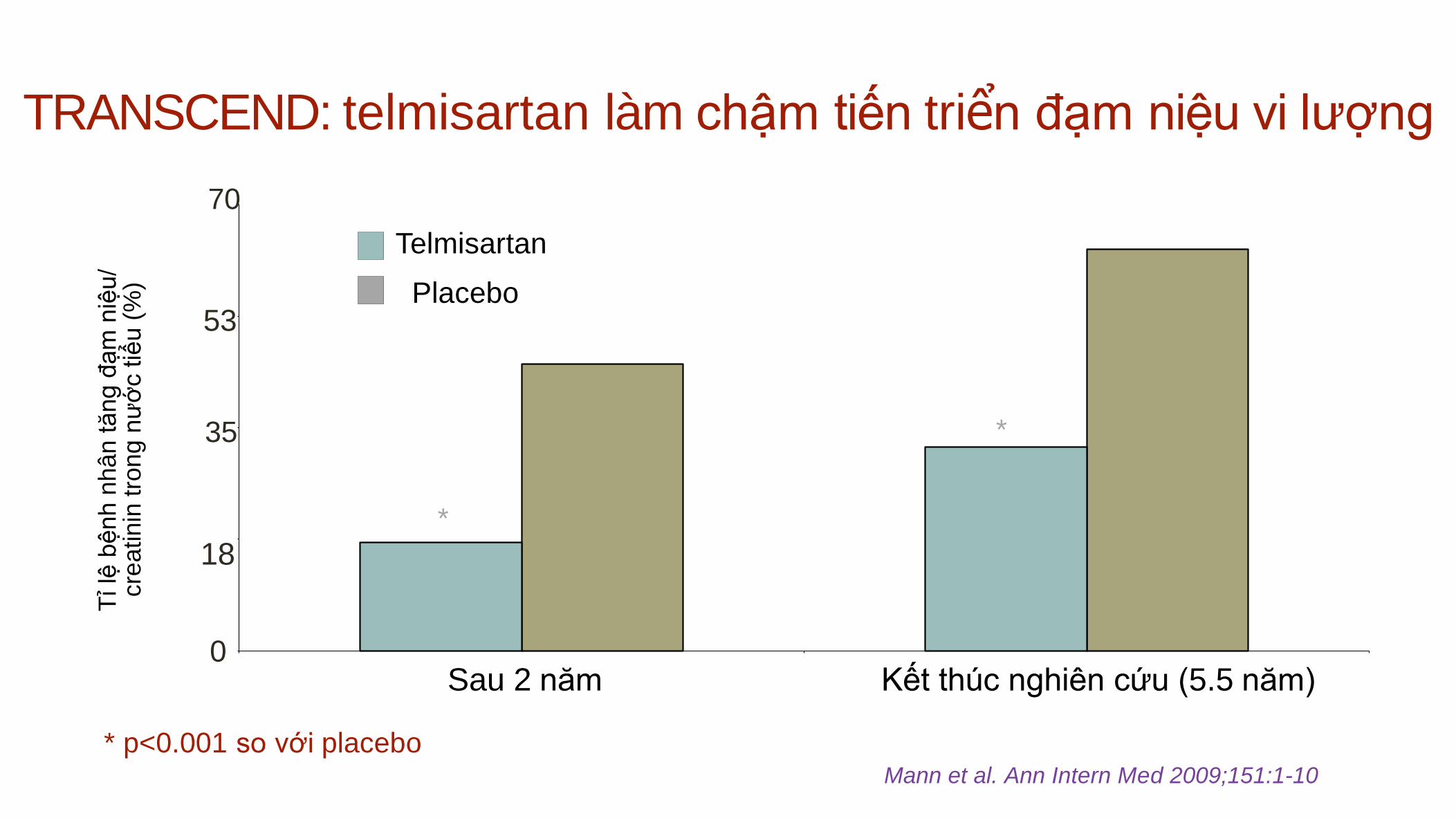
TRANSCEND: telmisartan làm chậm tiến triển đạm niệu vi lượng T
ỉ lệ
bệnh
nhân t
ăn
g đ
ạm
niệ
u/
cre
atinin
tro
ng
nư
ớc tiể
u (
%)
Sau 2 năm Kết thúc nghiên cứu (5.5 năm)
70
Telmisartan
Placebo
* p<0.001 so với placebo Mann et al. Ann Intern Med 2009;151:1-10
*
*
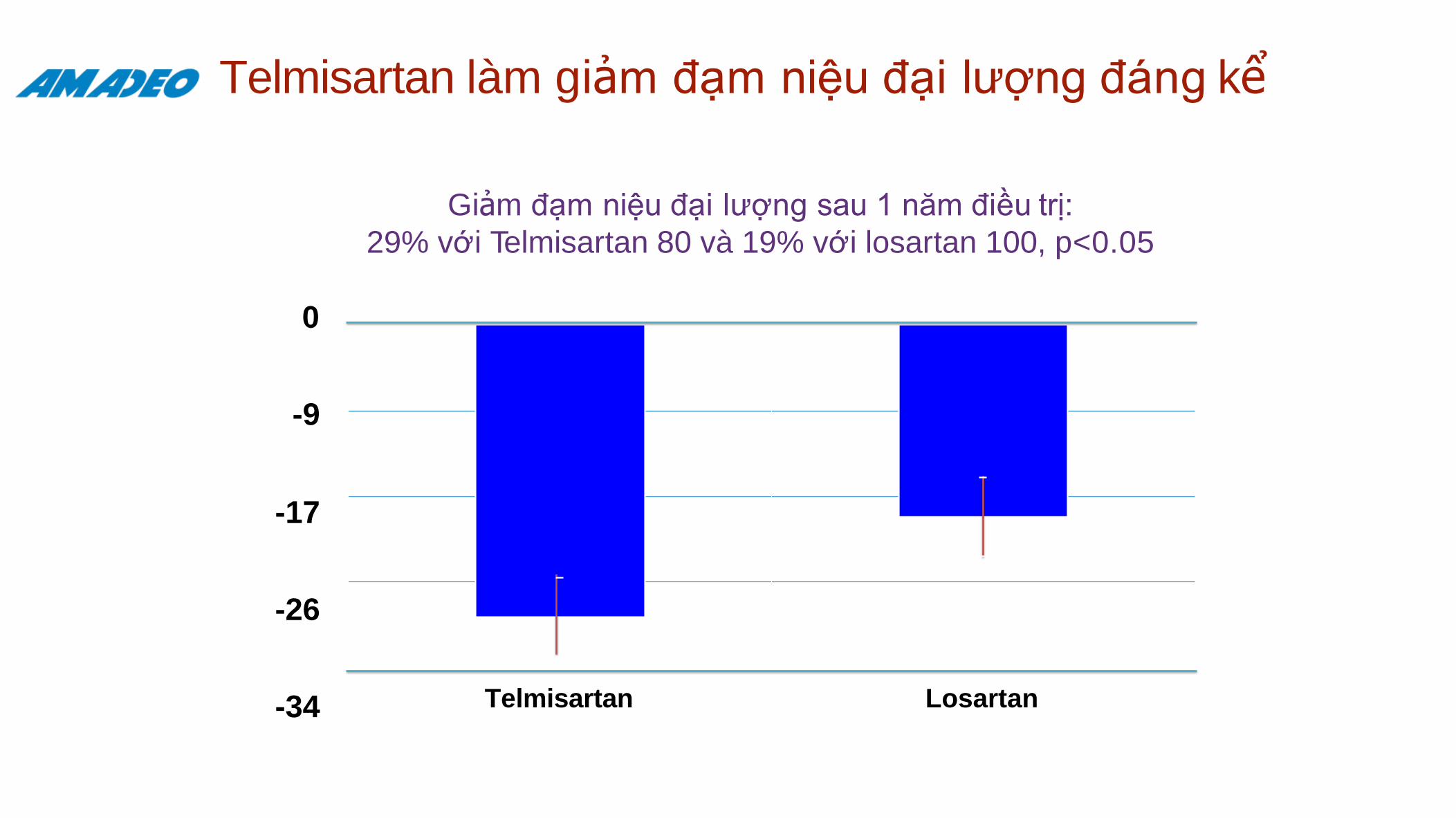
Telmisartan làm giảm đạm niệu đại lượng đáng kể
Giảm đạm niệu đại lượng sau 1 năm điều trị:
29% với Telmisartan 80 và 19% với losartan 100, p<0.05
0
-9
-17
