Embed Size (px)
Citation preview

ADVERSE DRUG REACTIONS (ADRs)
AND
DRUG ALLERGY
Achara Srisodsai, Ph.D.Department of Toxicology
Faculty of Pharmaceutical Sciences
Khon Kaen University

วั�ตถุ�ประสงค์�รายชั่��วัโมง
1 .เพื่��อให้�เข้�าใจค์วัามหมายข้องอาการไม่�พื่�งประสงค์�จากการใช้�ยา2. เพื่��อให้�เข้�าใจถึ�งการจำ�าแนกประเภทข้อง ADRs
3. เพื่��อให้�เข้�าใจถึ�งกลไกการเก�ด ADRs ประเภทต่�างๆ4. เพื่��อให้�เข้�าใจค์วัามหมายข้องอาการแพื่�ยา5. เพื่��อให้�เข้�าใจล�กษณะและกลไกการแพื่�ยา6. เพื่��อให้�เข้�าใจถึ�งอาการแพ้�ยาท#�เก�ดข้�$น

ADRs Definition
Classification of ADRs
Mechanisms
Drug allergy
Characteristics
Mechanisms
Clinical Manifestation
OVERVIEW

THE FIRST APPEARANCE OF THALIDOMIDE
'Thalidomide Babies'


First appeared in Germany on 1st
October 1957.
As a sedative with apparently remarkably
few side effects.
Prescribing to pregnant women to help
combat morning sickness.
The tests were conducted on rodents
which metabolise the drug in a different way
to humans.
Later tests on rabbits and monkeys
produced the same horrific side effects as
in humans.
Thalidomide

Towards the end of the fifties, children began to
be born with shocking disabilities.
Probably the most renowned is Phocomelia, the
name given to the flipper-like limbs which appeared
on the children of women who took thalidomide.
Babies effected by this tragedy were given the
name 'Thalidomide Babies'.

Why drugs can cause tragedy?

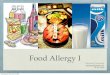
Compound Success Rates By Stages
0 2 4 6 8 10 12 14 16
Years
Discovery(2-10 Years)
Preclinical TestingLaboratory and animal testing
Phase I 20-80 healthy volunteers used to determine safety and dosage
Phase II 100-300 patient volunteers to look for efficacy and side effects
Phase III 1,000-5,000 patient volunteers usedto monitor adverse reactions to long-term use
FDA Review/Approval
Additional post-marketing testing
Compound SuccessRates by Stage
5,000-10,000screened
250Enter preclinical testing
5Enter clinical testing
1Approved by the FDA
Postmarketing survillence

Limitations of premarketing clinical trials
Short duration — effects that develop with chronic use or
those that have a long latency period are impossible to
detect.
Narrow population — generally do not include special
groups (e.g., children, elderly), to a large degree, and are not
always representative of the population that may be exposed
to the drug after approval.

Adverse Reaction Drug Time Lag (yr)
Pulmonary embolism Oral contraceptives 3
Myocardial infarction Oral contraceptives 5
Deaths from asthma Sympathomimetic aerosols 4
Jaundice Halothane 7
Colitis Lincomycin 6
Colitis Clindamycin 5
Aplastic anemia Phenylbutazone 6
Venning, GR. Br. Med. J. 286:365-368, 1983
Summary of time lags after U.S. marketing before
adverse drug reactions were widely recognized

Narrow set of indications — those for which
efficacy is being studied and do not cover actual
evolving use.
Small size (generally include 3,000 to 4,000
subjects) — effects that occur rarely are very difficult
to detect.
Limitations of premarketing clinical trials

Number of patients to be observed to detect
Incidence of ADR 1, 2 or 3 cases of ADR
1 2 3
1 in 100 300 480 650
1 in 200 600 960 1,300
1 in 1,000 3,000 4,800 6,500
1 in 2,000 6,000 9,600 13,000
1 in 10,000 30,000 48,000 65,000
Required sample size for detecting a rare adverse drug reaction

ADVERSE DRUG REACTIONS (ADRs)

WHO: Any response to a drug which is noxious and
unintended, and which occurs at doses normally
used in man for prophylaxis, diagnosis,
or therapy of disease, or for the modification of
physiological functions.
What is ADR?

