Embed Size (px)
DESCRIPTION
结直肠肿瘤病理诊断和治疗中的 几个新概念. 来 茂 德 二 O 一 0 年四月十六日. 一 . 恶性息肉. NCCN 对定义 原先是良性腺瘤(息肉),恶变后癌组织浸润超过黏膜肌层到达黏膜下层( pT1 ). 癌组织浸润不超过黏膜肌层不会发生转移 这个概念病理医生和临床医生都接受, 理解是一致的。病理的高级别上皮内瘤变(重度异型增生和原位癌)和黏膜内瘤变(黏膜内癌)都归入 pTNM 分期的 pTis 。. 恶性息肉. 有蒂 ( pedunculated polyp with invasive cancer ). - PowerPoint PPT Presentation
Citation preview
来 茂 德
二 O 一 0 年四月十六日
结直肠肿瘤病理诊断和治疗中的几个新概念
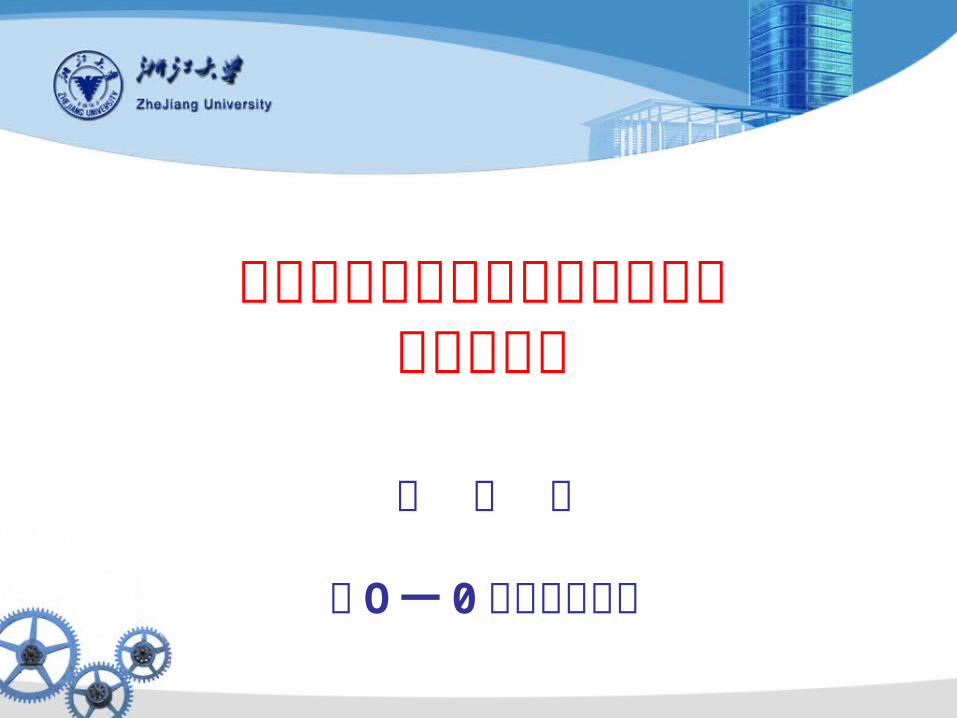
一 . 恶性息肉
• NCCN 对定义
原先是良性腺瘤(息肉),恶变后癌组织浸润超过黏膜肌层到达黏膜下层( pT1)

癌组织浸润不超过黏膜肌层不会发生转移 这个概念病理医生和临床医生都接受, 理解是一致的。病理的高级别上皮内瘤变
(重度异型增生和原位癌)和黏膜内瘤变(黏膜内癌)都归入 pTNM 分期的 pTis 。
Company Logo
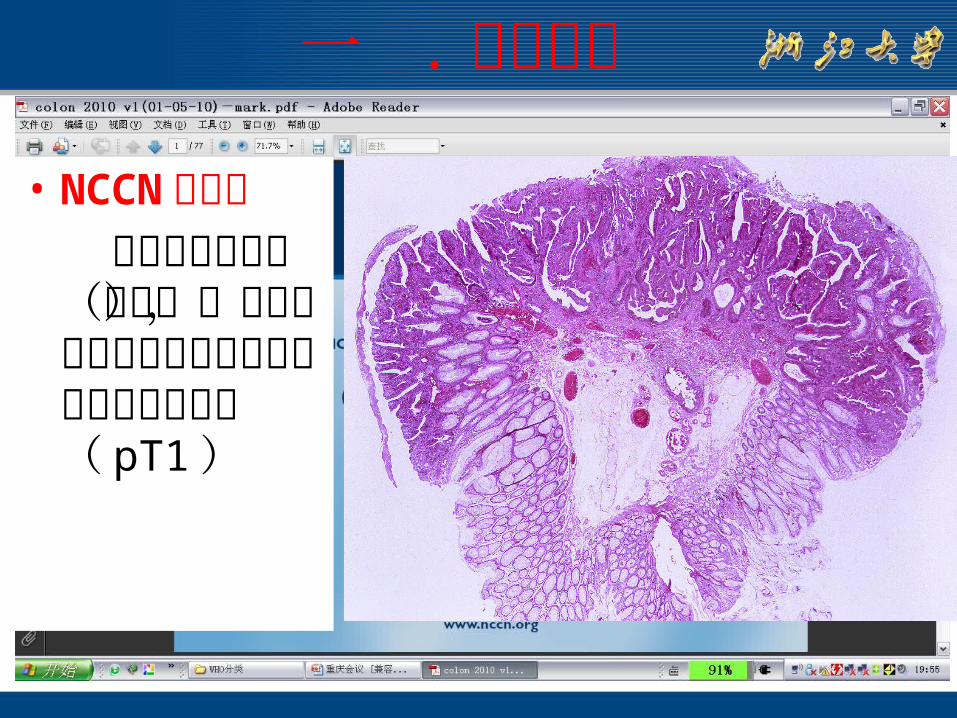
有蒂( pedunculated polyp with invasive cancer )
恶性息肉
无蒂 (sessile polyp with invasive cancer)
如是单一息肉内镜下切除干净,病理组织学检查为良好的组织学特征,切缘阴性,可以观察,不做进一
步处理
无蒂息肉情况同前也可以观察,也可以作进一步的外科手术(局部结肠和区域淋巴结的整块
切除)良好的组织学特征 : 分级 1-2 级, 无脉管浸润,切缘阴性; 不良组织学 : 分级 3-4 级,有脉管累犯,切缘阳性
二 . 关于淋巴结的取材问题
• TNM II 期( pN0 )的确定至少要取 12 枚
• 定义: pNx 不能确定 ,pN0 没有转移 , pN1a1 个有转移 ,pN1b2-3 个
有转移 pN1c 结肠的浆膜下有肿瘤细胞浸润或者结肠没有腹膜覆盖的部分的结肠或直肠周围组织有癌细胞的浸润,但没有区域淋巴结的转移
pN2a4-6 个转移 pN2b 有 7 个或 7 个以上的转移
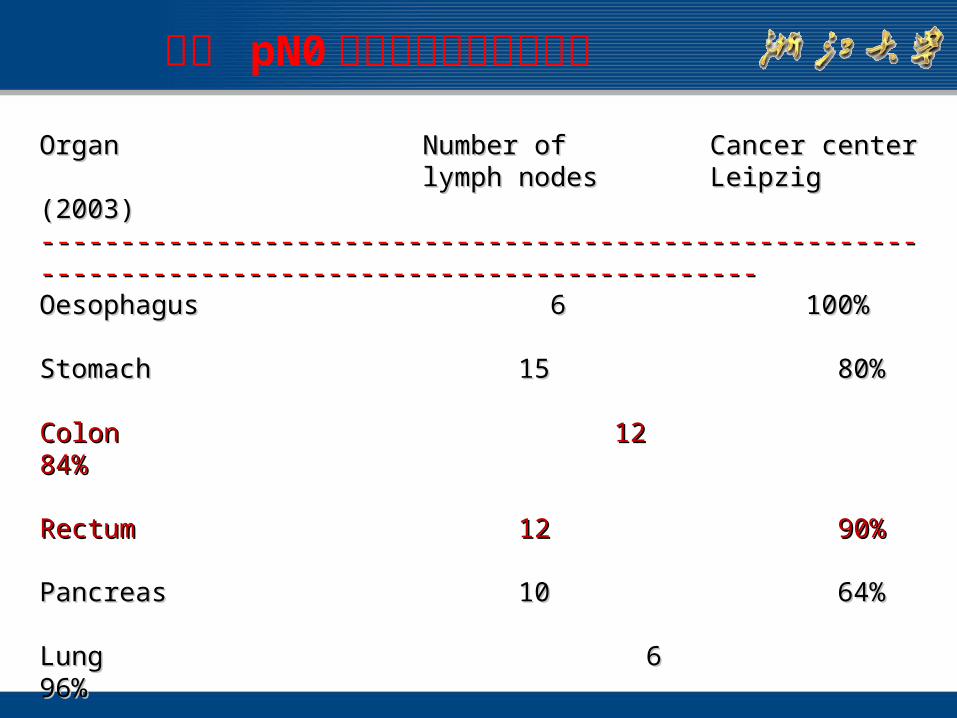
OrganOrgan Number ofNumber of Cancer centerCancer centerlymph nodeslymph nodes Leipzig (2003)Leipzig (2003)
--------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------Oesophagus Oesophagus 6 6 100%100%
StomachStomach 1515 80% 80%
