-
8/8/2019 09.2009 Eval Grantee Posters
1/14
U.S.-Mexico border in California, southern end of agricultural
belt
Adult Mexicans/Mexican-Americans; 23% live in poverty
336 patients randomly sampled from Clinicasroster
30 Peer Supporters: former participants in a diabeteseducation
program; seen as exhibiting mastery overdiabetes; qualities of
empathy, warmth, and referent power
Recruitment/Retention Innovation:
2 different recruitment letters to be sent October 2009
Test two messages to recruit and retain Peer Supporters:self vs.
other oriented
6 Training Sessions: 2 full-day on weekend, 4 shorter
sessions on weekdays to begin November 2009; total 32-40
hours
Peer Supporter assigned to 6 patients with diabetes:
Goal: Help improve diabetes self-management behaviorsrelevant in
multiple contexts (clinic, community, home)
Dose: Minimum of 8 contacts in first 6 months; lessfrequent
contact in subsequent 6 months
Modes: Family home visits, small groups, and clinic tours
Design and Methods
Approaches to Implementing Peer Support
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Organization:San Diego State University and Clinicas de Salud
del Pueblo
Principal Investigators: Gu ad alu p e X. Ayala, PhD, MPH an d
Joh n P. Elde r, PhD, MPH
Randomized controlled trial with two conditions: peer support
vs.usual care
Data to be collected at baseline, 6 months, and 12 months
Measures from medical records: HbA1C, BMI, BP, cholesterol,
ageof diabetes diagnosis, diabetes medications, hospitalizations,
lasteye and foot exams, other diagnosed medical conditions
Measures from survey: medication use/adherence, health
careaccess, health literacy, diabetes self-care, quality of
life,acculturation, demographics, other health behaviors
Process Evaluation to assess: participant engagement, nature
ofvolunteer peer supporters in Latino community, study design
usingRE-AIM model
Alliance to Control Diabetes/Alianza para
Controlar la Diabetes
Follow-up assessments at
6- and 12-months
Usual care (n=168)
Intervention (n=168)6 months of peer support
Each peer supporter assigned to 6adults with diabetes.
Randomly sample 336 patients fromclinic roster & conduct
baseline
Randomly assign to condition
Audience and Setting
Diabetes
control
Community navigation
Facilitate access toexternal resources(library, internet)
Problem-solveovercome social and
physical barriers(celebrations with
family, friends and co-workers; restaurant
eating; unsafeneighborhoods)
Targets for change in a diabetes peer support intervention
Modes of delivery include: family home visits, small group and
clinic tours
Health care systemnavigation
Meet with patientbefore provider visitto activate = improve
communication
Facilitate utilizationof diabetes
managementresources
Home navigation
Family support and
engagementHealthy control of thesocial and physical
environments of the home
Skill building
Other Investigators and Key Personnel: And rea Cherr ington ,
MD, MPH, Nad ia Camp bell,MPH, Mar k Sn yd er , Ph D, Afs h an N.
Baig, MD, Ming Ji, PhD, Let icia Ibar ra , MPH
-
8/8/2019 09.2009 Eval Grantee Posters
2/14
People with diabetes in rural (Bafut) and urban (Bamenda)health
districts of Cameroon
Peer supporters will be recruited from health care
providerscaring for people with diabetes and from people with
diabetes
themselves
People with diabetes (PWD) will be recruited though
diabetesclinics; Bafut has three clinics and 80 diabetes
patients;Bamenda has six diabetes clinics and 613 diabetes
patients
Audience and Setting
Study based in social ecological model to inform anintervention
with when, why, and how people engage in peersupport (social
ecology of health behaviors and triggers for
peer support) The project will identify peer support devices for
use by
people with diabetes and their peers (e.g., email,
textmessaging, telephone), train peers in the use of them,
andenable peers to interact amongst themselves usingnetworking
PWD will serve as the first contact with their peers who donot
attend clinics
Other activities will include promoting peer support
programs,encouraging networking among those active in peer
supportprograms, hosting a webpage to circulate program
materialsand curricula
STUDY: Design and Methods
Approaches to Implementing Peer Support
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Organization:Centre for Population Studies and Health
Promotion
Investigators: Pasch al Kum Awah, PhD and Andre- Pascal Kengne,
MD, PhD
80 people with diabetes and 80 as their peers (one
perpatient)
All participants allocated to intervention group;