Excluding……….
Therapeutic failures
Intentional and accidental overdose
Drug abuse
Errors in drug administration

Adverse Drug Events (ADEs)
- เหต�การณ� หร#อผลการร�กษาที่&�เลวัลงหล�งการใชั่�ยา
Risk assessment of drug
- กระบวันการที่างวั)ที่ยาศาสตร�ที่&�ใชั่�ส#บค์�นและประเม)นโอกาสและผลกระที่บจำากการใชั่�ยา- ประกอบด้�วัยการบ,งชั่&-ถุ.งอ�นตราย , การประเม)นค์วัามส�มพ้�นธ์�ขนาด้ยาที่&�ได้�ร�บก�บผลการตอบสนอง , การประเม)นโอกาสการได้�ร�บ , การอธ์)บายล�กษณะค์วัามเส&�ยง
Adverse Product Reaction (APR)
- อาหาร , สารเสพ้ต)ด้ , เค์ร#�องส�าอาง

Classification
of
Adverse Drug Reactions

Classification of Adverse Drug Reactions
จำ�าแนกตามค์วัามร�นแรงของอาการ (Severity classification) 1. ร�นแรงน�อย (Mild) อาการไม,พ้.งประสงค์� ที่&�ไม,ร�นแรงไม,ต�องการการร�กษาใด้ ๆ2.ร�นแรงปานกลาง (Moderate)อาการไม,พ้.งประสงค์�ที่&�เก)ด้แล�วัต�องม&การปร�บเปล&�ยนหร#อหย�ด้การใชั่�ยาน�-น3. ร�นแรงมาก (Severe) อาการไม,พ้.งประสงค์�ข�-นร�นแรงที่&�อาจำที่�าให�ผ2�ป3วัยเส&ยชั่&วั)ต

Serious adverse events:
เส&ยชั่&วั)ต (fatal)
ภาวัะวั)กฤต) (life-threatening)
พ้)การ (disabling)
ต�องร�บการร�กษาในโรงพ้ยาบาลนานข.-น (prolongs hospitalization)
ก,อค์วัามพ้)การต,อที่ารกในค์รรภ�โด้ยก�าเน)ด้ (congenital anomaly)
จำ�าเป6นต�องได้�ร�บการร�กษาเพ้#�อป7องก�นผลเส&ยอย,างถุาวัร (requires intervention)

จำ�าแนกตามเหต�และผล (Causality
classification)
- ม��นใจำมาก (Definite) ม่#รายงานวิ�เค์ราะห้�ย�นย'นวิ�าเป(นสาเห้ต่)ท#�แท�จร�งต่าม่องค์�ประกอบค์รบถึ�วินค์�อ สอดค์ล้�องก'บเวิล้าข้องการบร�ห้ารยา อาการห้ย)ดใช้�ยาอาการห้ายไป (dechallenge)
อาการจะกล้'บเป(นซ้ำ-$าเม่��อม่#การใช้�ยาน'$นอ#ก (rechallenge)
สาม่ารถึต่รวิจระด'บยาในร�างกายได�
- น,าจำะใชั่, (Probable) เป(นอาการไม่�พื่�งประสงค์�ท#�เก�ดข้�$นไม่�สาม่ารถึสน'บสน)นด�วิยเกณฑ์�ต่�างๆค์ล้�ายระด'บม่'�นใจม่าก

- อาจำจำะใชั่, (Possible) เป6นอาการไม,พ้.งประสงค์�ที่&�เก)ด้ข.-นในชั่,วังเวัลาที่&�อาจำสอด้ค์ล�องก�บเวัลาของการบร)หารยา แต,อาการแสด้งออกน�-นม&ค์วัามเก&�ยวัพ้�นก�บภาวัะโรค์ของผ2�ป3วัยเชั่,น อาการแที่รกซ้�อน
- ไม,น,าใชั่, (Doubtful/ Unlikely) เป6นอาการไม,พ้.งประสงค์�ที่&�เก)ด้ข.-นในชั่,วังเวัลาไม,สอด้ค์ล�องก�บเวัลาของการบร)หารยา

จำ�าแนกตามต�วัอ�กษร 1. Type A (augmented/predictable)
- สามารถุค์าด้การณ�ได้�ล,วังหน�าและม&ค์วัามส�มพ้�นธ์�ก�บขนาด้การใชั่�ยา
เชั่,น ภาวัะค์วัามด้�นโลห)ตต��าจำากการใชั่�ยาลด้ค์วัามด้�นเล#อด้
2. Type B (bizarre/unpredictable)- ไม,สามารถุค์าด้การณ�ได้�ล,วังหน�าเน#�องจำากค์วัามผ)ด้
ปกต)ที่&�เก)ด้ข.-นไม,ค์วัามส�มพ้�นธ์�ก�บฤที่ธ์)9ที่างเภส�ชั่วั)ที่ยาของยา
- พ้บในประชั่ากรส,วันน�อย และอาจำม&ค์วัามเก&�ยวัข�องก�บค์วัามแตกต,างที่างด้�าน
พ้�นธ์�กรรม

