Embed Size (px)
Citation preview
Epidemiological Study of Mandibular Fractures in Iraqi
Sample
Graduation projectsubmitted to the department of oral and maxillofacial surgery
Prepared byTasneem KareemIbrahim Ahmed
Supervised byAssist. Lecturer Dr. Zainab Mahmood AL-Bahrani
B.D.S, Dip. In oral and maxillofacial surgery M.Sc. In oral and maxillofacial radiology
2015
ح�يم� ح�من� الر� � الله الر� م �س� ب
} � �ي ع�لما �ي ز�دن ب } وق�ل� ر�
ص�د�ق� الله الع�ظيم�
INTRODUCTIONAnatomy of mandibleThe mandible (from Latin mandibula, "jawbone") or inferior maxillary bone is the largest, strongest and lowest bone in the face. It forms the lower jaw and holds the lower teeth in place.
The mandible is divided into eight regions. The symphysis is located in the midline, joining the right and left halves of the mandible. The parasymphyseal region is located on either side of the symphysis, and spans from canine to canine. Moving posterolaterally, the body is the region from the canine to the angle, which is the non-tooth bearing region between the body and the ramus. The ramus is the vertical portion of the mandible that extends from the angle toward the zygomatic arch, terminating at the
coronoid process and condyle .
Mandibular bone fracture
The mandibular bone consider as the unique facial bone having the ability to be a mobile bone that play a major role in mastication, speech, and deglutition. Mandibular fractures constitute a large proportion of cases of maxillofacial trauma, so the purpose of this study was to investigate the epidemiological pattern of mandibular fractures.
CLASSIFICATION
Mandible fractures can be classified in several ways. Standard fracture nomenclature for long bone fractures is the first classification (simple, compound, comminuted, or greenstick). The second method is by anatomic location. The third is by dentition status, and the fourth is by stability of the fracture, i.e. favorable versus
unfavorable .
CLASSIFICATION
1 -According to the fracture type*In a simple fracture the oral mucosa
and external skin are intact.*In a compound or open fracture there
is a laceration of the mucosa or skin present, or the fracture passes through a tooth root.
*Comminuted fractures have multiple bone fragments .
*Greenstick fractures involve only one cortex of the bone and occur most commonly in children.
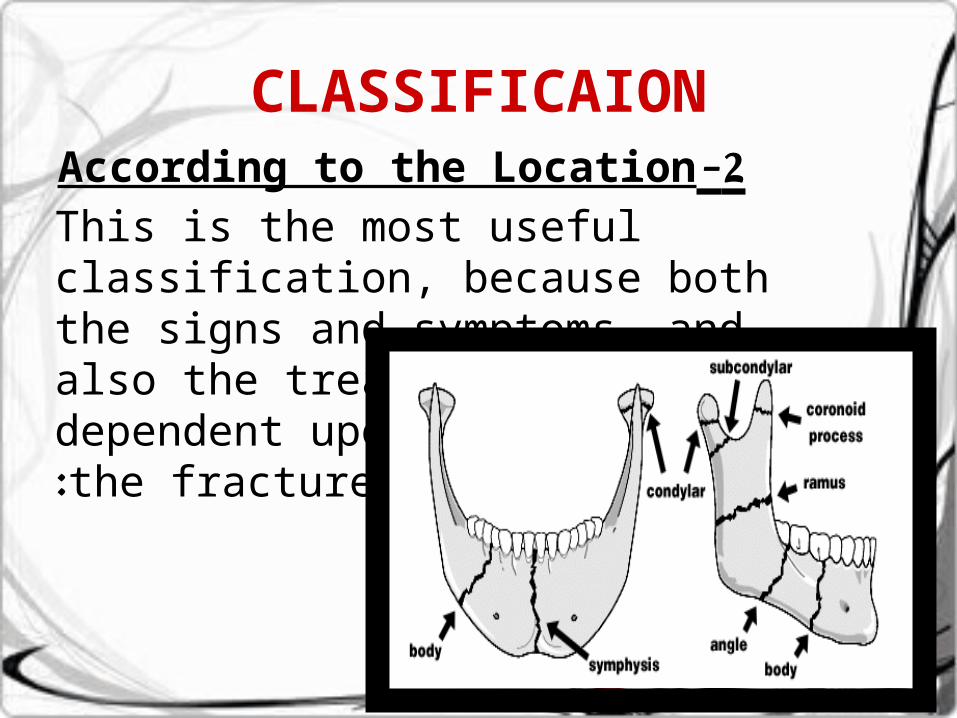
CLASSIFICAION2 -According to the Location
This is the most useful classification, because both the signs and symptoms, and also the treatment are dependent upon the location of the fracture:
CLASSIFICATION* Alveolar (Dento-alveolar)fractureThis type of fracture involves the alveolus (the alveolar process of the mandible).
