Upload
eryxs-persada
View
220
Download
0
Embed Size (px)
Citation preview
8/9/2019 2001_Vol8_1 transfusi
1/20
AUSTRALASIAN SOCIETY OF BLOOD TRANSFUSION INC.
Topics in
Transfusion
Medicine
Feb rua r y 200 1
Vo l 8 No 1
8/9/2019 2001_Vol8_1 transfusi
2/20
February 2001
Vol 8, No 1
2
u Ed i t o r i a l Board
Editor: Ken Davis
Board Members: Margaret Buring, Wendy Erber, Jim Faed, John Gibson,Robyn Minchinton, David Roxby
Ed i to r ' s Note
This first issue for 2001 provides an update on a couple of significant topics which provide ongoingdilemmas for Transfusion Medicine and treating specialists, namely AIHA and optimal platelettherapy.
William Stevenson & John Gibson have prepared a review of recent literature with synopses for thepathogenesis, diagnosis, investigation and treatment of AIHA.
Wendy Erber has kindly prepared a transcript of a presentation she gave at the Adelaide Blood Clubmeeting in October on ‘what constitutes optimal platelet therapy?’.
Both of these articles provide members with the latest update of information and matters forconsideration in both these areas.
One of our recent articles on TRALI has generated a response from Brian Fisher, WA.
Members are encouraged to let the Editor know what ‘topics’ they would like addressed in futureissues.
Ken Davis[[email protected]]
Extra copies of Topics in Transfusion Medicine are available from the ASBT office for $20 each.Please spread the word.
All Correspondence
The Australasian Society of Blood Transfusion Inc145 Macquarie Street, Sydney NSW 2000
8/9/2019 2001_Vol8_1 transfusi
3/20
February 2001Vol 8, No 1
3
CONTENTS
1. WHAT’S NEW IN AUTOIMMUNE HAEMOLYTIC ANAEMIA (1997-2000)William Stevenson & John Gibson
Institute of HaematologyRoyal Prince Alfred HospitalCamperdown, NSW
2. WHAT IS OPTIMAL PLATELET TRANSFUSION THERAPY?
Dr. Wendy Erber, Dr. Andrew McQuillan, Dianne GreyHaematology, WA Centre for Pathology Medical Research,Nedlands WA 6009
3. Re: TRALI prevention [Letter to the Editor]
Brian Fisher, ARCBS,Perth, WA
8/9/2019 2001_Vol8_1 transfusi
4/20
February 2001Vol 8, No 1
4
1 . Wha t ’ s New in Au t o imm une Haem o l yt i c Anaem ia ( 1997 -2000 )
William Stevenson & John GibsonInstitute of HaematologyRoyal Prince Alfred Hospital
Camperdown, NSW
Histo r i ca l Ove rv iew
Autoimmune Haemolytic Anaemia (AIHA) is an uncommon disorder characterised byautoantibody production against red cell antigens leading to premature red cell destruction. Asthe following review illustrates, AIHA may well have been recognised for almost 500 years.
Autoimmune Hemolytic Anemia: A History.Mack P. & Freedman J. Transfusion Medicine Reviews 2000; 14: 223-233
A comprehensive historical review starting with a report from 1529 giving, what theauthors suggest, was the first description of paroxysmal cold haemoglobinuria. Acourt physician in Constantinople described a condition in which the urine was
“azure and livid as well as black” in patients of melancholic disposition whocomplained of loss of strength after exposure to cold.
The authors then continue to describe changes in medical diagnosis with the development ofthe microscope and studies of serum culminating in the discovery of the Antiglobulin test. Thelast 20 years have focused on immunological mechanisms of AIHA enabled by the developmentof molecular techniques.
Historical Note: Past, Present and Future of the Antiglobulin Test.Coombs R. Vox Sanguinis 1998; 74: 67-73
An interesting personal account by Coombs of the time leading up to thedevelopment of the Antiglobulin test and subsequent uses and modifications of thetechnique. He describes the discovery of the test with Race and Mourant in 1945and then the development of isotype specific reagents in the 1960s. He finishes hisaccount with speculation about the future development of tests involving red celllabelled antiglobulins.
Pa thogenes i s
Recent experimental work has further elucidated some of the immunologicalabnormalities that may contribute to AIHA.
Altered control of self-reactive IgG by autologous IgM in patients with warmautoimmune hemolytic anemiaStahl D. et al. Blood 2000; 95: 328-335This study examined self reactive IgG and IgM in 20 patients with warm AIHA and comparedthem to 20 healthy sex matched blood donors. This disease cohort was weighted towards AIHAsecondary to a systemic disease with 14 of the 20 patients having a malignancy and only 4having idiopathic AIHA.
8/9/2019 2001_Vol8_1 transfusi
5/20
February 2001Vol 8, No 1
5
Stahl et al. suggest that the anti-erythrocyte IgG autoantibody of AIHA is similar to natural anti-red cell antibodies of healthy donors. This was demonstrated with IgG purified from red celleluates of these two groups which both caused agglutination of red cells. However, purifiedIgM from both groups differed in its autoreactive profile, and importantly, purified IgM fromnormal donors inhibited the agglutination between IgG and red cells whereas purified IgM from
patients with AIHA did not inhibit this agglutination.
The authors suggest that under normal conditions autoreactive IgG may be masked by idiotypeinteractions between IgG and IgM. In AIHA, this process is altered because of abnormalfunction of IgM allowing increased interaction between self reactive IgG and red cells causinghaemolysis. This mechanism seems particularly plausible in this cohort because of the relativelylarge number of patients that had an underlying B cell malignancy in which monoclonal IgM is alikely secretory product.