3. Type C (chronic) - เก)ด้ข.-นภายหล�งจำากการใชั่�ยาต)ด้ต,อก�นเป6นระยะ
เวัลายาวันาน แต,สามารถุค์าด้การณ�ล,วังหน�าได้� เชั่,น อาการต)ด้ยากล�,ม Benzodiazepines
4. Type D (delayed)
- เป6นการเก)ด้อ�นตรายจำากการใชั่�ยาแบบม&ระยะแฝงนาน เชั่,น การก,อมะเร;ง หร#อ การก,อค์วัามพ้)การต,อที่ารกในค์รรภ�
5. Type E (end-of-treatment)
- อาการเก)ด้ภายหล�งการหย�ด้ใชั่�ยา (withdrawal) อย,างกะที่�นห�น

Type A (augmented/predictable) reactions
Expected extensions of an individual drug’s known
pharmacologic properties and are responsible for the
bulk of ADEs encountered.
Even though their incidence and morbidity is high,
they are rarely life-threatening, although they can
produce significant disability.

Causes of Type A reactions
1. Pharmaceutical causes
- Drug quantity
- Drug release e.g. Osmosin® (slow release indomethacin) GI bleeding
2. Pharmacokinetic causes
- Drug absorption - Drug elimination
- Drug distribution - Drug metabolism
3. Pharmacodynamic causes
- Drug receptors
- Homeostatic mechanisms
- Disease

• Drug absorption
การเพ้)�มการด้2ด้ซ้.มยา เชั่,น การได้�ร�บยา digoxin
ร,วัมก�บ atropine ที่�าให�ร,างกายด้2ด้ซ้.ม digoxin ได้�มากกวั,าปกต) (ADR?)
• Drug distribution
Tetracycline ในเด้;กเล;กม&โอกาสที่�าอ�นตรายต,อโค์รงสร�างของกระด้2กและฟั=นได้�มากกวั,าในผ2�ใหญ่,
Pharmacokinetic causes

• Drug excretion การใชั่�ยา aspirin สามารถุรบกวันการข�บถุ,ายพ้วัก organic acid เชั่,น urate ออกจำากร,างกายที่างไต ผ2�ป3วัยจำ.งม&โอกาสเก)ด้ภาวัะ hyperuricemia
• Drug metabolism
Paracetamol เม#�อใชั่�ในขนาด้ปกต) หร#ออย2,ในร2ป unchanged form จำะม&โอกาสเก)ด้พ้)ษได้�น�อย แต,ส,วันน�อยเม#�อยาถุ2กเปล&�ยนแปลงโด้ย CYP2E1จำะเก)ด้ toxic metabolite ที่&�ม&พ้)ษร�ายแรงต,อต�บ

Paracetamol Metabolism
Glucuronide conjugation
50-60%
Sulphate conjugation
25-35%
N-acetylbenzoquinoimine (NAQI)
CYP 2E1
Hepatotoxicity
Glutathione conjugation
GSH
Mercapturic acid conjugates excreted in urine
2-4%
Covalently-boundparacetamol
Cell macromolecule

Factors predisposing to pharmacological adverse drug reactions
Factor Example Toxicity Mechanism
Pharmaceutical Osmosin Gastrointestinal Release of high(slow release bleeding concentrations ofindomethacin) active drug locally
in GI
Pharmacokinetic* Digoxin Digoxin toxicity Decreased elimination (nausea, arrhythmias) if renal function is
impaired
Pharmacodynamic Indomethacin Left ventricular Water and sodium failure retention
Drug-drug TerfenadineTM Prolonged QT Inhibition ofinteraction* Erythromycin interval and metabolism of torsades de terfenadine by
pointes erythromycin
*Can affect absorption, distribution, metabolism, or excretion.

