Embed Size (px)
Citation preview

行政院衛生署桃園醫院
胸腔內科 李世偉醫師
Effusions from parapneumoEffusions from parapneumonic infections and empyemanic infections and empyema
AGENDA• The clinical importance o
f infection in the pleural space
• Historical perspective• The epidemiology of pleu
ral infection• The pathophysiology of p
leural infection• Bacteriology• The diagnosis and clinical
asessment of pleural infection
• Differential diagnosis• Predictors of clinical out
come in pleural infection
• Radiology• Antibiotics• Chest catheter drainage• Intrapleural fibrinolytics• Future directions
NICK A MASKELL AND ROBERT JO DAVIES
TEXTBOOK OF PLEURAL DISEASE
The clinical importance of infection in the pleural space• Frank purulent pleural empyema has an overall m
ortality up to 20%, which rise further to about 35% in the immunocompromised host.
• The actual mortality rise from empyema is substantially influenced by the presence of co-morbid disease.
• In addition to this mortality, up to 40% of patients will fail treatment which chest tube drainage and antibiotics alone and still require surgical drainage of their pleural collection.
• Simple parapneumonic effusions arise in up to 57% of cases of pneumonia.NICK A MASKELL AND ROBERT JO DAVIES
TEXTBOOK OF PLEURAL DISEASE
The clinical importance of infection in the pleural space• Parapneumonic effusion occurred in 20 to 40
% of patients who are hospitalized with pneumonia.
• The mortality in patients with parapneumonic effusion is higher than that in patients with pneumonia without a parapneumonic effusion.
• Some of the excess mortality is due to mismanagement of the parapneumonic effusion.
Light RW. Pleural diseases, 4th ed. Baltimore: Lippincott, Williams and Wilkins; 2001.
Definition• Parapneumonic effusion is any pleural eff
usion secondary to pneumonia ( bacterial or viral ) or lung abscess.
• Empyema is , by definition, pus in the pleural space.
• A complicated parapneumonic effusion is a parapneumonic pleural effusion for which an invasive procedure is necessary for its resolution, or a parapneumonic effusion on which the bacterial cultures are positive.
Light RW. Pleural diseases, 4th ed. Baltimore: Lippincott, Williams and Wilkins; 2001.
Historical perspective• 500BC. Hippocrates: open thoracic drainage.• 1876-1891: chest tube and under water seal.• 1919 First World War: open early surgical drainage, mortalit
y as high as 70%.• Hewitt and Bulau: adequate pus drainage with a closed che
