-
7/29/2019 239_metabolik hastalklar (1)
1/17
METABOLIC EMERGENCIES IN THE NEONATEN. Guffon, Edouard Herriot
Hospital, Pediatrics, Lyon, France
U. Simeoni, Timone University Hospital, Neonatology, Marseille,
France
J.B. Gouyon, University Hospital, Neonatology, Dijon, France
-
7/29/2019 239_metabolik hastalklar (1)
2/17
Index
(Saudubray 2002, Saudubray & Ogier de Baulny 1995)
When to think metabolic
Immediate investigations
Which emergency measures need to be undertaken?
Diagnostic algorithm
Specific investigations
Case examples
E
MERGENCY
POSTEMERG
ENCY
-
7/29/2019 239_metabolik hastalklar (1)
3/17
When to think metabolic ( 1 )
Initial symptoms:
lethargy (or just not well)
refusal to feed, poor sucking,vomiting
poor weight gain
polypnoea
hypothermia
axial hypotonia
limb hypotonia
abnormal movements (boxing, pedalling,tremor, ...)
hepatomegaly
With possible progression to:
altered consciousness, seizures, coma, multivisceral failure
(Saudubray 2002, Saudubray & Ogier de Baulny 1995)
-
7/29/2019 239_metabolik hastalklar (1)
4/17
When to think metabolic ( 2 )
Note:symptoms are usually non specific,
metabolic disease may be excluded when obvious cause is
known
Careful!Metabolic diseases are often associated with
infections!
Additional factors
initial symptom free interval
consanguinity
family history (previous neonatal deaths, possibly
unexplained)
deterioration despite symptomatic therapy (possibly
unexplained)
(Saudubray 2002, Saudubray & Ogier de Baulny 1995)
-
7/29/2019 239_metabolik hastalklar (1)
5/17
Immediate investigations(parallel to screening for sepsis)
Blood: Ammonemia, Bicarbonates, Glucose, Transaminases,
Prothrombin time, Lactic acid, Uric acidUrine: Ketonuria
(colorimetric bedside test), unusual odour or colour, pH
Note:Ketonuria is always an indicator for a me tabolic disease
in the ne wborn.Increased Uric acid is indicative for organic
aciduria
Thrombopenia and Neutropenia are criteria for severity in
organic aciduria(an increased urine pH with acidosis, without
Ketonuria is suggestive of renal tubular acidosis)
Supplementary samples to be taken before starting emergency
therapy for specific investigations:
Blood: 4-5 ml blood, sampled on lithium heparinate, centrifuge
rapidly, store plasmafrozen at -20C, if not immediately
analysed
Urine: First miction (store at -20C)
-
7/29/2019 239_metabolik hastalklar (1)
6/17
Which emergency measures need to be undertaken? ( 1 )Within 24
to 48 hours of presentation, i.e. before the diagnosis of a
specific metabolic
disease and the respective treatment are established.
Scenario 1:
No acidosis, no ketonuria, hyperammonaemia
suspected UCD
High caloric, protein-free nutrition, preferentially through
continuous
enteral feeding (100-130 kcal/kg/day, 65-70% carbohydrates)
Insulin for reinforcement of anabolism (dose: 0.02 - 0.1
Units/kg/h);
Check regularly for glycaemia and readjust the dose if
needed
Ammonaps (Sodium Phenylbutyrate) through nasogastric tube:
250-600 mg/kg/day in 4 doses
Sodium Benzoate iv: 200-500 mg/kg/day in 4 doses
Arginine iv: 100-150 mg/kg/day in 4 doses
-
7/29/2019 239_metabolik hastalklar (1)
7/17
Which emergency measures need to be undertaken? ( 2 )
Scenario 2:
Acidosis and/or ketonuria, with or without hyperammonaemia
suspected Organic aciduria or MSUD (Maple Syrup Urine
Disease)
High caloric, protein free nutrition (as mentioned)
Insulin (as mentioned)
Hydroxocobalamine, 1-2 mg/day, IV
Biotine, 10-20 mg/day, IV or oral
Thiamine 10-50 mg/day, IV or oral in 1-2 doses
Riboflavine 20-50 mg/day, IV or oral in 1-2 doses
Carnitine 100-400 mg/kg/day, IV in 4 doses
In any case:an emergency toxin removal may be needed. Prepare
for toxin removal procedures.
-
7/29/2019 239_metabolik hastalklar (1)
8/17
Which emergency measures need to be undertaken? ( 3 )
Note: Bicarbonate infusion for correction of acidosis is NOT
recommended;
only in renal tubular acidosis or in pyroglutamic aciduria!