Identification of T-cell epitopes on the Rhesus polypeptides in autoimmunehemolytic anemia.Barker R. et al. Blood 1997; 90: 2701-2715Rhesus (Rh) polypeptides are the commonest target for anti-red cell antibodies. This studydemonstrated that T-cells from 7 out of 9 patients with idiopathic AIHA were able to mountproliferative responses in vitro to epitopes from Rh proteins. Significantly, all 4 cases frompatients with autoantibodies to Rh protein had T-cells that proliferated. Such responses wereuncommon in the control group with only 3 proliferative responses out of 18 control samples.The authors suggest that pathogenic autoantibody production in many cases of idiopathic AIHAmay be driven by helper T-cells with specific activity against Rh proteins.
Labo ra t o r y Me thods
Gel techniques for the Direct Antiglobulin Test (DAT) have been available for about 10 years.This method has reported advantages over the traditional tube technique. Red cells are directlyadded to the gel and the result read after centrifugation without any washing of red cellsrequired.
Comparison between the conventional tube technique and the gel technique indirect antiglobulin testsNathalang O. et al. Vox Sanguinis 1997; 72: 169-171In this study from Thailand, 75 blood samples were examined by both conventional tubetechnique and gel technique using reagents from the same manufacturer. 52 samples camefrom newborns with hyperbilirubinaemia and 23 from patients with known AIHA. Nathalang et
al. reports the overall sensitivity and specificity of the gel technique was 93.5% and 88.6%respectively. This was comparable to the tube method with significantly higher agglutinationscores observed by using the gel technique. These stronger agglutination scores allow morelaboratory staff to perform the test correctly, as subtle changes require more experiencedtechnicians to interpret.
The direct antiglobulin test: Still a place for the tube technique?Tissot J. et al. Vox Sanguinis 1999; 77: 223-226Tissot et al. collected 398 consecutive samples from 1997 to 1998 and evaluated each with geland tube technique. 87 of these samples were from newborns, 23 from foetuses and the restfrom adult patients.
8/9/2019 2001_Vol8_1 transfusi
6/20
February 2001Vol 8, No 1
6
The authors identified 58 discrepancies using polyspecific antisera with 51 cases positive onlywith the tube technique and 7 cases positive only with the gel method. The differences wereeven more pronounced when monospecific sera was used, with only 21.4% of samples showingconcordant results with these reagents.
Overall in this study, the gel technique appeared to be less sensitive than the conventional tubetechnique, especially when C3d was present on red cells. These results appeared contradictoryto the previous study (Nathalang et al.) and Tissot suggested this might have been due to theuse of different reagents. The results of this study may then reflect the distinct affinity ofvarious C3d antisera from different manufacturers.
Gel test application for IgG subclass identification in auto-immune haemolyticanaemia.Fabijanska-Mitek J. Vox Sanguinis 1997; 72: 233-237The authors adapted the DiaMed ID gel test to detect IgG subclasses by adding IgG specificsubclass antisera to sensitised red cells. IgG subclass was identified in all 49 samples from
AIHA patients tested. IgG1 was present in 96% of samples with other IgG subclasses alsopresent in 59%. In this study, the gel test was more sensitive than the tube technique fordetermining IgG subclass.
Serology of antibodies to second- and third-generation cephalosporins associatedwith immune hemolytic anemia and/or positive antiglobulin tests.
Arndt P. et al. Transfusion 1999; 39: 1239-46 A comprehensive study of cephalosporin related AIHA with samples referred to one laboratorybetween 1984 and 1999. This paper identified 43 patients with antibodies to cefotetan, 8 toceftriaxone and one case each with antibodies to cefoxitin and cefotaxime. Laboratory methodswere described to classify each of these antibodies as being secondary to drug adsorption,immune complex formation or the autoantibody (drug independent) mechanism. Antibodies to
cefotetan were identified using both the first two methods and in 40% the drug independentmethod as well. Ceftriaxone antibodies were identified using the immune complex method.
This study highlighted the second and third generation cephalosporins as an increasinglyrecognised cause of severe drug associated AIHA. The significance of this reaction wasreflected in the mortality rate with 8 deaths associated with cefotetan and 4 with ceftriaxonetherapy.
The detection of alloantibodies against red cells in patients with warm-typeautoimmune haemolytic anaemia.Engelfriet C. & Reesink H. Vox Sanguinis 2000; 78: 200-207
This article was presented in a question and answer format with questions related to thefrequency and investigation of alloantibodies in patients with AIHA. Experts from North
America, Europe and Asia individually answered the set questions and an attempt at aconsensus view was expressed.
The frequency of alloantibodies varied from 47% in America to 11% in Hong Kong. Themethods used to detect alloantibodies varied between centres but all agreed that detection bydilution was only recommended during emergencies and that autoabsorption should not beused if the patient had been recently transfused. Most centres transfused these patients withRh-phenotype and Kell-compatible cells.
8/9/2019 2001_Vol8_1 transfusi
7/20
February 2001Vol 8, No 1
7
Cl in ica l St ud ies
AIHA has been reported to occur relatively frequently in patients suffering from ChronicLymphocytic Leukaemia (CLL). It has also been increasingly recognised to occur aftertreatment of CLL with purine analogues such as fludarabine and cladribine.