st tube, avoidance of early open drainage, obliteration of the pleural space, proper nutritional support. Reduced the mortality to 4.3%.
• 1940s: Penicillin• 1940s Tillett: intrapleural fibrinolytic therapy; frequent anti
genic side effects• 1897 Estlander and 1890 Schede: thoracoplasty• 19th Century end Fowler and Beck: decortication of the ple
ura• Video assisted thoracoscopic surgery ( VATS)
NICK A MASKELL AND ROBERT JO DAVIES TEXTBOOK OF PLEURAL DISEASE
The epidemiology of pleural infection• More common in the elderly and childhood.
• Men are affected twice as often as women.• Higher in those with diabetes, alcoholism
and substance abuse, rheumatoid arthritis and chronic lung disease.
• Poor dentition and risk factors for aspiration are associated with an increase prevalence of anaerobic infection.
NICK A MASKELL AND ROBERT JO DAVIES TEXTBOOK OF PLEURAL DISEASE
Parapneumonic effusion 70%
post bacterial pneumonia
hospital acquired pneumonia
Primary empyema 4%
Post operative 12%
Traumatic 3%
blunt trauma
penetrating trauma
Iatrogenic 4%
e.g. post chest tube insertion
Abdominal infection 2%
e.g. subphrenic abscess
Miscellaneous 3%
esophageal perforation
bacteremia
rupture of lung abscess into pleural cavity
intravenous drug abuse ( contaminated needles )
NICK A MASKELL AND ROBERT JO DAVIES TEXTBOOK OF PLEURAL DISEASE
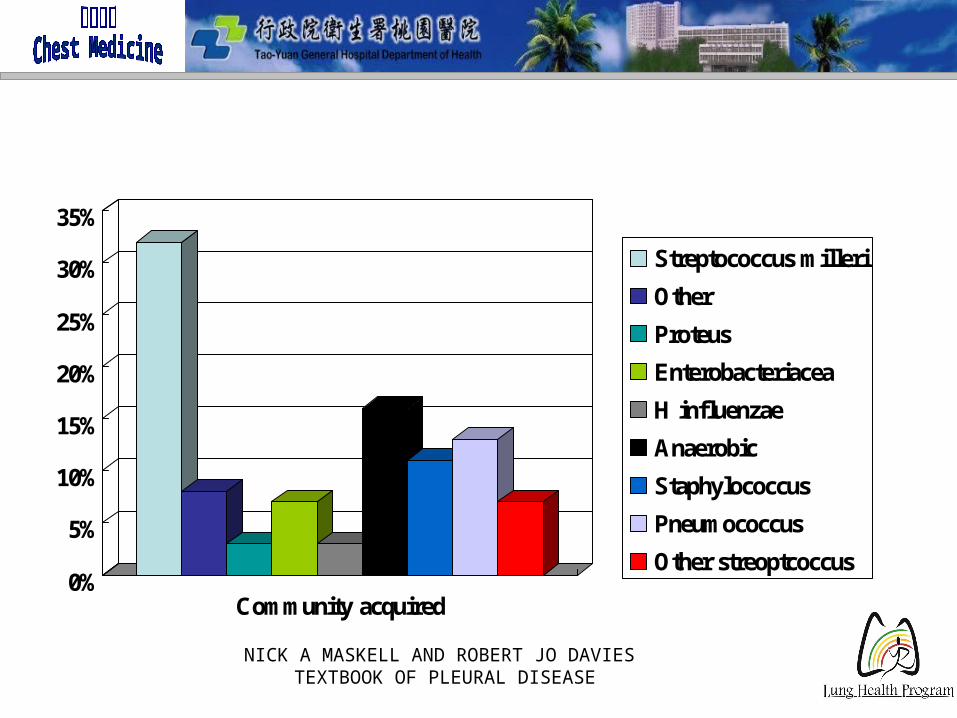
0%
5%
10%
15%
20%
25%
30%
35%
Community acquired
Streptococcus milleri
Other
Proteus
Enterobacteriacea
H influenzae
Anaerobic
Staphylococcus
Pneumococcus
Other streoptcoccus
NICK A MASKELL AND ROBERT JO DAVIES TEXTBOOK OF PLEURAL DISEASE
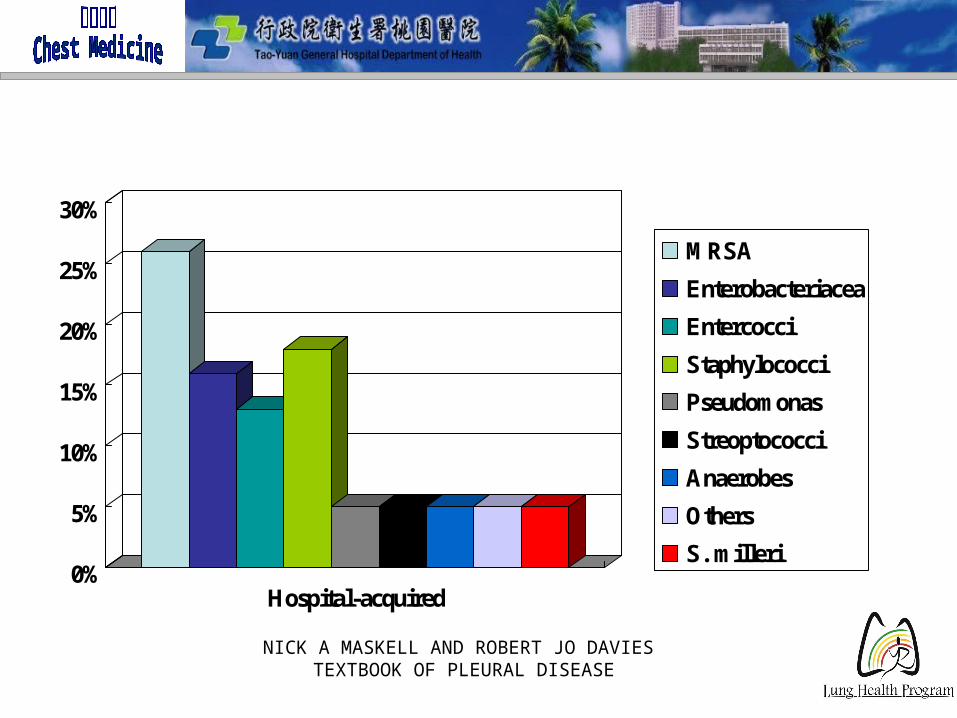
0%
5%
10%
15%
20%
25%
30%
Hospital-acquired
MRSA
Enterobacteriacea
Entercocci
Staphylococci
Pseudomonas
Streoptococci
Anaerobes
Others
S. milleri
NICK A MASKELL AND ROBERT JO DAVIES TEXTBOOK OF PLEURAL DISEASE
The pathophysiology of pleural infection • Development of the initial pleural effusi
on: the exudative phase• The evolution of infection: the fibropuru
lent phase• Natural healing: the organizing stage
Andrews NC, Parker EF, Shaw RR, Wilson NJ, Webb WR. Management of nontuberculous empyema. Am Rev Respir Dis 1962;85:935–936.
Development of the initial pleural effusion: the exudative phase
• There is rapid outpouring of fluid into the pleural space.
• Most of the fluid is due to increased pulmonary interstitial fluid traversing the pleura to enter the pleural space but some of this is due to increased permeability of the capillaries in the pleural space.
