Embed Size (px)
DESCRIPTION
Presented at AWS General Hospital, supervised by dr. Arie Ibrahim SpBS
Citation preview

HEAD TRAUMADr. Isa Basuki
Department of Surgery, AWS General Hospital
Faculty of Medicine, Mulawarman University

INTRODUCTION
Head trauma or Traumatic brain injury (TBI) is a disruption or alteration of brain function due to external forces
The external forces creating the injury may be the result of: acceleration or deceleration, direct compression, penetrating objects, combined effects, complex mechanisms

INTRODUCTION
It may produce: fractures, contusion, subarachnoid hemorrhage (SAH), subdural hemorrhage (SDH), epidural hemorrhage (EDH), Intraparenchymal hemorrhage (IPH), diffuse axonal injury (DAI).
All injuries and symptoms should be taken seriously

EPIDEMIOLOGY
Approximately 1.4 million people per year suffer TBI
1.1 million are treated and released, 240,000 are hospitalized, and 50,000 die
Common causes: Falls (28%), Motor vehicle accidents (20%), Pedestrian impact (19%), Assault (11%)
Age distribution with the greatest risk in 0–4 and 15- to 19-year-olds.
Males have 1.5 times the risk of females

PATHOPHYSIOLOGY
Primary injuries disruption of scalp (lacerations), bone (cranial vault, skull base,
facial bones), vasculature
(SDH/EDH/IPH/intraventricular hemorrhage [IVH], traumatic aneurysm),
brain parenchyma (contusion, DAI)
Secondary injuries hypoxemia, ischemia, initial hyperemia, cerebral edema, expansion of hemorrhages
increased intracranial pressure (ICP),
seizures, metabolic abnormalities systemic insults



GENERAL PRINCIPLES

SYSTEMIC EVALUATION AND RESUSCITATION
Assessment and treatment often begins in the prehospital setting
The basic principles of trauma resuscitation rapid assessment and maintenance of an airway, breathing, and circulation
medical and surgical history should be obtained including: the events preceding a trauma, a description of the accident scene, accurate description of the patient’s neurological baseline, any subsequent changes to the neurological status

SYSTEMIC EVALUATION AND RESUSCITATION
In the newborn or premature infant cephalohematoma may allow enough displacement of blood to produce hemodynamic instability
Raccoon’s eyes (periorbital ecchymosis),
Battle’s sign (postauricular ecchymosis), suggest a basilar skull fracture
otorrhea/rhinorrhea
Puncture wounds penetrating injury to the brain, spinal cord, sympathetic plexus, or vasculature
Bruits of the carotid artery carotid dissection or carotidcavernous fistula


NEUROLOGICAL EXAMINATION
Accurate neurological examination is essential
The exam may be limited due to: patient’s age level of education native language presence of sedative or paralytic medication
• Illicit drugs • hypotension • hypoxia • hypothermia• hypoglycemia


PUPILLARY RESPONSE
parasympathetic, pupilloconstrictor, and light reflex (pupillary reflex) can be easily and rapidly assessed in the unconscious patient
Damage to the Edinger–Westphal nucleus or uncal compression of CN III at the tentorial notch pupillary dilatation (≥4 mm)
Direct orbital trauma can also result in pupillary dilation/fixation in the absence of temporal lobe herniation or intracranial hypertension (ICHTN).

GLASGOW COMA SCALE
standard for objective measurement of TBI severity
three parameters: best eye opening [E] best verbalization [V], best motor function [M]
GCS = 13 – 15 mild TBI
GCS = 9 – 12 moderate TBI
GCS = 3 – 8 severe TBI
If the patient is intubated 1 for the verbal component and the overall scored is annotated with a “T.” Examples: M4/VT/E2 = 4 + 1 + 2 = 7T


GLASGOW COMA SCALE (RECOMMENDED FOR AGE ≥4)

GLASGOW COMA SCALE FOR CHILDREN (RECOMMENDED FOR AGE <4)