Colon Colon 1212 84% 84%
Rectum Rectum 1212 90% 90%
PancreasPancreas 1010 64% 64%
Lung Lung 6 6 96% 96%
Breast Breast 6 6 98% 98%--------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
分类 pN0 所需检查的淋巴结数量
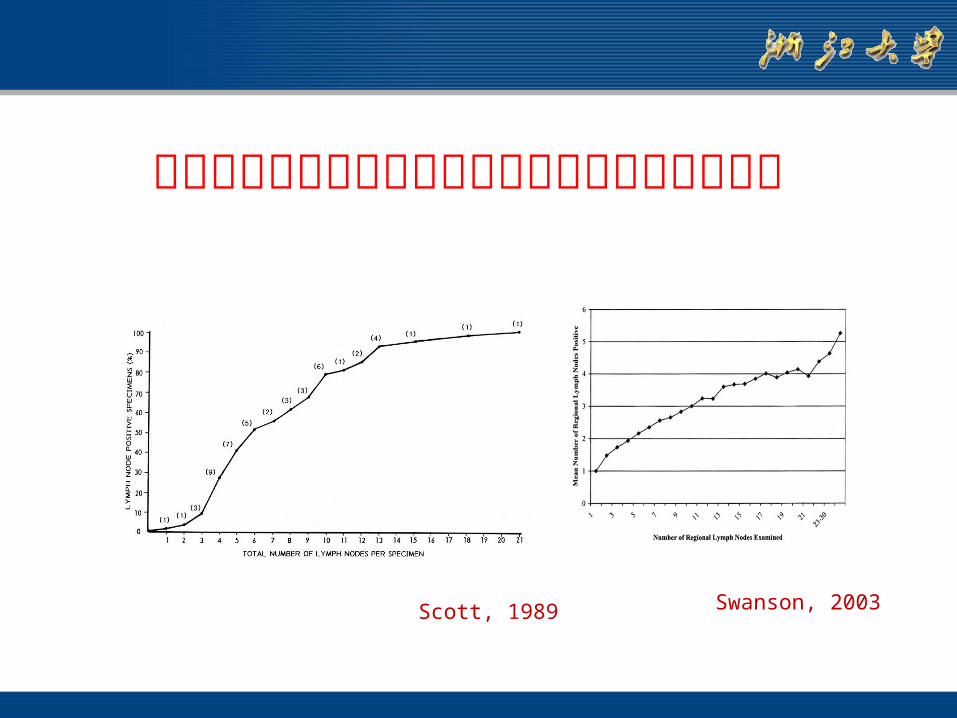
病人阳性淋巴结数随着所检淋巴结数的增加而增加
Scott, 1989 Swanson, 2003
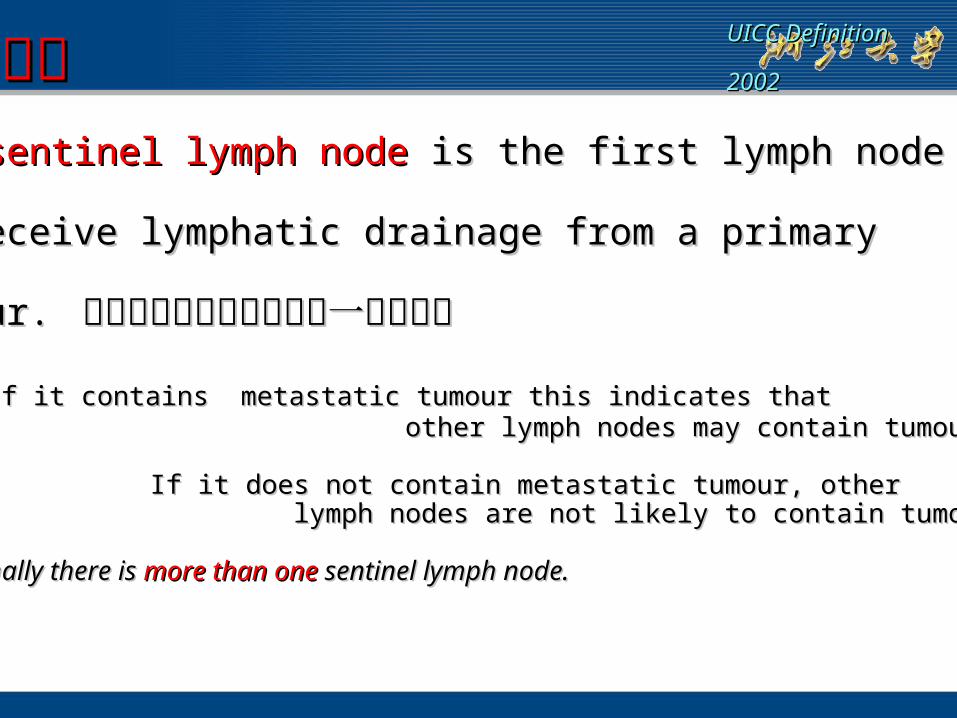
前哨淋巴结前哨淋巴结The The sentinel lymph node sentinel lymph node is the first lymph nodeis the first lymph node
to receive lymphatic drainage from a primaryto receive lymphatic drainage from a primary
tumour. tumour. 从原发瘤引流淋巴液的第一个淋巴结从原发瘤引流淋巴液的第一个淋巴结
意义:意义: If it contains metastatic tumour this indicates thatIf it contains metastatic tumour this indicates that other lymph nodes may contain tumour. other lymph nodes may contain tumour.
If it does not contain metastatic tumour, otherIf it does not contain metastatic tumour, other lymph nodes are not likely to contain tumour.lymph nodes are not likely to contain tumour.
Occasionally there is Occasionally there is more than one more than one sentinel lymph node.sentinel lymph node.
UICC DefinitionUICC Definition
20022002
有关前哨淋巴结出现癌细胞是否确定为转移还没有大家都接受的定义。
一般认为淋巴结内肿瘤细胞灶大于 0.2mm ,而小于 2mm 者称为微转移
如小于 0.2mm 则称为孤立性肿瘤细胞 (isolated tumor cells,ITC) 。
TNM Classification of isolated tumour cells TNM Classification of isolated tumour cells