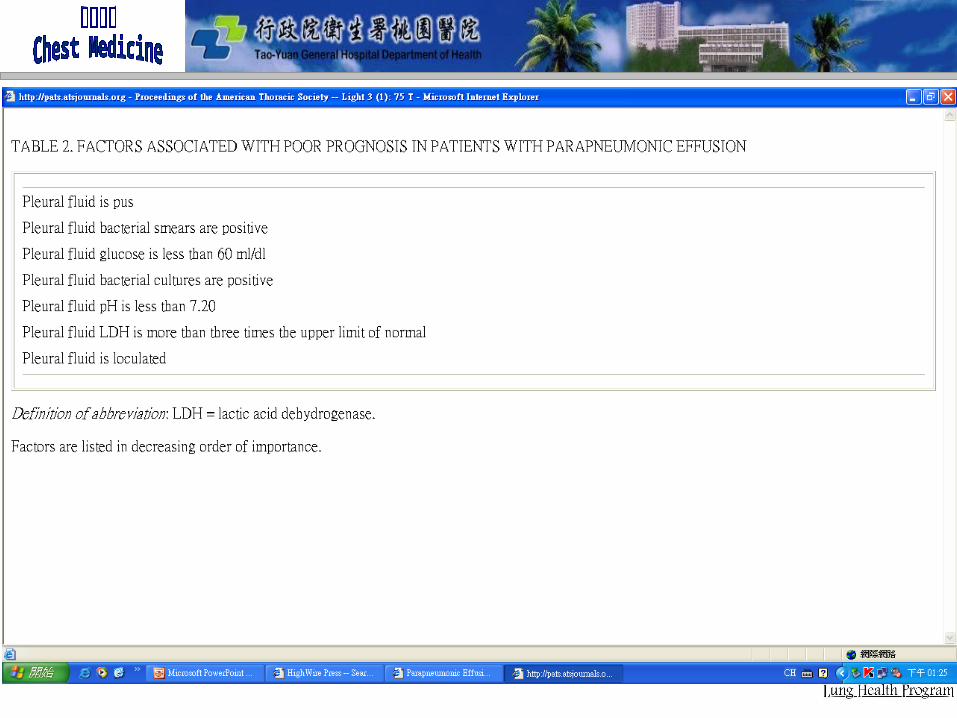
• The pleural fluid in this stage is characterized by negative bacterial studies, a glucose level above 60 mg/dl, a pH above 7.20, and a lactic acid dehydrogenase (LDH) level of less than three times the upper normal limit of serum.
• If the patient does not see a physician or receives the wrong antibiotic, the effusion may proceed to the second stage, which is the fibropurulent stage. The Proceedings of the American Thoracic Society 3:75-80 (2006)
The evolution of infection: the fibropurulent phase• The pleural fluid in this stage is characterized
by positive bacterial studies, a glucose level below 60 mg/dl, a pH below 7.20, and a pleural fluid LDH more than three times the upper normal limit for serum.
• In this stage, the pleural fluid becomes infected and progressively loculated.
• The pleural fluid needs to be drained in this stage and drainage becomes progressively difficult as more loculations form.
• If a stage 2 effusion is not drained, the effusion may progress to the third stage.The Proceedings of the American Thoracic Society 3:75-80 (2006)
Natural healing: the organizing stage• Fibroblasts grow into the pleural fluid
from both the visceral and parietal pleurae, producing a thick pleural peel.
• The peel over the visceral pleura prevents the lung from expanding.
• Because the pleural space must be eradicated if a pleural infection is going to be eliminated, this peel must be removed if the infection is going to be cured. The Proceedings of the American Thoracic Society 3:75-80 (2006)