RADIOGRAPHIC EVALUATION

PLAIN X-RAYS
For evaluating and clearing the cervical spine.
The spine is imaged from the occiput to T1 and a C-collar
AP, lateral and odontoid views are the most useful
T- and L-spine films are obtained based on: mechanism of injury, degree of neurological deficits, pain

CT SCAN
CT scan findings after trauma: SDH, EDH, SAH, IPH, IVH contusions hydrocephalus cerebral edema or anoxia skull fractures ischemic infarction (if >12 hours
old) mass effect midline shift
Indications for an initial post-traumatic CT scan: GCS ≤ 14 unresponsiveness, focal deficit, amnesia for the injury, altered mental status, signs of basilar skull fracture

MRI
better parenchymal resolution
can evaluate infarction, ischemia, edema, and DAI
helpful to determine ligamentous injury of the spine or traumatic cord injury
generally performed after the initial trauma evaluation and resuscitation have been completed
Disadvantages: limited availability slower image acquisition time increased cost

CLASSIFICATION AND SURGICAL MANAGEMENT OF SPECIFIC
INJURIES

SKULL FRACTURES
can be described by: The state of the overlying scalp (closed or open), The number of bone fragments (simple or compound), The relationship of bone fragments to each other (depressed or nondepressed), Whethert the fracture enters or widens an existing cranial suture (diastatic,
more common in children), and whether it involves the cranial vault or skull base
lower force impacts (falls from standing) more linear, closed, and without dural laceration
Higher force impacts (MVA, falls from heights, penetrating trauma) compound, open fractures with underlying dural or cerebral injury
“Ping-pong” fractures are greenstick-type fractures usually seen in newborns

CT bone windows showing ping-pong skull fracture.
The multiple nondisplaced linear lucencies are normal sutures.

SKULL FRACTURES
Associated clinical signs of: calvarial skull fractures gross deformity and palpable skull fracture in
patients with open scalp lacerations Basilar skull fractures postauricular or periorbital ecchymosis,
hemotympanum or laceration of the external auditory canal, and CSF rhinorrhea or otorrhea
Cranial nerve injuries: fractures of the cribriform plate (CN I, anosmia) optic canal (CN II, visual deficit) temporal bone (CN VII, facial weakness; or CN VIII, hearing loss)
Severe basilar skull fractures pituitary gland injury endocrinopathies

SKULL FRACTURES
Direct injury to vasculature that penetrates the skull base Arterial dissection, Traumatic aneurysm formation, Traumatic carotid-cavernous sinus fistula with symptoms:
cranial neuropathies chemosis bruits Strokes

SKULL FRACTURESRADIOGRAPHIC DIAGNOSIS
Differential Diagnosis of Fractures on Skull X-Rays

SKULL FRACTURESRADIOGRAPHIC DIAGNOSIS
Most skull fractures are discovered by CT scan
Plain films may be superior to CT scan in discovering linear calvarial fractures parallel to the skull base
CT angiograms/venograms to assess fractures involving skull base foramen containing vasculature (e.g.,
carotid canal, foramen magnum) fractures that cross major venous sinuses (superior sagittal or transverse
sinuses, jugular foramen).
Closed, nondisplaced fractures do not require immediate intervention
Open skull fractures should be debrided and carefully inspected and all should receive antibiotics

SKULL FRACTURES
Relative indications for surgical elevation of a depressed skull fracture: depression of more than 8–10 mm or more than the thickness of the
skull Focal neurological deficit clearly attributable to compressed underlying
brain, Significant intraparenchymal bone fragments (implying dural
laceration), Persistent deformity after all swelling has subsided
Current recommendations: surgical repair open fractures depressed greater than the thickness of
the cranium nonoperative management open depressed cranial fractures if there
is no evidence of dural penetration

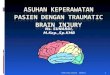
CT bone windows showing a depressed skull fracture that
required surgical elevation and dural repair.
The patient also had an underlying brain contusion and presented with
a receptive aphasia

