Embed Size (px)
Citation preview
Cardiogenic Shock: Which Mechanical Support Should We
Use as First Line Option?
Mariell Jessup MD FAHA, FACC, FESCProfessor of Medicine
University of PennsylvaniaPhiladelphia, Pennsylvania, USA

Disclosure: Mariell Jessup MD
• Speakers Bureau:• Advisory Board:• Honorarium:
University of Pennsylvania
NONE
Temporary support:Background
• Cardiogenic shock– Compromise of cardiac output leading to end-
organ hypo-perfusion– Complex cascade of end-organ dysfunction
combined with activation of inflammatory pathways
– Complicates about 7% of ST segment elevation MI1 and about 2.5% of non-ST segment elevation MI2
1Holmes DR Jr, Berger PB, et. al. Circulation 1999; 100:2067–2073.2Hasdai D, Harrington RA, et. al JACC 2000;36:685–692.

Who would benefit from temporary support?üAcute cardiogenic shock
Acute myocardial infarctionAcute myocarditisComplications post MI
Papillary muscle ruptureVentricular septal defect
üPost cardiotomy failureüAcute on chronic (end-stage) heart failureüElectrical “storm”, or post-VT ablation üDrug overdose with myocardial depressionüHypothermia
Windecker S. Curr Opin Crit Care 13:521–527. 2007
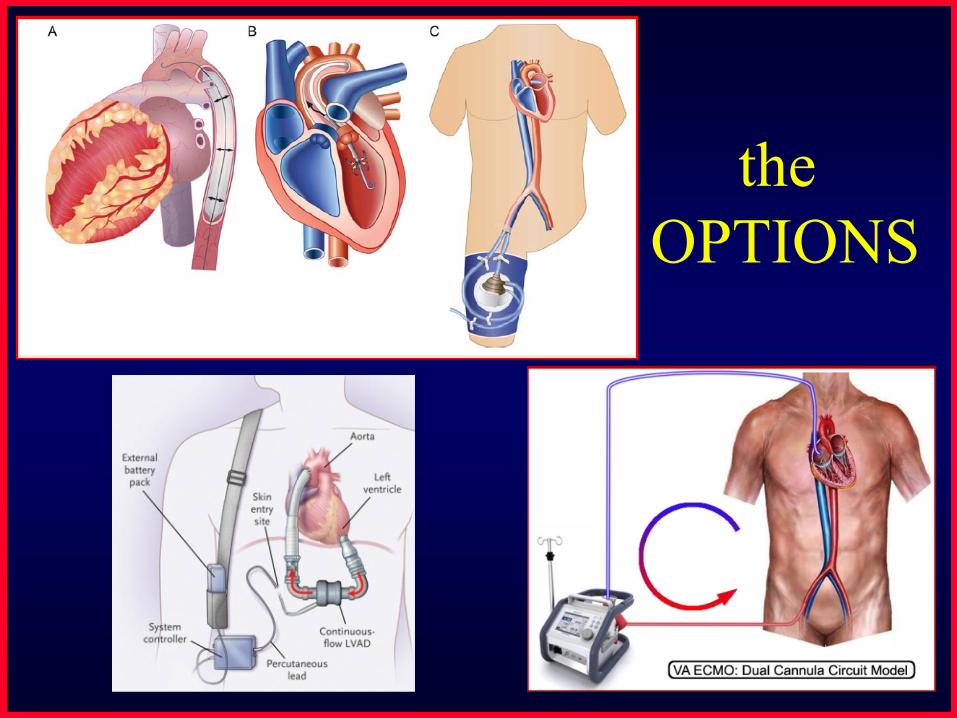
the OPTIONS

Sick patient
Temporary supportChronic support
Unclear situation
1. Support circulation2. Oxygenate patient
Choice dictated by clinical status:temporary supportECMO
Durable VADs pulsatile non-pulsatile

