Embed Size (px)
Citation preview

תזמון הניתוח במחלות כירורגיות חריפות
התערבות ניתוחית במחלות כירורגיות
חריפותבטן חריפה הם מתחום התמחותו אבחנה והערכה של bull
ומומחיותו של הכירורג הכללי
ACSACS -אם תרצו בעתיד bull
אתגר למנתח עדיין מהווה בזמן סביר אבחון המחלהbull
ניתוח דחוף הוא אחד מהאמצעים העומדים לרשות הכירורג bull
לאבחון וטיפול במחלות כירורגיות חריפות
bullldquoOnly skin separates us from the diagnosisrdquo
על תזמון הניתוחים מבוססת אין כיום בספרות הסכמהbull
הדחופים במגוון מחלות כירורגיות שכיחות
תזמון ניתוחים דחופים
o קיים דיון בספרות לגבי ניתוח באבחנה של דלקת
תוספתן קלה
o מסתמן כי ניתוח בעת דלקת חריפה של כיס המרה בטוח
o ברור כי דחיית ניתוח בחולים שלקו בדלקת לבלב קלה
על רקע אבנים תביא להישנות דלקת הלבלב או כיס
המרה
שינוי בפרדיגמה לעכלהאם כירורג יוכל
ברור כיום כי התקף שני ואף -דוגמא לשינוי בפרדיגמה
שלישי של דלקת סעיפים אינו הוריה לניתוח
הסיבה לכאבי הבטן
סיבות שכיחות לכאבי בטן 50 -בספרי הלימוד כbull
הכירורג אינו עובד עם רשימה מוכנה מראש אלא מזהה מאפיינים bull (CLINICAL PATTERNS)קליניים
ישתמש המנתח ברשימה קצרה של אפשרויות טיפול בפועלbull
It is as much an intellectual exercise to tackle the problems of belly ache as to It is as much an intellectual exercise to tackle the problems of belly ache as to
work on the human genomework on the human genome
Hugh DudleyHugh Dudley
Clinical patterns -מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
The abdomen is not a The abdomen is not a black box any moreblack box any more
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדם ברורbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

התערבות ניתוחית במחלות כירורגיות
חריפותבטן חריפה הם מתחום התמחותו אבחנה והערכה של bull
ומומחיותו של הכירורג הכללי
ACSACS -אם תרצו בעתיד bull
אתגר למנתח עדיין מהווה בזמן סביר אבחון המחלהbull
ניתוח דחוף הוא אחד מהאמצעים העומדים לרשות הכירורג bull
לאבחון וטיפול במחלות כירורגיות חריפות
bullldquoOnly skin separates us from the diagnosisrdquo
על תזמון הניתוחים מבוססת אין כיום בספרות הסכמהbull
הדחופים במגוון מחלות כירורגיות שכיחות
תזמון ניתוחים דחופים
o קיים דיון בספרות לגבי ניתוח באבחנה של דלקת
תוספתן קלה
o מסתמן כי ניתוח בעת דלקת חריפה של כיס המרה בטוח
o ברור כי דחיית ניתוח בחולים שלקו בדלקת לבלב קלה
על רקע אבנים תביא להישנות דלקת הלבלב או כיס
המרה
שינוי בפרדיגמה לעכלהאם כירורג יוכל
ברור כיום כי התקף שני ואף -דוגמא לשינוי בפרדיגמה
שלישי של דלקת סעיפים אינו הוריה לניתוח
הסיבה לכאבי הבטן
סיבות שכיחות לכאבי בטן 50 -בספרי הלימוד כbull
הכירורג אינו עובד עם רשימה מוכנה מראש אלא מזהה מאפיינים bull (CLINICAL PATTERNS)קליניים
ישתמש המנתח ברשימה קצרה של אפשרויות טיפול בפועלbull
It is as much an intellectual exercise to tackle the problems of belly ache as to It is as much an intellectual exercise to tackle the problems of belly ache as to
work on the human genomework on the human genome
Hugh DudleyHugh Dudley
Clinical patterns -מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
The abdomen is not a The abdomen is not a black box any moreblack box any more
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדם ברורbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

תזמון ניתוחים דחופים
o קיים דיון בספרות לגבי ניתוח באבחנה של דלקת
תוספתן קלה
o מסתמן כי ניתוח בעת דלקת חריפה של כיס המרה בטוח
o ברור כי דחיית ניתוח בחולים שלקו בדלקת לבלב קלה
על רקע אבנים תביא להישנות דלקת הלבלב או כיס
המרה
שינוי בפרדיגמה לעכלהאם כירורג יוכל
ברור כיום כי התקף שני ואף -דוגמא לשינוי בפרדיגמה
שלישי של דלקת סעיפים אינו הוריה לניתוח
הסיבה לכאבי הבטן
סיבות שכיחות לכאבי בטן 50 -בספרי הלימוד כbull
הכירורג אינו עובד עם רשימה מוכנה מראש אלא מזהה מאפיינים bull (CLINICAL PATTERNS)קליניים
ישתמש המנתח ברשימה קצרה של אפשרויות טיפול בפועלbull
It is as much an intellectual exercise to tackle the problems of belly ache as to It is as much an intellectual exercise to tackle the problems of belly ache as to
work on the human genomework on the human genome
Hugh DudleyHugh Dudley
Clinical patterns -מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
The abdomen is not a The abdomen is not a black box any moreblack box any more
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדם ברורbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
הסיבה לכאבי הבטן
סיבות שכיחות לכאבי בטן 50 -בספרי הלימוד כbull
הכירורג אינו עובד עם רשימה מוכנה מראש אלא מזהה מאפיינים bull (CLINICAL PATTERNS)קליניים
ישתמש המנתח ברשימה קצרה של אפשרויות טיפול בפועלbull
It is as much an intellectual exercise to tackle the problems of belly ache as to It is as much an intellectual exercise to tackle the problems of belly ache as to
work on the human genomework on the human genome
Hugh DudleyHugh Dudley
Clinical patterns -מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
The abdomen is not a The abdomen is not a black box any moreblack box any more
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדם ברורbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Clinical patterns -מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
The abdomen is not a The abdomen is not a black box any moreblack box any more
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדם ברורbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
The abdomen is not a The abdomen is not a black box any moreblack box any more
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדם ברורbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
The abdomen is not a The abdomen is not a black box any moreblack box any more
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדם ברורbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
The abdomen is not a The abdomen is not a black box any moreblack box any more
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדם ברורbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
כאבי בטן הקשורים למחלה לא כירורגיתbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
The abdomen is not a The abdomen is not a black box any moreblack box any more
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדם ברורbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
The abdomen is not a The abdomen is not a black box any moreblack box any more
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדם ברורbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדם ברורbull
טיפול לא ניתוחיbull
שחרור החולה הביתהbull
מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

מההסתמנויות הקליניות
כאבי בטן והלםbull
פריטוניטיס מפושטתbull
פריטוניטיס ממוקמתbull
חסימת המעיbull
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
מאפשרויות הטיפול שיכול הכירורג לבחור
ניתוח כעתbull
הכנה וניתוח מחר או בהקדםbull
כ טיפול לא ניתוחי בדbull
מחייבתההסתמנות הקלינית וניתוח רק במקרה
שחרור החולה הביתהbull
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
שינוי בפרדיגמה
כמעט כול פריטוניטיס נפתרה בניתוח בעברbull
כיום עם לימוד ונסיוןbull
הבנת הפיסיולוגיה
הכרת הפתופיזיולוגיה
זיהוי המהלך הטבעי של מחלות חריפות
שיפור ושימוש מושכל בהדמיה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
כירורגיה מודרנית
בחירה בגישה הכירורג יכול להפחית תמותה ותחלואה עי
פחות פולשנית ויותר סלקטיבית במגוון מחלות חריפות
ולמעשה
להשיג יותר בלעשות פחות
לאחר חשיבה והליך מושכל לברירת החלטות
האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

האם כדאי לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
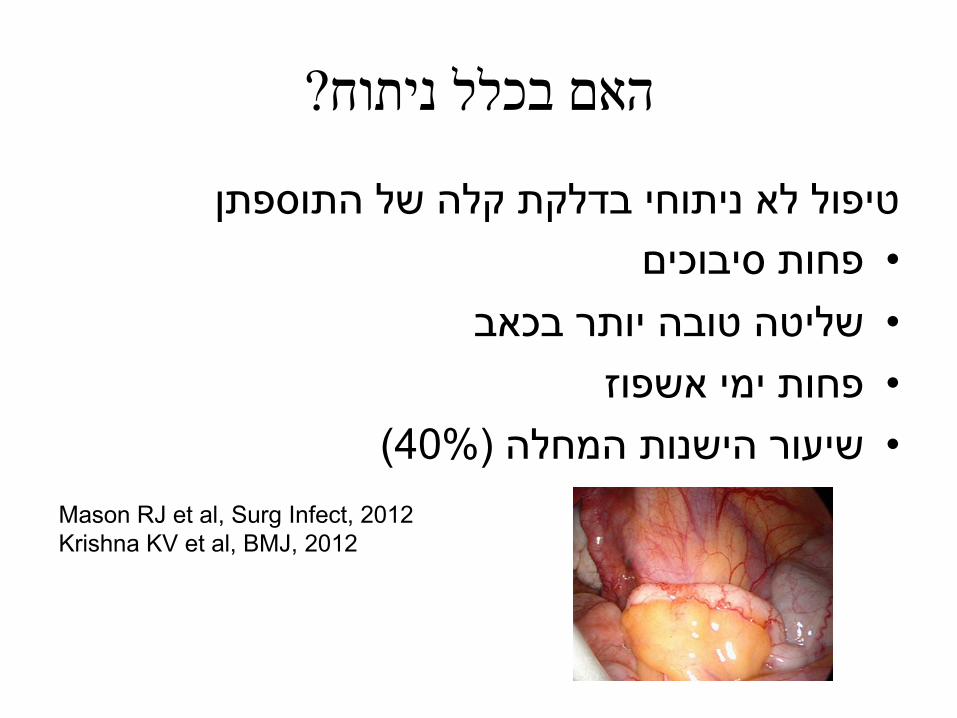
האם בכלל ניתוח
טיפול לא ניתוחי בדלקת קלה של התוספתן
פחות סיבוכיםbull
שליטה טובה יותר בכאבbull
פחות ימי אשפוזbull
( 40)שיעור הישנות המחלה bull
Mason RJ et al Surg Infect 2012
Krishna KV et al BMJ 2012
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
האם כדאי נעז לדחות ניתוח התוספתן לבוקר או בכלל לטפל רק
באנטיביוטיקה
מדוע לא ניתן לטפל באופן לא ניתוחי בחולים הלוקים בדלקת קלה
נטפל באופן שמרני בדיברטיקוליטיסשל התוספתן ולעומת זאת
האם כי פשוט יותר לנתח או כי אנו שבויים בפרדיגמות
האם כדאי לנתח חולה הלוקה בדלקת כיס המרה בליל התקבלותו
באשפוז נפרד לאחר החלמה מהמחלה החריפה למחרת אשפוזו
האם המערכת מעמידה לרשותנו חדרי ניתוח למחרת התורנות
האם נכון לדחות ניתוחים לבוקר והיה וכן
או שמא לנוחות הרופא האם הדחייה היא לטובת החולה
מה לגבי תזמון הניתוח בחולה הדחוף
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו על
משך האשפוז
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
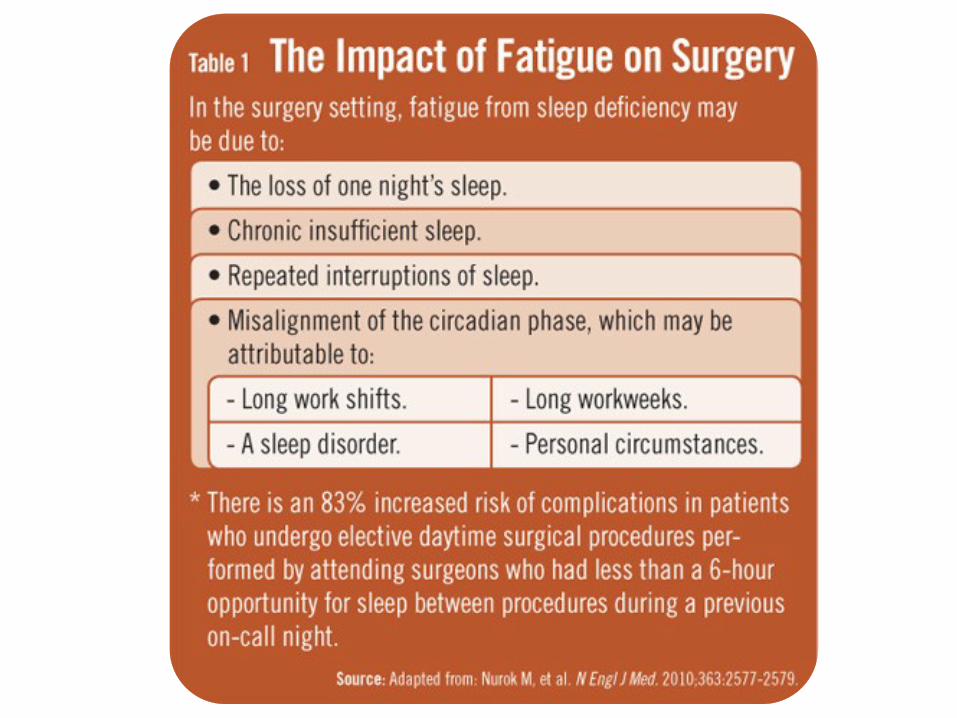
תזמון הניתוח
לתזמון מועד הניתוח השפעה על מהלך המחלה ואפילו bull
על משך האשפוז
בעוד מרביתנו חושבים כי לניתוח נינוח בשעות הבוקר bullמצאו משיקגו וחב Crandall השפעה מיטבה על חוליינו
כי ניתוחים בלילה מקצרים באופן משמעותי את משך
( ( Surg Infections 2009האשפוז הממוצע
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
מטרת הדיון
לבדוק
האם ראוי לשנות פרדיגמת טיפול במספר 1
שכיחות מחלות כירורגיות חריפות
מתי ראוי וכדאי לנתח חולים המתייצגים עם 2
מחלה כירורגית חריפה
-דיון בשלוש מחלות שכיחות
דלקת התוספתן
דלקת כיס המרה
חסימת מעי דק על רקע הדבקויות
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
למה בחרנו במחלות השכיחות
קיימת אבחנה מבדלת פריטוניטיס ממוקמת -דלקת התוספתןbullהתנקבות (בדיקת גניקולוג US טומוגרפיה)המחייבת בירור
כ מגיע התוספתן אינה מתחוללת תוך כדי הבירור אלא החולה בדuarr 5= שעות בניתוח 12עיכוב של למיון עם התנקבות בשיעור ההתנקבות
מספר רב רוב החולים יגיבו לטיפול אנטיביוטי -דלקת כיס המרהbull
של חולים מתקבלים בתורנות באבחנה זו
רוב החולים יחלימו בטיפול -חסימת המעי הדק על רקע הדבקויותbull
כיצד נקבע מי החולה הנדרש אל תיתן לחמה לזרוח שמרני
מתי נכריז על מי החולה שנכשל בטיפול שמרני לניתוח מידי
כשלון של טיפול שמרני
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
משתתפי הדיון
אריאל הלוי פרופbull
שמואל אביטל דרbull
שלמה קייזר פרופbull
בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

