Embed Size (px)
Citation preview

CASE REPORT
Acute portal vein thrombosis due to chronic relapsingpancreatitis: a fistula between a pancreatic pseudocystand the splenic vein
Masahiro Kikuchi • Yasuhiro Nishizaki • Kota Tsuruya •
Ikuko Hamada • Toru Higashi • Keiko Sakuma • Hirokazu Shiozawa •
Jun Aoki • Rena Nagashima • Jun Koizumi • Yoshitaka Arase •
Koichi Shiraishi • Masashi Matsushima • Tetsuya Mine
Received: 19 March 2013 / Accepted: 4 November 2013 / Published online: 12 December 2013
� Springer Japan 2013
Abstract Portal vein thrombosis (PVT) is a relatively
common complication in patients with liver cirrhosis, but
several other causes might play an important role in PVT
pathogenesis. We present a case of alcoholic chronic
pancreatitis complicated by acute extensive PVT. The
patient was managed conservatively with danaparoid
sodium at first, but the thrombosis gradually extended. We
then tried radiological intervention using the direct tran-
shepatic and transjugular intrahepatic postsystemic shunt
approaches. Although we were able to successfully cathe-
terize the percutaneous transhepatic portal vein (PTP), we
could not achieve recanalization of the portal vein.
Therefore, PTP catheterization and systemic intravenous
infusion of urokinase and heparin was performed to prevent
further progression of the thrombosis and cavernous
transformation was finally achieved. Computed tomogra-
phy (CT) and magnetic resonance cholangiopancreatogra-
phy revealed a pancreatic stone which had possibly
induced dilatation of the tail duct and formation of a
pancreatic pseudocyst and caused intractable pancreatitis.
We performed endoscopic retrograde cholangiopancrea-
tography and placed a stent in the pancreatic duct, which
completely cured the pancreatitis. Retrospectively, the
previous CT with curved multi-planar reconstruction was
reviewed and a fistula was detected between the pancreatic
pseudocyst and splenic vein. We concluded that the etiol-
ogy of the PVT was not only inflammatory extension from
pancreatitis but also a fistula between the pancreatic duct
and the splenic vein.
Keywords Portal vein thrombosis � Splenic vein
thrombosis � Pancreatic stent
Introduction
For activated portal vein thrombosis (PVT) an adequate
choice of treatment is required. There are two main
approaches to reduce PVT-associated morbidity and mor-
tality—(1) to reverse or prevent the progression of
thrombosis within the portal venous system, and (2) to treat
the complications of established PVT, specifically gastro-
intestinal varices or biliary complications. Recent studies
demonstrate the efficacy of thrombolytic therapy in acute
thrombosis, and the apparent safety and benefit of antico-
agulation in patients with chronic PVT.
Pancreatitis has been identified as the cause of PVT, and
the incidence of splenic vein thrombosis in patients with
chronic pancreatitis is 20-40 % [1–3]. In chronic pan-
creatitis, splenic vein thrombosis is considered to be
M. Kikuchi � K. Tsuruya � I. Hamada � T. Higashi �K. Sakuma � H. Shiozawa � J. Aoki � M. Matsushima
Department of Gastroenterology, Tokai University Tokyo
Hospital, Tokyo, Japan
e-mail: [email protected]
Y. Nishizaki (&)
Life Care Center, Tokai University Tokyo Hospital, 1-2-5,
Yoyogi, Shibuya-ku, Tokyo 153-0065, Japan
e-mail: [email protected]
R. Nagashima
Department of Radiology, Tokai University Tokyo Hospital,
Tokyo, Japan
J. Koizumi
Department of Diagnostic Radiology, Tokai University School
of Medicine, Isehara, Kanagawa, Japan
Y. Arase � K. Shiraishi � T. Mine
Department of Gastroenterology, Tokai University School of
Medicine, Isehara, Kanagawa, Japan
123
Clin J Gastroenterol (2014) 7:52–57
DOI 10.1007/s12328-013-0442-6

multifactorial in origin, namely due to local, pro-throm-
botic, inflammatory changes in the vascular endothelium,
extrinsic splenic vein compression by pseudocysts, rela-
tively low perfusion, and later in the course of the disease,
pancreatic fibrosis. This suggests that management of
pancreatitis is also required to prevent the progression of
thrombosis.