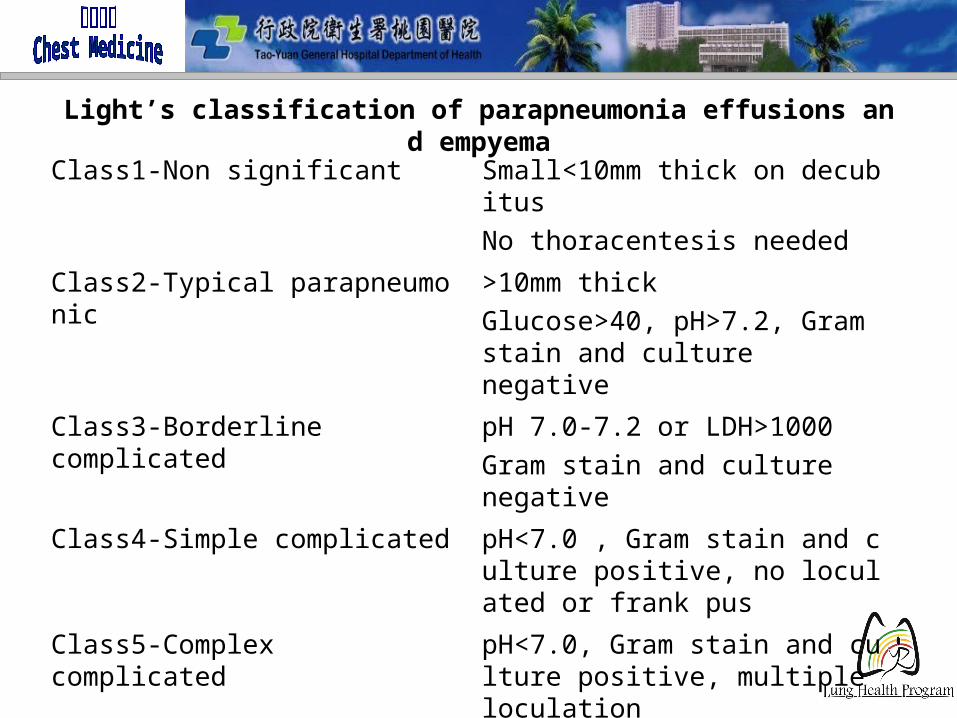
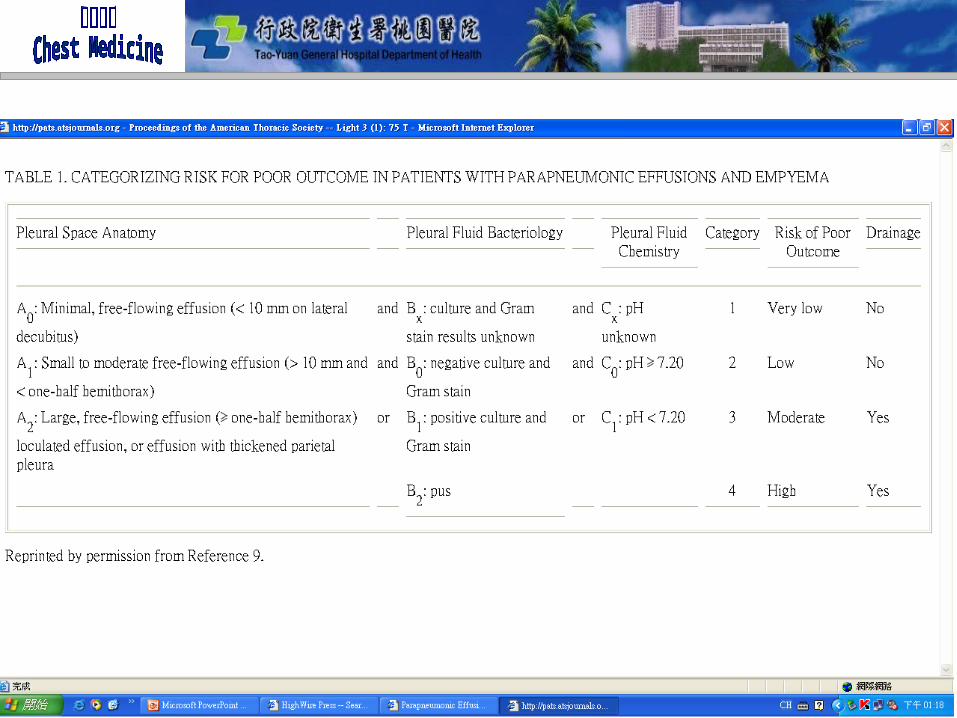
Light’s classification of parapneumonia effusions and empyema
Class1-Non significant Small<10mm thick on decubitus
No thoracentesis needed
Class2-Typical parapneumonic >10mm thick
Glucose>40, pH>7.2, Gram stain and culture negative
Class3-Borderline complicated pH 7.0-7.2 or LDH>1000
Gram stain and culture negative
Class4-Simple complicated pH<7.0 , Gram stain and culture positive, no loculated or frank pus
Class5-Complex complicated pH<7.0, Gram stain and culture positive, multiple loculation
Class 6-Simple empyema Frank pus, single locule or free
Class 7-Complex empyema Frank pus, multiple loculations
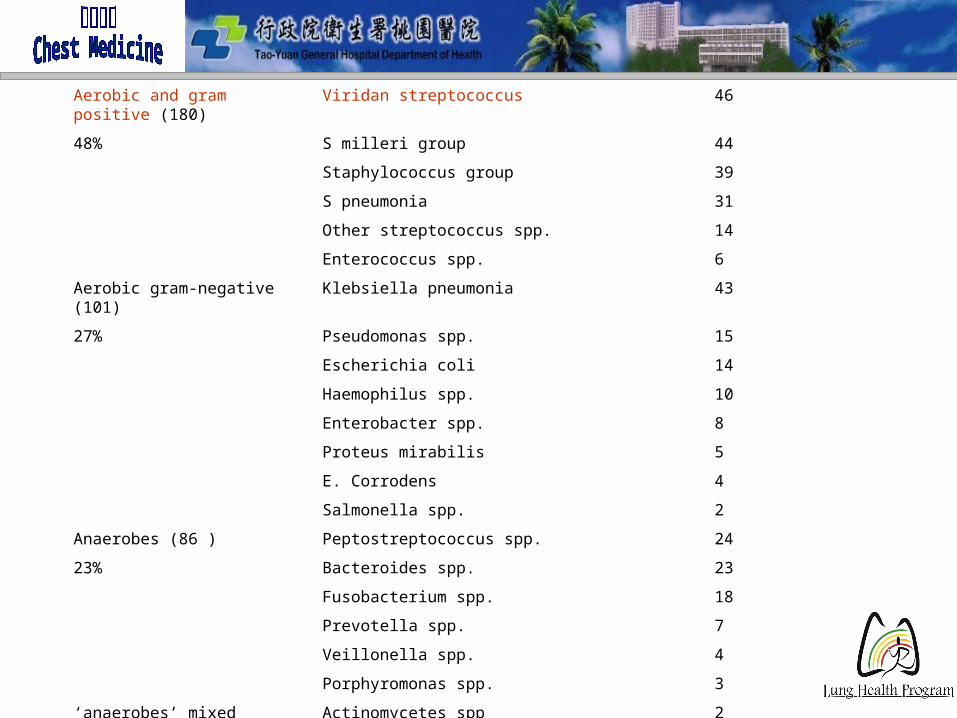
Aerobic and gram positive (180) Viridan streptococcus 46
48% S milleri group 44
Staphylococcus group 39
S pneumonia 31
Other streptococcus spp. 14
Enterococcus spp. 6
Aerobic gram-negative (101) Klebsiella pneumonia 43
27% Pseudomonas spp. 15
Escherichia coli 14
Haemophilus spp. 10
Enterobacter spp. 8
Proteus mirabilis 5
E. Corrodens 4
Salmonella spp. 2
Anaerobes (86 ) Peptostreptococcus spp. 24
23% Bacteroides spp. 23
Fusobacterium spp. 18
Prevotella spp. 7
Veillonella spp. 4
Porphyromonas spp. 3
‘anaerobes’ mixed Actinomycetes spp 2
Miscellaneous/ Others (8 ) 2%
Bacteriology• Aerobic organisms are the most frequent organi
sms identified from infected pleural fluid.• These are most commonly Gram-positive organi
sms from Streptococcal species, followed by Staphylococcus aureus.