בוחני הספרות
ערן בראונר דרbull
טטיאנה דורפמן דרbull
שחר גרונר דרbull
ידענים מופלגים בחומר הנדון מעודכנים (לאחרונה) בוגרי שלב ב
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Iמקרה
בריא 35גבר בן bull
אומביליקאליים שנדדו לבטן ימנית -כאבי בטן פריbull
תחתונה
הקאות בחילותbull
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Iמקרה
רגישות ניכרת בבטן ימנית תחתונהbull
סימני גירוי ציפקיbull
380חום bull
קתאים לסמ 13000 ספירה לבנהbull
דלקת התוספתן -אבחנה קליניתbull
-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

-שאלה
כיצד תתקדם
חשד סביר כי לחולה דלקת התוספתן אך אבצע 1
טומוגרפיה לאשר האבחנה ואז אנתח
חשד סביר כי לחולה דלקת התוספתן אך אבצע 2
במידה והאולטראסאונד אינו אולטראסאונד ואז אנתח
חד משמעי רק אז אבצע טומוגרפיה
אין צורך לחולה פריטוניטיס בבטן ימנית תחתונה 3
אעביר לחדר ניתוח ואבצע לפרוסקופיה בהדמיה
לא אכרות -אין דלקת אכרות -דלקת
אך אכרות בכול מקרה את התוספתן 3כבתשובה 4
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
של התוספתן קלהעדות ברורה לדלקת -בטומוגרפיה
ללא נוזל או אוויר חופשי
אתחיל אנטיביוטיקה ואעביר את החולה לחדר 1
הניתוח
אתחיל אנטיביוטיקה ואדחה הניתוח לבוקר2
אתחיל אנטיביוטיקה ואבדוק את החולה בבוקר 3
-במידה ויחוש היטב וסימני הגירוי הצפקי ייעלמו
אמשיך בטיפול אנטיביוטי אך לא אנתח
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
שאלות לצוות
מה זמן ההמתנה הממוצע לכריתת תוספתן מודלק bull
במחלקתך
האם במחלקתך מנותחים כיום חולים על סמך bull
קליניקה בלבד וללא הדמיה
מה הזמן הממוצע מאבחנה עד מתן מנה ראשונה bull
של אנטיביוטיקה במיון במוסדך
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
מחלה שכיחה ופשוטה -דלקת התוספתן
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

ערן בראונר דר
תזמון הניתוח בדלקת חריפה של
שינוי בפרדיגמה -התוספתן
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
1500השעה
חדר המיון -המקוםחולה עם כאבי בטן לא טיפוסיים אובחן עם דלקת bull
CT -פ השל התוספתן ע
לאור הנתונים בחדר המיון נראה כי נוכל לנתחוbull
0200בשעה במקרה הטוב
מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

מה לעשות
לקרוא לכונן ולנתח בשני חדרים במקבילbull
אולי אפנה אותו לבית חולים אחרbull
ונמתין לבוקר אולי אתן לו אנטbull
מנתח רענן יעשה את העבודה אולי טוב יותר
איני מסכן את החולה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
האם ננתח את החולה בכול שעה שהיאbull
זעקה במיון אשתו האפנדיציט יתפוצץ בבטןbull
מי כאן אולטראסול שמולטרסול של החולה
המנהל
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
האם ניתן לדחות ניתוח בדלקת של התוספתן
bull Acute appendicitis is the most common surgical emergency
bull Luminal obstruction increased mucus production bacterial overgrowth and stasis
increase appendiceal wall tension
blood and lymph flow is diminished
necrosis and perforation
A pathophysiology of a ldquoticking bombrdquo
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
הפרמטרים שנבדקים בספרות
זמן אשפוז לאחר הניתוחbull
פתולוגיה סופיתbull
סיבוכים כגון זיהום בפצע הניתוחיbull
יום לאחר הניתוח 30תחלואה ותמותה במשך bull
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
מבוגרים אשר עברו כריתת תוספתן עקב דלקת 1287עבודה רטרוספקטיבית של
2004למרץ 1998בתקופה שבין פברואר
דרגות 4הממצאים הניתוחיים והפתולוגיים חולקו ל
G1 דלקת פשוטה
G2 תוספתן גנגרנוטי
G3 תוספתן מנוקב
G4 אבצס פריאפנדיקולארי
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
The present study demonstrates that the severity of pathology and complication rate in adult patients with acute appendicitis are time dependent
Delaying appendectomy is unsafe
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
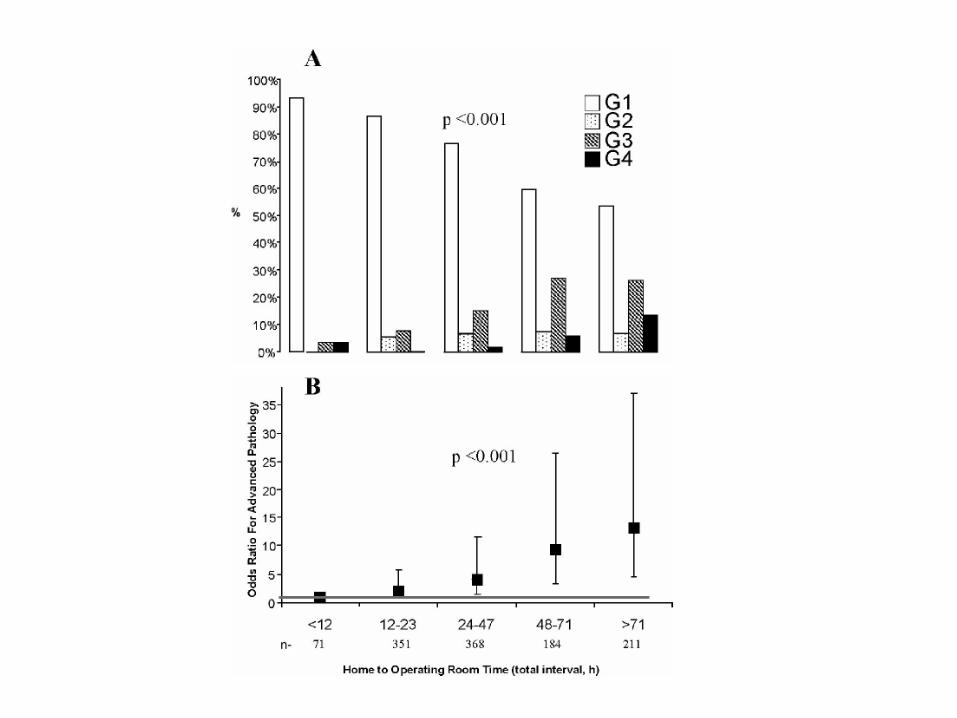
חולים 114עבודה אשר בדקה באופן פרוספקטיבי bull
אשר עברו כריתת התוספתן
ועד ההגעה לבית החולים זמן מתחילת הסימפטbull
זמן אשר עבר מההגעה לבית החולים ועד הניתוח bull
advancedמול earlyהפתולוגיות חולקו ל bull
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
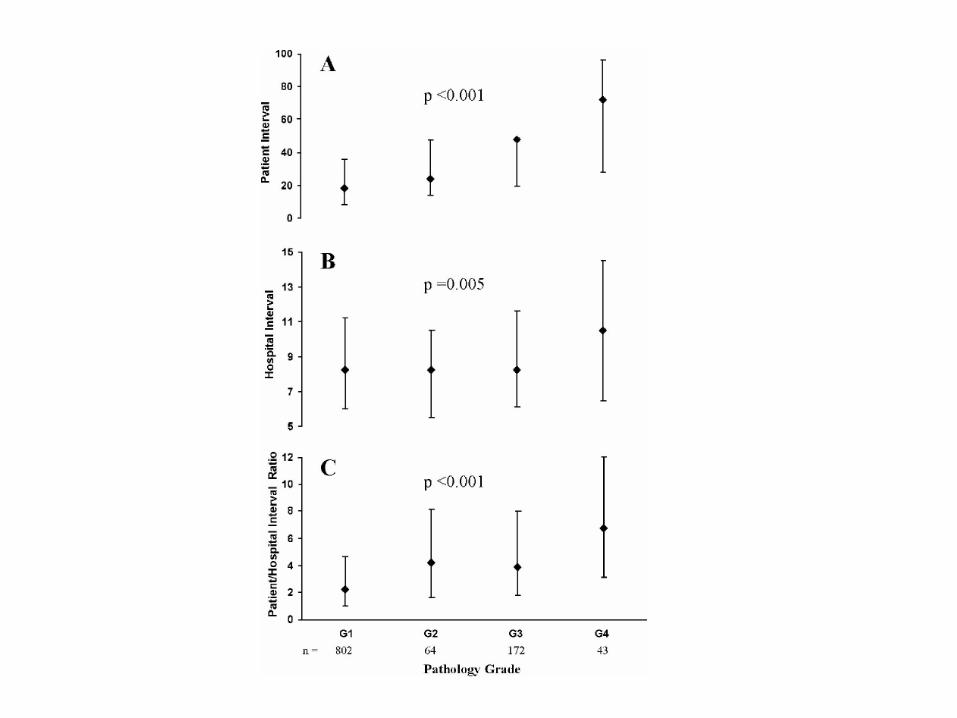
עבודה רטרוספקטיבית על גיליונות חולים אשר עברו כריתת
במוסד יחיד 2009התוספתן בשנת
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 10חולים אשר עברו ניתוח בתוך 1
שעות מהתקבלותם 10חולים אשר עברו ניתוח לאחר 2
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
מדוע לא לדחות ניתוח לכריתת התוספתן
ככול שנוקף הזמן הפתולוגיה מתקדמתbull
SSI -סיכוי גבוה יותר לbull
זמן האשפוז מתארךbull
הסיכוי לאשפוז חוזר גבוה יותרbull
החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

