Embed Size (px)
DESCRIPTION
頭暈. 新光醫院 神經科 許維志 醫師. Balance and Equilibrium. Equilibrium The ability to maintain orientation of the body and its parts in relation to external space. Interaction between self and environment . Sensory input from visual , vestibular , and proprioceptive information. - PowerPoint PPT Presentation
Citation preview
頭暈頭暈
新光醫院 神經科新光醫院 神經科許維志 醫師
Balance and Equilibrium Equilibrium
The ability to maintain orientation of the body and its parts in relation to external space.
Interaction between self and environment. Sensory input from visual, vestibular, and
proprioceptive information. Integration in the brain stem and cerebell
um.
Disorders of Equilibrium Diseases affect
Central or peripheral vestibular pathways Cerebellum Proprioceptive sensation
Mismatch of input signals and disintegration
Symptoms Vertigo Ataxia
Vertigo and Dizziness Vertigo 眩暈
Illusion of movement of the body or the environment.
Impulsion, oscillopsia, nausea, vomiting, cold sweating, or unsteadiness
Dizziness 頭昏 No association of illusion of movement Light-headedness, faintness, giddiness, swimmi
ng
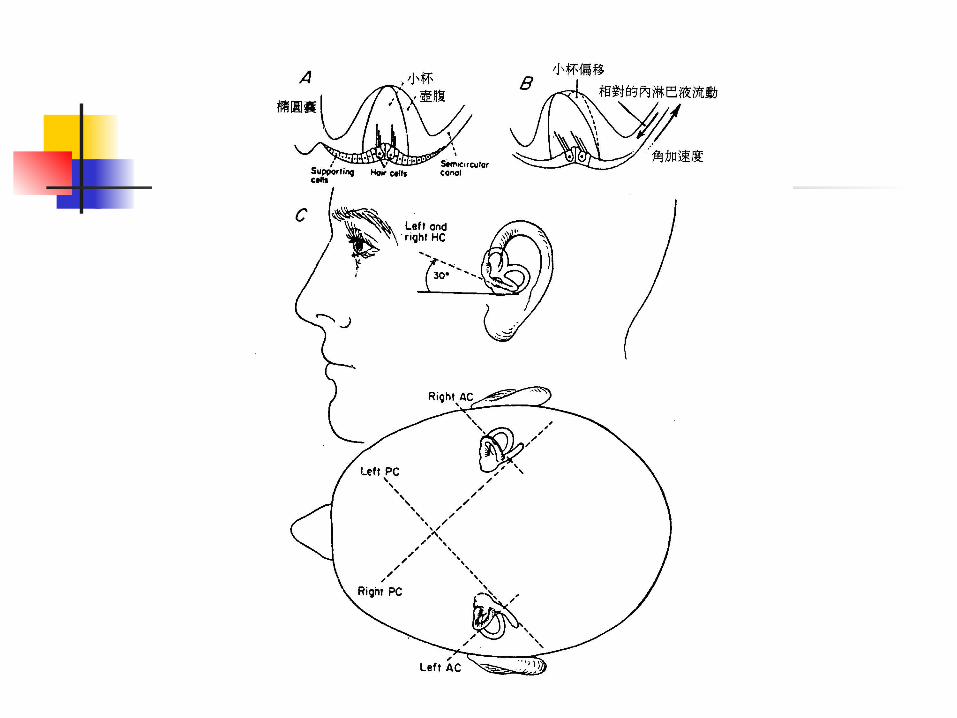
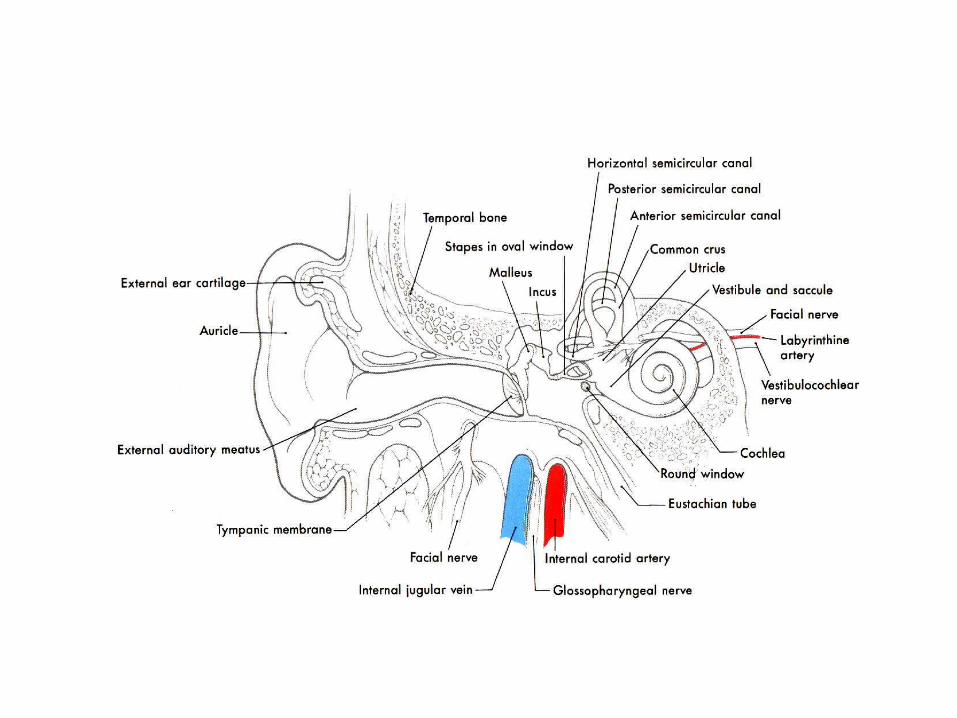
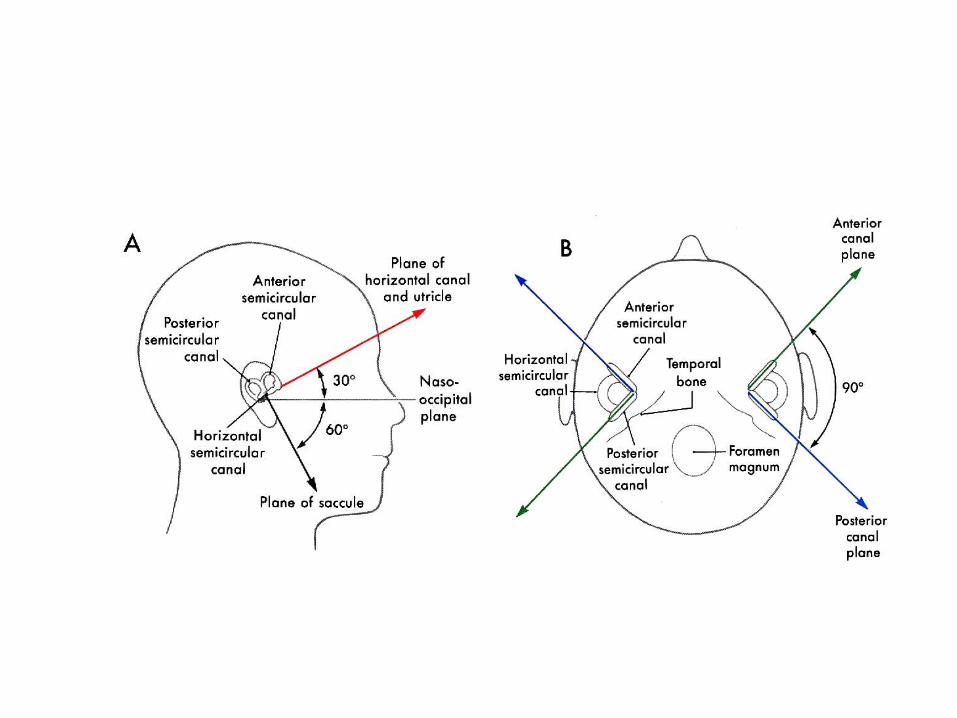
Vestibular System Semicircular canal
Sense angular acceleration Head rotation
