Embed Size (px)
Citation preview
Aderenza alle Linee Guida internazionali nei pazienti con Sindrome Coronarica Acuta
Antonio Manari
Key points:
• 1‐ Linee Guida STEMI e NSTEMI• 2‐ Razionale delle indicazioni delle Linee Guida• 3‐ Risultati nella pratica clinica (aspetti logistici)
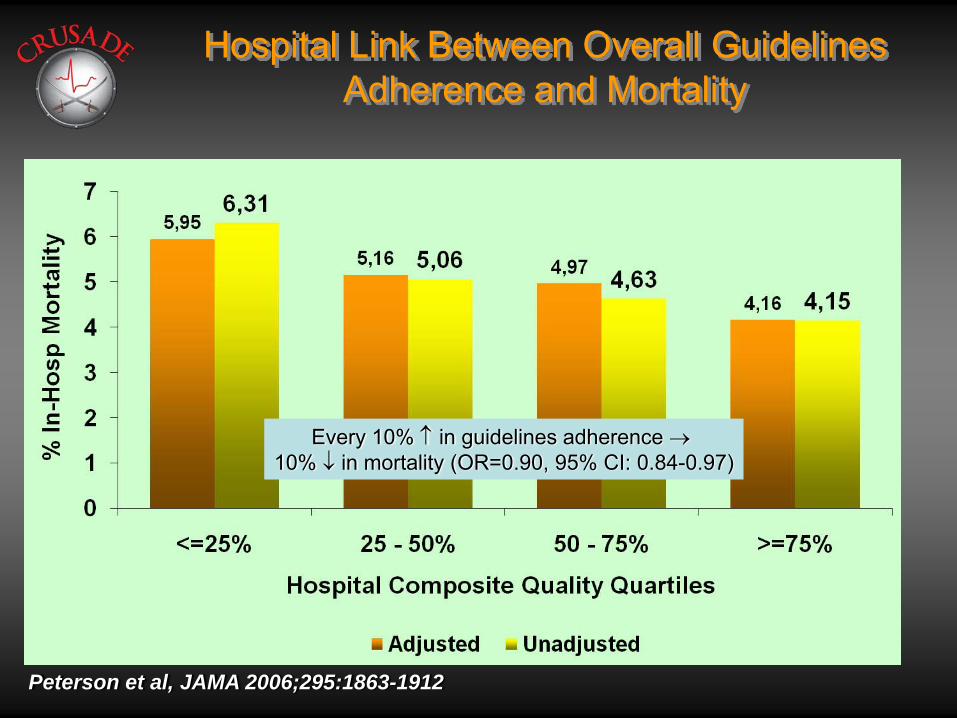
Hospital Link Between Overall Guidelines Adherence and Mortality
Peterson et al, JAMA 2006;295:1863-1912
Every 10% ↑ in guidelines adherence →10% ↓ in mortality (OR=0.90, 95% CI: 0.84-0.97)
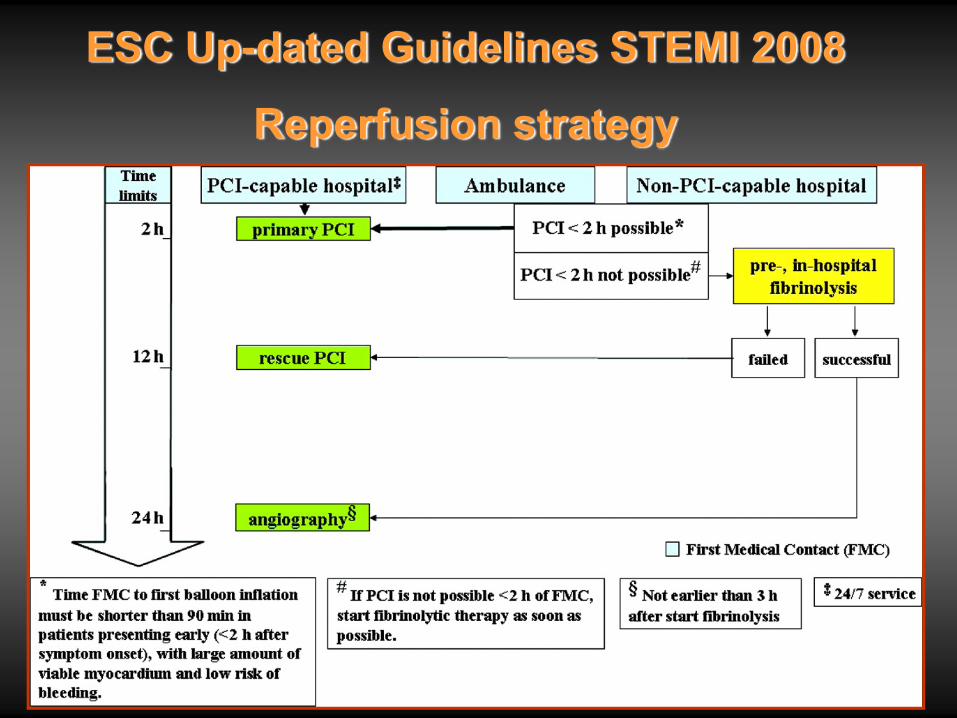
ESC Up-dated Guidelines STEMI 2008
Reperfusion strategy

Recommended Logistics
• Pre-hospital triage/care:● EMS
• unique telephone number• tele-consultationAmbulance• 12-ECG recorder/defibrillator• staff able to provide basic and advanced life support
• Networks:● implementation of a network of hospitals with different levels of
technology connected by an efficient ambulance service using the same protocol
• Targets:● < 10 min ECG recording/ transmission● < 120 min to first balloon inflation
ESC Guidelines STEMI 2008
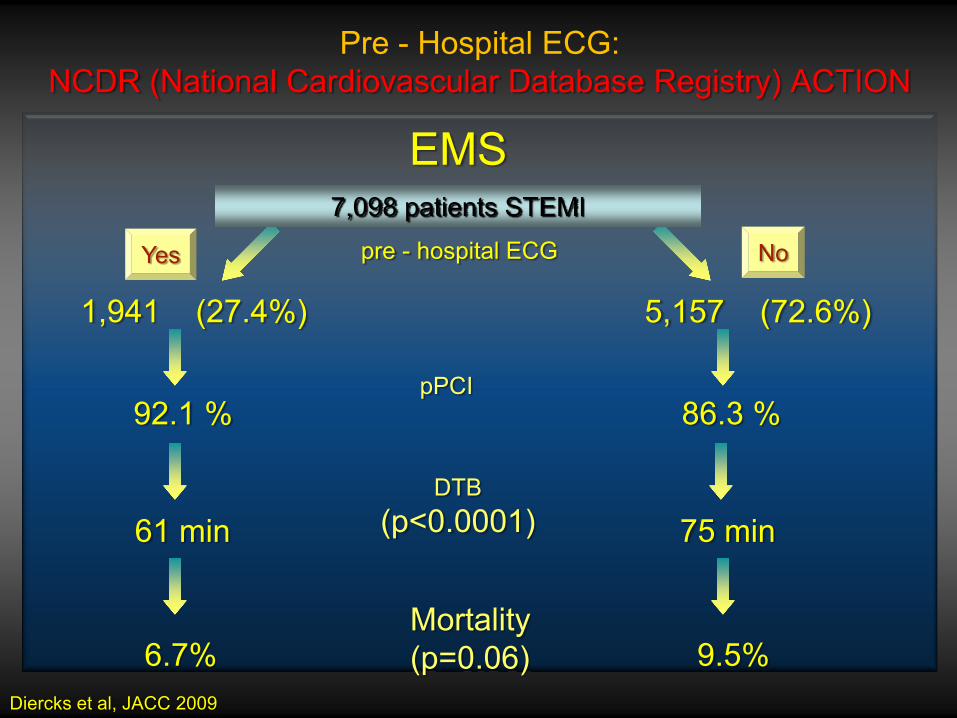
Pre - Hospital ECG: NCDR (National Cardiovascular Database Registry) ACTION
EMS7,098 patients STEMI
pre - hospital ECG
1,941 (27.4%) 5,157 (72.6%)
pPCI92.1 % 86.3 %
DTB(p<0.0001)61 min 75 min
Mortality(p=0.06)6.7% 9.5%
