Embed Size (px)
Citation preview

Adverseeventstoan,bio,csandvaccines:Approachtodiagnosis&management
MasaoYamaguchi,MD,PhDDivisionofRespiratoryMedicineandAllergology,DepartmentofMedicine,TeikyoUniversitySchoolofMedicineTokyo,Japan�
JointCongressofAPAAACIandAPAPARI2016
ConflictofInterest(COI)MasaoYamaguchi
Nothingtodisclose�
• Overview
• TrendsinJapan
• Basisofdesensi,za,onprocedure
• Whatneedstobekeptinmind?�
immunological mechanism in drug hypersensitivity
typical case: anaphylaxis induced by β-lactam antibiotics
typical cases:
anaphylaxis triggered by radiocontrast media
aspirin-exacerbated respiratory disease
ciprofloxacin-induced acute reaction
isoniazid-induced liver damage
vancomycin-induced red-man syndrome
non-immunological mechanism in drug hypersensitivity
modified from: Allergy: Principles and practice 8th edition�2013 � Allergy: Principles and practice 8th edition �2013�
type� mechanism� examples�
�� IgE-mediated� anaphylaxis urticaria
���complement-dependent cellular damage�
hemolytic anemia thrombocytopenia�
����immune complex-mediated�
serum sickness drug fever eruption, vasculitis (in part)�
���delayed, cellular immunology�
contact dermatitis erythema multiforme SJS/TEN hepatitis
Penicillincaninducevarioustypesofadversereac,on�

Diagnos,cprocedure�
Thestar,ngpointistokeepinmindthepossibili,esofdrugallergy.Precisehistory-takingisveryimportant."Isthe,mecoursereasonable?"1)OccuraWerstar,ngtheadministra,onofthedrug?"2)ResolveaWerdiscon,nua,on?"3)Reproduciblereac,on?
Searchforsimilarcasereportsisalsoimportant.
Whattestscanbedone?�
1.Skintest&&Intradermal,prick,scratchtestsforimmediatereac,on&&Patchtestfordelayed-typereac,on2.Challengetest&&Ifnecessary.Butavoidinpa,entsdemonstra,ngseverecutaneousreac,onorhematologicaldisorders.3.Invitrotests:notalwaysuseful&&Serumtryptaseandhistamineforanaphylaxis&&RASTorELISAetc.forspecificIgE&&Basophilac,va,ontestordegranula,ontest&&Lymphocytes,mula,ontest(LST)
BackgroundPenicillinallergyisthemostcommonlyreportedmedica,onallergy,withaprevalencerateof5%to10%.Inolderlarge-scalestudies80%to90%ofpa,entswithahistoryofpenicillinallergyarefoundnottobeallergic,butrecentdatasuggestthishasincreasedto95%.Poten,alreasonswhymostpa,entswithalabelof‘‘penicillinallergy’’areabletotoleratepenicillinsincludethefollowing:(1)thereac,onwasmislabeledasallergic,(2)thesymptomswereacributabletotheunderlyingillnessoraninterac,onbetweentheillnessandthean,bio,c,and(3)levelsofpenicillin-specificIgEwaneover,meandpenicillinallergyiscommonly(butnotalways)outgrown.
SolenskyR.JACI2012;130:1441.
Case:35-y.o.femaleSheexperiencedthese2episodes4yearsago.1stepisodeofanaphylaxisoccurredjustaWershetookcefcapenepivoxileandloxoprofen2ndepisodeofanaphylaxisoccurredjustaWershefinishedinhala,onofbetamethasoneandcefmenoxime.
�"�#35����Acasewithβ-lactam-inducedanaphylac,cepisodes�
Allpoten,altriggersshouldbelistedandcollected�
1stepisodecefcapenepivoxileloxoprofenhormonaldrug
2ndepisodecefmenoximelidocainebetamethasoneandothers
Skintests(pricktests,intradermaltests)wereperformed.Latexshouldalsobeconsideredwhenneeded.�
Results�
Cefcapenepivoxile:pricktest:nega,veintradermaltest:posi,veat1µg/ml(healthyvolunteersshowednega,veresults)
Allotherdrugsshowednega,veresults�
Cefmenoxime:pricktest:nega,veintradermaltest:nega,veat1µg/ml

Case:35-y.o.femaleSheexperiencedthese2episodes4yearsago.1stepisodeofanaphylaxisoccurredjustaWershetookcefcapenepivoxileandloxoprofentabletsprobablythisreac,onisbasedonhighspecificity2ndepisodeofanaphylaxisoccurredjustaWershefinishedinhala,onofbetamethasoneandcefmenoxime.probablythisreac,onisbasedonlowsensi,vity,orcross-reac,on
�"�#35����
cefotaxime ceWriaxone cefditrenepivoxile
wheal5x4,flare8x7mmat10µg/ml
cefmenoxime:skintestnega,ve
cefcapenepivoxile:intradermalposi,ve
skintestnega,ve skintestnega,ve
Skintestsmaybeusefulinsomepa,entswithquinolonehypersensi,vity�
�$#��� ����� ����� ����� ����� ����� ����� ���
��# �"!� �� �� �� �� �� �� ����
���# �"!��%��
�� �� �� �� ��%�
����# �"!��%� �� �� �� �� ��
��%���
�����# �"!��%�� �%�� �� �� �� ��
��%�� % �
�����������
������������������$#��� ����� ����� ����� ����� ����� ����� ���
����# �"!� �� �� ��� ��� ��� ��� ����
��# �"!� �%�� �% � �� �� �� ���%��� ��%��
���# �"!� �%�� �� �� �� %���%� �% �
����# �"!� �% � �� �% � %���%��� �%��� �%�
�����# �"!� % �
%�
� ����������� ����������������������������������!��������������������������
allergytovaccines�Tetanus toxoid also has some potential association with GBS andwith a rare local neurologic event called brachial neuritis, whichinvolves shoulder pain followed by weakness.26 However, neitherGBS nor brachial neuritis is a contraindication to the receipt of ad-ditional doses of tetanus-containing vaccines.104