Autoimmune hemolytic anemia in chronic lymphocytic leukaemia: clinical,therapeutic, and prognostic features.Mauro F. et al. Blood 2000; 95: 2786-2792This is a large retrospective study looking at 1203 consecutive CLL patients at a singleinstitution between 1986 and 1996. In this cohort, 52 cases (4.3%) of autoimmune haemolyticanaemia were identified using standard clinical criteria. 19 cases were identified at diagnosisand 33 during follow-up with 90% of these patients showing evidence of active CLL at the timeof their anaemia. The authors identified three risk factors at diagnosis that correlated with anincreased risk of developing AIHA: an absolute lymphocyte count >60x109 /L, age greater than65 years and male gender.
Most patients (84%) achieved a response to treatment of the anaemia with either prednisonealone (4 patients) or prednisone and chlorambucil (46 patients). However, this response wasslow with a median time of 4.5 months to reach a haemoglobin value of 120g/L.
Interestingly, only 13 of the 52 patients had previous treatment and in this group AIHAdeveloped with a similar frequency in those treated with chlorambucil and prednisone comparedto those treated with fludarabine and prednisone. The risks of fludarabine in this study werenot demonstrated to be as significant as previous observations relating to the use of this agentin CLL.
Autoimmune haemolytic anaemia in patients with chronic lymphocytic leukaemiatreated with 2-chlorodeoxyadenosine (cladribine).Robak T. et al. European Journal of Haematology 1997; 58: 109-113In this smaller retrospective study, Robak et al. reviewed 114 patients with advanced CLL (Raistage III or IV) treated with cladribine between 1992 and 1995. AIHA was detected in 25 ofthese patients. This high rate of anaemia (21.9%) was attributed to the more advanceddisease in this cohort. The majority of the patients (23 out of 25) developed the anaemia priorto commencement of the purine analogue. After commencement of cladribine, with or withoutprednisone, the anaemia completely resolved in 6 patients and in 8 patients there was asignificant improvement in the haemoglobin level. In this study, only 2 of the patientsdeveloped AIHA after cladribine. These two patients developed moderate to severe anaemiaafter 5 and 6 courses of the drug respectively. One of these patients died after a central
nervous system haemorrhage associated with thrombocytopenia.
Purine analogue drugs have been increasingly used in the treatment of lymphoproliferativedisorders, however, concern regarding the initiation or exacerbation of AIHA has remained.This study demonstrates a relatively low, but significant risk of haemolytic anaemia withcladribine.
The relatively high frequency of AIHA in CLL has been attributed to immune dysregulation. Thepurine analogues may further contribute to this process by their profound suppressive effect onT lymphocytes. Similar immune system dysregulation is present after bone marrowtransplantation and AIHA is an increasingly recognised complication of this procedure.
8/9/2019 2001_Vol8_1 transfusi
8/20
February 2001Vol 8, No 1
8
Late onset haemolysis and red cell autoimmunisation after allogeneic bone marrowtransplant.Chen F. et al. Bone Marrow Transplantation 1997; 19: 491-495 Chen et al. retrospectively reviewed the records of 293 patients who received an allogeneicbone marrow transplant at one centre from 1989 to 1994. An autoimmune reaction against
erythrocytes (identified by DAT or cold agglutination) was demonstrated in 9 patients with 7having significant haemolysis. The authors divided the reaction into 2 types: an early onsettype characterised by the appearance of a cold reacting antibody 2-8 months after transplant.This occurred in 4 of the patients. The other 5 patients developed a warm panreactiveautoantibody 6 to 18 months after the transplant.
This overall incidence of 3.1% is significantly higher than the general population and mayreflect abnormal immune system function in the recipient of the transplant. The authorssuggest that the predominant antibody in the two categories may reflect the kinetics of immunesystem reconstitution after transplantation. The cold reacting antibody was clinically present 2to 6 months after the transplant, when IgM levels typically return to normal. The warmautoantibody appeared later, when IgG levels return to normal 12-16 months after theprocedure.
Autoimmune hemolytic anemia in patients with SCID after T cell-depleted BM andPBSC transplantation.Horn B. et al. Bone Marrow Transplantation 1999; 24: 1009-1013
A cohort of 41 children with severe combined immunodeficiency (SCID) who had a non-myeloablative T cell depleted stem cell or bone marrow transplant were examined. Eight ofthese patients developed AIHA at a median of 8 months after the transplant. Unlike theprevious study, all of these patients had warm reacting antibodies with 2 of the cases havingadditional cold reactive autoantibodies. The only risk factor identified to predict AIHA was thesource of stem cells with more children developing AIHA after a peripheral blood stem cell
transplant than those receiving a bone marrow transplant.
This study demonstrated a particularly high rate (19.5%) of AIHA post transplant in thisspecialised cohort of immunodeficient children. The authors attribute this high rate to thedelayed reconstitution of T cell immunity secondary to the T cell depleted transplant and to theimmunosuppressive conditioning.
T r ea tmen t
Comparative response to splenectomy in Coombs-positive autoimmune hemolytic
anemia with or without associated disease. Akpek G. et al. American Journal of Hematology 1999; 61: 98-102 Akpek et al. retrospectively reviewed 30 cases of AIHA that progressed to splenectomy in theirinstitution from 1978 to 1997. Eleven patients with idiopathic AIHA progressed well, with 9patients obtaining a complete response and 2 patients attaining a partial remission. This wascompared with 18 patients who had AIHA associated with other systemic diseases (CLL in 9,Non Hodgkins Lymphoma in 4, Systemic Lupus Erythematosus in 1, Collagen vascular disease in1, Myelofibosis in 1). Responses in this group were comparatively poor with only 3 patientsobtaining a complete response and 6 achieving a partial response. Postoperative morbidity andmortality were also greater in the group with haemolysis secondary to a systemic illness.