Case presentation
A 63-year-old male presented to our outpatient clinic with a
history of alcoholic chronic pancreatitis. He complained of
dull pain in his upper abdomen for 5 days without fever or
other symptoms in the digestive organs. He had been con-
suming alcohol (140 g/day) for the last 40 years (last drink
5 days before admission). Laboratory tests revealed white
blood cells (10,800/ll; normal \8,200), C-reactive protein
(6.1 mg/dl; normal \0.6), D-dimer (1,000–2,000 ng/ml;
normal \200), total bilirubin (0.9 mg/dl; normal \1.2),
aspartate amino transferase (34 IU/l; normal \40), alanine
amino transferase (39 IU/l; normal \35), alkaline phos-
phatase (302 IU/l; normal\338), c-glutamyl transpeptidase
(86 IU/l; normal \79), amylase (404 IU/l; normal \134),
lipase (1,023 U/l; normal\57), and elastase-1 (4,704 ng/dl;
normal\300). The prothrombotic work-up, including anti-
phospholipid antibody, protein C and S, and antithrombin III
was negative. By ultrasonography and CT, the patient was
diagnosed with extensive PVT from the superior mesenteric
vein to the portal and splenic veins caused by chronic active
pancreatitis (Figs. 1, 2). Initially, the patient was managed
conservatively with danaparoid sodium for thrombosis, and
gabexate mesilate and antibiotics for pancreatitis, but his
abdominal pain developed with fever spikes. CT examina-
tion showed the thrombosis had gradually extended and
limited activity of pancreatitis at the head was detected. We
diagnosed thrombophlebitis, not pancreatitis activity,
because the level of pancreatic enzymes was not high. The
clinical course is shown in Fig. 3.
Ten days after admission, we twice attempted radio-
logical intervention using the transjugular intrahepatic
postsystemic shunt (TIPS) approach, but we could not
achieve recanalization of the portal vein. However, we
were able to successfully catheterize the percutaneous
transhepatic portal vein (PTP) (Fig. 4). Therefore, PTP
catheterization and systemic intravenous infusion of anti-
biotics, urokinase and heparin was performed to prevent
further progression of the thrombosis. The range of
thrombosis did not decrease but the patient’s abdominal
pain and high fever gradually disappeared. CT showed
cavernous transformation was finally achieved (Fig. 5).
Although the thrombophlebitis was stable, the patient
noticed low-grade fever and epigastric pain after starting a
diet. CT revealed a pancreatic stone which may have
induced dilatation of the tail duct and formation of a
pancreatic pseudocyst and caused intractable pancreatitis
(Fig. 6a). Therefore, we performed endoscopic retrograde
cholangiopancreatography (ERCP) and placed a stent in
Fig. 1 Ultrasonography shows
a thrombosis at the main branch
of the portal vein (arrow),
b right PVT (arrow), and c left
PVT (arrow)
Clin J Gastroenterol (2014) 7:52–57 53
123

the pancreatic duct after dilation with a balloon, which
completely cured the pancreatitis (Fig. 6b).
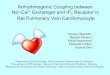
Retrospectively, we reviewed the previous CT (day 1)
image using curved multi-planar reconstruction (MPR).
We detected a fine low-density structure between the
pancreatic pseudocyst and the splenic vein, surrounded by
edematous and necrotic tissue. We diagnosed this as a
fistula which had developed in necrotic tissue bridged over
the pancreatic pseudocyst to the splenic vein. This might
have had an influence on the formation and extension of the
PVT in this patient (Fig. 7).
The patient has been progressing well since discharge
with the pancreatic stent being exchanged every 3 months.
When he underwent ERCP after discharge, we tried to
detect the existence of a fistula but could not find one. At the
same time, we performed upper gastrointestinal endoscopy
every 3 months. We detected a mild esophageal varix [F1,
Li, Cb, Rc(-), Lg(-)], but it has not changed or enlarged.