Isolated tumour cells (ITC) are single tumour cellsIsolated tumour cells (ITC) are single tumour cells
or small clusters of cells not more than 0.2mm inor small clusters of cells not more than 0.2mm in
greatest dimension that are greatest dimension that are usuallyusually detected by detected by
immunhistochemistry or molecular methods.immunhistochemistry or molecular methods.
ITCs do not typically show evidence of metastaticITCs do not typically show evidence of metastatic
activity (e.g., proliferation or stromal reaction) oractivity (e.g., proliferation or stromal reaction) or
penetration of vascular or lymphatic sinus walls.penetration of vascular or lymphatic sinus walls.
前哨淋巴结状态的表述前哨淋巴结状态的表述
pNX(sn)pNX(sn) Sentinel lymph node could noSentinel lymph node could nott be be
assessedassessed
pN0(sn) pN0(sn) No sentinel lymph node metastasisNo sentinel lymph node metastasis
pN1(sn)pN1(sn) Sentinel lymph node metastasisSentinel lymph node metastasis
UICC DefinitionUICC Definition
20022002
三 . 微乳头癌
• 微乳头结构是指排列紧密的肿瘤细胞团,周围包绕以裂隙,无中心纤维脉管束。其内的肿瘤细胞往往具有嗜酸性胞浆和多形性核。
• 微乳头结构很少独立存在,往往和其它组织学类型并存,当微乳头结构占肿瘤实质的 5% 以上时,可称之为微乳头癌。
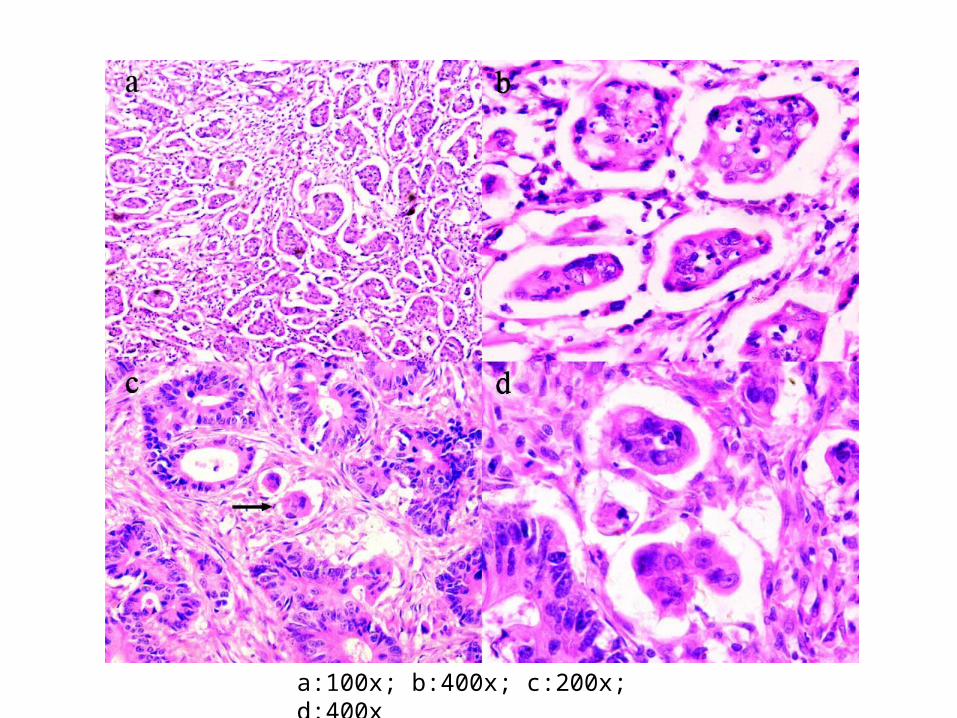
a:100x; b:400x; c:200x; d:400x
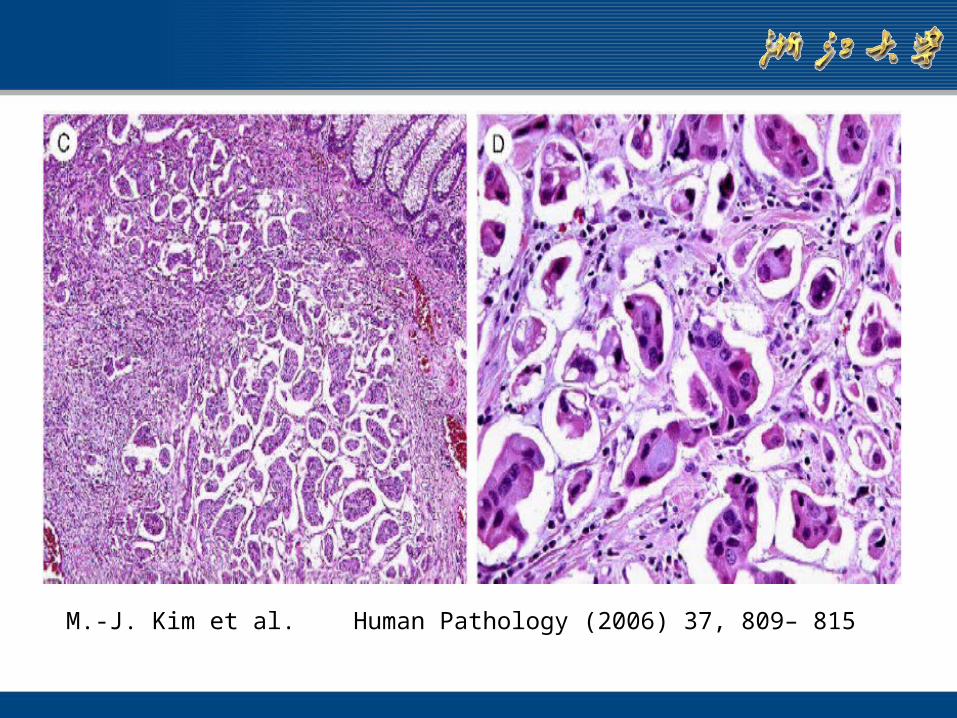
M.-J. Kim et al. Human Pathology (2006) 37, 809– 815
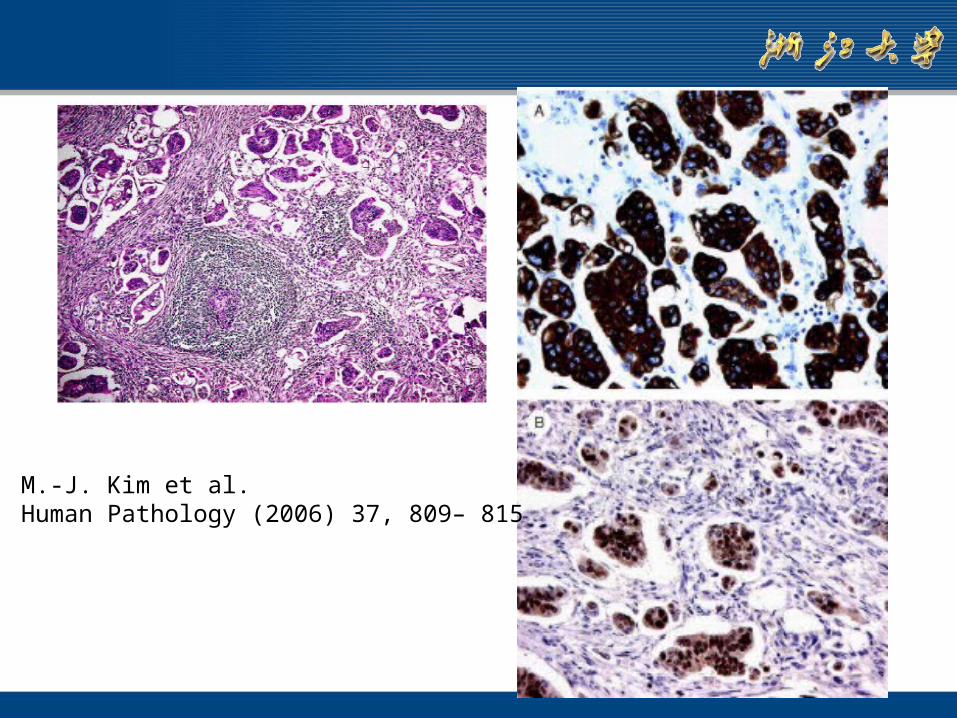