החולשות בעבודות
העבודות לא מזכירות את הזמן מההתיצגות ועד bull
קבלת הטיפול האנט
אין קבוצת ביקורת שכן הנתונים הם bull
רטרוספקטיביים גם אם החולים נאספים
פרוספקטיבית
לחולים קשים יותר ניגשים מהר יותרbull
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
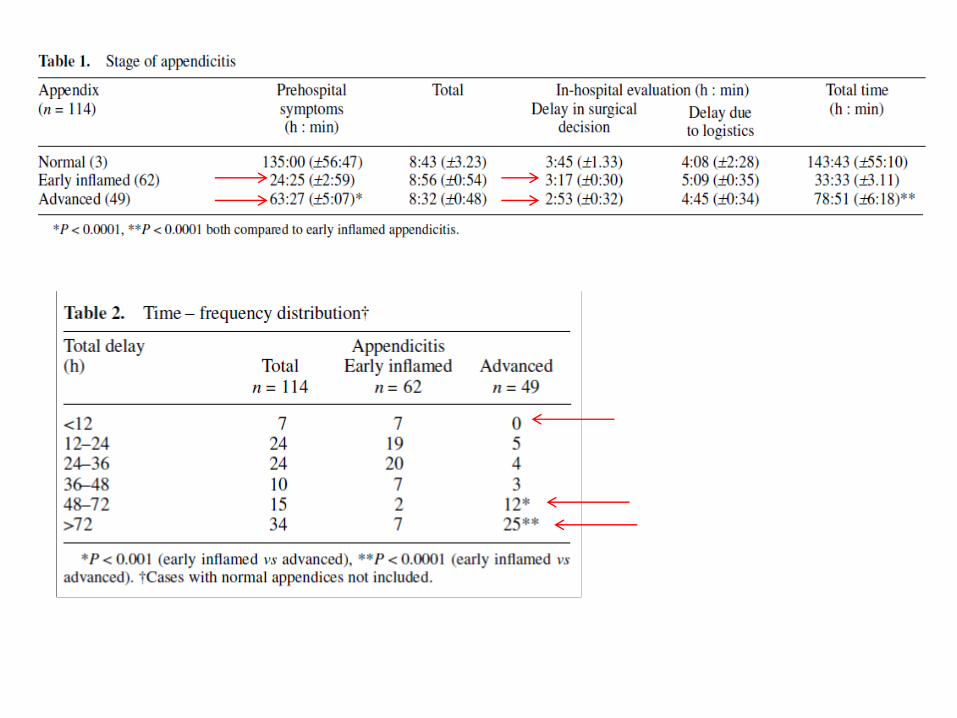
A retrospective chart review of all patients undergoing
appendectomy in a single community surgical specialty
practice between August 2002 and May 2007
A total of 1198 patients underwent appendectomy during
the study period
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Similar
relationships were seen related
to reported duration of
symptoms (data not shown)
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
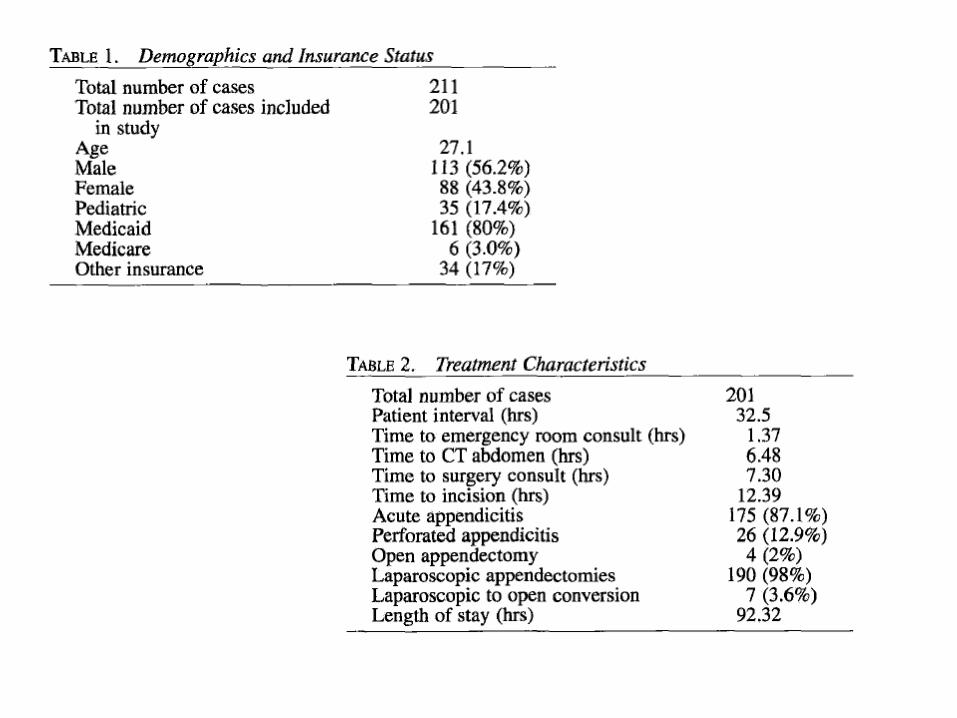
Outcome in acute appendicitis is related most closely to the severity of the acute appendicitis at presentation
Unaffected by timing of
surgical intervention
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
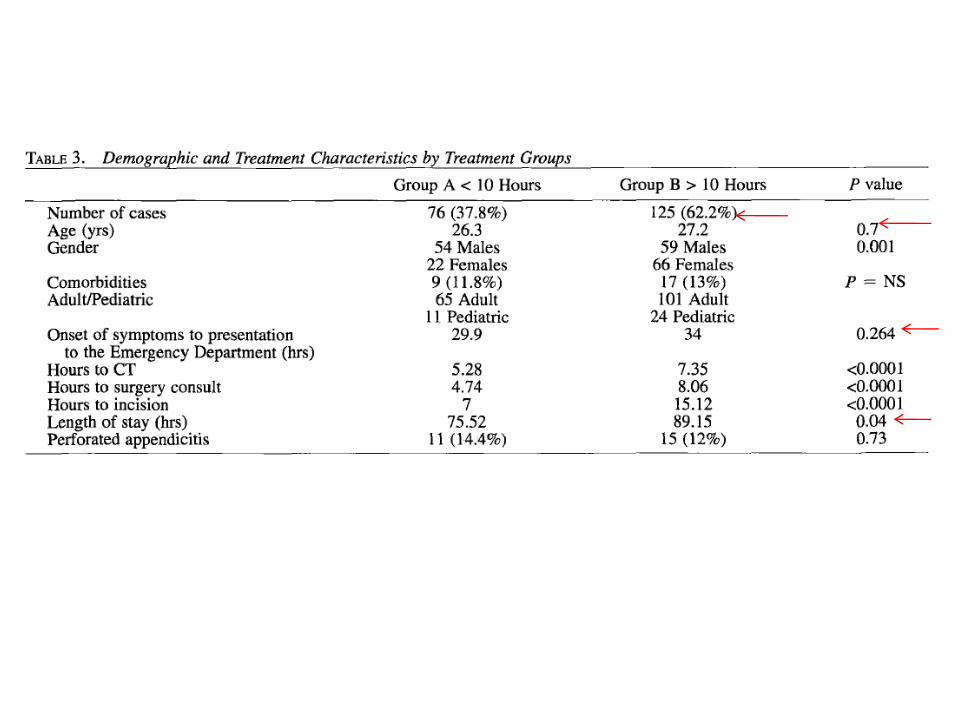
מחקר רטרוספקטיבי
ממאגר מיידע
ACS national surgical quality improvement program (ACS NSQIP)
חולים אשר עברו כריתת התוספתן 32782
2008ועד דצמבר 2005ינואר
יום לאחר הניתוח 30תחלואה ותמותה במשך
שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

שעות מהתקבלותם 6נותחו תוך פחות מ ( 752) 24647
שעות מהתקבלותם 12ל 6נותחו בין ( 151) 4937
שעות מהתקבלותם 12נותחו לאחר ( 98) 3201
38גיל ממוצע
גברים( 539) 17672
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
simple appendicitisסבלו מ ( 834) 27334
complicated appendicitisסבלו מ ( 166) 5448
שעות 49זמן ממוצע כולל מקבלה לניתוח
6gtשעות בקבוצה 15
12gt6ltשעות בקבוצה 85
12ltשעות בקבוצה 26
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
שעות יש השפעה מרעה 12לבדוק האם לדחייה של כריתת התוספתן ב מטרת העבודה
ועד דצמבר 2002גיליונות של חולים אשר עברו ניתוח מינואר 380 עבודה רטרוספקטיבית
2004
אוכלוסיית החולים חולקה לשתי קבוצות
שעות מהתקבלותם 12חולים אשר נותחו בתוך 1
שעות מהתקבלותם 24ל 12חולים אשר נותחו בין 2
ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

ודחיית הניתוח לשעות מתן נוזלים ואנט
שעות מהאשפוז היא 24היום בטווח של
אופציה בטוחה ופרקטית
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
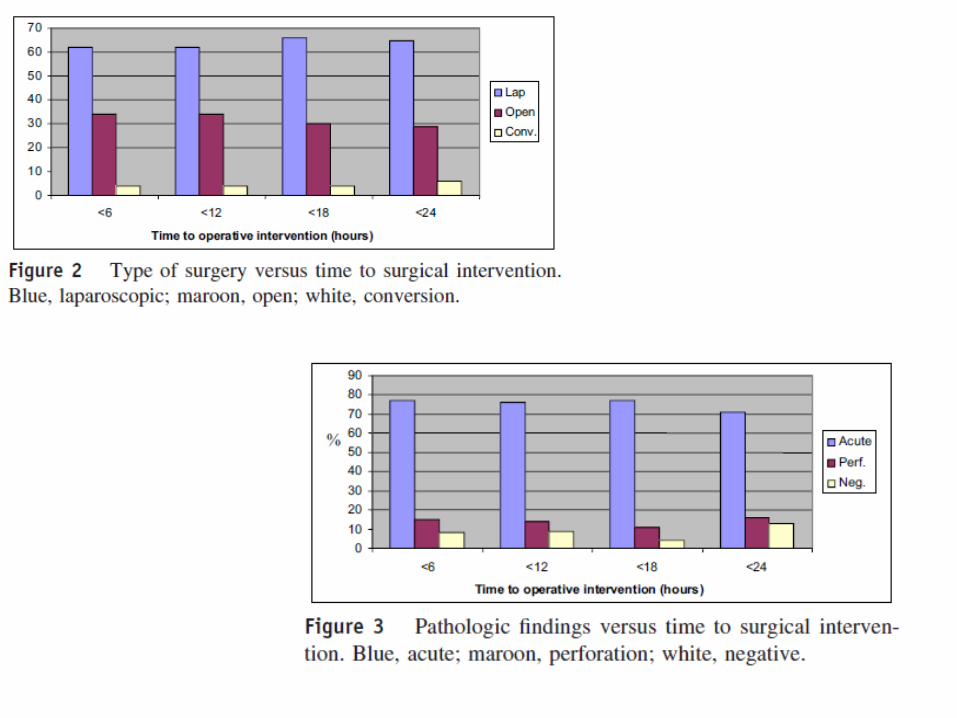
מסקר הספרות עולה כי
העבודות אשר בודקות השפעת דחיית הניתוח אינן1
עבודות פרוספקטיביות מבוקרות
ואשר אין עבודה אחת אשר בודקת את הזמן למתן אנט2
הזמן לניתוחמבטלת את משתנה
בקומץ עבודות בלבד נמצא כי ניתן להחליף ניתוח באנט3
בלבד ידרשו לניתוח מאלו שטופלו באנט 40כ 4
אחוז לא מבוטל המעמיד בספק את ערך -בהמשך
הטיפול האנטיביוטי לבדו
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
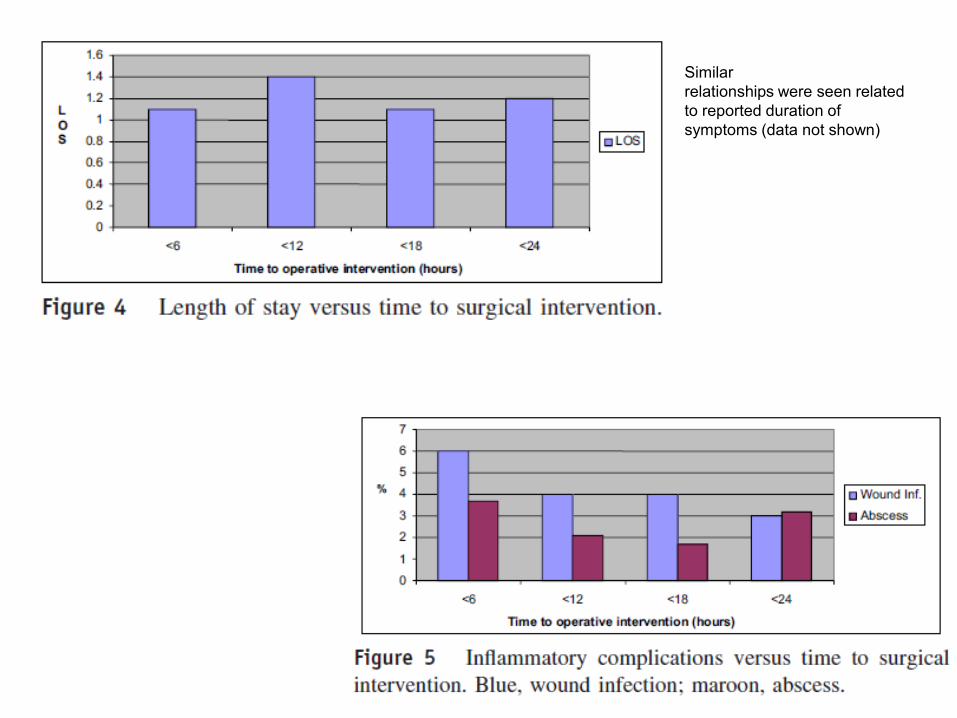
מה נציע
24 -לכריתת התוספתן מעבר ללא לדחות ניתוח 1
שעות
בחולה המאובחן עם טיפול אנטלא לדחות כלל 2
דלקת של התוספתן
הינו הטיפול ניתוח3
בדלקת התוספתן
IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