*Condylar fractureCondylar fractures are classified by location compared to the capsule of ligaments that hold the temporomandibular joint (intracapsular or extracapsular.(
* Coronoid fractureBecause the coronoid process of the mandible lies deep to many structures, including the zygomatic complex (ZMC), it is rare to be broken in isolation. It usually occurs with other mandibular fractures or
with fracture of the zygomatic complex or arch .
CLASSIFICATION
* Ramus fractureRamus fractures are said to involve a region inferiorly bounded by an oblique line extending from the lower third molar.
*Angle fractureAngle fractures are defined as those that involve a triangular region bounded by the anterior border of masseter muscle and an oblique line extending from the lower third molar (wisdom tooth) region to the posteroinferior attachment of the masseter muscle.
CLASSIFICATION *Body fracture
defined as those that involve a region bounded anteriorly by the parasymphysis (defined as a vertical line just distal to the canine tooth) and posteriorly by the anterior border of the masseter muscle.
*Parasymphysis fractureParasymphyseal fractures are defined as mandibular fractures that involve a region bounded bilaterally by vertical lines just distal to the canine tooth.
*Symphysis fracture•Symphyseal fractures are linear fractures
that run in the midline of the mandible (the symphysis).
CLASSIFICATION3- According to the Dentition
Classification: Developed by Kazanjian and Converse
*Class I: teeth are present on both sides of the fracture line
*Class II: Teeth present only on one side of the fracture line
*Class III: Patient is edentulous. 4- According to the stabilityFractures can be classified as favorable or unfavorable based on the stability (or lack thereof) afforded by the pull of muscles on the fractured segments of bone.
ETIOLOGY
The Major etiologic factors of Mandible fracture are varying by the time period and the region studied. In some countries, blunt force trauma (a punch) is the leading cause of mandible fracture, where as in others, motor vehicle collisions are now a leading cause. On battle grounds, it is more likely to be high velocity injuries (bullets and shrapnel). Prior to the routine use of seat belts, airbags and modern safety measures, motor vehicle collisions where a leading cause of facial trauma.
•Mandibular fracture is a rare complication of third molar removal, and may occur during or after the procedure. Children injuries are usually resulted from fall accidents in addition to sporting accidents.
EXAMINATIONHistoryPain and malocclusion after a blow to the lower face strongly suggest mandibular fracture. Additional symptoms include anesthesia of the lower lip and chin caused by trauma to the inferior alveolar nerve.Unfortunately attempts to obtain history is often limited by the patient being intubated, unconscious, confused, or intoxicated.If the patient is awake and cooperative, he or she should be questioned about the presence and location of pain, malocclusion, trismus, intraoral bleeding, and loss of sensation, particularly in the mental nerve region.
EXAMINATION
Physical ExaminationThe physical examination of the patient means the general appearance to be first assessed and any lacerations, ecchymosis, edema, or areas of distortion are noted.The entire mandible is palpated for tender areas, mobility, step-offs, and crepitus. The occlusion should be checked bilaterally and note made of any deviation of the mandible .
EXAMINATIONRadiographic Evaluation
Proper treatment of fractured mandible is dependent on proper diagnosis. Panoramic radiography has become the standard of care for the evaluation of mandibular fractures in many institutions.
Panoramic views with posteroanterior or reverse Towne's views are likely to give a higher yield than the panoramic view alone. The periapical view can be useful to identify specific dental trauma or abscesses. Occlusal views are under utilized, and can be very useful when used intra-operatively on patients with symphyseal and parasymphyseal
fractures .
EXAMINATIONRadiographic Evaluation
The use of computed tomography (CT) as a diagnostic tool has been controversial in the past. Early studies comparing the sensitivity of CT to other modalities of the radiographic workup suggested that CT was not as sensitive. More recent studies performed with improved, higher resolution CT suggest that CT is superior to panoramic radiography, both in sensitivity and in offering the surgeon a better understanding of the nature of the fractures. Three-dimensional CT may have an important role in the future for evaluating pre- and postreduction techniques
COMPLICATIONSComplications may be related to the trauma of the mandible or related to delay in fixing the fractured mandible that increases the risk of complications, but neurological complications or other problems such as airway compromise may make this
inevitable .If there is bilateral fracture of the body of mandible, parasymphyseal, or condylar fractures, there is risk of impairment of airways.