outcomescompared between urban and rural participants
(repeatedmeasures; participants serve as own control)
Anthropometric, risk factor, biological, behavioral,psychosocial
wellbeing, self care, compliance, and quality oflife data
Baseline, mid-duration, and end-of-project evaluations (20-
month study period)
Peer Collaboration in Diabetes Care
PEERSDIACARE Cameroon
Study aims: To identify and create enabling environments for
peer support between people withdiabetes, families, and healthcare
providers in rural and urban Cameroon
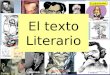
Me n
43 %Women
57 %
58.6
57
57.7
56
56.5
57
57.5
58
58.5
59
Men Wom en Overa l l
Mean age (years)
29.9
28.5
26.5
24
25
26
27
28
29
30
31
Vis it 1 Vis it 2 Vis i t 3
Mean BMI by v is i t (kg/m2)
Preliminary results
180.5
176.1
170.7
16 5
17 0
17 5
18 0
18 5
V is i t 1 Vis i t 2 Visi t 3
Mean FBG by v is i t (mg/dl )
13 8 14 2 14 1
81 82 83
0
20
40
60
80
10 0
12 0
14 0
16 0
Vis it 1 Vis it 2 Visi t 3
Mean SBP by v is i t (mmHG)
Mean DBP by visi t (mmHG)
-
8/8/2019 09.2009 Eval Grantee Posters
3/14
400 low income English and Spanish-speaking patients with type
2diabetes and HbA1C >8% recruited from 4 community health
clinicsin San Francisco, California
Potential peer coaches (patients with diabetes, HbA1c
-
8/8/2019 09.2009 Eval Grantee Posters
4/14
People with diabetes (PWD) in Hong Kong, SAR, CHINA
Patients receiving structured care augmented by a
web-baseddisease management program enrolled in the Joint Asia
DiabetesEvaluation Program (JADE)
Audience and Setting
Motivated and knowledgeable peer leaders will undergo a
32-hourTrain the trainer program (4 workshops, 8-hours each) for
furtherempowerment and development of leadership skills
Supported by a program manager, peer leaders will maintain
regularcontact with their assigned mentees in the intervention
groupthrough phone calls, sharing sessions and other forms
oftelecommunications
Peer leaders will encourage their peers to use the Telephone
LinkedCare (TLC) automated system for knowledge enhancement
andmotivational support
Each peer leader will contact their mentees (10 per mentor)
twiceper month by 15-20 minute phone calls for 3 months
After 3 months, peer leaders will call their mentees between
clinicvisits or more often, if needed
Design and Methods
Approaches to Implementing Peer Support
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Organization: Asia Diabetes Foundation and Hong Kong Institute
of Diabetes and Obesity,The Chinese University of Hong Kong, Hong
Kong SAR, CHINA
Principal Investigator: Julian a C. N. Cha n, MD, FRCP
Co-Investigators: Gar y T.C. Ko, MD FRCP, Rebe cca Y.M. Won g,
RN MA, Sh im en Au, RN, Lan ce lot Mu i, BSc, MPH,
Eva Kan, RN MPH, Alice P.S. Kong, MBChB, FRCP, Ronald C.W. Ma,
MB, BChir, MRCP, Peter C.Y. Tong, PhD FRCP,
Joseph Lau, MSc, PhD, Brian Oldenburg, PhD, Robert H. Friedman,
MD, Wingyee So, MD FRCP.
Aim: To use peer support and information technology to
facilitatecare providers to implement structured care and empower
PWD toacquire self-management skills and improve quality of
care
A 12-month, multi-center, randomized, parallel study involving
600PWD receiving structured care through the JADE program, with
halfof them randomized to receive peer support (n=300)
Primary outcomes HbA1c, BP, body weight and lipid profile
Secondary outcomes Cognitive-psychological-behavioralmeasures
using Chinese validated questionnaires:
Mental Health (Depression Anxiety and Stress Scale (DASS21)
Self-efficacy (Diabetes Empowerment Scale (C-DES)
Diabetes Self Care Activities (SDSCA)
User acceptability and cost-effectiveness of programs
Peer Support, Empowerment And Remote Communication
Linked by Information Technology (PEARL):
A Multi-Component Program to Improve Community-Based Diabetes
Care
-
8/8/2019 09.2009 Eval Grantee Posters
5/14
Audience and Setting
STUDY: Design and Methods
Approaches to Implementing Peer Support
Organization:National Research Council of Argentina (CONICET)
with the CENEXA. Centre ofExperimental and Applied Endocrinology
(UNLP-CONICET),
PAHO/WHO Collaborating Centre for Diabetes (ARGENTINA)
Principal Investigator: Juan Jose Gagliard ino, MDOther
Investigators:Charles Clark Jr., MD and Kate Lorig, DrPH
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Optimizing Diabetes Outcomes: The Role of Peers
Study aims:To compare the benefits of a diabetes education
program with peers as part of the education team, forthe provision
of ongoing psychological and practical support in an 18-month pilot
trial.
