Embed Size (px)
Citation preview
PROPTOSIS :
INVESTIGATION & MANAGEMENT
Dr Ramchandra D Hendge
Proptosis
Definition :
Abnormal protrusion of globe
Displacement of globe relative to orbital rims
Exophthalmos : abnormal protrusion of eye balls in
endocrine disorders specially in thyroid dysfunction
Classification
1) Based on direction
2) Based on severity
3) Based on presentation
4) Based on etiology
5) Based on movement
Etiology
Axial Proptosis- Eccentric/Abaxial Proptosis
Optic nerve tumours Thyroid orbitopathy
Intra conal haemangioma Dermoid cyst
Infections & Inflammations
Neurofibroma
Lacrimal gland tumour
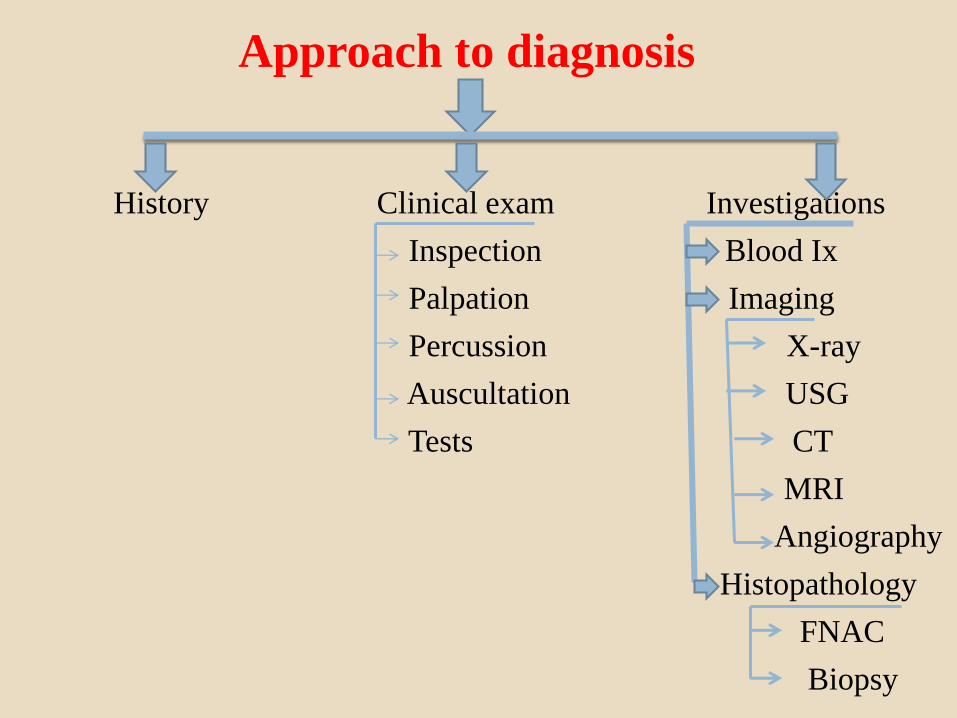
Approach to diagnosis
History Clinical exam Investigations
Inspection Blood Ix
Palpation Imaging
Percussion X-ray
Auscultation USG
Tests CT
MRI
Angiography
Histopathology
FNAC
Biopsy
History
Onset , duration, progress
DOV, colour vision defect
Diplopia
Discoloration of lids