Varicella vaccine is another live virus immunization that cancause vaccine-induced illness, particularly the appearance ofvaricella lesions. These reactions occur at the injection site inapproximately 3% of recipients and are more generalized inanother 3%.110 The rash typically appears within 3 weeks of vac-cination.111 The disease caused by coincident natural exposuremight be difficult to distinguish from vaccine-induced varicella,and most rashes are due to wild-type virus.111 A zoster-typerash can rarely appear after a varicella vaccination and might con-tain either vaccine-strain or wild-type virus.112,113 As with MMRvaccine described above, varicella vaccine can cause a late-onsetfever and rarely febrile seizures, again without long-term seque-lae. Although varicella disease (chickenpox) itself can be moresevere in children with atopic dermatitis, the varicella vaccinecan be safely administered to children with atopic dermatitiswithout an increased risk of complications,114 and humoral andcellular immune responses to the vaccine are similar in childrenwith and without atopic dermatitis.115
A serious adverse effect of yellow fever vaccine is encepha-litis.116 The risk for this complication is as high as 4 per 1000 in-fants, and for this reason, the vaccine is relatively contraindicatedin this age group. It should not be given to any infant younger than6 months; it should only be given to those younger than 9 monthsif their risk from the disease is very high.117 The yellow fever vac-cine has recently been associated with a very severe multisystemillness in adults with features that are strikingly similar to those ofyellow fever disease itself.117 This adverse reaction, now termedyellow fever vaccine–associated viscerotropic disease, has oc-curred exclusively in first-time vaccine recipients and has a65% mortality rate.117 Most yellow fever vaccine–associated vis-cerotropic disease has occurred in patients who are not known tobe immunocompromised; however, a history of a thymus disorderand age 60 years or greater have been identified as risk factors,making these a contraindication and a precaution, respectively.117
The cause of these reactions is still unknown, but this vaccineshould not be given to patients unless they are at risk of acquiringyellow fever, typically by traveling to an area in which the diseaseis endemic. An inactivated, and thus presumably safer, vaccine isbeing developed.118
Summary Statement 11: Pregnant women should not bevaccinated with live vaccines. However, pregnant womenshould be given inactivated influenza vaccine, as well as teta-nus and hepatitis B vaccine, if otherwise indicated. (B)
Because of a theoretic risk of transmitting the live agent to thefetus, pregnant women should not receive live vaccines, such asMMR, varicella vaccine, or LAIV.119 There is an increased risk ofhospitalization from influenza in pregnancy, and therefore (inacti-vated) influenza vaccine is specifically indicated in women whowill be pregnant during the influenza season.119Hepatitis B vaccineand tetanus and diphtheria vaccines should also be administered topregnant women if they would otherwise be indicated.119
Summary Statement 12: In general, live vaccines should notbe given to persons who are immune compromised because ofa risk of generalized infection with the immunizing agent. (B)
Live vaccines (Table VI) are generally contraindicated in pa-tients with immune suppression, specifically those with severe
humoral or cellular immune deficiency.11,50,120 This includes pa-tients with X-linked agammaglobulinemia, common variable im-mune deficiency, severe combined immune deficiency, severeHIV infection, leukemia, lymphoma, or other malignant neo-plasms or patients requiring treatment for these or other condi-tions with treatment modalities that impair immune responses,such as high-dose corticosteroids (2 weeks of daily treatmentwith prednisone, 20 mg or 2 mg/kg or equivalent per day). Thereare, however, exceptions even to this general rule that immune-compromised patients should not receive live viral vaccines,and readers are referred to other published guidelines fordetails.11,50,120,121
Summary Statement 13: Specific vaccines or vaccination ingeneral have been purported to have long-term consequences,including atopy, autism, andmultiple sclerosis. Epidemiologicstudies have not supported such associations. (B)
There are a number of controversies related to the long-termconsequences of particular vaccines or of vaccination in general.There have been claims that receiving childhood vaccinationsincreases the likelihood of atopic disease, autism, diabetes, ormultiple sclerosis. The associations have all been extensivelyevaluated by using many appropriate research methods andepidemiologic studies, and no relationship between vaccinationsand any of these outcomes has been demonstrated in thesestudies.122-127 There has been particular concern about thimero-sal, which was previously used as a preservative in vaccines.Although studies have not supported any adverse effect from thi-merosal exposure in vaccines,128-130 all routinely recommendedvaccines for infants and children in the United States are nowavailable only as thimerosal-free formulations or contain onlytrace amounts of thimerosal, with the exception of some inacti-vated influenza vaccines. Inactivated influenza vaccine for pediat-ric use is available as a thimerosal preservative–containingformulation, a trace thimerosal–containing formulation, and athimerosal-free formulation.50
ADDENDUMAdministering influenza vaccine to recipients withegg allergy
Influenza vaccines are grown on embryonated chicken eggs,leading to concern that residual egg protein (ovalbumin) could