People with type 2 diabetes from La Plata city (Argentina)
Recruitment and Selection:Physicians and patients from a local
primary care institution;
Peers from our team based upon good diabetes control,motivation,
communication skills and interest.
Peers addressing diabetes education, provision of emotional
support, solving of daily self-care problems.
Peers will have scheduled contacts with supportees and members
of education team:
bimonthly encounters at buffet restaurant with a nutritionist
(food selection and meal plan);weekly (first 6 months), biweekly
(next 3 months) and monthly (remaining study period)
telephonecommunications to assess patients problems and clinical,
metabolic and psychological progress;
monthly group teleconference (peer plus supportees) (telephone
company contract for cell phoneprovision and discount rates).
Knowledge(solve problems)
Motivation(sustained healthybehaviour)
Skills(self-carepractices)
Empowerment
Improved diabetes control
Better quality of life
Randomly selected patients allocated into 2 groups (94
peopleeach; 6 months). Follow-up: 12-months.
Patient education courses: 4 small interactive group
weeklysessions (2 h each), including knowledge, skills and
attitudes;reinforcement session at 6 months.
Peer support group: patients attend the education courses
andreceive peer support.
Evaluation
A1C changes will be the primary outcome variable; it was used to
estimate sample size.
QUALIDIAB data set (clinical, metabolic, therapeutic and
economic data; complications) (0-12 months)
Abbreviated QUALIDIAB data collection at 6 months;
WHO-5 and patient and peer satisfaction (SF-8 questionnaire) at
6 months.Statistical analyses: test and chi2 for continuous and
categorical data, respectively.
-
8/8/2019 09.2009 Eval Grantee Posters
6/14
Insured middle-class patient population in San Antonio, TX
Mentors and mentees are patients recruited from 15
practiceswithin WellMed
Recruitment strategies include: electronic reminders to
physicians,referrals, informational pamphlets, posters, word of
mouth, andmailings
Audience and Setting
Adapting a successful Diabetes Peer Mentoring Program, Carpeta
Roja (CR), from low income, uninsuredpopulation to middle-class
population
Mentors receiving formal training and drawing on their own
experiences will provide support to menteesthrough in-person
meeting, telephone, and other communication
Mentors will work with 1-5 mentees at a time for 3-14 months,
depending on patient need and will completean 8-week
self-management course prior to beginning mentoring phase
Design and Methods
Approaches to Implementing Peer Support
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Organization:The American Academy of Family Physicians National
Research Network (with
Latino Health Access, LA Net, and WellMed Medical Group)
Principal Investigator: Lynd ee Knox
Co-Investigators: Ame rica Brach o, MD, Debo ra h Grah am ,
MSPH, MPH, Jess ica Huf f, Pat ricia
Cantero, PhD, Margie Gomez, Michelle Henry, MSN
Practice-level randomized controlled trial and multiple start
date, wait list design. 3 arms: Usual care, 101course only, 101
plus CR. Outcomes for mentees and mentors assessed.
