ADR Reporting, Medication Error Reporting System (MERS) &
Cold Chain ManagementUpdates from Bengkel Laporan Kesan Advers
Ubat-Ubatan dan Vaksin 18-20 March 2009 Organized By: Bahagian
Perkhidmatan Farmasi, KKM
Pharmacovigilance: Ensuring the Safe use of Medicine and Role of
Pharmacists
Registration Criteria
Efficacy
Evaluated from data obtained from clinical trials Compliance to
established standards, manufacture by GMP licensed premise
Toxicology, clinical trials
Quality
Safety**
** (Very limited information)(Further established through post
registration studies) (Discovering new dangers of drugs after
marketing is common)
What is Pharmacovigilance (PV)?
The science and activities relating to the detection,
assessment, understanding and prevention of adverse effects or any
other medicinerelated problem - WHO
Why is PV needed?
HISTORY
Registration of New Chemical Entities was very much dependent on
the status of products in the reference countries Changes to
product information was mainly industry driven Few pre-clinical
studies conducted in the region and hardly any Phase IV studies
Adverse drug reaction reporting was very minimal involved reports
submitted by health care professionals
CONT..
Most reports were for known reactions involving older drugs
which were used in government-run hospitals Signal detection not
possible as there were too few reports Only able to detect some
quality defects of generics which manifested as ADRs
Pharmacovigilance was mainly about getting ADR reports and
submitting them to WHO No significant regulatory changes made based
on these reports
CURRENT SCENARIO
Increased awareness and interest amongst doctors and pharmacists
to report ADRS as they have seen some benefit in reporting
Increasing number of clinical trials being conducted especially in
Singapore, Thailand and Malaysia GCP training for investigators
served to increase awareness of SAE and ADR reporting amongst
health care professionals and the industry
CONT.
More hospitals and companies using on-line reporting system less
hassle than submitting hard copy reports Increasing involvement by
hospital pharmacists in pharmacovigilance during clinical ward
rounds and when counseling patients
The aims of Phamacovigilance
To improve patient care and safety To improve public health and
safety To contribute to the assessment of benefit, harm,
effectiveness and risk of medicines To promote understanding,
education and clinical training
Who are the partners?
Government Industry Hospitals and academia Medical and
pharmaceutical associations Poisons information centres Health
professionals Patients Consumers Media WHO
DEFINITION
Adverse Drug Reaction
"A response to a drug which is noxious and unintended, and which
occurs at doses normally used in man for the prophylaxis,
diagnosis, or therapy of disease, or for the modification of
physiological function." Any untoward medical occurrence that may
present during treatment with a pharmaceutical product but which
does not necessarily have a causal relationship with this treatment
Any unintended effect of a pharmaceutical product occurring at
doses normally used in man which is related to the pharmacological
properties of the drug
Adverse Event
Side Effect
WHAT TO REPORT?SERIOUS ADRS A serious adverse event (experience)
or reaction is any untoward medical occurrence that at any dose:
results in death, is life-threatening, requires inpatient
hospitalization of prolongation of existing hospitalization, is a
congenital anomaly/birth defect. NOTE: The term life-threatening in
the definition of serious refers to an event in which the patient
was at risk of death at the time of the event; it does not refer to
an event which hypothetically might have caused death if it was
more severe.