Diercks et al, JACC 2009
Yes No

Bypassing the ER impacts outcomes in STEMI
5,13,8
12
8,37,9 8,4
16,4
13
0
5
10
15
20
All Reperfusion Rx
All Reperfusion Rx
Direct CCU
via ER
5 days 1 year
P=0.03
P=0.04
P=0.02
P=0.006
Steg et al. Heart 2006;92:1378-83
Recommended Logistics
• Pre-hospital triage/care:● EMS
• unique telephone number• tele-consultationAmbulance• 12-ECG recorder/defibrillator• staff able to provide basic and advanced life support
• Networks:● implementation of a network of hospitals with different levels of
technology connected by an efficient ambulance service using the same protocol
• Targets:● < 10 min ECG recording/ transmission● < 120 min to first balloon inflation
ESC Guidelines STEMI 2008
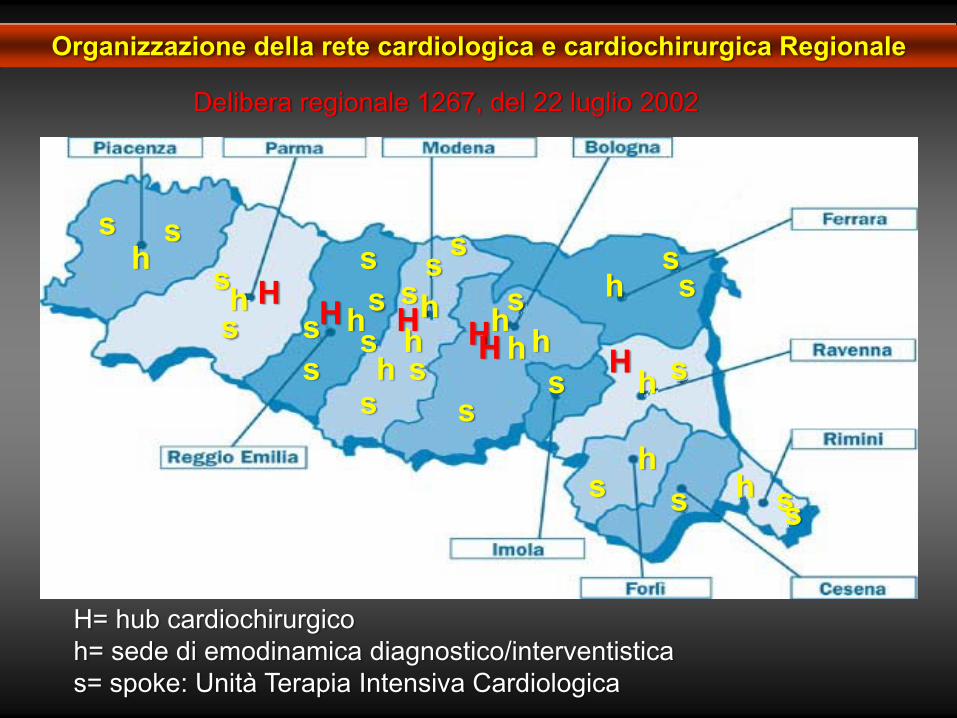
H= hub cardiochirurgico h= sede di emodinamica diagnostico/interventisticas= spoke: Unità Terapia Intensiva Cardiologica
h
hss
Hss H s
ss
s
sh h h
hH HH
s
s
ss
ssh H h
h hs
s
hh
h
s s s
s
s
ss
Organizzazione della rete cardiologica e cardiochirurgica Regionale
Delibera regionale 1267, del 22 luglio 2002

RIDEFINIZIONE DEI PERCORSI DI TEMPESTIVO ACCESSO AI
SERVIZI, DIAGNOSI E CURA PER PAZIENTI CON INFARTO MIOCARDICO ACUTO
Agenzia Sanitaria Regionale Em-Rom.Commissione Cardiologica-Cardiochirurgica
PRIMARER
Documento approvato dalla Commissione il 27 gennaio 2003