Assessing reach by tracking number of patients assessed as
eligible, the number who sign-up for mentoring,and the number who
receive mentoring
Diabetes Distress Scale, EQ-5D for quality of life, and
Perceived Diabetes Self-Management Scale
HbA1c, blood pressure and LDL
Implementation/process: Recruitment strategies, retention,
adaption for senior patient population, adaption forwell resourced
healthcare setting, adaption for diverse SES and ethnic
background
Evaluating the Implementation and Effectiveness
of a Diabetes Peer Mentoring Program
-
8/8/2019 09.2009 Eval Grantee Posters
7/14
Peer champions and partners were recruited by anurse at the
Mityana Diabetes Clinic
In May 2009, 19 champions attended first meeting
Champions were matched with 27 partners in thesame age group and
gender, and in close livingproximity
Audience and Setting
Training for champions conducted in English using the Champion
Diabetes Guidebook
Initial peer meeting held in May 2009 (27 attendees) and booster
sessions were held in July and August(34 attendees)
Community meetings educated participants on diabetes and
emotional and psychosocial issues thatmay arise, and trained
champions in communication skills
All participants and health care providers were given cell
phones using a closed network to maintainregular contact between
peers and providers without airtime charges
Champions made contact with partners at least once per week over
3 months
A meeting was held in September 2009 to obtain feedback about
the program and post-measures fromall participants
STUDY: Design and Methods
Approaches to Implementing Peer Support
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Organization:The University of Wisconsin-Madison School of
Nursing (USA); andMulago Hospital, Department of Medicine, Kampala
and Mityana District Hospital,
Mityana (UGANDA)
Principal Investigator: Lind a C. Bau m an n , PhD, RN
Other Investigators: Agath a Nam bu ya, MD, Fre d Nakwa gala,
MD, MS, andJosep h ine Ejan g, RN (Mulago Hos p ital Dep ar tm en t
of Med icine)
Pre-test post-test design of a 12-week pilot intervention
Measures included a self-administered questionnaire, HbA1c,
blood pressure, and BMI
Mityana Clinic Nurse kept a log of all champion-partner
contacts
Cell phone records to track usage among champions, partners, and
health care providers
A Peer Champion Program for Ugandan
Adults with Diabetes
Study Aims/Questions: To test the feasibility and short-term
impact of a peer champion program foradults with type 2 diabetes in
the community of Mityana, Uganda
-
8/8/2019 09.2009 Eval Grantee Posters
8/14
People with diabetes (PWD) in the community in Yaound,
Cameroon
All enrolled participants are diabetes patients being
followed-up at thediabetes clinic of the National Obesity
Centre
Potential peer supporters recruited for training based on health
careprovider recommendation, area of residence, cultural
background, andsuccess in controlling diabetes
10 Peer Supporters selected after completion of training based
on HbA1c
-
8/8/2019 09.2009 Eval Grantee Posters
9/14
People living with Type 2 diabetes in the state of Victoria,
Australia
Participants selected from people with Type 2 diabetes who are
registered on the database of DiabetesAustralia-Victoria
(non-governmental organization)
At least 20 peers selected as peer supporters based on personal
characteristics (e.g., acceptance of diverseviews)
Participants ages 25-75 with diabetes at least 12-months
Audience and Setting
Lay peer supporters/group facilitators will complete three-days
of training to acquire group facilitation,communication and other
basic skills aimed at helping the group members to achieve the
desired individualand group health and social outcomes of the Peers
for Progress Diabetes Program.
One group leader per 8-15 people with diabetes to encourage
behavioral change, build problem solving,risk assessment and
communication skills, assist participants to access to local
resources, provide a venuefor informal information exchange and
feedback,
12-monthly peer-led sessions in participants local communities
over 12 months; sessions addressbehavior change, chronic disease
self-management, emotional, appraisal, and informational
support;supported by workbook of content and resources
Approaches to Implementing Peer Support
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Evaluate efficacy of peer support intervention and its
transferability to other settings, populations, andcountries
Participants will be clustered by region and these groups
randomly assigned to intervention or waitlistcontrol arms
Create 32 groups of 8-15 people with diabetes (16 groups to each
arm with at least 99 participants in eacharm)
Reach and engagement of intended audience per RE-AIM
Measuring outcomes (HbA1c, BMI. behaviors, quality of life,
psychosocial, group effectiveness, and system