Illustrative cartoons are helpful….
but these patients are desperately ill.
Important Principles
• Definition of success– Survival without device– Transplant– Survival on dialysis– Transplant on dialysis– Durable device on dialysis
• Availability of devices• The appropriate setting of care
– Should the patient be transferred?
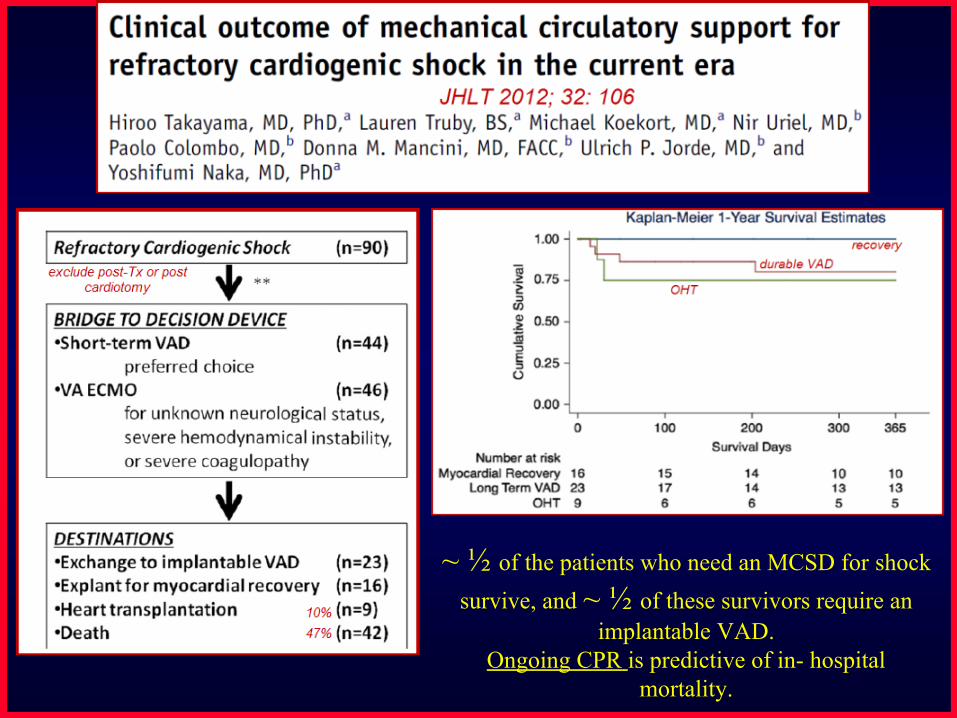
~ ½ of the patients who need an MCSD for shock survive, and ~ ½ of these survivors require an
implantable VAD. Ongoing CPR is predictive of in- hospital
mortality.