IIמקרה
בלונדינית שמנה קלות 40חולה בת bull
מזה מספר שעות כאבים ברום הבטן הימניתbull
מלווים בבחילות קשות
אירועים נשנים של כאבים מהסוג הזה -ברקעbull
IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

IIמקרה
בבדיקת הבטן רגישות ממוקמת לבטן הימנית bull
העליונה מלווה ברבאונד קל
380חום הגוף bull
3תאים לממ 13000ספירה לבנה -בבדיקות הדםbull
(בילירובין בלבד)תפקודי הכבד תקינים bull
דיאסטאז בדם ובשתן תקינים bull
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
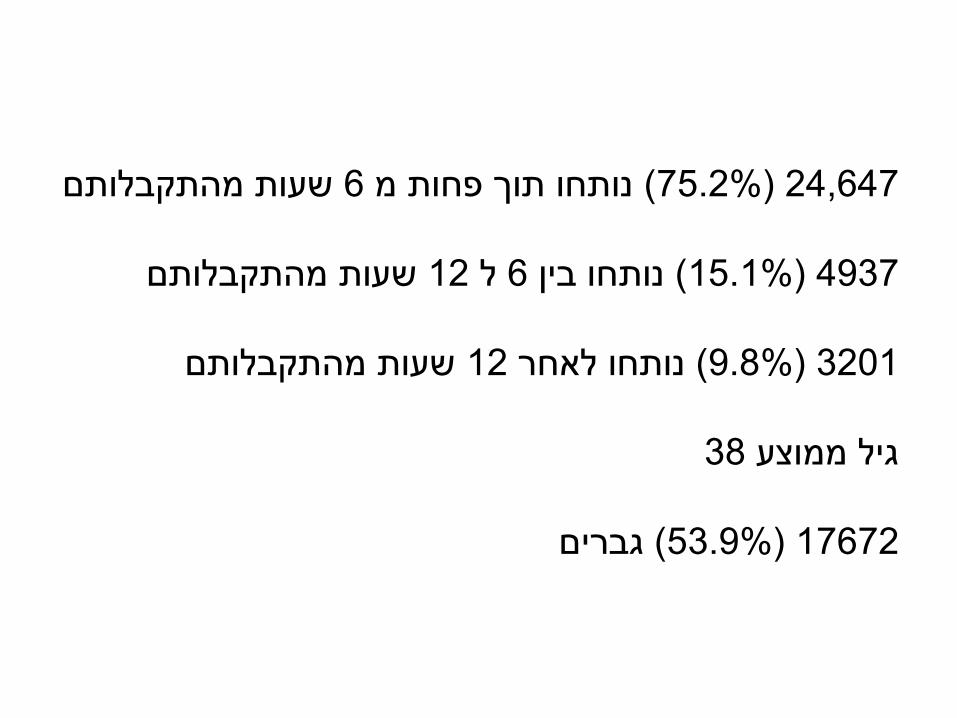
שאלה
באיזה מהלך תבחר
לאור מצבה הכללי הטוב אנתחה במהלך הלילה 1
בגישה לפרוסקופית
לאור מצבה הכללי הטוב אנתחה הלילה בגישה 2
פתוחה
לאור מצבה הכללי הטוב אתחיל טיפול אנטיביוטי 3
ואנתחה בבוקר
לאור מצבה הטוב אתחיל טיפול אנטיביוטי 4
ואנתחה באשפוז נפרד
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
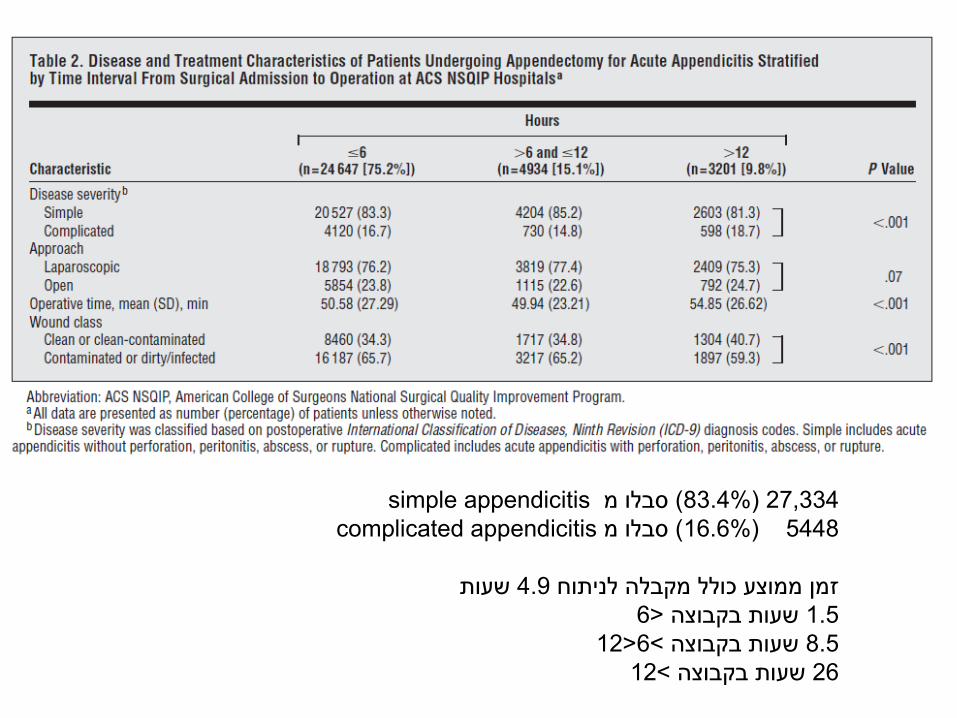
בחרת לטפל בחולה באנטיביוטיקה בלבד
חום שעות מהתקבלותה 24 במהלך האשפוז
כאבי הבטן מתגברים 390גופה
כעת הזמן לנתחה1
אשנה את הטיפול לאנטיביוטיקה רחבת טווח2
אזמין ניקוז כיס המרה באולטראסאונד3
מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

מתי תבחר לנתח את בחרת לנקז את כיס המרה
החולה
למחרת הניקוז 1
שלושה -תוך שבועיים2
בעוד שישה שבועות ללא צילום דרכי המרה3
בעוד שישה שבועות ולאחר צילום דרכי המרה4
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
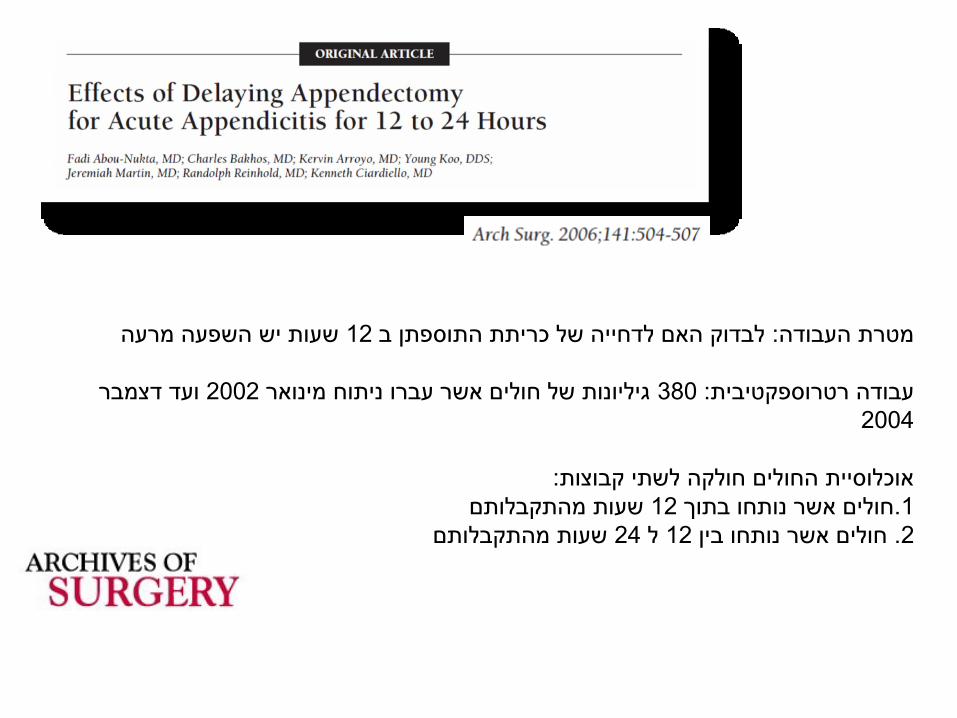
בדיקות הדם הראשונות במיון -לאותה חולה המתוארת
באולטראסאונד בדם ובשתן בדיאסטאזהראו עליה
דרכי המרה אינם נצפתה בצקת קלה של ראש הלבלב
רחבים ואנזימי הלבלב ירדו לנורמה לאחר יומיים
חולה זו אנתח בתוך האשפוז הראשון וכעבור מספר 1
ימים מהתקבלותה
אשחרר את החולה ואזמנה לניתוח בתוך שישה 2
שבועות
אשחרר את החולה ואזמנה לניתוח לאחר שישה 3
שבועות
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
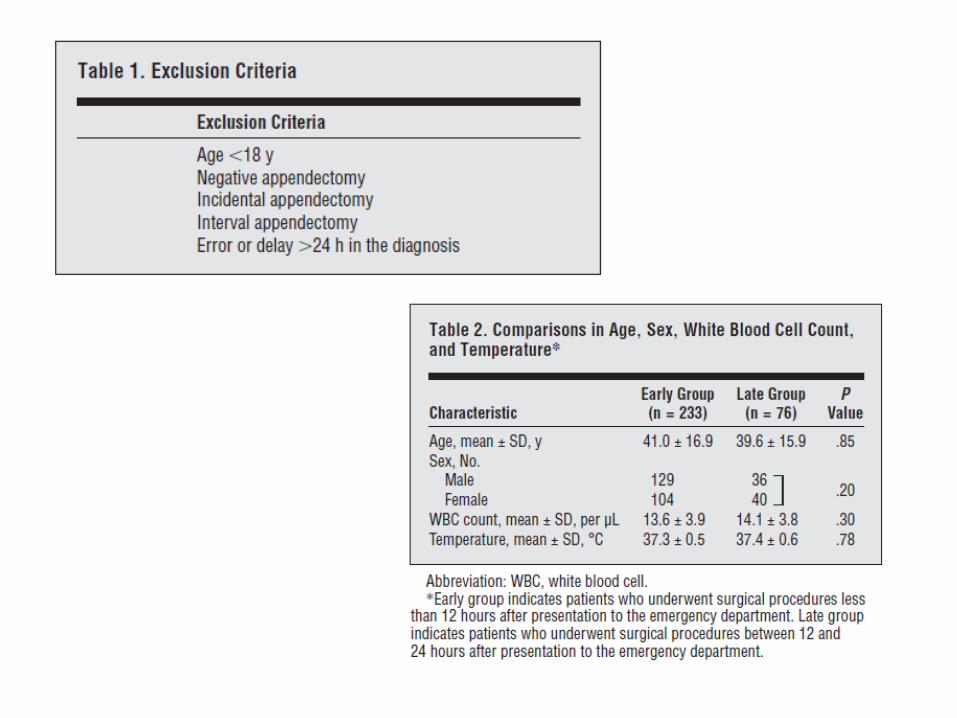
שאלות לצוות
כמה חולים מתאשפזים במחלקתך בממוצע ביום bull
תורנות באבחנה של דלקת חריפה של כיס המרה
כמה חולים מנותחיםbullמיד
למחרת
באשפוז נוכחי
באשפוז אחר
לאיזה חולה תמליץ על התקנת מנקז מלעוריbull
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
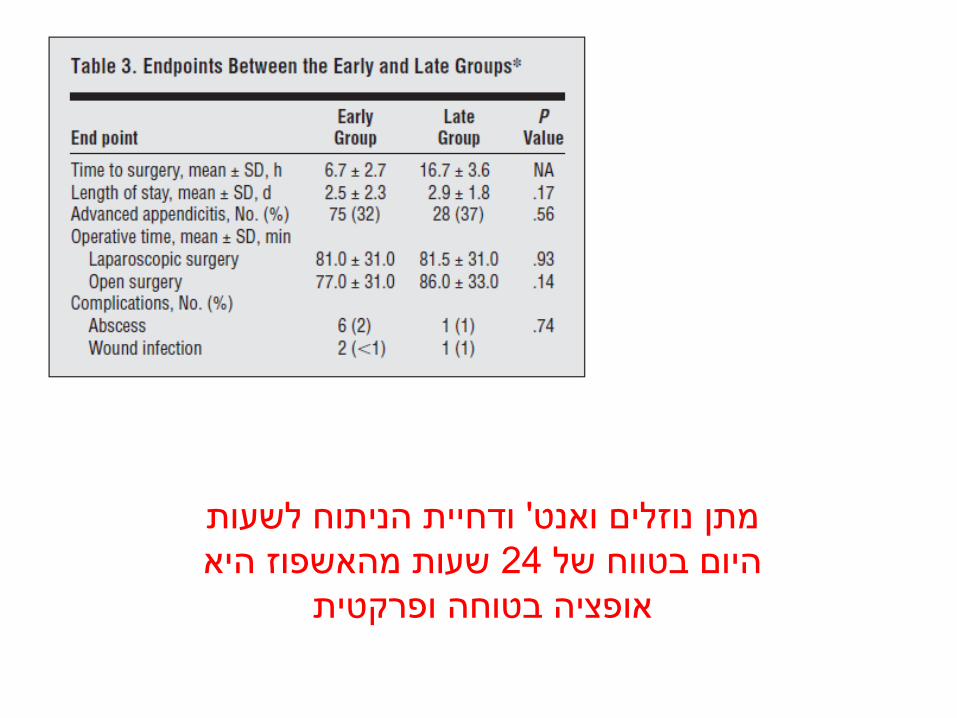
מחלה שכיחה ופשוטה -דלקת כיס המרה
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
עומס על חדרי הניתוח
נוכחות רופא בכיר במיון
קיומה של מערכת חדרי ניתוח זמינה בבוקר
מודעות
ניקוז מלעורי
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
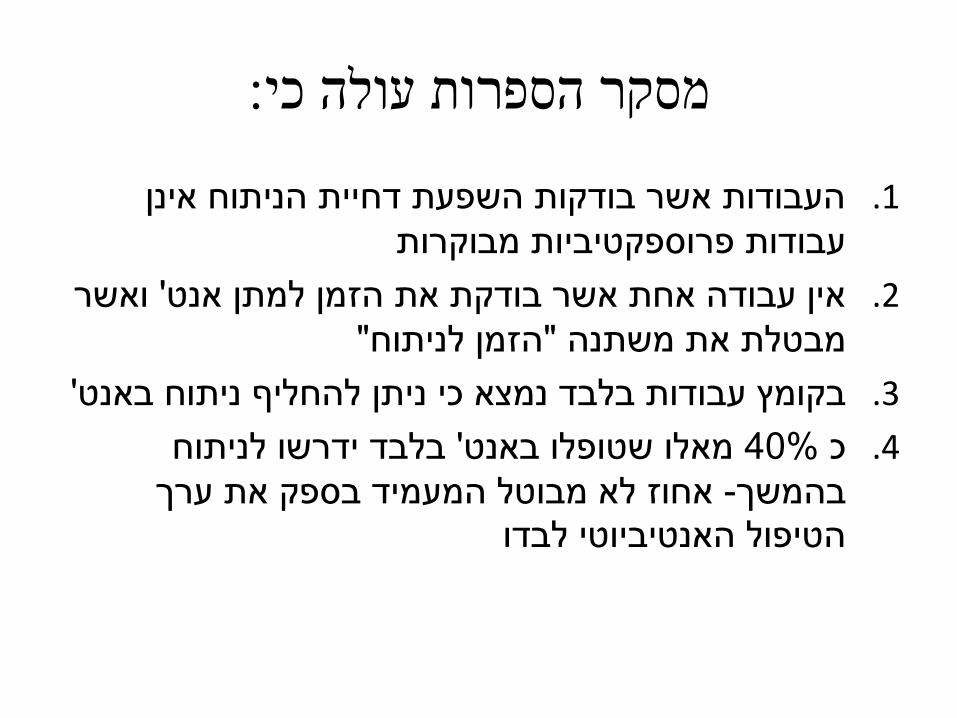
טטיאנה דורפמן דר
תזמון הניתוח בדלקת חריפה של כיס
שינוי בפרדיגמה -המרה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Statistics
bull 90 of Acute Cholecystitis ndash gallstones
bull AC is the admission diagnosis in 11- 50 of patients subjected to cholecystectomy
bull In 27- 51 of patients AC can progress to serious complications such as gallbladder empyema gangrene perforation or pericholecystic abscess
bull Elderly diabetics obese patients debilitated patients increased incidence of gallstones
bull Aging is the most significant factor higher incidence of AC
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Management of Acute Cholecystitis
bull Supportive care with IVFs bowel rest amp Abx
bull Almost half of patients have positive bile cultures
bull E Coli is most common organism
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Clinical Questions
bull What is the best therapy for Acute Cholecystitis conservative or surgical
bull Which surgical procedure should be adopted for Acute Cholecystitis laparoscopic Cholecystectomy or open Cholecystectomy
bull When is the optimal time for Cholecystectomy in Acute Cholecystitis
When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