SKULL FRACTURES
Indications for surgery: significant intracranial hematoma, depression >1 cm, frontal sinus involvement, Gross cosmetic deformity, wound infection, pneumocephalus, gross wound contamination

FOCAL CEREBRAL INJURIESCEREBRAL CONTUSION
Injuries to the superficial gray matter of the brain
External forces acceleration of the intact skull or fractured skull fragments toward the
brain surface or the brain continues to move toward the rapidly decelerating skull and
dural folds of the falx or tentorium
“Coup” lesions ipsilateral to the impact site adjacent calvarial fractures
“Contrecoup” lesions opposite the coup lesion rebounding brain striking the inner table of the skull
CT scans patchy, hyperdense lesions with a hypodense background

FOCAL CEREBRAL INJURIESINTRAPARENCHYMAL HEMORRHAGE
8.2% of all TBI and up to 35% of severe TBI cases
Delayed traumatic intracerebral hemorrhage (DTICH) approximately 20% of cases and most occur within 72 hours of the initial trauma
Indications for surgical decompression: neurological decline referable to the TICH lesion TICH > 50 cm3
GCS = 6 – 8 with frontal or temporal contusions >20 cm3 with midline shift ≥5 mm and/or cisternal compression on CT scan
Surgical procedures range Localized frontal or temporal craniotomy with resection of underlying focal
clot Extensive craniectomies with duraplasty, evacuation of severely contused
brain, or temporal lobectomy

FOCAL CEREBRAL INJURIESEPIDURAL HEMORRHAGE
blood collects in the potential space between the dura and inner table of the skull
1% of all head trauma admissions and in 5–15% of patients with fatal head injuries
more common in males (M:F = 4:1)
usually occurs in young adults
90% of EDHs are due to arterial bleeding fracture at the middle meningeal artery groove
10% are due to venous bleeding violation of a venous sinus by an occipital, parietal, or sphenoid wing fracture

FOCAL CEREBRAL INJURIESEPIDURAL HEMORRHAGE
Location of EDH: lateral convexity of a cerebral hemisphere (70%), frontal (5–10%), parieto-occipital (5–10%), posterior fossa locations (5–10%)
CT scan hyperdense, biconvex (lenticular) mass adjacent to the inner table of
the skull (84%) medial edge being straight (11%) crescentic resembling an SDH (5%)
Additional associated findings SDHs and cerebral contusion

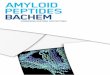
CT showing epidural hemorrhage. Note the biconvex- or lenticular-shaped hemorrhage.
On the bone windows this was adjacent to a diastatic left lambdoid suture.

FOCAL CEREBRAL INJURIESEPIDURAL HEMORRHAGE
Clinical presentation: Brief post-traumatic loss of consciousness
(LOC) 40% Lucid interval (80%) Obtundation Contralateral hemiparesis, Ipsilateral (85%) pupillary dilatation (60%)
Kernohan’s phenomenon (a false localizing sign) local hemispheric mass effect compression of the contralateral brainstem
against the tentorial notch ipsilateral hemiparesis
Mortality unilateral EDH (5–12%) Bilateral EDH (15–20%) no lucid interval (20%) posterior fossa location (25%)
concurrent acute SDH (25–90%)


FOCAL CEREBRAL INJURIESEPIDURAL HEMORRHAGE
Rapid diagnosis and intervention when indicated optimize the outcome
Guidelines: Surgical EDH of >30 cm3 should be evacuated regardless of GCS score Conservative EDH of <30 cm3 and <15 mm of thickness and >5 mm
midline shift (frequent neurological examinations and serial CT scan)
Relative indications EDHs that are neurologically symptomatic or have a maximal thickness >1 cm.
Absolute indication acute EDH in coma (GCS ≤ 8) and anisocoria
Craniotomy complete clot evacuation with meticulous hemostasis and use of tackup sutures to decrease the potential epidural space