Association with straining
Postural variation
Oral hygiene
Clinical Examination
Inspection
Palpation
Percussion
Auscultation
Clinical Tests
Auscultation
Globe/temporal region for bruit
Differential Tonometry
Useful in fibrosis of muscles & lesions compressing globe
Rise in IOP >6mmHg suggestive of pathology
Rise in IOP due to mechanical compression of globe
Gaze- Upward for muscles & in direction of mass in
space occupying lesions
Ruler Test
Exophthalmometry/ Proptometry
1) Clinical
2) Stereo Photographic
3) Radiographic
Clinical Exophthalmometry
1. Hertel
2. Luedde
3. Naugle
4. Gormaz
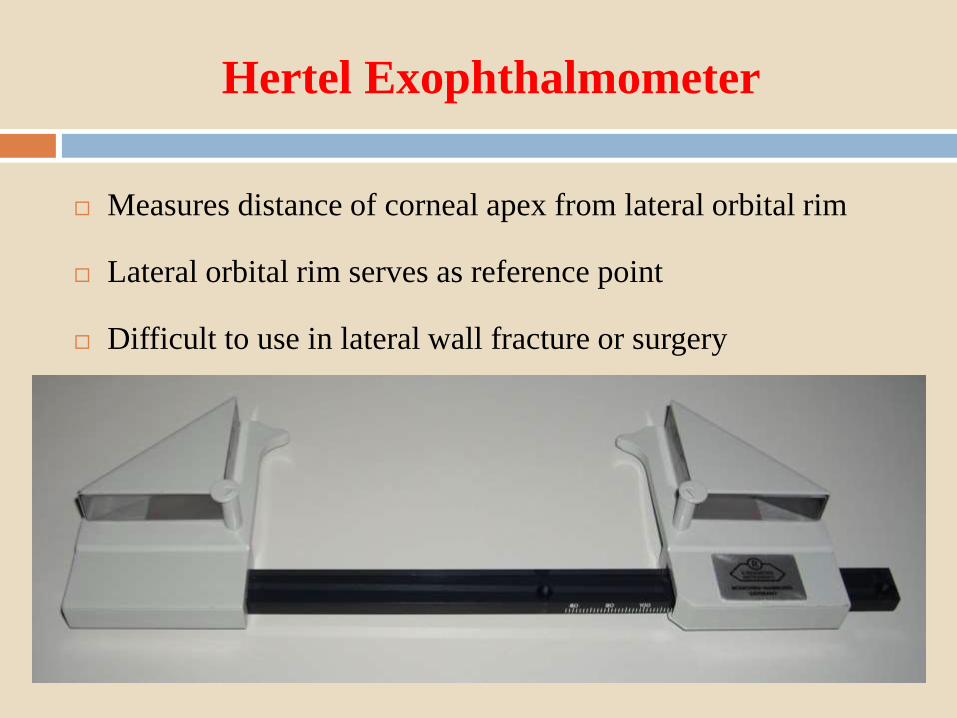
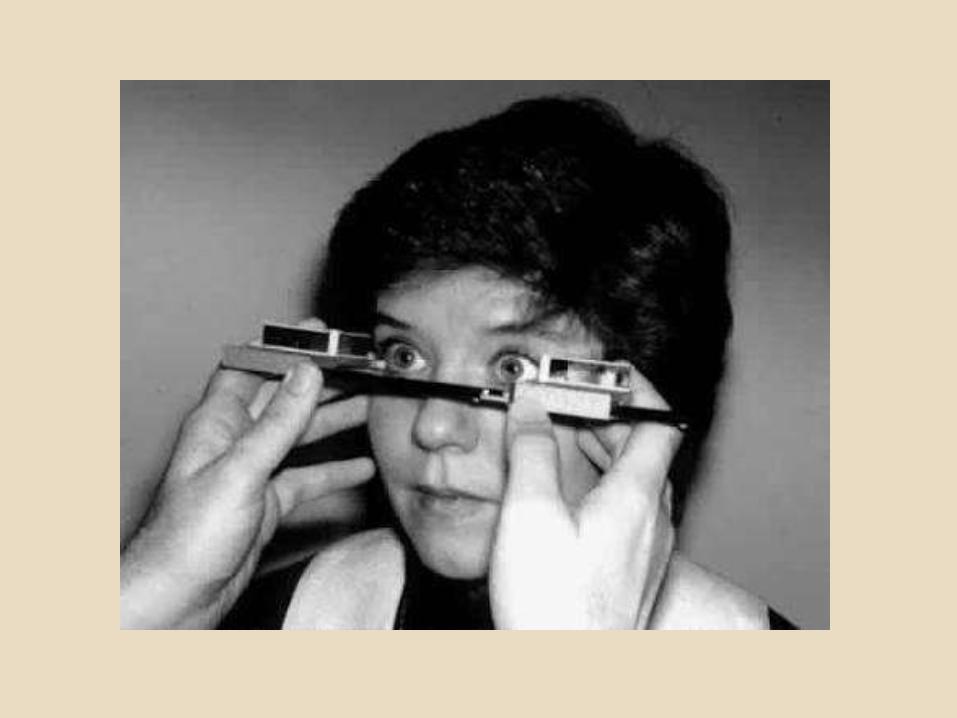
Hertel Exophthalmometer
Measures distance of corneal apex from lateral orbital rim
Lateral orbital rim serves as reference point
Difficult to use in lateral wall fracture or surgery
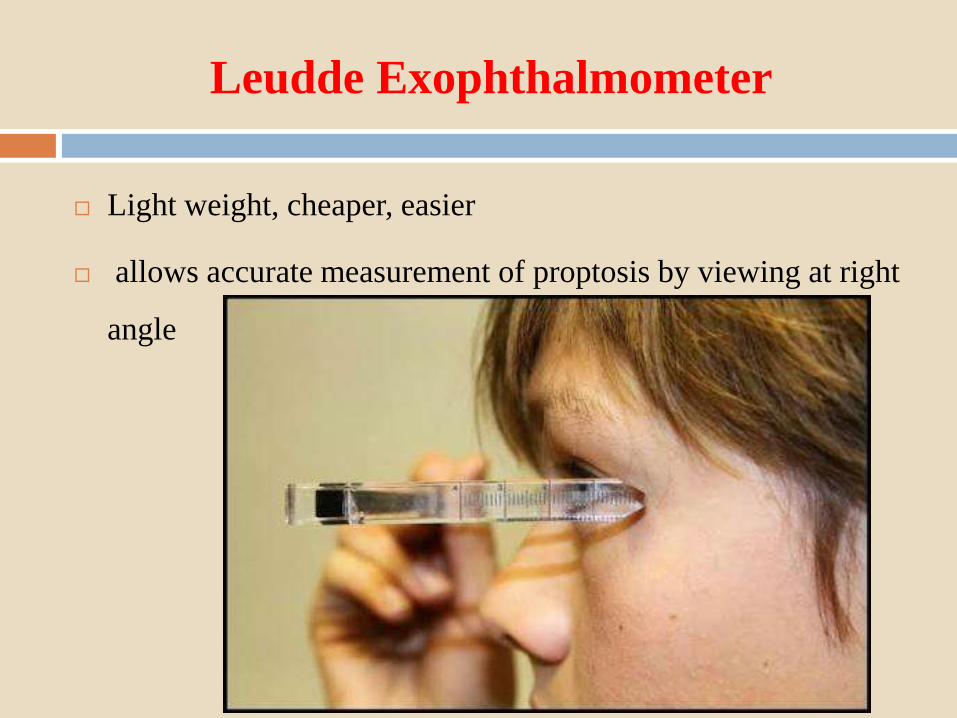
Leudde Exophthalmometer