M.-J. Kim et al.Human Pathology (2006) 37, 809– 815
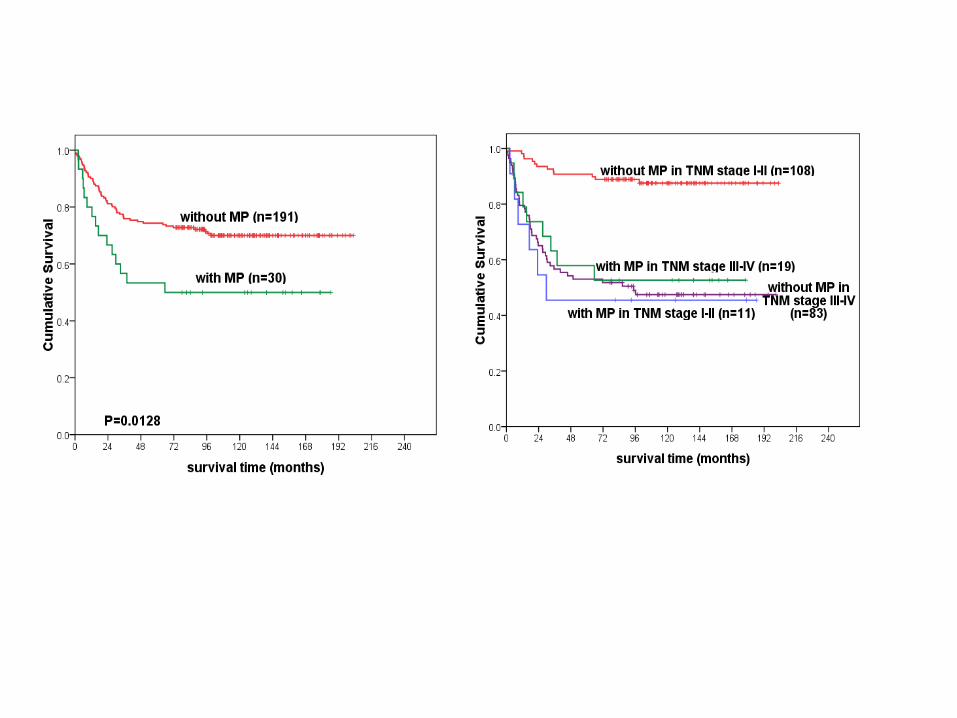
• 一般而言,微乳头结构所占比例的多少和结直肠癌的发展和预后并无关系。微乳头结构存在时, T1-2 期结直肠癌患者中淋巴结转移发生率更高, TNMI-II 期患者的预后更差
• 微乳头结构的判断对于早期结直肠癌患者的诊断和后续治疗选择很有意义。
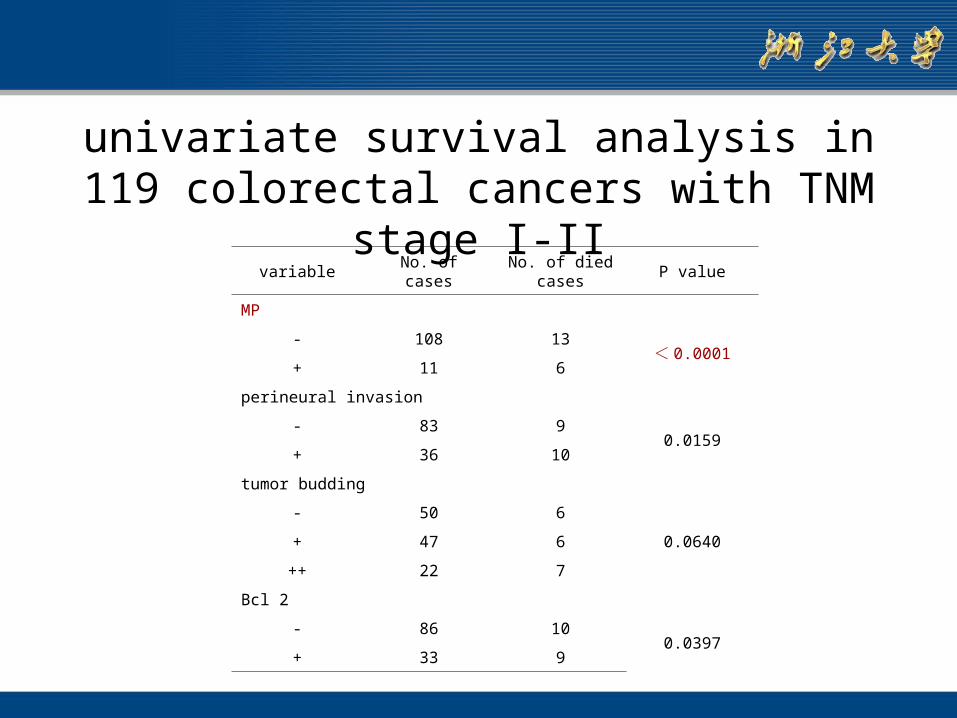
univariate survival analysis in 119 colorectal cancers with TNM stage I-II
variable No. of cases No. of died cases P value
MP
- 108 13< 0.0001
+ 11 6
perineural invasion
- 83 90.0159
+ 36 10
tumor budding
- 50 6
0.0640+ 47 6
++ 22 7
Bcl 2
- 86 100.0397
+ 33 9
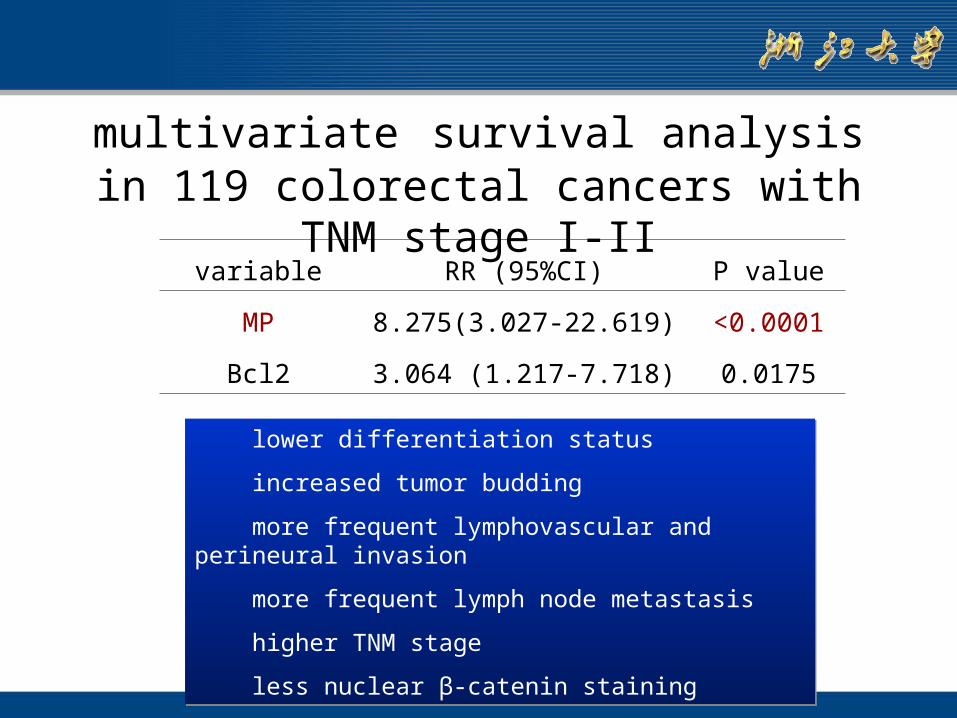
multivariate survival analysis in 119 colorectal cancers with TNM stage I-II
variable RR (95%CI) P value
MP 8.275(3.027-22.619) <0.0001
Bcl2 3.064 (1.217-7.718) 0.0175
lower differentiation status
increased tumor budding
more frequent lymphovascular and perineural invasion
more frequent lymph node metastasis
higher TNM stage
less nuclear β-catenin staining
lower differentiation status
increased tumor budding
more frequent lymphovascular and perineural invasion
more frequent lymph node metastasis
higher TNM stage
less nuclear β-catenin staining
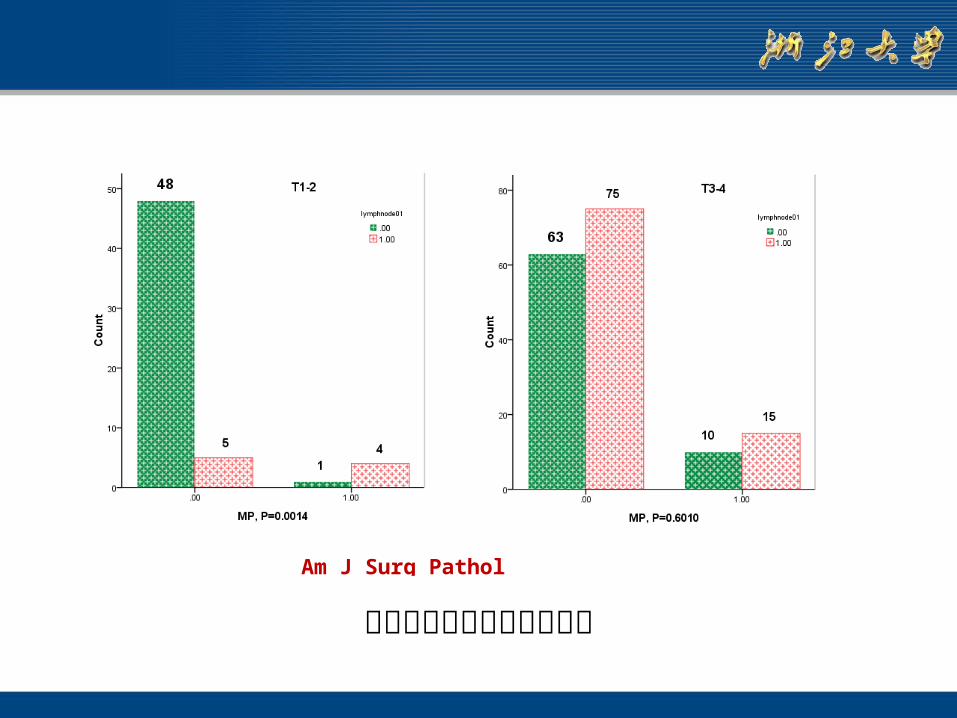
Am J Surg Pathol 2009,33(9):1287-92
微乳头与淋巴结转移的关系
四 . 微卫星不稳定检测
• 如是高频MSI 则很可能是 HNPCC ,应该对其家属进行筛查,有利于早期发现病人或突变基因携带者。
• 高频MSI 肿瘤病人预后较好,而且对基于5-Fu 为基础的化疗较低频或稳定的肿瘤更为有效。
50岁以前发生的结直肠癌或者结直肠癌伴发有 HNPCC相关癌如胃癌,宫内膜癌,肾盂肾盏癌应该检测MSI