Adverse Reactions: Possible Causes
Intrinsic factors of the drug
Pharmacological Idiosyncratic Carcinogenicity, Mutagenicity
Teratogenicity Adulterants Contamination
Extrinsic factors
Underlying medical conditions Interactions Wrong usage
WHAT SHOULD BE REPORTED
New drugs
Report all suspected reactions including minor ones All serious,
unexpected, unusual ADRs
For established or well known drugs
Change in frequency of a given reaction ADRs to generics not
seen with innovator products ADRs to traditional medicines
WHAT SHOULD BE REPORTED
All suspected drug-drug, drug-food, drug-food supplement
interactions
Statement highlighting marine source of supplements such as
glucosamine so that can be avoided by those with allergy to sea
food
ADRs associated with drug withdrawals ADRs due to medication
errors eg
vincristine given IT
ADRs due to lack of efficacy or suspected pharmaceutical
defects
INNOVATOR PRODUCTS
Limited information available at time when drug is first
marketed Minimal information on use in Asian population,
interactions with indigenous medicines Conduct intensive monitoring
to identify new, unlabeled adverse reactions, monitor for rare
reactions Provide updates to prescribers on new findings, labeling
changes, safety issues
GENERIC PRODUCTS
Monitor efficacy Monitor adverse effect profile to study
differences in ADR pattern compared with innovator products Help in
improving quality of generics used
Does the problem arise due to ADR or quality defects?
Problems appearing in sequence Abrupt increase in frequency
Problem only arises with certain brands
NON-PRESCRIPTION MEDICATIONS
Quality defects can also lead to ADRs e.g. Pan Pharmaceuticals
(Australia) case Patients can develop ADRs to food supplements,
health products Overuse of supplements Current issue of dioxin
contamination in Cod Liver Oil preparations resulting in product
withdrawals in UK
TRADITIONAL & COMPLEMENTARY MEDICINES
Minimal information available on traditional medicines ADRs Drug
interactions At risk groups e.g. alfalfa and exacerbation of SLE
Misnomer of because it is natural, it is safe Association of Black
Cohosh with liver problems Health professionals should try to get
as much information as possible Name of product Indication Place of
purchase (esp for unregistered products)
PREGNANCY
Very little information on outcome data for drugs used in
pregnancy
Current issue of association between lamotrigine use and cleft
palate syndrome
Should follow-up cases where drugs are prescribed intentionally
or have been used inadvertently to monitor outcome of pregnancy,
effect to the foetus/baby
COMMUNICATING THE OUTCOME OF PV
DHCP Letter product holders Product Alerts National Health
Authorities Media statements - National Health
Authorities/Pharmacovigilance Centres Newsletters National
Pharmacovigilance Centres and WHO Feedback to reporters National
Pharmacovigilance Centres
INTERNATIONAL COOPERATIONMALAYSI A
WHO
OTHER REGULATORY AGENCIES eg USFDA, EMEA, TGA, HSA
WHO PROGRAMME FOR INTERNATIONAL DRUG MONITORING
Started 1968 Located in Uppsala, Sweden Collaborating centre for
maintaining global ADR database Vigibase The National Drug Safety
Monitoring Centre, was accepted as the 30th member of the WHO
Safety Monitoring Program in 1990.
Roles of WHO Collaborating Centre
Identify early warning signals of serious adverse reactions to
medicines Evaluate the hazard Undertake research into the
mechanisms of action to aid the development of safer and more
effective medicines
SO.WHAT IS OUR ROLE?
SEND NOT ONLY QUANTITY BUT.
QUALITY REPORTS
HOW?
Monitor clinical status of patients Identify the correct ADRs
not side effects Get more information Investigate at hospital level
Help doctors to fill-up the forms Keep patients record if more
information needed
Recognizing, Reporting and Reducing Adverse Drug Reactions
Limitations of Clinical Trials
too few - normally < than 1500 patients too simple - use
patients without complications, other medical conditions too narrow
- limited indications too brief - limited time too median - very
old/very young patients, pregnant women not included
Classification of ADRs
Type A (Augmented ) reactions Reactions which can be predicted
from the known pharmacology of the drug Dose dependent, can be
alleviated by a dose reduction E.g. Bleeding with anticoagulants,
bradycardia with beta blockers, headache with nitrates, postural
hypotension with prazosin
Classification of ADRs
Type B (Bizarre) reactionsCannot
be predicted from the pharmacology of the drug Not dose
dependent, host dependent factors important in pre-disposition E.g.