8/9/2019 2001_Vol8_1 transfusi
9/20
February 2001Vol 8, No 1
9
Transfusions of polymerized bovine hemoglobin in a patient with severeautoimmune hemolytic anemia.Mullon J. et al. New England Journal of Medicine 2000; 342: 1638-1643
A case report of a 21 year old woman who developed severe AIHA refractory to all standardtherapies. She was transfused on 7 separate occasions with a solution of bovine haemoglobin
(HBOC-201) over a seven day period. This solution reversed electrocardiographic andbiochemical evidence of end organ ischaemia during and after infusion.
The Editorial in the same issue of this journal reviews the three general classes of red cellsubstitutes: perfluorochemicals, liposome-encapsulated haemoglobin and haemoglobin basedoxygen carriers. Potential advantages and clinical complications associated with the differentformulations are discussed. As these substitutes lack cell surface antigens they may have anincreasing role in the treatment of severe AIHA in the future. However, refractory AIHA isobviously a limited indication for a red cell substitute and a successful product would have manyvaried indications as a safe alternative to blood transfusion.
8/9/2019 2001_Vol8_1 transfusi
10/20
February 2001Vol 8, No 1
10
2 . W HAT I S O PTI MAL P LATELET T RANSFUSI ON T HERAPY ?
Dr. Wendy Erber, Dr. Andrew McQuillan, Dianne Grey
Haematology, WA Centre for Pathology Medical Research, Nedlands WA 6009
Platelet transfusion therapy became available in the 1970s and although the major uses arecurrently in haematology, oncology and haemopoietic transplantation, platelets are also used insurgery and massive transfusion. Platelet transfusion therapy is now common practice in thesesettings but there are many aspects that remain unresolved. These include the indications fortransfusion, the optimal method for platelet preparation, the platelet dose and frequency ofadministration and how best to monitor the efficacy of the platelet transfusion. This paperoutlines the current situation with platelet transfusion therapy in Australia and addresses someof these issues. The text is a transcript from the talk entitled “What is Optimal PlateletTherapy?” presented at the Adelaide Blood Club in October 2000.
H i st o r y o f p l a t e l et t r ans f u s ion
Unlike red cells, the history of platelet transfusions is short and has only developed over thepast 40 years. However, it was in 1910 that Duke first noted that platelets from whole bloodreduce the bleeding time 1. This was the first evidence of a potential role for platelet transfusiontherapy. In the 1950s platelets were collected and transfused, but only for diagnostic purposes.In the 1960s plastic blood bags became available which enabled platelets to be separated fromwhole blood collections by centrifugation. In the 1970s it was discovered that platelet functionwas best preserved if the platelets were stored at room temperature with agitation. Thisresulted in the introduction of prophylactic platelet transfusions for patients with leukaemia.
New methods for platelet transfusion were introduced in the 1980s using cytapheresistechniques and this was further refined in the 1990s with methods of collecting leucocytereduced platelet products. The success of platelet transfusion therapy has been critical fordevelopments in many areas of modern medical and surgical management. In the 1990s wewitnessed a 5% annual increase in platelet transfusion therapy, primarily to supportmyelosuppressive therapies associated with haemopoietic transplantation. Currently,approximately 70-80% of platelets are used for prophylaxis in haemato-oncology. Despite thenow widespread use of platelets there have been few clinical trials to define a practicalconsensus approach to prophylactic platelet transfusion.
I n d i ca t i ons fo r p l a t e l e t t r ansf u s ion
Put simply, platelet transfusion therapy is providing temporary platelet replacement therapy fora reduction in platelet number or platelet function. Some of the physiological factors that shouldbe taken into consideration prior to administering platelets are:
1. The bleeding time prolongs when the platelet count falls to < 100 x 109 /L2. Normal homeostasis results in daily utilisation of 7 x 109 /L platelets3. Spontaneous small blood vessel bleeding occurs at a platelet count of < 5 x 109 /L
8/9/2019 2001_Vol8_1 transfusi
11/20
February 2001Vol 8, No 1
11
Platelet transfusions are given either as therapy or for prophylaxis. The therapeutic indicationsfor platelet transfusion therapy outlined at a recent Consensus Conference 2 are: -
1. Thrombocytopenic bleeding with platelet count < 50 x 109 /L
2. Dilutional thrombocytopenia (eg: massive transfusion)3. Platelet dysfunction and bleeding.
However, the major indication for platelet transfusion therapy is prophylaxis forthrombocytopenia secondary to myelosupression (eg. marrow transplantation). What is theplatelet trigger at which platelets should be administered to avoid haemorrhage? This has beenaddressed in a number of studies but remains controversial. One randomised study3 suggestedthat the trigger for prophylaxis could be set at < 5 x 109 /L for patients with leukaemia. Anotherrecent randomised controlled study of acute myeloid leukaemia patients showed that withplatelet counts of < 10 x 109 /L there was no increase in bleeding resulting in mortality than withhigher platelet thresholds4. Although this study has not been repeated in other haematologicaldisorders with myelosupression, the trigger of 10 x 109 /L has been adopted by many centres forprophylaxis regardless of the nature of the underlying disease. If additional risk factors (eg.sepsis, drugs) are present it is still unclear whether the platelet trigger should be at a higherplatelet count. For myelosuppressed patients who require platelet prophylaxis prior to aninvasive procedure, a trigger of > 50 x 109 /L is usually accepted.