一般使用 1998 年 NCI推荐的 5 个位点的检测方法。没有条件的单位可以用免疫组织化学方法检测MLH1,MSH2,MSH6和 PMS蛋白的表达来初筛。
MSS: No microsatellite instabilityMSI-L: 1 instable markerMSI-H: 2 instable markers
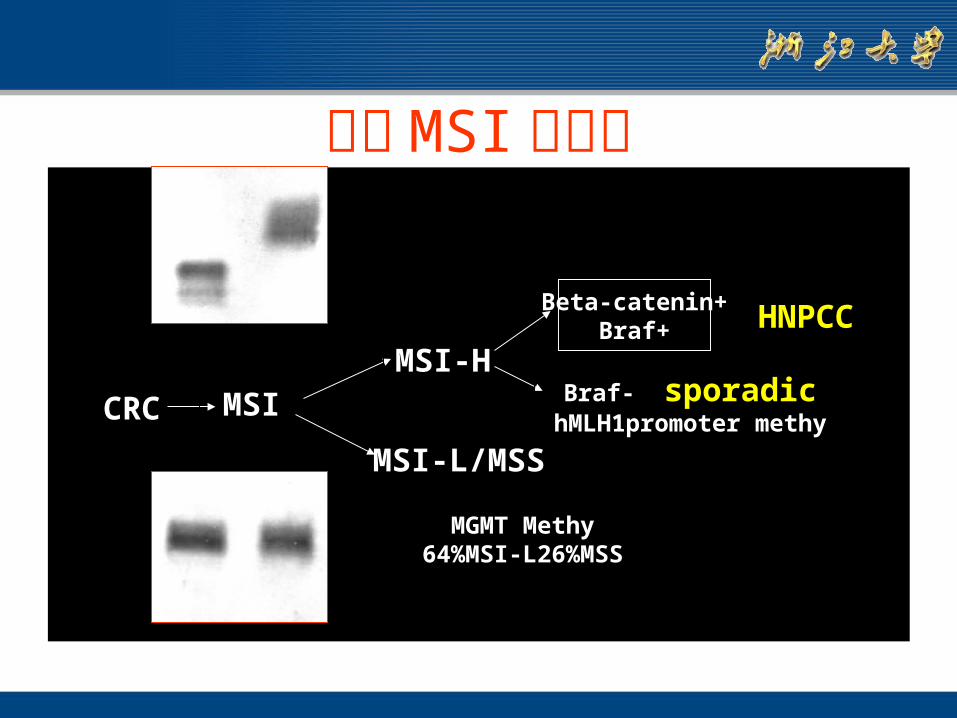
基于 MSI 的分类
• CRCCRC MSI
MSI-H
Beta-catenin+Braf+ HNPCC
MSI-L/MSS
Braf- sporadichMLH1promoter methy
MGMT Methy64%MSI-L26%MSS
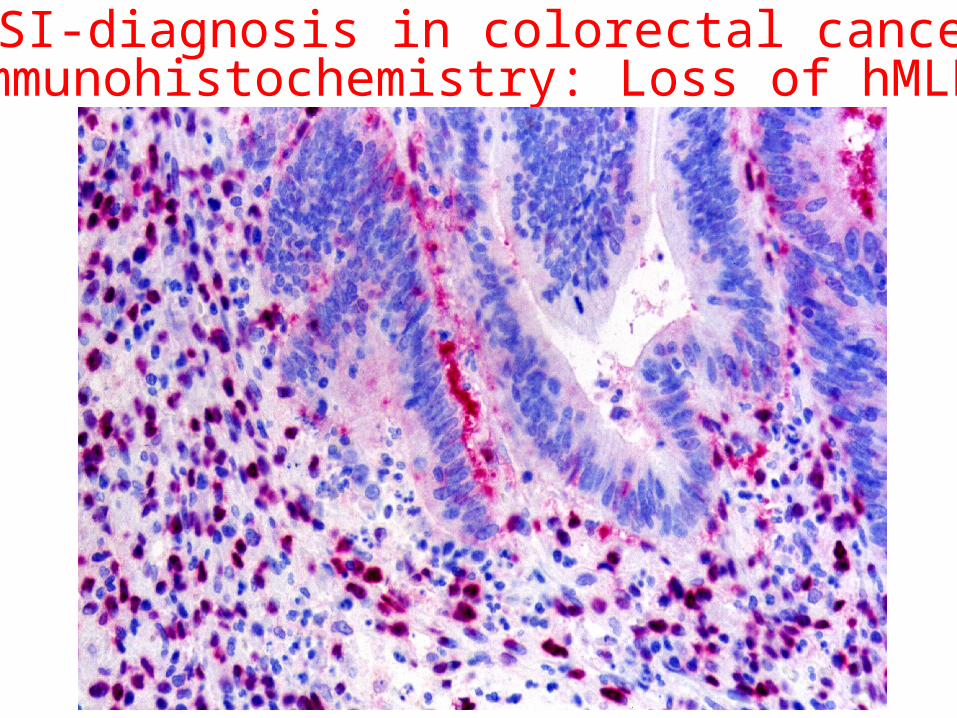
MSI-diagnosis in colorectal cancerImmunohistochemistry: Loss of hMLH1
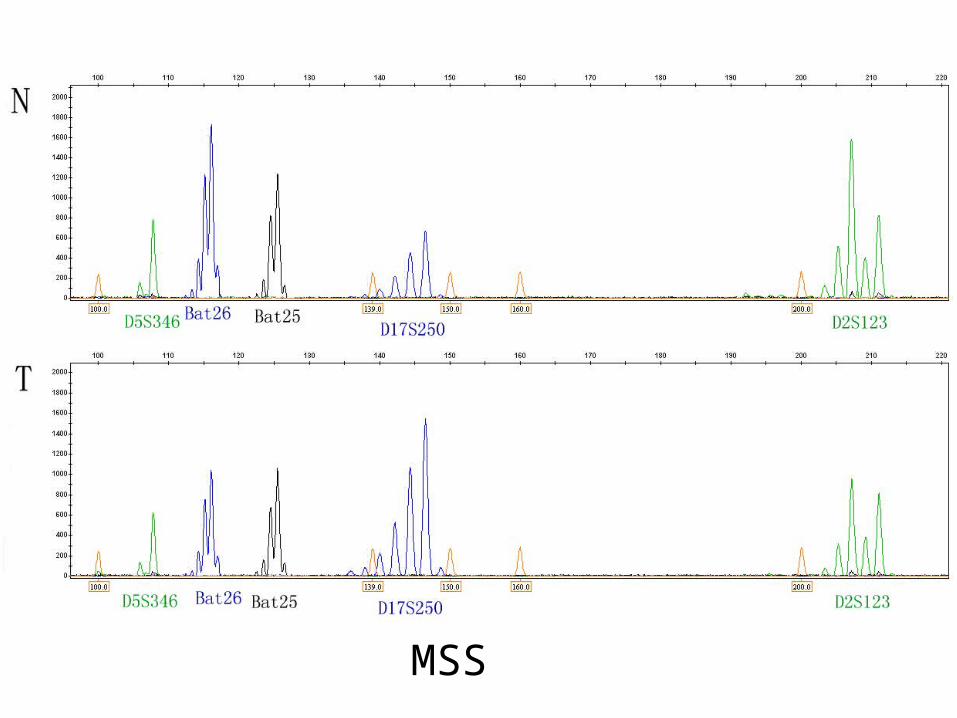
MSS
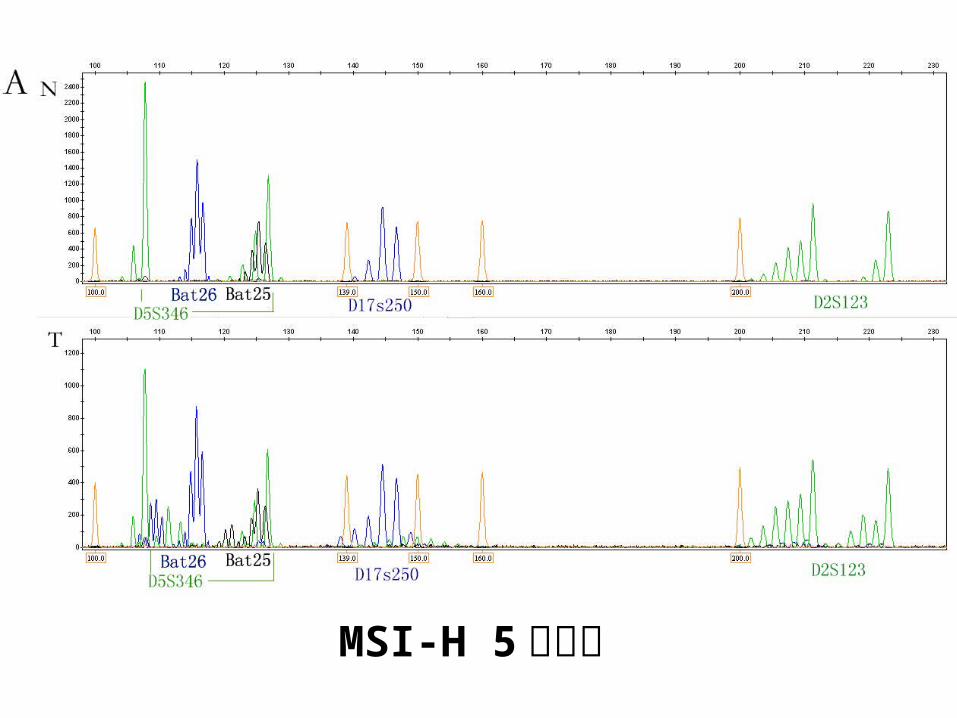
MSI-H 5 个位点
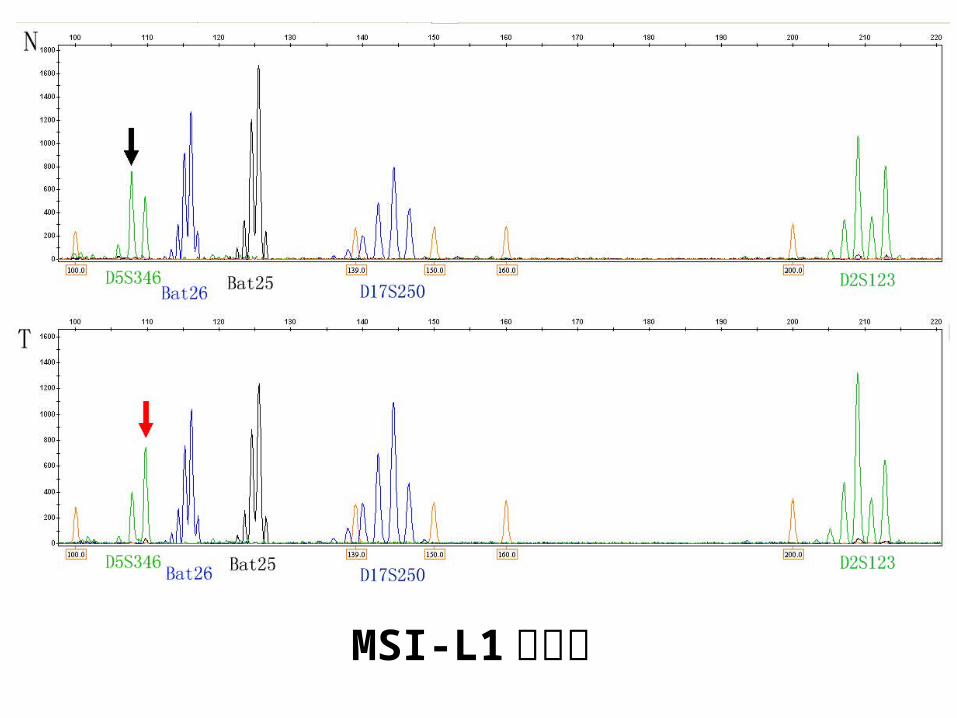
MSI-L1 个位点
临床意义
MSI-H CRC
Proximal colonic location
Mucinous and undifferentiated histology
Crohn’s lymphoid reaction
Better prognosis
Usually without liver metastasisAnd expansile growth pattern
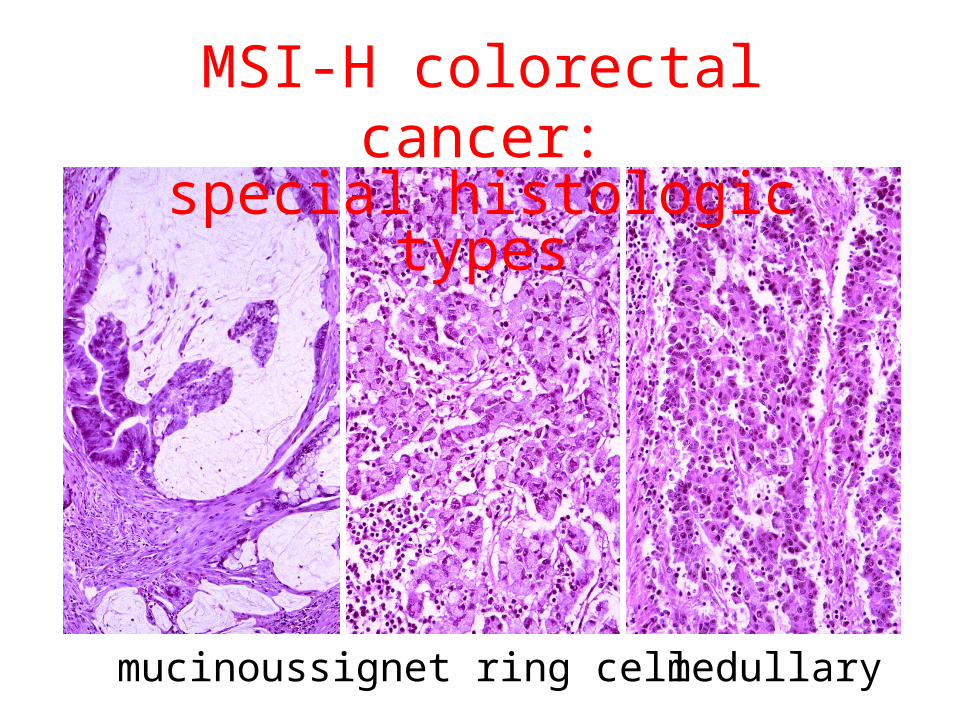
MSI-H colorectal cancer:special histologic types
mucinous signet ring cell medullary
六 .K-ras突变的检测
K-ras突变的检测在应用抗 EGFR抗体靶向治疗时必须要做,盲目用药不仅费用高还有毒副作用,而且以后还会有医疗纠纷。
有 K-ras突变的结直肠癌不能再用 ( cetuximab,panitumumab )。
B-raf V600E突变的检测也列入 NCCN标准。最近基本肯定 B-raf V600E突变的病例也不能用这种靶向治疗。
KRAS status 与靶向治疗
• July 2008 the european medicines evaluation agency has extended the approval for cetuximab to any line of treatment and any fluoropyrimidine-based chemotherapy combination in mCRC, but only in patients with a wild-type KRAS tumor.