If no improvement after 4-6 hours of treatment then start toxin
removal procedure, such as:
Peritoneal dialysis
Continuous Hemodialysis/Hemodiafiltration
Note: Hemodialysis is shown to be the most effective method
(Gouyon et al 1994, Ogier de Baulny 2002, Schfer 1999)
however, the choice for a particular method may depend on local
availability and experience.
-
7/29/2019 239_metabolik hastalklar (1)
9/17
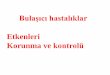
Diagnostic algorithm
METABOLIC ACIDOSIS
HYPERAMMONEMIA
Ketonuria Ketonuria
Hyperlactatemia
Hypoglycemia
Major hyperlactatemia Maple Syrup Urine
Disease (MSUD)
Maple Syrup Urine
Disease (MSUD)
HypoglycemiaOrganic
aciduria
Organic aciduria
Pyroglutamicaciduria
Non-ketonic hyperglycinemia
Sulfite oxydase deficiency - XO
Urea Cycle
Disorders
Respiratory
chain
Fatty acid oxydation
Variant hyperinsulinism
(glutamate dehydrogenase)
Fatty acid oxydation
Glycogen storage disease
Glyconeogenesis defects
Mitochondrial
defect
no
no
no no
no
no no
no
yes
yes
yes
yes
yes
yes
yes yes
-
7/29/2019 239_metabolik hastalklar (1)
10/17
Specific investigations(with the aid of a metabolic
specialist)
From initial samples: Blood: Amino acids, Acyl carnitine
profile
Urine: Organic acids, Oroticuria
Main diagnostic pathways: Urea Cycle Disorders: Plasma amino
acids, oroticuria; then specific enzymatic activity
Organic aciduria: Urinary organic acids; then specific enzymatic
activity
Fatty acid oxidation: blood carnitine and acylcarnitine profile,
urinary organic acids then
specific enzyme activity
Respiratory chain disorders: very high lactatemia then specific
enzyme activity, very poor
prognosis eventually post mortem samples (see below)
Postmortem cases:In the absence of a specific orientation
towards a diagnostic pathway the following
samples need to be taken (in addition to blood and urine) :
skin biopsy (in saline solution at RT)
muscle and liver biopsy (freeze immediately at 80C)
-
7/29/2019 239_metabolik hastalklar (1)
11/17
Case examples ( 1 )
Case 1
Child born at 37 weeks of gestation, birthweight 2450 g,
consanguineous parents
Day 1: episode of cyanosis while breast feeding
Day 2: poor feeding
Day 3: oliguria, trembling, slight hypotonia
Day 4: generalized seizure, progressing lethargy and hypotonia,
abnormal movements of the
lower limbs
Day 5: coma
Blood ammonia: 500 mol/l
Emergency measures: peritoneal dialysis, sodium benzoate,
arginine hydrochloride, high caloric nasogastric feeding without
protein
-
7/29/2019 239_metabolik hastalklar (1)
12/17
Case examples ( 2 )
Case 1 (cont.)
Further investigations: low citrulline, ornithine, arginine and
isoleucine, normal organic acids
Carbamylglutamate given at day 25 because of recurrent
ammonaemia (CPS or NAGS deficiency?)
Enzyme test for enzyme activity showed decreased NAGS
Function
Diagnosis: NAGS deficiency
Treatment: Carbaglu (ongoing)
(Guffon et al 1995)
Comment: in this case screening for metabolic diseases
especially hyperammonemia would
have been indicated at day 2, parallel to septic screening.
-
7/29/2019 239_metabolik hastalklar (1)
13/17
Case examples ( 3 )
Case 2
Child born at 39 weeks of gestation, birth weight 3250g, no
consanguinity
1st hospitalisation at day 3: admission with poor feeding,
weight loss (16%), intravenousrehydratation then discharged after
24 h
At home: poor feeding, no weight gain, attempts of feeding with
different milk formulas
2nd hospitalisation at day 17: poor feeding, no weight gain
since birth, diagnosis
of low urinary infection (104 E Coli) : Antibiotics, no
screening for ketonuria
At home: persistent poor feeding and no weight gain, patient
sleeps a lot
3rd hospitalisation at 1.5 months: poor feeding, weight 3 600 g,
vomiting, infectious screeningnegative, normal abdominal X ray and
ultrasound, improvement with glucose infusion.
After reintroduction of milk: vomiting, drowsiness, moaning,
altered general condition, transferedwith the diagnosis of
intestinal occlusion.
-
7/29/2019 239_metabolik hastalklar (1)
14/17
Case examples ( 4 )
Case 2 (cont.)