Progetto presentato ai Direttori Generali e Sanitari il 18 marzo 2003
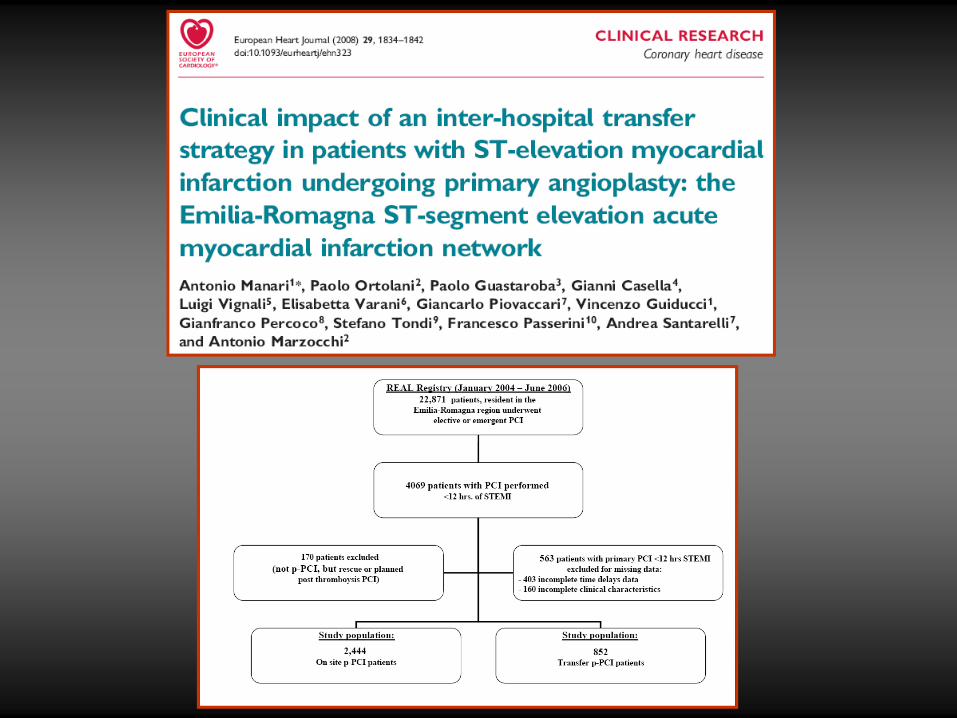
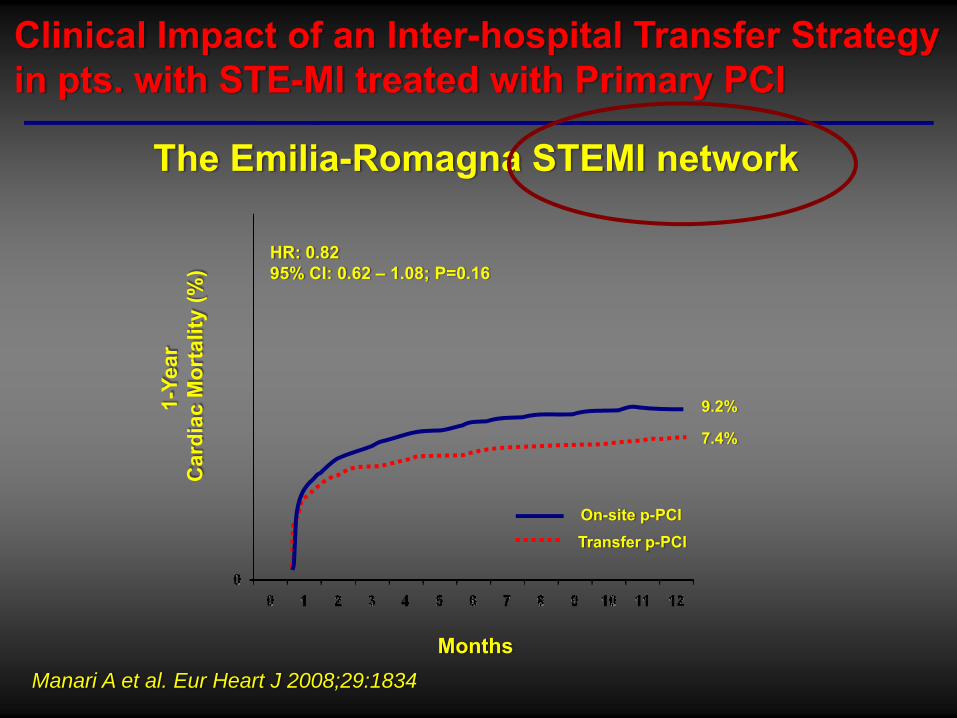
Clinical Impact of an Inter-hospital Transfer Strategy in pts. with STE-MI treated with Primary PCI
The Emilia-Romagna STEMI network
Manari A et al. Eur Heart J 2008;29:1834
On-site p-PCITransfer p-PCI
9.2%
7.4%
HR: 0.8295% CI: 0.62 – 1.08; P=0.16
Months
1-Ye
ar
Car
diac
Mor
talit
y (%
)
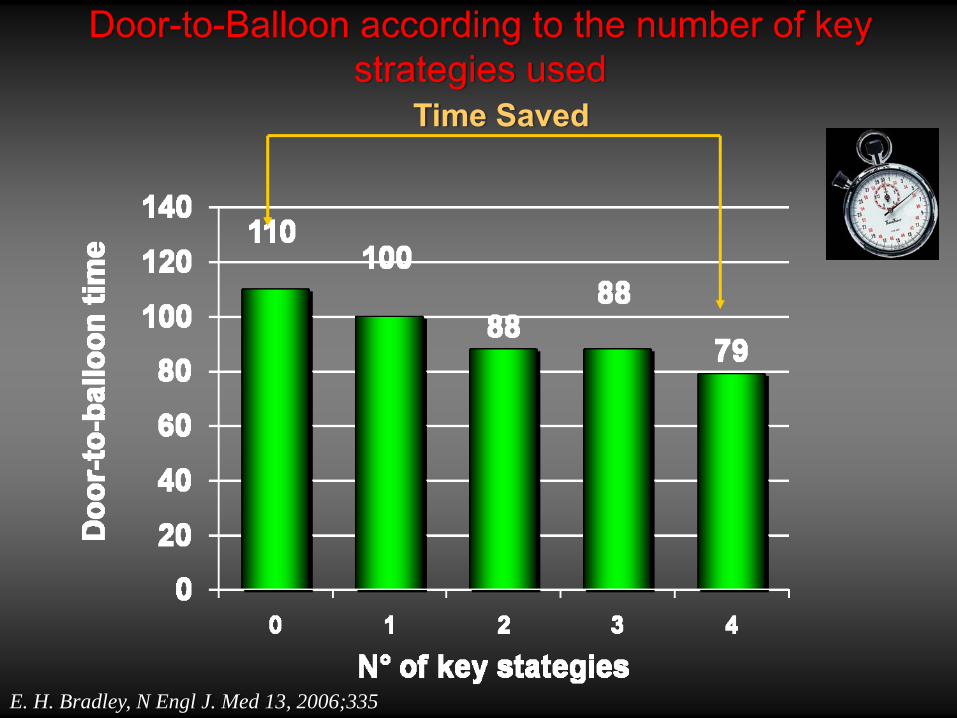
Door-to-Balloon according to the number of key strategies used
Time Saved
E. H. Bradley, N Engl J. Med 13, 2006;335
Recommended Logistics
• Pre-hospital triage/care:● EMS
• unique telephone number• tele-consultationAmbulance• 12-ECG recorder/defibrillator• staff able to provide basic and advanced life support
• Networks:● implementation of a network of hospitals with different levels of
technology connected by an efficient ambulance service using the same protocol
• Targets:● < 10 min ECG recording/ transmission● < 120 min to first balloon inflation
ESC Guidelines STEMI 2008
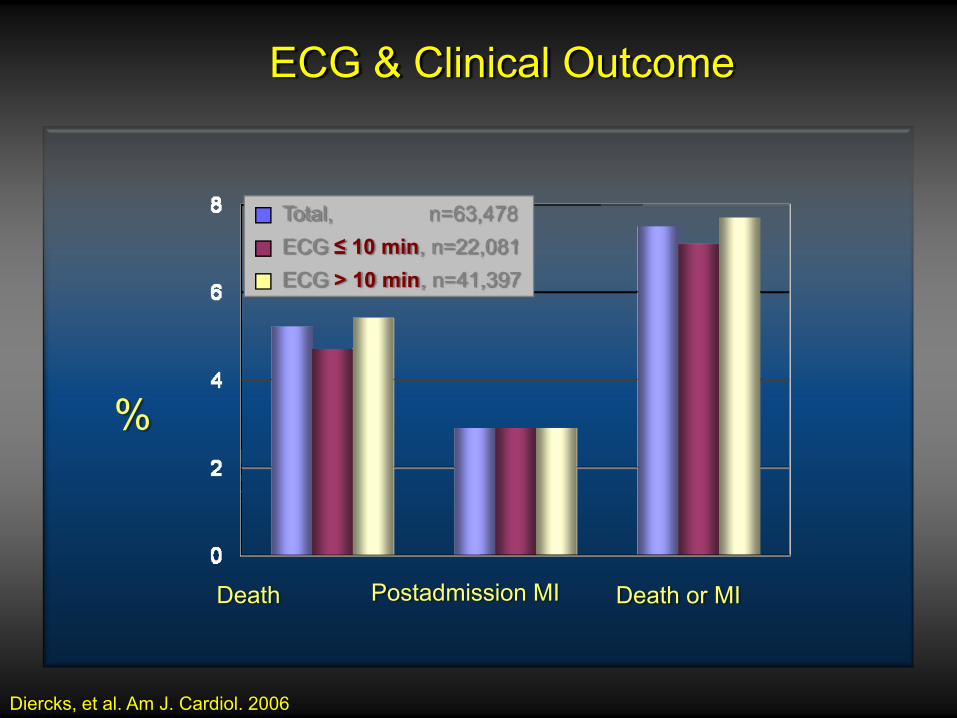
Total, n=63,478ECG ≤ 10 min, n=22,081ECG > 10 min, n=41,397
Death Postadmission MI Death or MI
Diercks, et al. Am J. Cardiol. 2006
%
ECG & Clinical Outcome
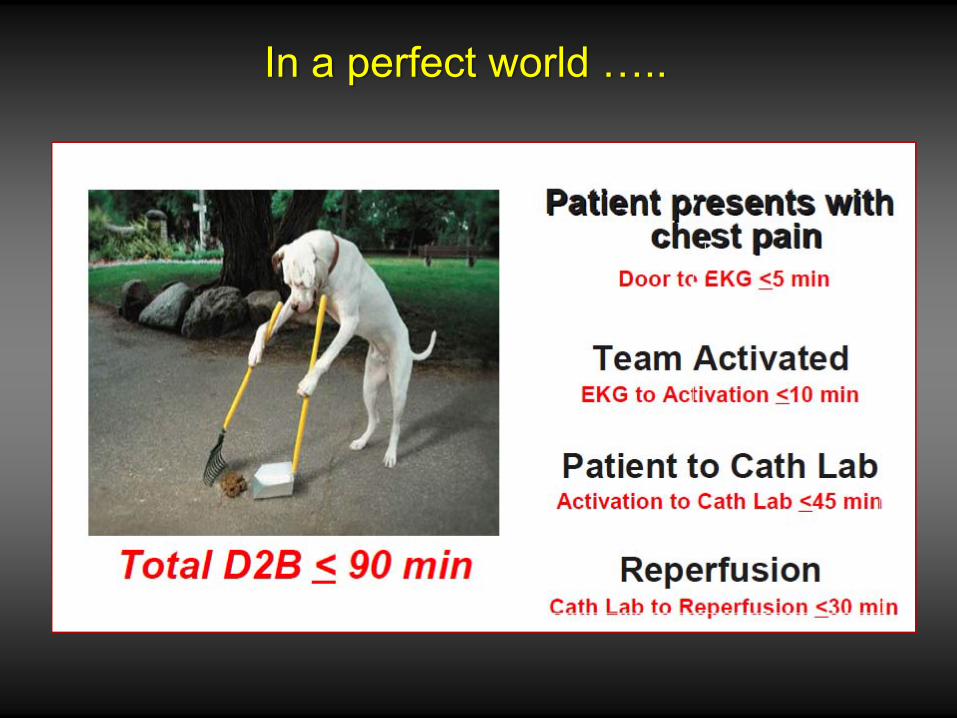
In a perfect world …..