One issue complicating the platelet trigger for prophylaxis is the accuracy of haematologyanalysers at low platelet counts. It has been shown that platelet counts obtained usinganalysers that use impedance methods tend to overestimate the platelet count and have poorreproducibility at low platelet counts. Analysers using optical methods and CD61 monoclonalantibody (recognising platelet glycoprotein IIIa) have greater accuracy and reproducibility atlow platelet levels. Improving the accuracy of the platelet count could result in lowering the
platelet transfusion threshold without increasing the bleeding risk.
Other causes of thrombocytopenia must be considered individually prior to considering whetherplatelet transfusion therapy is indicated5. In immune thrombocytopenic purpura, platelettherapy is usually only given to patients with active haemorrhage. For post-transfusion purpuraand neonatal alloimmune thrombocytopenia, antigen-negative platelets are required. In clinicalsituations where there is increased platelet activation and consumption (eg: HUS, TTP) platelettransfusion therapy is contraindicated due to the risk of thrombotic episodes. For patients withuraemia, DIC and hepatic failure platelet therapy should be considered on an individual basis.
Pla t e l e t p r odu c t s
In Australia, the majority of platelets for transfusion are obtained from whole blood donations.These undergo centrifugation to prepare random donor platelets or buffy coat platelets. Inrecent years there has been a move, in some states, to single donor platelets (SDP) collectedby cytapheresis. This has been the case in Western Australia where up to 90% of platelets arecollected by cytapheresis. Table 1 outlines the properties of random donor platelets (RDP),buffy coat platelets and single donor (cytapheresis) platelets.
8/9/2019 2001_Vol8_1 transfusi
12/20
February 2001Vol 8, No 1
12
Table 1: Properties of platelet concentrates
Random
donor
platelets
Buffy coat
platelets
Cytapheresis
platelets
Preparation Prepared from
centrifugation of
whole blood
derived platelet
rich plasma
Prepared from
centrifugation of
whole blood derived
buffy coats
Prepared by
apheresis from a
single donor
Donor number Multiple Multiple One
Volume 45-60 mL 40-60 mL 200-300 mL
Platelets 5.5 x 10
10
3 x 10
11
5 x 10
10
Leucocytes 7-9 x 1010 1 x 107 < 1 x 106
Red Cells < 1 mL rare < 1 mL
pH 7.35 7.16 7.30
IL-1 (Day 1) 0 6 pg/mL 0
IL-6 (Day 1) 140 pg/mL 73 pg/mL
8/9/2019 2001_Vol8_1 transfusi
13/20
February 2001Vol 8, No 1
13
In most centres the only in vitro testing performed is the platelet count, pH and macroscopicassessment of platelet swirling. Other tests which could be performed to assess platelet qualityinclude assessment of platelet morphology, platelet aggregation, platelet glycoproteinmeasurements and production of platelet activation markers (eg: RANTES, PF4, TGF). In vivo testing of the quality of the transfused platelets is even more difficult. The post-transfusion
platelet count increment is a simple test which should be performed routinely. Radio-labelledplatelet kinetics are also available but are impractical clinically.
Does the method of platelet collection affect the degree of platelet activation? Sloand et al8 found decreased membrane expression of glycoprotein Ib (CD42b) and increased expression ofCD62 (P-selectin) in random donor platelets, reflecting greater platelet activation compared tosingle donor platelets. A recent study9 compared platelet activation in single donor plateletscollected by two methods. With both methods there was accumulation of RANTES, PF4 and TGFwith storage. Serotonin, a dense granule constituent of platelets, was also found in highconcentration. The study concluded that there is a high degree of platelet activation in plateletscollected by apheresis methods.
P la t e l e t con tam ina t i on
Febrile non-haemolytic transfusion reactions (FNHTR) to platelet concentrates commonly occurand have been attributed to the presence of leucocyte-derived cytokines in the plasma. Theseadverse reactions increase in frequency and severity with storage time of the platelets. Theconcentration of the cytokines interleukin-6 (IL-6), tissue necrosis factor alpha (TNFα) andinterleukin-1 beta (IL-1β) increase with storage particularly in platelet concentrates containing
> 3 x 109 /L leucocytes10,11. Cytokine accumulation commences from day 1 but is most markedafter day 3 and levels are highest at 5 days of storage12. Leucocyte depletion of plateletproducts has been shown to reduce the incidence of FNHTR; in the presence of adequateleucocyte depletion of platelet products (< 5 x 106) the incidence of FNHTR is not affected by
platelet storage time. The type of platelet product has no effect on the incidence of FNHTRprovided it is sufficiently leucocyte depleted.
RANTES, a monocyte and T-cell chemoattractant stored in platelet α-granules, has been
detected in the supernatant of platelet products. Platelet concentrates involved in allergicreactions have been found to contain high concentrations of RANTES13.
Platelet products can also potentially be contaminated with infectious agents. Bacterialcontamination has an incidence of 0.1%-10% and is greatest with older platelets 14. Viruses arealso carried by contaminating leucocytes. The current discussions of variant CJD suggests that
the potential infective agent is carried by platelets. Table 2 lists some of the problemsassociated with leucocyte contamination of platelet products.