Otolith organs Sense linear acceleration Head translation and uprightness
The Vestibules
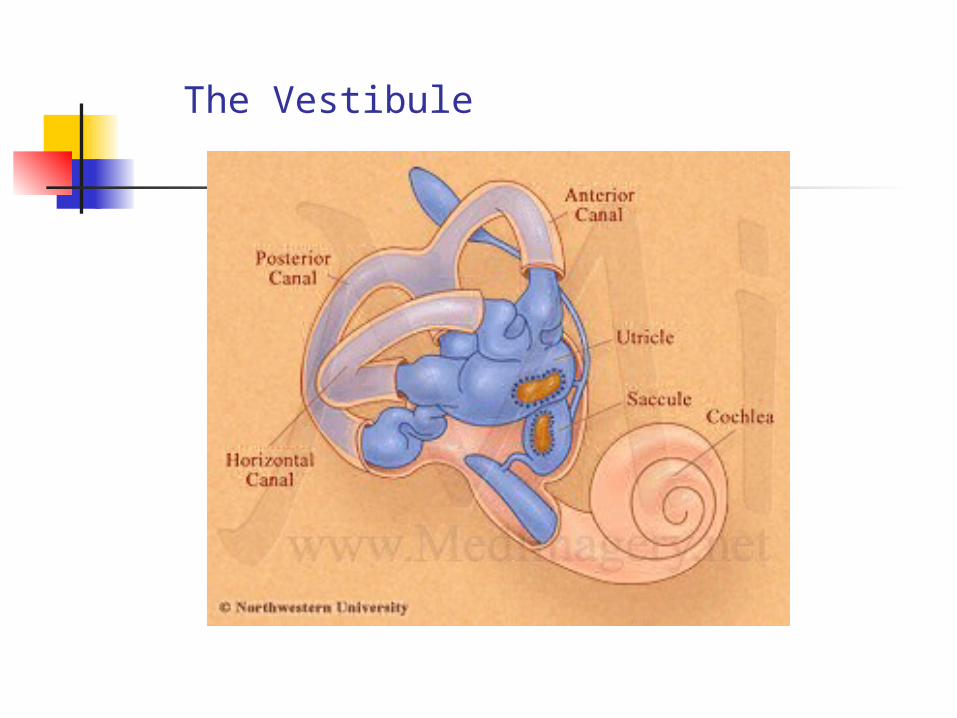
The Vestibule
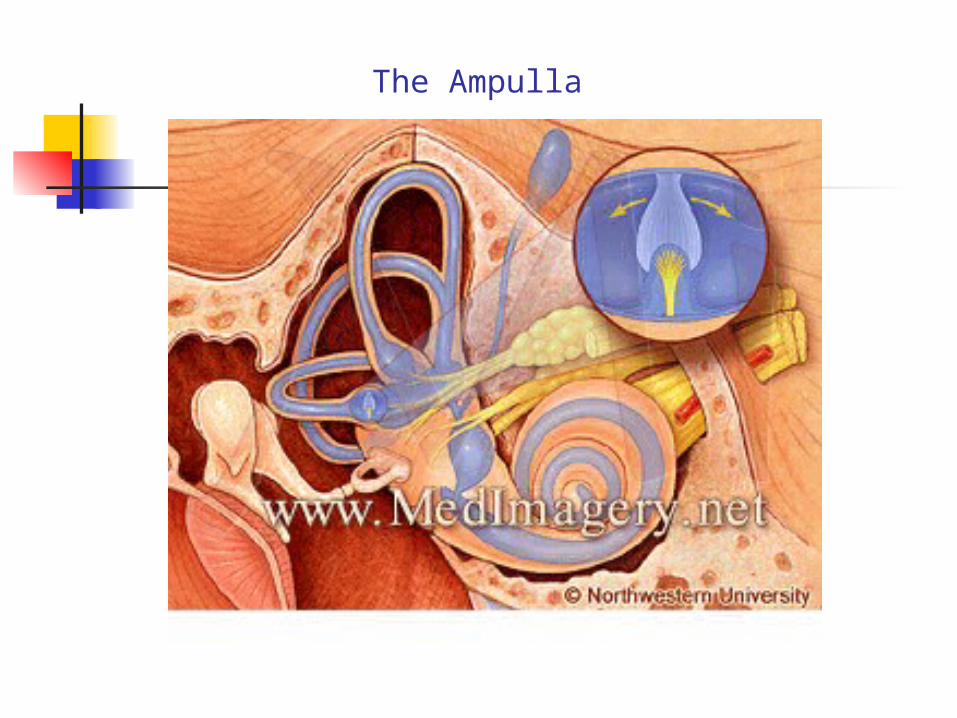
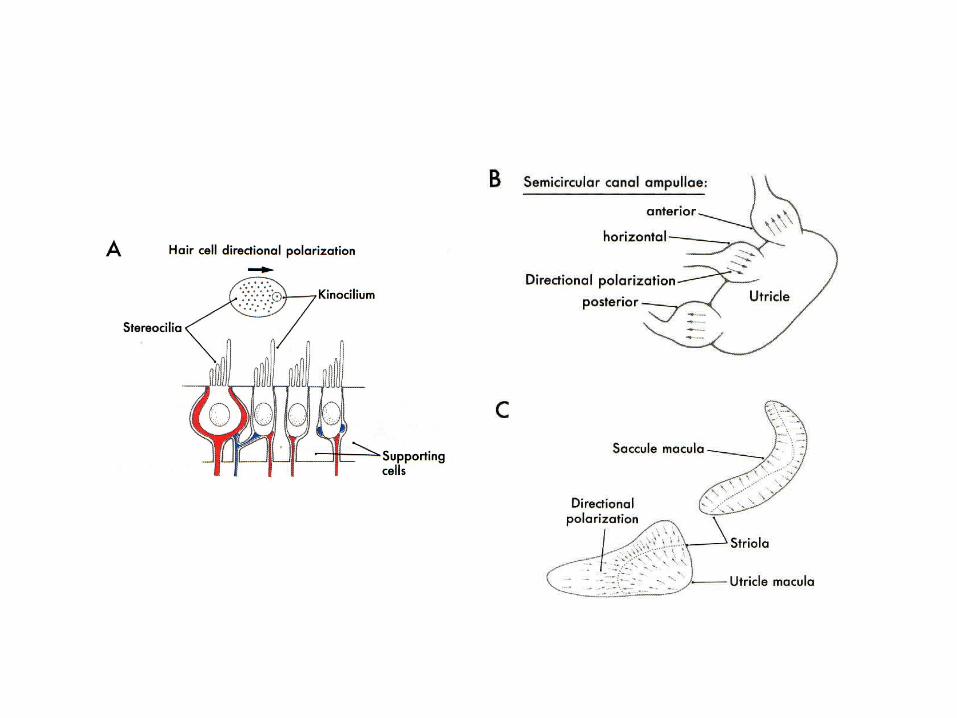
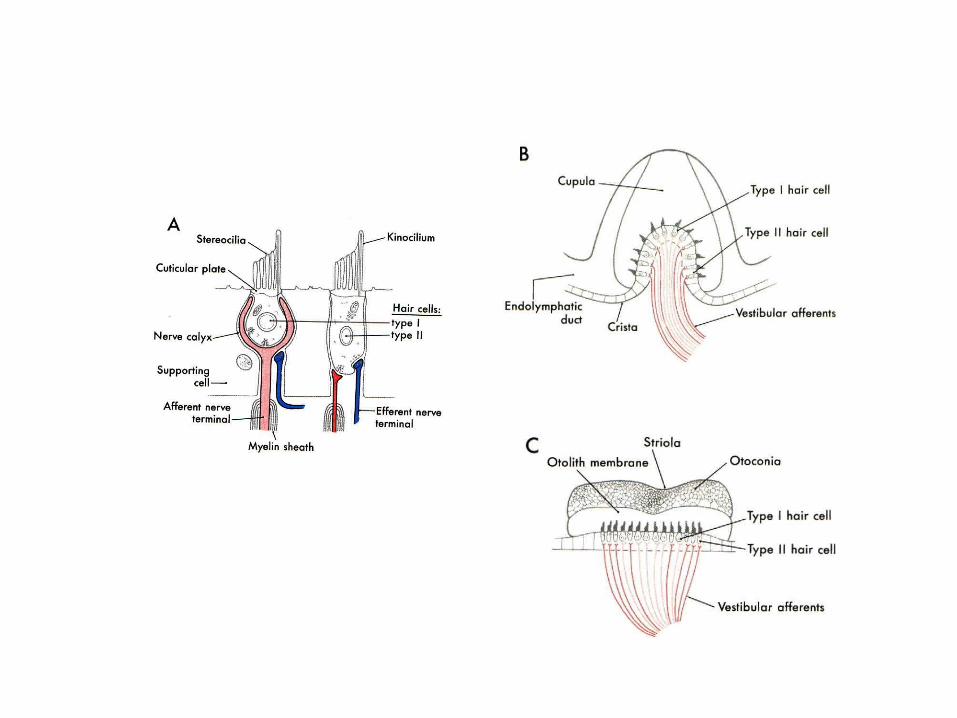
The Ampulla
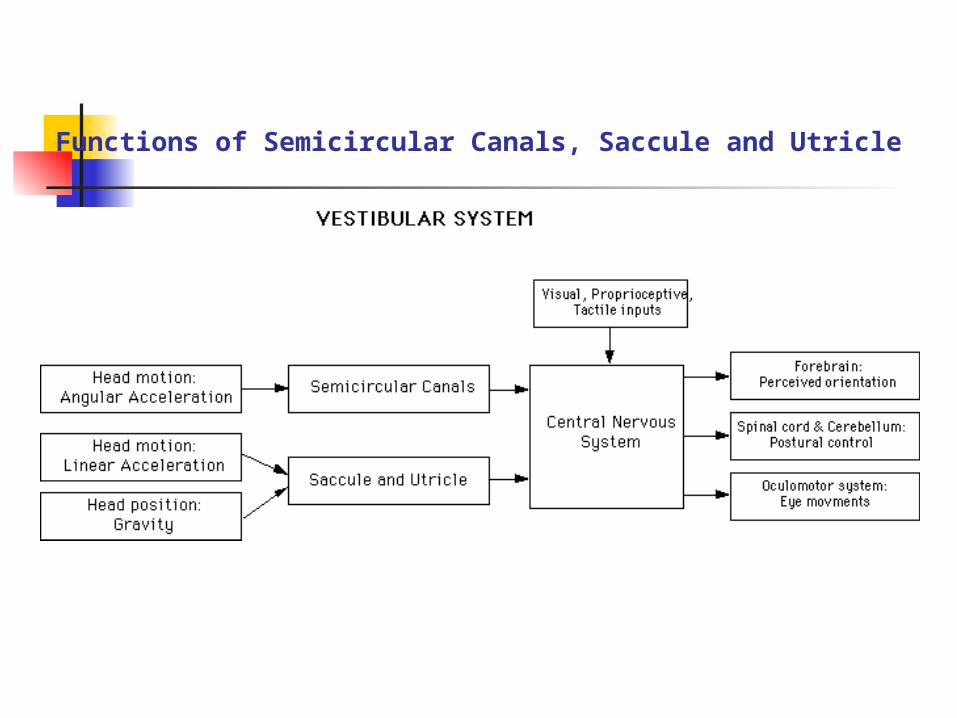
Functions of Semicircular Canals, Saccule and Utricle
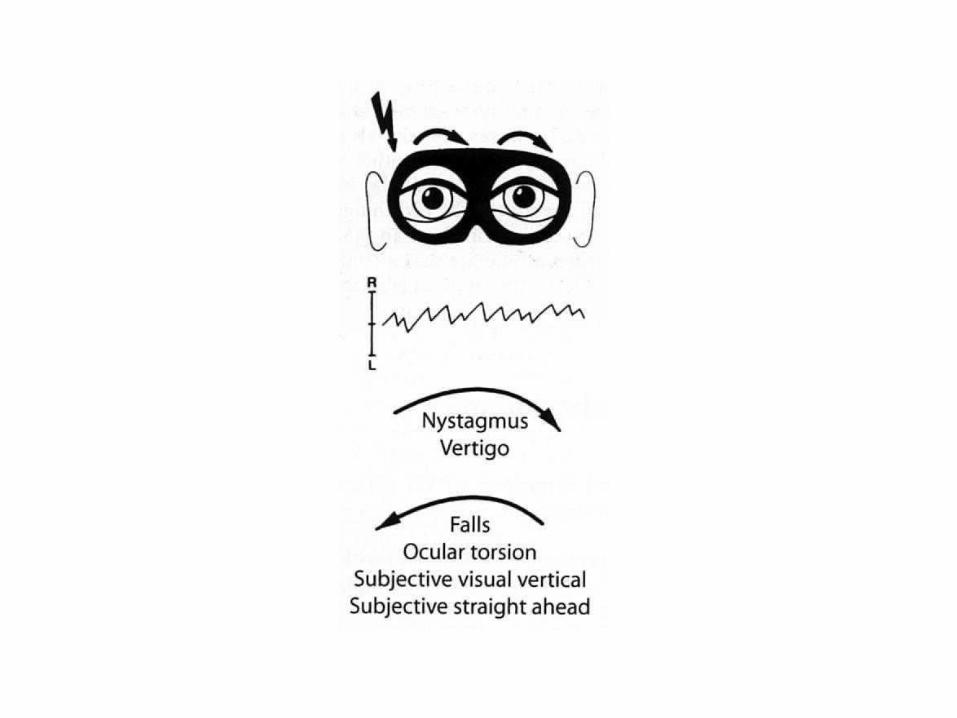
Vertigo
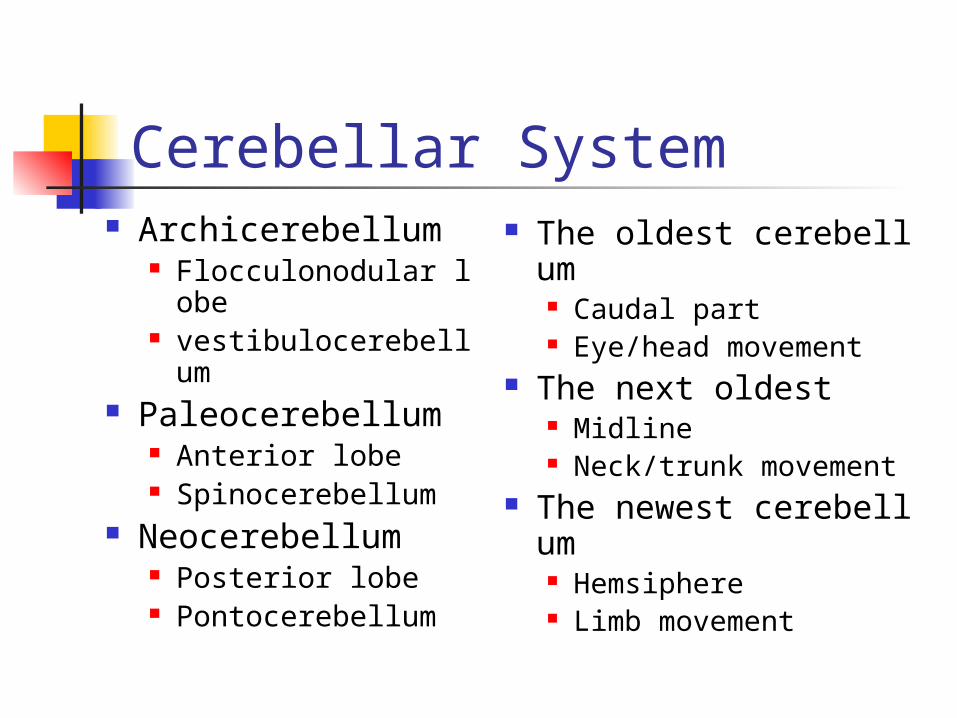
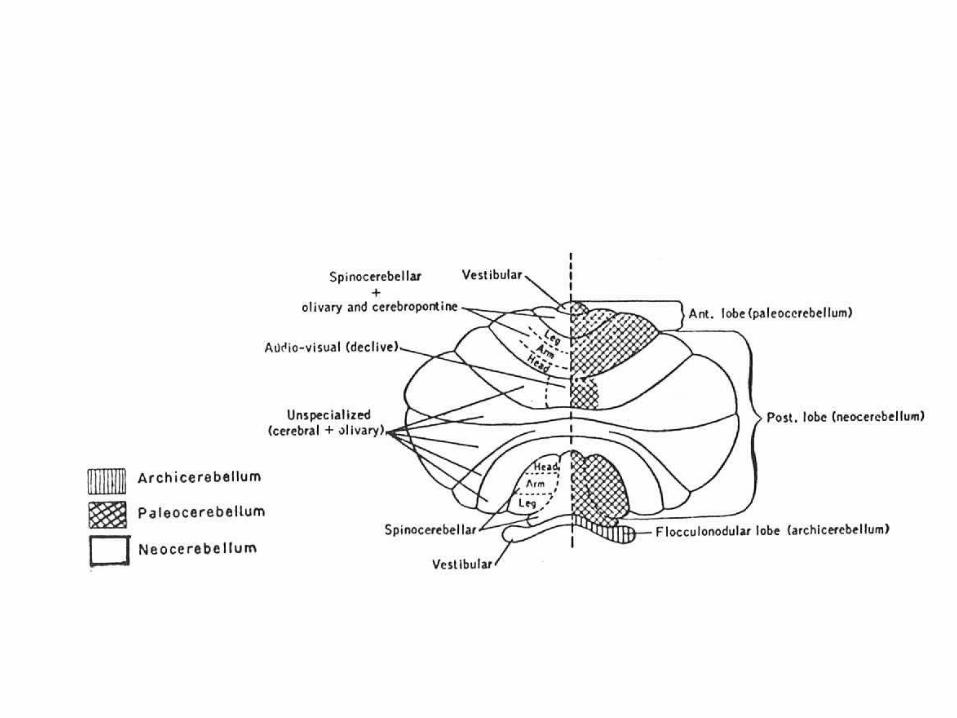
Cerebellar System Archicerebellum
Flocculonodular lobe vestibulocerebellum
Paleocerebellum Anterior lobe Spinocerebellum
Neocerebellum Posterior lobe Pontocerebellum
The oldest cerebellum Caudal part Eye/head movement
The next oldest Midline Neck/trunk movement
The newest cerebellum Hemsiphere Limb movement
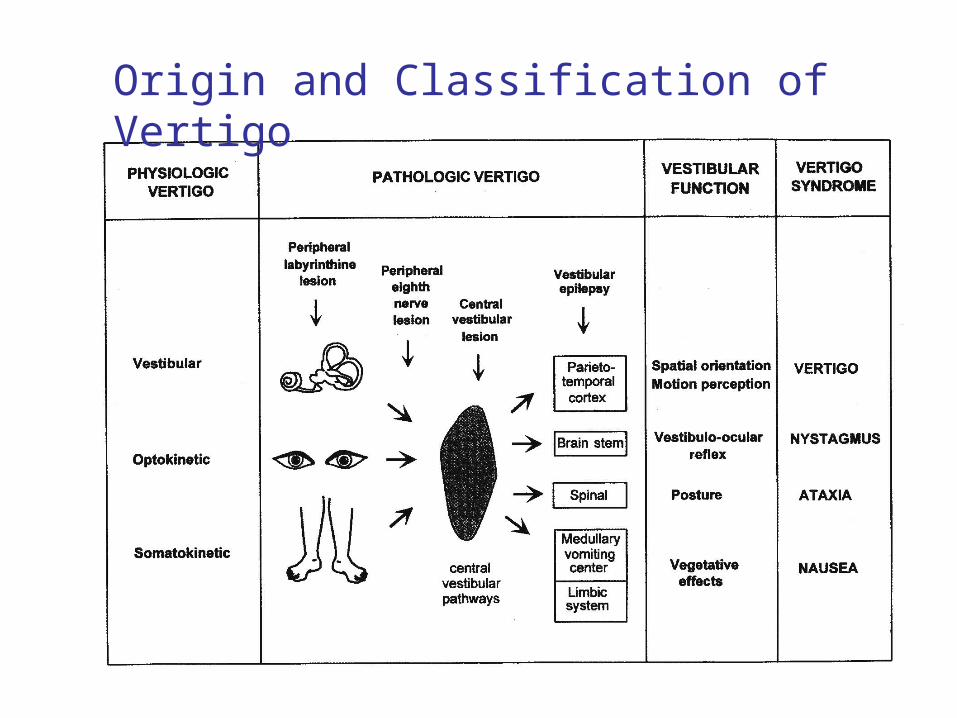
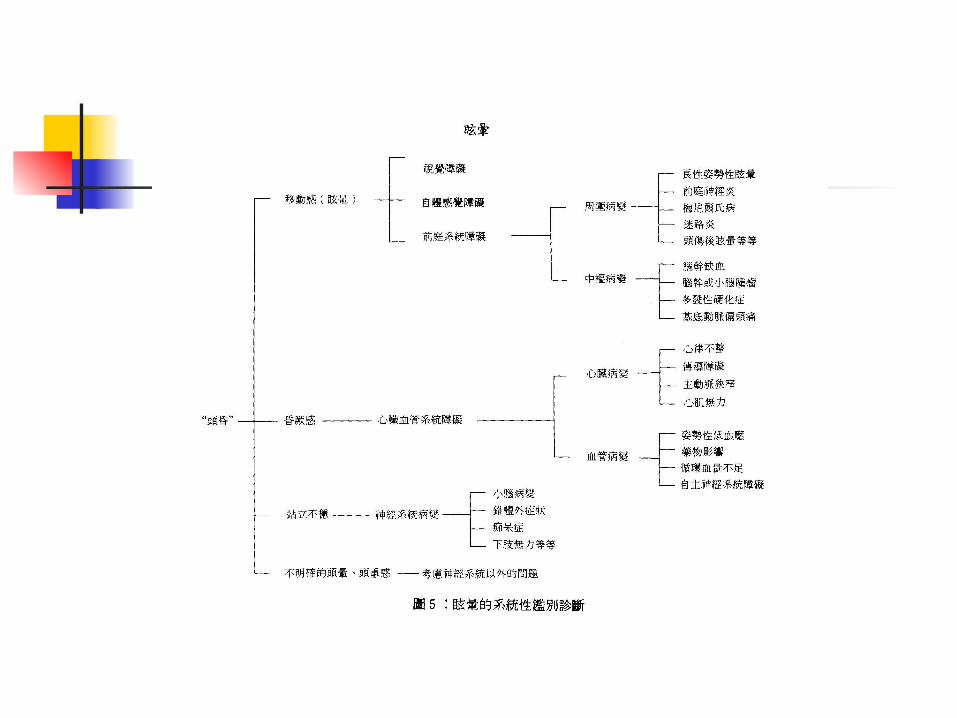
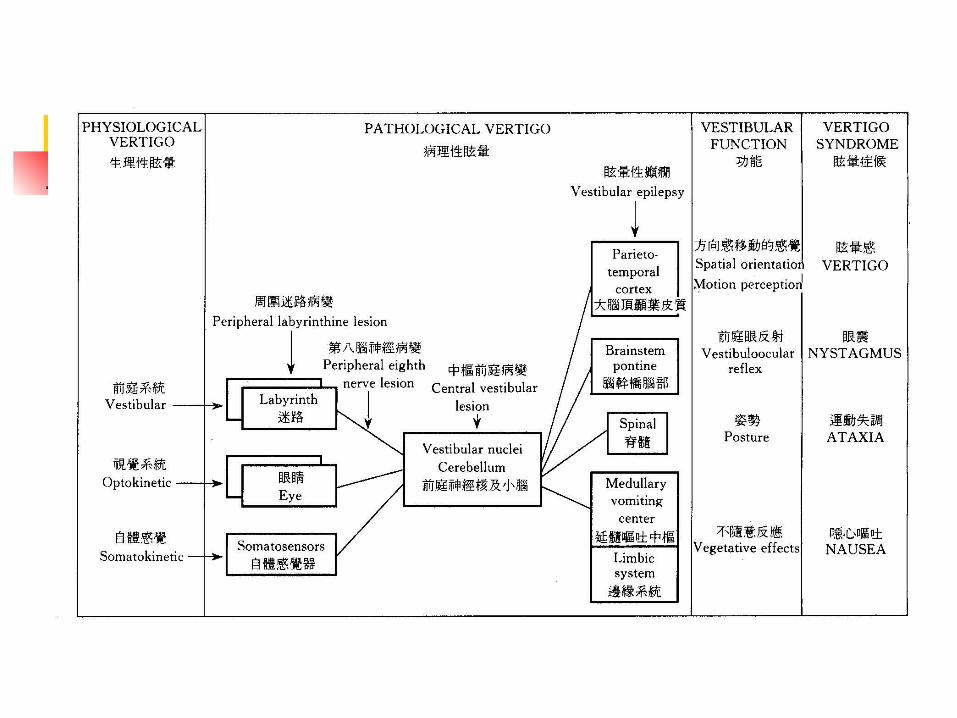
Origin and Classification of Vertigo
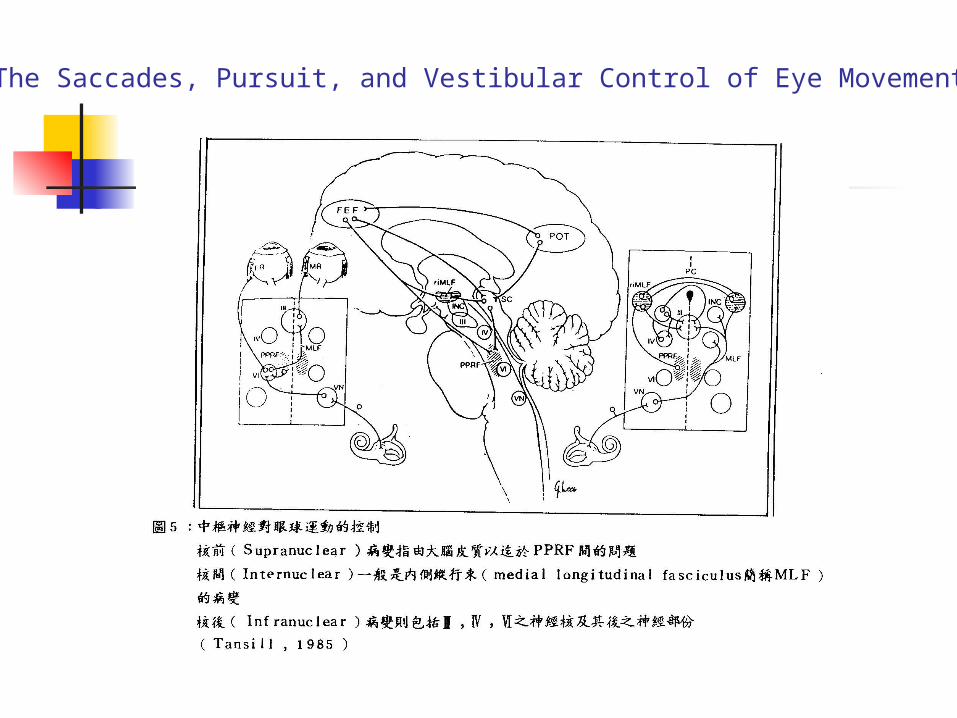
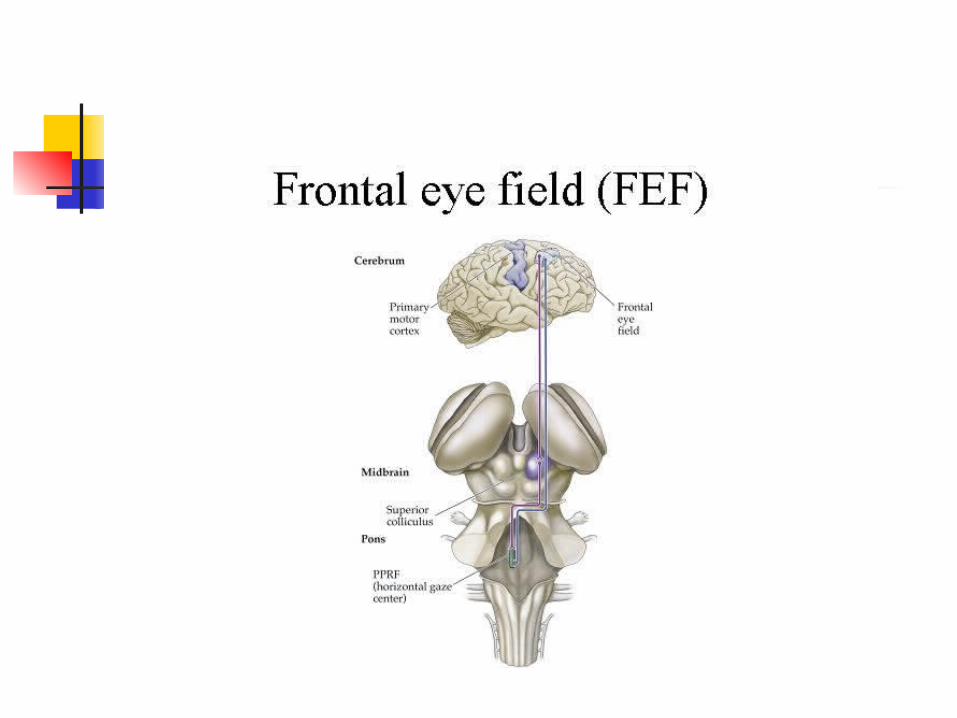
The Saccades, Pursuit, and Vestibular Control of Eye Movements
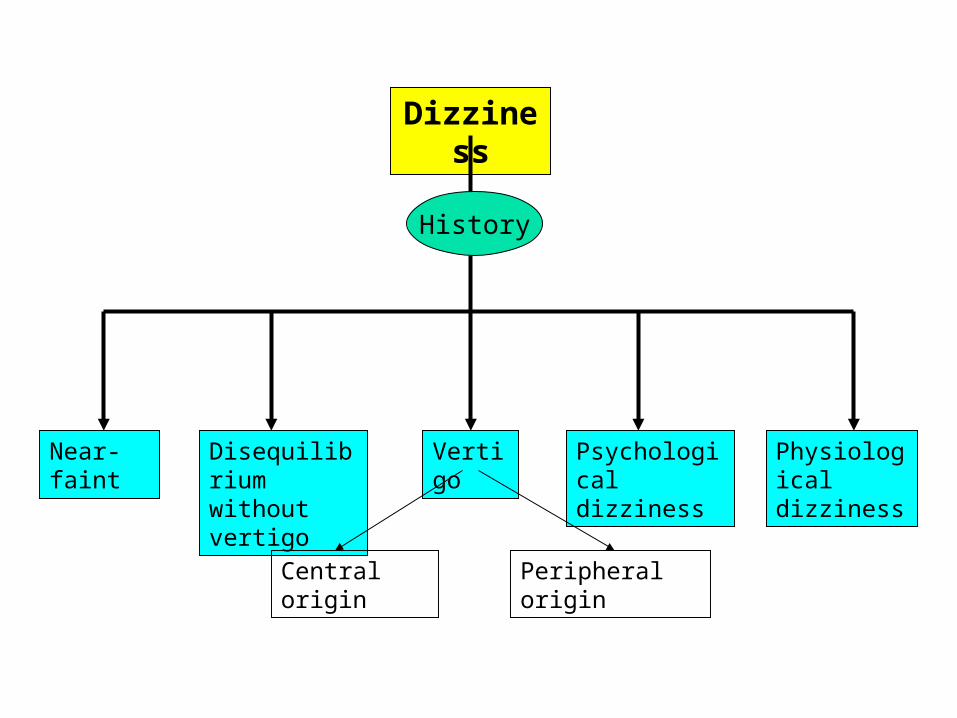
Dizziness
History
VertigoDisequilibrium without vertigo
Near-faint Psychological dizziness
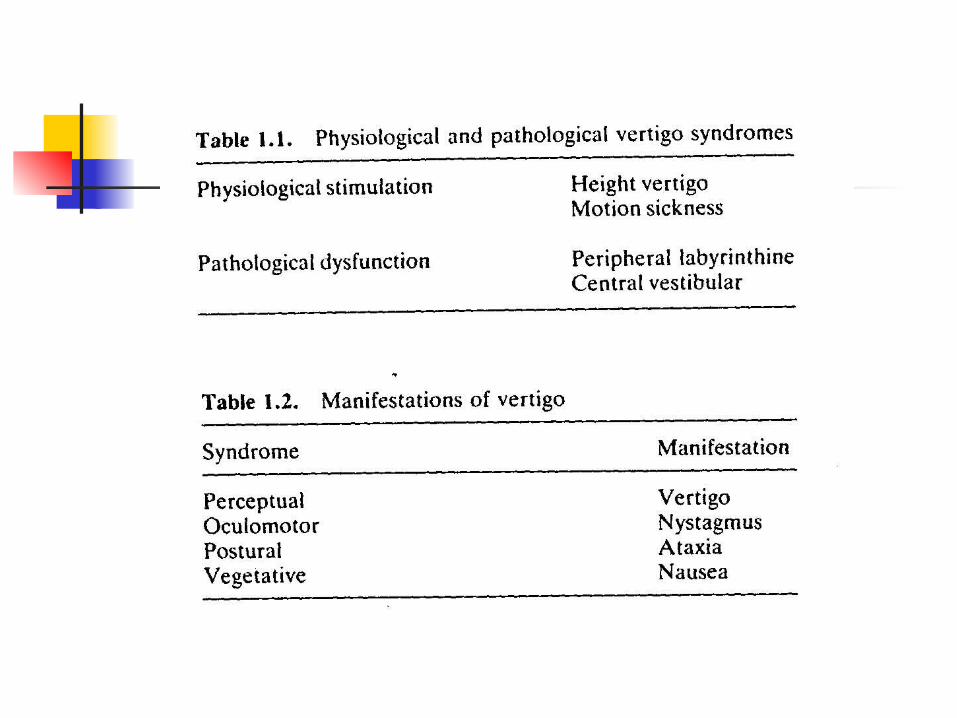