TABLE VI. Live versus killed vaccines
Live vaccines Killed vaccines
Bacille Calmette-Guerin (BCG) Diphtheria, tetanus, acellular pertussis(DTaP, Tdap)
Influenza (intranasal) Diphtheria-tetanus (DT, Td)Measles, mumps, rubella (MMR) Hepatitis AOral poliovirus (OPV) Hepatitis BRotavirus Hib conjugatesTyphoid (oral) Human papillomavirus (HPV)Vaccinia (smallpox) Inactivated poliovirus (IPV)Varicella Influenza (injectable)Yellow fever Japanese encephalitisZoster Meningococcal
Meningococcal conjugatePneumococcalPneumococcal conjugateRabiesTyphoid (injectable)
J ALLERGY CLIN IMMUNOL
VOLUME 130, NUMBER 1
KELSO ET AL 35
NichlasRA,etal.JACI2012;120:25.�
Adversereac,onstovaccinesprac,ceparameter2012update
ReportfromJointTaskForceofAAAAI&ACAAI.NichlasRA,etal.JACI2012;120:25.�
testing.50 Egg protein is present in higher amounts in yellow feverand influenza vaccines46 and could, in theory, cause reactions inrecipients with egg allergy. However, numerous studies havedemonstrated that injectable influenza vaccine can be safely ad-ministered even to patients with severe egg allergy with appropri-ate precautions,51-59 likely because of the very low amount of eggprotein (ovalbumin) contained in recent years’ vaccines.60-62Rec-ommendations regarding the administration of influenza vac-cine to recipients with egg allergy are specifically addressed inan addendum at the end of this practice parameter.
If patients have a history of reaction to the influenza vaccineitself, as opposed to a history of a reaction to the ingestion of eggs,evaluation as per Fig 1 is appropriate. Patients can be allergic toheat-labile egg proteins in raw egg and, because they toleratethe ingestion of cooked egg, do not think of themselves as havingegg allergy.63 Thus the clinical history might not identify all per-sons allergic to egg proteins present in influenza or yellow fevervaccines. Chicken proteins other than those found in chickeneggmight be present in yellow fever vaccine and could be respon-sible for reactions in recipients with chicken allergy.64
Hepatitis B vaccines are grown in Saccharomyces cerevisiae(baker’s yeast or brewer’s yeast) and contain residual yeast pro-tein,12 but adverse reactions to these, if any, appear to be rare.65
Quadrivalent human papillomavirus vaccine (HPV4) might alsocontain residual yeast protein.12
The ‘‘rubber’’ in vaccine vial stoppers or syringe plungers canbe either dry natural rubber (DNR) latex or synthetic rubber.Those made with DNR pose a theoretic risk to the patient who isallergic to latex. There is one report of an anaphylactic reaction ina patient with latex allergy after hepatitis B vaccine, which wasattributed to rubber in the stopper.66 A review of more than160,000 VAERS reports found only 28 cases of possibleimmediate-type allergic reactions after receiving a DNR-containing vaccine, and these might have been due to other com-ponents.67 The latex content of vaccine packaging is providedin Table III and is updated at www.cdc.gov/vaccines/pubs/pinkbook/pink-appendx.htm.68
There is a single report of an immediate-type allergic reactionto a vaccination that was attributed to neomycin.69 However, thepatient had a maculopapular (not urticarial) rash to the topicalapplication of neomycin, and no testing for IgE to neomycinwas performed. There is a single case report of an immediate-type reaction that might have been caused by thimerosal in avaccine.70
However rare, if a patient provides a history of an immediate-type reaction to yeast, latex, neomycin, or thimerosal, it isappropriate to investigatewith immediate-type skin testing beforeimmunization with a vaccine containing these constituents.A recent publication described 8 children with anaphylaxis
within 1 hour of receiving diphtheria, tetanus, and pertussisvaccines (diphtheria and tetanus toxoids and acellular pertussisvaccine [DTaP] or tetanus toxoid, reduced diphtheria toxoid, andacellular pertussis [Tdap]).71 Six had histories of past allergic re-actions to cow’s milk, and all had very high levels of milk-specificserum IgE. These vaccines might contain trace (nanogram) quan-tities of residual casein from the medium in which they are pro-duced. The results of this report require further investigation.72
Anaphylactic reactions to DTaP or Tdap vaccines are rare, andthe majority of patients with cow’s milk allergy tolerate themwithout reaction. It is recommended that all patients, includingthose with milk allergy, continue to receive these vaccines onschedule71,72 but perhaps with some additional observation aftervaccination in those with very high levels of milk sensitivity.Table IV lists vaccine excipients by vaccine. Updated lists of
vaccine excipients by vaccine and by excipient are available atwww.cdc.gov/vaccines/pubs/pinkbook/pink-appendx.htm.12,73
Summary Statement 7: Patients who have had an apparentanaphylactic reaction after immunization should undergoimmediate-type allergy skin testing to help confirm that thereaction was IgE mediated and determine the responsiblecomponent of the vaccine. (B)Skin testing with vaccine should be performed to determine