Infection, malunion or non-union, ankylosis are considered major complications which can result in poor ability to open the mouth. The psychological implications of facial trauma are such that the risk of post-traumatic stress disorder is increased in this condition.
MATERIAL AND METHOD
A retrospective cross sectional study on the medical data base records of (30 patients) aged over (15 years) who had been diagnosed with a Mandibular bone fracture referred to the hospital of Al- Shaheed Ghazi Al Hariri in 2 years duration.
This study carried out on the recorded information of each patients including age, gender, type and site of fractured mandible, etiology, and the type of radiographic view
MATERIAL AND METHOD
Age was classified into 3 groups: 15 to 30 years old, 31 to 49 years old, and >50 years old.
*The causes of the accidents were grouped into the following categories:
*Road traffic accidents (RTA)*Interpersonal violence (IPV)
*Sports, falls, and occupational accidents*Blast injury
*Pathological conditions
MATERIAL AND METHODThe fracture area was recorded from different
diagnostics radiographic views such as: anteroposterior, lateral-oblique,orthopantomograms, and computed tomography.
According to radiographic findings, the fractured mandibles were classified according to location into six anatomical sites including:
*Symphysis/parasymphysis* Body* Angle
* Ramus,*Condyle
*Coronoid process.All data were analyzed using descriptive statistical analysis.
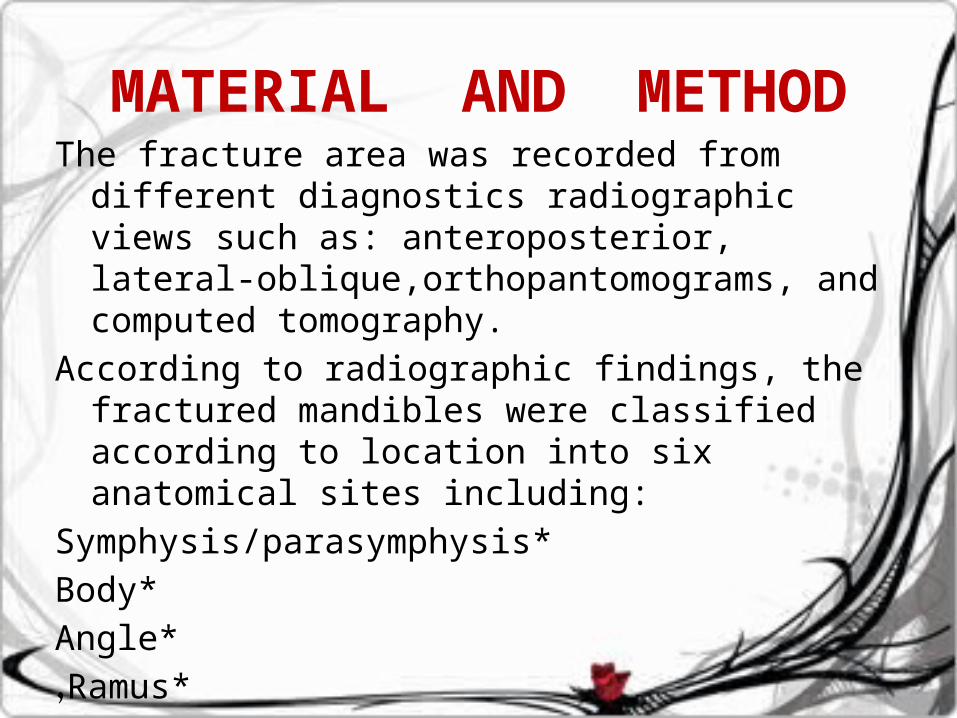
CT scan image shows symphyseal fracture.