When is the optimal time for Cholecystectomy in Acute
Cholecystitis
Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Early Vs Delayed Surgery for Acute Cholecystitis
Lahtinen J et al
bull 100 patients with AC were randomly divided into 2 groups
bull Early surgery in the treatment of acute cholecystitis is recommended
bull The complications of failed medical treatment can be avoided by early operation without added risk of mortality or complications
Scand J Gastroenterol 1978
DS ( 2--3 m after the as) ES (7 days after the onset of as )
980 +- 73 min 767 +- 46 min Operative time
8 pts 2 pts Wound infection
2 pts 0 Mortality
24 Recurrence
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Early vs Delayed Surgery for Acute Cholecystitis
Jaumlrvinen HJ et al
bull 130 patients with AC were randomly divided into 2 groups
Conclusion bull Early surgery is preferable when performed by an experienced surgeon
bull Besides lower costs it offers the advantage of avoiding recurrent attacks and emergency operations without increasing mortality or morbidity
Ann Surg 1980
DS n=50 ES n=80
182 plusmn86 107 plusmn49 Hospital Stay (days)
173 138 Postoperative morbidity
15 Recurrence
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
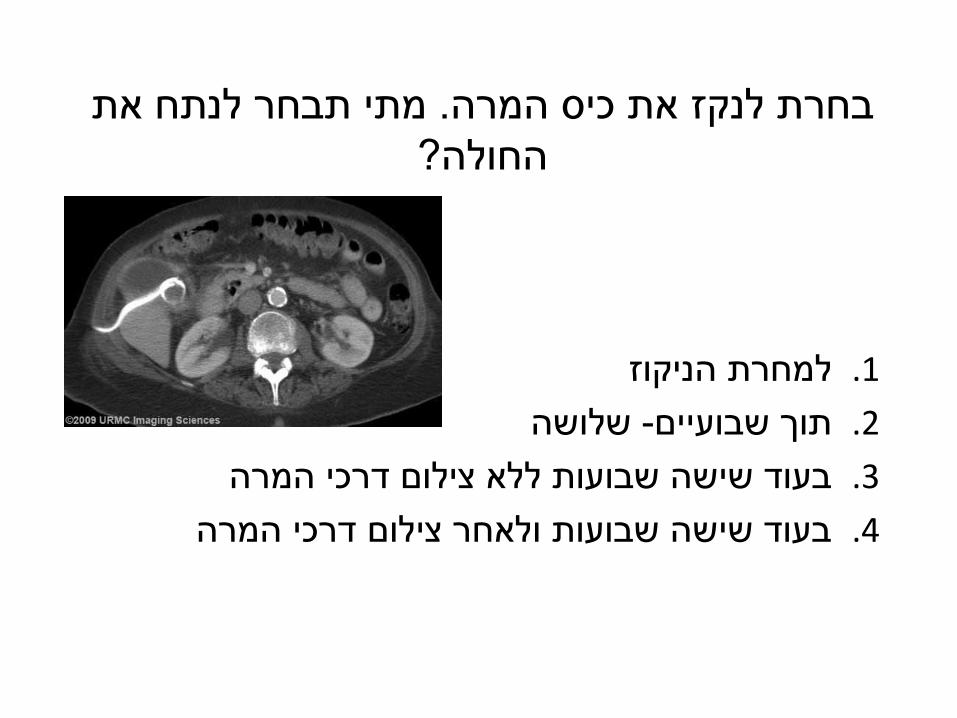
Koo KP et al
Retrospective study January 1993 and February 1995
bull 60 pts with Acute Cholecystitis confirmed by clinical laboratory operative and histopathological findings
bull 3 groups based on timing of surgery
Group 1 LC within 72 hours of onset of symptoms
Group 2 LC between 4th and 7th day of symptom onset
Group 3 LC after 7 days of symptoms
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Koo KP et al
ConclusionsConclusions
bull Duration of symptoms prior to LC affected the outcome bull Group 1 (within 72 hours of onset of symptoms)
lower conversion rate shorter and less costly operations shorter convalescent rates
bull Interval cholecystectomy may be a superior option in patients
presenting after 72 hr of onset of symptoms
Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Lo CM Liu CL Fan ST Lai EC Wong J
Prospective study
March 1991 - July 1994
497 patients underwent LC in the Department of Surgery the University of Hong Kong at Queen Mary Hospital
bull 52 (105) had a clinical diagnosis of acute Cholecystitis confirmed by ultrasonography
o Early -27 pts had surgery within 120 hrs ( 5days) of admission
o Delayed -25 pts were treated conservatively discharged and readmitted for surgery after an interval of 1104 plusmn 680 days (3-6 mo)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Lo CM Liu CL Fan ST Lai EC Wong J
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Lo CM Liu CL Fan ST Lai EC Wong J
Successful LCSuccessful LC
Conclusion
Both early and delayed laparoscopic cholecystectomies performed by experienced surgeons are safe and effective for the treatment of acute Cholecystitis
Early surgery is technically demanding and time consuming and involves a longer postoperative hospital stay
However its economic advantage is a markedly reduced total hospital stay
p n=20 Delayed (25)
Early n=25 (27)
lt005 980 1372 Operative time (min)
lt0005 25 36 Postop hospital stay (d)
lt0001 124 64 Total hospital stay (d)
Ann Surg 1996
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Lo CM Liu CL Fan ST Lai EC Wong J
bull Prospective randomized study during 26-month period
bull 99 pts w AC (13 pts were excluded)- 86 pts
bull Early (45) = LC within 72 hrs of admission
bull Delayed (41) = LC 8-12 weeks after resolution of acute attack
bull 8 (20) of 41 patients in the delayed group underwent urgent operation at a median of 63 hrs
bull All laparoscopic Cholecystectomies were carried out by either one of the first two authors (CML and CLL) with the assistance of a resident
bull Each surgeon had previous experience with more than 300 laparoscopic cholecystectomies including early or delayed surgery for patients with acute Cholecystitis
p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

p Dilate n=41 Earle n=45
2(1-7) 2(1-7) Duration of acute symptoms (days)
0174 23 11 Conversion rate
0022 105(50-290) 135(75-220) Operative time (min)
007 29 13 Morbidity
lt0001 11(5-33) 6(2-16) Total hospital stay (d)
lt0001 19(5-59) 12(3-30) Total recuperation period (d)
0017 26(11-59) 15(7-30) Duration of loss of working capacity (d)
Conclusion Initial conservative treatment followed by delayed interval surgery cannot reduce the
morbidity and conversion rate of laparoscopic cholecystectomy for AC
Early operation within 72 hours of admission has both medical and socioeconomic benefits
Early operation is the preferred approach for patients managed by surgeons with
adequate experience in laparoscopic cholecystectomy
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Chandler CF et al Objective To compare the safety and cost effectiveness of early versus delayed
LC in AC 43 patients presenting with AC were prospectively randomized to early
versus delayed LC during their first admission 21 21 pts ELCpts ELC pts underwent LC as soon as the operating schedule allowed
23 23 pts DLCpts DLC pts received anti-inflammatory medication in addition to bowel rest and
antibiotics and underwent operation after resolution of symptoms or within 5 days if symptoms failed to resolve
Am Surg 2000
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Complication ELC = DLC p
Operative time ELC
lt DLC
ns
Conversion rate ELC
lt DLC
ns
Blood loss ELC
lt DLC
lt005
Total hospital stay ELC
lt DLC
lt005
Hospital charges ELC
lt DLC
lt005
Chandler CF et al
Am Surg 2000
Conclusion
bull Delay in operation showed no advantage with regard to operative
time conversion or complication rate
bull Early laparoscopic intervention significantly reduced operative blood
loss hospital days and hospital charges
Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Timing of laparoscopic Cholecystectomy for acute Cholecystitis
George Tzovaras et al
Prospective non randomized study
January 2002 - December 2005
ASA 1-3 patients with AC were treated laparoscopically during the urgent (index) admission
The patients were divided into three groups according to the timing of surgery regarding to onset of symptoms
(1) within the first 3 d
(2) between 4 and 7 d
(3) beyond 7 d
Patients with strong evidence of concomitant common bile duct (CBD) stones were treated initially ERCP
Surgeon (GT) with a special interest in HPB and laparoscopic surgery
Patients were followed for 4 weeks
World J Gastroenterol 2006
George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