whether the vaccine was responsible for a patient’s apparentallergic reaction.36,37 The vaccine should first be tested by usingthe prick method. If the past vaccine reaction was life-threatening, it is appropriate to use dilute vaccine for the skinprick test; in all other cases, full-strength vaccine should beused for the skin prick test. If the full-strength skin prick test resultis negative, with appropriate positive and negative controls, an in-tradermal test with the vaccine diluted 1:100 should be per-formed,74 again with appropriate controls.Aswith any skin test reagent and particularly withmaterials not
standardized for skin testing, such as vaccines, false-positive(irritant) results and clinically irrelevant positive results can
TABLE I. Levels of antibody associated with protection from
vaccine-preventable diseases
Vaccine Protective level of IgG antibody >_
Diphtheria 0.1 IU/mL11
Haemophilus influenzae b 0.15 mg/mL29
Hepatitis A 10 mIU/mL30
Hepatitis B Surface Antibody 10 mIU/mL31
Measles (Rubeola) 120 PRN titer32
Polio types 1, 2, and 3 1:8 neutralizing antibody titer33
Rabies 0.5 IU VNA/mL34
Rubella 10 IU/mL35
Tetanus 0.1 IU/mL11
Yellow fever 0.7 IU/mL29
IU, International units; mIU, milli-international units; PRN, plaque reductionneutralization; VNA, virus-neutralizing antibodies.
TABLE II. Gelatin content of vaccines, 2011
Vaccine Gelatin content
Influenza (Fluzone, Sanofi Pasteur) 250 mg per 0.5 mL doseInfluenza (FluMist, MedImmune
Vaccines, Gaithersburg, Md)2,000 mg per 0.2 mL dose
Measles, mumps, rubella(ATTENUVAX, MERUVAXII,MMRII, MUMPSVAX; Merck,Whitehouse Station, NJ)
14,500 mg per 0.5 mL dose
Measles, mumps, rubella, varicella(ProQuad, Merck)
11,000 mg per 0.5 mL dose
Rabies (RabAvert; Novartis, Emeryville,Calif)
12,000 mg per 1.0 mL dose
Typhoid vaccine live oral Ty21a(VIVOTIF, Berna, Coral Gables, Flo)
Capsule
Varicella (VARIVAX, Merck) 12,500 mg per 0.5 mL doseYellow fever (YF-VAX, Sanofi Pasteur) 7,500 mg per 0.5 mL doseZoster (ZOSTAVAX, Merck) 15,580 mg per 0.65 mL dose
J ALLERGY CLIN IMMUNOL
JULY 2012
30 KELSO ET AL
Adversereac,onstovaccinesprac,ceparameter2012update
NichlasRA,etal.JACI2012;120:25.�
48,614 (average 23,607) deaths occur each year in the UnitedStates as a result of influenza, including 57 to 197 (average,124) children.134 Many of these events could have been preventedby vaccination.135 Higher influenza vaccine coverage rates, in-cluding among those who are or who think they are allergic toeggs, can reduce these preventable hospitalizations and deaths.Summary Statement 15: Persons with a history of suspected
egg allergy should be evaluated by an allergist to determinethe status of their egg allergy, but this should not delay theirinfluenza vaccination. (A)Persons with a history of suspected egg allergy should be
evaluated by an allergist.136 The evaluation should include a de-tailed history of the nature and timing of prior suspected reactionsto egg. If the clinical history is consistent with egg allergy, thenskin prick testing to egg or specific in vitro IgE antibody testingfor egg is indicated to confirm sensitization. With a convincingclinical history and evidence of specific IgE, the diagnosis canbe confirmed, but in certain circumstances an oral food challengeto egg might be necessary or desired.136 Influenza vaccine shouldnot be withheld from those undergoing egg allergy evaluation orfrom those with confirmed egg allergy. Suspected egg allergy de-serves evaluation, regardless of the influenza vaccination status.Summary Statement 16: A growing number of studies sug-
gest that influenza vaccines can be safely administered, evento patients with a history of anaphylaxis to egg ingestion. (B)
Most studies on influenza vaccine in patients with egg allergyhave specifically included patients with histories of anaphylaxisto egg ingestion.52,54,55,57,58 The number of such patients now col-lectively reported is 185, about 13% of the total population of pa-tients with proved egg allergy studied. These patients with severeegg allergy have tolerated the vaccine without serious reactions,as is the case with patients with less severe egg allergy.Summary Statement 17: Skin testing (prick, intradermal,
or both) with the influenza vaccine itself in patients with eggallergy (but without a history of reacting to the vaccine itself)does not reliably identify patients who are at increased risk ofreacting to the vaccine and is not recommended. (A)In studies in which vaccine skin testing was done because of a
history of egg allergy, vaccinated patients with skin test resultshad no reactions or no greater rate of reactions than subjects withnegative skin test results.52,53,55,57,58 In one study the vaccine waswithheld from patients with positive prick or intradermal vaccineskin test results.53 However, skin testing was later removed fromthe protocol; all patients were vaccinated, and the rate (low) of re-actions (minor) was the same as when skin testing had been in-cluded in the protocol. The authors concluded that vaccine skintesting was unnecessary.53
Skin testing is of utility in evaluation of a patient with a historyof an allergic reaction to the influenza vaccine itself and isaddressed in another section of this parameter and below.