8/9/2019 2001_Vol8_1 transfusi
14/20
February 2001Vol 8, No 1
14
Table 2: Effects of leucocyte contamination of platelet products
Cytokine accumulation IL-1, IL-6, TNFα
FNHTR: 5% incidence
HLA allo-immunisation
Platelet refractoriness HLA-antibody mediated
Transfusion transmitted
infection
Viral infections, eg. CMV, HIV
Immuno-modulation Post-operative sepsis
Tumour recurrence
How to avo i d t he p l a t e l e t s t o r age l esi on?
The platelet storage lesion appears to be primarily due to platelet activation in vitro andaccumulation of leucocyte derived cytokines. In Western Australia, to avoid transfusingplatelets affected by the storage lesion, attempts are made to transfuse platelets after no morethan 3 days storage. This avoids the degradation in platelet quality over time and the time-
dependent increase in pro-inflammatory cytokines. This can be achieved by altering theinventory management strategy to a last-in-first-out (ie. the freshest platelets are issued first)approach. This contrasts with the traditional policy of first-in-first-out (ie. issue the oldestplatelets first). The last-in-first-out approach results in fresher platelets being transfused topatients with similar out-dating of platelets15. This approach requires further discussion betweenthe producers of platelets and the users.
Pre -p l at e l e t t r ans f u s i on tes t i ng
In most transfusion laboratories the only pre-platelet transfusion testing is a baseline plateletcount and ABO and Rh (D) blood groups. Screening for HLA and HPA antibodies is usually onlyperformed for refractory patients, those with neonatal alloimmune thrombocytopenia orthrombocytopenia for investigation. Platelet HPA and HLA typing are also not routinelyperformed prior to transfusion in Australia. As a result, in Australia, as in most countries, ABOand Rh (D) compatible platelets are used.
There have been few studies comparing transfusion outcomes of HPA and/or HLA matchedplatelets with ABO compatible platelets. One study of acute myeloid leukaemia patients showedno significant difference in the platelet increment achieved when HPA-matched platelets wereused routines. However, some centres in France are routinely providing HLA and HPA matchedplatelets to platelet dependent patients. For refractory patients crossmatched platelets, HLAand/or HPA matched platelets or HLA-antigen negative platelets are usually transfused.
8/9/2019 2001_Vol8_1 transfusi
15/20
February 2001Vol 8, No 1
15
Pla t e l e t dose
There is no standard dose for platelet transfusion in medical practice. Historically, ten units ofrandom donor platelets (RDP) were issued but now a more common dose is either four or sixunits of RDP or one single donor platelet (apheresis) unit. In a few centres, the dose ofplatelets is based on patient weight (eg: 5 x 1010 / 10 kg body weight). At present the optimal
platelet dose remains poorly defined and is often determined by supply.
Wh a t i s t he op t im a l p l a t e l e t dose?
Should one platelet dose be used for all adult patients, and, if so, what is that dose? There isuniversal controversy over the platelet dose and the frequency of its administration. Whenreviewing the literature on this subject, one must be careful in the definition of “dose”. In theUSA, the definitions of “dose” are:
§ Low dose : 2.5 – 3.5 x 1011 platelets§ Medium dose: 3.5 – 6.0 x 1011 platelets§ High dose : 6.0 – 8.0 x 1011 platelets§ Very high dose: > 8.0 x 1011 platelets
In Australia the platelet dose varies from 2.4 – 3.0 x 10 11 platelets (ie. equivalent to USA “lowdose”). The type of platelet product and product availability often determine the precise doseof platelets administered. For random donor platelets and buffy coat platelets, the number ofplatelets per bag are generally fixed by the method of preparation; the number of bagstherefore determines the dose and dose escalation is possible. Single donor platelet collectionsresult in a total of approximately 6.0 x 1011 platelets. Collections are frequently split into twobags giving a therapeutic dose of 3.0 x 1011. Platelet collection by cytapheresis does allow for
“dial-a-dose” to tailor the platelet dose to the specific patient.
If the platelet dose is poorly defined by the producers of platelet products, is it possible todetermine the appropriate dose on clinical grounds? For therapeutic platelet transfusion, asimple dose definition would be: “sufficient platelets to control the bleeding”. However, thispresumes that the bleeding is solely due to thrombocytopenia; this is rarely the case (eg.massive transfusion; DIC). For prophylactic platelet therapy, the aim should be to increase theplatelet count to a haemostatic level (eg. minimum of 40 x 109 /L). The platelet dose cantherefore be based on sufficient platelets being transfused to achieve this target platelet count.However, in the clinical setting, the outcome of platelet transfusion is also influenced by anumber of clinical factors such as splenomegaly, fever, antibiotics and current bleeding.
Pla te le t t ran s fus ion do se–response st ud ies
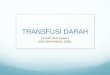
Studies have been performed to establish the optimal platelet dose for prophylaxis inhaematological malignancies. Norol et al16 performed a dose-response study comparingmedium (4-6 x 1011 platelets), high (6-8) and very high (>8) platelet doses for prophylaxis forpatients with haematological malignancies. The results showed that the higher the platelet doseadministered, the greater the transfusion interval and the smaller the number of plateletsrequired (Figure 1). In a similar prospective, randomised double-blind trial17, 46 patientsreceiving myelosupressive therapy received either low dose (2.5-3.5 x 1011) or high dose (4.5-6.1) platelets. Results showed that low platelet dose resulted in a lower platelet increment,shorter transfusion free interval and a greater risk of acquiring additional transfusions.