-26
-34 Telmisartan Losartan
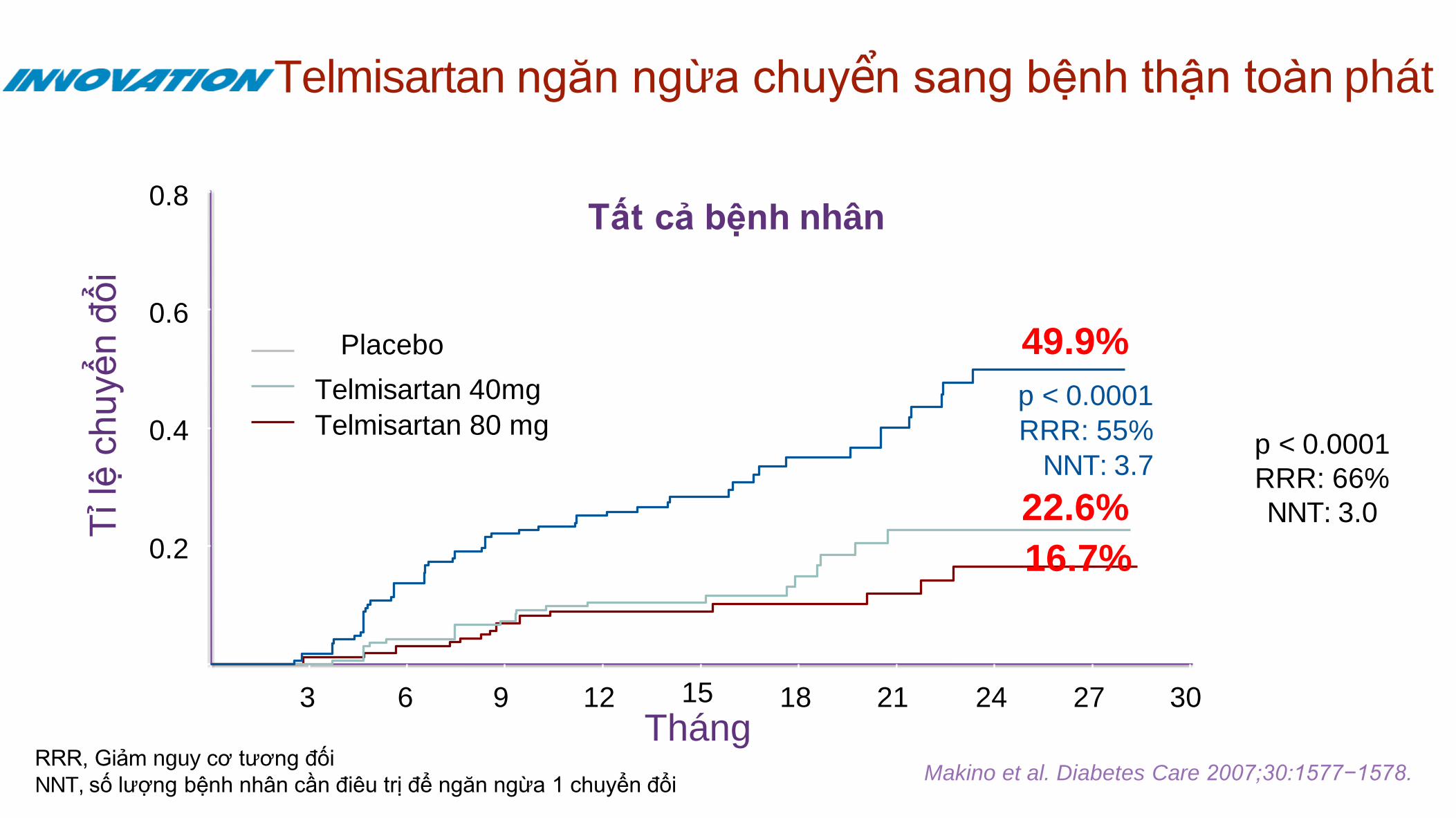
Telmisartan ngăn ngừa chuyển sang bệnh thận toàn phát
3 6 9 12 15
Tháng 18 21
0.2
0.4
0.6
0.8
Telmisartan 80 mg
Telmisartan 40mg
Placebo
16.7%
22.6%
49.9%
Tỉ lệ
ch
uyể
n đ
ổi
p < 0.0001
RRR: 66%
NNT: 3.0
p < 0.0001
RRR: 55%
NNT: 3.7
Tất cả bệnh nhân
RRR, Giảm nguy cơ tương đối
NNT, số lượng bệnh nhân cần điêu trị để ngăn ngừa 1 chuyển đổi
24 27 30
Makino et al. Diabetes Care 2007;30:1577−1578.
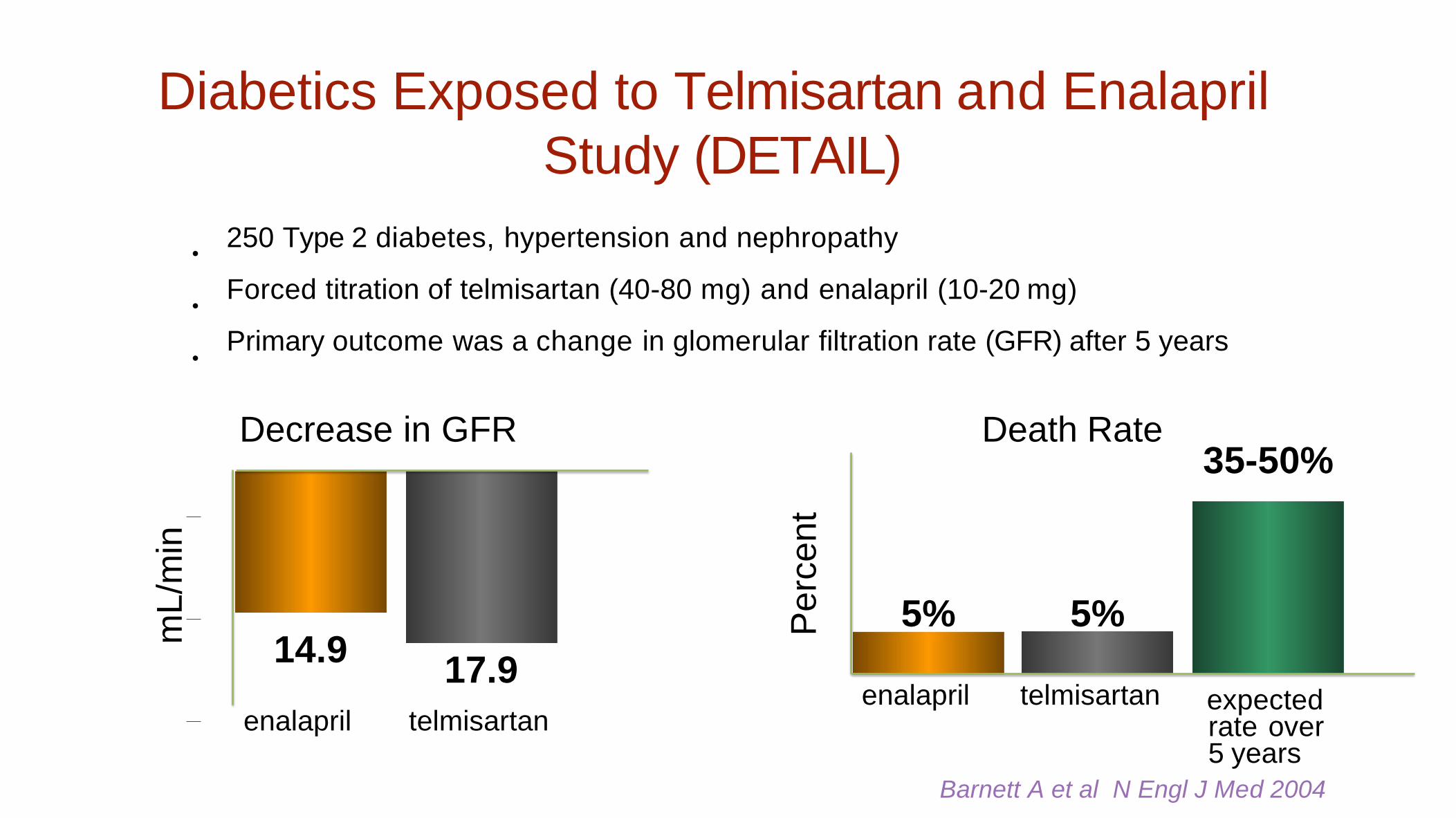