Ways to minimize both pharmacokinetically- and
pharmacodynamically-derived ADEs include
Understanding the pharmacology of the drug
being prescribed
Monitoring drugs with a narrow therapeutic
window
Avoiding polypharmacy whenever possible

Type B (bizarre/unpredictable) reactions
• Type B reactions include idiosyncratic reactions,
immunologic or allergic reactions (e.g.anaphylaxis),
and carcinogenic/teratogenic events.
• While uncommon, are often among the most
serious and potentially life-threatening of all
ADEs, and are a major cause of important
drug-induced disease.

Receptor abnormality —malignant hyperthermia with general anesthetics
Mechanisms of Type B reaction
- Autosomal dominant genetic disorder of SM
- Mutation in the gene loci corresponding to
skeletal muscle ryanodine receptor (RYR1),
the calcium release channel of sarcoplasmic
reticulum.
-Tachycardia, HT, severe muscle rigidity,
hyperthermia

• Abnormal biological system unmasked by
drug —primaquine induced haemolysis in
patients deficient in glucose 6-phosphate
dehydrogenase

- Genetic heterogeneity among affected individuals with
over 400 variants of the enzyme identified.
- The severity of the problem can vary from hemolysis even in the
absence of oxidative stress to hemolysis only on exposure
to mild to marked oxidant stress.

Abnormalities in drug metabolism
- Atypical pseudocholinesteraseในผู้1�ป2วิยท#�ใช้� succinylcholine เก�ดภาวิะ prolong apnea เพื่ราะ cholinesterase ท-างานแบบผู้�ดปกต่�จ�งไม่�สาม่ารถึก-าจ'ดยาออกได�ต่าม่อ'ต่ราเร3วิข้องค์นปกต่�ได� Atypical ChE ม่# affinity ต่�อ substrate ต่-�าท-าให้� half life นาน
- Polymorphism drug oxidationเชั่,น CYP2D6 polymorphism (debrisoquine/sparteine) CYP2C19 polymorphism (Mephenyltoin)


ตารางเปร&ยบเที่&ยบ Type A และ Type B ADRs
Type A Type B
1. Predictability
2. Dose-dependent
3. Incident
4. Mortality
5. Treatment
6. Pharmacological basis
7. Seriousness
Yes No
Yes No
Common Rare
No Yes
Adjust dose No
Yes No
No Yes

Summary points• Adverse drug reactions are a common clinical problem
• They are diagnosed on clinical grounds from the temporal
relation between the start and finish of drug treatment
and the onset and offset of the reaction
• Pharmacological adverse reactions are generally
dose-dependent, related to the pharmacokinetic properties
of the drug, and resolve when the dose is reduced

• Idiosyncratic adverse reactions are not related to the
known pharmacology of the drug, do not show any
simple dose-response relation, and resolve only when
treatment is discontinued
• Vigilance by clinicians in detecting, diagnosing, and
reporting adverse reactions is important for continued
drug safety monitoring

อาการไม่�พื่�งประสงค์�ท#�เก�ดจากการท#�ยาไปกระต่)�นระบบภ1ม่�ค์)�ม่ก'นข้องผู้1�ป2วิยท-าให้�เพื่��ม่การสร�างสารantibodyม่ากข้�$น ห้ร�อเก�ดจากการท#�เซ้ำล้ล้�เม่3ดเล้�อดข้าวิม่#ค์วิาม่ไวิต่�อการต่อบสนองข้องยาม่ากข้�$น
Drug allergy

ล�กษณะที่&�ส�าค์�ญ่ของการแพ้�ยา1 . เป(นอาการท#�ไม่�เค์ยเก�ดข้�$น จากการใช้�ยาช้น�ดน'$นในค์ร'$งก�อน2. ม่#ระยะแฝงช้�วิงห้น��ง3. ข้นาดน�อยห้ร�อข้นาดปกต่�ท#�ใช้�เพื่��อการร'กษา4. อาการไม่�ส'ม่พื่'นธ์�ก'บฤทธ์�8ทางเภส'ช้วิ�ทยา5. พื่บในประช้ากรกล้)�ม่น�อย6. อาการเก�ดม่#ล้'กษณะเฉพื่าะ7. บางรายต่รวิจพื่บ Ab ห้ร�อ T-lymphocyte
8. ยาท#�ม่#โค์รงสร�างทางเค์ม่#ใกล้�เค์#ยงก'นจะท-าให้�เก�ดการแพื่�แบบเด�ม่