Summary Statement 18: Influenza vaccine can be adminis-tered as a single dose to patients with egg allergy. (B)
In those studies of influenza vaccine in patients with egg allergythat have divided the dose (first administering 10% and, if noreaction in 30 minutes, the administering the remaining 90%), thevast majority of patients ultimately tolerate the entire dose,52-58
and studies administering the vaccine as a single dose also reportno serious reactions.54,55,57,58 The CDC and AAP have concludedthat persons who have experienced only hives after exposure toegg should receive influenza vaccine and that in these patientsvaccine skin testing and dividing the dose are no longer necessaryor recommended.51,132
In those patients with a history of more severe reactions to eggingestion, the CDC and AAP recommend that before receipt ofvaccine, such persons should be referred to an allergy special-ist.51,132 Studies support the single-dose approach, even in thesepatients with severe egg allergy. Collectively from among thesestudies, 185 patients with a history of anaphylaxis to egg ingestion
TABLE VII. (Continued)
Study Year MethodNo. ofsubjects
Mean age(range [y])
Patients withhistory of
anaphylaxis toegg ingestion
Vaccine(maximumovalbumin
content, mg per0.5 mL dose) Protocol*
No. (%) ofsystemicreactions(skin only)
No. (%) ofsystemicreactions
(respiratory,cardiovascular,gastrointestinal,
or other)
No. (%)treatedwith
epinephrine
14 controlsubjects
NR 2 (14) 0 0
Webbet al58
2011 Retrospective 152 with eggallergy
3 (0.6-30) 34 TIV and H1N1(0.7)
Skin pricktesting; singledose ifnegative;divided doseif positive(n 5 1)
0 0 0
NR, Not reported; URI, upper respiratory tract infection.*Divide dose: 10% of dose administered, observe for 30 minutes, and, if no reaction, 90% of dose administered.
TABLE VIII. Ovalbumin content of injectable TIVs approved for
the 2011-2012 season
Brandname Manufacturer
Approvedages
Ovalbumincontent (mg per0.5 mL dose*)y
Afluria CSL Biotherapies (Merck) >_9 y <_1Fluarix GlaxoSmithKline >_3 y <_0.05FluLaval ID Biomedical Corporation
of Quebec (GlaxoSmithKline)>_18 y <_1
Fluvirin Novartis >_4 y <_1Fluzone Sanofi Pasteur >_6 mo ;0.1Fluzone
High-DoseSanofi Pasteur >_65 y ;0.1
*Dose: 0.25 mL, 6-35 months; 0.5 mL, >_3 years.!Information in package inserts except Fluzone and Fluzone High-Dose from SanofiPasteur by telephone (1-800-822-2463) or e-mail ([email protected]).