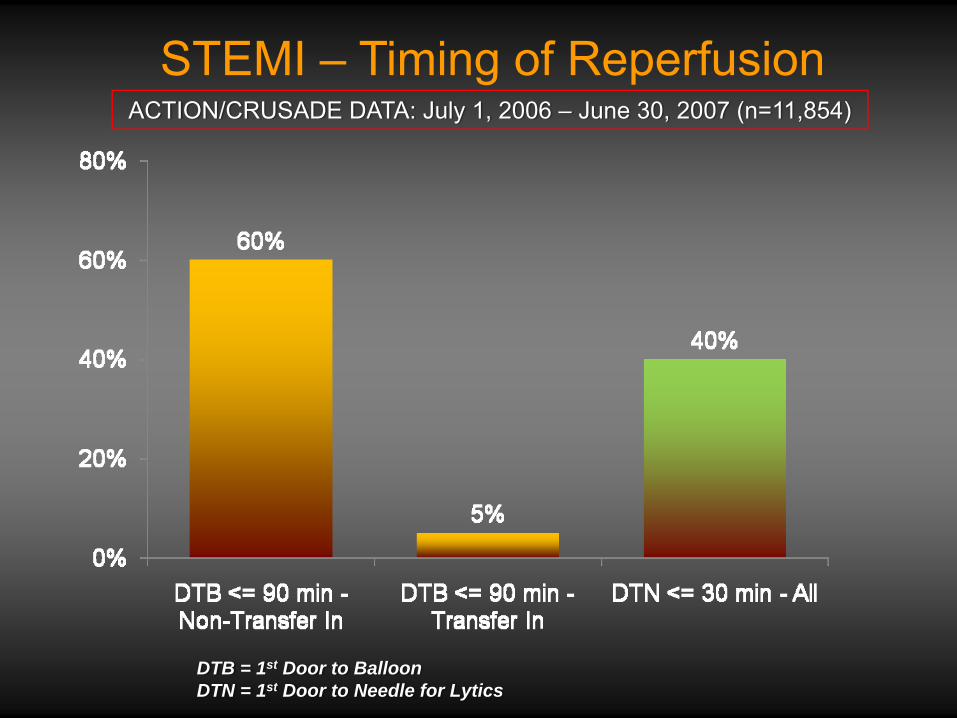
DTB = 1st Door to BalloonDTN = 1st Door to Needle for Lytics
ACTION/CRUSADE DATA: July 1, 2006 – June 30, 2007 (n=11,854)
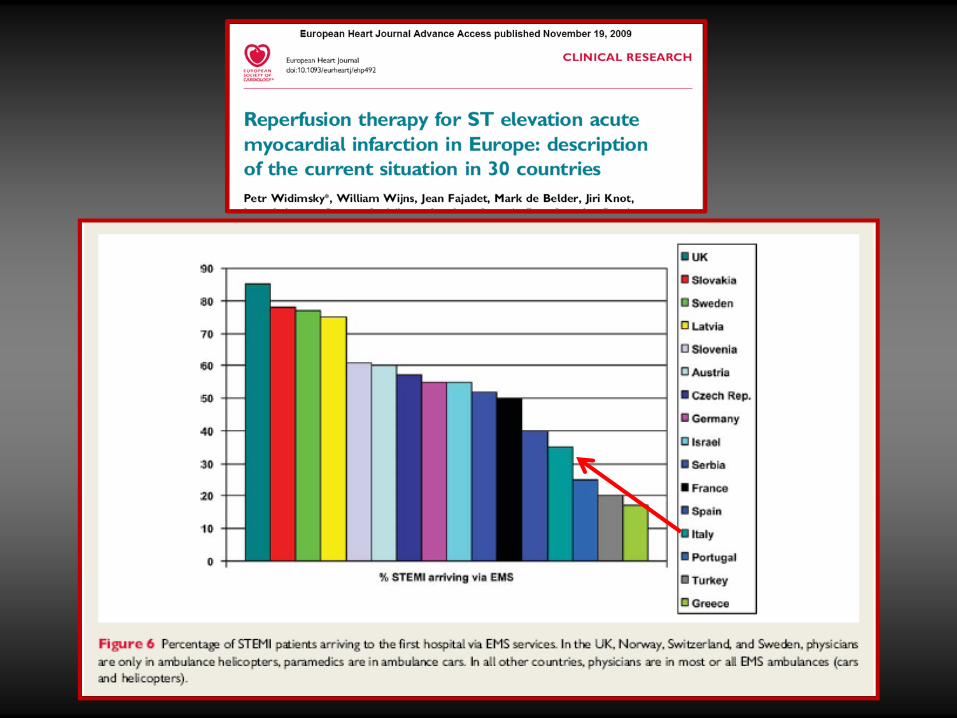
STEMI – Timing of Reperfusion
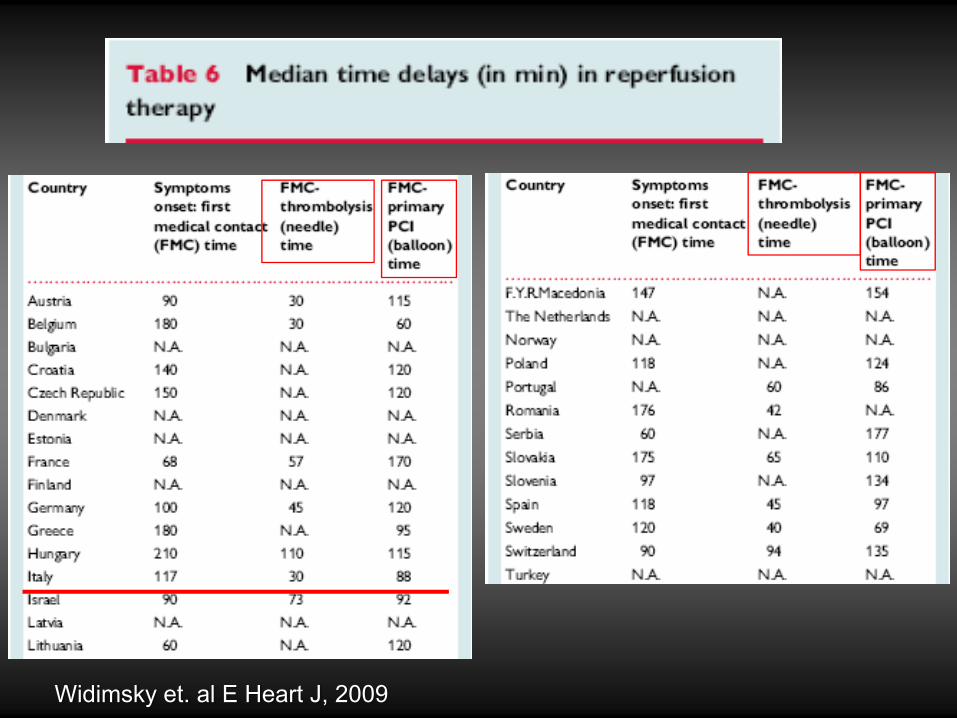
Widimsky et. al E Heart J, 2009
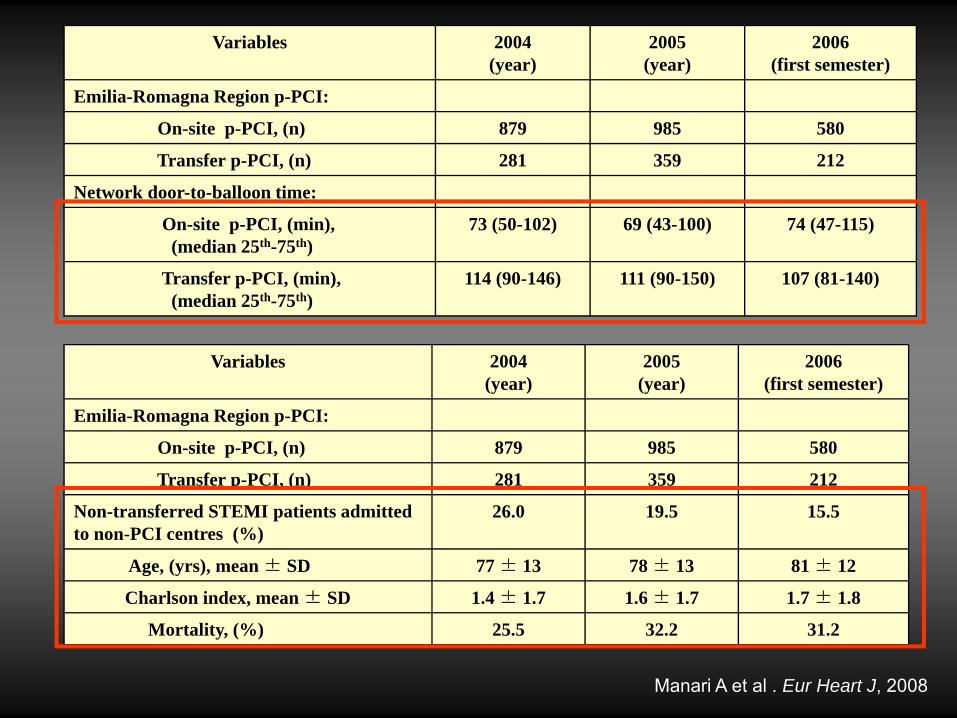
Variables 2004(year)
2005(year)
2006(first semester)
Emilia-Romagna Region p-PCI:
On-site p-PCI, (n) 879 985 580
Transfer p-PCI, (n) 281 359 212
Network door-to-balloon time:
On-site p-PCI, (min), (median 25th-75th)
73 (50-102) 69 (43-100) 74 (47-115)
Transfer p-PCI, (min), (median 25th-75th)
114 (90-146) 111 (90-150) 107 (81-140)
Manari A et al . Eur Heart J, 2008
Variables 2004(year)
