Embed Size (px)
Citation preview

Basic Cardiac Electrophysiology Basic Cardiac Electrophysiology and ECG Conceptsand ECG Concepts
胡瑜峰醫師胡瑜峰醫師台北榮總心臟內科台北榮總心臟內科

Outline Outline
• Ion current, action potential and cardiac conduction
• Surface EKG• Intracardiac mapping• Mechanism and catheter ablation

Electrical System of the HeartElectrical System of the Heart
Purkinje fibers
Bundle of His
Sinoatrial node
Atrioventricular node
Pacemakers – Sinoatrial node, Atrioventricular node, Purkinje fibers

Pacemaker ActivityPacemaker Activity
• Spontaneous time-dependent depolarization leading to action potentials
• Pacemaker with highest frequency sets the heart rate. – SA node – 60 beats/min – smallest electrical region in the
heart, sum of 3 ion channels produces pacemaker (ca, k, f)– AV node – 40 beats/min – can take over for SA node,
pacemaker determined by same three channels as SA node. – Purkinje fibers –20 beats/min – unreliable pacemaker, but
great conducting system, pacemaker determined by ‘f’ channels only.

INa+
rapiddepolarizing(non-nodal)
IK+
repolarizing(all myocytes)
ICa+
depolarizing(nodal AP
and myocytecontraction)
If
“funny channel” or HCNPacemaker current
(activated during hyperpolarization)Hyperpolarization activated Cyclic
Nucleotide gated channel
Na+/K+
(activated during depolarization)
MAJORMYOCYTE
ION CHANNELS
Which channelis absent in SA and AV node?Absent in ventricular myocytes?
Read-Table 20-1

Pacemaker Action PotentialPacemaker Action Potential

Cardiac Muscle DepolarizationCardiac Muscle Depolarization

Ventricular Action PotentialVentricular Action Potential5 Phases
0 – upstroke of APICa+ – slowICa+/INa+ - fast
1 – rapid repolarizationIk+ – activationICa+/INa+ - inactivation
2 – plateau phaseICa+/INa+ - activated
3 – repolarizationIk+
4 – diastolic potential Ik+, ICa+, If
Produce pacemaker activitySA/AV node, purkinje use If
Phase 1 and 2 not present in SA/AV nodePhase 1 and 2 not present in SA/AV node

Comparison of Slow Nodal and Comparison of Slow Nodal and Fast Non-nodal Cardiac Action PotentialsFast Non-nodal Cardiac Action Potentials


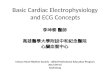
Velocity of Electrical ConductionVelocity of Electrical Conduction
Purkinje fibersPurkinje fibers
Bundle of HisBundle of His
(0.05 m/s)(0.05 m/s)
(0.05 m/s)(0.05 m/s)
(1.0-2.0 m/s)(1.0-2.0 m/s)
(1 m/s)(1 m/s)
(2.0-4.0 m/s)(2.0-4.0 m/s)
Functionally, how might the speeds be important?
(0.3-1.0 m/s)(0.3-1.0 m/s)
Ventricdular myocardiumVentricdular myocardium

Fletcher G F et al. Circulation 2001;104:1694-1740Copyright © American Heart Association
12 Lead ECG Electrode Placement12 Lead ECG Electrode Placement

Surface EKG MorphologySurface EKG Morphology

As the heart beats action potentials on the heart cause an electrical signal on the body surface.
The larger the structure the greater the voltage it induces. This voltage pattern is called the electrocardiogram

Atrial depolarization gives Atrial depolarization gives rise to the P wave rise to the P wave

Conduction through Conduction through the small AV node is the small AV node is
associated with associated with virtually no electrical virtually no electrical
signal on the skin.signal on the skin.

Depolarization of Depolarization of the ventricle causes the ventricle causes the QRS complex. the QRS complex.
QRS is large QRS is large because the because the ventricular ventricular mass is largemass is large
QRS is short QRS is short because because conduction over conduction over the ventricles is the ventricles is very fast very fast

Repolarization of the ventricle causes the T wave
Dispersion causes it to be smaller and last longer than the QRS complex. Repolarization is not a conducted wave.

Conduction/ Surface EKG MorphologyConduction/ Surface EKG Morphology

12 Lead-12 Directions12 Lead-12 DirectionsHelp to Analyze Gross Heart conductionHelp to Analyze Gross Heart conduction

Normal atrial depolarization

12 Lead-12 Directions12 Lead-12 DirectionsHelp to Analyze Gross Heart conductionHelp to Analyze Gross Heart conduction

12 Lead-12 Directions12 Lead-12 DirectionsTransition of Precordial LeadsTransition of Precordial Leads


12 Lead-12 Directions12 Lead-12 DirectionsHelp to Analyze Gross Heart conductionHelp to Analyze Gross Heart conduction


Accessory PathwaysAccessory Pathways

Different Morpholgy indicates Different Morpholgy indicates different location-Atrial Tachycardiadifferent location-Atrial Tachycardia

12 Lead-12 Directions12 Lead-12 DirectionsHelp to Analyze Gross Heart conductionHelp to Analyze Gross Heart conduction


Limb Leads • 1. R1 + SIII > 25 mm• 2. R wave in aVL > 11 mm• 3. R wave in aVF > 20 mm• 4. S wave in aVR > 14 mmPrecordial Leads • 5. R wave in V5 or V6 > 26 mm• 6. R wave in V5 or V6 + S wave in V1 > 35 mm• 7. Largest R wave + largest S wave in the
precodial leads > 45 min
Voltage Indicates Ventricular MassVoltage Indicates Ventricular Mass-Left Ventricular Hypertrophy-Left Ventricular Hypertrophy

12 Lead-12 Directions12 Lead-12 DirectionsHelp to Analyze Gross Heart conductionHelp to Analyze Gross Heart conduction

Left Ventricular HypertrophyLeft Ventricular Hypertrophy

Intracardiac MappingIntracardiac Mapping

HRAHRA
HisHis
RVRV
CSCS

Example-Atrial TachycardiaExample-Atrial Tachycardia

Intracardiac MappingIntracardiac Mapping
Voltage imply the tissue electrical Voltage imply the tissue electrical function or viabilityfunction or viability

Aging Changes of Typical AFL
Huang JL, Heart rhythm 2008

Intracardiac MappingIntracardiac Mapping
The timing of signal indicate the activation timeThe timing of signal indicate the activation time

Isochronal Map (Activation map)Isochronal Map (Activation map)

Distribution of AF triggerDistribution of AF trigger
Haissagurre et al. NEJM 1998Haissagurre et al. NEJM 1998 Chen et al. Circulation 1999Chen et al. Circulation 1999

Circumferential PV Isolation and Segmental Circumferential PV Isolation and Segmental AblationAblation

Thank you for your attention!Thank you for your attention!