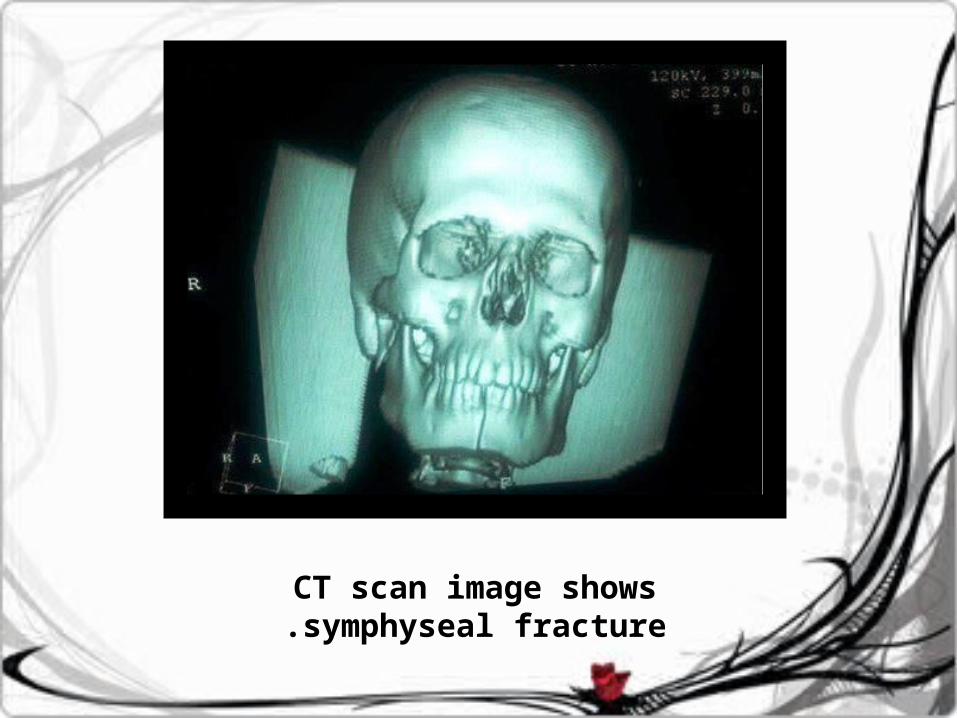
OPG image shows Mandibular body fracture
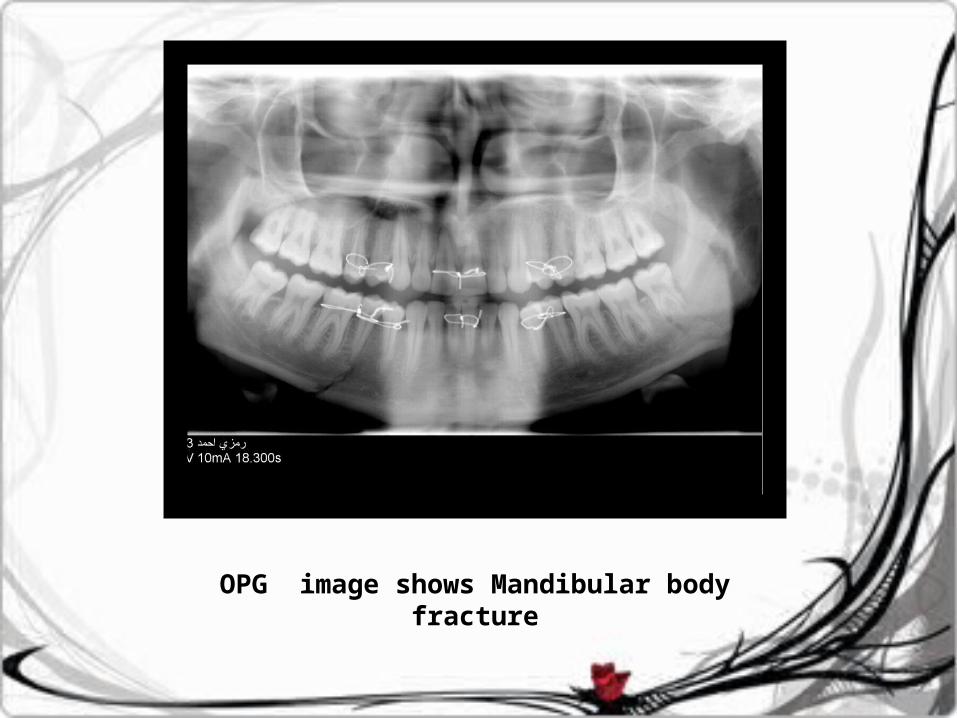
OPG image shows multiple fracture lines.