FOCAL CEREBRAL INJURIESSUBDURAL HEMORRHAGE
blood collects between the arachnoid and inner dural layer
Type/variants: hyperacute (<6 hours), acute (6 hours to 3 days), subacute (3 days to 3 weeks), chronic (3 weeks to 3 months)
Etiologies: traumatic stretching and tearing of cortical bridging veins coagulopathy, subdural dissection of ICH, rupture of a vascular anomaly (AVM, aneurysm, cavernoma, dural AV
fistula) into the subdural space



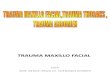
CT showing an acute subdural hemorrhage. Note that crescentic hemorrhage crosses under the right coronal suture.

APPEARANCE OF SDH ON CT AND MRI

FOCAL CEREBRAL INJURIESSUBDURAL HEMORRHAGE
Guidelines suggestion for SDH evacuation: acute SDH with thickness >1 cm or a midline shift >5 mm regardless GCS
score acute SDH <1 cm thick and midline shift <5 mm and in coma (GCS ≤8) if:
GCS decreases by 2 points. pupils that are asymmetric or fixed/dilated. the ICP ≥20 mm Hg.
Craniotomy ASAP, may require craniectomy and duraplasty for ICP control
Mortality 50% to 90% (related more to the underlying injury, increased in the elderly and in patients on anticoagulants)
Outcome mortality improvements from 66–90% down to 30–59% if the patient was operated on in less 4 hours


FOCAL CEREBRAL INJURIESSUBARACHNOID HEMORRHAGE
blood located between the pial and arachnoid membranes
results from venous tears in the subarachnoid space
33% of patients with moderate head injury and is found in nearly 100% of trauma patients at autopsy.
CT scan sulcal hyperdensity
MRI FLAIR hyperintensity
Clinical presentation headache, emesis, and lethargy
Treatment supportive using IV fluids, anticonvulsants, and nimodipine (to prevent vasospasm)

CT with arrow pointing to a small traumatic subarachnoid hemorrhage in left central sulcus

CT AND ANGIOGRAM OF ICH

DIFFUSE CEREBRAL INJURIESCONCUSSION
an alteration of consciousness resulting from nonpenetrating injury to the brain
Classic symptoms: headache confusion amnesia LOC
Additional symptoms: Deficits of motor function (incoordination, stumbling), Speech (slowed, slurred, incoherent), Memory or processing (amnesia, short-term memory loss, difficulty concentrating or
focusing, inattention, perseveration, easy distractibility), Orientation (vacant stare, “glassy eyed,” unable to orient to time/date), Irritability

CONCUSSION GRADING

DIFFUSE CEREBRAL INJURIESCONCUSSION
Physiological responses transient increase in cerebral blood volume due to loss of vascular autoregulation
mild cases mild cerebral swelling, or hyperemia
more severe cases malignant cerebral edema elevated ICPs refractory to nearly all measures and 50–100% mortality “second impact syndrome”
CT scan subtle or nonexistent and include mild diffuse swelling secondary to hyperemia
Treatment recognition of injury

DIFFUSE CEREBRAL INJURIESDIFFUSE AXONAL INJURY
traumatic axonal stretch injury caused by overlying cerebral cortex and underlying deep brain structures moving at different relative speeds
Mild axonal stretching + transient neuronal dysfunction
Severe axonal shearing + permanent neuronal damage
80% microscopic and nonhemorrhagic with impaired axonal transport and delayed axonal swelling
CT scans normal (50–80%) or hyperdense petechial hemorrhage (20–50%)
MRI multifocal hyperintense T2 at frontal lobes (67%), corpus callosum (20%), and brainstem (10%)
Prognosis generally related to the patient’s age, presenting neurological status, and trajectory of neurological improvement.