Light weight, cheaper, easier
allows accurate measurement of proptosis by viewing at right
angle
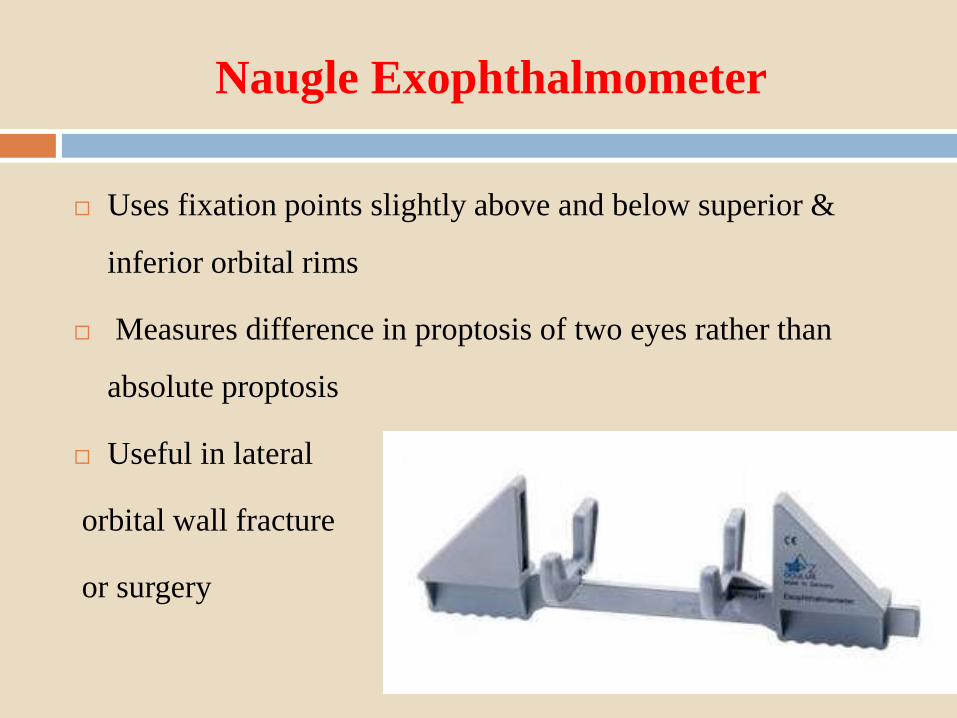
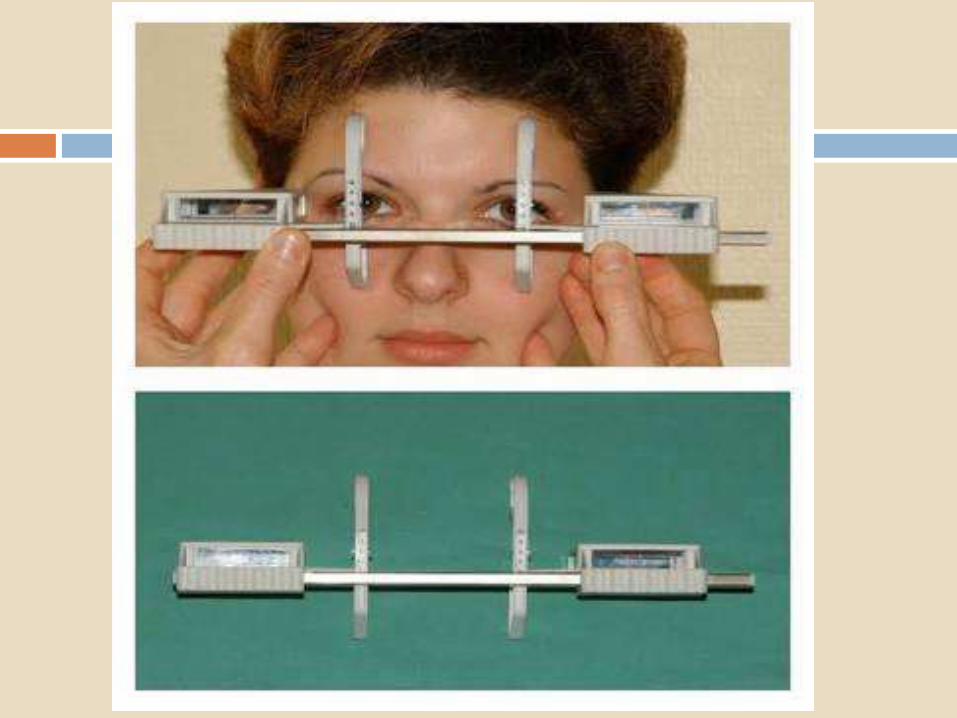
Naugle Exophthalmometer
Uses fixation points slightly above and below superior &
inferior orbital rims
Measures difference in proptosis of two eyes rather than
absolute proptosis
Useful in lateral
orbital wall fracture
or surgery
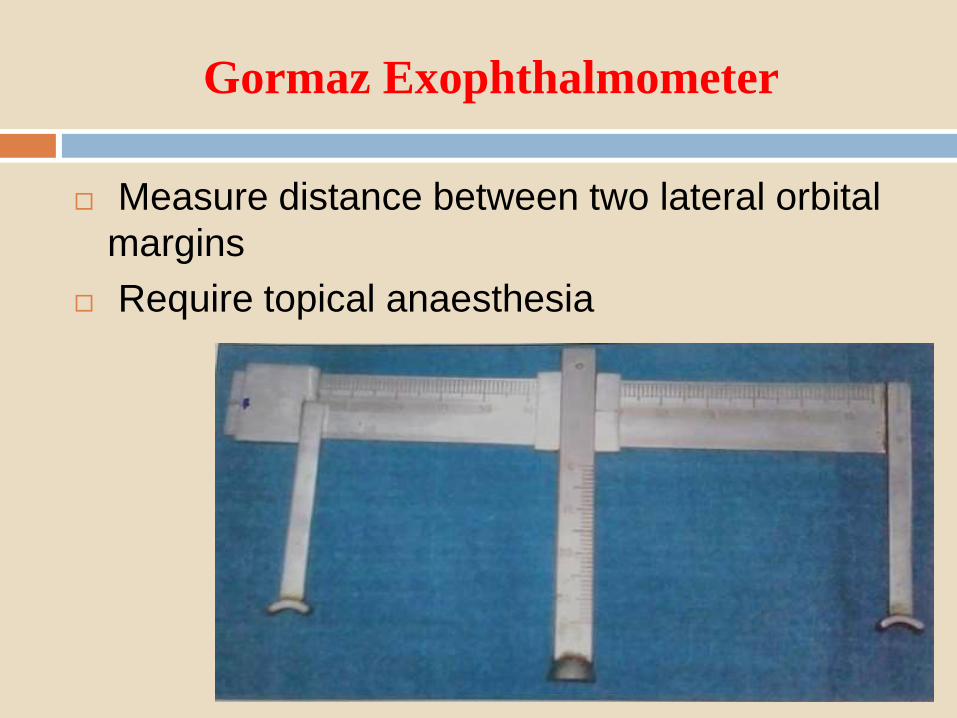
Gormaz Exophthalmometer
Measure distance between two lateral orbital
margins
Require topical anaesthesia
Blood Investigations
Complete haemogram
ESR
FBS/PPBS
Thyroid function tests
Serum c-ANCA levels
Serum ANA levels
Other Investigations
Sputum for AFB
Montoux test
X -ray
Should be the first screening imaging investigation
Useful specially for bony pathology
Useful in detecting :
Benign tumours
Calcification( Meningioma, retinoblastoma,
lacrimal gland carcinoma)
Hyperostosis( Meningioma, fibrous dysplasia,