J ALLERGY CLIN IMMUNOL
JULY 2012
38 KELSO ET AL
Otheraddi,ves,suchaslatexand2-phenoxyethanol,mayalsobeimportant(NagaoM,etal.JACI2016;137:861.)�

Adversereac,onstovaccinesprac,ceparameter2012update
NichlasRA,etal.JACI2012;120:25.�
immediately available to promptly treat an anaphylactic reactionshould it occur.79 Such challenges can be performed in an office orhospital setting with or without an intravenous line in place, de-pending on the severity of the original reaction to the vaccineand the patient’s medical condition.79
As above, for patients with a history of a suspected allergicreaction to the influenza vaccine itself, evaluation as per Fig 1 isappropriate. This differs from the approach to patients with a his-tory of reactions to the ingestion of egg but no history of a reactionto influenza vaccination. Recommendations regarding the ad-ministration of influenza vaccine to recipients with egg allergyare specifically addressed in an addendum at the end of thispractice parameter.Summary Statement 10: Some nonanaphylactic reactions
to vaccines might also require evaluation, but only a few areabsolute contraindications to future doses. (B)In addition to anaphylactic reactions, some vaccines are
capable of causing other rare but serious reactions that mightcontraindicate the administration of future doses.11
The ‘‘swine flu’’ influenza vaccine administered in 1976 wasassociated with an increased risk for Guillain-Barr!e syndrome(GBS), which was estimated at 1 additional case per 100,000vaccinations (over the annual background rate of 1 to 2 cases per100,000 adults).83 In subsequent years, influenza vaccines havebeen carefully monitored for this possible adverse effect andhave shown no consistent increased risk. If there is any increasedrisk, it is on the order of 1 per million.83,84 A low level of GBScases continues to be reported in temporal association with previ-ous influenza infection85,86 and with influenza and other vac-cines.87,88 Specific attention was paid to the potential for GBSafter the 2009 pandemic influenza A (H1N1) vaccine campaign,and no increased rate was found.89,90 Persons with GBS within6 weeks of influenza vaccination should avoid subsequent immu-nization with influenza vaccines.83 However, patients with a his-tory of GBS unrelated to influenza infection or vaccination whowould benefit from immunization can be vaccinated, particularlyif the influenza infection risk is high.83
MMR vaccines can cause adverse reactions related to the liveviruses they contain. Transient rashes appear in as many as 5% ofrecipients of measles vaccine, and this probably representsvaccine-induced modified measles.32 There is a late-onset feveroccurring 5 to 12 days after vaccine administration in as manyas 15% of recipients of the MMR vaccine.32,50,91 As with any fe-ver in young children, this increases the risk of febrile seizures;however, such seizures do not have any sort of long-term seque-lae.92,93 For reasons that are not clear, when the MMR is givenin a combination vaccine with varicella (ie, measles, mumps, ru-bella, and varicella vaccine), there is a 2-fold higher risk of febrileseizures than if the MMR and varicella vaccines are given as
separate injections at the same visit (one additional febrile seizureper 2500 children vaccinated).94 This increased risk exists onlyfor the first dose of the vaccines, which is typically given between12 and 15 months of age, and not for the second dose, which istypically given between 4 and 6 years of age. For this reason,the preferred strategy is to administer theMMR and varicella vac-cines as separate injections at the same visit for the first dose andcombined as measles, mumps, rubella, and varicella vaccine forthe second dose.94 Recipients of the MMR vaccine can alsohave thrombocytopenia, which is usually without any significantclinical consequence but can rarely cause hemorrhage.26,91,95,96
The rate of thrombocytopenia is much higher with the measlesdisease itself.91 Rubella vaccine can cause acute arthritis in ap-proximately 15% of adult women who receive the vaccine.35,97
This might represent a direct infection of the joints by the vaccinevirus but has a questionable association with chronic arthritis.35,97
Rubella vaccine can also cause transient arthralgia in children.None of these events are contraindications to the administrationof subsequent doses of MMR vaccine.11
The most serious adverse effect related to pertussis vaccine istermed encephalopathy. This term describes a specific and quitesevere reaction characterized as an ‘‘acute, severe CNS [centralnervous system] disorder occurring within 7 days followingvaccination and generally consisting of major alterations inconsciousness, unresponsiveness, generalized or focal seizuresthat persist more than a few hours, with failure to recover within24 hours.’’26 The estimated additional risk of this event attributedto the vaccine is 0 to 10 per million doses of diphtheria and tetanustoxoids and whole-cell pertussis (DTP) vaccine.91 This can havepermanent neurologic sequelae and is an absolute contraindica-tion to further pertussis vaccination (including acellular pertus-sis).11 Pertussis vaccine can cause less severe apparentneurologic events, including febrile seizures,92 inconsolable cry-ing,50 and hypotonic-hyporesponsive episodes.98 Although theseare clearly concerning episodes for parents to witness, none ofthem result in permanent sequelae, and none of them are contra-indications to further doses of these vaccines.11,91,99 Of note is thefact that all these serious and less serious neurologic events afterpertussis-containing vaccines have been significantly reducedsince changing from DTP to the DTaP.34,50,99-103
About 5% of immunizations with tetanus toxoid–containingvaccines cause large local swelling at the injection site.104,105 Thisprobably represents an Arthus reaction in patients with preexist-ing IgG anti-tetanus antibodies from prior immunizations whothen receive a large injection of antigen in the vaccine. These re-actions can cause discomfort but are not serious. Because of in-creasing rates of pertussis in adolescents and adults, newvaccines were recommended in 2006 for those 11 to 64 years ofage to provide not only booster doses for tetanus and diphtheria(Td) but also pertussis (Tdap).104,106 The recommended intervalbetween doses of Td had been 10 years, with shorter intervalsthought to be associated with increased rates of Arthus reactions.However, in a recent study the rate of Tdap injection-site reactionswas the same in patients who had received Td less than 2 yearspreviously or more than 2 years previously.107 Another studyfound no higher rates of injection-site reactions whether a Tdap-containing vaccine was administered 1 month after a Td-containing vaccine or placebo.108 Thus with the pertussis diseaseburden continuing to be substantial, it is now recommended thatTdap be given to all adolescents and adults (including those >_65years of age), regardless of the interval since the last Td.109
TABLE V. Administration of vaccines in graded doses
For a vaccine in which the full normal dose volume is 0.5 mL, give thefollowing doses at 15-minute intervals as tolerated*:
0.05 mL 1:10 dilution0.05 mL full-strength0.1 mL full-strength0.15 mL full-strength0.2 mL full-strength
*Must be done under direct medical supervision prepared with emergencymedications and equipment to promptly treat an anaphylactic reaction should it occur.Observe for at least 30 minutes afterward.