Physiological dizziness
Central origin Peripheral origin
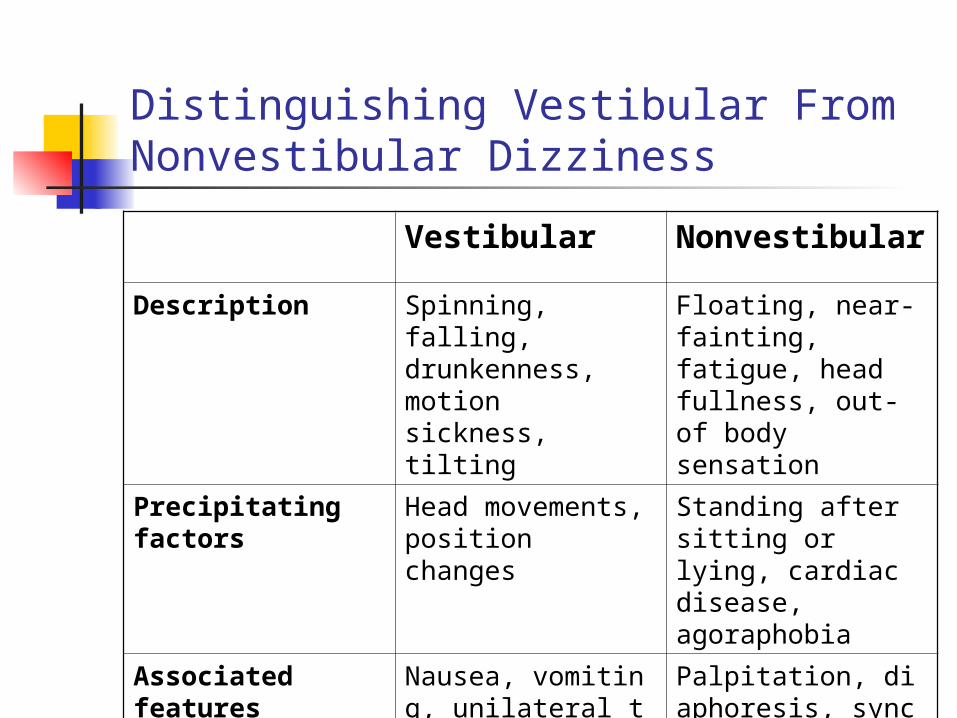
Distinguishing Vestibular From Nonvestibular Dizziness
Vestibular Nonvestibular
Description Spinning, falling, drunkenness, motion sickness, tilting
Floating, near-fainting, fatigue, head fullness, out-of body sensation
Precipitating factors Head movements, position changes
Standing after sitting or lying, cardiac disease, agoraphobia
Associated features Nausea, vomiting, unilateral tinnitus or hearing loss, imbalance, oscillopsia
Palpitation, diaphoresis, syncope, loss of concentration, dyspnea
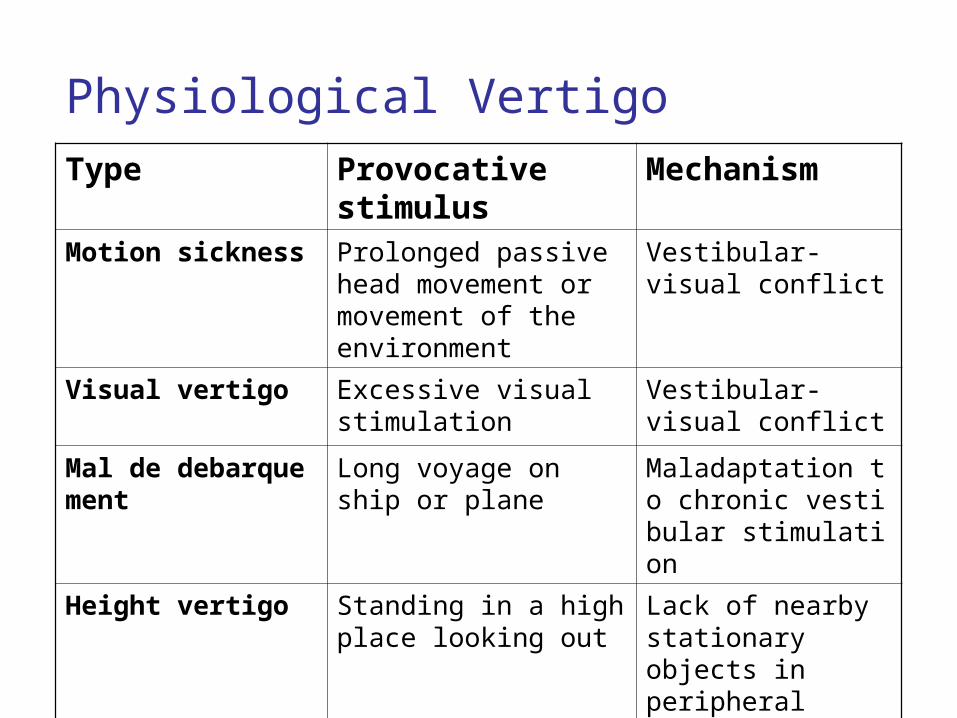
Physiological VertigoType Provocative stimulus Mechanism
Motion sickness Prolonged passive head movement or movement of the environment
Vestibular-visual conflict
Visual vertigo Excessive visual stimulation
Vestibular-visual conflict
Mal de debarquement Long voyage on ship or plane
Maladaptation to chronic vestibular stimulation
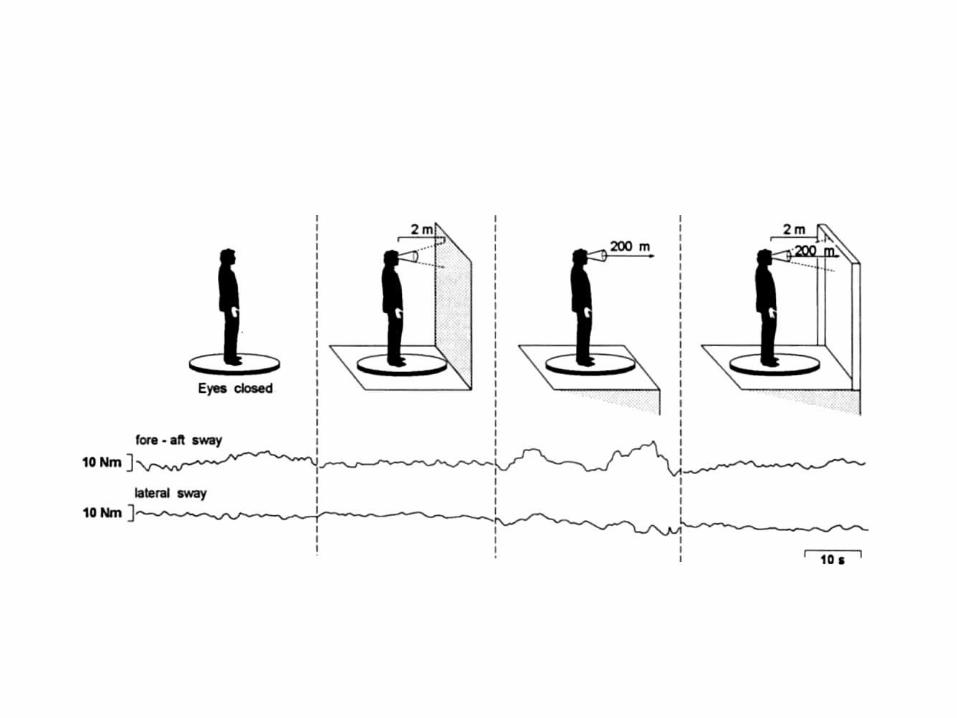
Height vertigo Standing in a high place looking out
Lack of nearby stationary objects in peripheral vision
Space sickness Zero gravity Canal-otolith conflict
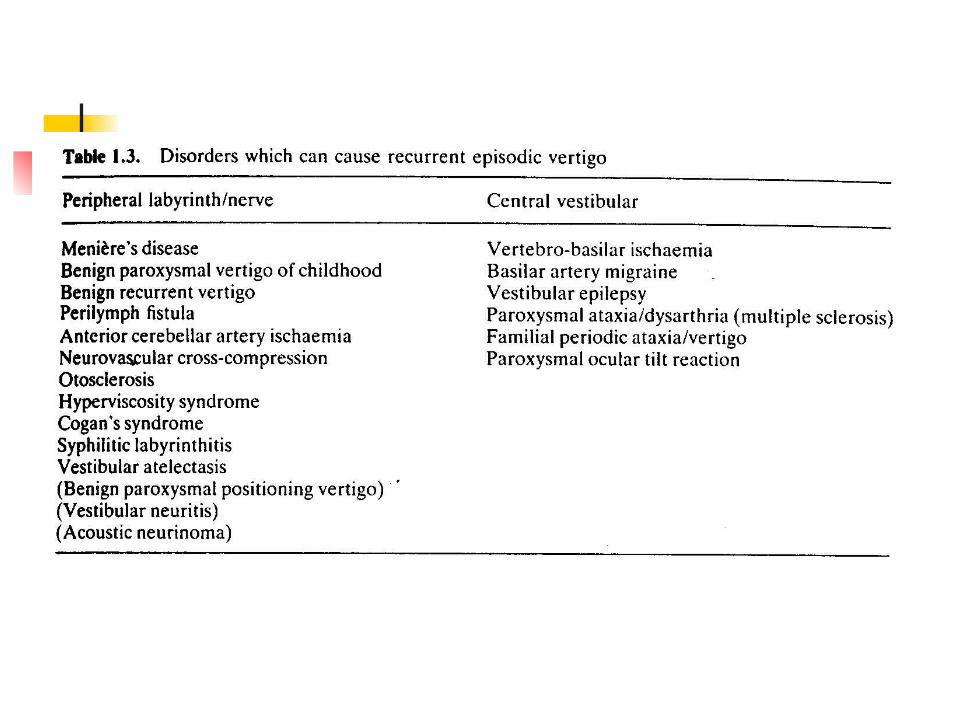
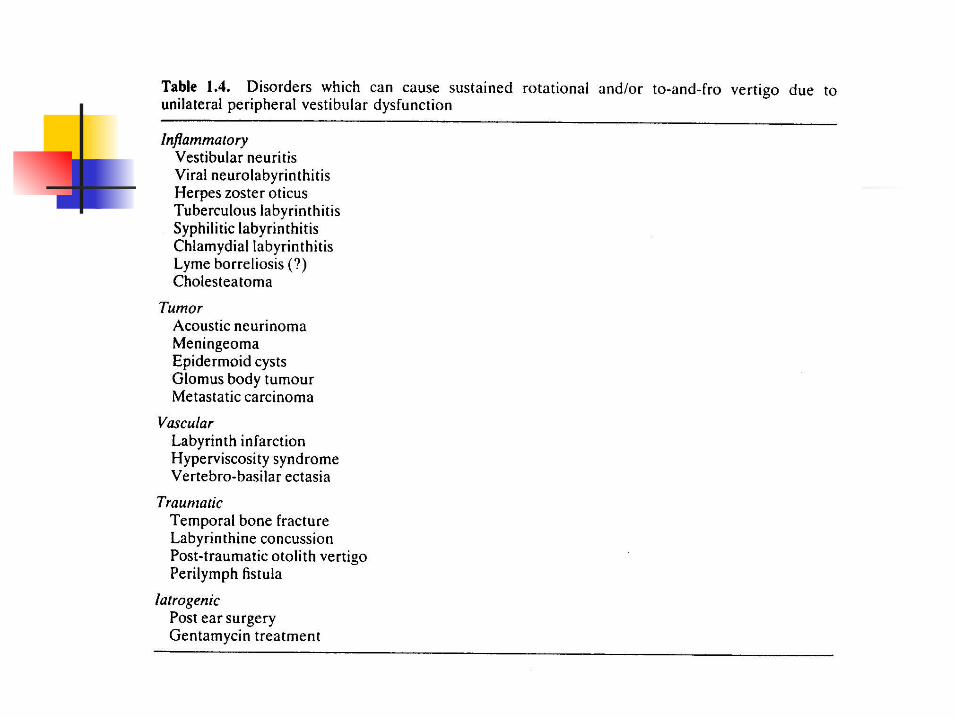
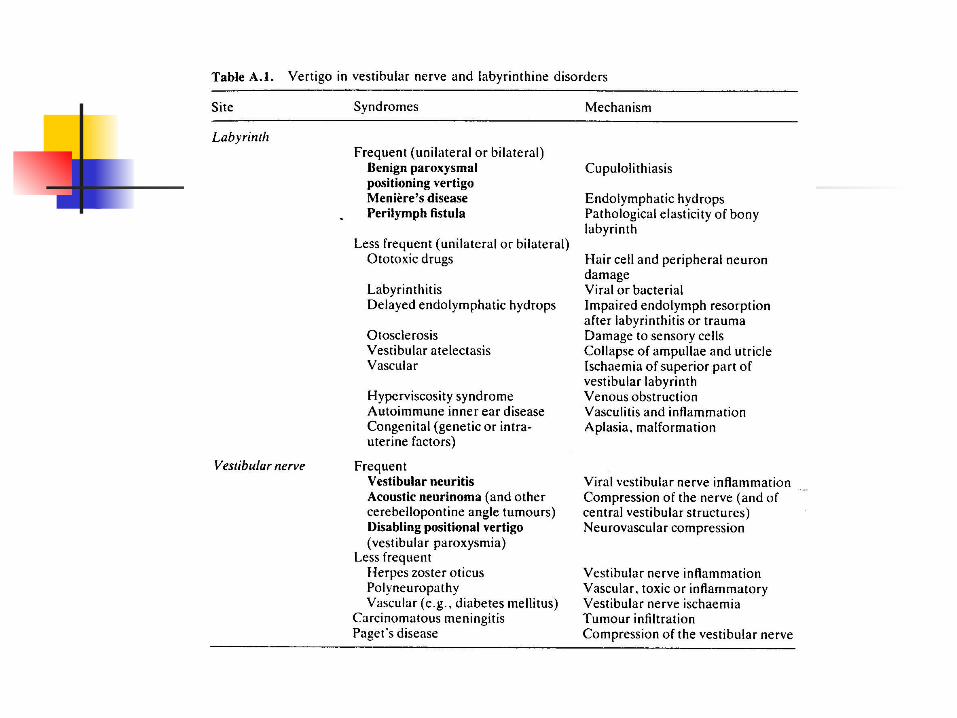
Causes of Pathological Vertigo