Fig. 2 Enhanced CT (portal phase) shows a pancreas head swelling
and new appearance of a pancreatic stone at the body (arrow),
b expansion of inflammation from the pancreas head to the portal vein
(arrow), c left PVT (arrow), d right PVT (arrow), and e expansion of
splenic vein thrombosis to the splenic hilum (arrow)
Fig. 3 Clinical time course
54 Clin J Gastroenterol (2014) 7:52–57
123

Discussion
The presentation of PVT has been divided into two cate-
gories—acute PVT or chronic PVT. No definitive time-
frame distinguishes acute from chronic PVT, but studies of
the former have considered patients who developed
symptoms \60 days prior to hospital assessment [4]. The
typical presentation of acute PVT is with abdominal pain,
nausea and fever. In a patient with proven PVT, the
absence of clinical, endoscopic or radiological evidence of
portal hypertension may also suggest that thrombosis is of
recent onset. In the present case, we diagnosed acute PVT
because of the recent development of thrombosis without
the establishment of cavernous transformation.
In a retrospective study of 172 adult patients with
established PVT, the overall 10-year survival rate was
54 %, but this figure increased to 81 % in those without
cirrhosis, cancer or mesenteric vein thrombosis [5]. In non-
cirrhotic and non-neoplastic patients, PVT generally has a
good outcome [6, 7]. In addition, acute PVT, when rec-
ognized and treated before the occurrence of intestinal
infarction, has a good prognosis [8–10].
The treatment of portal vein thrombosis remains some-
what controversial and has ranged from conservative
strategies such as watchful waiting for spontaneous
recanalization, bowel rest and anticoagulation to more
active approaches such as stenting, thrombolytics, and
surgery.
The effectiveness of anticoagulation in patients with
evidence of acute PVT has been reported in a small number
of studies and case reports [9, 11].
In one study, anticoagulation achieved recanalization in
approximately 40 % of patients and recanalization (com-
plete or partial) was observed in [60 % of patients in
whom anticoagulation was initiated within the first week
but in \20 % of patients who started later [12]. Another
study, clearly showed that in acute PVT onset, the sooner
the treatment is given the better the outcome will be; the
rate of recanalization is approximately 69 % if anticoagu-
lation is instituted within the first week after diagnosis,
Fig. 6 CT shows a the pancreatic stone which possibly induced
dilatation of the tail duct and formation of the pancreatic pseudocyst
and caused an intractable pancreatitis, b pseudocyst reduction and
calming of pancreatitis after stenting the pancreatic duct
Fig. 4 Portography with percutaneous transhepatic portal vein cath-
eterization (PTP) shows an obstinate PVT. Infusion of antibiotics and
urokinase with PTP catheterization was performed to prevent further
progression of the thrombosis
Fig. 5 CT shows the constitution of cavernous transformation and
mass reduction of the PVT
Clin J Gastroenterol (2014) 7:52–57 55
123
while it falls to 25 % when instituted in the second week
[4, 12, 13]. Thus, early anticoagulation is recommended for
the prevention of thrombosis extension.
In the present case, we started administering danaparoid
sodium instead of heparin as soon as possible. Danaparoid
sodium is a drug for deep venous thrombosis and pul-
monary embolism in Western countries and does not need
monitoring unlike heparin and warfarin. The drug is
expected to be useful for treating PVT because it is
effective for the treatment of thrombosis and has a low risk
of bleeding tendency [14]. In the present case, unfortu-
nately the thrombosis appeared to gradually extend and the
patient developed abdominal pain with fever spikes.
Thrombolytic therapy, given either into the systemic
venous circulation, the superior artery, or the portal vein
via the transjugular or transhepatic route, is also effective
for achieving recanalization in acute PVT [15–19]. Despite
the high incidence of adverse effects, thrombolysis should
be considered when initial anticoagulation therapy has
failed, even if there is no consistent evidence concerning
the conditions in which anticoagulation therapy is prefer-
able [15]. PTP catheterization might also be effective in
cases with recent thrombosis, but vascular traumas are
frequent and may stimulate rethrombosis [16], so we
decided to attempt thrombolytic therapy via the transju-
gular route after TIPS placement. However, a technical
problem with a sharp angle in the TIPS route prevented us
from placing the TIPS. We achieved alternative thrombo-
lytic therapy with PTP catheterization which enabled us to
inject highly concentrated thrombolytic agents directly into
the portal vein. PTP catheterization and systemic intrave-
nous infusion of antibiotics, urokinase and heparin was
performed to prevent further progression of the thrombosis
and finally the thrombophlebitis was calmed.