outcomes), implementation, and comprehensive economic
evaluation
Measurement at baseline, 6, 12, and 18 months
A controlled evaluation of the Australasian Peer
for Progress Diabetes Program (PfP-DP) and its
Transferability to Other Countries
Organization: Monash University, School of Public Health &
Preventive Medicine
Principal Investigator: Brian Oldenburg, PhD
Co-Investigators: James A. Dunb ar an d Prasu na Redd y (Flind
ers a nd Deakin Universities,
Aus tra lia); Dr. Ralph Aud ehm and Greg John son (Diabet es Aus
tra lia- Victor ia, Aus tra lia);
Rob Carte r (Deakin University, Aus tr alia); Maximilian d e
Cour ten an d Rory Wolfe (Mon as h
Univers ity, Aust ralia); Dr. Pilvikki Abs etz (Nation al Ins
titu te o f Public Health , Finlan d );
Anua r Zaini (Mon as h University Malaysia)
Design and Methods
-
8/8/2019 09.2009 Eval Grantee Posters
10/14
African American adults in a community-based setting (Ypsilanti,
MI) and Latino adults (Spanish and English-speaking) in a
clinic-based setting (Detroit, MI)
Participants recruited by provider/community organization
referral, advertisements in newspapers and flyers,clinic-based
computerized databases, invited presentations at churches
Audience and Setting
Peer Leader Training focuses on diabetes-related
knowledge, behavioral strategies (e.g., 5-step goal
setting model) and communication skills Intervention consists of
a 3-month, theoretically-driven
diabetes self-management education (DSME) program
(monthly one-on-one sessions, monthly phone calls,
MD appointment preparation) followed by a Peer-Led
Empowerment-based Approach to Self-management
Efforts in Diabetes (PLEASED)
Approaches to Implementing Peer Support
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Organization: University of Michigan Medical School, Department
of Medical Education andDepartment of Internal Medicine, and the
University of Michigan School of Public Health,Department of Health
Behavior and Health Education
Principal Investigators: Tricia S. Tang, PhD an d Miche le
Heisle r, MD, MPA
Co-Investigators: Robe rt And ers on , MEd , Ed D; Mar th a Fun
n ell, MS, RN, CDE; Joh n Piet te ,PhD; Micha el Spen cer , MSW, Ph
D; Felix Valb u en a, MD (Com m u n ity Healt h & Social
Services )
Randomized controlled design
Participants are randomized to receive either DSME co-led by
CDE/CHW and 2 peer leaders followed by 12months of DSMS or DSME
followed by 12 months of self-directed support (control group).
Peer-led self management support in real
world clinical and community settings
Design and Methods
Investigating impact of PLEASED intervention following 3-months
DSME at 6-months and 12-months compared tosame duration of
self-directed support; also confirming impact of 3-months DSME to
improve outcomes
Outcome measures include A1C, blood pressure, lipd control,
self-management behaviors (Summary of Diabetes
Self-Care Activities), quality of life (Diabetes Distress
Scale), and reach to and engagement of intended audience(RE-AIM
framework)
PLEASED: 12-months of ongoing, peer-led diabetes self-management
support (DSMS) weekly sessions based on
patients priorities, questions, and concerns to build
motivation, set goals, draft action plans, problem-solve;
follow-up
phone calls as needed; matched with at least one peer buddy for
ongoing support)
-
8/8/2019 09.2009 Eval Grantee Posters
11/14
Adult patients with type 2 diabetes receiving care from
CommunityHealth Centers in rural, impoverished Alabamas Black
Belt
Recruiting only patients with A1c >7.5%
Networked Recruitment of peer advisors: 2-3 peers
initiallyrecruited by practice staff, then use peer social networks
and otherestablished community networks to recruit additional
peers
Audience and Setting
Pilot peer advisor training program in September 2009, piloting
recruitment and the intervention November 2009
Peer advisors collaborated in developing training curriculum;
pilot peer advisors to assist in further refinement oftraining and
intervention
Beginning early winter, 2-day peer advisor training to occur in
each target geographic area (Central, West)
Peers will deliver a 12-month intervention to support diabetes
self-management goals, facilitate patientempowerment, and raise the
BAR (Be prepared; Ask and learn; Reflect) to get the most out of
office visits with theprovider
Peer advisors will make weekly, 15-20 minute contacts with
clients for the first 8 weeks of intervention, and monthlycontacts
thereafter; in addition, there will be contacts before and after
office visits with the provider
Design and Methods
Approaches to Implementing Peer Support
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Organization:University of Alabama at Birmingham, School of
Medicine
Principal Investigator: Mon ika M. Saffo rd , MD
Co-Principal Investigators: Mon a Fou ad , MD, MPH; An d rea
Cher rin gto n , MD, MPH
Co-Investigators: Su sa n Ap p el, Ph D; W. Tim ot h y Gar vey,