Diabetics Exposed to Telmisartan and Enalapril
Study (DETAIL)
•
•
•
Barnett A et al N Engl J Med 2004
14.9 17.9
enalapril telmisartan
mL
/min
250 Type 2 diabetes, hypertension and nephropathy
Forced titration of telmisartan (40-80 mg) and enalapril (10-20 mg)
Primary outcome was a change in glomerular filtration rate (GFR) after 5 years
Decrease in GFR Death Rate
enalapril telmisartan
Pe
rce
nt
35-50%
expected rate over 5 years
5% 5%
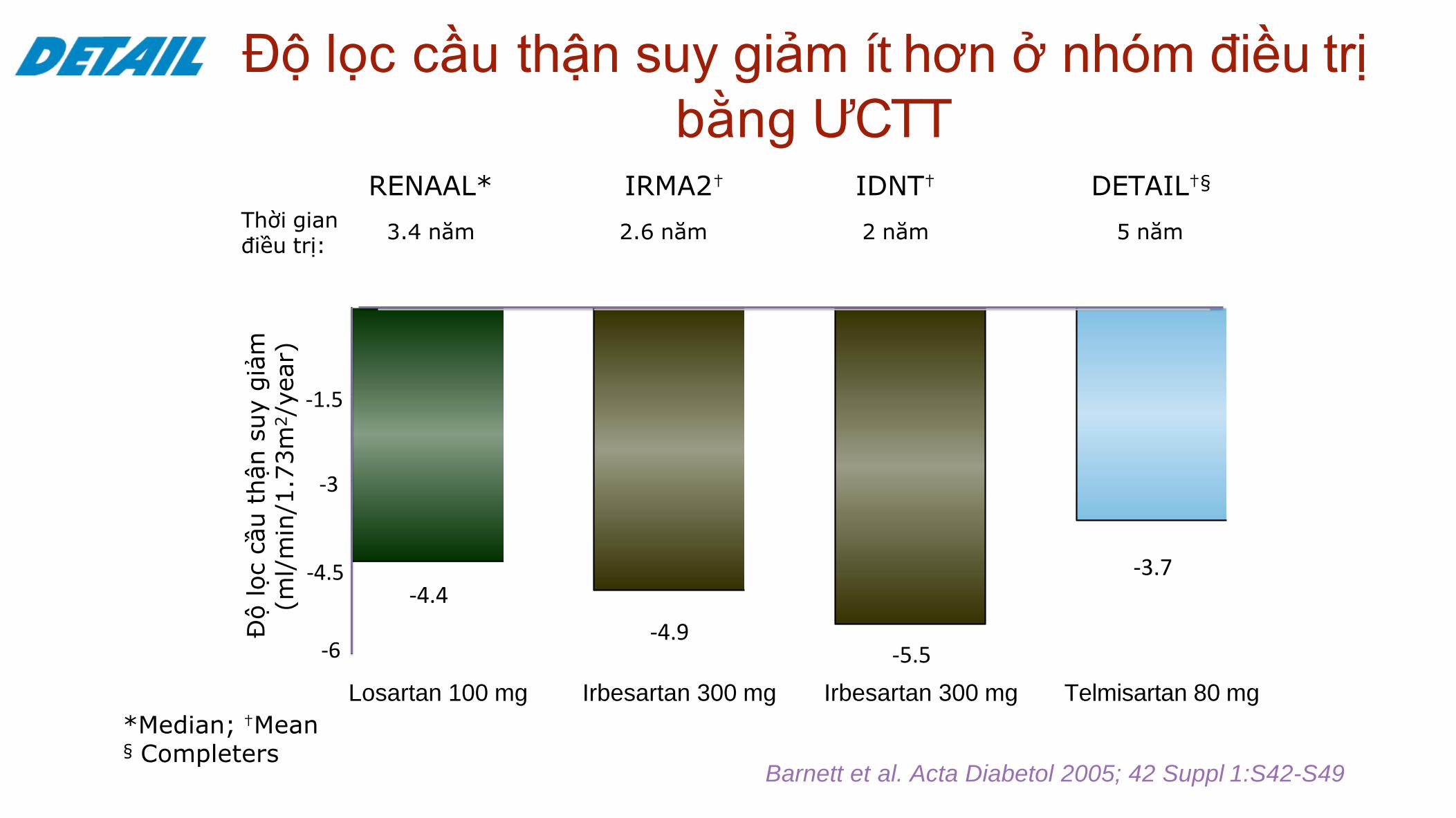