• January 2009, American Society of Clinical Oncology published guidelines that strongly support the use of anti-EGFR drugs in mCRC only in patients with wild-type KRAS.
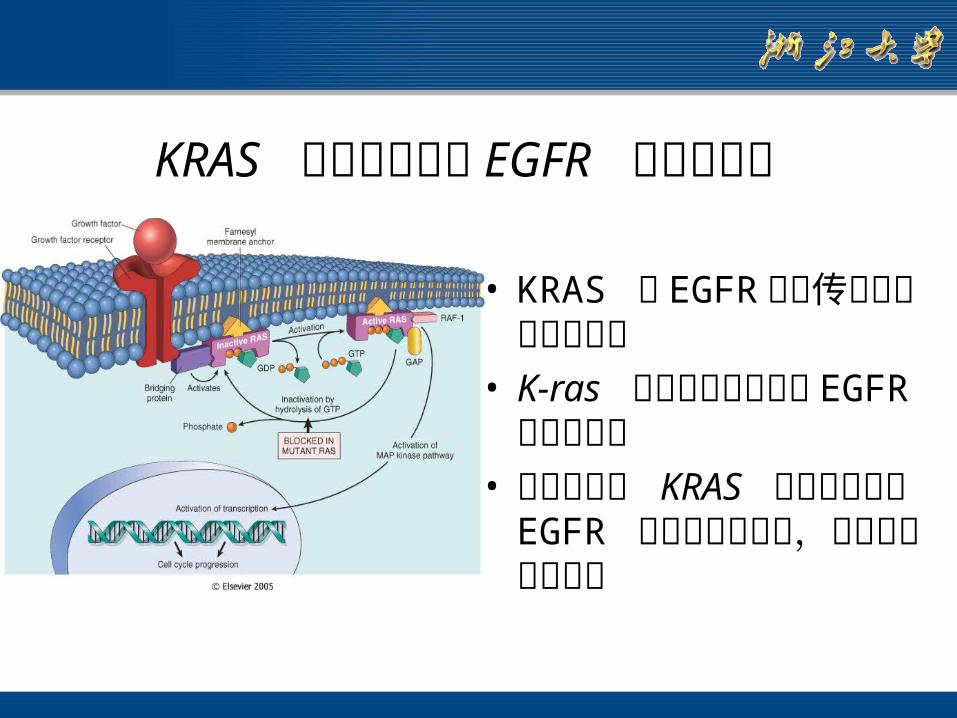
• KRAS 是 EGFR 信号传导下游的重要分子
• K-ras 突变病人不适合于EGFR 抑制剂治疗
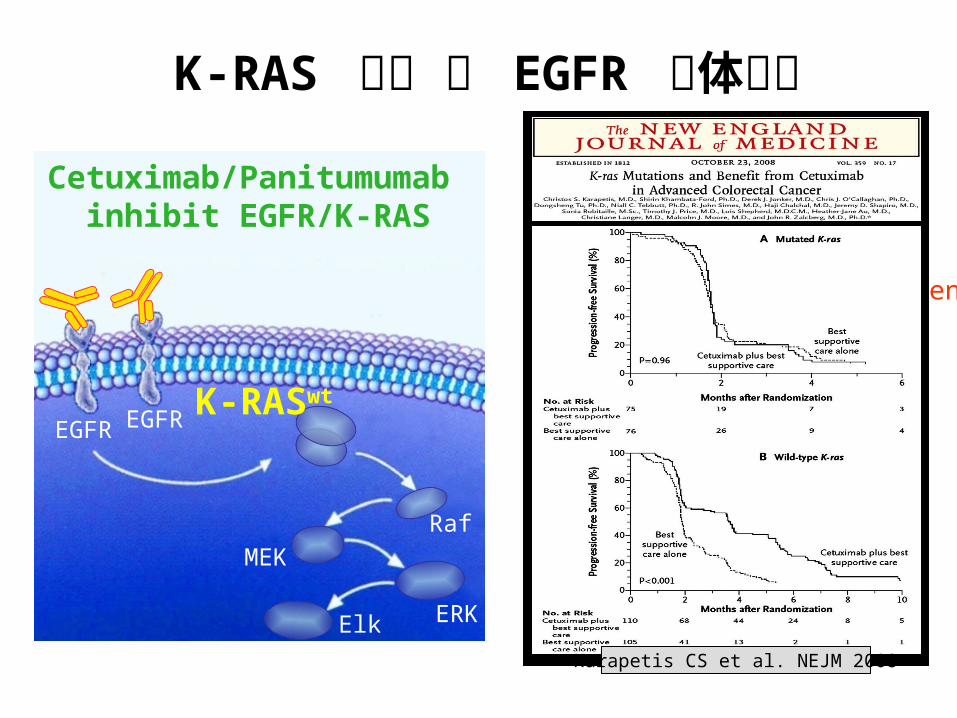
• 具有野生型 KRAS 基因的病人对 EGFR 抑制剂治疗反应,明显延长生存时间
KRAS 突变检测确定 EGFR 抑制剂治疗
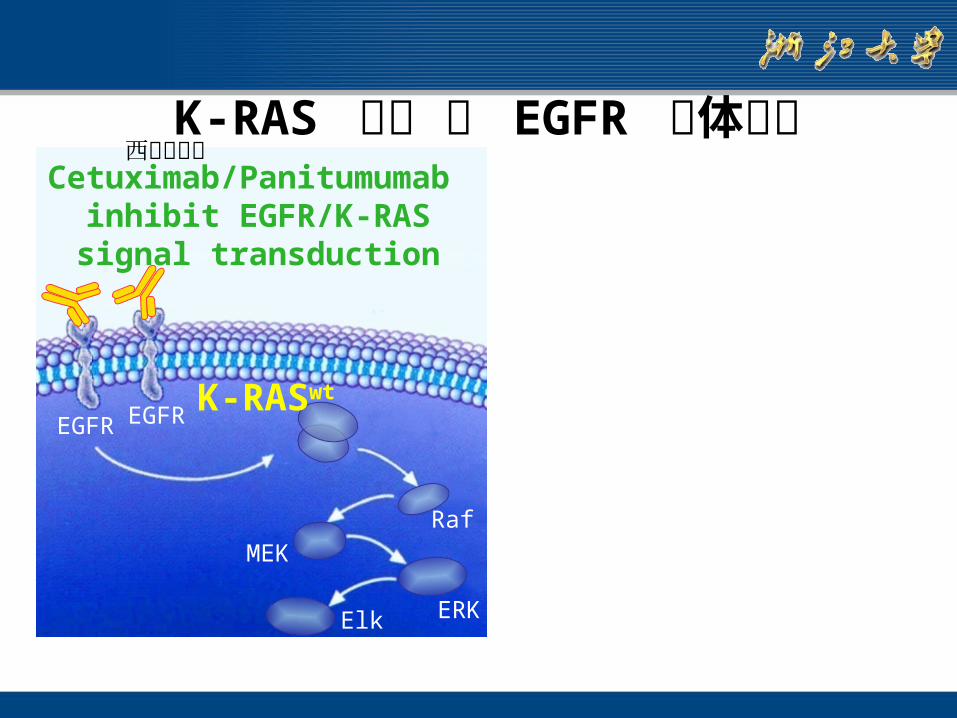
K-RAS 突变 和 EGFR 抗体治疗
K-RASwt
MEK
Elk
Raf
EGFREGFR
ERK
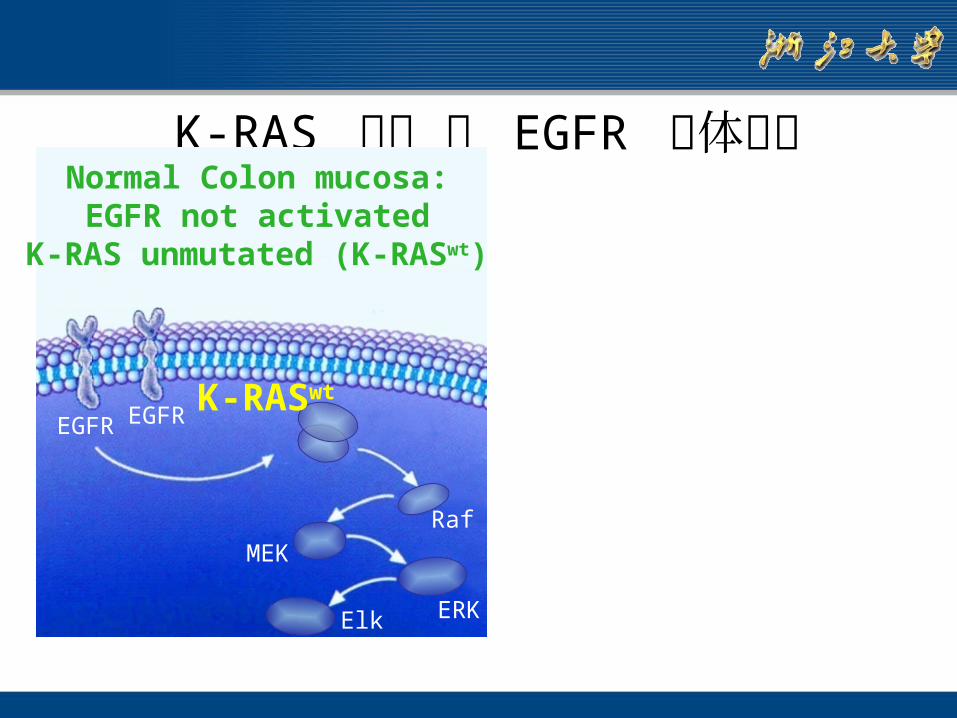
Normal Colon mucosa:EGFR not activated
K-RAS unmutated (K-RASwt)
K-RASwt
MEK
Elk
Raf
EGFREGFR
ERK
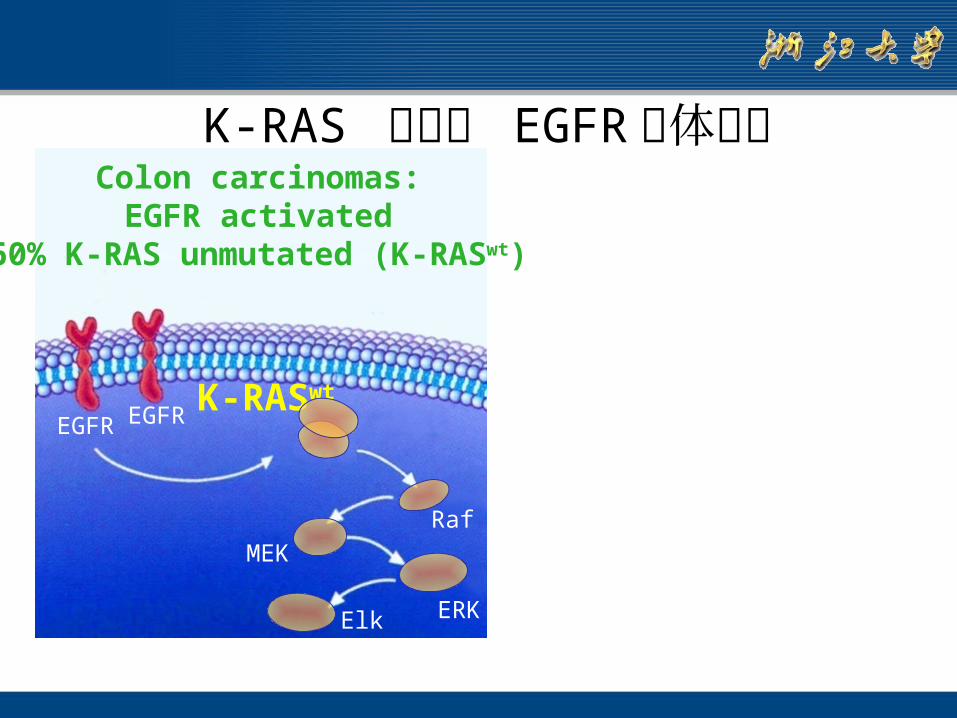
Colon carcinomas:EGFR activated
60% K-RAS unmutated (K-RASwt)