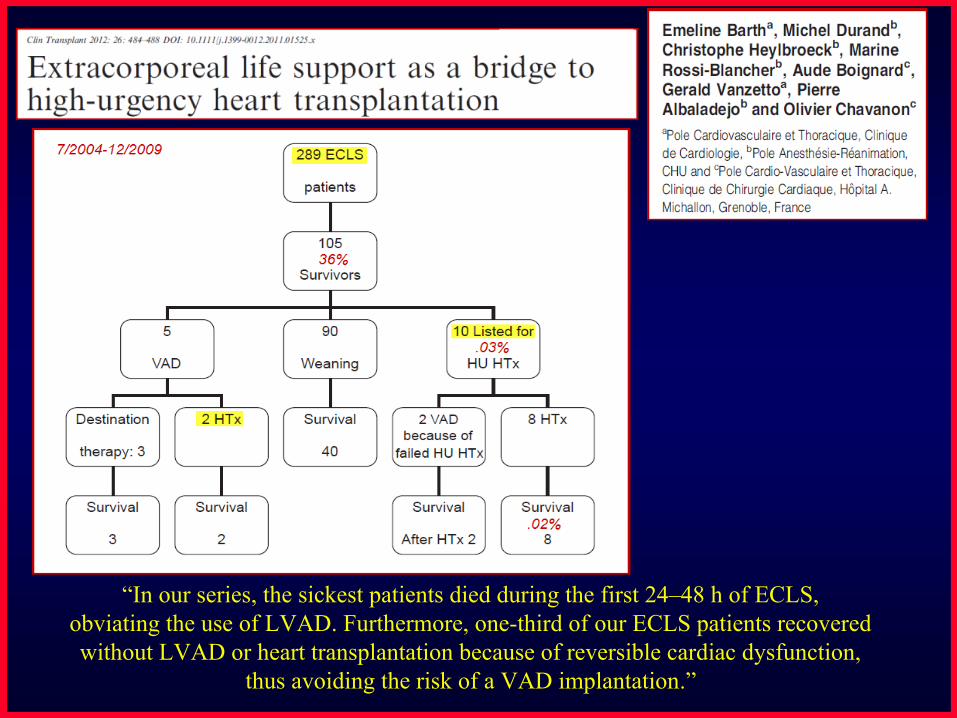
“In our series, the sickest patients died during the first 24–48 h of ECLS,obviating the use of LVAD. Furthermore, one-third of our ECLS patients recovered without LVAD or heart transplantation because of reversible cardiac dysfunction,
thus avoiding the risk of a VAD implantation.”
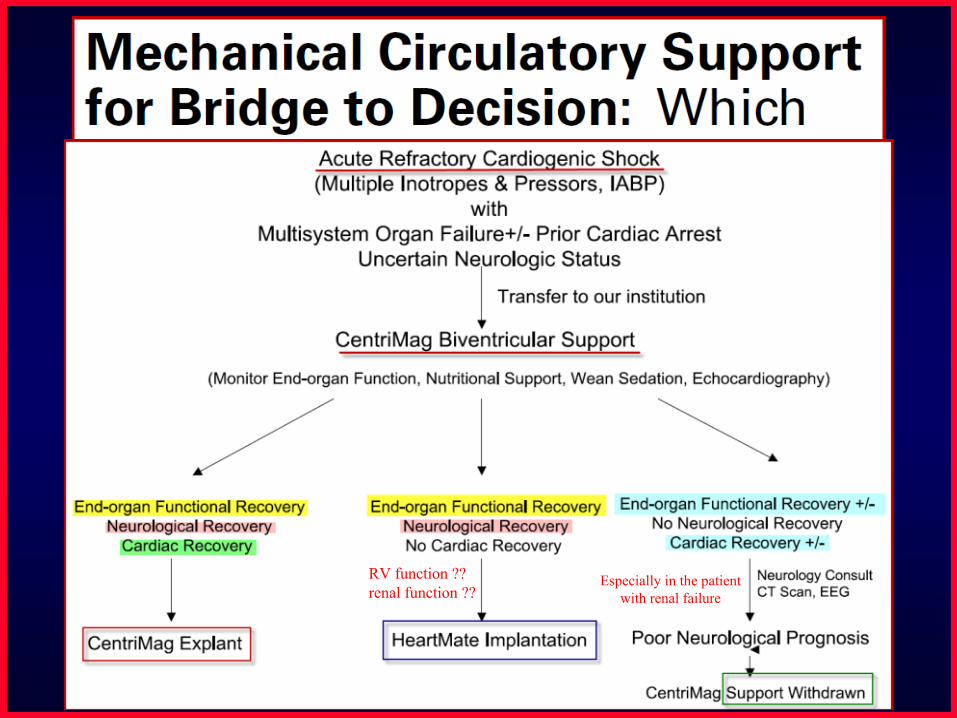
RV function ?? renal function ??
Especially in the patient with renal failure

UNOS registry2000-2010
13,250 patients with first transplant

The overall survival in our cohort was 31%. While patients without the need for RRT showed a 98-day survival of 53%, patients
with RRT had an overall survival of 17%.

Decisions to make during the “bridge to decision”
• Age of the patient• Frailty of the patient• Social support of the patient• End of life wishes• Transplant candidate?
– Infection, pulmonary infarct, cancer• Co-morbidities
– Weight, vascular disease, neurologic status

The pump choices for the acutely ill patient.
• Intra-aortic balloon pump• Extracorporeal membrane oxygenation
(peripheral cardio-pulmonary bypass)• Tandem Heart• Impella
• Traditional ventricular assist devices• Total Artificial Heart
Percutaneous
SurgicalCentriMag

Advantages of Percutaneous Device
• Placed quickly• Avoid need for “open surgery”• Placed at many centers: even those without
VAD or transplant program• More easily removed in setting of recovery• Placed by interventional cardiologists and
surgeons• Allow for recovery or transport to another
center