ค์�ณสมบ�ต)ของยาที่&�ที่�าให�เก)ด้การแพ้�ได้�บ,อย1. ม&ขนาด้หร#อน�-าหน�กโมเลก�ลมาก เช้�นสารช้#วิวิ'ต่ถึ)ห้ร�อยาท#�ท-าจากโปรต่#น ซ้ำ��งสาม่ารถึท-าห้น�าท#�เป(นแอนต่�เจนไปกระต่)�นการท-างานข้องสารantibodyแล้ะท-าให้�เก�ดอาการแพื่�ได�โดยต่รง2. ม& Reactive metabolite ที่&�ที่�าให�เก)ด้การแพ้�
โดยสาร metabolite สาม่ารถึรวิม่ต่'วิก'บโปรต่#นได�ง�ายข้�$นห้ร�อม่#ค์วิาม่ไวิต่�อปฏิ�ก�ร�ยาทางเค์ม่#ม่ากข้�$น e.g. penicillin
3. ม&สารที่&�ที่�าให�แพ้�ที่&�เก)ด้จำากการสลายต�วัของยาเช้�น penicillenic acid, pennicilloic acid

4. เก)ด้ polymerization ได้�ง,าย ยาเต่ร#ยม่บางช้น�ดเก�ดข้บวินการ polymerization ท-าให้�ได�เป(นสารให้ม่�ท#�ม่#โม่เล้ก)ล้ให้ญ่�ม่ากข้�$น เช้�น ampicillin
5. ม& contaminants or additives ที่&�ที่�าให�เก)ด้การแพ้�เช้�นโปรต่#นท#�เก�ดระห้วิ�างข้บวินการผู้ล้�ต่ benzylpenicillin สาม่ารถึรวิม่ต่'วิก'บ
ยาได�สารเช้�งซ้ำ�อน ในร1ป pennicilloylated protein
6. ม&โค์รงสร�างใกล�เค์&ยงก�บยาที่&�เค์ยแพ้�มาก,อน เช้�น penicillins, cephalosporins

Type I — Anaphylactic/ Immediate type
(e.g., Penicillin, insulin urticaria or anaphylaxis)
Type II — Cytotoxic type
(e.g., drug-induced haemolytic anaemia or thrombocytopenia [reduced platelets])
Type III — Immune complex type
(e.g., serum sickness-like drug reactions)
Type IV — Cell-mediated or delayed hypersensitivity
(e.g., neomycin contact dermatitis)
กลไกของการแพ้�ยา

• เก�ดข้�$นรวิดเร3วิ แล้ะร)นแรง• กล้ไกการเก�ดจากยาท-าห้น�าท#�เป(น Ag เข้�าท-าปฏิ�ก�ร�ยาก'บ IgE ท#�อย1�บนผู้�วินอกข้อง mast cells แล้ะ basophils• Systemic anaphylaxis, ล้ม่พื่�ษ , ห้�ดช้น�ดภ1ม่�แพื่� , angioneurotic edema
Type I: Anaphylactic/Immediate type

• เก)ด้จำากการที่�าลายของเซ้ลล�ของระบบเล#อด้เป6นส,วันใหญ่,• hemolytic anemia, thrombocytopenia, granulocytopenia
Type II: Cytolytic Reactions
The Fab of IgG reacts with epitopes on the host cell membrane. Phagocytes bind to the Fc portion.
Phagocytes binding to the Fc portion of the IgG and discharge their lysosomes causing cell lysis.

Type III: Immune Complex Reactions
• ยาจำะที่�าปฏิ)ก)ร)ยาก�บ IgG ได้�เป6นสารประกอบเชั่)งซ้�อน immune complexes
แล�วักระต��นระบบ complement ที่�าให�เก)ด้การที่�าลายเซ้ลล� หร#อเน#-อเย#�อ• Glomerulonephritis

IgG และ IgM ที่�าปฏิ)ก)ร)ยาก�บ antigen ที่&�จำ�าเพ้าะในกระแสเล#อด้แล�วัเก)ด้ immune complex ไปตกตะกอนสะสมอย2,ในหลอด้เล#อด้ตามอวั�ยวัะต,างๆในร,างกาย

