Handoffs and Transitions in Critical Care (HATRICC)
Evanie Anglade University
of Pennsylvania, 2019 SUMR Scholar,
2017
Meghan Lane-Fall, MD, MSHP Anesthesiology and Critical Care,
Perelman School of Medicine

Outline� Background
� Project Overview
� My Role� Phase 3� Phase 4
� My Learning Experience

Handoffs� Transfer of patient care and accountability
� Found in various care settings because of specialization of care across providers and disciplines1
1. Cohen, Michael D., and P. Brian Hilligoss. "The published literature on handoffs in hospitals: deficiencies identified in an extensive review." Quality and Safety in Health Care (2010): qshc-2009.

The Big Four

Significance� Handoffs are high-risk events for acutely ill patients
� delays in diagnosis or treatment� medication errors � physical movement of patients� Transfer of information among providers of different
disciplines� Patient is incapacitated
� 4 – 8 million preventable serious adverse events annually2
� 70% caused by communication problems3
� Of those, 50% handoff-related3
2. James, JT. "A new, evidence-based estimate of patient harms associated with hospital care." Journal of patient saf 2013): 122-128.3. Dunn, Edward J., Peter D. Mills, Julia Neily, Michael D. Crittenden, Amy L. Carmack, and James P. Bagian. "Medical team training: applying crew resource management in the Veterans Health Administration." The Joint Commission Journal on Quality and Patient Safety 33, no. 6 (2007): 317-325.

Specific Aims1. Perform a needs assessment of the OR-to-ICU
handoff process in two ICUs that serve mixed surgical populations.
2. Adapt and implement a standardized OR-to-ICU handoff process.
3. Evaluate the implementation and effectiveness of a standardized OR-to-ICU handoff process.

Hypotheses� Intervention effectiveness hypothesis: After
implementing a standard handoff process, the number of information omissions per handoff will decrease by 50%.
� Implementation hypothesis: Clinician acceptance of a new standardized OR-to-ICU handoff process will be high, as assessed qualitatively.

Study Design
Phase 1 Needs
Assessment
Phase 2 Implementation
Phase 3 EffectivenessEvaluation
Phase 4Sustainability

HATRICC Conceptual Model

Standardized Process1. Introduction of providers
2. Stabilization of patient3. Transfer of technology4. Huddle of providers5. Surgery presentation6. Anesthesia presentation
7. ICU presentation8. Physical exam of patient9. Exchange of contact information10.Questions




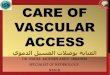
Study Results
Quality ofInformation Transfer
Quality of Teamwork
Quality of Professionalism
Number of information omissionsper handoff decreased 22.7%(p=0.028)
Percentage of handoffs rated unsatisfactory teamwork decreased 26.7% (p<0.001)
Percentage of handoffs rated unsatisfactory professionalismdecreased 17.8%(p<0.001)
Before After Before After Before After
4.4±2.7 3.4±1.8 45.3% 18.6% 25% 7.2%

My Role
Phase 1 Needs
Assessment
Phase 2 Implementation
Phase 3 EffectivenessEvaluation
Phase 4Sustainability

My Role: Specific Aims1. Help determine accuracy of handoffs before and
after implementation of the standardized process.
2. Consider ways to sustain the standardized handoff process for future care.

Phase 3: Handoff Accuracy� Question: How did accuracy change after
implementation, if it did?
� Methods: Comparison between handoff observation forms and chart abstraction forms of Phase 1 and those of Phase 3� REDCap

Accuracy MeasuresAllergies Estimated Blood Loss
Past medical/surgical history Urine output
IV Fluids Current infusions
Blood products

Accuracy Schematic
Was the info discussed accurate?
Does the patient have allergies?
Was the information discussed complete?
Were allergies discussed during the handoff?
Was the information discussed accurate?

Ranking System

Phase 4: Sustainability� HATRICC has improved handoff communication
� Observations in TSICU on HUP Rhoads 5, Presbyterian TSICU4, and NICU on HUP Rhoads 2
� Real-time feedback for clinicians

Real-Time Feedback� Question: How does real-time feedback for
clinicians affect performance?
� Methods: Literature review� PubMed and Scopus� Included 8 studies between 2005 – 2015
� Results� Sometimes there is a delay in “real-time” feedback
� Passive visual cues for actual real-time � Earlier studies use higher-ups to provide feedback� Later studies use IT to provide feedback
� Computer-mediated feedback

Remaining Questions� Is real-time feedback conducive to the kind of
environment handoffs take place in?� If so, what would this feedback system look like?
� Who should be providing the feedback?

My Learning Experience� Making thorough observations
� Maintaining uniformity in observations
� REDCap basics
� Better focusing a literature search
� Thinking critically about already published studies

AcknowledgementsDr. Meghan Lane-Fall Leonard Davis Institute
Hannah Peifer Wharton Dean’s Office
Lane-Fall Lab 2017 SUMR Cohort
Joanne Levy
Safa Browne

Questions?
Recommended