MANAGEMENT OF TRAUMATIC BRAIN INJURY

MEDICAL MANAGEMENT
Basic measures: ICU setting with frequent monitoring of:
vital signs, fluid intake and output neurological examinations (as permitted)
Multiple invasive lines for: blood pressure (arterial line), volume assessment (Swan–Ganz), administration of fluids, medication, or nutrition (central venous catheter), urine output or temperature (Foley catheter), ICP, cerebral tissue oxygenation, or cerebral blood flow (CBF)

MEDICAL MANAGEMENT
kept normothermic and euvolemic with isotonic fluids
GI prophylaxis against Cushing’s (stress) ulcer
head of bed should be elevated to 30–45°
neck should be kept midline
cervical collar and endotracheal tube stabilizer prevent compression of the jugular veins promote venous outflow from the head

BLOOD PRESSURE AND OXYGENATION
single episode of hypoxemia (apnea, cyanosis or O2 saturation <90% in the field, or PaO2 < 60 mmHg) or hypotension (SBP < 90 mmHg) predictor of worse outcome
Oxygen saturation and blood pressure monitoring started in the field and continued at hospital setting
Goal identifying, avoiding, and rapidly correcting hypoxemia or hypotension
Oxygen administration start as early as possible (may require endotracheal intubation)
isotonic or hypotonic saline, plasma, colloid, blood, or intravenous pressors to avoid hypotension

INTRACRANIAL PRESSURE ASSESSMENT
modified Monro–Kellie hypothesis Assuming that the skull is completely inelastic, the ventricular space is
confluent pressures are equally and readily transmitted throughout the intracranial space
balance between the brain, blood volume, and CSF in the intracranial space Increases in the volume or addition of new components compensatory
decreases in other constituents to maintain the same ICP
Mildly increased, localized pressure in the brain neurological dysfunction of the immediate area
severe pressure increases local tissue compression, shift of intracranial structures, subfalcine and transtentorial herniation
most severe compression at the level of the brainstem, occlusion of brainstem vasculature, infarction, and death.


ICP MONITORING
Normal ICPs: <10–15 mm Hg in adults 3–7 mm Hg in children 1.5–6 mm Hg in infants
ICP monitoring is recommended for: patients with severe TBI (GCS= 3 – 8) abnormal CT scan or with severe TBI considered in patients without an accurate neurological examination
due to sedatives, paralytics, or general anesthesia required
Higher mortality ICP persistently above 20 mm Hg.


ANALGESICS AND SEDATIVES
Pain and agitation can cause increased sympathetic tone, increased temperature, and hypertension increased venous and ICP, increased metabolic demand, resistance to controlled ventilation
may require sedatives or psychotropic medication to prevent self-injurious behavior and dislodgement of airway, vascular lines, or monitoring equipment
If on ventilators, may require sedatives or paralytics to allow appropriate lung excursion or timing of breath patterns.
side effects hypotension, alteration or obliteration of the neurological examination, and rebound ICP elevation

ANALGESICS AND SEDATIVES
AGENTS ADVANTAGESHaloperidol relatively nonsedating quality useful for
agitation
fentanyl and its related derivatives (remifentanil, sufentanil)
short acting, reversible, and conducive to administration by continuous infusion for acute and longer-term analgesia
Midazolam short-acting benzodiazepine effective for sedation of the ventilated TBI patient.
Propofol hypnotic anesthetic with rapid onset and a very short half-life facilitates rapid neurological assessment, reduces cerebral metabolism and oxygen consumption and exerts a neuroprotective effect

HYPEROSMOLAR THERAPY
Mechanism of Mannitol: first few minutes produces immediate plasma expansion with reduced
hematocrit and blood viscosity improved rheology, and increased CBF and O2 delivery reduces ICP
Over the next 15–30 minutes produces an osmotic effect with increased serum tonicity and withdrawal of edema fluid from the cerebral parenchyma.
Bolus ICP reduction is evident at 1–5 minutes and peaks at 20–60 minutes
Initial bolus of mannitol 1 g/kg
Subsequent administration at smaller doses and longer intervals (i.e., 0.25–0.5 g/kg Q 6 hours)
Furosemide may also be used synergistically with mannitol