anaphylaxis with penicillin, anticonvulsant hypersensitivity
Classification of ADRs
Type C (Chemical) reactions Biological characteristics can be
predicted from the chemical structure of the drug/metabolite E.g.
paracetamol hepatotoxicity Type D (Delayed) reactions Occur after
many years of treatment. Can be due to accumulation E.g. Secondary
tumours after treatment with chemotherapy, teratogenic effects of
phenytoin taken during pregnancy, analgesic nephropathy, tardive
dyskinesia with antipsychotic agents
Classification of ADRs
Type E ( End of treatment) reactions Occur on withdrawal
especially when drug is stopped abruptly E.g. withdrawal seizures
on stopping phenytoin, adrenocortical insufficiency on withdrawal
of steroids
How to recognize ADRs?
Since ADRs may act through the same physiological and
pathological pathways as different disease, they are difficult and
sometimes impossible to distinguish
Drug administered Pt develops a new condition/symptoms Drug
suspected? Check literature
Documented ? (for the product or similar class of products)
Highly suggestive of ADR
Not documented in literature Drug continued Drug
discontinuedSymptoms improve (+ve dechallenge)
Worsening of symptoms
Drug restarted Any other possible causes? Concomitant therapy
Underlying conditions
Symptoms recur (+ve rechallenge)
Definitions
Dechallenge withdrawing the drug(s) and recording the outcome
improved or not improved Rechallenge giving one drug again under
the same conditions as before and recording the outcome recurrence
or no recurrence.
Preventing, Reducing and Reporting ADRs
Completely avoiding ADRs may be impossible Some simple
approaches to prevent the occurrence can be applied
HOW?
Charting all medications when ordered and refilled drug
allergies, types of allergy Close attention to the written
prescription correct dosing, proper dosage form, avoid
abbreviations, cautious of drugs with similar names Being familiar
with all potential side effects, interactions Choosing the oral
route when possible Taking careful history of patients esp. elderly
pts
CONT.
Initiate a committee of Post-Marketing Drug Risk Management at
hospital level Initiate active surveillance (rather than relying on
spontaneous reporting) Assess whether physicians are following
recommended DCA warnings Having a high index of suspicion for
ADRs
ADR ReportingIntensive safety surveillance New Zealand
Prescription event monitoring US, UK Spontaneous adverse drug
reaction monitoring Australia, Malaysia
SPONTANEOUS REPORTING SYSTEM
Passive surveillance system Spontaneous ADR reporting system has
3 phases: Data
collection most problematic Data processing Data analysis and
interpretation
HOW TO REPORT?
ONLINE REPORTING www.bpfk.gov.my ADR
forms
REPORTING MECHANISM Directly by the prescribers Through the
pharmacists Through the drug companies
CAUSALITY ASSESSMENT OF SUSPECTED ADVERSE DRUG REACTION
INTRODUCTION
Spontaneous reporting system data acquisition, assessment,
presentation and interpretation. Causality assessment part of the
1st step in case assessment and is based on a general system that
is intended for all reactions and all drug.
Standardized case causality assessment has become a routine at
pharmacovigilance centre around the world. Decrease the ambiguity
of the data and prevention of erroneous conclusion It neither
eliminates nor quantifies uncertainty but, at best, categorizes it
in a semi quantitative way
METHODS OF CAUSALITY ASSESSMENTThere were several method that
can be use to make a causality assessment of ADRs reports. The
literature (9 points of consideration Morges, Switzerland , 1981)
Probability calculation (Bayes Theorem) Aetiological Diagnostic
Systems (Bnchious group method) French imputation systems The
European ABO Systems The US Reasonable Possibility Systems The
Naranjo ADR Probability Scale WHO Causality Categories
The Naranjo ADR Probability ScaleQuestions 1) Are there previous
conclusive reports on this reaction? 2) Did the ADR appear after
the suspected drug was administered? 3) Did the ADR improve when
the drug was discontinued? 4) Did the ADR appear with re-challenge?