Peripheral vertigo Vestibular end organs: inner ear, labyrithi
ne apparatus Vestibular nerve
Central vertigo Brainstem: vestibular nucleus Archicerebellum (flocculonodular lobe)
Peripheral Causes of Vertigo Benign paroxysmal positional vertigo Meniere’s disease Acute peripheral vestibulopathy (vesti
bular neuritis) Head trauma Cerebellopontine angle tumor Toxic vestibulopathies
Disorders of the Semicircular Canal
Vertigo (spinning of the environment or the self)
Nystagmus Past-pointing of the li
mbs Ataxia Positive Romberg sign Turning during steppa
ge test
Tilt, a false sense of linear motion
Vertical diplopia Skew deviation Ataxia Positive Romberg sign Translation on the ste
ppage test
Disorders of the Otolith Organs
Central Causes of Vertigo Vertebrobasilar ischemia & infarction Cerebellar hemorrhage Alcoholic cerebellar degeneration Multiple sclerosis Posterior fossa tumors Paraneoplastic cerebellar degeneration Spinocerebellar degneration
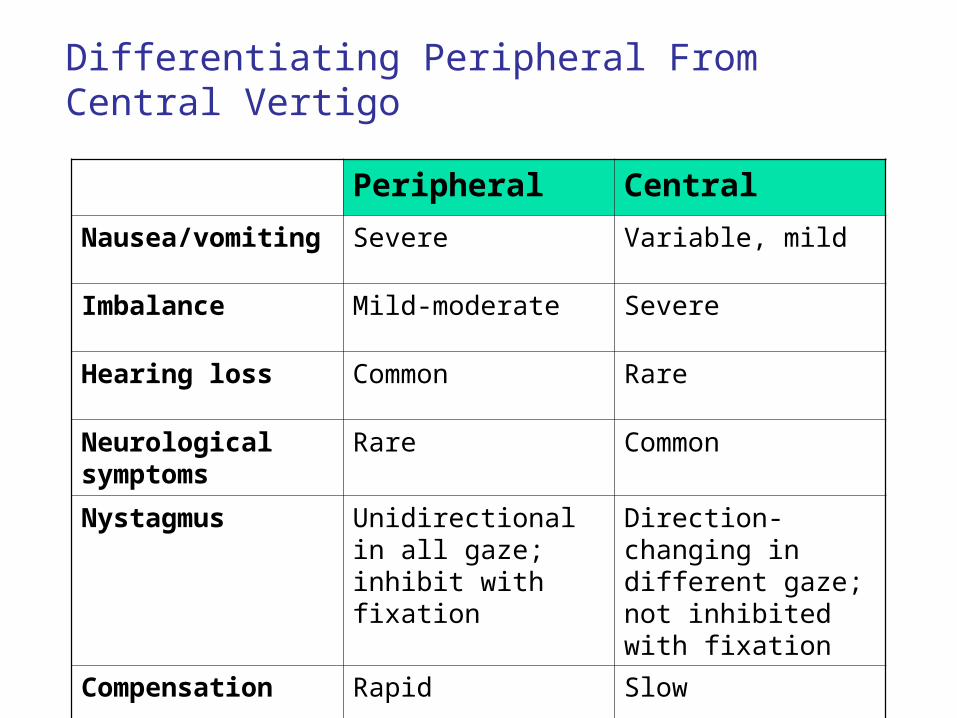
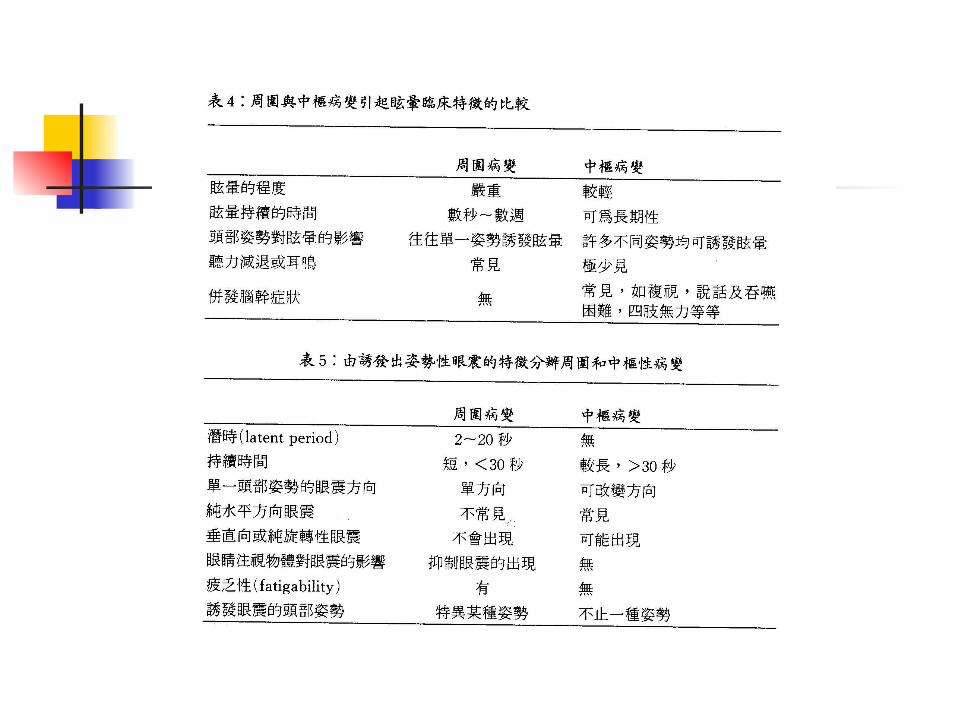
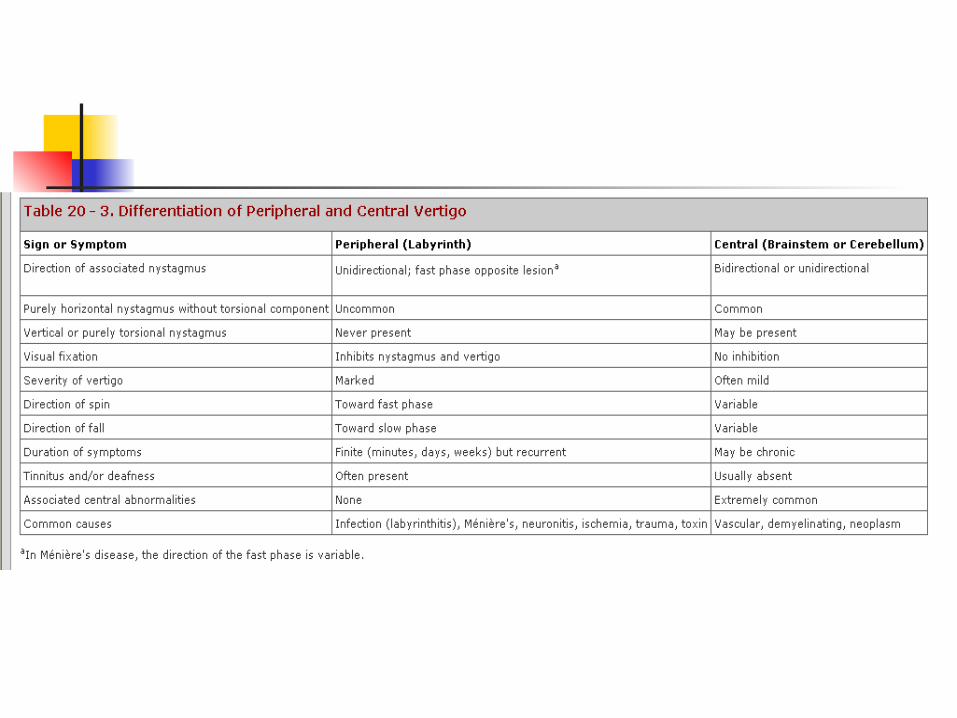
Differentiating Peripheral From Central Vertigo
Peripheral Central
Nausea/vomiting Severe Variable, mild
Imbalance Mild-moderate Severe
Hearing loss Common Rare
Neurological symptoms
Rare Common