At arrival: hypothermia (36C), bad general condition,
drowsiness,a reactivity, no eye contact,huge axial and peripheral
hypotonia, polypnea, normal visceral exam
Metabolic acidosis (HCO3-: 13 mmol/l), ketonuria ++,
hyperammonaemia 349 mol/l,
leuconeutropaenia
suspicion of organic aciduria
emergency care: continuous free protein, high caloric
nasogastric feeding
IV carnitine 350 mg x 4/day
IV vitamine B12 : 1 mg/day
IV biotine 10 mg/day
IV insulin
Diagnosis: methylmalonic aciduria (mut-)
(plasma methyl malonic acid (MMA) 846 mol/l, urinary MMA 38 245
mol/l)
Good outcome
-
7/29/2019 239_metabolik hastalklar (1)
15/17
Blau N et al (2003) Simple test in urine and blood. In:
Physicians guide to the laboratory diagnosis of metabolic diseases.
Blau N, Duran M,Blaskovics ME, Gibson KM Editors. Springer Verlag,
Berlin Heidelberg, 3-10.
Guffon N. et al (1995): A new neonatal case of N-acetylglutamate
synthase deficiency treated by carbamylglutamate. J Inherit Metab
Dis 18(1): 61-5.
Gouyon JB et al (1994): Removal of branched-chain amino acids by
peritoneal dialysis, continuous arterivenous hemofiltration, and
continuous
arterivenous hemodialysis in rabbits: implications for maple
syrup urine disease treatment; Ped Res 35: 357-61.
Leonard JV (1985): The early detection and management of inborn
errors presenting acutely in the neonatal period. Eur J Pedia tr
143: 253-7.
Ogier de Baulny H (2002): Management and emergency treatments of
neonates with a suspicion of inborn errors of metabolism. Semin
Neonatol 7:
17-26.
Saudubray JM et al (1995): Clinical approach to inherited
metabolic diseases. In: Inborn metabolic diseases. Fernandez J,
Saudubray JM, van den
Berghe G Editors. Springer Verlag, Berlin Heidelberg, 3-39.
Saudubray JM et al (2002): Clinical approach to inherited
metabolic disorders in neonates : an overview. Semin Neonatol 7:
3-15.
References and further reading
-
7/29/2019 239_metabolik hastalklar (1)
16/17
Other documents on this topic are avai lable from Orphan Europe
Headquarter at:
FRANCE
ORPHAN EUROPESARL
Immeuble Le Wilson
70, avenue du Gnral de Gaulle
92058 PARIS LA DEFENSE
FRANCE
Tel.: +33 (0)1 47 73 64 58
Fax: +33 (0)1 49 06 00 04
e.mail: [email protected]
www.orphan-europe.com
Or one of its local affiliates:
UNITED KINGDOM ITALY
ORPHAN EUROPE (UK) Ltd. ORPHAN EUROPE (Italy) Srl.
Isis House, 43 Station Road Via Cellini, 11
Henley-on-Thames 20090 SEGRATE (MILANO)
OXFORDSHIRE RG9 1AT ITALY
UNITED KINGDOM Tel.:+ 39 02 26 95 01 39
Tel.: +44 (0) 1491 414 333 Fax: + 39 02 26 95 36 74Fax: +44 (0)
1491 414 443 e.mail: [email protected]
e.mail: [email protected] www.orphan-europe.com
www.orphan-europe.com
-
7/29/2019 239_metabolik hastalklar (1)
17/17
SPAIN PORTUGAL GERMANY
ORPHAN EUROPE S.L. ORPHAN EUROPE (Germany) Gmbh
Gran Via de les Corts Catalanes, 649 Max-Planck-Strasse 6
Despacho n1 63128 DIETZENBACH
08010 BARCELONA GERMANYSPAIN Tel.: + 49 (0) 60 74 81 21 60
Tel.: + 34 93 342 51 20 Fax : + 49 (0) 60 74 81 21 66
Fax: + 34 93 270 10 50 e.mail: [email protected]
e.mail: [email protected] www.orphan-europe.com
www.orphan-europe.com
POLAND NORDIC COUNTRIES
ORPHAN EUROPE (Germany) Gmbh ORPHAN EUROPE AB
Przedstawicielstwo w Polsce Banrgatan 37Ul. Czeresniowa 98 S 115
22 STOCKHOLM
02 456 WARZAWA SWEDEN
POLAND Tel.: + 46 8 545 80 230
Tel.: + 48 22 863 86 01 Fax: + 46 8 660 5078
Fax: + 48 22 863 58 96 e.mail: [email protected]
e.mail: [email protected] www.orphan-europe.com
www.orphan-europe.com
BENELUXORPHAN EUROPE
King Albert I Avenue 48 bus 3
1740 WEMMEL
BELGIUM
www.orphan-europe.com