• Gram-negative empyema is more frequent in patients with underlying diseases, especially those with diabetes and alcoholism.
• Staphylococcus aureus and Gram-negative enteric bacteria such as Klebsiella pneumonia have a particular propensity to cause pleural infection.
NICK A MASKELL AND ROBERT JO DAVIES TEXTBOOK OF PLEURAL DISEASE
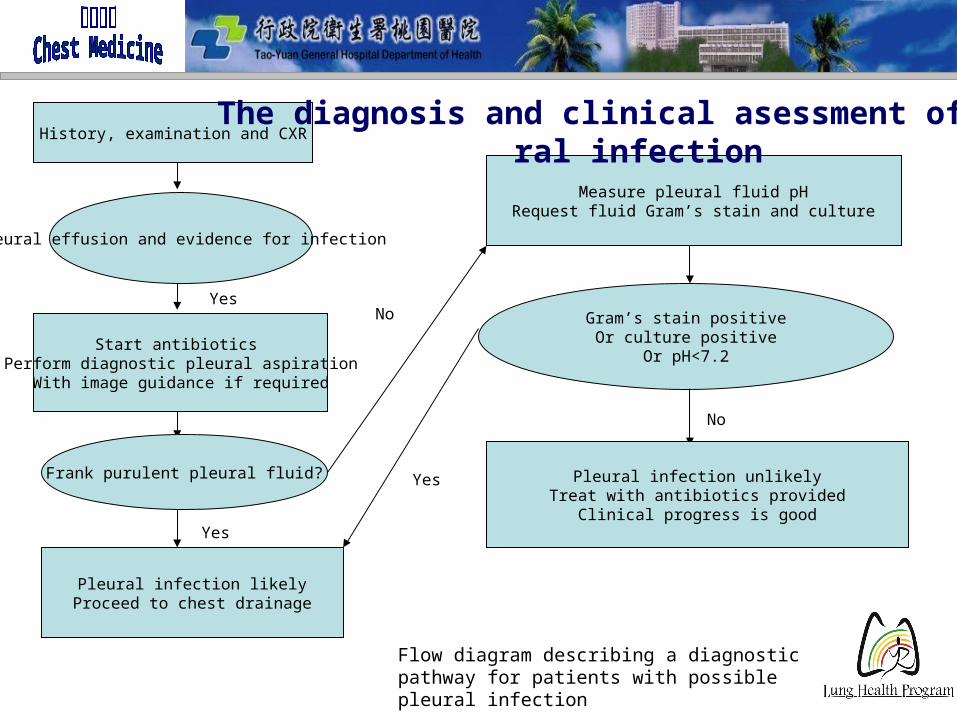
History, examination and CXR
Pleural effusion and evidence for infection
Start antibiotics Perform diagnostic pleural aspiration
With image guidance if required
Frank purulent pleural fluid?
Measure pleural fluid pHRequest fluid Gram’s stain and culture
No Gram’s stain positiveOr culture positive
Or pH<7.2
Pleural infection unlikelyTreat with antibiotics provided
Clinical progress is good
No
Pleural infection likelyProceed to chest drainage
Yes
Yes
Yes
Flow diagram describing a diagnostic pathway for patients with possible pleural infection
The diagnosis and clinical asessment of pleural infection
Differential diagnosis• Pleural involvement occurs in up to 5
% of patients with rheumatoid arthritis.
• Pleural malignancy• Chylothorax and pseudochylous effusi
on• Pulmonary embolism• Esophageal ruptureNICK A MASKELL AND ROBERT JO DAVIES
TEXTBOOK OF PLEURAL DISEASE
Predictors of clinical outcome in pleural infection• Pleural infection has a high mortality an
d morbidity and presents a clinical challenge in the timing of surgical intervention.
• Frankly purulent pleural fluid, co-morbid diabetes, delayed referral and pleural drainage, the presence of fluid loculation and a low pleural fluid white count may predict a poor outcome.