2005(year)
2006(first semester)
Emilia-Romagna Region p-PCI:
On-site p-PCI, (n) 879 985 580
Transfer p-PCI, (n) 281 359 212
Non-transferred STEMI patients admitted to non-PCI centres (%)
26.0 19.5 15.5
Age, (yrs), mean ± SD 77 ± 13 78 ± 13 81 ± 12
Charlson index, mean ± SD 1.4 ± 1.7 1.6 ± 1.7 1.7 ± 1.8
Mortality, (%) 25.5 32.2 31.2
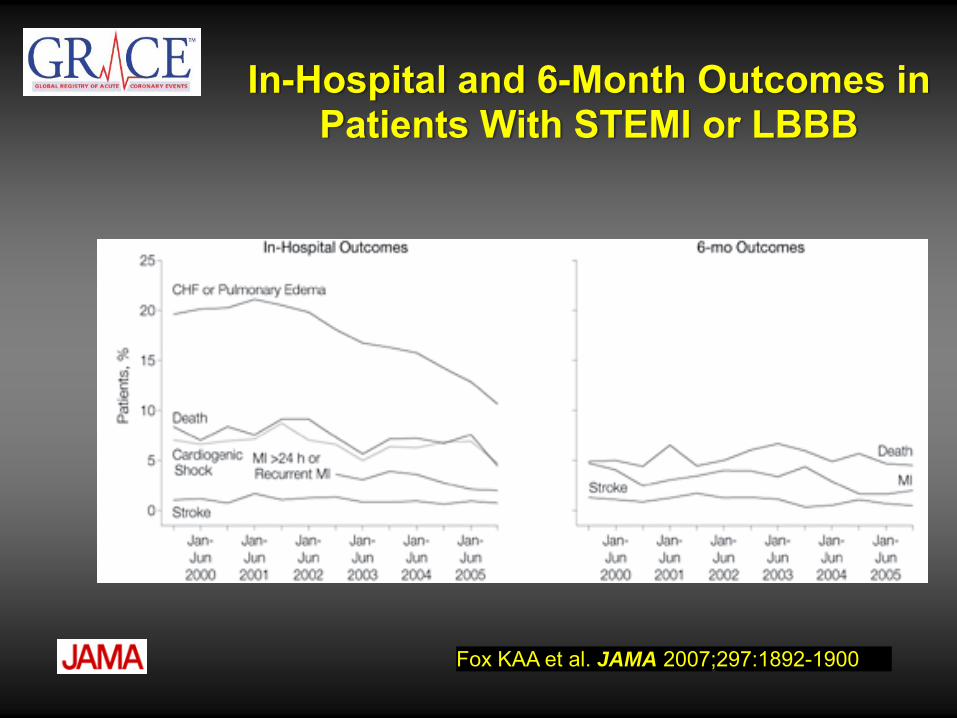
Fox KAA et al. JAMA 2007;297:1892-1900
In-Hospital and 6-Month Outcomes in Patients With STEMI or LBBB
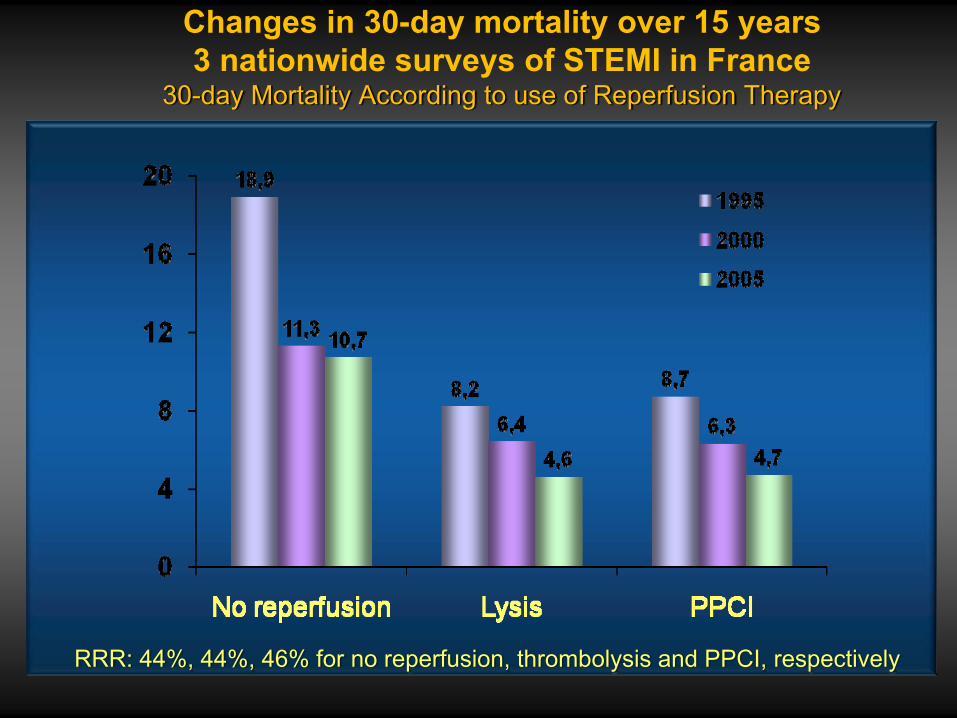
Changes in 30-day mortality over 15 years3 nationwide surveys of STEMI in France
30-day Mortality According to use of Reperfusion Therapy
RRR: 44%, 44%, 46% for no reperfusion, thrombolysis and PPCI, respectively