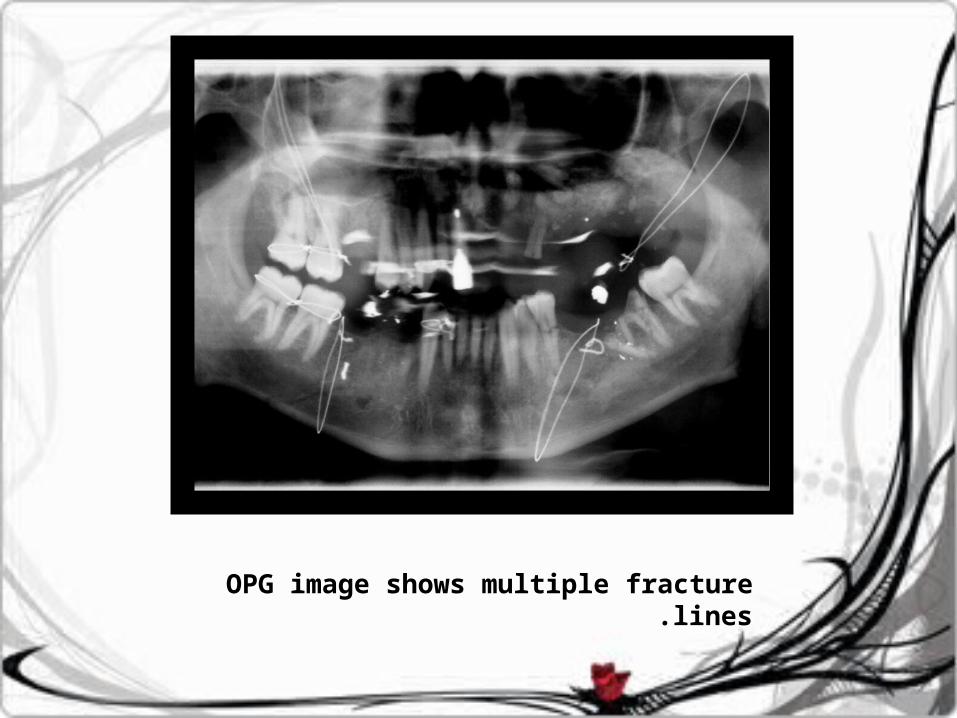
PA image shows ramus fracture
RESULT
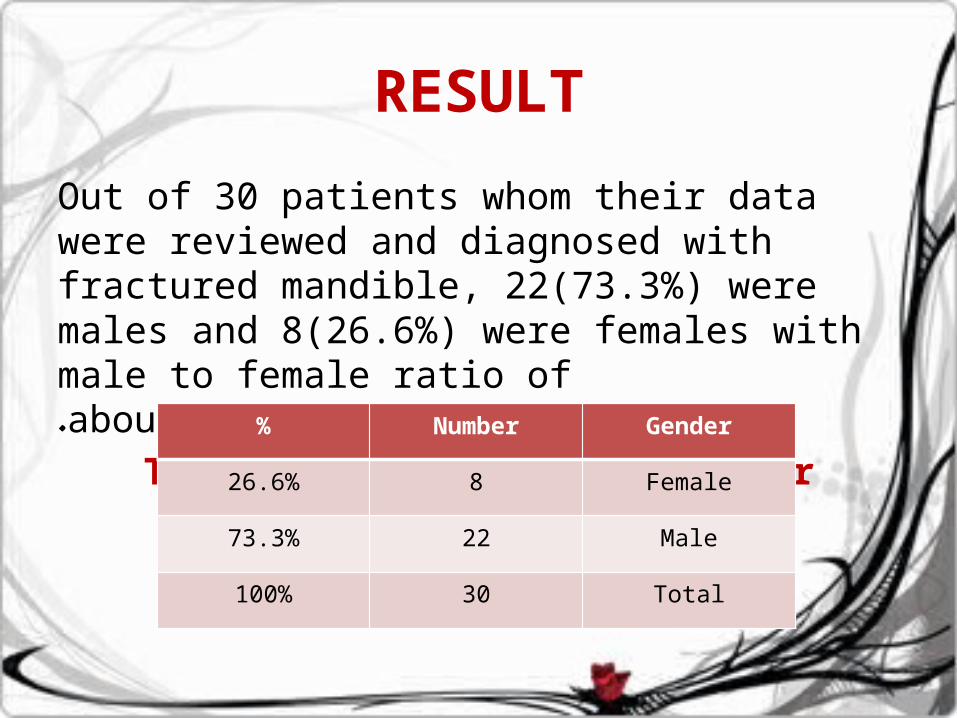
Out of 30 patients whom their data were reviewed and diagnosed with fractured mandible, 22(73.3%) were males and 8(26.6%) were females with male to female ratio of about(2.75:1).