Nystagmus Unidirectional in all gaze; inhibit with fixation
Direction-changing in different gaze; not inhibited with fixation
Compensation Rapid Slow
Systemic Causes of Vertigo
Drugs: anticonvulsants, sedatives, antihypertensives
Hypotension, presyncope: heart diseases, postural hypotension
Infectious diseases: syphilis, meningitis Endocrine diseases: DM, hypothyroidism Vasculitis: collagen vascular disease, giant-cell ar
teritis Others: anemia, polycythemia, systemic toxins
Causes of Dysequilibrium without Vertigo
Disorders of afferent senses Bilateral vestibular loss Sensory ataxia Multisensory disequilibrium
Disorders of central processing and motor responses Cerebellar degeneration Frontal lobe syndrome Extrapyramidal syndrome
Approach to Vertigo and Dizziness
General examination BP in the lying and standing Look for cardiac arrhythmia Examination of extracranial and peripher
al vasculature
Approach to Vertigo and Dizziness
Neurological examination (1) Consciousness and mental status Visual acuity and visual field Fundus Screening for hearing impairment Ocular motor examination
Nystagmus Ocular motor palsy Slow or ataxic ocular movement
assessing current history Ask the patient to describe the symptoms without using the wor
d dizzy. Have the patient differentiate vertigo from presyncope or near-syncope.