George Tzovaras et al
World J Gastroenterol 2006
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
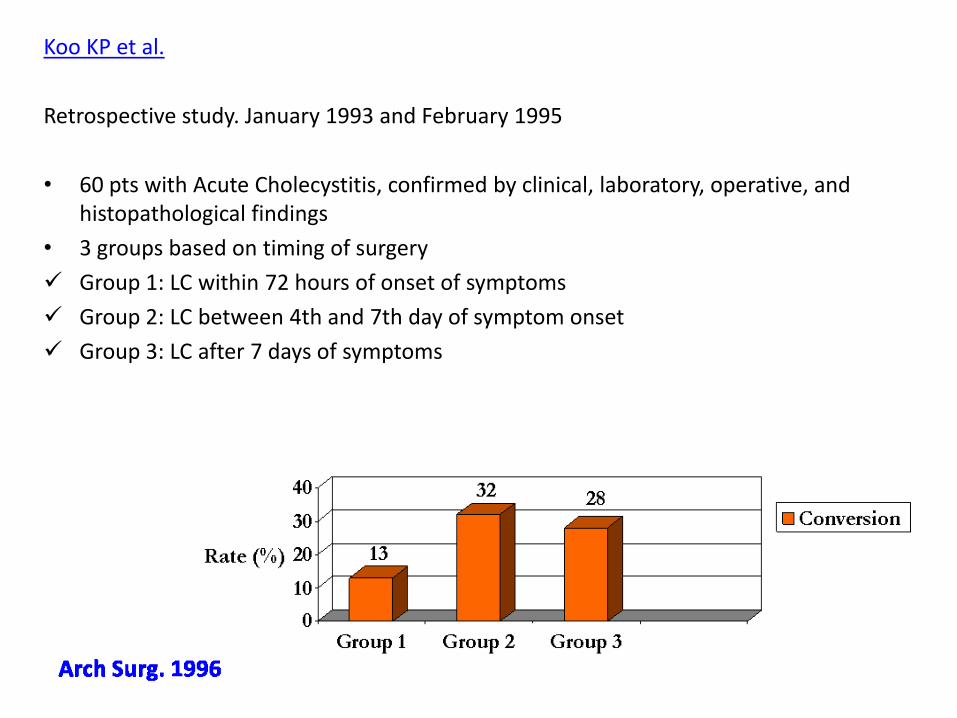
CONCLUSION
bull LC for AC during the index admission is safe and associated with a low morbidity and a low conversion rate not only to those patients who undergo surgical treatment very early but also to those treated after the window of the first 3 or 7 days from the onset of symptoms
bull It appears reasonable to state that in units with expertise in laparoscopic surgery every effort should be made to operate on all patients with AC during the index admission as soon as diagnosis is made and co-morbidities are dealt with regardless of the time delay from the onset of symptoms
bull This policy is safe not associated with a higher conversion rate or morbidity and results in an overall shorter hospitalization by avoiding re-admissions
World J Gastroenterol 2006
George Tzovaras et al
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Timing of Early Laparoscopic Cholecystectomy for Acute Cholecystitis
Al-Mulhim AA
To compare the outcome of LC performed within and after 72 hours of admission in patients with Acute Cholecystitis
January 2001 - December 2006 LC was performed in 196 pts with AC 82 pts (group 1) within 72 hours of admission in 114 patients (group 2) after 72 hours Data were collected prospectively LC was performed in both groups by 5 surgeons with similar distribution of early
and delayed LCs Patients were followed up for 6 weeks and were discharged home unless they
had postoperative complications
JSLS 2008
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Al-Mulhim AA
Conclusion
bull Early LC can be performed safely in most patients with acute cholecystitis
bull They recommend intervention within 72 hours of admission to minimize the complication rate and shorten the operation time and total hospital stay
JSLS 2008
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
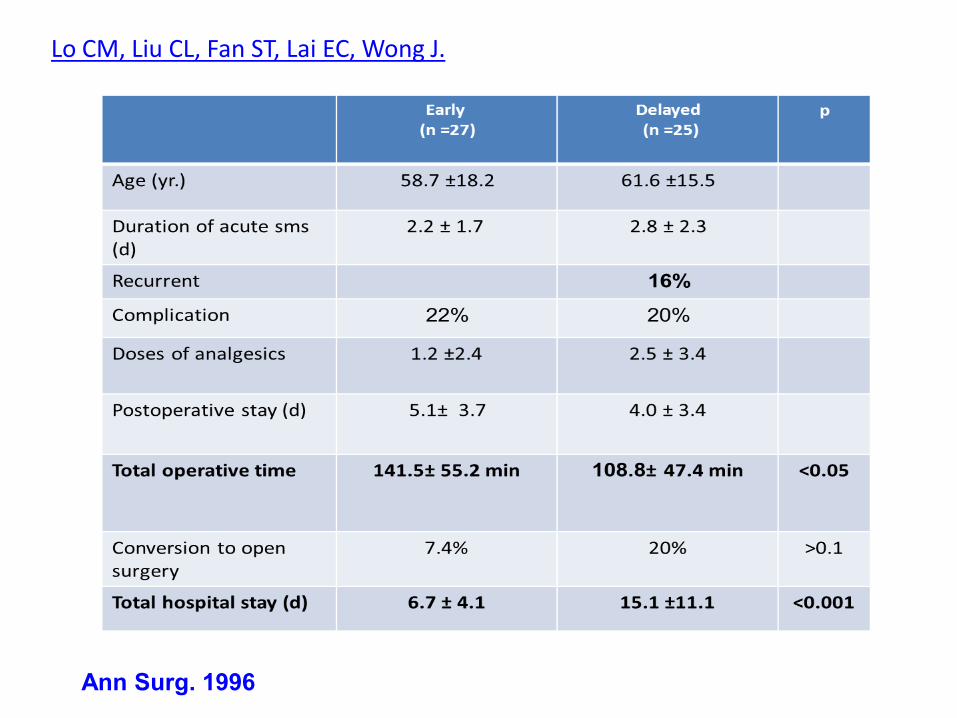
Evaluation of early versus delayed laparoscopic Cholecystectomy in the treatment of acute Cholecystitis
Chang TC et al
January 2004 and January 2006 Retrospective study
CONCLUSIONS
bull Both ELC and DLC appears to be effective and safe in the treatment of AC
bull ELC may be more technically demanding and time-consuming it also tends to shorten the total length of hospital stay and reduce the risk of repeat cholecystitis
bull They recommend early LC for AC
Hepatogastroenterology 2009
ELC n=56 DLC n=33 p
operation time
109 +- 3759 min 77 +- 2565 min lt 0001
blood loss 76ml 28ml 0006
post-operation hospital stay d 45 26 lt 0001
conversion rate 456 233 084
total hospital stay d 453 779 d lt 0001
admission times 1 time 24 times lt 0001
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
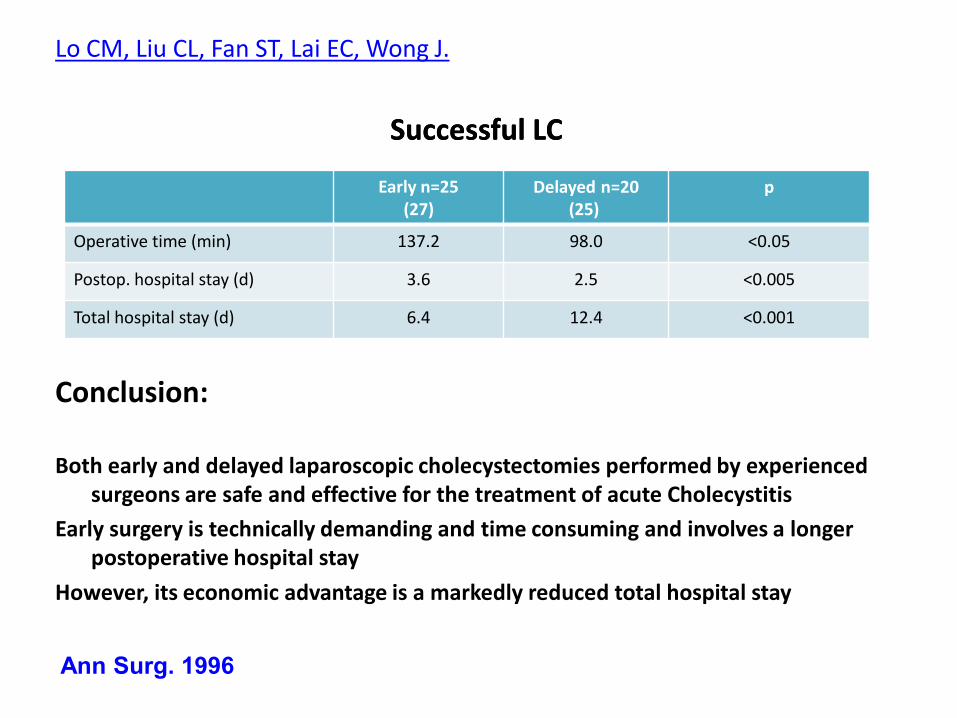
Population-based analysis of 4113 patients with acute Cholecystitis defining the optimal time-point for laparoscopic Cholecystectomy
Banz V et al prospective 1995 ndash 2006 4113 pts with AC Patients were grouped according to the time-points of LC since hospital admission day d0
d1 d2 d3 d45 d ge6 RESULTS Delaying LC resulted in significantly higher conversion rates 279(d ge6) vs 119 (d0) P lt 0001 surgical postoperative complications 13 vs 57 P lt 0001 re-operation rates 3 vs 09 P = 0007 postoperative hospital stay P lt 0001
CONCLUSIONS Delaying LC for acute Cholecystitis has no advantages This investigation-one of the largest in the literature-provides compelling evidence that
acute Cholecystitis merits surgery within 48 hours of hospital admission if impact on the patient and health care system is to minimized system costs
Annals of Surg 2011
bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

bull Randomized and nonrandomized studies have documented the feasibility and safety of early LC for AC in experienced hands
bull Upon diagnosis of AC most patients should be scheduled for cholecystectomy
bull EC allows for the disease process to be halted before progression of the inflammatory process to necrosis gangrene perforation and abscess
bull Exception to the recommendation for prompt (same admission) cholecystectomy include critically ill patients and parents with significant hemodynamic instability
bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

bull Initial medical treatment for AC followed by delayed LC is associated with several shortcomings
20 to 26 of patients fail to respond to conservative treatment or develop early complications during the first admission and require an urgent and technically demanding cholecystectomy
15 to 30 of patients are readmitted with recurrent symptoms and undergo an unplanned emergency cholecystectomy while waiting for their scheduled elective procedure
22 of patients are lost during the interval period
Cholecystectomy is preferable early after admission
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
מה נציעלנתח חולים הלוקים בדלקת כיס המרה עם ראוי וניתן 1
התקבלותם
את השיטה לנתח חולים שכאלה ביום כדאי למצוא 2
הניתוחים האלקטיבי הבא ולחסוך בהוצאות ובאשפוזים
ייטב -ככול שנקדים3
כיס המרה את ניקוז 4
לחולים המורכבים נשמור
ביותר
IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

IIIמקרה
70גבר בן bull
שנה 20ניתוח לכריתת כיס המרה לפני -ברקעbull
באופן פתוח
בכול פעם -אשפוזים חוזרים בשל חסימת מעי דקbull
טיפול שמרני
כאבי בטן מזה יומיים כאבי בטן וביום התקבלותוbull
עזים מלווים בהקאות וחוסר מעבר גאזים
IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

