-
8/22/2019 05_Retinal Vasculitis in SLE_Kessara
1/4
Chiang Mai Med J 2009;48(4):159-162.
Address requests for reprints: Kessara Pathanapitoon, M.D.,
Department of Ophthalmology, Faculty of Medicine,
Chiang Mai University, Chiang Mai 50200, Thailand:
E-mail:[email protected]
Received 15 June 2009, and in revised form 15 July 2009.
Case report
SEVERE OCCLUSIVE RETINAL VASCULITIS IN
SYSTEMIC LUPUS ERYTHEMATOSUS: A CASE REPORT
Paradee Kunavisarut, M.D.,1 Kessara Pathanapitoon, M.D.,1
Yodpong Chantarasorn, M.D.,1 Janejit Choovuthayakorn, M.D.,1
Aniki Rothova, Ph.D.2
1Department of Ophthalmology, Faculty of Medicine, Chiang Mai
University,2Uveitis Centre, Department of Ophthalmology, University
Medical Centre Utrecht,
The Netherlands
Abstract
Severe vaso-occlusive retinopathy, as the primary manifestation
of systemic lupus
erythematosus (SLE), is relatively rare. We report a 30-year-old
female, who gradually
suffered bilateral visual loss. Fundus examination revealed
bilateral severe occlusive
retinal vasculitis and development of neovascularizations. Her
clinical manifestations and
laboratory findings were compatible with the diagnosis of
systemic lupus erythematosus.
Chiang Mai Medical Journal 2009;48(4):159-162.
Keywords: occlusive retinal vasculitis, systemic lupus
erythematosus, bevacizumab
Systemic lupus erythematosus (SLE) is a
chronic systemic autoimmune disease, which
may affect multiple organ systems. It is char-
acterized by the production of pathological
autoantibodies that lead to end-organ damage
via inflammatory mechanisms. Keratocon-
junctivitis sicca is the most common mani-festation in
ophthalmic lupus, while the pos-
terior segment involvements have important
implications for visual function. The retinal
arterial occlusion is less common than
office ocular complication.(1) The presence
of retinal manifestations parallels disease
activity elsewhere.(2-4) We, herein, describe a
case of systemic lupus erythematosus, which
who initially presented with bilateral severe
vaso-occlusive retinopathy.
Case report
A previously healthy 30-year-old Thaifemale presented with
gradual bilateral visual
loss for 2 months. Visual acuity was finger
counting in both eyes; retinal examination
revealed severe occlusive vasculitis with
diffuse sheathing of the arteries and develop-
ment of neovascularizations located on both
-
8/22/2019 05_Retinal Vasculitis in SLE_Kessara
2/4
160 Kunavisarut P, et al.
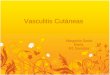
optic discs. Multiple areas of retinal edema
with hemorrhages and lipid exudates were
present and all vessels exhibited gross caliber
changes (Fig. 1). She had malar rash, discoid
rash, oral ulcer and a history of photosensi-
tivity, arthralgia, and alopecia for one year.
She used no medications. Systemic lupus
erythematosus was initially suspected, so
she consulted a rheumatologist for further
investigations. Complete blood count in-
cluded hemoglobin at 8.3 g/dL without
hemolytic blood features, and normal white
blood cell and platelet count. Erythrocyte
sedimentation rate (ESR) was 139 mm/hour.
Urine analysis found trace proteinuria, with-
out granular cast, and urine protein = 0.35 g
per day. An antinuclear antibody test was
positive at a titer of 1:1280. Renal and liver
function tests were normal. The diagnosis of
systemic lupus erythematosus was made
following the American College of Rheu-matology criteria. The
results of serologic
evaluation for HIV and syphilis were nega-
tive. Anticardiolipin antibodies, both Ig G
and Ig M, were negative. Her blood pressure
was normal. The patient was treated with
systemic corticosteroid (1 mg/kg/day) and
posterior subtenon injection with triamcino-
lone (20 mg/0.5 cc), panretinal laser photo-
coagulation and intravitreal injection of 1.25
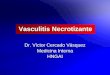
mg of bevacizumab in both eyes. Within
6 weeks, retinal edema decreased and the
majority of exudates and hemorrhages had
been absorbed. Retinal neovascularizations
disappeared in the right eye and were grossly
reduced in the left one (Fig. 2). Optic disc
pallor developed and arterial sheathing as
well as extremely variable caliber of the
retinal vessels persisted. In the left eye,
adjacent to the optic disc, a development of
fibrous tissue in previous neovascular mem-
branes could seen, which caused traction on
the retina. Unfortunately, within one year, the
neovascularizations of optic discs in both eyes
reappeared. The patient was subsequently
treated with extensive laser photocoagulation
as well as intravitreal bevacizumab injectionsin both eyes.
However, vitreous hemorrhage
developed in both eyes, and pars plana vi-
trectomy was required to remove vitreous
hemorrhage and release macular traction.
During the surgery, additional endophoto-
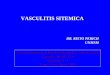
Figure 1. Fundus photograph at the onset of the disease
demonstrating severe occlusive vasculitis in
systemic lupus erythematosus.