NICK A MASKELL AND ROBERT JO DAVIES TEXTBOOK OF PLEURAL DISEASE
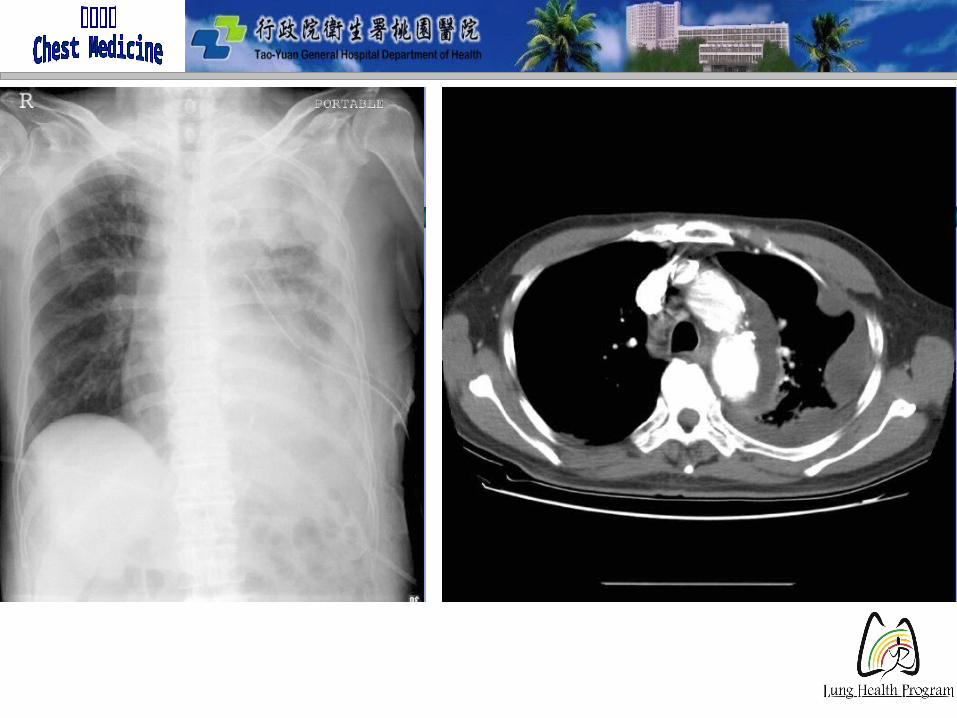
Radiology
• The presence of fever, pulmonary infiltrates and fluid should always alert clinician to the possibility of a parapneumonic collection.
• Ultrasound is good visualizing septations within loculations that are not usually seen on CT images, but may not identify some separate fluid loculations in inaccessible areas of the thorax.
NICK A MASKELL AND ROBERT JO DAVIES TEXTBOOK OF PLEURAL DISEASE


Tu, C.-Y. et al. Chest 2004;126:1274-1280
Five basic ultrasound patterns of pleural effusions
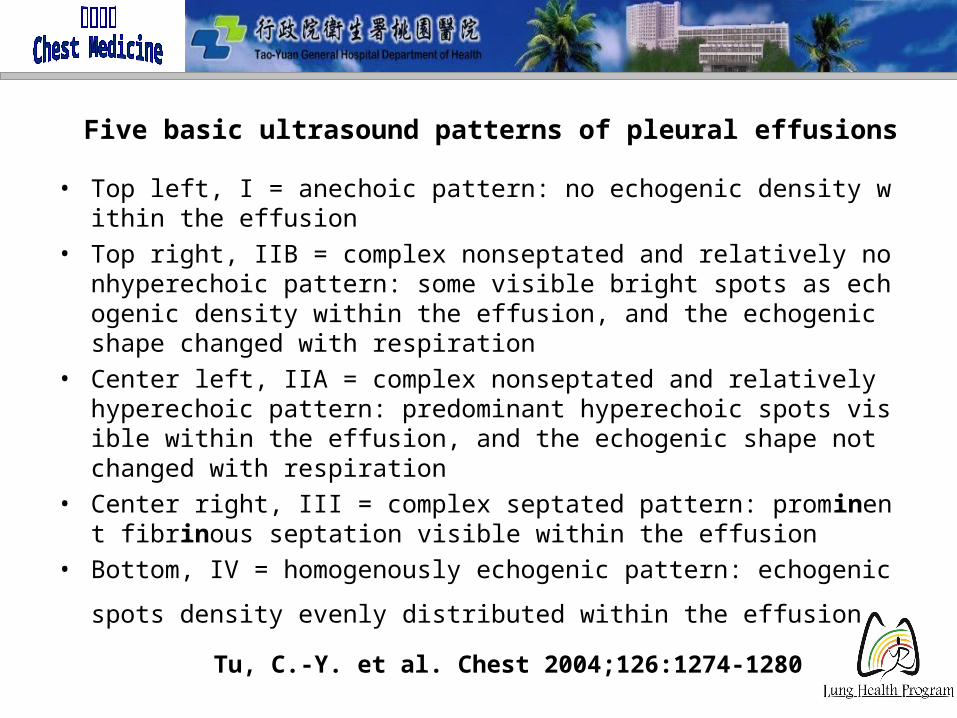
• Top left, I = anechoic pattern: no echogenic density within the effusion
• Top right, IIB = complex nonseptated and relatively nonhyperechoic pattern: some visible bright spots as echogenic density within the effusion, and the echogenic shape changed with respiration
