Embed Size (px)
Citation preview

Cervical spine issues
M PerryConsultant craniofacial surgeon
Londonwww.facialsurgery.centre

Cervical spine issues
• Up to 20% “severe” facial injuries
ATLS - “Trauma above the clavicles”

• When should we worry?
• What can / should we do?
Cervical spine issues

• When should we worry?
Cervical spine issues

Mechanism of Injury
• Blunt
• Penetrating

Mechanism of Injury
• Blunt 1. Deceleration 2. High energy
impacts
• RTAs / Falls • Interpersonal violence • Sports
High risk activities
• Diving • Equestrian activities • Football / rugby • Gymnastics • Skiing / Hang gliding
High risk groups
• Elderly • Children
Cervical spine issues

Issue 1
• We will encounter them
• Can be easily overlooked
• “Diffuse responsibility”
• Actively consider
• Anaesthetic refusal

• Walking wounded
• Multiply injured / unconscious
Recognition - 2 groups

• Walking wounded Ask this about the neck- • When injury occurred• Mechanism of injury• Where are they sore • Any loss of consciousness or signs of head injury • Any peripheral neurological symptoms• Progression of symptoms since time of injury• Any other injuries (remember the entire spine)
Look for • Peripheral neurological deficit• Bony tenderness • ROM
Recognition-Group 1
• Walking wounded Low risk factors • Simple rear end collision where the car wasn’t forced into the car in front • Ambulatory at any point after the injury • Sitting in the emergency department • Absence of midline spinal tenderness • Delayed onset of neck pain
NEXUS / Canadian C Spine rule Low risk patients - can they rotate their head >45 degree’s bilaterally ? If low risk symptoms and low risk factors then their collar can be removed and the neck carefully assessed. If cannot reach 45 degree / severe pain >7/10 or neurological symptoms, imaging is required.
Recognition-Group 1

• Assess the neurological state of the limbs. (Tone, Power, Sensation, Reflexes, Proprioception and Coordination)
• Examine relevant imaging • Are there any other distracting injuries? • Has analgesia (opiates) been given? • Is there any spinal pain? • Is the patient mentally alert? (Head injury / Alcohol / Drugs etc)
If all ok, take the front of the collar off. Assistant to support the head. • Assess for spinal tenderness. • Feel for any swelling, steps or crepitus. • Assess active movement - Lateral flexion first, then rotation, then lift head. • If complains of any neurological symptoms or pain, the neck is not cleared. • Cleared if can move the neck freely without pain or neurological symptoms
How to “clear” the neck

• GCS 15, alert and orientated • No drugs / alcohol • No “distracting” injuries • No neurological deficit • No midline tenderness and • Normal examination
= C Spine cleared
How to “clear” the neck

Do I really need to know all this?
You may have to do this
Ward
Clinic

Issue 2
Deceptive injuries
Beware hyperextension injuries in the elderly
Often mobile, so not suspected
? NS in hands

ATLS
Know how to protect
Know how to immobilise
Recognition-Group 2

ATLS
Know how to protect
Know how to immobilise
Interventions difficult (unfasten collar)
Recognition-Group 2

Issue 3Know your role in trauma team
Know your limitations
Protect neck during any interventions

KEEP SUPINE SIT UP
Issue 4“Can I sit up ?”

“Can I sit up ?”