-
8/22/2019 05_Retinal Vasculitis in SLE_Kessara
3/4
Retinal Vasculitis in systemic lupus erythematosus 161
coagulation was also performed. Several
months later, the neovascularizations of optic
discs regressed. Herfinal visual acuity was
0.1 in both eyes
Discussion
Retinal vascular lesions are one of the most
common forms of intraocular involvement in
patients with SLE, and present in 2-30% of
all SLE patients, depending on the activity
and severity of the disease.(5) The retinopathy
in SLE usually consists of cotton-wool spots,
with or without intraretinal hemorrhage, and
does not compromise visual acuity unless it is
located in the macular area. A more severe
variant of retinal vaso-occlusive disease is
less common, and may present with localized
features as central and branch retinal vas-
cular occlusions or diffuse occlusive retinal
disease, as in our patient. Clinicians should
be aware of clinical pictures that resemble
hypertensive retinopathy, which could be
present secondary to lupus renal hyperten-
sion. Still, this patient had lupus retinopathy,
which occurred as an independent manifes-
tation of the underlying disease process in
the absence of hypertension.(6) Severe occlu-
sive SLE retinopathy is associated with CNS
involvement, which did not present in our
patient however. The presence of antiphos-
pholipid antibodies is mostly found when
a search is made in patients with severe
occlusive SLE retinopathy.(7) However, the
test was negative in our patient. The visual
prognosis of diffuse occlusive retinal vascu-
lar disease is poor, and retinal neovascular-
izations with subsequent vitreous hemorrhage
and tractional retinal detachment commonly
develop.(1,5,8) In our patient, visual acuity was
slightly improved in both eyes after treat-
ment. Systemic SLE treatment combined
with scatter laser photocoagulation, and/or
vitreoretinal surgery, contributed to the treat-
ment of retinal neovascularizations. The role
of anti-VEGF agents in the treatment of
SLE retinal vasculopathy or further autoim-
mune diseases have not been systematically
evaluated yet.(9) We illustrated the promising
role of anti-VEGF agents as an adjuvant in
the treatment of retinal neovascularizations
from severe occlusive retinal vasculitis.
In conclusion, this study demonstrated
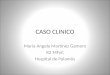
Figure 2. Fundus photograph six weeks after treatment with
systemic and periocular corticosteroids,
panretinal laser photocoagulation and intravitreal injection of
1.25 mg of bevacizumab in both eyes
demonstrating decreased neovascularizations and hemorrhages.
-
8/22/2019 05_Retinal Vasculitis in SLE_Kessara
4/4
162 Kunavisarut P, et al.
that SLE might initially manifest with ocular
symptoms, which are potentially severe, and
it also illustrated novel treatment possibilities
with anti-VEGF agents.
References1. Jabs DA, Fine SL, Hochberg MC, Newman SA,
Heiner GG, Stevens MB. Severe retinal vaso-
occlusive disease in systemic lupus erythema-
tous. Arch Ophthalmol 1986;104:55863.
2. Read RW. Clinical mini-review: systemic lupus
erythematosus and the eye. Ocul Immunol In-
flamm 2004;12:87-99.
3. Arevalo JF, Lowder CY, Muci-Mendoza R. Ocu-
lar manifestations of systemic lupus erythemato-
sus. Curr Opin Ophthalmol 2002;13:404-10.
4. Yap EY, Au Eong KG, Fong KY, et al. Oph-
thalmic manifestations in Asian patients with
systemic lupus erythematosus. Singapore Med J
1998;39:557-9.
5. Foster CS. Systemic Lupus Erythematosus In:
Albert & Jakobiec, editors. Principles and Prac-
tice of Ophthalmology. 2nd ed. Philadelphia;
Saunders 2000: 4563-70.
6. Ushiyama O, Ushiyama K, Koarada S, et al.
Retinal disease in patients with systemic lupus
erythematosus. Ann Rheum Dis 2000;59:7058.
7. Montehermoso A, Cervera R, Font J, et al. Asso-
ciation of antiphospholipid antibodies with reti-
nal vascular disease in systemic lupus erythema-
tosus. Semin Arthritis Rheum 1999;28:32632.
8. Au A, ODay J. Review of severe vaso-occlusive
retinopathy in systemic lupus erythematosus and
the antiphospholipid syndrome: associations, vi-sual outcomes,
complications and treatment. Clin
Experiment Ophthalmol 2004;32:87-100.
9. Carvalho JF, Blank M, Shoenfeld Y. Vascular
endothelial growth factor (VEGF) in autoim-
mune diseases. J Clin Immunol 2007;27:246-56.
:
systemic lupus erythematosus
, ..,1 , ..,1 , ..,1, ..,1 Aniki Rothova, Ph.D.2
1, 2Uveitis Centre, Department ofOphthalmology, University
Medical Centre Utrecht, The Netherlands
Systemic LupusErythematosus 30 systemic lupus erythematosus
2552;48(4):159-162.
: occlusive retinal vasculitis, systemic lupus erythematosus,
bevacizumab