HYPEROSMOLAR THERAPY
Serum osmolality should be monitored (>320 mOsm/L use of mannitol should be restricted)
Larger dose (1,4 g/kg) improved outcome of the comatose patients with: operative subdural hematomas operative intraparenchymal temporal lobe hemorrhages abnormal pupillary dilatation

HYPERTONIC SALINE
lower ICP through two mechanisms:1. oncotic pressure gradient, across the BBB, results in mobilization of water from brain
tissue and hypernatremia2. rapid plasma dilution and volume expansion, endothelial cell and erythrocyte dehydration,
and increased erythrocyte deformability improvements in rheology, CBF, and oxygen delivery
Administration: continuous infusion of 25–50 mL/h of 3% saline bolus infusions of 10–30 mL of 7.2%, 10%, or 23.4% saline solution
Onset minutes and may last for hours
Serum sodium and osmolality levels should be aggressively followed central pontine myelinolysis (most often in patients with preexisting, chronic hyponatremia)
may also induce or exacerbate pulmonary edema in patients with underlying cardiac or pulmonary deficits

HYPERVENTILATION
lowers PCO2 with subsequent vasoconstriction, reduction of cerebral volume, and reduction in ICP
Time of onset 30 seconds to 1 hour,
Peak effect 8 minutes and may last up to 15–20 minutes
should be avoided during the first 24 hours postinjury CBF is most reduced
after the first 24 hours short-term, mild HPV (PCO2 = 30 – 35) ICP control
moderate HPV should be avoided
Prophylactic HPV (PCO2 ≤ 25) is contraindicated increased ischemia and worse outcomes

DECOMPRESSIVE CRANIECTOMY
The bone is removed, the lesion is resected, and the dura and bone are replaced
Severe cases diffuse cerebral edema, contusions of large size in eloquent areas, or multiple, coalesced contusions leave the bone flap off.
Most common unilateral hemispheric
Bifrontal and bilateral hemispheric craniectomies based on the location and severity of the underlying lesion(s)
The dura is opened widely and areas of noneloquent contused and devitalized brain can be removed if required
hemispheric technique at least 12-cm cranial flap is removed

CT of a bilateral hemispheric decompressive craniectomy performed in a patient with severe edema from a likely second impact syndrome.

BARBITURATES
Benefit: decreasing metabolic demand for oxygen (CMRO2) decreasing free radicals and intracellular calcium lowering ICPs
Side effects: immunosuppression hypotension (reduced sympathetic tone and mild cardiodepression)
Patients exclusion: hemodynamic instability, sepsis, respiratory infection, cardiac risk factors

BARBITURATES
loading dose 10 mg/kg over 30 minutes followed by a 5 mg/(kg h) infusion for 3 hours
maintenance dose 1 mg/(kg h)
Serum barbiturate levels 3–4 mg%

HYPOTHERMIA
Improve outcome in patients with severe TBI through reduction of: cerebral metabolism, ICP, inflammation, lipid peroxidation, excitotoxicity, cell death, Seizures
Side effects: Decreased cardiac function thrombocytopenia elevated creatinine clearance pancreatitis shivering

HYPOTHERMIA
patients who were hypothermic on admission had improved outcomes when hypothermia was maintained
target temperature 32–33°C (maintained for greater than 48 hours)
patients should be closely monitored for electrolyte abnormalities, hypocoagulability, and cardiac rhythm alterations
Rewarming very slow (not exceeding more than 1° per 24 hours)

STEROIDS
Glucocorticoids are not recommended
Side effects of steroid: coagulopathies, hyperglycemia, increased infection