K-RAS 突变和 EGFR 抗体治疗
K-RASwt
MEK
Elk
Raf
EGFREGFR
ERK
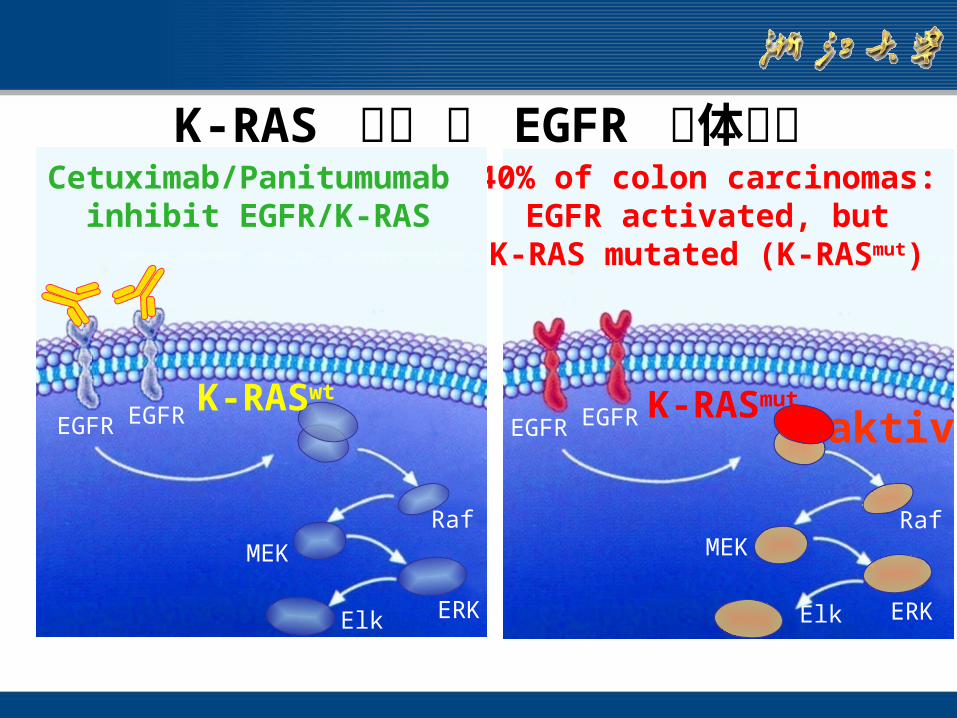
Cetuximab/Panitumumab inhibit EGFR/K-RASsignal transduction
K-RAS 突变 和 EGFR 抗体治疗西妥昔单抗
MEK
Elk ERK
Raf
aktivEGFREGFR
40% of colon carcinomas:EGFR activated, but
K-RAS mutated (K-RASmut)
K-RASmutK-RASwt
MEK
Elk
Raf
EGFREGFR
ERK
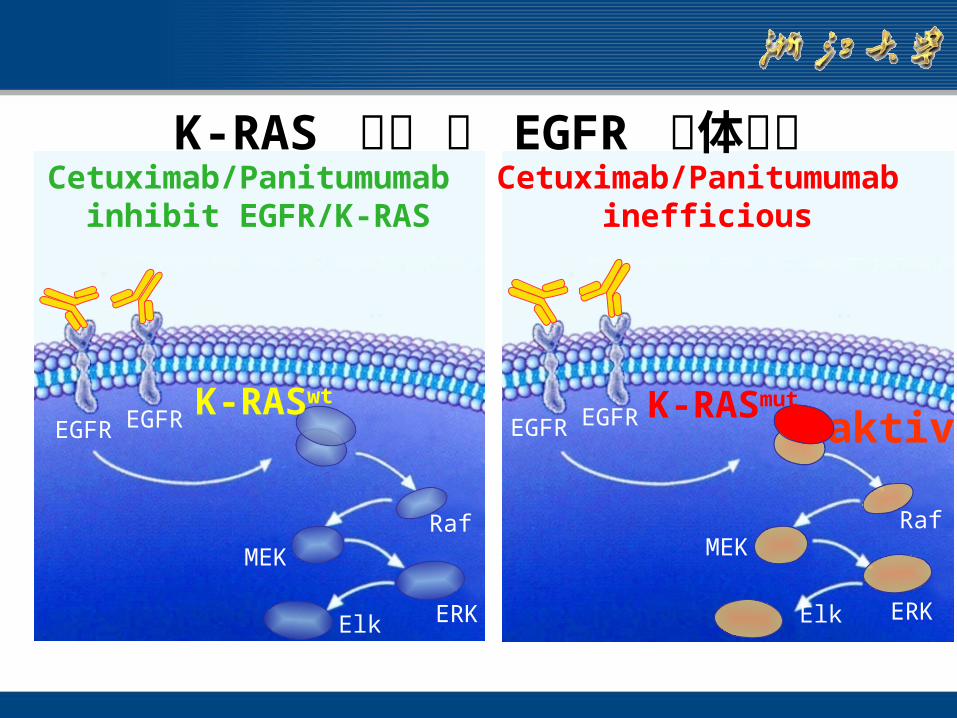
K-RAS 突变 和 EGFR 抗体治疗Cetuximab/Panitumumab
inhibit EGFR/K-RAS
K-RASwt
MEK
Elk
Raf
EGFREGFR
ERK
MEK
Elk ERK
Raf
aktivEGFREGFR
Cetuximab/Panitumumab inefficious
K-RASmut
K-RAS 突变 和 EGFR 抗体治疗Cetuximab/Panitumumab
inhibit EGFR/K-RAS
K-RASwt
MEK
Elk
Raf
EGFREGFR
ERK
Cetuximab/Panitumumab wirkungslos
ca. 40% der Patienten
EGFR EGFR
MEK
Elk