8/9/2019 2001_Vol8_1 transfusi
16/20
February 2001Vol 8, No 1
16
Figure 1: Platelet-dose response study showing that higher platelet increments and greater transfusion
intervals are obtained with transfusion of higher doses of platelets (from Norol et al16)
Brecher and Goodnough18 further analysed the data of Klumpp et al. 17 and agreed that highdose platelets resulted in a better platelet transfusion increment and increased transfusioninterval. However there was a 15% increase in the overall number of platelets transfused inthose receiving high dose platelets. In contrast, the lower platelet dose, in this study 2.5-3.5 x
1011
platelets, resulted in fewer platelets transfused overall. Another study by Hersh et al19
ofmathematical modelling and platelet transfusion therapy, predicted that large dose platelettransfusions would result in a greater transfusion interval but more platelets would be used.This model confirmed the Brecher and Goodnough18 analysis that optimal platelet therapyrequires more frequent use of smaller doses of platelets, comparable to doses currently used in
Australia.
The above-mentioned studies show that the optimal dosing strategy remains far from certain.The data suggest that small (2.5-3.5 x 1011) frequent fixed dosage schedules result in lessplatelet usage than larger doses. However, this approach will result in greater donor exposurepotentially increasing the risk of allo-immunisation and disease transmission. Platelet dose may
also be influenced by the clinical situation of the patient. For example, small frequent plateletdosing may be appropriate for an in-patient cohort but a larger platelet dose at greatertransfusion intervals may be more acceptable for out-patients. Studies have not addressedwhether a variable dosing regimen (eg. based on patient weight) may be preferable to a fixedadult dose. A number of clinical studies therefore remain to be performed to finally answer thequestion of appropriate dose. In the meantime, in Australia, product availability rather thanoutcomes of randomised studies or scientific rationale will probably determine platelet dosing.Unfortunately the advent of donor deferral strategies to minimise the theoretical risk oftransfusion of variant CJD by transmission may further impact on platelet supply and dictate theplatelet dose.
33
28
62
29
2.6
51
30
3.3 4.1
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
Platelet increment Recovery (%) Tx interval (days)
Medium
High
Very High
8/9/2019 2001_Vol8_1 transfusi
17/20
February 2001Vol 8, No 1
17
Mon i t o r i ng o f p la te l e t t r ans fus ion e f f i cacy
How should we best monitor the effectiveness of the platelet transfusion? For therapeuticindications the best monitor is control of bleeding. For prophylactic platelet transfusions, thepost-transfusion platelet count, platelet increment and corrected count increment provide a
guide to optimal outcome21
. The post-transfusion platelet count should be performed at 10minutes to 1 hour post-transfusion and again repeated at 16 to 24 hours. The immediate post-transfusion platelet count gives a good indication as to whether there has been the appropriateresponse or whether there may be antibody-mediated platelet destruction. By 16 to 24 hours,recurrent thrombocytopenia is more commonly disease-related. A poor immediate post-transfusion platelet count and corrected count increment should be followed by antibodyscreening for HLA or HPA antibodies to diagnose antibody mediated platelet refractoriness.
A l t e r na t i v es to p l a t e l e t s
Currently there are no commercial available alternatives to platelets for transfusion. Cytokinessuch as thrombopoietin and PEG-hMGDF and interleukin-11 have undergone clinical trials forthe management of myelosuppressive-induced thrombocytopenia. Fixed, freeze-dried plateletsand infusible platelet membranes have also undergone clinical studies. Synthetic products suchas fibrinogen-coated albumin microspheres and thromboerythrocytes are currently in phase I/IItrials and pre-clinical trials. However, these have already been shown to have limited t½, and,when adopted for clinical practice, will primarily be used for haemostasis in acute settings.Currently, there is little published data on their efficacy. There does not appear to be anappropriate alternative to platelets for prophylaxis for thrombocytopenic patients.
SO, WHAT IS OPTIMAL PLATELET THERAPY?
This review has raised a number of questions regarding optimal platelet transfusion therapy.The trigger for platelet prophylaxis appears to be reasonably well accepted as 10 x 109 /L. Tominimise the effects of the platelet storage lesion, fresh platelets (stored less than 3 days) areadvocated. This will optimise platelet quality and maximises patient benefit. This could best beachieved by adopting a last-in-first-out inventory management approach. Random donorplatelets, cytapheresis (SDP) platelets and buffy coat platelets all suffer problems of plateletactivation on storage. Leucocyte depletion of the product, ideally at source or within 24 hoursof collection, will result in less accumulation of leucocyte-derived pro-inflammatory cytokinesthat cause FNHTR (5% of platelet transfusion recipients).
The optimal platelet dose remains controversial and randomised dose finding studies areneeded. In particular, variable dosing versus fixed dose studies are needed. It would also be
beneficial to assess whether continuous platelet infusions are possible, particularly in the settingof prophylaxis for patients with concurrent clinical problems (eg. sepsis, drugs). Studies arealso required to determine the best way to show clinical efficacy of the platelet transfusiontherapy. Progress in these areas should occur over the next 3 to 5 years. Immediate post-transfusion platelet counts and platelet antibody screening need to be adopted universally todetect early evidence of alloimmunisation and thereby prevent the serious managementproblems associated with platelet transfusion refractoriness.
In addition to the clinical issues described above, further studies are required to address thequality of the platelet products.
8/9/2019 2001_Vol8_1 transfusi
18/20
February 2001Vol 8, No 1
18
Issues such as the optimal method for collection and preparation of platelets, the role ofplatelet additive solutions, the optimal platelet storage time and conditions, viral inactivationand methods for optimal preservation and reconstitution of autologous platelets. The role of thevarious alternatives to platelets will need to be addressed once clinical studies of the newsynthetic products are available. Finally, communication between suppliers and users of
platelet products are critical to ensure optimal platelet transfusion therapy is administered toour patients.