Registries and RCTs enroll different populations with different outcomes
example of STEMI outcomes in RCT participants, RCT-eligible and RCT-ineligible pts within GRACE
3,63,0
7,1
4,8
11,4
7,7
0
4
8
12
In-hospital mortality Post-discharge mortality
Mor
talit
y ra
te (%
)
RCT participants: 11.3%
RCT-eligible patients: 55.1%
RCT-ineligible patients: 33.6%
Steg et al. Arch Int Med 2007;167:68-73
P=0.001
P=0.001
N=8469
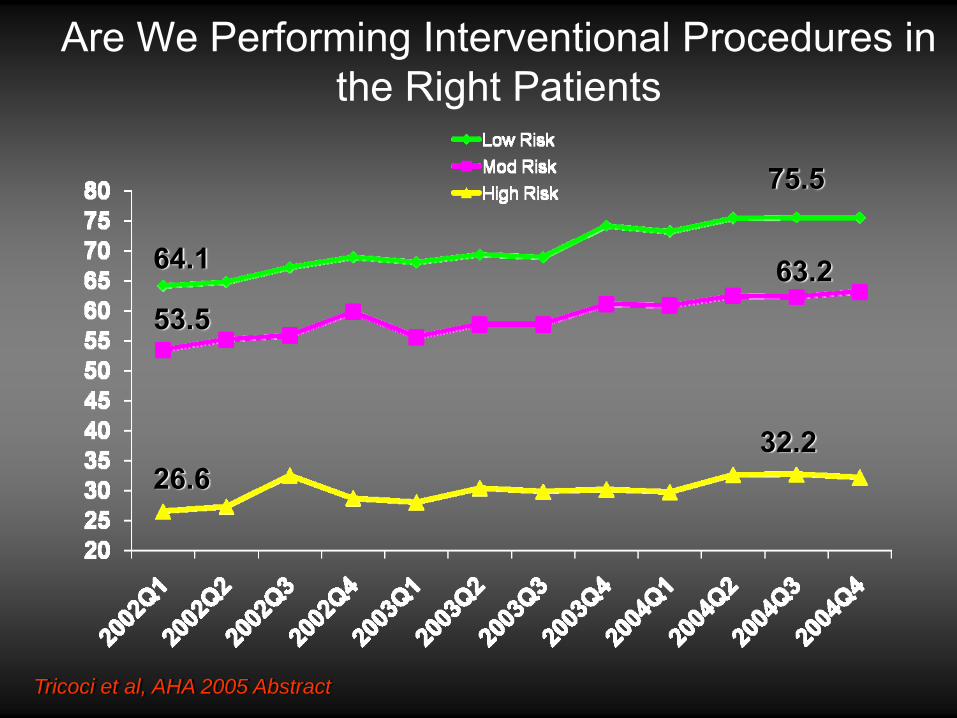
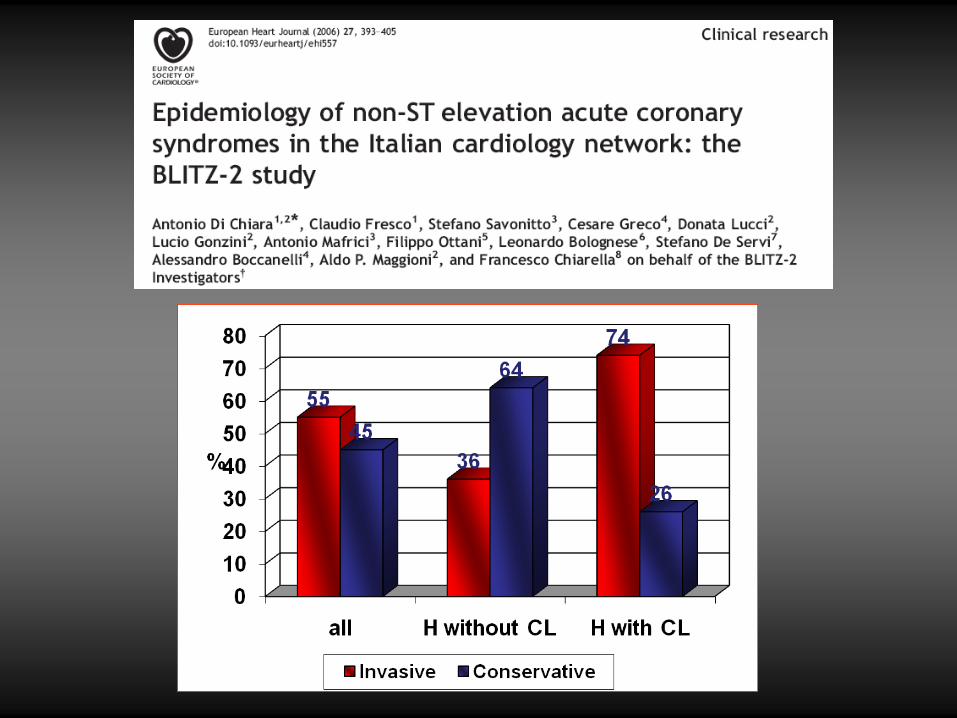
Are We Performing Interventional Procedures in the Right Patients
26.632.2
53.563.264.1
75.5
Tricoci et al, AHA 2005 Abstract

“…Establishing networks of reperfusion at regional and national level…is a key issue.”
NSTEMI Inter-hospital networks?