Độ lọc cầu thận suy giảm ít hơn ở nhóm điều trị
bằng ƯCTT
Losartan 100 mg Irbesartan 300 mg Irbesartan 300 mg Telmisartan 80 mg
Độ lọc c
ầu t
hận s
uy g
iảm
(m
l/m
in/1
.73m
2/y
ear)
*Median; †Mean § Completers
Barnett et al. Acta Diabetol 2005; 42 Suppl 1:S42-S49
Thời gian điều trị:
RENAAL*
3.4 năm
IRMA2†
2.6 năm
IDNT†
2 năm
DETAIL†§
5 năm
-1.5
-3
-4.5
-6
-4.4
-4.9 -5.5
-3.7
Hypertension treatment for people with
nephropathy
Recommendations Additonal considerations
Consider lowering SBP to <140 mmHg
Consider SBP <130 mmHg with overt proteinuria • Monitor changes in eGFR
RAS blockers more effective to reduce albuminuria than other agents
• Indicated in presence of microalbuminuria or overt proteinuria
Combination therapy usually required to reach BP goals • Combine RAS blockers with other agents
Combination of two RAS blockers • Not recommended
Aldosterone antagonist not recommended in CKD • Especially in combination with a RAS blocker
• Risk of excessive reduction in renal function, hyperkalemia
SBP, systolic blood pressure; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; RAS, renin–angiotensin system.
Kết luận
Nên tầm soát bệnh thận mạn trên bệnh nhân tăng huyết áp
Mục tiêu điều trị bệnh thận mạn: bệnh căn nguyên, chậm tiến
triển suy thận
Thuốc ức chế hệ RAA được khuyên dùng cho bệnh nhân tăng
huyết áp có bệnh thận mạn- su phoi hop thuoc luon can de dat HA
Telmisartan giảm đạm niệu vi lượng, giảm sự diễn tiến đạm niệu
vi lượng sang đại lượng, giảm tiến triển bệnh thận mạn
Recommended

















