Embed Size (px)
Citation preview
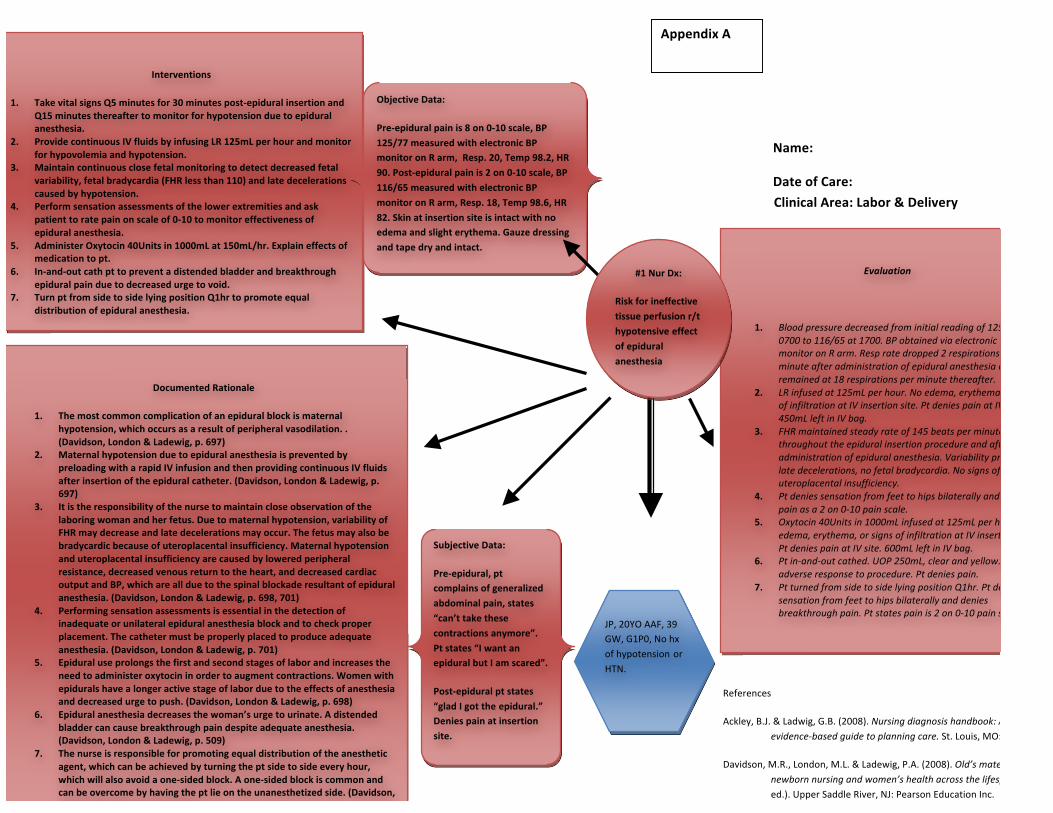
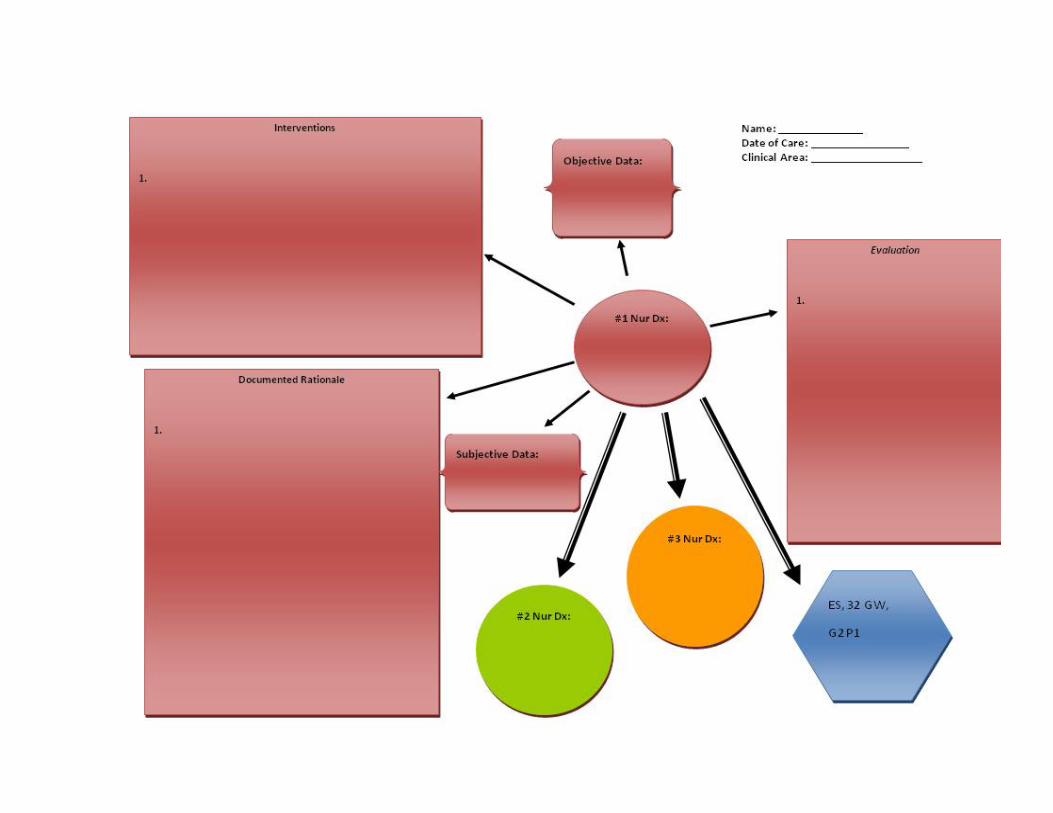
Name:
Date of Care:
Clinical Area: Labor & Delivery
JP, 20YO AAF, 39 GW, G1P0, No hx of hypotension or HTN.
sdfasjdfjasdf
Interventions
1. Take vital signs Q5 minutes for 30 minutes post-‐epidural insertion and Q15 minutes thereafter to monitor for hypotension due to epidural anesthesia.