IIIמקרה
חום מדדים המודינמיים תקינים נינוח -בבדיקהbull
הגוף תקין
ניע ער ומתכתי טמפנית הבטן תפוחהbull
הבטן רגישות קלה עפbull
ללא צואה -בדיקה רקטאליתbull
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
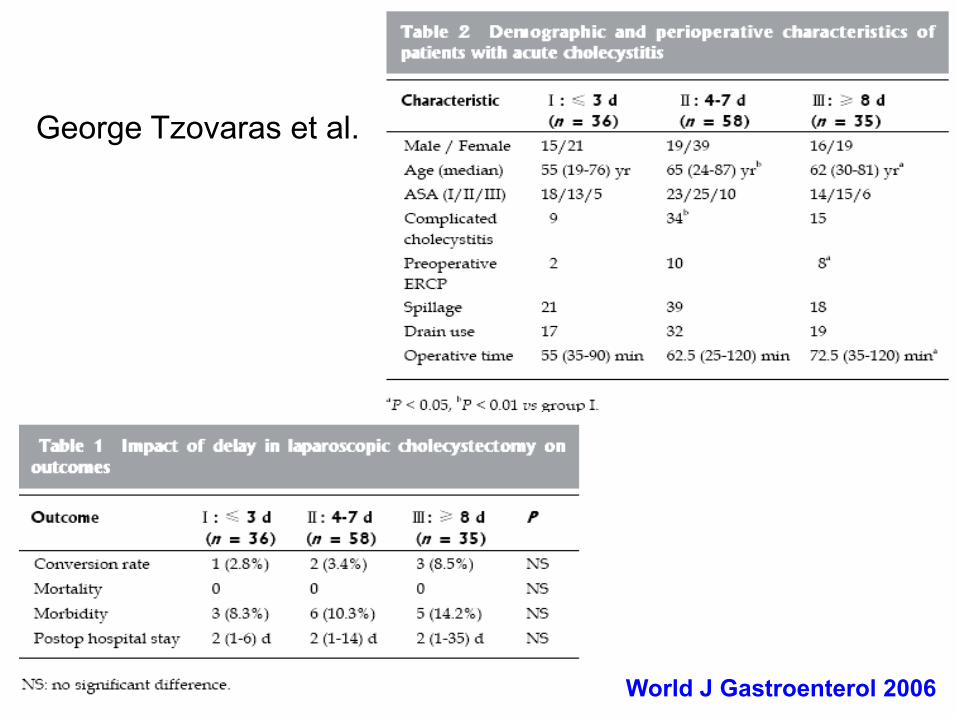
שאלה
לאור ממצאי הבדיקה והצילום אחליט על השלבים הבאים
בטיפול
הגיע החולה לוקה בחסימות חוזרות -ניתוח מידי1
הזמן לשים סוף לדבר
מתן נוזלים והשגחה ניטור השתן הכנסת זונדה2
מתן נוזלים ניטור השתן הכנסת זונדה3
וטומוגרפיה
מתן גסטרוגרפין במיון ומעקב צילומי בטן4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
(קסמ 3000)הפרשה מרובה בזונדה חולה יציב1
החולה אינו מעביר פעולת מעיים מזה שלושה 2
ימים
החולה סובל מכאבי בטן למחרת התקבלותו 3
לאופיאטיםונצרך
כול התשובות נכונות4
שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

שאלה
באיזה מהתנאים הבאים תחליט לנתח את החולה
בטומוגרפיה עדות למעבר קוטר ואין מעבר חומר 1
הניגוד
החולה במחלקה שלושה ימים ואינו משתפר כלל 2
אך גם אינו מחמיר
או צילומי בטן עוקבים אינם מראים התקדמות ו3
שיפור
כול התשובות נכונות 4
שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

שאלות לצוות
בחולה הלוקה בחסימת מעי דק על רקע הדבקויות bull
לאחר כמה ימים תחליטו לנתחו -וללא סימני סבל
ובאיזה תנאים קליניים
מתי תתזמנו מתן גסטרוגרפין לחולה הלוקה bull
בחסימת מעי דק על רקע הדבקויות הנבדק במיון
לאיזה חולה תבחרו בטומוגרפיה ככלי אבחנתיbull
מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

מחלה שכיחה שאינה פשוטה -חסימת המעי
הדעות אינן אחידותbull
-המשתניםbull
מצב החולה
מידת החסימה
גורמי סיכון לחסימה מלאה או כזו שלא תחלים
מודעות
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
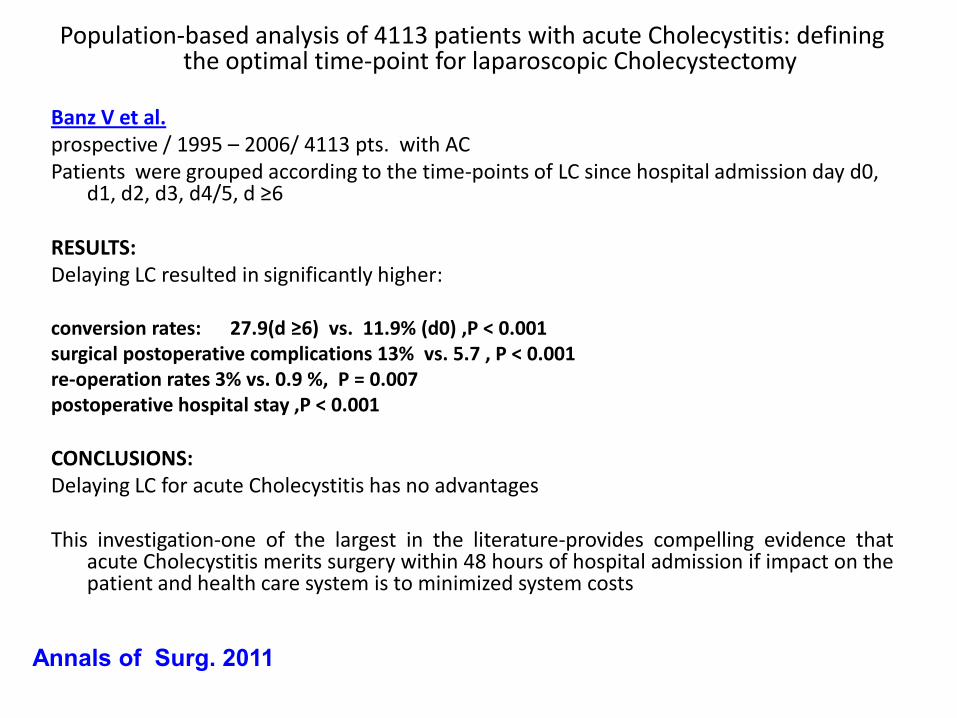
שחר גרונר דר
תזמון הניתוח בחסימת מעי דק על רקע
שינוי בפרדיגמה -הדבקויות
Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Small bowel obstruction
In contrast to few decades ago
Causes of SBO
-Adhesions 49-67
-Neoplasm 13-162
-Hernia 5-6
12-17 suffer SBO in the initial 2 years
after abdominal operation
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Predicting Strangulation
bull Any patient with bowel ischemia needs urgent operation
bull Incidence of strangulation differs with etiology
-28 in hernia
-8 in adhesions
-4 in neoplasm
Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Non Operative Treatment
bull Patients with signs of strangulation or perforation fever tachycardia diffuse peritonitis- operation
bull No single sign symptom or laboratory indices can predict strangulation
bull Senior surgeon physical examination
48 sensitivity in predicting strangulation
83 specificity in predicting strangulation
bull In case of non operative treatment close observation is mandatory
Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Laboratory values in SBO
bull Difference of WBC count in patients who were operated
Vs patient who were not operated was about 2000mm3
Normal WBC doesnt ldquorule outrdquo strangulationNormal WBC doesnt ldquorule outrdquo strangulation
bullLactate was abnormal
in 86 of patients with strangulation
in 4 of patients with simple SBO
bullAmylase
elevated in 55 of patients with strangulation
elevated in 5 of patients with non strangulated
obstruction
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Decrease in Mortality
bull Less hernia as cause for SBO
bull Better ICU care
Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Decrease in mortality- adhesions
Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Complete Vs Partial SBO
bull Is completecomplete obstructionobstruction an indication for operation
bull How to define complete obstructioncomplete obstruction
In early obstruction the patient still passes gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Complete Vs Partial SBO
bull Is complete obstruction an indication for operation
bull How to define complete obstruction
In early obstruction the patient may pass gas and stool
PR by itself introduces gas into the rectum
Abdominal X ray normal in 8-17 of strangulated SBO
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Complete Vs Partial SBO
bull Sarr et al
297 patients
complete and partial SBO
treated non operatively
No significant difference in rate of bowel strangulation
surgery morbidity or mortality
bull Borlin et al
342 patients
All patients with complete SBO underwent operation
Only 19 of patients with partial SBO underwent
operation
Difference insert of etiology
Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Upper GI radiographic studies
bullChung at al
51 patients with SBO
Gastrographin was given and abdominal X rayrsquos were done after 4 hours
ldquosignificant obstructionrdquo- If contrast failed to reach the Cecum
Surgeon ldquoblindedrdquo to the study
1719 that underwent operation had ldquosignificant obstructionrdquo
132 with no ldquosignificant obstructionrdquo underwent operation
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Water-soluble contrast study facilitate non operative management
Abbas et ak 2007
Water-soluble contrast administration does not
improve resolution of SBO but it may shorten
hospital stay in patients managed non-operatively
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

ldquoSpecial casesrdquo
bull Post- Laparotomy SBO Vs Post- Laparoscopic SBO
bull Malignant SBO
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
SBO in the malignant patient
bull Patients with SBO secondary to malignancy may tolerate
a longer period of non-operative treatment
Timing of reoperation donrsquot correlate with postoperative
complications
Low incidence of bowel ischemia (4)
Relatively high incidence of in-hospital mortality (21-
28)
With known recurrence- extended period of non-
operative treatment is acceptable due to
1 low incidence of strangulation
2 high surgical mortality
Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Early post- Laparotomy SBO
bull Causes adhesions internal hernia volvolus
edematous anastomosis abscess
Low incidence of bowel strangulation
Recommendation 10-14 days of non-operative
treatment
Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Early post Laprascopic SBO
bull Post laparoscopic SBO less common due to darrdarr adhesions
Hernia in port site calls for early intervention
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
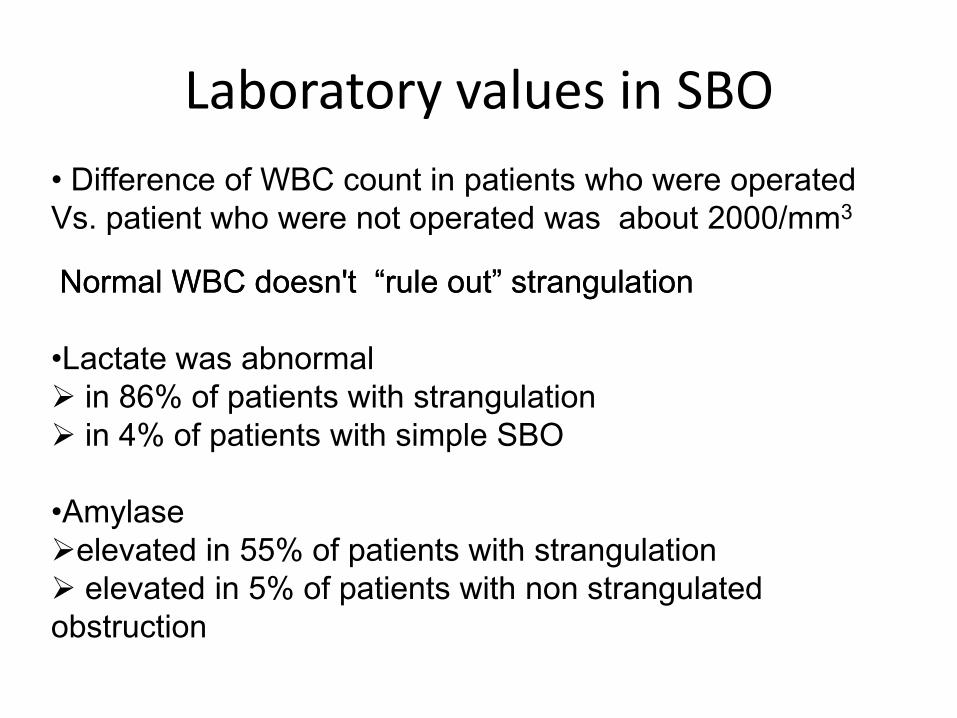
Duration of non operative management or- timing of operationtiming of operation
bull No prospective randomized trials
bull Only few retrospective studies pointed that 48 h is
a reasonable time limit (under close observation)
bull Other studies pointed that observation longer than
5 days doesnt increase rate of resolution
מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