Determine if the patient has a sense of being pushed down or pushed to one side (pulsion). A peculiar sense of movement of objects viewed when the patient moves is termed oscillopsia.
Ascertain whether the symptoms are related to an anxiety attack; patients with agoraphobia may describe their symptoms as dizziness.
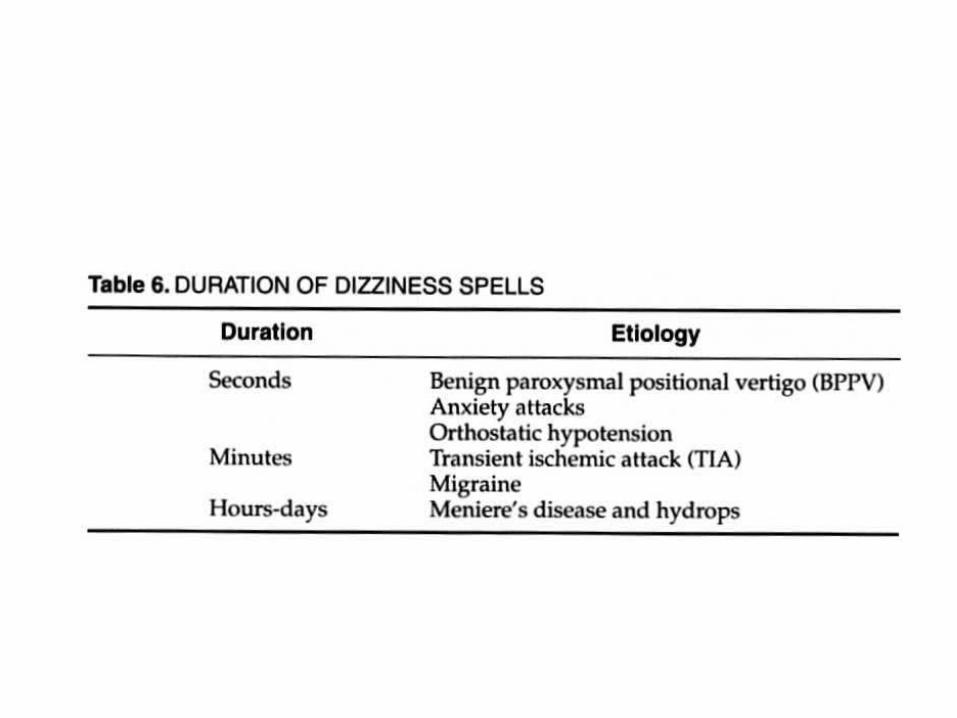
Determine if the sensation is continuous or episodic (ie, attacks); if episodic, find out if the sensation is fleeting or prolonged.
Ascertain whether the onset and progression of symptoms were slow and insidious or acute.
Ask the patient about head trauma and other illnesses to determine the setting of the initial symptoms. Trauma resulting in damage to an ear often manifests as unilateral hearing loss, which may be the cause of episodic vertigo even years later (posttraumatic hydrops).
Determine if the attacks are associated with turning the head, lying supine, or sitting upright.
Determine if symptoms of an upper respiratory infection or flu-like illness preceded the onset of vertigo.
Inquire about associated symptoms such as hearing loss or tinnitus (ringing in the ears), aural fullness, diaphoresis, nausea, or emesis.
Determine if the patient has an aura or warning before the symptoms start. If hearing loss is evident, find out if hearing fluctuates. Determine if the patient has a headache or visual symptoms such as scintilla
ting scotoma. Ask the patient about brainstem symptoms such as diplopia, dysarthria, fac
ial paresthesia, or extremity numbness or weakness. Ascertain the degree of impairment during an attack
Examination of Vestibulo-ocular Reflexes
Spontaneous nystagmus Elicit slow phases with slow head
rotation, in yaw (horizontal), pitch (vertical), and roll (torsion), and with high accelerations in yaw and pitch (head thrust)
Caloric test Head-shaking nystagmus
Vestibulospinal Testing
Past-pointing with arms, with eyes closed Romberg: feet apposed, in tandem, in
tandem on toes, on one foot at a time, standing on compliant foam rubber
Fukuda stepping test or walking around a circle
Tandem gait, forward and backward
Approach to Vertigo and Dizziness
Neurological examination (2) Motor system examination
Focal or diffuse weakness Reflex changes
Sensory examination Stock-and-gloving sensation loss: polyneuro