Disadvantages of Percutaneous Devices
üBleedingüLimited to left ventricular support (except ECMO)
Not for biventricular support Not for RV support (CentriMag can be used)Ventricular arrhythmias
üIschemic limbüUnable to mobilize or rehabüSepsis
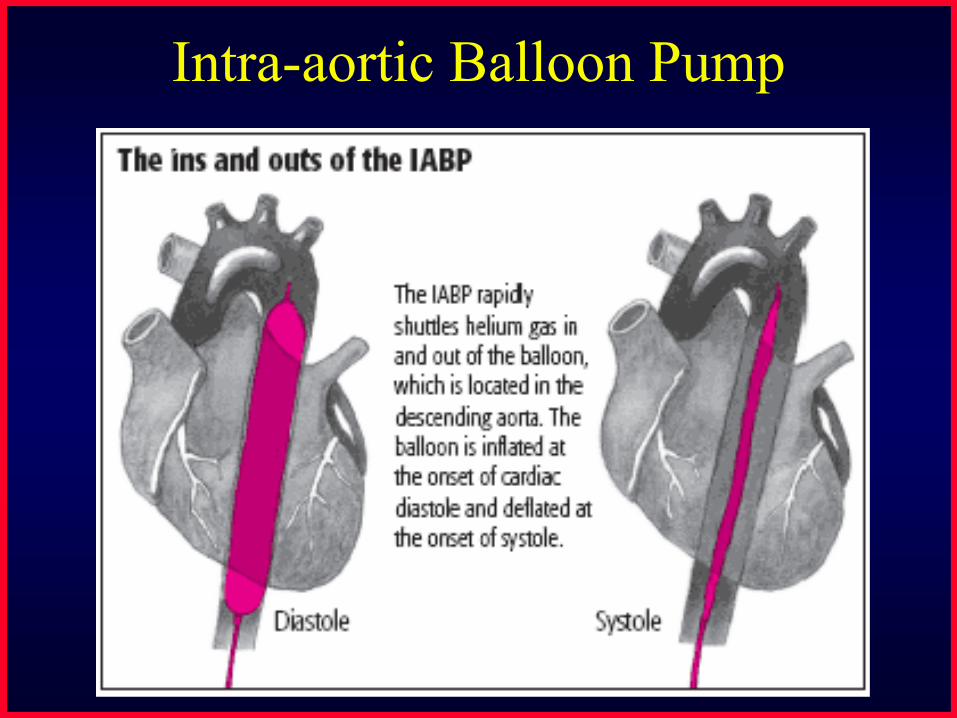
Intra-aortic Balloon Pump

IABP - Advantages• Easily placed in the catheterization
laboratory or operating room• Improves coronary perfusion• Decreases afterload• Decreases myocardial oxygen demand• Can transport patient to another center• Established technology that is widely
available
IABP Disadvantages
• Does not directly support cardiac output• Limited support in the setting of tachycardia
and arrhythmia• May be less effective in older patients with
significant atherosclerosis in aorta

Impella

Impella Advantages
• Small rotary pump• Can be placed percutaneously from femoral
artery across aortic valve without need of trans-septal puncture or venous access
• Can be easily removed
Impella Disadvantages
• Hemolysis – although not felt to be clinically relevant
• Provides partial cardiac output support – up to 2.5 liters/minute in percutaneous model; up to 4-5 liters/minute with model 5.0
• Difficult to place in setting of severe peripheral vascular disease

Impella: Datathe ISAR-SHOCK trial
Seyfarth M, Sibbing D., et. al. JACC 2008;52:1584–8
Improved cardiac power index No difference in survival

Tandem Heart

Tandem Heart Advantages
• Can be placed easily in the catheterization laboratory
• Can supply up to 5 l/min flow• Can be easily removed

Tandem Heart Disadvantages
• Requires trans-septal placement• Difficult to place in setting of severe
peripheral vascular disease

Tandem Heart Data
• Compared to IABP in acute MI with shock (n=41) (Single Center)– Improved cardiac power index, decreased
lactate, improved renal function as compared to IABP
– No difference in 30 day survival and more complications in Tandem Heart group
Thiele H, Sick P, et al. Eur Heart J 2005; 26:1276–1283.

Tandem Heart Data
• Multi-center trial comparing Tandem Heart and IABP in acute MI with shock (N=42)– Tandem Heart improved cardiac output,
decreased PCWP and increased mean arterial pressure as compared to IABP
– No difference in 30 day survival– Similar complication rates
Burkhoff D, Cohen H. Amer Heart J, 152:3, September 2006.