REFERENCES
1. Duke WW. The relation of blood platelets to hemorrhagic disease. JAMA 1910; 55: 1185-92
2. Contreras M. Final statement from the consensus conference on platelet transfusion.Transfusion 1998; 38: 796-7.
3. Gmür J, Bwger J, Schanz U, Fehr J and Schaffner A. Safety of stringent prophylactic platelet
transfusion policy for patients with acute leukaemia. Lancet 1991; 338: 1223-6.4. Rebulla P, Finazzi G, Marangoni F et al. The threshold for prophylactic platelet transfusions
in adults with acute myeloid leukaemia. N Engl J Med. 1997; 337: 1870-5.
5. Friedberg RC and Geupp B. Platelet transfusion: Indications considerations and specificclinical settings. In: Current issues in platelet transfusion therapy and platelet alloimmunity.Kickler TS and Herman JH (Eds). AABB Press 1999: 1-32.
6. Kickler TS and Herman JH. Issues in platelet storage. In: Current issues in platelettransfusion therapy and platelet alloimmunity. AABB Press. 1999: 63-76.
7. Bode AP. Platelet activation may explain the storage lesion in platelet concentrates. BloodCells 1990; 16: 109-26.
8. Sloand EM, Yu M and Klein HG. Comparison of random-donor platelet concentratesprepared from whole blood units and platelets prepared from single-donor apheresiscollections. Transfusion 1996; 36: 955-9.
9. Wadhwa M, Seghatchian MJ, Dilger P, Sands D, Krailadisiri P, Contreras M and Thorpe R.Cytokines in WBC–reduced apheresis PCs during storage: a comparison of two WBC-–reduction methods. Transfusion 2000; 40: 1118-26.
10. Muylle L, Wouters E, DeBock R et al. Reactions to platelet transfusions, the effect of thestorage time of the concentrates. Transfusions Medicine 1992; 2: 289-93.
11. Stack G and Snyder E. Generation of cytokines in stored platelet concentrates. Transfusion
1993; 34:20-5.
12. Grey D, Erber WN, Saunders KM and Lown JAG. Monocyte activation in plateletconcentrates. Vox Sang 1998; 75: 110-4.
13. Klüter H, Bubel S, Kirchner H and Wilhelm D. Febrile and allergic transfusion reactions afterthe transfusion of white cell-poor platelet preparations. Transfusion 1999; 39: 1179-84.
14. Marrow JF, Braine HG, Kickler TS et al. Septic reactions to platelet transfusion, a persistentproblem. JAMA 1991; 266: 555-8.
8/9/2019 2001_Vol8_1 transfusi
19/20
February 2001Vol 8, No 1
19
15. Lasky LC, Gannon T, Kennedy MS, Agarwal IT, Counts F and Ng A. Last-in-first-out plateletconcentrate inventory practice allows fresher and better matched transfusions thantraditional first-in-first-out. Transfusion 1999; 39: 140-1.
16. Norol F, Bierling P, Roudot-Thoraval F et al. Platelet transfusion: a dose-response study.Blood 1998; 92: 1448-53.
17. Klumpp TR, Herman JH, Gaughan JP et al. Clinical consequences of alterations in platelettransfusion dose: a prospective randomised, double-blind trial. Transfusion 1999; 39: 674-81.
18. Brecher ME and Goodnough LT. Clinical consequences of alterations in platelet transfusiondose: a prospective randomised, double-blind trial (letter). Transfusion 2000 40: 383-4
19. Hersh JK, Ham EG and Brecher ME. Mathematical modeling of platelet survival withimplications for optimal transfusion practice in the chronically platelet-transfusion dependentpatient. Transfusion 1998; 38: 637-44.
20. Benson K. Criteria for diagnosing refractoriness to platelet transfusions. In: Current issues
in platelet transfusion therapy and platelet alloimmunity. Kickler TS and Herman JH (Eds). AABB Press 1999; 33-61.
8/9/2019 2001_Vol8_1 transfusi
20/20
February 2001Vol 8, No 1
20
3 . Le t t e r t o t he Ed i t o r
Dear Sir.
Re: TRALI prevention.
The reprinted paper “TRALI: Transfusion Related Acute Lung Injury” from America’s BloodCenters in the December 2000 issue of “Topics” was a useful summary of various aspects ofthis potentially fatal condition. However, it should be pointed out that two of therecommendations in the “Prevention” section are by no means universally accepted, arecertainly not followed in Australia, and could even be considered clinically dangerous:
1. "P lasm a f rom im p l i ca ted donors shou ld be d ive r ted fo r pro t e in f ract i ona t i on " iscompletely contrary to the approach taken here in Australia. Our plasma fractionator, CSLBioplasma, will not accept plasma for fractionation from such donors when the causative
antibody has been shown to have anti-granulocyte specificity.2. "Transfus ion of pRBCs f rom such don ors . .. .. .i s acceptab le due t o t he sm al lvo lume o f p lasm a in the componen t " is a very dangerous generalisation indeed. Thecases we have investigated have led us to conclude that even the small amount of plasmain a single unit of concentrated red cell is most definitely capable of causing severe TRALI.
To ensure the safety of the Australian blood supply The Australian Red Cross Blood Serviceensures that any blood donor whose donation has been shown to be the cause of a TRALI ispermanently removed from the normal donor panel.
Brian Fisher ARCBSPerth, WA