5) Are there alternative causes for the ADR? 6) Did the reaction
appear when placebo was given? 7) Was the drug detected in blood at
toxic levels? 8) Was the reaction more severe when the dose was
increased, or less severe when the dose was decreased? 9) Did the
patient have a similar reaction to the same or similar drug in any
previous exposure? 10) Was the ADR confirmed by any objective
evidence? Yes +1 +2 +1 +2 -1 -1 +1 +1 No 0 -1 0 -1 +2 +1 0 0 Dont
Know 0 0 0 0 0 0 0 0
+1 +1
0 0
0 0
The Naranjo Probability ScaleThe score :> 8 = Highly probable
5-8 = probable 1-4 = possible 0 = doubtful
WHO Causality Categories C1
Certain C2 Probable C3 Possible C4 Unlikely C5
Unclassifiable
WHO Causality Categories
C1: Plausible time, not related to underlying condition,
concurrent disease, other drugs or chemicals, related
pharmacologically, +ve dechallenge, +ve rechallenge C2: Reasonable
time, unlikely to be related to concurrent disease, other drugs,+ve
dechallenge, no rechallenge
CAUSALITY ASSESSMENT
C3: Reasonable time, may be due to concurrent disease, other
drugs, no information on dechallenge C4: Improbable temporal
relationship, other confounding factors such as drugs, chemicals,
underlying disease C5: Insufficient information to analyse the
report
Case causality assessmentHow close is the relationship between
drug and event? Did the drug cause the event?
CONSUMERS MEDICINES SURVEILLANCE
The protocol for the medicines surveillance integrating consumer
reporting
The surveillance of medicines integrating consumer reporting
will be an extension and expansion of the existing surveillance
activities carried out by NPCB NPCB will be the focal point which
will receive, analyze and investigate the reports submitted by the
consumers.
The importance of involving consumer in medicines
surveillance
The ultimate goal is to improve the quality, efficacy and safety
of the marketed product Empower consumers to be aware ofQuality
Safety Correct usage of medication
Alleviate the problem of consumers wasting their valuable
resources on medicines which may expose their health to risks.
Reporting by consumers can be done through
Reporting forms On-line reporting Other channels eg: letters,
phone calls, emails and complaints done personally to Drug
Regulatory Agencies (DRA) Information channeled through health
professionals, the product owner, consumer associations or other
trade and industry organizations which will then be directed to
NPCB
What to report?
Quality defects Lack of efficacy Adverse drug reactions
Suspected counterfeit product Unregistered product Suspected
adulterated products Medication error / near misses Fraudulent /
misleading claims
WORK PROCESSReceive product complaint Verify registration
status
Inform reg. holder without identifying complainant - Must
respond with findings within 2 wks
BPFK conduct own investigations based on nature of complaint
Decide on action to be taken based on outcome of the findings
-Product recall - Intensified surveillance -GMP inspection of
premises, of manufacturer/other products -No generalised action
because problem is not due to product per se Inform complainant on
action taken QAP indicator: 85% of all complaints received must be
resolved within 6 weeks
Quality DefectsCan arise due to Manufacturing problems Improper
storage and handling by Manufacturer End
/ distributor
user
Inappropriate handling during repacking
Decision Making Process
Problem identified confined to a particular batchBatch recall
Warning letter
Problem involves product in generalTotal product recall
Suspension / cancellation of registration GMP inspection of
premise
Cancellation of manufacturing license
Legal action if necessary
Regulatory actions taken
Active ingredients withdrawn Revocation of product,
manufacturing license Product withdrawn from the market Restriction
of usage Carries a warning Precautionary statement included Review
of labeling requirements Make changes to product information based
on new findings
Report acknowledgement
All complainants will receive an acknowledgement from NPCB
Information on actions which are taken based on the report will be
made known to the complainant after the necessary actions have been
taken
Confidentiality