The mechanism of pancreatitis associated with thrombus
formation within the splenic vein seems to involve both
extrinsic and intrinsic factors. This means that a direct
mass affects the venous wall or there is cellular infiltration
into the venous wall and that there is an inflammatory
process involving the vein. The anatomic location of the
splenic vein might greatly contribute to these mechanisms
[20].
In addition, fibrotic extension involving the splenic vein
is important in this phenomenon. Long-standing compres-
sion of the wall of the splenic vein by fibrosis induces a
mild mechanical trauma [21] of the vein, which might
injure the endothelial cells and finally lead to venous
involvement, such as phlebosclerosis and thrombus for-
mation [22]. In the present case, long-standing inflamma-
tion of pancreatic parenchyma due to chronic alcoholic
pancreatitis which led to formation of a pseudocyst was
related to the formation of PVT. Moreover, an abnormal
communication between the pseudocyst and the splenic
vein was detected.
Development of a fistula between a pseudocyst and
portal or splenic vein has been only rarely reported [23–
25]. Pseudocyst rupture into surrounding structures is a
result of pancreatic enzymes, without the inhibitory cas-
cades of the normally functioning pancreas, and inflam-
matory cells within the pseudocyst weakening the
surrounding tissues and vessel walls [26]. Sometimes such
a rupture is responsible for disseminated subcutaneous fat
necrosis and recurrent bacteremia, and surgical treatment is
needed. Most patients with a pancreaticoportal fistula have
Fig. 7 CT (day 1) with curved
MPR shows that a fistula existed
between the pancreatic
pseudocyst and splenic vein
(white large arrow)
56 Clin J Gastroenterol (2014) 7:52–57
123

thrombosis of the portal venous system which suggests that
pancreatic enzymes and inflammatory cells within the
pseudocyst directly worsen endothelial inflammation of the
vein.
In the present case, the patient had a high fever and
remarkably elevated inflammatory observation (CRP was
nearly 30 mg/dl) on days 7-10, and a blood culture test
revealed bacteremia (Corynebacterium). Considered ret-
rospectively, direct infusion of antibiotics through the PTP
route might have contributed to the treatment of bacteremia
which was thought to have been caused by a fistula.
Finally, treatment for the pancreatic stone which had
induced intractable pancreatitis and formation of the
pseudocyst led to the remission of pancreatitis.
We consider that the optimum therapy would have been
to eliminate the pancreatic stone by extracorporeal shock
wave lithotripsy or basket catheterization with ERCP, but
these methods have a high risk under anticoagulation
therapy, so we chose stenting for the pancreatic duct and
then exchanged the stent every 3 months with gradual
dilatation.
Acknowledgment Authors express deep appreciation to Professor T
Tajiri (Department of pathology, Tokai University Hachioji hospital)
for his valuable comments and advices in discussion part of this
paper.
Disclosures Conflict of Interest: M Kikuchi, Y Nishizaki, K
Tsuruya, I Hamada, T Higashi, K Sakuma, H Shiozawa, J Aoki, R
Nagashima, J Koizumi, Y Arase, K Shiraishi, M Matsushima and T
Mine declare that they have no conflict of interest.Human/AnimalRights: All procedures followed were in accordance with the ethical
standards of the responsible committee on human experimentation
(institutional and national) and with the Helsinki Declaration of 1975,
as revised in 2008(5).Informed Consent: Informed consent was
obtained from all patients for being included in the study.
References
1. Weber SM, Rikkers LF. Splenic vein thrombosis and gastroin-
testinal bleeding in chronic pancreatitis. World J Surg.
2003;27:1271–4.
2. Heider RT, Azeem S, Galanko JA, et al. The natural history of
pancreatitis-induced splenic vein thrombosis. Ann Surg.
2004;239:876–80.
3. Sakorafos GH, Sarr MG, Farley DR, et al. The significance of
sinistral portal hypertension complicating chronic pancreatitis.
Am J Surg. 2000;179:129–33.
4. Malkowski P, Pawlak J, Michalowicz B, et al. Thrombolytic
treatment of portal thrombosis. Hepatogastroenterology. 2003;
50:2098–100.
5. Janssen HL, Wijnhoud A, Haagsma EB, et al. Extrahepatic portal
vein thrombosis: etiology and determinants of survival. Gut.