pathy Loss of vibratory and proprioceptive sensatio
n: Vit B12 deficiency or tabes dorsalis Romberg’s sign
Approach to Vertigo and Dizziness
Neurological examination (3) Cerebellar examination
Observation of sitting and standing and walking
Bending backward Tandem gait Walking around a chair Finger-nose-finger Heel-knee-shin
Approach to Vertigo and Dizziness
Neurological examination (3) Cerebellar examination
Pronation-supination Knee-patting Rapid touching of each finger to the thumb Arm deviation Arm tapping Rebound test
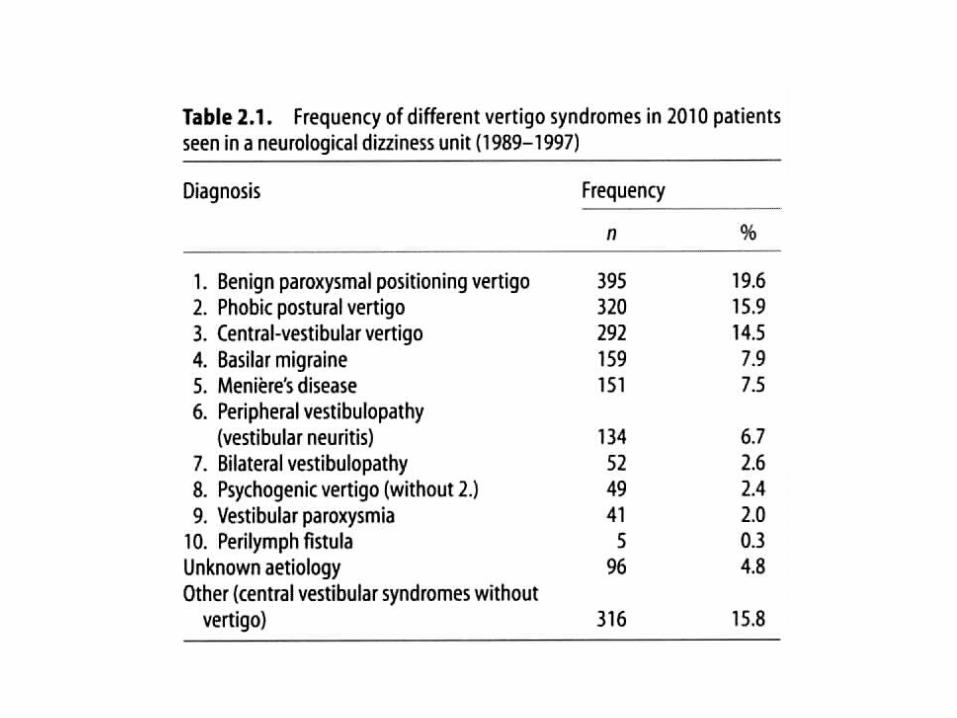
The Most Common Causes of Vertigo Syndromes Seen in a Neurological Clinic
Benign paroxysmal positioning vertigo
Phobic postural vertigo Basilar migraine Meninere’s disease Vestibular neuritis
(T. Brandt, “Vertigo, its multisensory syndrome”)
Benign Paroxysmal Positioning Vertigo
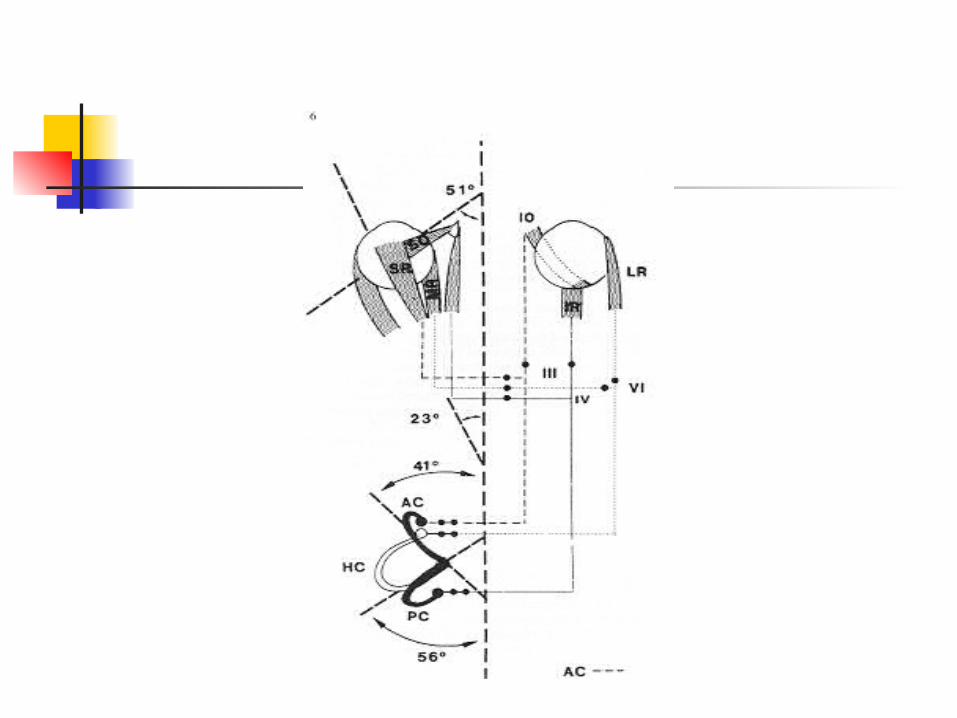
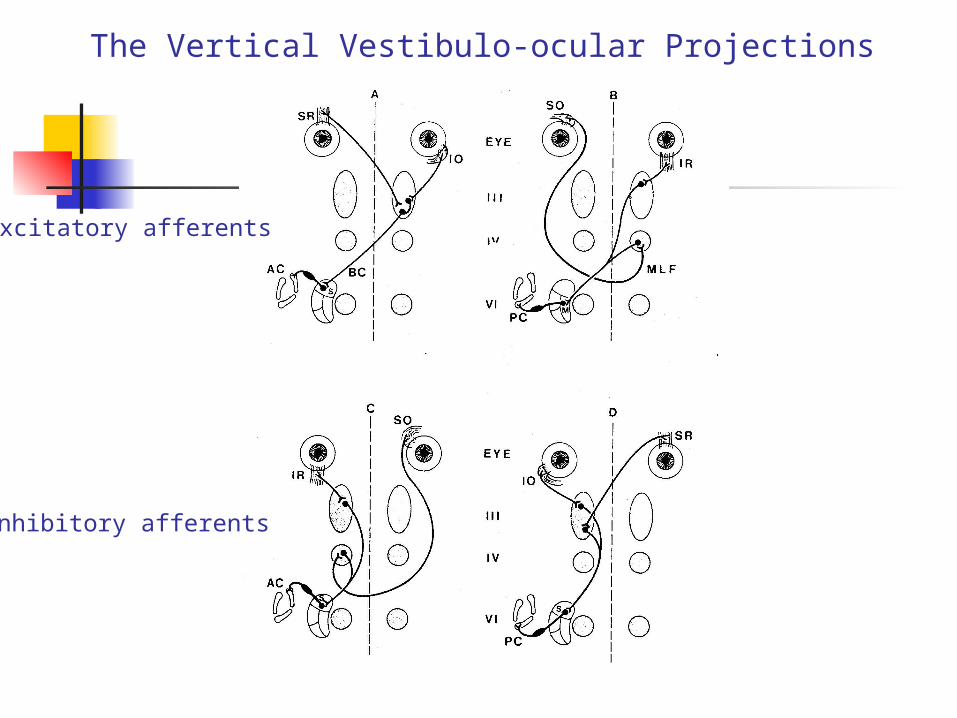
The Vertical Vestibulo-ocular Projections
Excitatory afferents
Inhibitory afferents
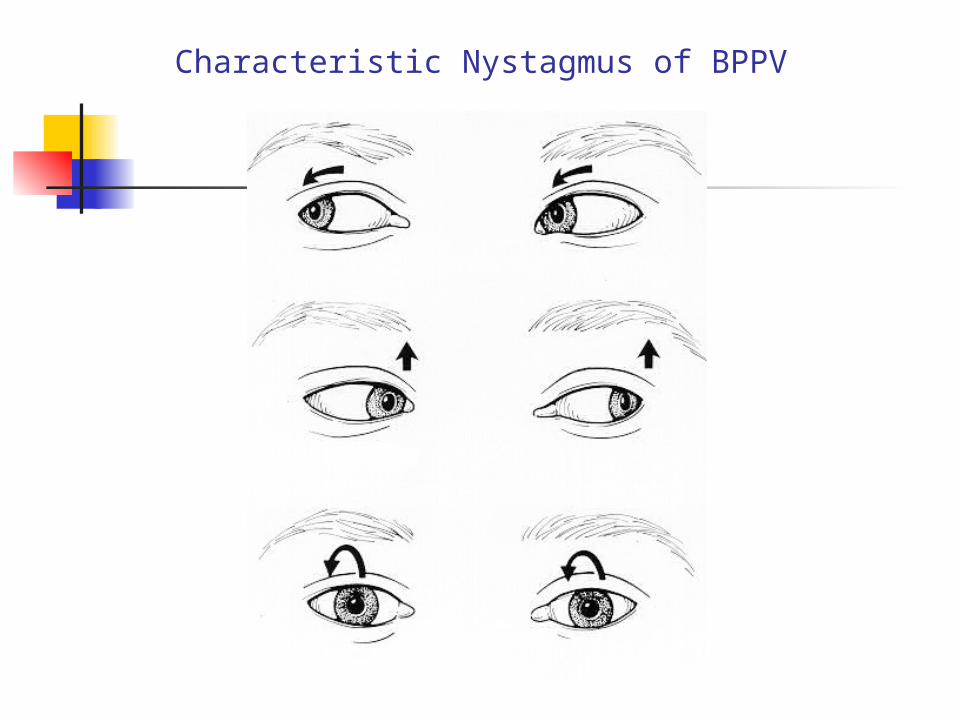
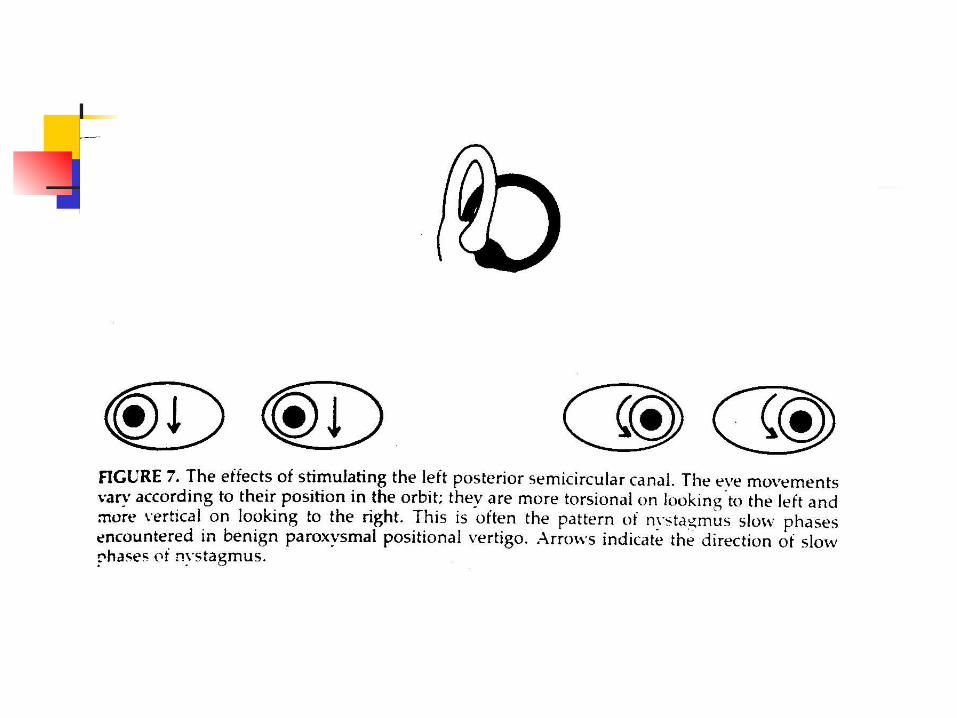
Characteristic Nystagmus of BPPV
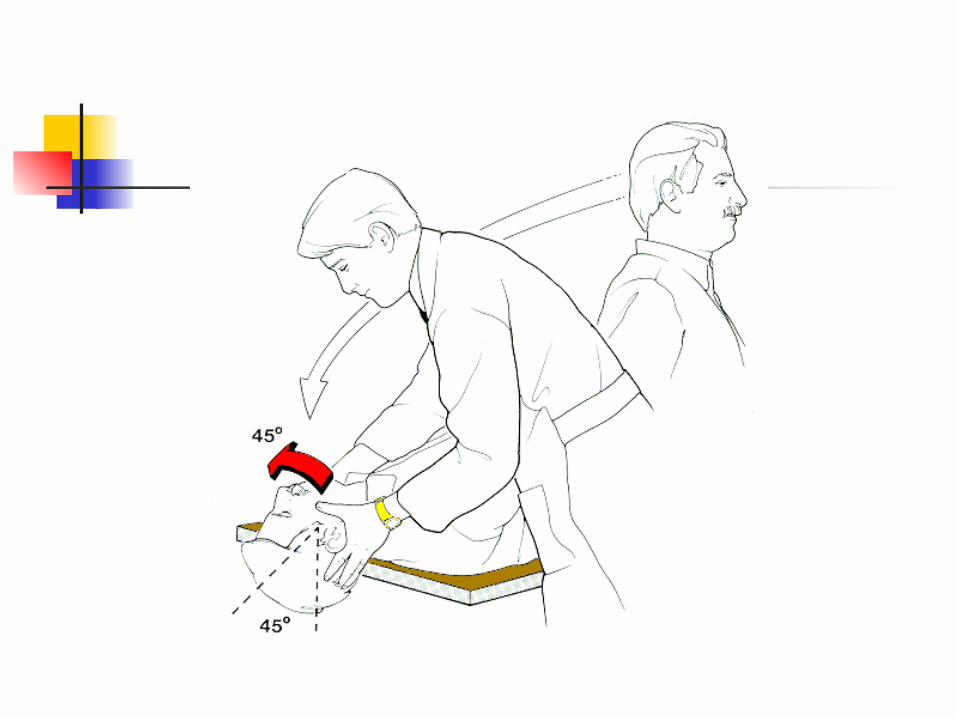
Benign Paroxysmal Positional Vertigo (BPPV) – Symptoms & Signs
Brief attacks of rotational vertigo and concomitant rotatory nystagmus precipitated by rapid head tilt, turning or extension.
The symptoms can be induced by Hallpike maneuver.
Typical peripheral vestibular nystagmus, short latency, limited duration, reversal on returning to the upright position, and fatigability on repeated provocation.
Benign Paroxysmal Positional Vertigo (BPPV) – Pathogenesis & Treatment
Otolith debris floats freely within the endolymph of the semicircular canal: canalolithiasis.
Heavy debris settles on the cupula transforming it as a transducer of angular acceleration into a transducer of linear acceleration: cupulolithiasis.
Treatment by canal repositioning or libratory maneuvers.
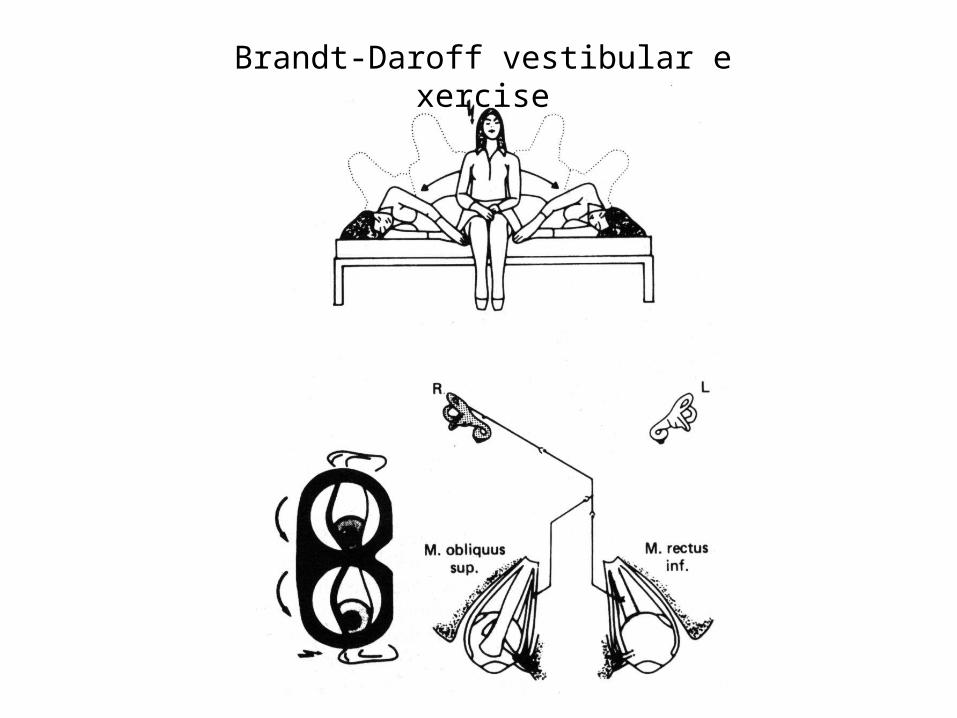
Brandt-Daroff vestibular exercise
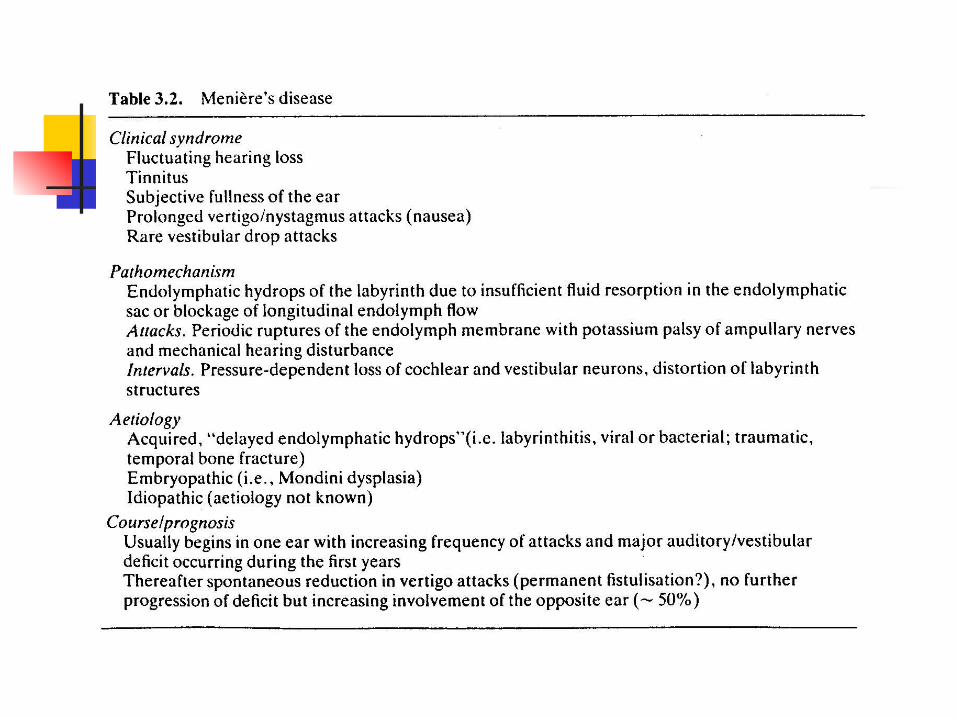
Meriere’s Disease
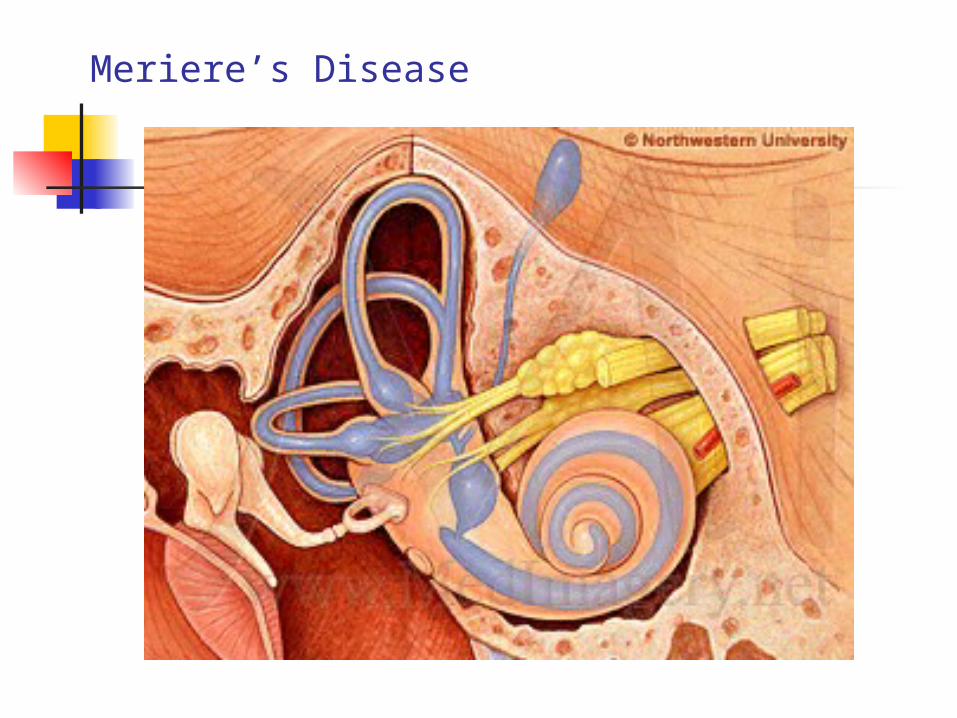
Meriere’s Disease
Meniere’s Syndrome – Symptoms & Signs Fluctuating hearing loss, tinnitus,
episodic vertigo and a sensation of fullness or pressure in the ear.