• Center left, IIA = complex nonseptated and relatively hyperechoic pattern: predominant hyperechoic spots visible within the effusion, and the echogenic shape not changed with respiration
• Center right, III = complex septated pattern: prominent fibrinous septation visible within the effusion
• Bottom, IV = homogenously echogenic pattern: echogenic spots den
sity evenly distributed within the effusion
Five basic ultrasound patterns of pleural effusions
Tu, C.-Y. et al. Chest 2004;126:1274-1280
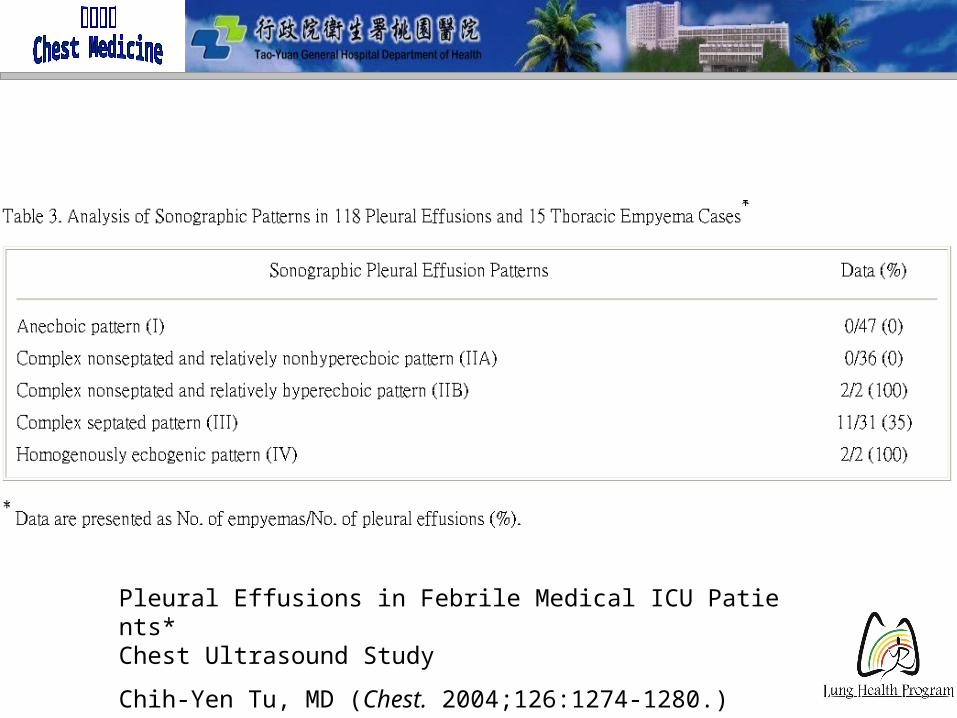
Pleural Effusions in Febrile Medical ICU Patients* Chest Ultrasound Study
Chih-Yen Tu, MD (Chest. 2004;126:1274-1280.)
Antibiotics
• Antibiotics• 40% culture negative• It is not uncommon to need at least 2
weeks of therapy and some times longer.
• Decisions on the length of treatment can be guided by repeated measurements of serum CRP.
NICK A MASKELL AND ROBERT JO DAVIES TEXTBOOK OF PLEURAL DISEASE
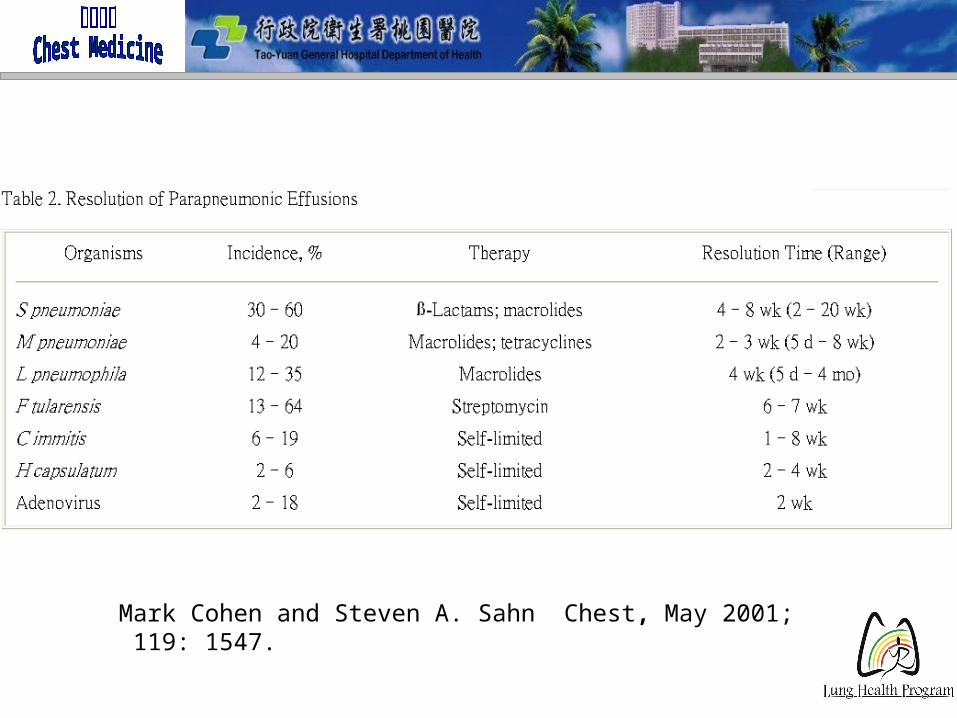
Mark Cohen and Steven A. Sahn Chest, May 2001; 119: 1547.