osteoblastic secondaries)
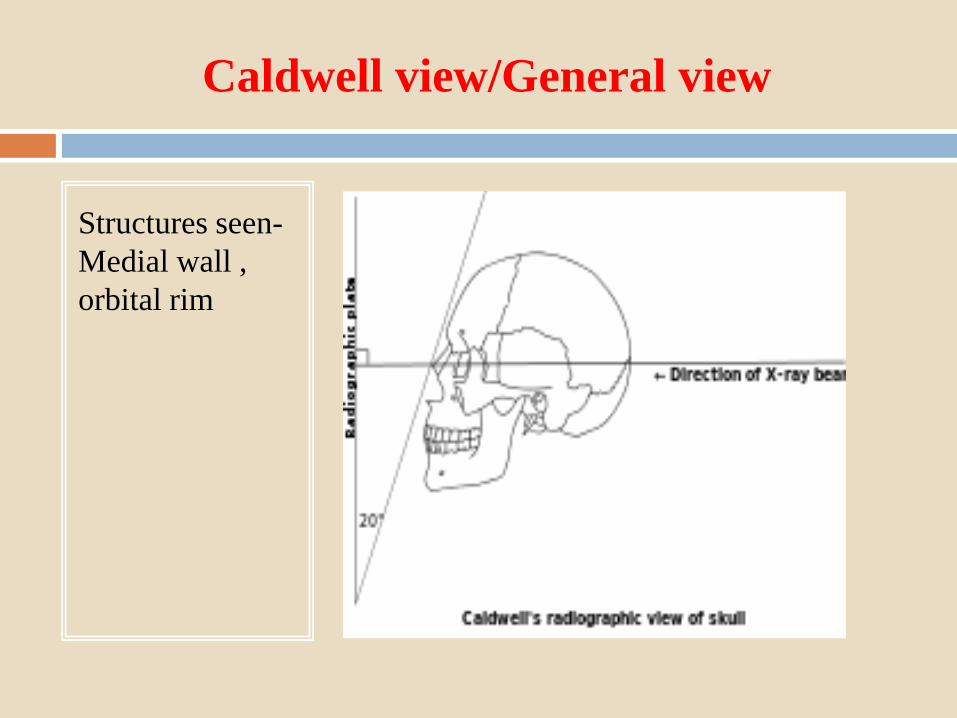
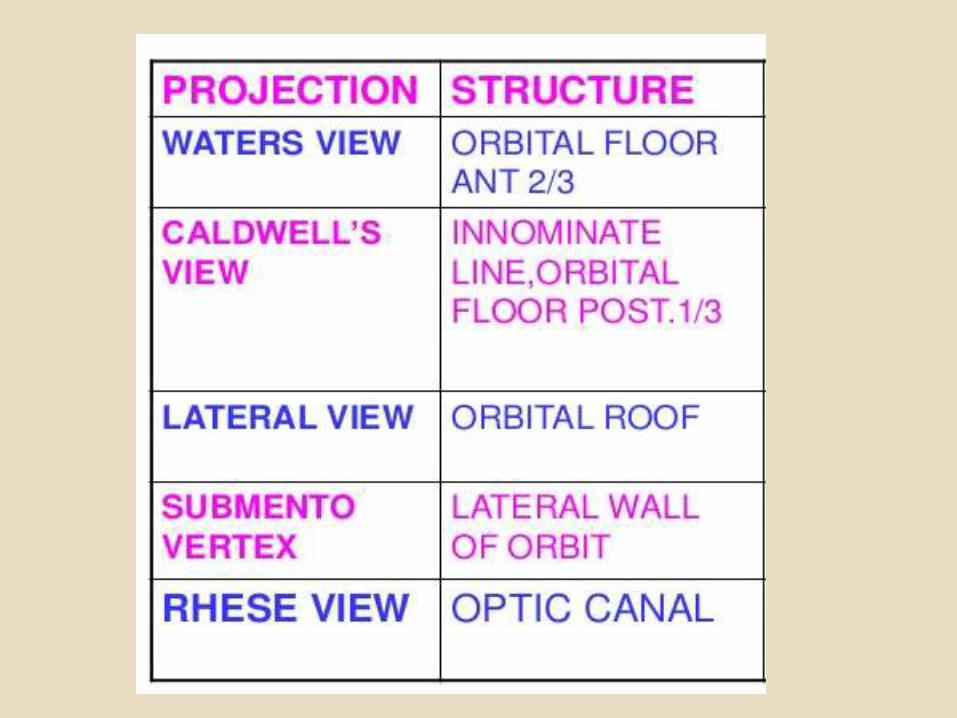
Caldwell view/General view
Structures seen-
Medial wall ,
orbital rim
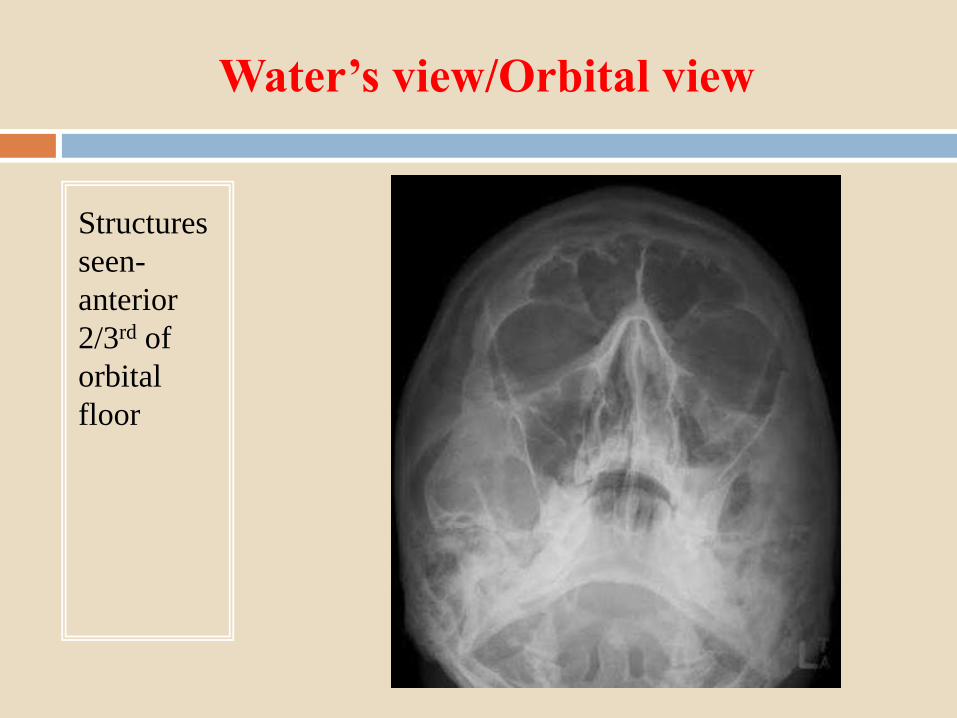
Water’s view/Orbital view
Structures
seen-
anterior
2/3rd of
orbital
floor

Lateral
Structures
seen-
Orbital
roof
Ultra sonography
Rapid, non invasive , simple, no radiations
Compact & Portable
Can be done in OPD & before surgery by ophthalmologist
No need to depend upon radiologists
Gives information about characteristics of lesions
Size of lesion can be measured
Principle- Piezo electric effect
Probes- Sound waves-6-20 MHz
Lower frequencies-> lower resolution->better penetration
Higher frequencies-> higher resolution->lesser penetration
Gives echogenicity based on reflectivity of structure
TYPES
A scan/Amplitude scan
B scan/ Brightness scan Trans ocular
C scan/ Coronal scan Para ocular