The confidentiality of complaints will be maintained as far as
possible Only the outcome of actions may need to be publicized in
the interest of public safety
R P R IN EO T G
T e in rm n th y u p h fo atio at o b u fo th so p rp s e sed r
e le u o T e r ep rter is req ire h o u in rm n is req ired fo atio
u an p n o tsid th d g y erso u e e ru
Links
Form BPFK 418.3 Product Comp
ADVERSE EVENTS FOLLOWING IMMUNIZATION
Definition of Adverse Events Following Immunization Any adverse
event that follows immunization that is believed to be caused by
the immunization
Classification of AEFIsVaccine reaction Event caused or
precipitated by the vaccine when given correctly, caused by the
inherent properties of the vaccine Programme error Event caused by
an error in vaccine preparation, handling or administration
Coincidental Event that happens after immunization but not caused
by the vaccine a chance association Injection reaction Event from
anxiety about, or pain from, the injection itself rather than the
vaccine Unknown Events cause cannot be determined
A. Vaccine Reactions
Classified as common, minor reactions and rare, serious
reactions Most reactions are minor and settle on their own Serious
reactions very rare and generally do not result in long-term
problems
Common, Minor Reactions
Immune responses such as local reactions (pain, swelling,
redness of inj. site), systemic reactions (fever, irritability,
malaise, loss of appetite) Some vaccines components such as
adjuvant, stabilizers or preservatives can lead to reactions Only
last for one/two days except measles/MMR (6-12 days)
Rare, Serious Reactions
Eg : seizures, thrombocytopenia, hypotonic hyporesponsive
episodes, persistent inconsolable screaming, anaphylaxis, paralytic
poliomyelitis, disseminated BCG infection
Prevention and Treatment
Rarely contraindicated check allergy status (vaccines and its
components) Advice parents on managing common reactions/serious
reactions
B. Programme Errors
Result from errors and incidents in vaccine preparation,
handling or administration Eg
: reuse of syringes/needles, incorrect diluents, wrong injection
sites, improper storage/transport, contraindications ignored
May lead to a cluster of events
How to avoid programme errors?
Reconstituted with correct diluents (supplied by manufacturers)
Discard any leftover at the end of immunization session Provide
refrigerator specially for vaccines Trained workers, closely
supervised and procedures followed Investigation team for AEFI
C. Coincidental Events
Falsely considered to be caused by immunization (event happens
after immunization) Eg : sudden death after the mass campaign
D. Injection Reactions
Unrelated to the content of the vaccine Eg
: fainting (older children due to stress), hyperventilation,
vomiting, convulsion (due to anxiety), hysteria (needle-phobic)
AEFIs vs ADRs
Vaccines administered to large numbers of healthy people
Vaccines not only benefited to individuals but community as well
Vaccines given to an entire cohort of population Events normally
serious, clusters and cause public concern
AEFI is part of the monitoring system of adverse drug reactions
(not similar to individual drugs) The priority for immunization
safety surveillance is to identify and correct programme errors
Estimated AEFI Rates Following Vaccination (WHO figures)Vaccine
Estimated rate (severe reactions only) 1 in 1 000 1 in 50 000 doses
1 in 2-3 million doses (or 1 in 750 000 doses for the first dose) 1
in 1 million doses 1 in 750 000 doses
BCG Oral Polio Vaccine
Measles DTP
Errors Which Can Lead to AEFIs
Too much vaccine given/dose Improper immunization site or route
Syringes/needless improperly sterilized Incorrect diluents, wrong
amount used Drug given instead of vaccine Vaccine prepared
incorrectly (not to be shaken) Vaccine/diluent contaminated Vaccine
stored incorrectly Contraindications ignored Expired vaccines have
been used
List of reportable AEFIsOccurring within 24 hours of
immunizationAnaphylactoid reaction (acute hypersensitivity
reaction) Anaphylaxis Persistent (more than 3 hours) inconsolable
screaming Hypotonic hyporesponsive episode (HHE) Toxic shock
syndrome (TSS) # Severe local reaction # Sepsis # Injection site