Rasmut
Karapetis CS et al. NEJM 2008
K-RAS 突变 和 EGFR 抗体治疗
Cetuximab/Panitumumab inhibit EGFR/K-RAS
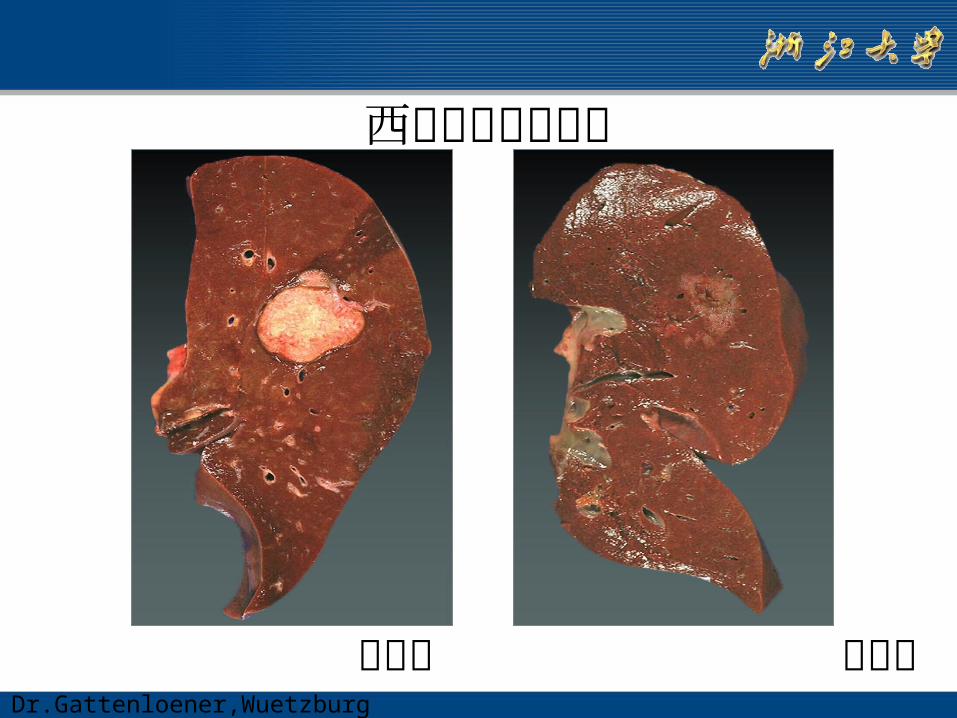
西妥昔治疗肝转移
治疗前 治疗后Dr.Gattenloener,Wuetzburg
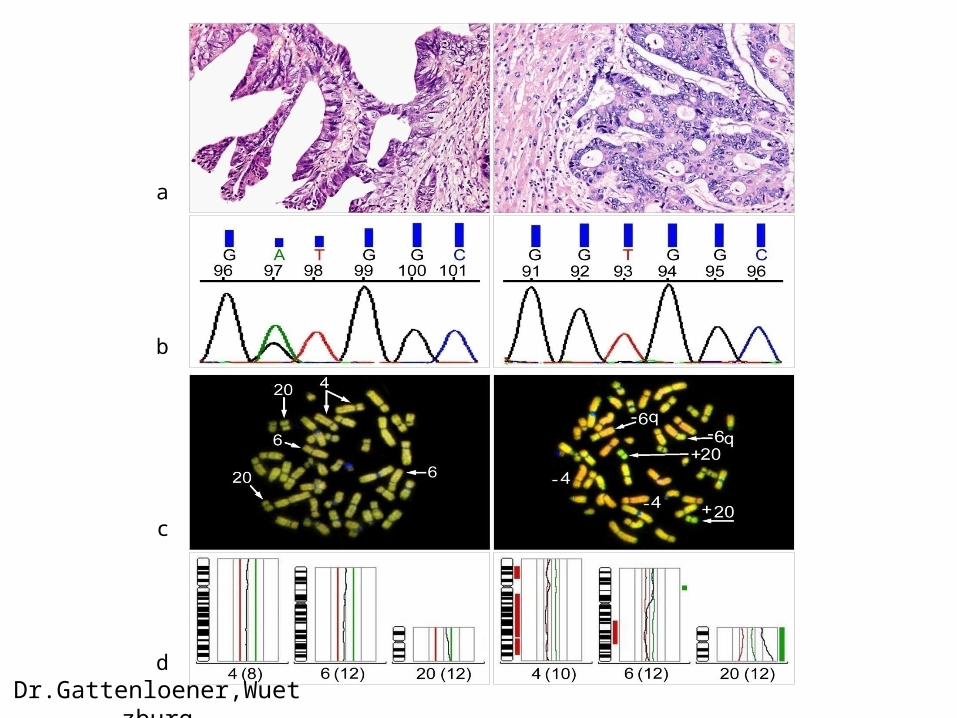
a
b
c
d
Dr.Gattenloener,Wuetzburg
KRAS突变的意义• KRAS mutations 与 sex, age, tumor
site or Dukes stage 无关• KRAS mutation 增加 recurrence and
death危险• Only the glycine to valine mutation in
codon 12 was found to retain an independent increased risk of
recurrence and death.
• KRAS mutations 病人较没有突变者 a worse outcome
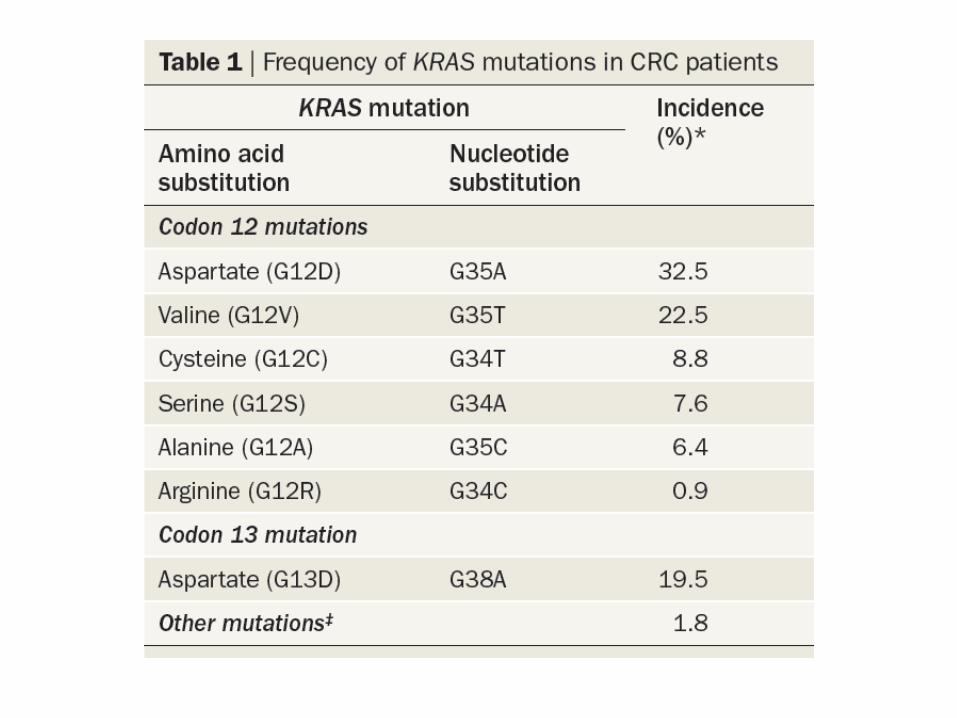
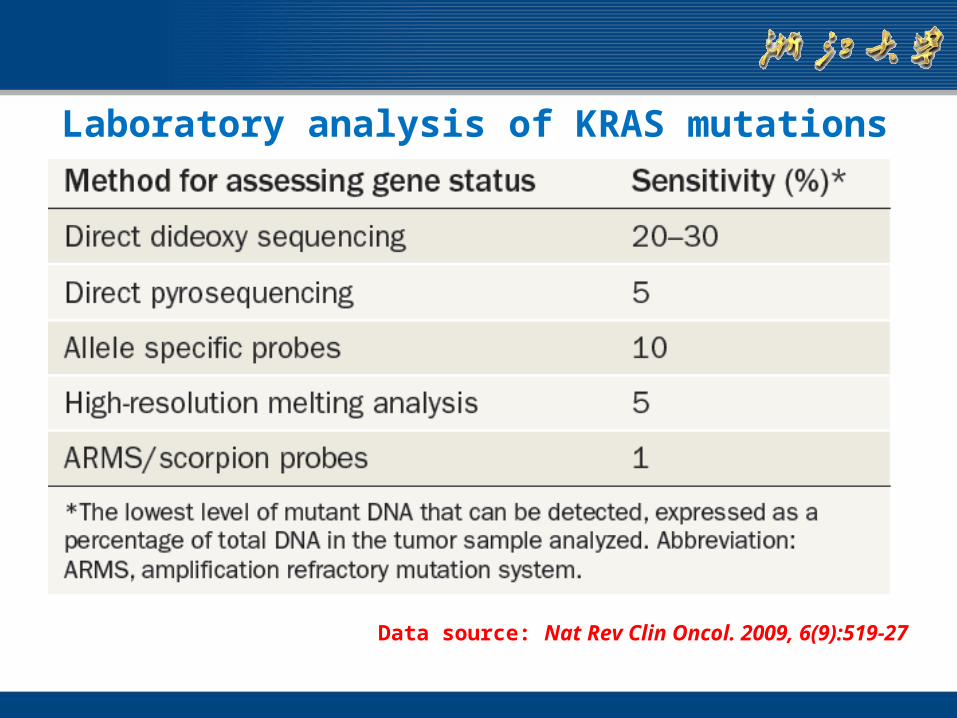
Laboratory analysis of KRAS mutations
Data source: Nat Rev Clin Oncol. 2009, 6(9):519-27

谢谢