D scan / 3D scan
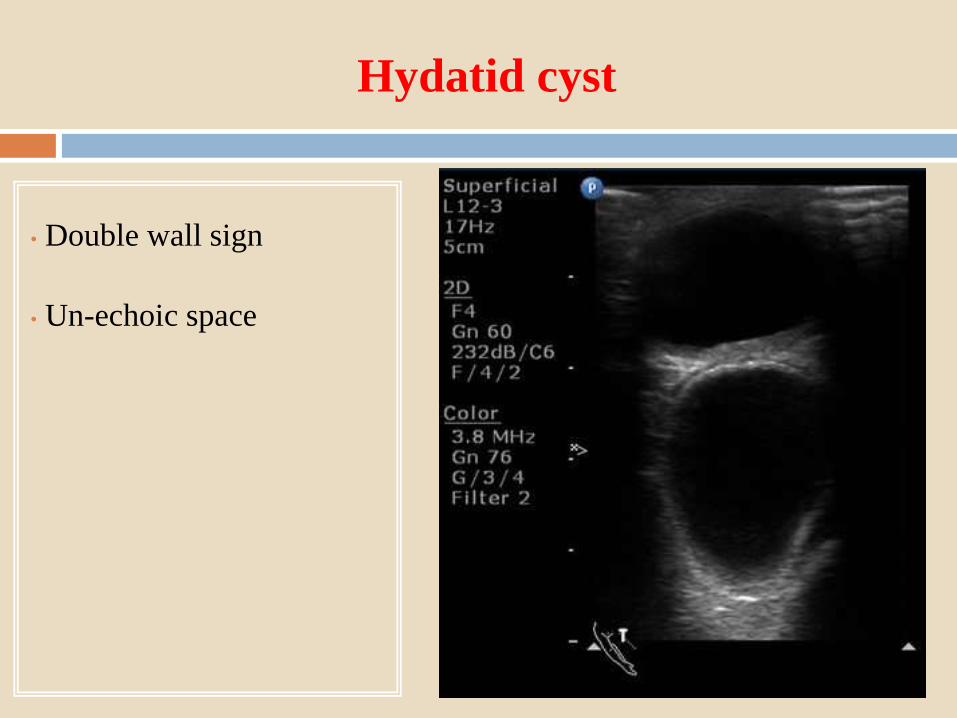
Hydatid cyst
• Double wall sign
• Un-echoic space
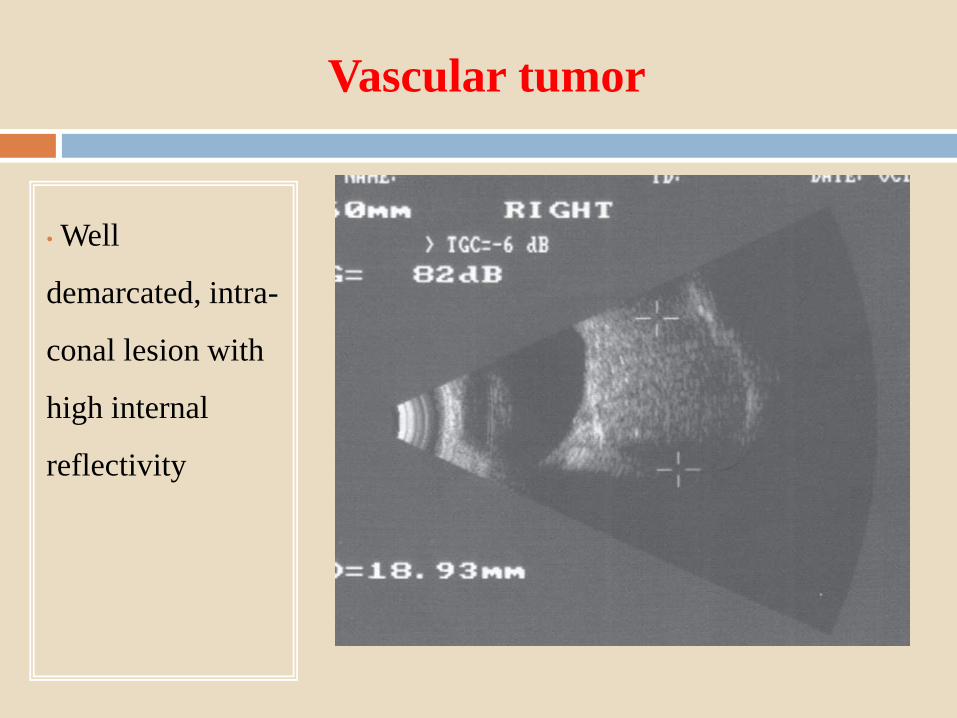
Vascular tumor
• Well
demarcated, intra-
conal lesion with
high internal
reflectivity
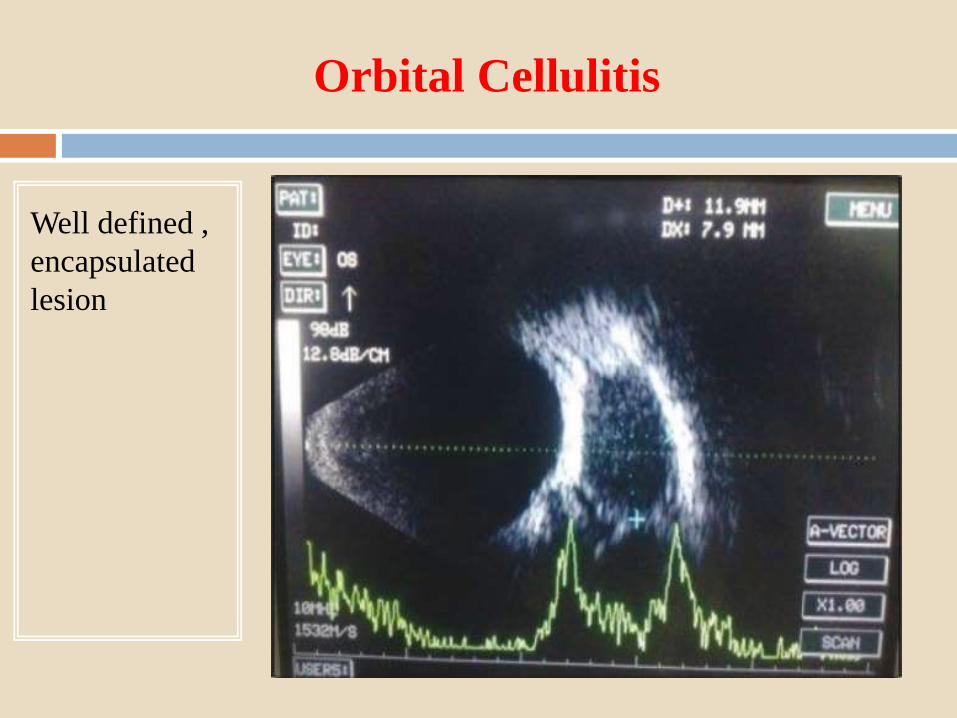
Orbital Cellulitis
Well defined ,
encapsulated
lesion
CT Scan
Is superior to X ray & USG
Gives shape , size , location & nature of lesion
Resolution ~0.5 mm
8 slices required to scan orbit
Causes radiation exposure but its comparable with orbital X
ray
HRCT with 1mm sections gives information about optic nerve
tumours
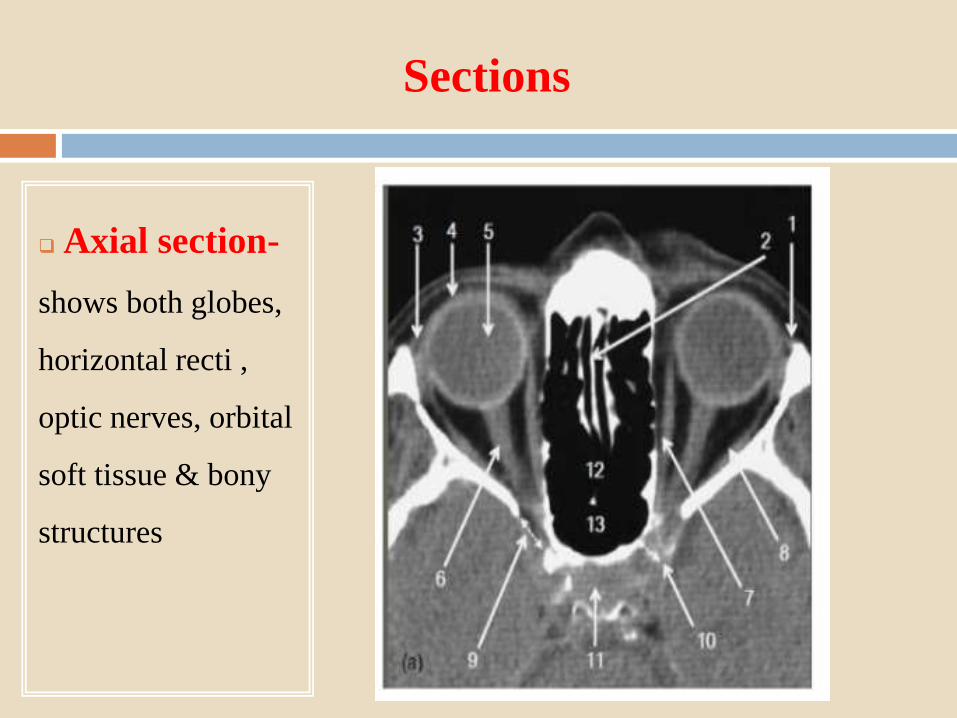
Sections
Axial section-
shows both globes,
horizontal recti ,
optic nerves, orbital
soft tissue & bony
structures
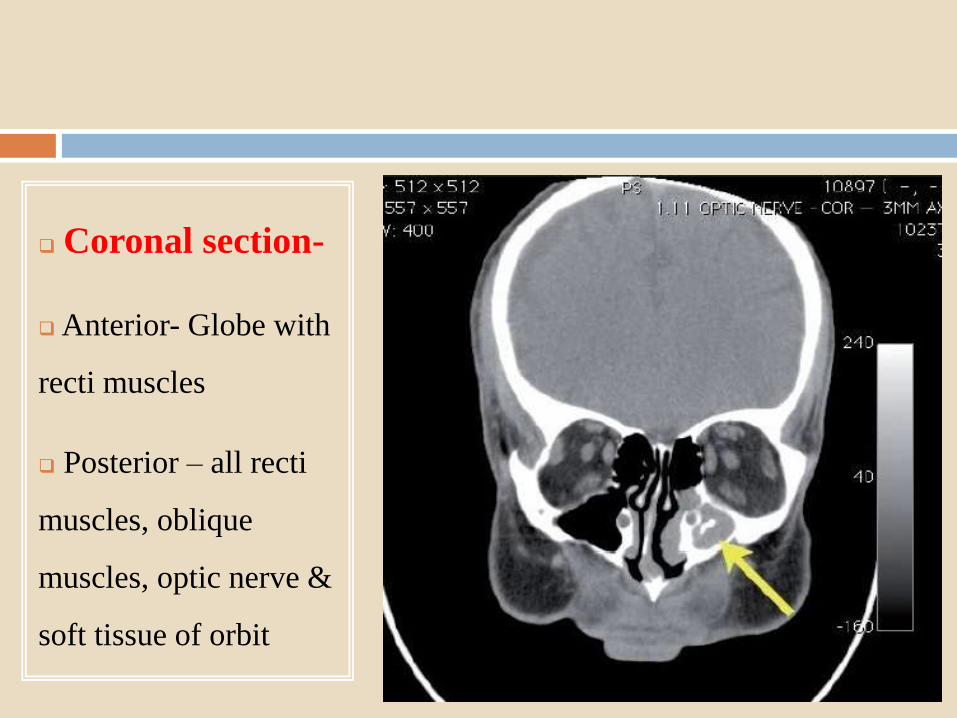
Coronal section-
Anterior- Globe with
recti muscles
Posterior – all recti
muscles, oblique
muscles, optic nerve &
soft tissue of orbit