Table (1): Frequency of gender distribution of the sample.
% Number Gender
26.6% 8 Female
73.3% 22 Male
100% 30 Total
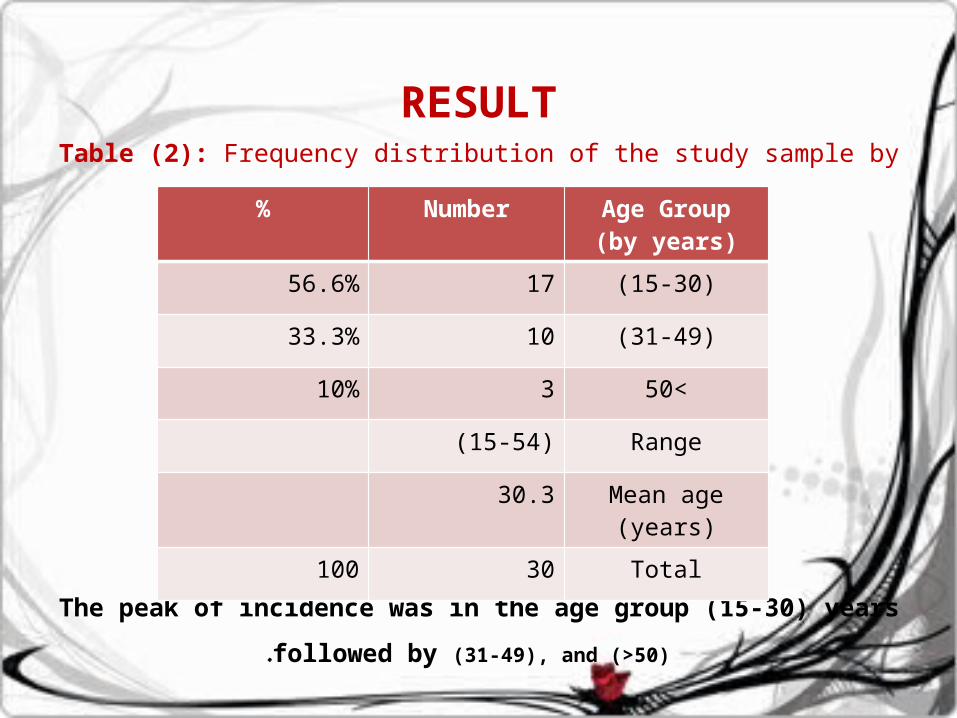
RESULTTable (2): Frequency distribution of the study
sample by age.
The peak of incidence was in the age group (15-30) years followed by (31-49), and (>50) .
% Number Age Group(by years)
56.6% 17 (15-30)
33.3% 10 (31-49)
10% 3 >50
(15-54) Range
30.3 Mean age (years)
100 30 Total
RESULT
The prevalence of fractures of one area of mandible (86.7%) was more compared with multiple areas (13.3%)
•The type of requested x-ray in most cases were panoramic radiography as in table (3), the recorded data of some patients were with more than one x- ray view due to overlapping.