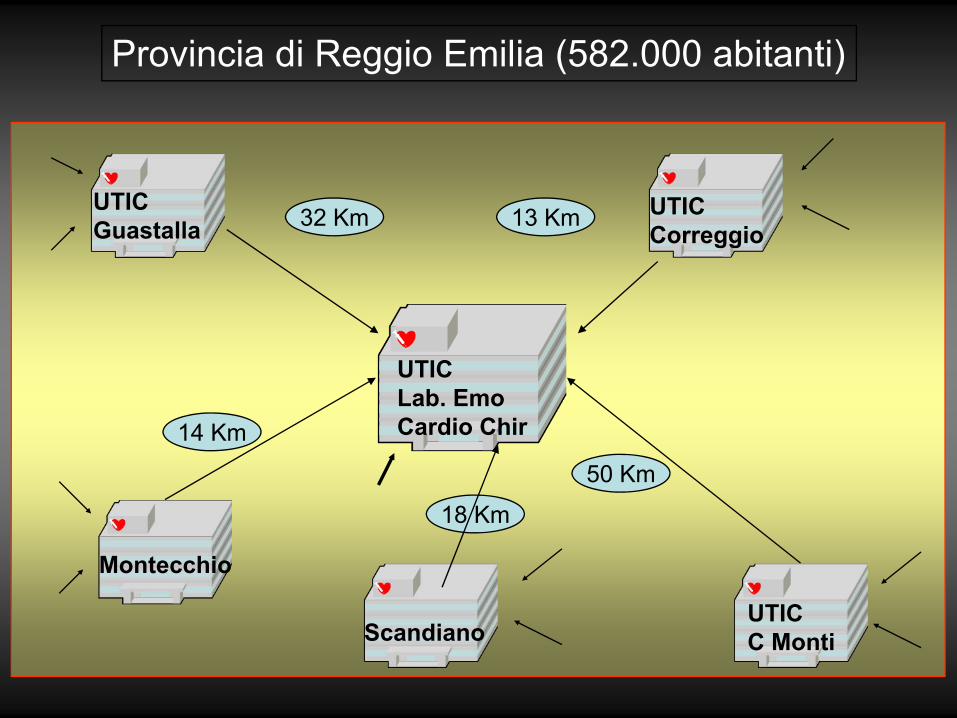
UTICCorreggio
UTICC Monti
Montecchio
14 Km
50 Km
13 Km32 Km
UTICLab. Emo Cardio Chir
18 Km
UTICGuastalla
Scandiano
Provincia di Reggio Emilia (582.000 abitanti)
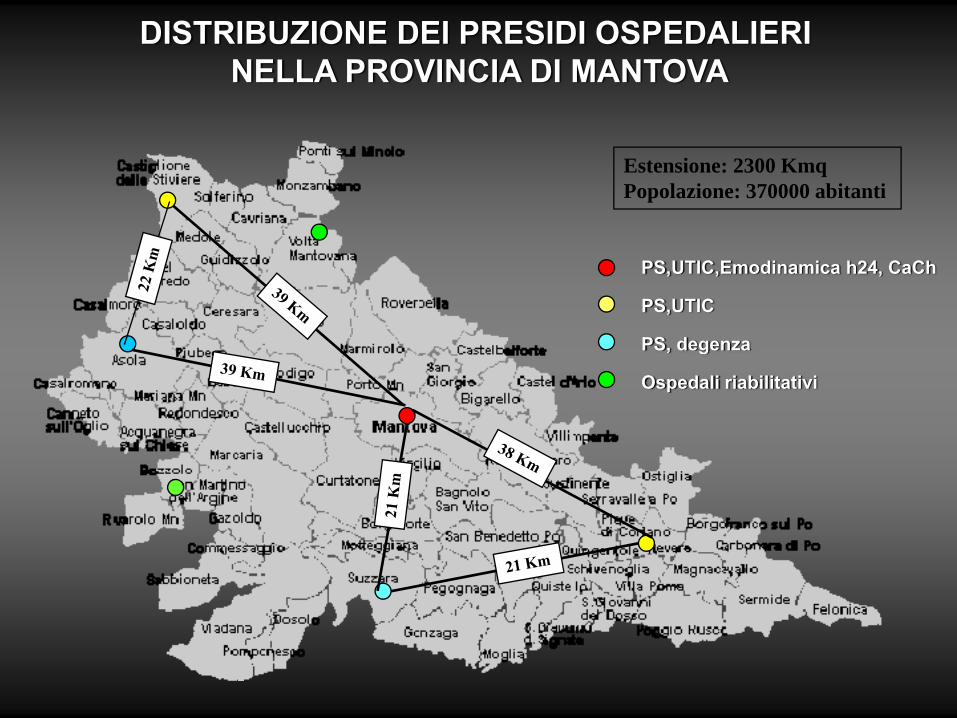
DISTRIBUZIONE DEI PRESIDI OSPEDALIERINELLA PROVINCIA DI MANTOVA
PS,UTIC,Emodinamica h24, CaCh
PS,UTIC
PS, degenza
Ospedali riabilitativi
Estensione: 2300 KmqPopolazione: 370000 abitanti
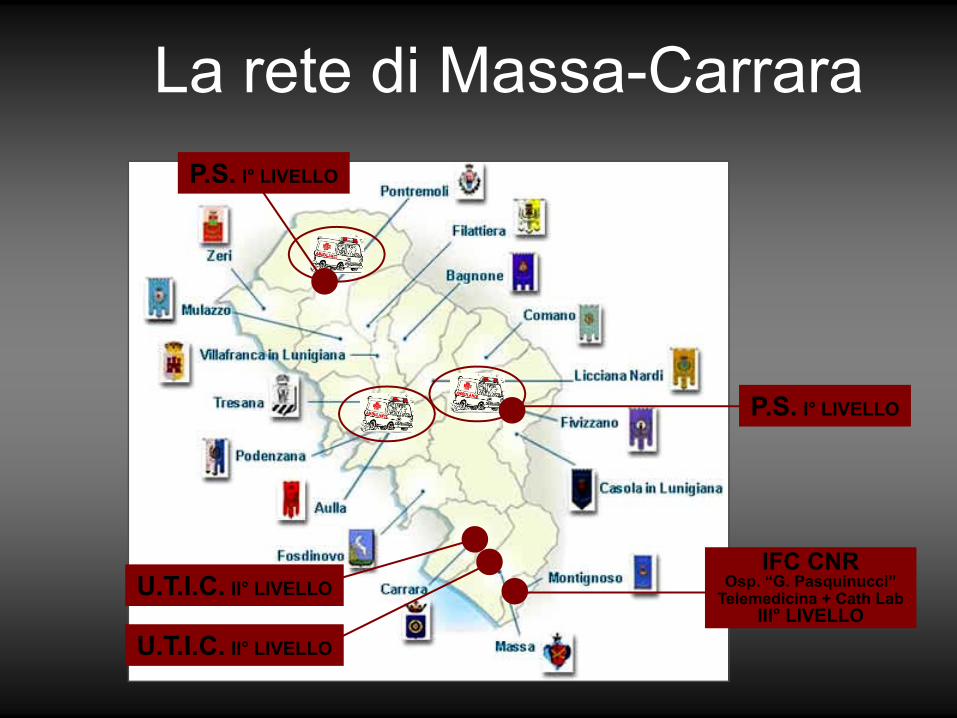
La rete di Massa-CarraraP.S. I° LIVELLO
P.S. I° LIVELLO
U.T.I.C. II° LIVELLO
U.T.I.C. II° LIVELLO
IFC CNROsp. “G. Pasquinucci”
Telemedicina + Cath LabIII° LIVELLO

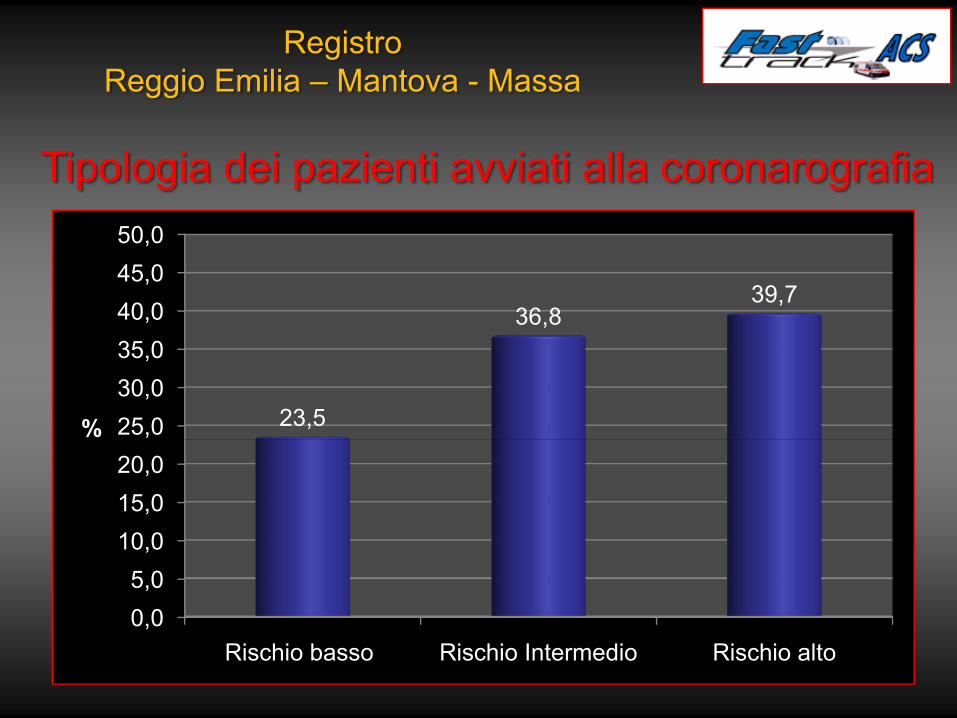
0,05,0
10,015,020,025,030,035,040,045,050,0
Rischio basso Rischio Intermedio Rischio alto
23,5
36,839,7
%
RegistroReggio Emilia – Mantova - Massa
Tipologia dei pazienti avviati alla coronarografia