מה נציע בחסימת מעיים הוא עניין למקצועניםתזמון ניתוח 1
לאיסכמיה ניתן לטפל באופן שמרני בניטור קפדני ללא עדות 2
שעות עד להחלטה על הצעד הבא 48סבל ניתן להמתין ללא סימני 3
צילום בטן לאחר ארבע שעות מבליעת חומר ניגוד יכול לשמש מדד למי מתאפשר 4
המשך טיפול שמרני
בחולה האונקולוגי ובחולים הלוקים בחסימה לאחר חקירת בטן פתוחה ניתן 5
להשהות התערבות ניתוחית
ימים 10-14עד
בחולה החסום לאחר לפרוסקופיה6
יש להתערב בשל השכיחות לבקע
במקום הטרוקר
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
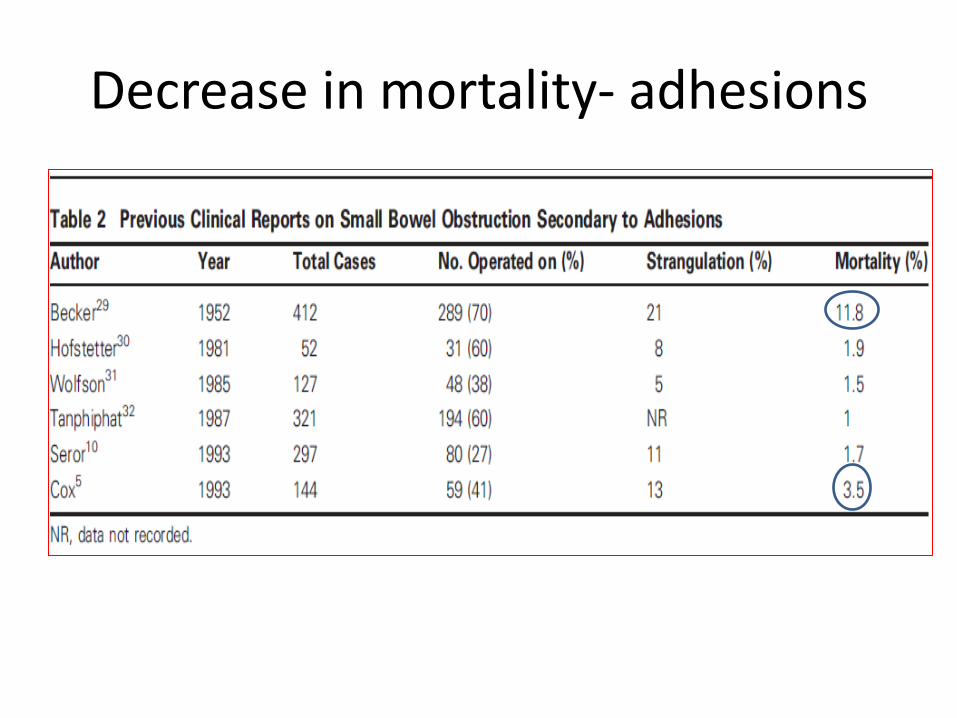
סיכום
תישאר כאן לנצח באישון הלילה כירורגיה דחופהbull
מקצת מהמחלות אשר נדרשו בעבר לניתוחים דחופים bull
בלילה מאפשרות דחיית הניתוח לשעות נוחות למנתח
ולצוות בלא להחמיר את המחלה או מצבו של החולה
ראוי כי הכירורג ינקוט מידה הגונה של שיקול דעת bull
אך גם בניתוח בהול בשעות הקטנות בדחיית ניתוחים
של הלילה
ראוי כי קברניטי המערכת ישכילו להקים מערכות bull
המסוגלות לתת מענה בזמן סביר לניתוחים דחופים (IN TIMELY MANNER )
לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

לגבי התוספתן
במקרים פשוטים ניתן לדחות את הניתוח לבוקרbull
במקרים מורכבים עם עדות להתנקבות יש לבצע bull
את הניתוח בדחיפות
ניתוח ולא טיפול אנטיביוטי -למרות המאמריםbull
לבדו הוא הטיפול המועדף בשל הישנות ניכרת של
דלקת התוספתן
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
לגבי כיס המרה
בטוח לנתח חולים הלוקים בדלקת של כיס המרה עם bull
התקבלותם
ניתן לדחות את הניתוח ליום הניתוחים האלקטיבי הבא bull
במידה והמערכת מאפשרת זאת
חולים שלקו בפנקראטיטיס קלה בטוח לנתח במסגרת bull
האשפוז הראשון ולחסוך לחלקם דלקת לבלב או כיס מרה
עד מועד הניתוח
ולא מורכביםאת ניקוז כיס המרה כדאי לייחד לחולים bull
להשתמש באמצעי זה ככלי טיפולי בכול חולה אשר אינו
מגיב לטיפול האנטיביוטי
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
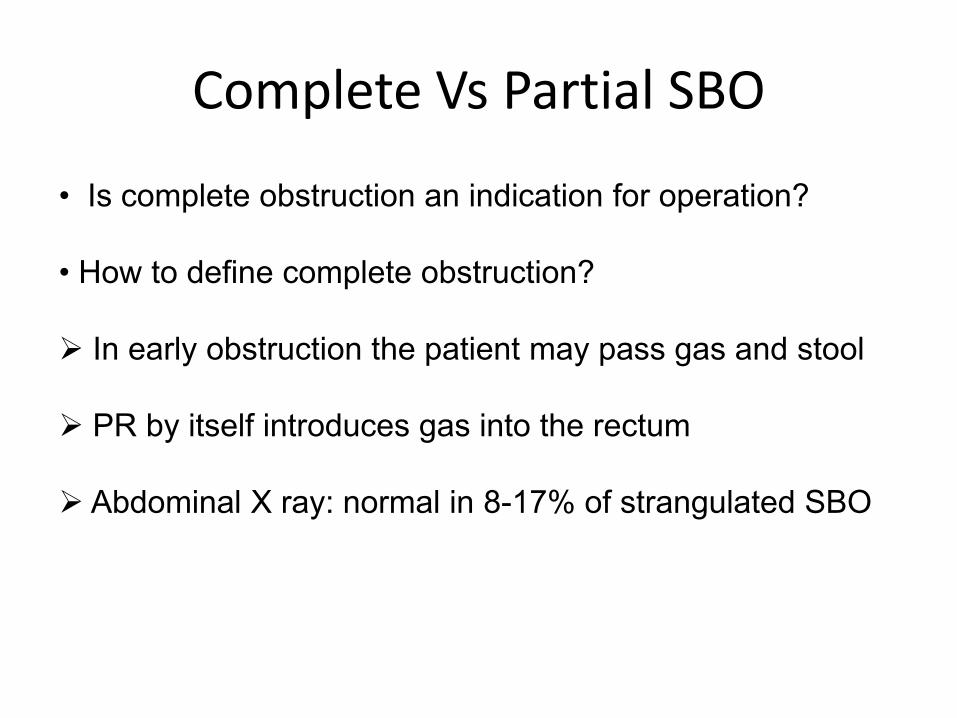
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
לגבי חסימת המעי הדק על רקע הדבקויות
רוב החולים הלוקים בחסימה על רקע הדבקויות יחלימו בטיפול bull
שמרני
-בזונדה או הקאה פקאלית( חיידקים)מסריח פקאלי תוכן רבbull
סימן פרוגנוסטי רע
סימן פרוגנוסטי רע -כאב בטן עוויתיbull
סימן פרוגנוסטי רע -חסימת מעי מלאהbull
סימן פרוגנוסטי רע ndashחסימה ממושכת bull
סימן פרוגנוסטי רע -חוסר התקדמות גסטרוגרפין למעי הגסbull
הקליניקה חשובה -מדדים מעבדתיים אינם מדדים מהימניםbull
Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה

Patients with plain film finding of small bowel obstruction and Clinical markers
(fever leukocytosis tachycardia metabolic acidosis and continuous pain) or
peritonitis on physical exam warrant exploration LEVEL I
Patients without the above mentioned clinical picture and a partial SBO or a
complete SBO can undergo non-operative management safely although
complete obstruction has a higher level of failure LEVEL I
Patients without resolution of the there SBO by day 3-5 of non-operative
management should undergo water soluble study or surgery LEVEL III
Water soluble contrast (Gastrograffin) given in the setting of partial SBO can
improve bowel function (time to BM) decrease length of stay and is both
therapeutic and diagnostic LEVEL II
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
Clinical recommendation Evidence rating Comments Abdominal radiography is an effective
initial examination in patients with suspected intestinal obstruction
C Radiography has greater sensitivity in high-grade obstruction than in partial
obstruction
Computed tomography is warranted when radiography indicates high-grade intestinal obstruction or is inconclusive
C Computed tomography can reliably determine the cause of obstruction and
whether serious complications are present in most patients with high-
grade obstructions
Upper gastrointestinal fluoroscopy with small bowel follow-through can determine the need for surgical
intervention in patients with partial obstruction
C Contrast material that passes into the cecum within four hours of oral
administration is highly predictive of successful nonoperative management
Antibiotics can protect against bacterial translocation and subsequent
bacteremia in patients with intestinal obstruction
C Enteric bacteria have been found in cultures from serosal scrapings and mesenteric lymph node biopsy in
patients requiring surgery
Clinically stable patients can be treated conservatively with bowel rest
intubation and decompression and intravenous fluid resuscitation
A Several randomized controlled trials have shown that surgery can be avoided
with conservative management
Surgery is warranted in patients with intestinal obstruction that does not
resolve within 48 hours after conservative therapy is initiated
B Study found that conservative management beyond 48 hours does not
diminish the need for surgery but increases surgical morbidity
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
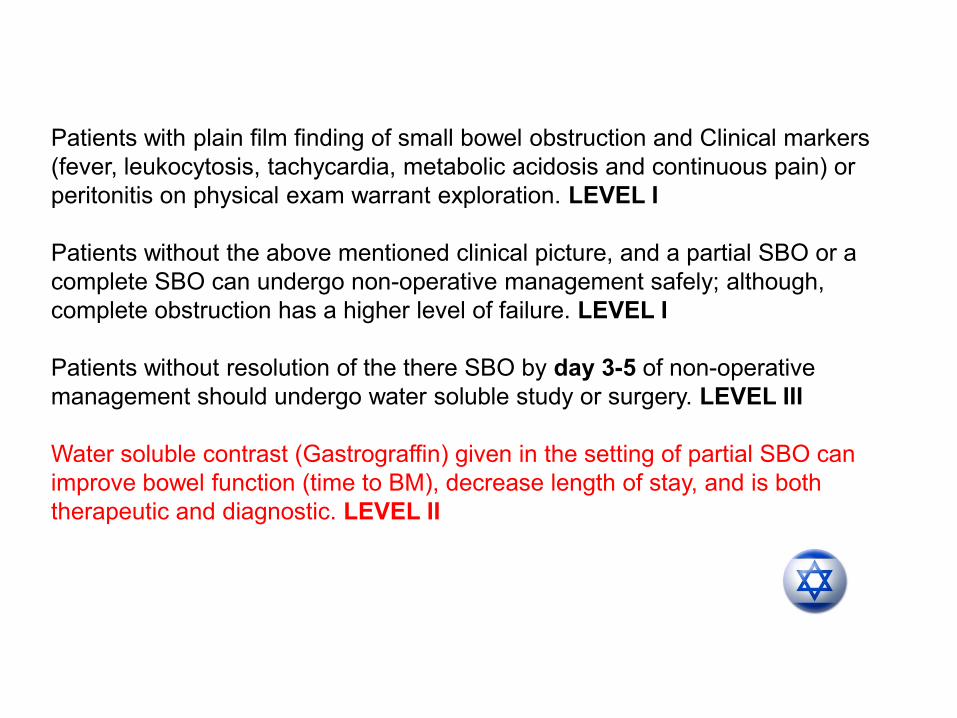
All patients with inconclusive plain films for complete or high grade SBO should
have a CT as CT scan gives incremental information over plain films in regard to
differentiating grade of obstruction and etiology of small bowel obstruction
leading to changes in planned management LEVEL I
Multiple signs on CT suggesting strangulation should suggest a low threshold for
operative intervention LEVEL II
There is a variety of literature that contrast studies should be considered in
patients who fail to improve after 48 hours of conservative management as a
normal contrast study can rule out operative small bowel obstruction LEVEL II
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה
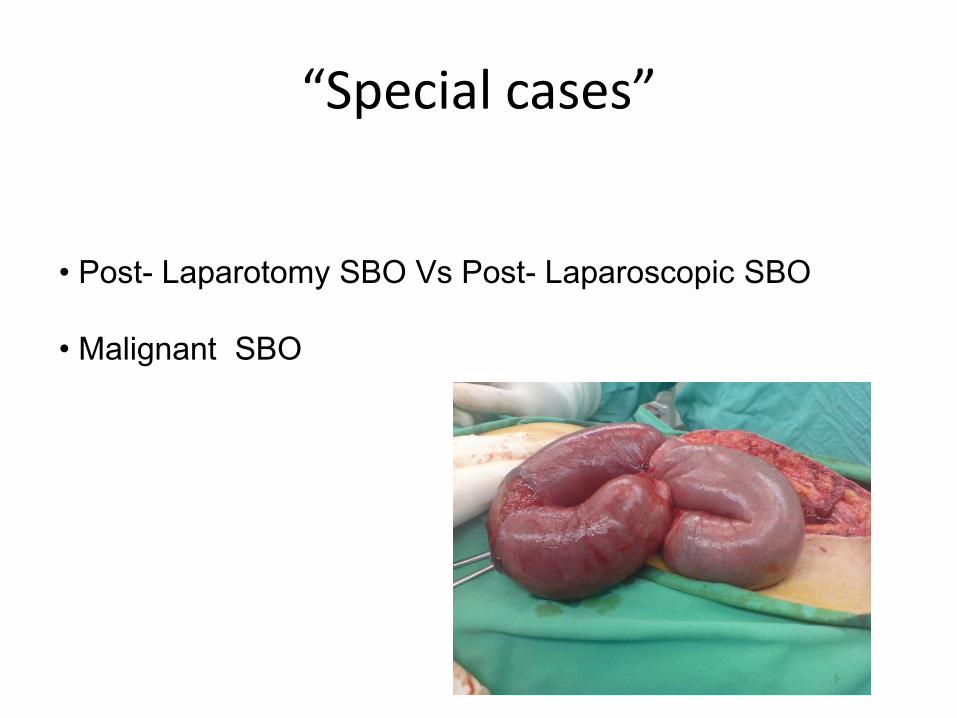
Paradigm shift Donrsquot let the sun rise or the sun set
over bowel obstruction
תודה