MD, PhD; Jewell Halan ych ,MD, MPH; Miche lle Mar tin , PhD; Mar ia
Pisu , Ph D; Rober t Ost er , PhD, Mar y Ann et te
Wright, PhD
Group-randomized, controlled implementation trial(randomized at
the practice level)
Reach evaluated by comparing number of eligible
patientsapproached for recruitment with the number enrolled
200 patients in each trial arm, total of 400
Data collected at baseline and 12 months
Primary outcomes: HbA1c, blood pressure, cholesterol
Secondary outcomes: Self-management behaviors, quality of life,
and psychosocial factors
Health care utilization will be measured through medical record
review
UAB Diabetes Research Translation Center is supporting 6-month
data collection and cost-effectiveness analysis
Encourage: Evaluating Community Peer Advisors and
Diabetes Outcomes in Rural Alabama
-
8/8/2019 09.2009 Eval Grantee Posters
12/14
People with type 2 diabetes (PWD) in four districts (two urban,
two rural) fromtwo provinces central and northeast regions of
Thailand
20 VHVs and six health staff selected for training (Selection
Criteria: must haveat least 3 PWDs in their areas of
responsibility; read/write in Thai; can completetraining and
project)
VHVs (peers) function as link between communities and frontline
health careproviders
Audience and Setting
Training curricula for VHVs to be developed during 5-day
workshop including selected PWDs, VHVs, local healthpersonnel,
medical doctors, and project researchers
20 VHVs and 6 health staff attend 4-day training based on
previously developed curricula and develop activityplan at end of
training
VHV work with PWDs and families (e.g., identify problems, set
goals, identify approaches for addressing them);includes regular
home visits for problem solving and providing feedback
Frequency of home visits mutually agreed upon by VHVs and PWDs;
no less than 2 visits per month
Meetings among all PWD, families, and VHVs every two months for
group support, follow-up on activities,problem-solving,
network-building, and ensuring continuity of care between community
and health center
STUDY: Design and Methods
Approaches to Implementing Peer Support
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Quasi-experimental, Two groups, pre-post test design; aim to pre
and post test all 20 VHVs and 60 PWDs undertheir responsibility
Comparison group: same number of VHVs and PWDs from
non-participating, similar socio-economic districts inthe same
provinces
Among participants, measuring dietary intake, physical activity,
proper skin and foot care, HbA1C, bloodpressure, BMI, quality of
life, perceived susceptibility, severity, self-efficacy and
benefits, perceived supportreceived
Among VHVs, measuring self-efficacy in providing support and
motivation
Peer supports for sustainable self-care and enhancing
quality
of life among diabetes mellitus type 2 patients in Thailand
Study Aims/Questions: Build the capacity of village health
volunteers (VHV) in motivating DM type 2patients to develop and
maintain self management behaviors by applying an ecological
approach
Organization:Mahidol University, Faculty of Public Health,
Department of Health Educationand Behavioral Science
Principal Investigator: Boos aba San gua np ras it, PhD, MPH
Co-Investigators: Chaisr i Sup orn silaph ach ai, MD, MPH
(Minist ry o f Pub lic Health ); Rewad eeChon gsu wat , PhD, MS;
Cha nu an th on g Tana su garn , MPH, DrPH; Prasit Leera p an ,
MEd, PhD;
Sun ee Lakam pa n, EdD
-
8/8/2019 09.2009 Eval Grantee Posters
13/14
Xhosa women with type 2 diabetes in Mfuleni Township, CapeTown,
South Africa
Women recruited to be Diabetes Buddies (DB) at the Women for
Peace center, an NGO
Audience & Setting
22 women to be assigned to buddy-pairs (DBs) with the purpose of
providing reciprocal, ongoing support
12-week program (weekly meetings for 3 months) attended by DBs,
covering nutrition, exercise, providingreciprocal support, and
managing relationships with health care providers
Training program, based on Diabetes Prevention Program (DPP),
led by a paid peer mentor
DBs given cell phones and trained to use SMS application to
record daily blood glucose levels, text messagetheir buddies, and
receive motivational prompts
Study Methods & Findings
Approaches to Implementing Peer Support
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Organizations:University of California-Los Angeles,
Global Center for Children and Families (USA) with
the Stellenbosch University and Women for Peace (SOUTH
AFRICA)
Investigators: Mary Jane Roth eram - Boru s, Margaret
Gwegwe,
Mark Tom lin so n, Marion Keim
One group, pretest-posttest design
Average age of DBs was 53 years old; almost all had lived for
over 5 years in their homes: formal brickstructures with running
water on the premises, flush toilet, and electricity. Fewer than
half had any
employment. All participants were assessed at baseline, 3
months, and 6 months later.