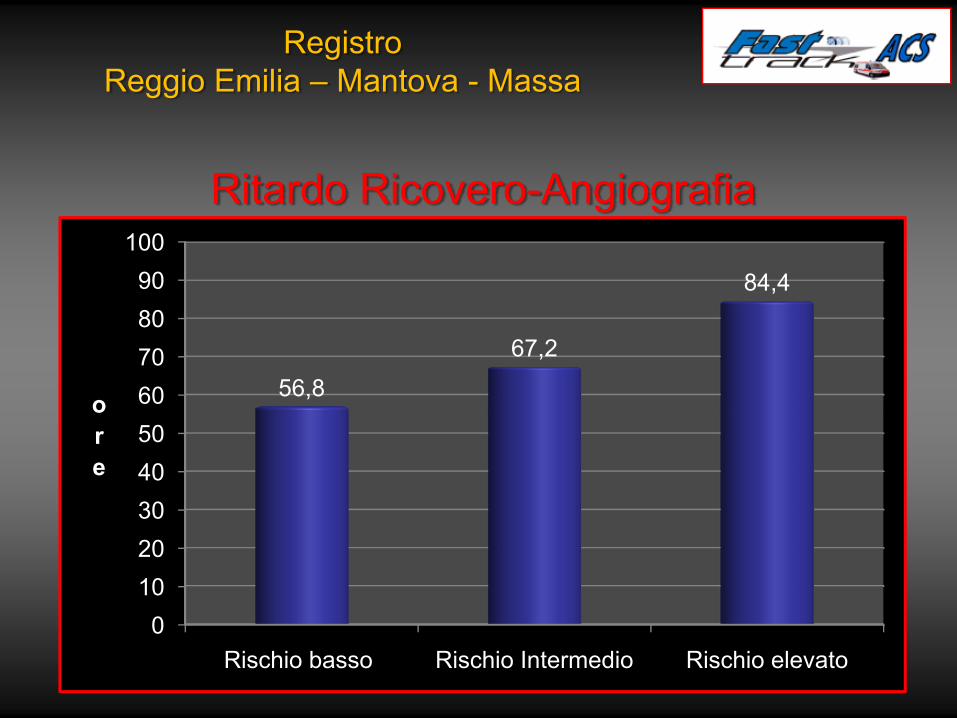
Ritardo Ricovero-Angiografia
0102030405060708090
100
Rischio basso Rischio Intermedio Rischio elevato
56,867,2
84,4
ore
RegistroReggio Emilia – Mantova - Massa
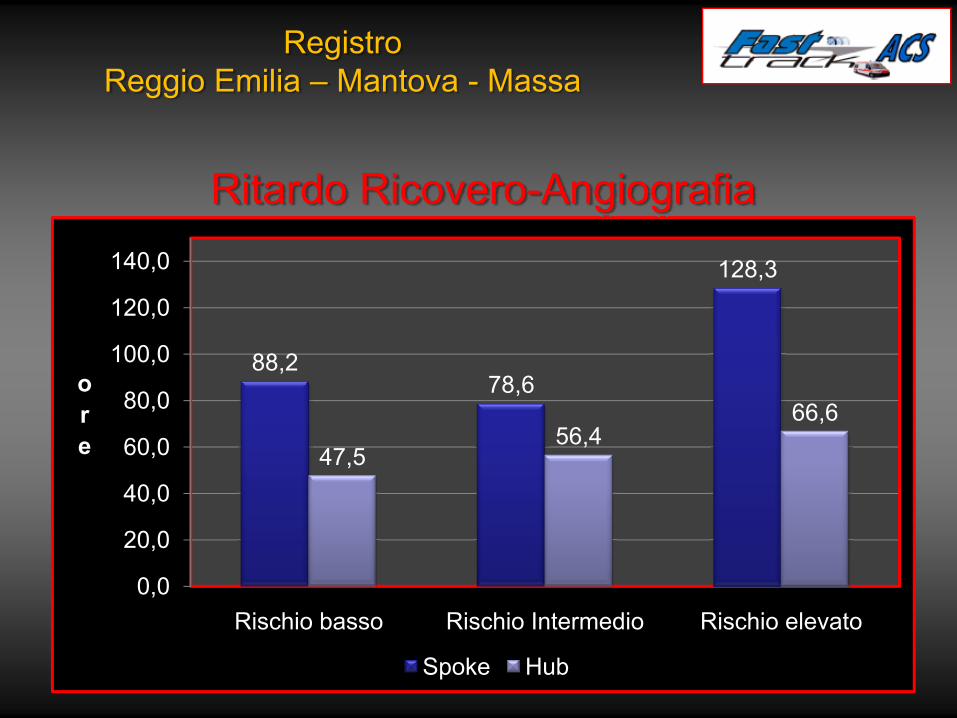
88,278,6
128,3
47,556,4
66,6
0,0
20,0
40,0
60,0
80,0
100,0
120,0
140,0
Rischio basso Rischio Intermedio Rischio elevato
ore
Spoke Hub
RegistroReggio Emilia – Mantova - Massa
Ritardo Ricovero-Angiografia
Conclusioni • I risultati osservati nella pratica clinica
indicano che oltre il 50% dei pazienti con SCA non è trattato secondo i parametri organizzativi delle L. G.
• Ciò non ostante, i dati di registri sulle SCA indicano una prognosi “buona/accettabile”
• Le Linee Guida individuano comportamenti “virtuosi” analizzando dati di studi randomizzati e controllati;
Conclusioni
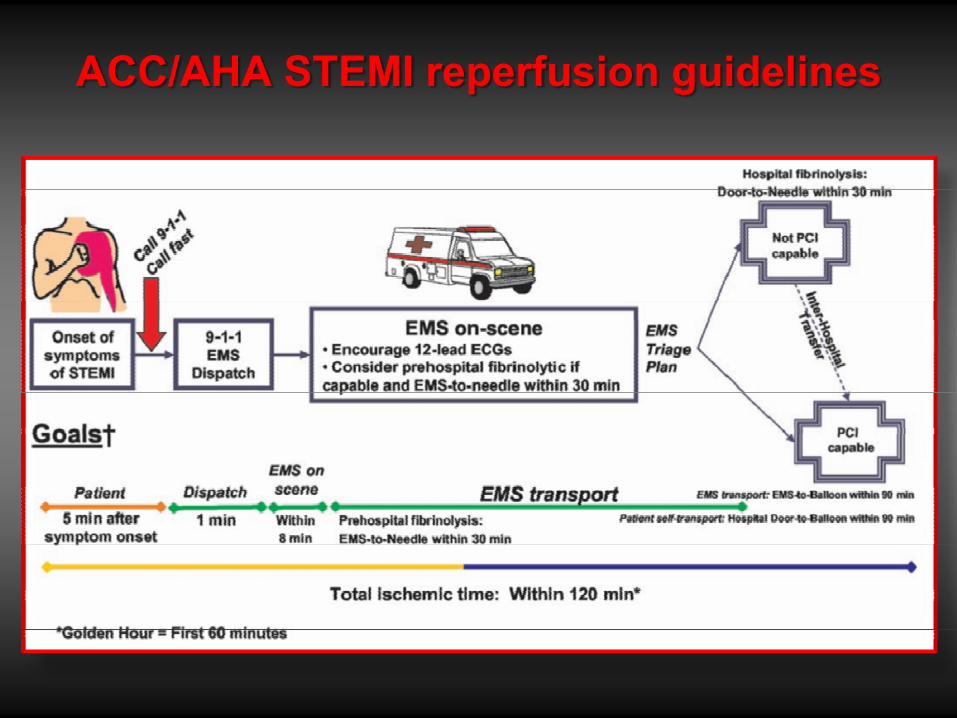
ACC/AHA STEMI reperfusion guidelines