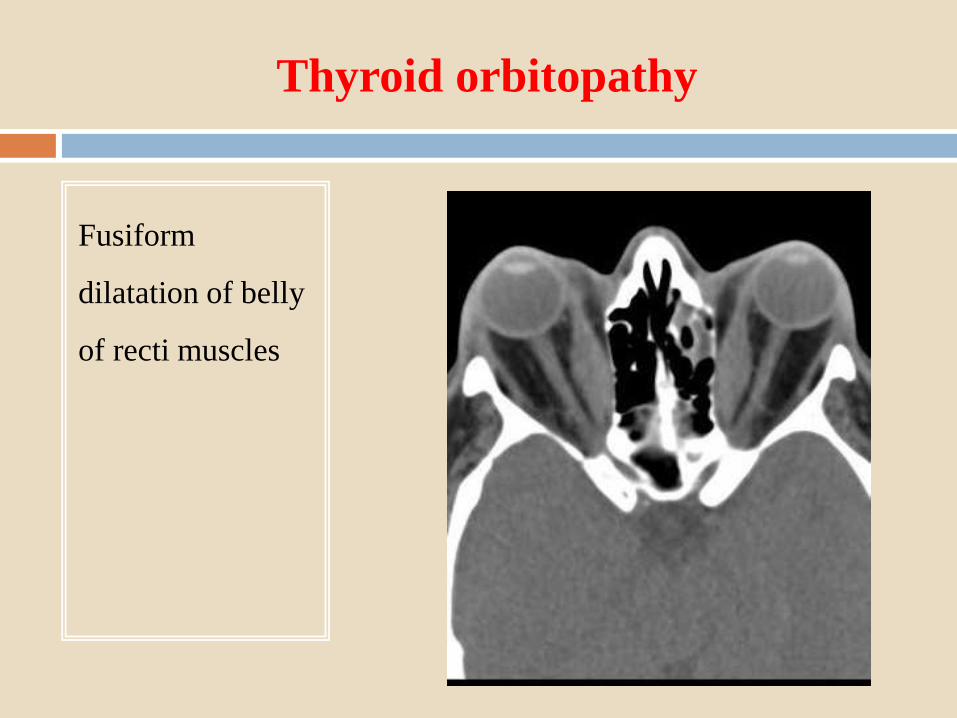
Thyroid orbitopathy
Fusiform
dilatation of belly
of recti muscles
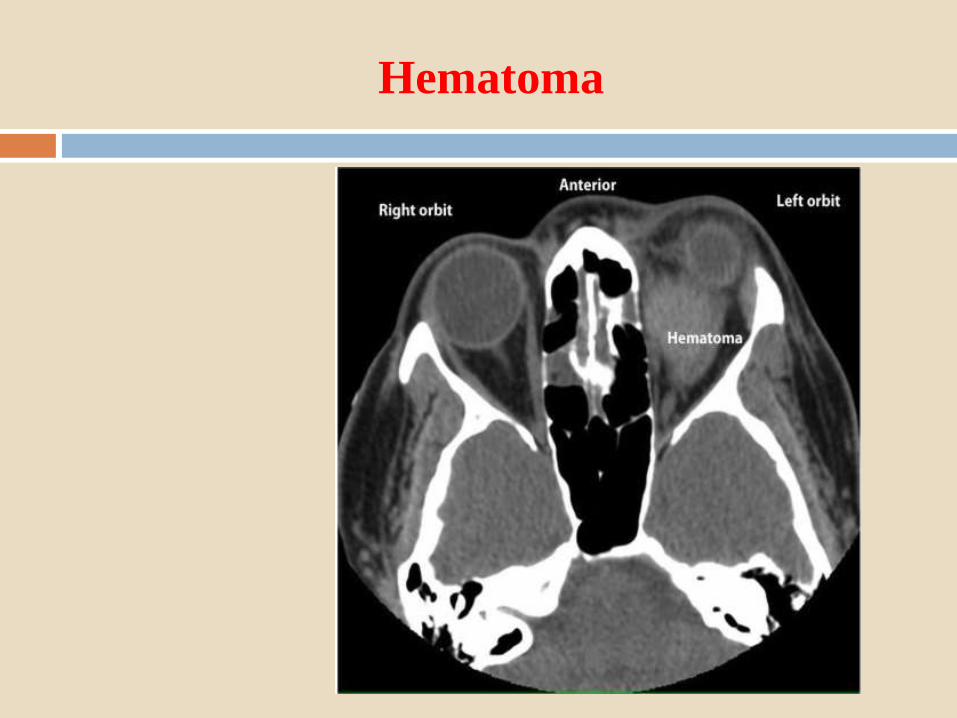
Hematoma
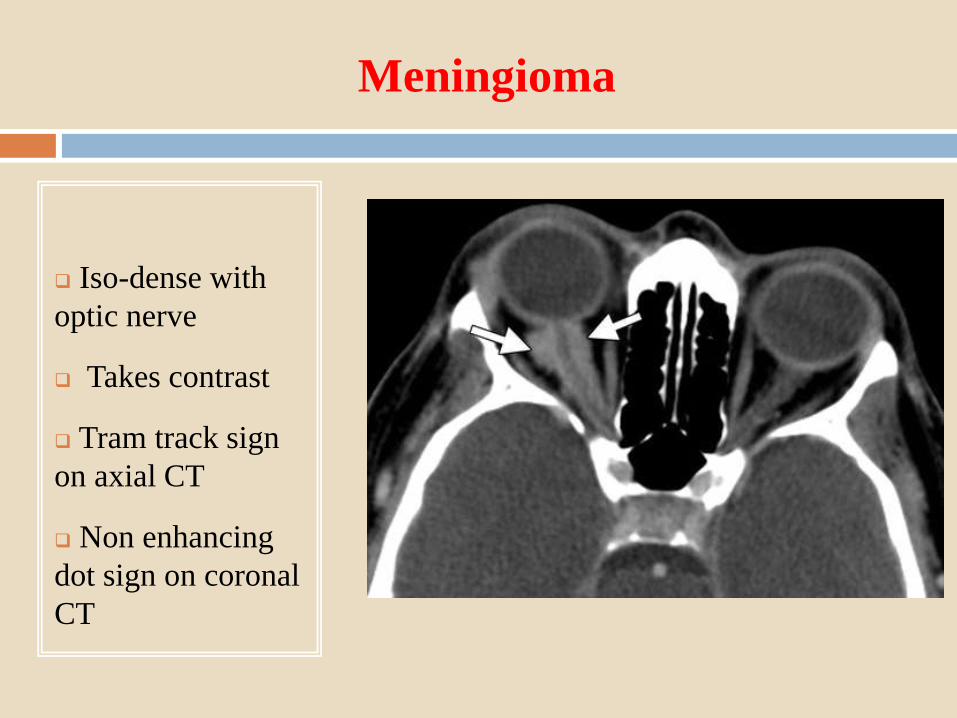
Meningioma
Iso-dense with
optic nerve
Takes contrast
Tram track sign
on axial CT
Non enhancing
dot sign on coronal
CT
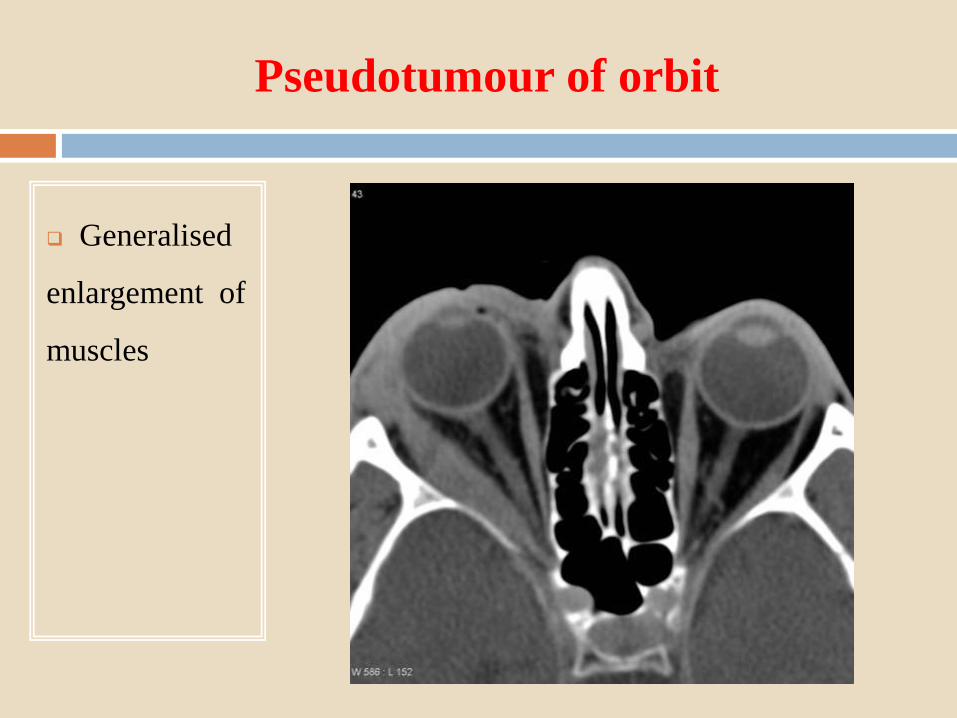
Pseudotumour of orbit
Generalised
enlargement of
muscles
MRI
Most sensitive modality for soft tissue lesions
No radiation exposure
Specially useful in optic nerve lesions, pseudo tumour, orbital
metastasis & tumours having intra cranial expansion
Metallic implants/ metallic foreign bodies are the only
absolute contraindications
T1/T2 weighting- refers to methods of measuring the
relaxation times of excited protons after magnetic field is
switch off.
T1- Fat-Bright
Vitreous- Dark
T2- Fat-Dark
Vitreous- Bright
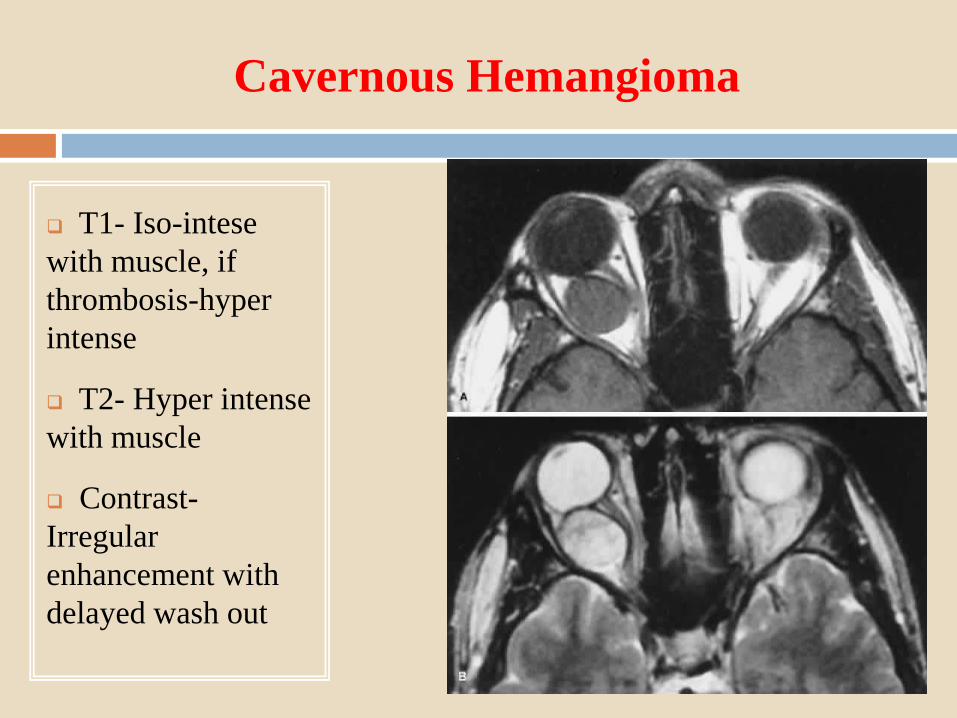
Cavernous Hemangioma