Chest catheter drainage• Optimal size of catheter?• Excellent outcomes may be achieved with such small cath
eter especially when combined with fibrinolytic therapy.• Drainage may fail if the fluid is of high viscosity and direct
blocks the tube.• The balance of forces drawing it down the tube is inadequ
ate.• If the fluid is partitioned by fibrinous septaeFig.ppt.• The rapidity of chest tube drainage might be improved by i
ncreasing the drain size, but the successful drainage is unchanged.
• Here again, provide that the catheter is patent, its bore is irrelevant.
NICK A MASKELL AND ROBERT JO DAVIES TEXTBOOK OF PLEURAL DISEASE


Intrapleural fibrinolytics• 1949 Tillet and Sherry: partial purified streptococcal fibrin
olysin• Highly purified streptokinase: 250000IU• Urokinase: 100000IU• It form a complex with plasminogen that converts additio
nal circulating plasminogen to plasmin. Plasmin lyses fresh fibrin clot and digests prothrobin and fibrinogen.
• Improvement in the chest radiograph and greater volume pleural drainage, not outcome of mortality, surgical frequency, or hospital stay.
• Tube drainage with streptokinase and early surgical intervention showed reduced length of hospitalization
• Potential side effect: hemorrhage, pleuritic pain and feverNICK A MASKELL AND ROBERT JO DAVIES
TEXTBOOK OF PLEURAL DISEASE
Surgery for pleural infecetion• No definite data that define the point at which a p
atient with empyema should proceed to surgical intervention.
• Open thoracotomy with decortication• Mini-thoracotomy• Video-assisted thoracoscopic surgery (VATS)• Rib resection with open drainage• VATS: reduced hospital inpatient time, postoperat
ive complications and length of operating time• VATS: failures are with empyema in the organizing
stage of the diseaseNICK A MASKELL AND ROBERT JO DAVIES
TEXTBOOK OF PLEURAL DISEASE

Copyright ©2003 BMJ Publishing Group Ltd.
Jaffe, A et al. Arch Dis Child 2003;88:839-841
Figure 2 Surgical scars: open decortication.

Copyright ©2003 BMJ Publishing Group Ltd.
Jaffe, A et al. Arch Dis Child 2003;88:839-841
Figure 1 Surgical scars: VATS.
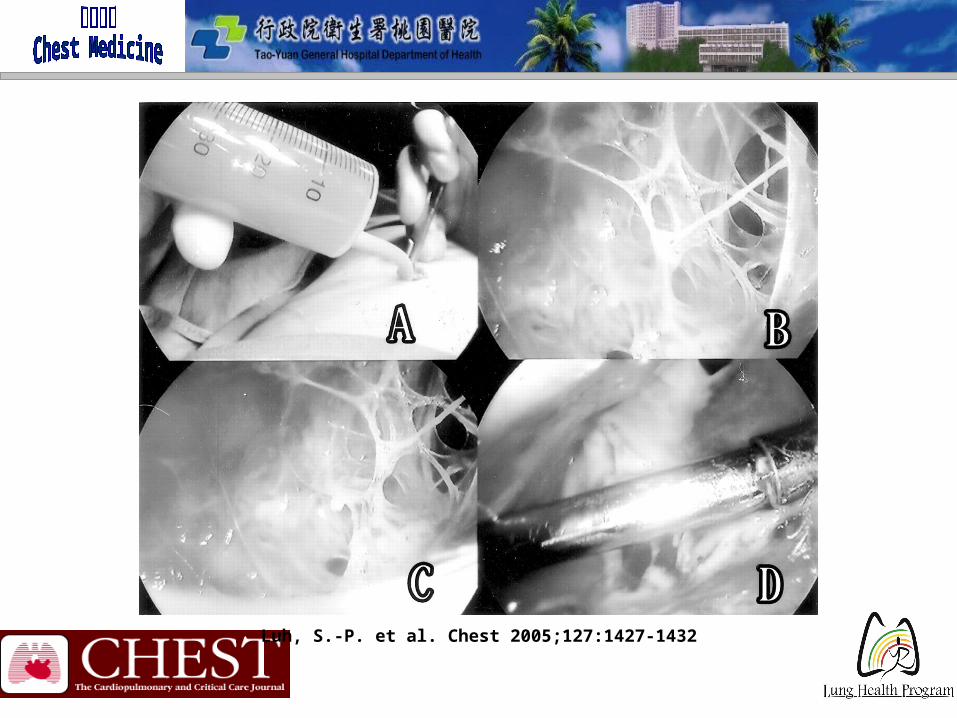
Luh, S.-P. et al. Chest 2005;127:1427-1432
Future Directions
• Increasing resistant micro-organism• intrapleural fibrinolytics still no know
if they actually reduce mortality and need for surgical intervention.
• Comparing the use of intrapleural fibrinolytics with early VATS
NICK A MASKELL AND ROBERT JO DAVIES TEXTBOOK OF PLEURAL DISEASE

THANKS FOR YOUR ATTENTION