2001;49:720–4.
6. Plessier A, Murad SD, Hernandez-Guerra M, et al. A prospective
multicentric follow-up study on 105 patients with acute portal
vein thrombosis (PVT): results from the European network for
vascular disorders of the liver. Hepatology. 2007;46:310a-a.
7. Amitrano L, Guardascione MA, Scaglione M, et al. Prognostic
factors in non-cirrhotic patients with splanchnic vein thromboses.
Am J Gastroenterol. 2007;102:2464–70.
8. Kumar S, Sarr MG, Kamath PS, et al. Mesenteric venous
thrombosis. N Engl J Med. 2001;345(23):1683–8.
9. Sheen CL, Lamparelli H, Milne A, et al. Clinical features,
diagnosis and outcome of acute portal vein thrombosis. QJM.
2000;93(8):531–4.
10. Lagasse JP, Bahallah ML, Salem N, et al. Acute thrombosis of the
portal system. Treatment with alteplase and heparin or with heparin
alone in 10 patients. Gastroenterol Clin Biol. 1997;21:919–23.
11. Baril N, Wren S, Radin R, et al. The role of anticoagulation in
pylephlebitis. Am J Surg. 1996;172:449–52.
12. Turnes J, Garcıa-Pagan JC, Gonzalez M, et al. Portal hyperten-
sion-related complications. After acute portal vein thrombosis:
impact of early anticoagulation. Clin Gastroenterol Hepatol.
2008;6(12):1412–7.
13. Hoekstra J, Janssen HL, et al. Vascular liver disorders (II): portal
vein thrombosis. Neth J Med. 2009;67(2):46–53.
14. Uchiyama T, Hirokazu T, Hosono K, et al. Portal vein thrombosis
treated using danaparoid sodium and antithrombin III. Hepato-
gastroenterology. 2010;57(97):52–3.
15. Schafer C, Zundler J, Bode JC, et al. Thrombolytic therapy in
patients with portal vein thrombosis: case report and review of
the literature. Eur J Gastroenterol Hepatol. 2000;12:1141–5.
16. Henao EA, Bohannon WT, Silva MB Jr, et al. Treatment of portal
venous thrombosis with selective superior mesenteric artery
infusion of recombinant tissue plasminogen activator. J Vasc
Surg. 2003;38:1411–5.
17. Tateishi A, Mitsui H, Oki T, et al. Extensive mesenteric vein and
portal vein thrombosis successfully treated by thrombolysis and
anticoagulation. J Gastroenterol Hepatol. 2001;16:1429–33.
18. Aytekin C, Boyvat F, Kurt A, et al. Catheter-directed thrombol-
ysis with transjugular access in portal vein thrombosis secondary
to pancreatitis. Eur J Radiol. 2001;39:80–2.
19. Lopera JE, Correa G, Brazzini A, et al. Percutaneous transhepatic
treatment of symptomatic mesenteric venous thrombosis. J Vasc
Surg. 2002;36:1058–61.
20. Moosa AR, Gadd MA. Isolated splenic vein thrombosis. World J
Surg. 1985;9:384–90.
21. Hoff HF. Ultrastructural changes of large rabbit blood vessels
following mild mechanical trauma. Virchows Arch Abt A Pathol
Anat. 1968;345:93–106.
22. Takase M, Suda K, Suzuki F, et al. A histopathologic study of
localized portal hypertension as a consequence of chronic pan-
creatitis. Arch Pathol Lab Med. 1997;121:612–4.
23. Demetrick DJ, Kelly JK. Variceal hemorrhage as a consequence
of spontaneous rupture of a pancreatic pseudocyst into the splenic
vein. Am J Gastroenterol. 1989;84:1103–5.
24. Procacci C, Mansueto GC, Graziani R, et al. Spontaneous rupture
of a pancreatic pseudocyst into the portal vein. Cardiovasc In-
tervent Radiol. 1995;18:399–402.
25. Van Steenbergen W, Ponette E. Pancreaticoportal fistula: a rare
complication of chronic pancreatitis. Gastrointes Radiol.
1990;15:299–300.
26. Willis SM, Brewer TG. Pancreatic duct-portal vein fistula. Gas-
troenterology. 1989;97:1025–7.
Clin J Gastroenterol (2014) 7:52–57 57
123