T1- Iso-intese
with muscle, if
thrombosis-hyper
intense
T2- Hyper intense
with muscle
Contrast-
Irregular
enhancement with
delayed wash out
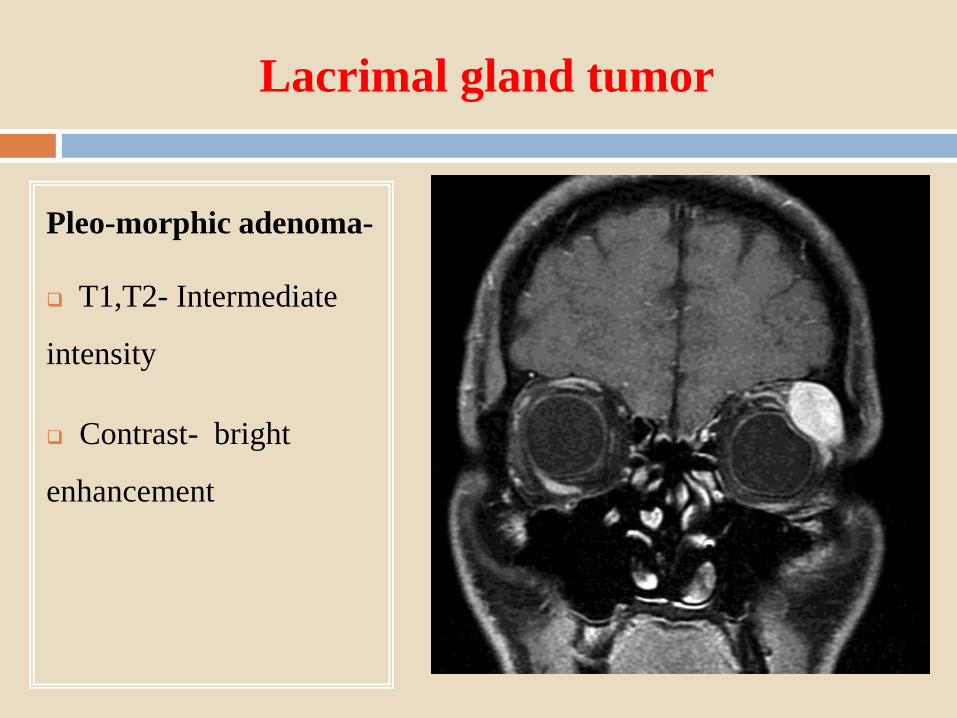
Lacrimal gland tumor
Pleo-morphic adenoma-
T1,T2- Intermediate
intensity
Contrast- bright
enhancement
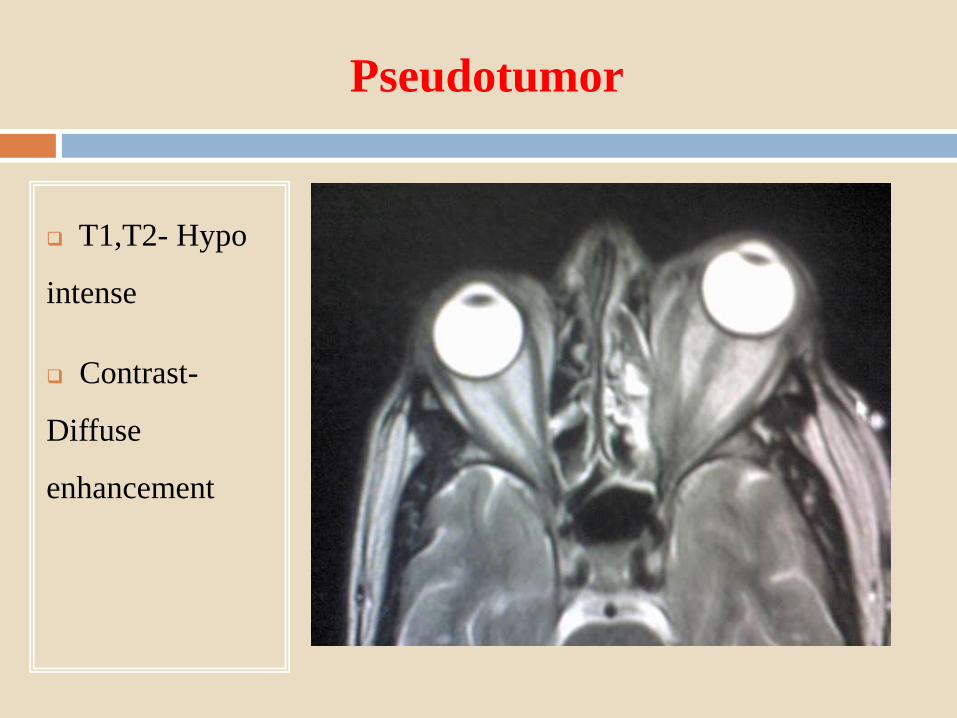
Pseudotumor
T1,T2- Hypo
intense
Contrast-
Diffuse
enhancement
Angiography
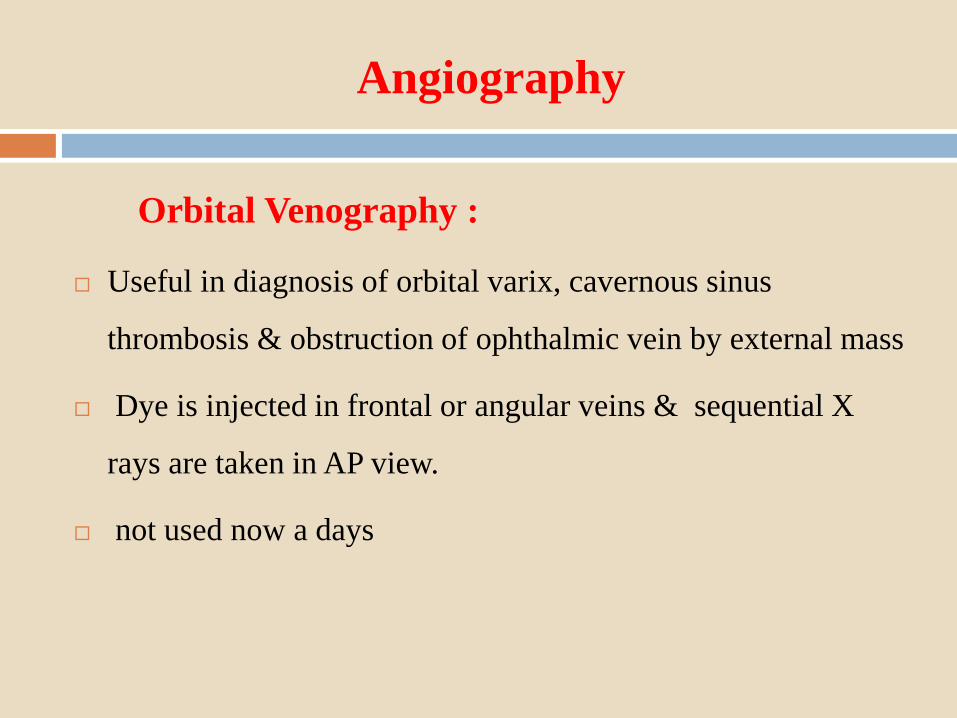
Orbital Venography :
Useful in diagnosis of orbital varix, cavernous sinus
thrombosis & obstruction of ophthalmic vein by external mass
Dye is injected in frontal or angular veins & sequential X
rays are taken in AP view.
not used now a days
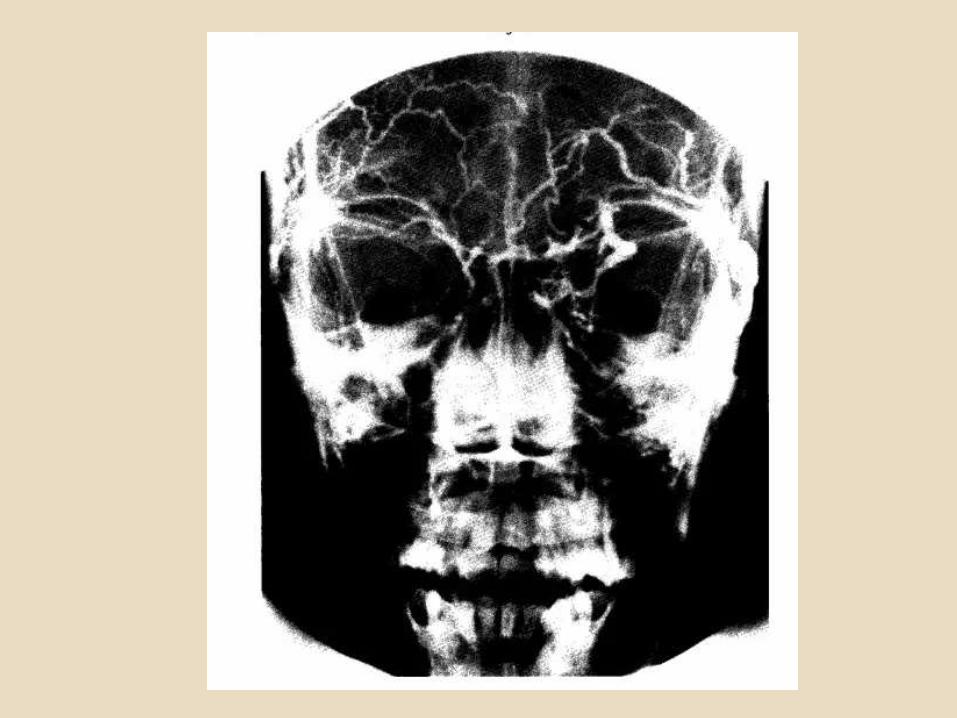
Orbital Arteriography :
Useful in diagnosis of A-V malformations , carotid-cavernous
fistula , aneurysms etc
Contrast dye is injected in ipsi-lateral common or internal
carotid artery and sequential X rays are taken.