2. Provide continuous IV fluids by infusing LR 125mL per hour and monitor for hypovolemia and hypotension.
3. Maintain continuous close fetal monitoring to detect decreased fetal variability, fetal bradycardia (FHR less than 110) and late decelerations caused by hypotension.
4. Perform sensation assessments of the lower extremities and ask patient to rate pain on scale of 0-‐10 to monitor effectiveness of epidural anesthesia.
5. Administer Oxytocin 40Units in 1000mL at 150mL/hr. Explain effects of medication to pt.
6. In-‐and-‐out cath pt to prevent a distended bladder and breakthrough epidural pain due to decreased urge to void.
7. Turn pt from side to side lying position Q1hr to promote equal distribution of epidural anesthesia.
SdfasjdfjasdfRationale
Documented Rationale
1. The most common complication of an epidural block is maternal hypotension, which occurs as a result of peripheral vasodilation. . (Davidson, London & Ladewig, p. 697)
2. Maternal hypotension due to epidural anesthesia is prevented by preloading with a rapid IV infusion and then providing continuous IV fluids after insertion of the epidural catheter. (Davidson, London & Ladewig, p. 697)
3. It is the responsibility of the nurse to maintain close observation of the laboring woman and her fetus. Due to maternal hypotension, variability of FHR may decrease and late decelerations may occur. The fetus may also be bradycardic because of uteroplacental insufficiency. Maternal hypotension and uteroplacental insufficiency are caused by lowered peripheral resistance, decreased venous return to the heart, and decreased cardiac output and BP, which are all due to the spinal blockade resultant of epidural anesthesia. (Davidson, London & Ladewig, p. 698, 701)
4. Performing sensation assessments is essential in the detection of inadequate or unilateral epidural anesthesia block and to check proper placement. The catheter must be properly placed to produce adequate anesthesia. (Davidson, London & Ladewig, p. 701)
5. Epidural use prolongs the first and second stages of labor and increases the need to administer oxytocin in order to augment contractions. Women with epidurals have a longer active stage of labor due to the effects of anesthesia and decreased urge to push. (Davidson, London & Ladewig, p. 698)
6. Epidural anesthesia decreases the woman’s urge to urinate. A distended bladder can cause breakthrough pain despite adequate anesthesia. (Davidson, London & Ladewig, p. 509)
7. The nurse is responsible for promoting equal distribution of the anesthetic agent, which can be achieved by turning the pt side to side every hour, which will also avoid a one-‐sided block. A one-‐sided block is common and can be overcome by having the pt lie on the unanesthetized side. (Davidson, London & Ladewig, p. 701-‐702 )
Objective Data:
Pre-‐epidural pain is 8 on 0-‐10 scale, BP 125/77 measured with electronic BP monitor on R arm, Resp. 20, Temp 98.2, HR 90. Post-‐epidural pain is 2 on 0-‐10 scale, BP 116/65 measured with electronic BP monitor on R arm, Resp. 18, Temp 98.6, HR 82. Skin at insertion site is intact with no edema and slight erythema. Gauze dressing and tape dry and intact.
Subjective Data:
Pre-‐epidural, pt complains of generalized abdominal pain, states “can’t take these contractions anymore”. Pt states “I want an epidural but I am scared”.
Post-‐epidural pt states “glad I got the epidural.” Denies pain at insertion site.
sdfasjdfjasdf
Evaluation
1. Blood pressure decreased from initial reading of 125/77 at 0700 to 116/65 at 1700. BP obtained via electronic BP monitor on R arm. Resp rate dropped 2 respirations per minute after administration of epidural anesthesia and remained at 18 respirations per minute thereafter.
2. LR infused at 125mL per hour. No edema, erythema, or signs of infiltration at IV insertion site. Pt denies pain at IV site. 450mL left in IV bag.
3. FHR maintained steady rate of 145 beats per minutes throughout the epidural insertion procedure and after the administration of epidural anesthesia. Variability present, no late decelerations, no fetal bradycardia. No signs of uteroplacental insufficiency.
4. Pt denies sensation from feet to hips bilaterally and rates pain as a 2 on 0-‐10 pain scale.
5. Oxytocin 40Units in 1000mL infused at 125mL per hour. No edema, erythema, or signs of infiltration at IV insertion site. Pt denies pain at IV site. 600mL left in IV bag.
6. Pt in-‐and-‐out cathed. UOP 250mL, clear and yellow. No adverse response to procedure. Pt denies pain.
7. Pt turned from side to side lying position Q1hr. Pt denies sensation from feet to hips bilaterally and denies breakthrough pain. Pt states pain is 2 on 0-‐10 pain scale.
#1 Nur Dx:
Risk for ineffective tissue perfusion r/t hypotensive effect of epidural anesthesia
References
Ackley, B.J. & Ladwig, G.B. (2008). Nursing diagnosis handbook: An evidence-‐based guide to planning care. St. Louis, MO: Mosby.
Davidson, M.R., London, M.L. & Ladewig, P.A. (2008). Old’s maternal-‐newborn nursing and women’s health across the lifespan. (8th ed.). Upper Saddle River, NJ: Pearson Education Inc.
Appendix A