Attacks lasted for hours but dizziness and unsteadiness remain for a few days.
Repeated attacks lead to progressive tinnitus, hearing loss, and impaired vestibular function.
Usual in the fourth to sixth decades.
Endolymphatic hydrops: increase of volume of endolymph associated with distension of entire endolymph system.
The attacks are caused by rupture of membranous labyrinth leading to paralysis of the surrounding vestibular or cochlear hair cells and neural structures.
Symptomatic treatment of acute spells. Salt restriction and diuretics. Intratympnic treatment with ototoxic antibiotics. Labyrinthectomy or vestibular neurectomy.
Meniere’s Syndrome – Pathogenesis & Treatment
Basilar Migraine – Symptoms & Signs
Vertigo may occur in about one-fourth of migraine patients, and can occur without headache.
Other symptoms of basilar migraine include ataxia, dysarthria, diplopia, visual symptoms, tinnitus, decreased hearing, bilateral pareses or paresthesia and decreased level of consciousness.
Benign paroxysmal vertigo of childhood. Benign recurrent vertigo of adulthood. Motion sensitivity with frequent bouts of motion si
ckness occurs in at least one-half of patients with migraine.
Basilar Migraine – Pathogenesis & Treatment Vasoconstriction (?). Neuronal depression (?). Genetic. Channelopathy. Symptomatic treatment of acute attack
Antivertiginous medications. Antiemetics. Sumatriptans and ergotamines often are ineffective and e
ven aggravate vertigo. Prophylactic treatment of attacks
Beta-blockers. Calcium channel blockers. Valproic acid. Tricyclics.
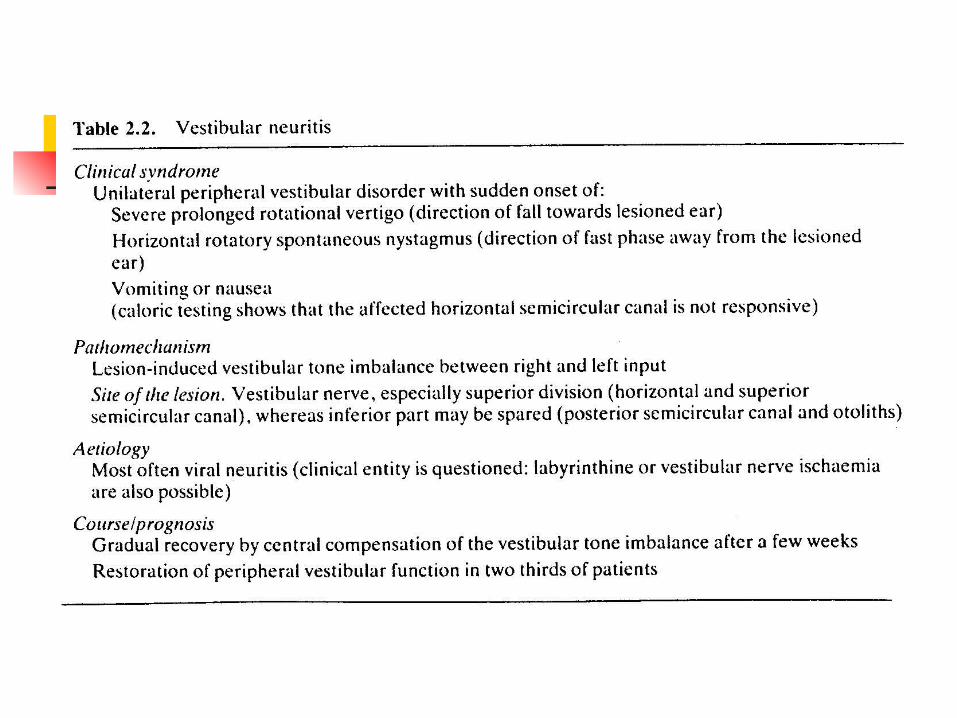
Vestibular Neuritis
Vestibular Neuritis – Symptoms & Signs
Vertigo, nausea, and vomiting developed over several hours, reach a peak within 24 h, and resolve gradually over several weeks.
Generally without hearing symptoms. Diagnosis is based on acute unilateral peripheral v
estibular loss and exclusion of other inner ear diseases.
Ramsay Hunt syndrome by varicella-zoster infection may causes facial paresis, tinnitus, hearing loss, and a vestibular defect.
Presumed of viral origin. Similar to Bell’s palsy caused by reactivation of d
ormant herpes infection in the Scarpa’s ganglion within the vestibular nerve.
Treatment is symptomatic. Antivertiginous medication should not be given as long as nausea and vomiting subsides. These drugs suppress central compensation.
Corticosteroid may shorten the clinical course. Vestibular rehabilitation exercise.
Vestibular Neuritis – Pathogenesis & Treatment
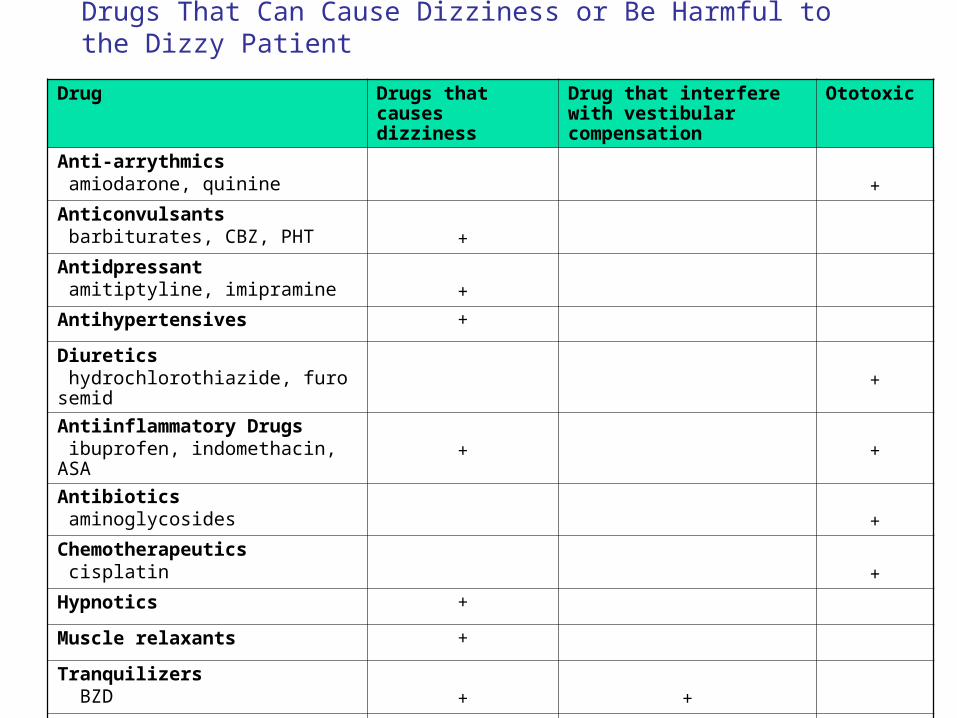
Drugs That Can Cause Dizziness or Be Harmful to the Dizzy Patient
Drug Drugs that causes dizziness
Drug that interfere with vestibular compensation
Ototoxic
Anti-arrythmics amiodarone, quinine +
Anticonvulsants barbiturates, CBZ, PHT +
Antidpressant amitiptyline, imipramine +
Antihypertensives +
Diuretics hydrochlorothiazide, furosemid +
Antiinflammatory Drugs ibuprofen, indomethacin, ASA + +
Antibiotics aminoglycosides +
Chemotherapeutics cisplatin +
Hypnotics +
Muscle relaxants +
Tranquilizers BZD + +
Vestibular suppressants meclizine, scapolamine + +
The End
Thank You.
The Supranuclear Control of Eye Movements

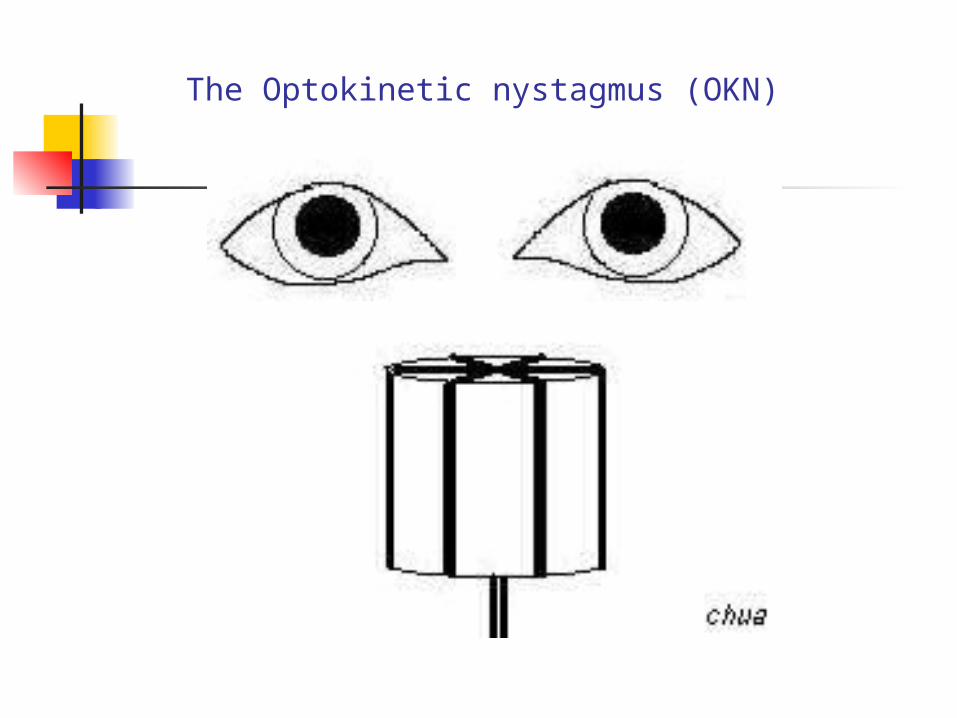
The Optokinetic nystagmus (OKN)
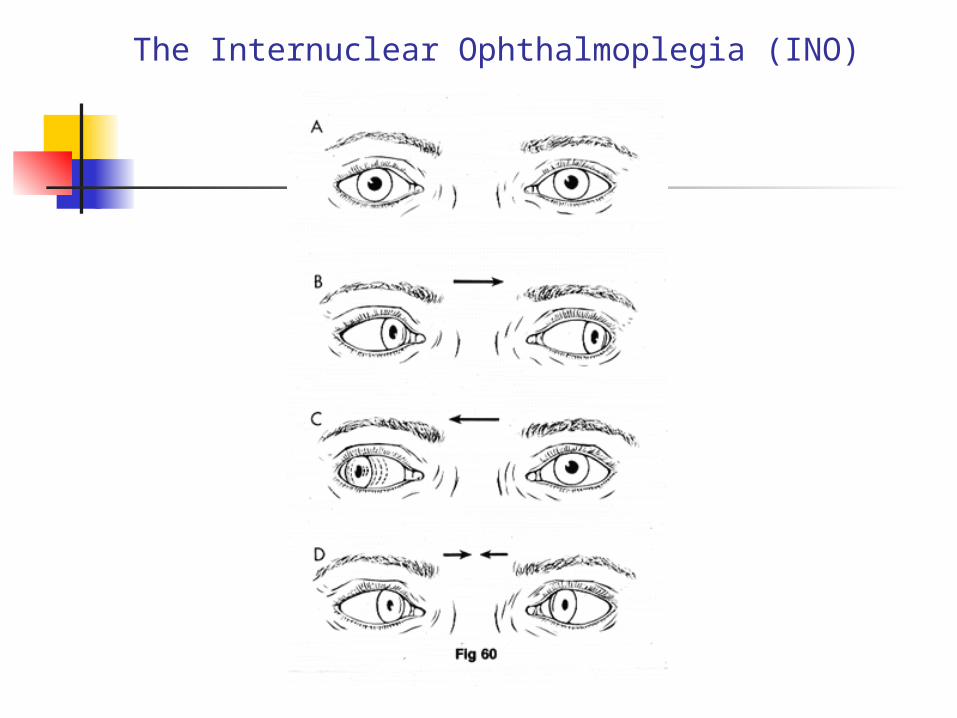
The Internuclear Ophthalmoplegia (INO)