Outcomes monitored: exercise, social support, anxiety, blood
sugar, BMI, blood pressure.
Social support showed immediate improvement at 3 months and
continued to increase at 6 months.
Exercise and diastolic blood pressure did not improve over
time.
For anxiety, BMI, blood sugar, and systolic blood pressure,
outcomes appeared slightly worse at the 3-month assessment compared
to baseline, but between 3 and 6 months either leveled off or
showedimprovement.
The women who did the most text messaging with their buddies had
much higher BMIs than those whotexted less, at all time points.
Preliminary results indicate that some improvements might not
occur immediately, but appear over time.
Diabetes Buddies
-
8/8/2019 09.2009 Eval Grantee Posters
14/14
People with type 2 diabetes in East of England UK
(mainlyCambridgeshire)
Participants will be recruited through their general
practitioners(assisted by Primary Care Research Network) and
communitynetworking
Peers will be recruited through an initial survey, and will
beselected and trained by the study team
Audience and Setting
Peers will receive training to offer assistance with living
withdiabetes, motivational interviewing, and in support skills
A diabetes nurse will assist in providing linkages to care
Peer support will occur through individual and/or group
settings
Peers will have up to 10 individuals at one time for 1:1
meetings,give 4-10 hours per week for 6 months
Group settings will have 20 individuals and two leads
Approaches to Implementing Peer Support
A program of the American Academy of FamilyPhysicians Foundation
and supported by the Eli
Lilly and Company Foundation, Inc.
Organization:Cambridge University Hospitals NHS Foundation
Trust, Institute of MetabolicScience, University of Cambridge
General Practice and Primary Care Research Unit
Principal Investigators: David Sim m on s, FRCP FRACP MD, Jon at
h an Graf fy, FRCGP MD
Co-Investigators: Simo n Coh n, PhD; Sara h Don ald, BSc; Pete r
Rob ins, MA, Vet MB; Cha rlot te Padd ison ,
PhD; Toby Provost, PhD; Mark Evans, MD, FRCP; Amanda Adler, PhD,
FRCP; Catherine Walsh, FRCPsych
East of England, United Kingdom
Cluster randomized trial with 2X2 comparison of
individual,group, combined individual/group support, and normal
care
Aim to recruit 1520 participants in 80 community clusters
Reach assessed by recruitment rate from initial
survey,attendance for support sessions, intervention fidelity,
andcomparison with routine health service data
HbA1c over 12 months, body weight, blood pressure
Surveys: self-management (DSCAM), self-efficacy (DMSES),and
quality of life (EQ-5D)
Qualitative (e.g., meaning of peer support) and
economicanalyses
RAPSID: Can Peer Support (Group or Individual Intervention)
Enable People with Diabetes and Improve Health?
Design and Methods
Diabetes PLUSPeer-Led Understanding & Support
Overview of different support approaches
1:1 Peer Support
GroupBasedSupportgroup
Control 1:1 only
Group only Both
Content: Eductn& usual
care
Assist in dailymanagement
and livingwith diabetes
Discussion ofsocial andemotionalaspects of lifewith diabetes
Socialcontextualsupport
Linkage toclinicalCare
Individual1:1support
Yes Sharingexperiences& mentoring
Individualdiscussion
No Individualreview of careaccess, linkvia Nurse if
needed
Groupsupport
Yes Sharingexperiences& co-mentoring ingroup
Groupdiscussion
Yes Groupdiscussn ofaccessing
services. Linkvia Nurse if
need
Combinedsupport
Yes Sharingexperiences& mentoring(group +/-individually)
Individualand/or group
discussion
Yes BothcomponentsAs above.
NormalCare
Yes - - - -
2 x 2 factorial study design
East Cambs
Fenland
Hunts
SouthCambs
Main study areas