abscess (bacterial/sterile) # Seizures, including febrile seizures
(6-12 days for measles/MMR; 0-2 days for DTP) Encephalopathy (6-12
days for measles/MMR; 0-2 days for DTP) Acute flaccid paralysis
(4-30 days for OPV recipient; 4-75 days for contact) Brachial
neuritis (2-28 days after tetanus containing vaccine)
Thrombocytopenia (15-35 days after measles/MMR) Lymphadenitis #
Disseminated BCG infection Osteitis/Osteomyelitis Any death,
hospitalization, or other severe and unusual events that are
thought by health workers or the public to be related to
immunization #
Occurring within 5 days of immunization Occurring within 15 days
of immunization Occurring within 3 months of immunization Occurring
between 1 and 12 months after BCG immunization No time limit
# limit reporting to these events, if only limited reporting
capacity
Reporting AEFIs Who should report?Peripheral health
workersDetect and report event
Doctors/Pharmacists/IndustriesStimulates report, investigates,
filters, provides feedback, proposes classification National Drug
Safety Monitoring Centre
Product holders
Receives, transmits, share database, evaluates, take action,
notifies
WHO
Reporting AEFIs
When to report? Immediately
Reporting AEFIs
How to report?ON-LINE REPORTING www.bpfk.gov.my MANUAL ADR Forms
(Fax & Mail)
Reporting AEFIs
Barriers to reporting? Not considering the event as related to
immunization Not knowing about the reporting system and process
Lethargy lack of interest/time, inability to find report form Fear
that the report will lead to personal consequences Guilt about
having caused harm and being responsible for the event Diffidence
about reporting an event when not confident
Reporting AEFIs
How to overcome? Increase
awareness
Importance of reporting, system of reporting, user friendly,
posters, training, talks
Emphasizing
that investigations are finding problems, not blaming
individuals Giving positive feedback for reporting
Investigating AEFIs
Which reports should be investigated?
May have been caused by programme error Not listed events
defined for AEFI surveillance Serious event of unexplained cause
Causing significant parental or community concern
[accurate denominator of vaccine use (to get the rate) is
important compared to the number of reports]
Who should investigate?
National Drug Safety Monitoring Centre together with the
state/districts committee
When to investigate?
As soon as practicable
Why local reports are important?
Differ among countries in the occurrence of AEFIs and other
related problems Due to differencesdiseases and prescribing
practices genetics, diet, traditions drug manufacturing process
drug distribution and use use of traditional and complementary
drugs
Actions taken upon completion of the investigation/assessment by
DCA Recall Suspension Withdrawal Advice logistics, procedure,
storage, training Labeling changes boxed warning, CI DHCP Letter
Circulars Media
RATIONAL DRUG USE
Knowledge of AEFIs should be used to
Minimise adverse events in susceptible patients, at risk groups
Advice prescribers/consumers on the proper use of vaccines Monitor
patients in order to further enhance knowledge on safety issues
Provide information to regulators, decision makers on vaccines
being used so that appropriate action may be taken if warranted
CASE REPORT - PEDIACEL A 3-month old female child was vaccinated
with a second dose of Pediacel which contains DPT/Polio/HIB on 29th
December 2006 at 9.50am. The child developed lethargy, poor feeding
and intermittent cry with no fever in the afternoon of the
vaccination day. The child was only brought back to the clinic on
30th December 2006 at about 4.20pm in near collapse condition. The
child was pallor with perfusion > 3 second, heart rate 100/min,
poor pulse volume and poor lung function. She was resuscitated at
the clinic but collapsed at 5.45pm. CPR was given for about one
hour but unfortunately the child passed away at 6.45pm. Her body
was sent to Hospital Kajang. The post mortem was done in Hospital
Kajang and the result shown she died due to Acute Lymphocytic
Infiltration to Heart and Mild Endocarditis (viral). This report
was sent to MADRAC on 3rd January 2007. The reporter also reported
that the child was well prior to the 1st dose of Pediacel.