J ALLERGY CLIN IMMUNOL
JULY 2012
34 KELSO ET AL
Ifvaccineorvaccinecomponentskintestresultsareposi,ve,thevaccinemights,llbeadministered,ifnecessary,ingradeddoses.
Changeingela,ncontentofvaccinesassociatedwithreduc,oninreportsofallergicreac,ons
ReportfromJapan.NakayamaT,AizawaC.JACI2000;106:591.�
592 Nakayama and Aizawa J ALLERGY CLIN IMMUNOLSEPTEMBER 2000
ing urticaria with mild wheezing, was reported afteradministration of mumps vaccine containing Prionex.IgE antibodies against gelatin were borderline, and thestimulation index was 1.92 when lymphocytes werestimulated with native bovine gelatin. We could notexamine the comparative tests for native bovine gelatinand modified porcine gelatin in this case. When other IgEantibody–positive sera were used, modified porcinegelatin showed low binding activity less than one tenth ofnative bovine gelatin. We speculate that the use of modi-fied porcine gelatin decreases the reactivity but that themajor reason for the reduction of the cases with gelatinallergy is discontinuation of gelatin-containing DTaP.Infants are no longer being sensitized by DTaP because itno longer contains gelatin.
REFERENCES
1. Kelso JM, Jones RT, Yunginger JW. Anaphylaxis to measles, mumps, andrubella vaccine mediated by IgE to gelatin. J Allergy Clin Immunol1993;91:867-72.
2. Sakaguchi M, Ogura H, Inouye S. IgE antibody to gelatin in childrenwith immediate-type reactions to measles and mumps vaccines. J. Aller-gy Clin Immunol 1995;96:563-5.
3. Sakaguchi M, Yamanaka T, Ikeda K, Sano Y, Fujita H, Miura T, et al. Sys-temic immediate-type reactions including anaphylaxis to gelatin in vari-cella vaccine. J Allergy Clin Immunol 1997;99:263-4.
4. Nakayama T, Aizawa C, Kuno-Sakai H. A clinical analysis of gelatinallergy and determination of its causal relationship to the previous admin-istration of gelatin-containing acellular pertussis vaccine combined withdiphtheria and tetanus toxoids. J Allergy Clin Immunol 1999;103:321-5.
TABLE I. Incidence of allergic reactions after live attenuated vaccines with different gelatin materials from June 1994to December 1999
Measles vaccine Mumps vaccine Rubella vaccine
Allergic reactions Bovine* Porcine† Bovine* Porcine† Bovine* None‡
Anaphylaxis 18 (11) 0 (–) 17 (24) 1 (8) 9 (4) 0 (–)Urticaria 64 (38) 1 (2) 22 (31) 0 (–) 9 (4) 0 (–)Eruption 178 (107) 2 (4) 48 (69) 0 (–) 76 (37) 5 (15)No. of doses shipped (in millions) 1.67 0.47 0.70 0.13 2.05 0.33
Numbers in parentheses reveal the rate of reported reactions per million doses of vaccine shipped. We analyzed the data obtained from June 1994 to December1999.*Native bovine gelatin was used at a concentration of 0.2% as a stabilizer until August 1998.†Hydrolyzed modified porcine gelatin (Prionex) was used at a concentration of 0.2% as stabilizer from September 1999.‡Neither gelatin nor human serum albumin was used as a stabilizer since July 1999.
• Overview
• TrendsinJapan
• Basisofdesensi,za,onprocedure
• Whatneedstobekeptinmind?�
Fatal anaphylaxis in Japan�
2001� 2002� 2003�2004�2005�2006�2007�2008�2009�2010� 2011� 2012�2013� total�
Total� 58� 53� 53� 46� 73� 66� 66� 48� 51� 51� 71� 55� 77� 768�Bee/wasp
stings 26� 23� 24� 18� 26� 20� 19� 15� 13� 20� 16� 22� 24� 266�
Foods 3� 0� 3 2� 1� 5� 5� 4� 4� 4� 5� 2� 2� 40�Drugs 17� 17� 19� 19� 31� 34� 29� 19� 26� 21� 32� 22� 37� 323�Serum� 0� 0� 1� 0� 1� 1� 1� 0� 1� 0� 0� 0� 1� 6�
Unknown� 12� 13� 6� 7� 14� 6� 12� 10� 7� 6� 18� 9� 13� 133�
Data from Ministry of Health, Labor and Welfare of Japan�
Antibiotics�&penicillin�&cephem�&calbapenem�&quinolone &others� Radiocontrast media�&X-ray�&MRI �Aspirin and NSAIDs�Local analgetics�Others�
Reported severe, hospitalized cases of drug-induced anaphylaxis �
33 (36%) 1 20 3 7 2 �27 (29%) 25 2 �16 (17%) 11 (12%)
34 (36%) 4���12 0���15����3��29 (30%) 28����1��11 (11%) 5 ( 5%) 20
2005 ""92 cases�
2012 ""98 cases�
Data from remedial office in Pharmaceuticals and Medical Devices Agency, Japan�
Survey of anaphylaxis patients from 2005 to 2015 (a hospital in Yokohama)
Total 387 cases (<15 y.o. 218 cases, >= 15 y.o. 169 cases) In patients >= 15 y.o., various triggers were observed 56.8% foods, 24.3% drugs, 13.0% insect stings
Among these patients, 43.9% NSAIDs 29.3% antibiotics 9.8% drugs for common cold
Nakamura Y, et al. Allergy & Immunology(in Japanese) 23(11):1536,2016�
• Overview
• TrendsinJapan
• Basisofdesensi,za,onprocedure
• Whatneedstobekeptinmind?�
“A New Era for Drug Desensitizations” Rapid drug desensitization (RDD) protocols address type I reactions with mast cell/ basophils/IgE involvement, and slow drug desensitization protocols address delayed type IV reactions with T-cell involvement. �
Castells MC. JACI Pract 3: 639, 2015.