-จำากน�-นม&การกระต��น complement ที่�าให�เม;ด้เล#อด้ขาวัมาชั่�มน�มก�นและจำ�บก)นเพ้#�อก�าจำ�ด้ antigen น�-น เม;ด้เล#อด้ขาวัและ phargocyte ที่&�มารวัมก�นน�-นจำะหล��ง lysosomal enzyme ที่�าให�เก)ด้ขบวันการอ�กเสบและที่�าลายเน#-อเย#�อใกล�เค์&ยงอวั�ยวัะน�-นๆ- ถุ�าปฏิ)กร)ยาเก)ด้เฉพ้าะที่&�เร&ยกวั,า arthus reaction- ถุ�าเก)ด้ก�บอวั�ยวัะต,างๆที่��วัร,างกายเร&ยกวั,า serum sickness

Type IV: Cell-Mediated Reactions
• เก)ด้จำากยาไปจำ�บก�บต�วัร�บเฉพ้าะที่&�อย2,บนเซ้ลล� หร#อ ม& macrophage มาก)น แล�วัที่�าให�เก)ด้การกระต��นการที่�างานของ T cells • Contact dermatitis, fixed-drug eruptions

ม่#อาการค์'น ห้ล้'งจากน'$นจะม่#อาการบวิม่อาจจะเป(นข้นาดเล้3กห้ร�อข้นาดให้ญ่�ต่รง
กล้างแผู้�นส#จะจางแล้ะไม่�น1น โดยม่าก ผู้��นจะห้ายไปใน 24 ช้'�วิโม่ง
ม�กเก)ด้จำากยากล�,ม penicillin, sulfonamide
Urticaria:

- กล้ไกการเก�ดจะเห้ม่�อนก'บ ล้ม่พื่�ษ- อาการบวิม่จะล้�กถึ�งช้'$นห้น'งแท�แล้ะ
ช้'$นไข้ม่'น- ต่-าแห้น�งท#�เก�ดม่'กจะอย1�บร�เวิณใบห้น�า, ห้น'งต่า, ล้�$น อวิ'ยวิะเพื่ศ- ไม่�ค์�อยพื่บบร�เวิณแข้นห้ร�อข้า ผู้��นม่'กไม่�ค์'น- ม่'กเก�ดจากยากล้)�ม่ penicillin,
sulfonamide
Angioedma

- ผ#�นแด้งแบนราบ ต�,มแข;ง ต�,มน�-าใสและต�,มพ้องตรงกลางอาจำเป6นต�,มน�-าหร#อเล#อด้ออกตรง
กลางเหม#อนม,านตา iris หร#อtarget ซ้.�งเป6นล�กษณะเฉพ้าะของโรค์- ม�กเก)ด้จำากยากล�,มpenicillin,
sulfonamide,
barbiturate, NSAIDs,
phenyltoin,
allopurinol
Erythema multiforme:

- เร)�มเป6นผ#�นวังแด้งขอบ ชั่�ด้เจำน
ม&อาการปวัด้แสบปวัด้ร�อน ต,อ มาจำะเปล&�ยนเป6นส&ค์ล�-า เป6น
รอยด้�าขอบชั่�ด้เจำน ม�กเก)ด้ซ้�-าบร)เวัณเด้)ม- ม�กเก)ด้จำากยากล�,มtetracyclin, sulfonamide
Fixed-drug eruptions:

- ผู้�วิจะล้อกออกเห้ม่�อนแผู้ล้ถึ1กไฟไห้ม่�- ม�กเก)ด้จำากยากล�,มpenicillin, sulfonamide, barbiturate, hydantoin, NSAIDs, phenyltoin, allopurinol
Toxic Epidermal Necrolysis (TEN):

- นอกจากผู้��นท#�ผู้�วิห้น'งล้'กษณะเห้ม่�อนerythema multiforme
ม่'กจะม่#ผู้��นท#�ต่าท-าให้�เก�ดต่าแดง ปากม่#แผู้ล้ ห้ล้ายแห้�ง อ�าปากไม่�ข้�$น อวิ'ยวิะเพื่ศ
ม่#แผู้ล้รวิม่ท'$งทวิารห้น'ก ท-าให้�ถึ�ายเห้ล้วิ- ม่'กเก�ดจากยากล้)�ม่ penicillin,
sulfonamide, barbiturate, hydantoin,
NSAIDs, phenyltoin, allopurinol
Steven Johnson Syndrome:

เอกสารอ,านเพ้)�มเต)ม1 .สาระพื่�ษวิ�ทยา : จากพื่�$นฐานส1�ข้�างเต่#ยงผู้1�ป2วิย2 . www.who.int
3 . www.fda.gov/medwatch

THE END