Thoracolumbar trauma (10%)
Delayed diagnosis in 25%

Prolonged immobilisation
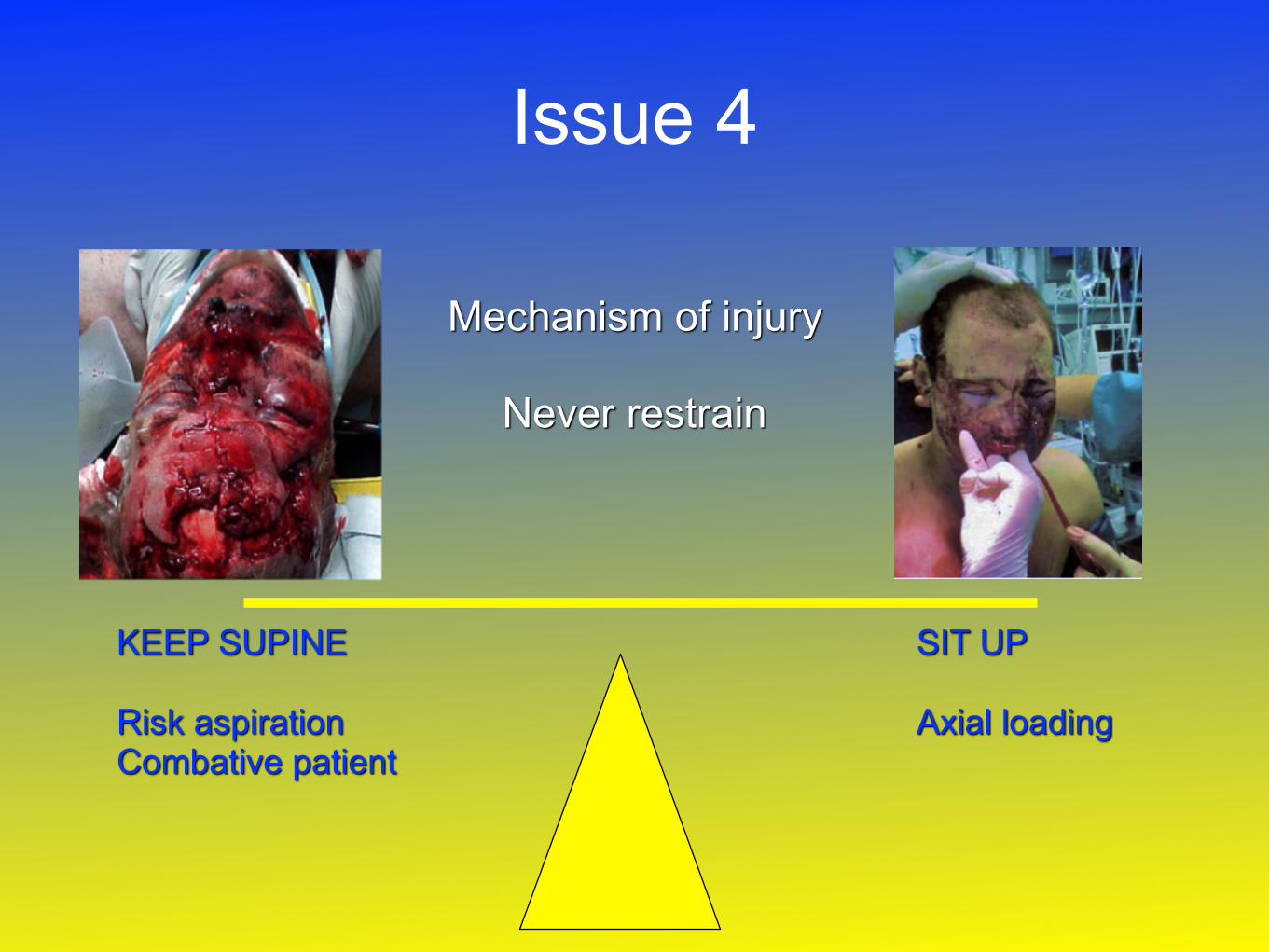
KEEP SUPINE
Risk aspiration Combative patient
SIT UP
Axial loading
Issue 4
Mechanism of injury
Never restrain

Make no assumptions
When will neck be cleared ?
What to do if not
The unconscious ICU patient

Mayfield clampMake no assumptions
When will neck be cleared
What to do if not

Summary
• Identifying those at risk (esp. occult) • Screening in the clinic or on the ward • How to ‘clear' a neck • How to protect a neck • Limitations in intervention • ICU patients • When to sit up