SPECIFIC SYSTEM CONSIDERATIONS

NUTRITION
All injured patients show an increase in basal energy expenditure (BEE)
Patients who are sedated and paralyzed 120–130% of baseline
Comatose patients (GCS ≤8) with isolated head injury 140% (range 120–250%)
at least 15% of calories should be supplied as protein
nutritional replacement should start by 72 hours postinjury
Enteral feeding is preferred over parenteral nutrition enhanced immunocompetence and a reduced risk profile
Total parenteral nutrition if enteral feeding is not possible if higher nitrogen intake is required

INFECTION
Source of infection: gross wound contamination immunosuppression, iatrogenically from open surgical procedures, intubation for mechanical ventilation, invasive monitoring equipment
Antibiotic coverage should be targeted toward specific organisms
Perioperative antibiotics only recommended for the first 24 hours

COAGULOPATHY PROPHYLAXIS
Coagulopathies should be rapidly and aggressively treated normal coagulation profile.
Effects of warfarin anticoagulation may be reversed by: vitamin K, fresh frozen plasma (FFP), prothrombin complex concentrate
Effects of heparin may be reversed with protamine sulfate
Thrombocytopenia or platelet deactivation may be treated with donor platelet transfusion

DVT PROPHYLAXIS
Neurological risk factors for DVT and PE: stroke spinal cord injury, prolonged surgery prolonged bed rest
incidence of DVTs in neurosurgical patients 19% to 50%.
Prophylactic measures passive range of motion, early ambulation, rotating beds, electrical stimulation of calf
muscles
Pharmacologic anticoagulation increase the effectiveness of DVT prophylaxis
Low-molecular-weight heparins can be added to pneumatic compression boots (PCBs) without significantly increased risk of hemorrhage

ALGORITHM FOR MANAGEMENT OF MINOR BRAIN INJURY

ALGORITHM FOR MANAGEMENT OF MODERATE BRAIN INJURY

ALGORITHM FOR INITIAL MANAGEMENT OF SEVERE BRAIN INJURY

OUTCOMEGLASGOW OUTCOME SCORE

PROGNOSIS
Worse prognosis when: bilaterally dilated (> 4 mm) absent pupillary light reflexes, absent oculocephalic or
oculovestibular reflexes, increased injury severity scale
(> 40), extreme age (> 60 and possibly
< 2),
hypotension (SBP < 90 mmHg , worse with concomitant hypoxemia),
abnormal CT scan (extensive tSAH, compression or obliteration of basal cisterns),
persistent ICP > 20 mm Hg, elevated ICP during the first 24
hours lower GCS subscores (motor ≤3,
eye opening ≤2, verbal response ≤2)

BRAIN DEATH DETERMINATION AND ORGAN DONATION
Brain death the absence of any observable neurological activity in the brain and the irreversibility of cessation of the cardiopulmonary system or the entire brain.
Requirements No complicating conditions: Hypothermia <32.2°C, Hypotension [SBP<90] Exogenous sedatives, Paralytics drug/alcohol Hepatic encephalopathy, Hyperosmolar coma, Atropine Recent CPR/shock/anoxia

BRAIN DEATH DETERMINATION AND ORGAN DONATION
Patient’s condition: fixed, dilated pupils no observable corneal, oculocephalic, oculovestibular, gag, or cough
reflexes no movement to deep central or peripheral pain no spontaneous breathing is seen on disconnection from the ventilator
with PaCO2 >60 mm Hg (i.e., apnea test).
Head-injured patients who progress to brain death may be candidates for organ donation
Organ donation can provide family members with a slightly more positive conclusion to a series of unfortunate events.

REFERENCES
1. Mattox K, Moore E, Feliciano D. Trauma, Seventh Edition. McGraw Hill Professional; 2012.
2. Jr HRJ Jr, Srinivasan J, Allam GJ, Baker RA. Netter’s Neurology. Elsevier Health Sciences; 2011.
3. American College of Surgeons, Committee on Trauma. ATLS, advanced trauma life support for doctors: student course manual. 8th ed. Chicago, IL: American College of Surgeons; 2008.

THANK YOU