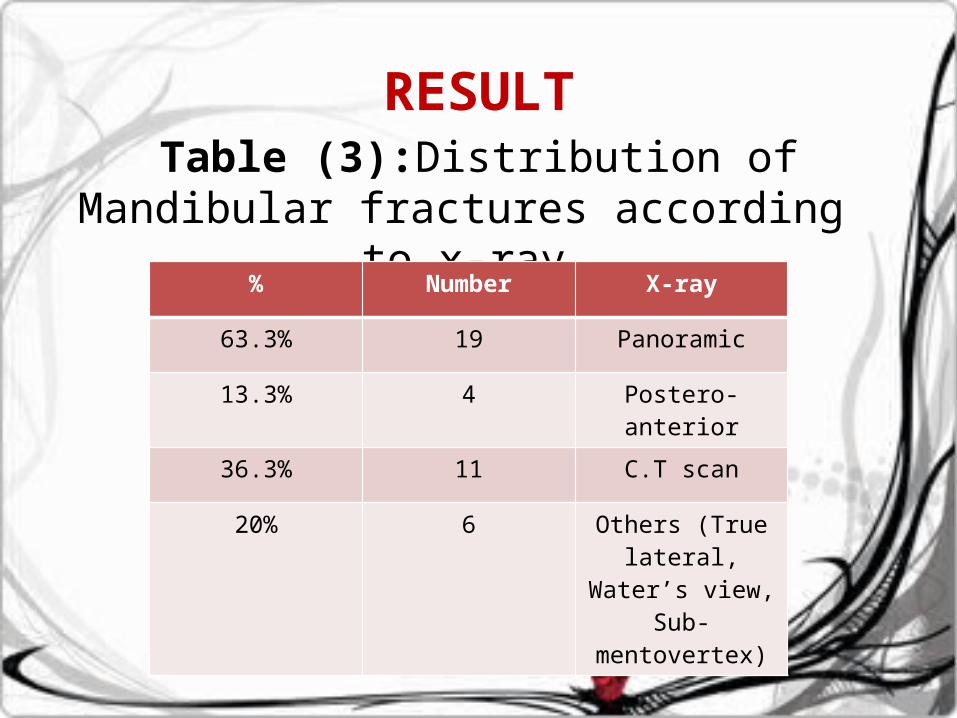
RESULTTable (3):Distribution of Mandibular
fractures according to x-ray Type.% Number X-ray
63.3% 19 Panoramic
13.3% 4 Postero-anterior
36.3% 11 C.T scan
20% 6 Others (True lateral, Water’s
view, Sub-mentovertex)
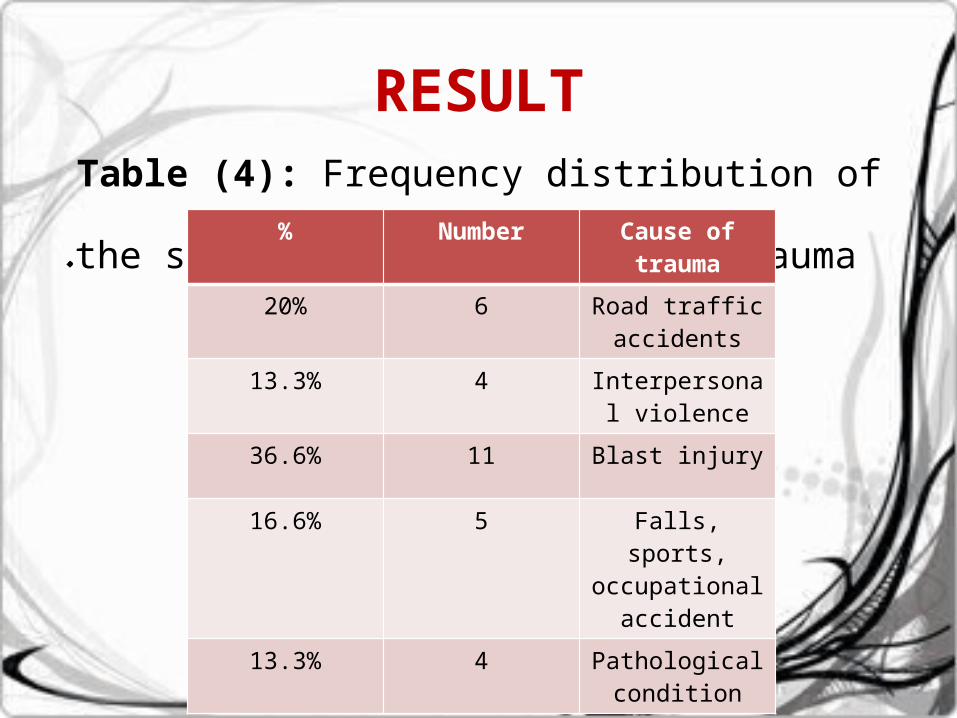
RESULTTable (4): Frequency distribution of the
study sample by cause of trauma. % Number Cause of trauma
20% 6 Road traffic accidents
13.3% 4 Interpersonal violence
36.6% 11 Blast injury
16.6% 5 Falls, sports, occupational
accident
13.3% 4 Pathological condition
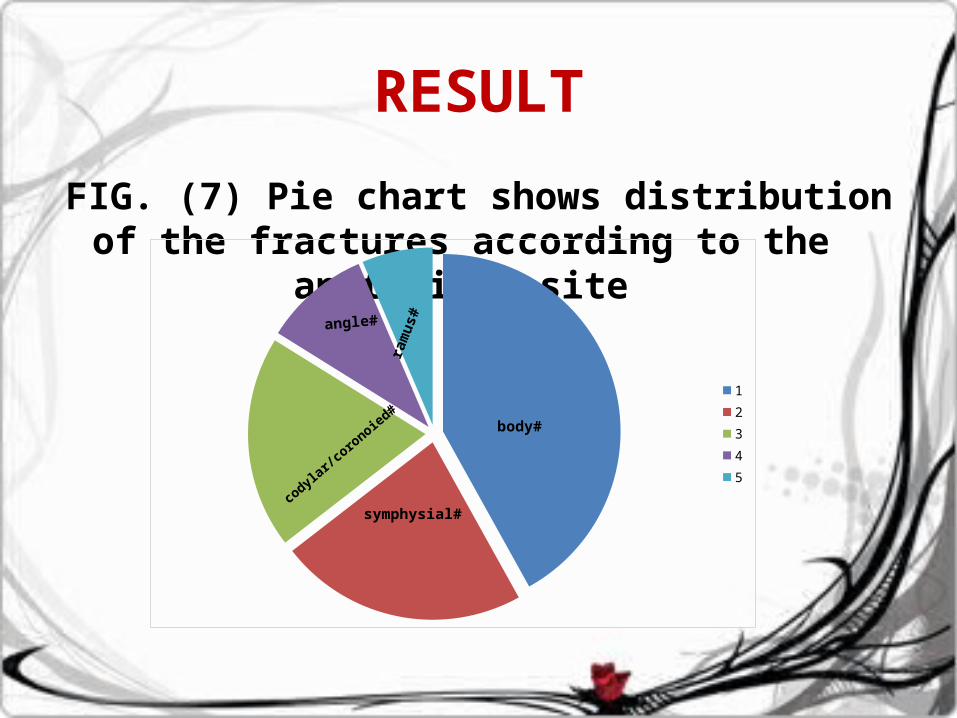
RESULT
FIG. (7) Pie chart shows distribution of the fractures according to the
anatomical site
12345
body#
symphysial#co
dylar/coro
noied#
angle#
ram
us#
DISCUSSION
The rapid continuous developmental growth of society, industry and life style resulted in high number of variant type of accidental injuries and associated with fractures of any part of the body including Mandibular bone fractures.
In this study the reviewing of patients with mandibular fracture shows that the majority of patient with a mandibular fracture are males this may be due to the fact that males are more presence in outdoor activity also there is a strong relationship between blunt force trauma and mandible fractures which explains why most of fractures occur in males, this result was similar to the result of Sakr et al (2006) , Khorasani M. and Khorasani B. (2009) (,AndreasaZ. J. et al (2011)
DISCUSSION
Based on this study most patients were in the age group (15-30) years this related to the etiological factors of a mandibular fracture which was in agreement with several studies that reported the this young adult age group as the most common like Abbas et al. (2003) and Al-Ahmad et al. (2004)