Cheng, JM et al. European Heart J 2009; 30: 2102
30-day mortality
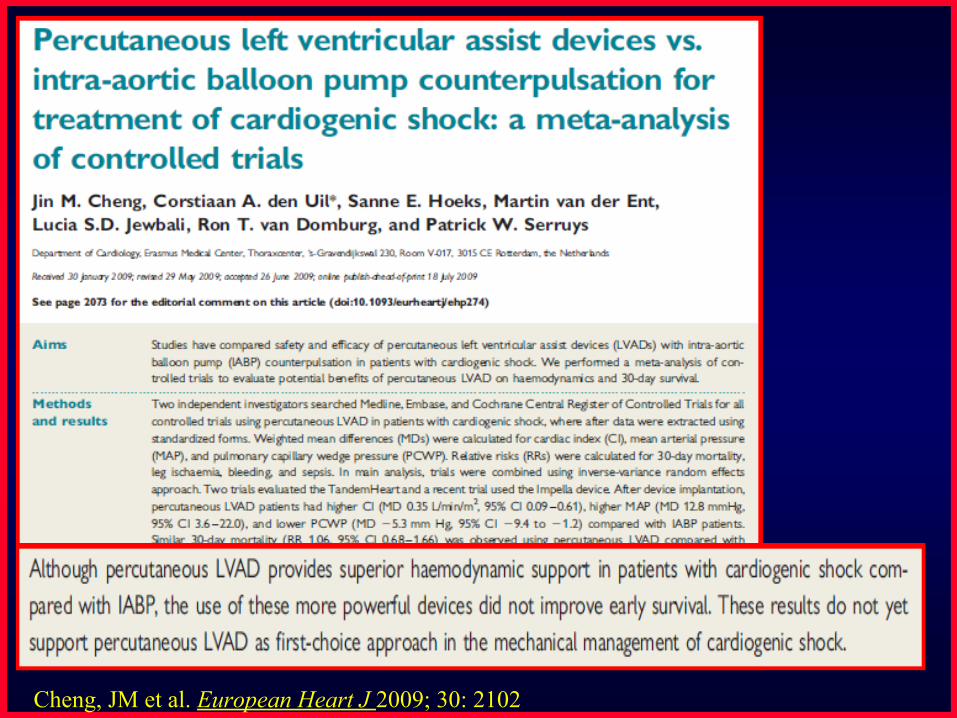
Cheng, JM et al. European Heart J 2009; 30: 2102

ECMO
http://www.emedicine. medscape.com/article/904996-overview

ECMO - AdvantagesüCardio-pulmonary bypassüCan be placed peripherally (without
thoracotomy)üThe only percutaneous option for biventricular
support üThe only option in the setting of lung injury

ECMO - Disadvantages
• Requires trained team and equipment availability on-site and early in resuscitation
• Higher risk of infection, bleeding and vascular injury

Acute Refractory Cardiogenic ShockAcute Refractory Cardiogenic Shock
Temporary VAD/ECMO SupportTemporary VAD/ECMO Support
Recovery/AssessmentRecovery/Assessment
Long-term MCSLong-term MCS
Bridge toBridge to TransplantTransplant DestinationDestination TherapyTherapy BridgeBridge to Recoveryto Recovery
MSOFMSOFNeurologic DeficitNeurologic Deficit
MCS ExplantMCS Explant
Medical TherapyMedical TherapyIABPIABP
Revascularization,Revascularization, surgery surgery
Palliative CarePalliative Care
RehabilitationRehabilitation
Rapid Deterioration (hrs)
MCS in Cardiogenic Shock: Management Algorithm
Gregoric I, Bermudez C. Braunwald Comp., Mechanical Support 2011
Days -Weeks

Limitations of all of this….
• Studies done to date have been small and at a limited number of centers
• Inclusion and exclusion criteria are challenging in the setting of sudden shock
• Populations studied have been somewhat heterogeneous including acutely and chronically ill patients
• The data for “prophylactic use” to support procedures is very encouraging

Issues in the implantation of durable VADs
• Proper selection of patients– Recognizing the patient who is “too sick”, with end-
organ damage– Recognizing the patient who is too debilitated or
malnourished– Recognizing the patient who needs bi-ventricular
support• Timing of surgery
– Especially important in the elderly “destination” patient

Sick patient
Temporary supportChronic support
Unclear situation
1. Support circulation2. Oxygenate patient
Choice dictated by clinical status:temporary supportECMO
Durable VADs pulsatile non-pulsatile
Which Mechanical Support Should We Use as First Line Option?
• The one you have experience with…..• Start simple and think about the appropriate
setting for the patient.• Before you transfer the patient, get all the
details of the medical and social history!• Ask for help, please

Thank You