CASE REPORT ON TRITANRIX HB HiB VACCINEA 3 month old infant
received the 2nd dose Tritanrix HB HiB and OPV Vaccine given at
Klinik Desa Mata Air. The vaccine was administered intramuscularly
into left thigh at around 9am on the 18/06/2008. Within 2 hours
after administration, the baby started crying excessively and soon
collapsed. She was immediately brought to Hospital Tuanku Fauziah,
where she was confirmed dead upon arrival at the hospital. Previous
exposure, 1st dose vaccination with the same vaccine did not result
in any adverse event. The baby was otherwise well with no
significant background medical history or known allergies. From the
post mortem and toxicology findings, the cause of death was
interstitial pneumonia. There is no objective evidence showed the
possibility of fatal anaphylaxis reaction towards the vaccine.
Information from the WHO Immunization Safety Programme, showed the
expected rate for crying abnormal and collapsed after vaccinated
with the DTP was 1/100 dose and 1/1750 doses respectively. After
the discussion, MADRAC agreed that the adverse event crying
abnormal and collapsed cause by the vaccine. Causality C1 (certain)
had been given for the reaction because, there was no other
concomitant drug given together with the vaccine, with a plausible
temporal relation time and there was no other underlying disease
which can be link to the ADR.
CASE REPORT - Pentaxim and Euvax 2 month old male infant
received the 1st dose of DTAP-IPV given at Klinik Kesihatan WP
Labuan. The vaccine was administered on 12/1/2009 (time was
unknown). The baby then developed low grade fever at 12.00 noon on
the same day and 1.5mls Syrup Paracetamol given. The baby fed as
usual after that. The mother then noticed that the baby had an
injection site swelling and the mother put a warm compress at the
injection site. The baby was again given Paracetamol Syrup at 8 pm
and a last dose at 4 am. The mother noticed that the infant choked
a little after the administration of the last dose of paracetamol
and had fed the child immediately after giving the medicine. Mother
and child went to sleep. At around 6 am the mother found that the
baby was not moving, looked pale and had bleeding from the ears and
nose. The parents brought the baby to the Hospital WP Labuan at
7.50 am. At the A&E Department the baby was found to have
already stopped breathing. The parents refused to do a postmortem.
Cause of death - UNKNOWN. Suspected drug - Pentaxim and Euvax ADR-
low grade fever Concomitant drug Paracetamol MADRACs Causality
C2
February 13, 2007 The Food and Drug Administration (FDA) is
notifying health care providers and consumers about 28
post-marketing reports of intussusception following administration
of Rotavirus, Live, Oral, Pentavalent vaccine (trade name RotaTeq),
manufactured by Merck and Co., Inc. Intussusception is a serious
and potentially life-threatening condition that occurs when the
intestine gets blocked or twisted. One portion of the intestine
telescopes into a nearby portion, causing the intestinal
obstruction. The most common site is where the small intestine
joins the large intestine. In Malaysia, Rota Teq, marketed by MSD
and the company has been informed to disseminate this information
to relevant healthcare professionals.
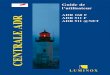
T R E N D L A P O R A N V A K S IN140 120 100 BIL. LAPORAN
VAKSIN 80 60 40 20 0 2000 2001 2002 2003 2004 2005 2006 2007 2008
TAHUN 14 26 10 13 52 68 39 75 132
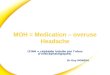
T R E N D L A P O R A N A D R D A N V A K S IN6000 5000 BIL.
LAPORAN 4000 3000 2000 1000 3068 2 3 6 32 5 4 3 1665 1 0 0 01 0 6 3
4826 B IL . L A P O R A N A D R B IL . L A P O R A N V A K S IN
792 787 0 14 10 26 13 52 68 39 75 132 2 0 0 02 0 0 12 0 0 22 0 0
32 0 0 42 0 0 52 0 0 62 0 0 72 0 0 8 T AH U N
THANK YOU