DISCUSSIONThe etiology of mandibular fracture varies significantly between countries. Almost all authors try to explain this variability by socioeconomic, cultural and environmental factors, In the comparison of the socioeconomic status of populations of different countries, the factor “income” , “education”, “occupation” and “wealth” account for the socioeconomic status in addition to traffic safety which responsible for road traffic accident, so the result of this study according to causes of fracture differ from other studies since most of referral cases to the hospital of Al- Shaheed Ghazi Al Hariri in were marital injuries comparing with Khorasani M. and Khorasani B. (2009) Sakr et al (2006) Abbas et al. (2003)(25)studies that reviles most cases were due to motor vehicles accident, while In contrast to several studies, which report very high rates of interpersonal violence Lee (2008) and Oikarinen et al (2005)
DISCUSSION
Regarding the relationship of trauma mechanism and fracture site, our study confirms previous findings of a correlation between etiology and fracture pattern.
Body of the mandible shows the highest rate of fractures and this was agreed with the result of Qudah et al (2005), Fnseca and Walker(1997), Fasola et al (2001)
King et al.(2004)( study shows the prevalent fractures resulting from motor vehicle collisions are in the parasymphseal and condylar region, The same applies to falls, which are most commonly associated with condylar fracture in Lee (2008).
DISCUSSION
As a conclusion the Mandibular fractures occur in people of all ages and races, in a wide range of social settings. Their causes often reflect shifts in trauma patterns over time.
It is hoped that a careful assessments such as detailed history, radiographical and clinical examination will be valuable to government agencies and health care professionals involved in planning future programs of prevention and treatment.

�ح�ـم�ـد� الله مq ب ـ� ت
Thank You For Listening