Contrast medium may cause allergic reactions
Not used now a days due to CT,MRI & MR Angiography.
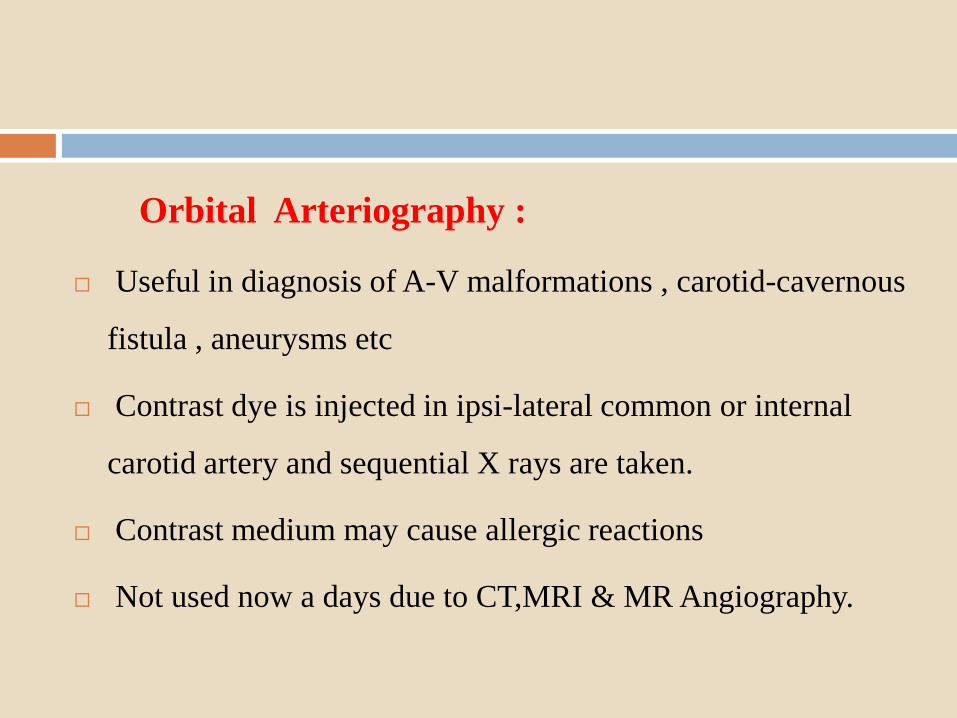
Ophthalmic artery Anurysm
Hyper lucent
mass in orbit
Histopathology
Definitive diagnosis is by histopathology
Biopsy Techniques :
FNAC
Core biopsy
Incisional biopsy
Excisional biopsy
FNAC
Minimal invasive
Rapid diagnosis
USG/CT guided FNAC
Accuracy >80%
Indications :
Lymphoma,melanoma,meningioma
Scanty material, difficult to evaluate
Risk of globe perforation,h’age
Core biopsy –better than FNAC
Inscisional biopsy- sample obtained under direct visualisation
Excisional biopsy- Best method for tissue sampling
Both diagnostic &therapeutic
Pathology Techniques
1. Cytology
2. Gross examination
3. Routine histopathology
4. Histochemistry-Sudan black(Fat)
5. Immuno-histochemistry –HMB45 for melanomas, S100 for
schwannomas & neurofibromas
6. Electron microscopy
Management of proptosis
Local measures
Medical therapy
Radiation
Surgical options
Local measures
Sun glasses
Sleep in supine position with head elevated
Taping of lids at night
Prisms in diplopia
Medical therapy
Topical tear substitutes
Systemic diuretics - minimal role
Parenteral antibiotics
Pain killers
Corticosteroids
Corticosteroids
Indications
Compressive optic neuropathy
Prior to orbital decompression
Pseudo tumor
Traumatic optic neuropathy
Hydatid cyst
Corticosteroids - regimen
60-100mg(1mg/kg) orally prednisolone in divided
doses
Pulse intravenous therapy of methyl prednisolone
1gm on alternate days for 3-5days
Local steroid injections have no role
Complications
Weight gain
Gastrointestinal irritation
Reactivation infections (tuberculosis)
Cataract
Glaucoma
Osteoporosis
Adrenal gland suppression
Immunosuppressive
Indications-
Refractory cases of thyroid orbitopathy, pseudotumour,
sarcoidosis , hematological malignancies etc
Commonly used drugs- Cyclosporin, methotrexate,
azathioprine, cyclophosphamide etc
Anti tumor necrosis factor drugs – infiximab
Radiation Therapy
Indications-
Pseudotumour
Lymphoma
Rhabdomyosarcoma
Meningioma
Thyroid orbitopathy
Surgical management
Orbital decompression
Strabismus surgery
Eye lid surgery
Orbital decompression
Done in stable cases
Severe exophthalmos
Exposure keratopathy
Optic nerve compression
Cosmetic purpose
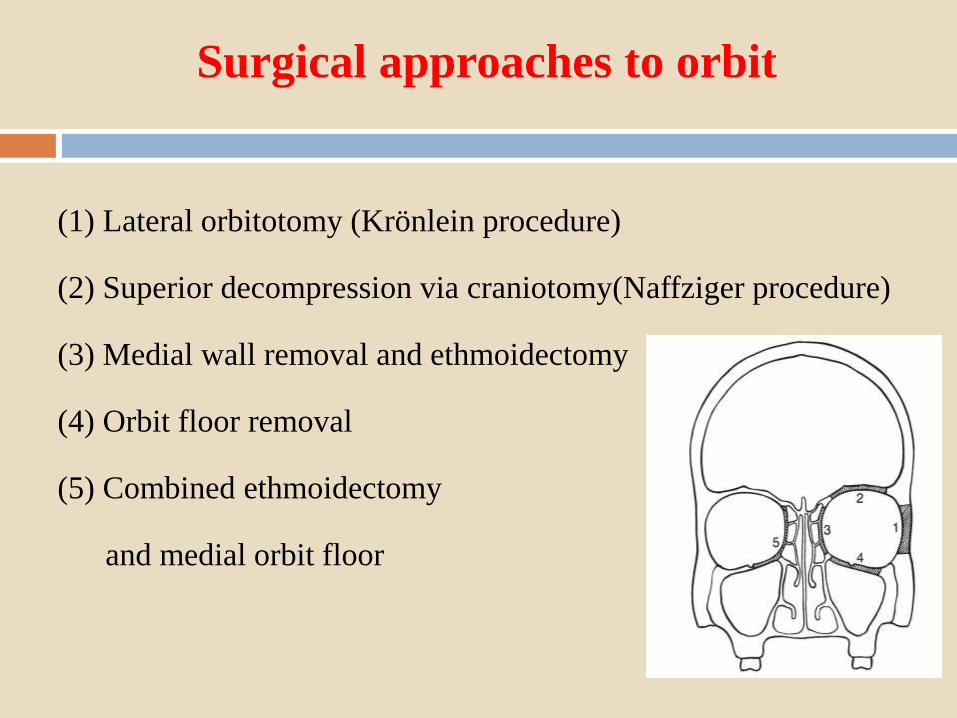
Surgical approaches to orbit
(1) Lateral orbitotomy (Krönlein procedure)
(2) Superior decompression via craniotomy(Naffziger procedure)
(3) Medial wall removal and ethmoidectomy
(4) Orbit floor removal
(5) Combined ethmoidectomy
and medial orbit floor
Complications: Orbital Decompression
Diplopia
Hyper aesthesia in distribution of infra orbital nerve
Nasolacrimal duct obstruction
Cerebrospinal fluid leak
Frontal lobe hematoma
Strabismus surgery
Indications :
Done in stable inactive thyroid orbitopathy
Angle of deviation stable for at least 6–12 months
Goal :
To minimize diplopia in primary position
Eye lid surgeries
Mild eyelid retraction- no surgeries
Main indication is exposure keratopathy
Conclusion
Proptosis is an important manifestation of a large number of
orbital diseases. Thorough clinical examination coupled with
appropriate investigations clinches the diagnosis and helps in
management.

THANK YOU