Usually, very tiny starting dose; then 2-fold increase every 15 minutes; full dose is achieved in the same day
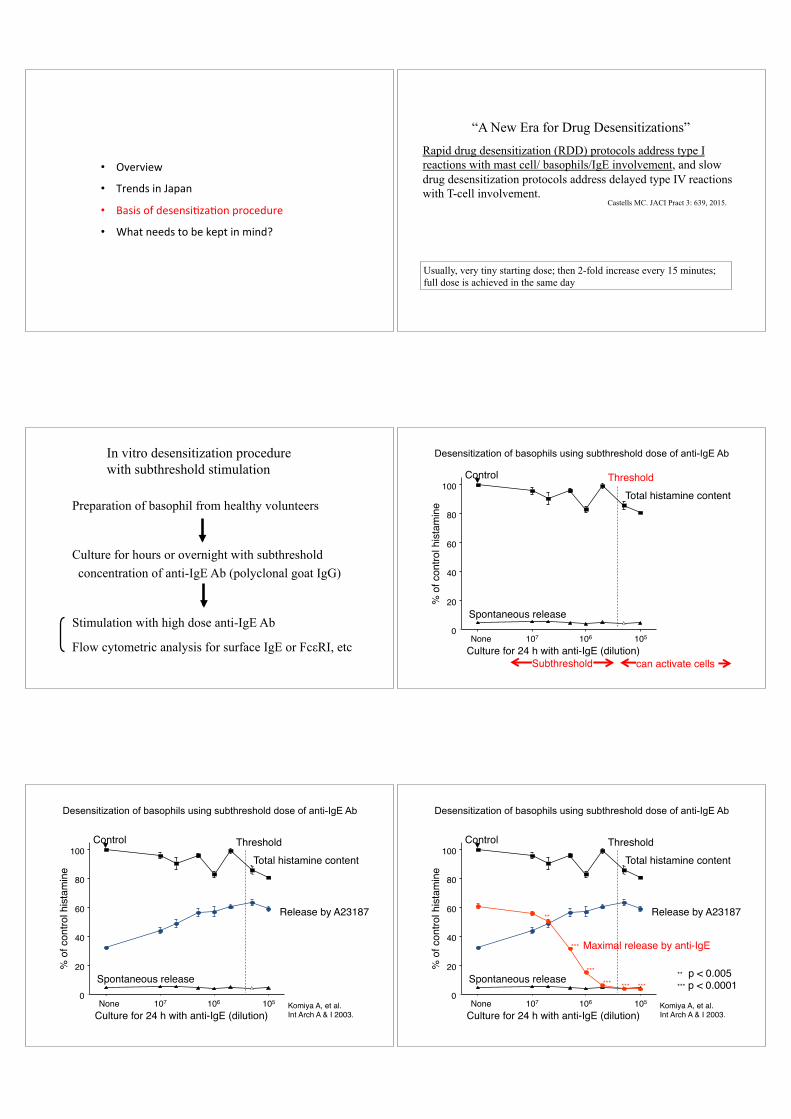
Preparation of basophil from healthy volunteers
Culture for hours or overnight with subthreshold concentration of anti-IgE Ab (polyclonal goat IgG)
Stimulation with high dose anti-IgE Ab
Flow cytometric analysis for surface IgE or FcεRI, etc�
In vitro desensitization procedure with subthreshold stimulation
Desensitization of basophils using subthreshold dose of anti-IgE Ab�
Total histamine content"
Culture for 24 h with anti-IgE (dilution)"
% o
f con
trol h
ista
min
e"
Spontaneous release"0"
20"
40"
60"
80"
100"
105"107" 106"None"
Control Threshold"
Subthreshold" can activate cells"
Release by A23187"
Total histamine content"
Culture for 24 h with anti-IgE (dilution)"
% o
f con
trol h
ista
min
e"
Spontaneous release"0"
20"
40"
60"
80"
100"
105"107" 106"None"
Control Threshold"
Komiya A, et al."Int Arch A & I 2003."
Desensitization of basophils using subthreshold dose of anti-IgE Ab�
Release by A23187"
Maximal release by anti-IgE"
Total histamine content"
Culture for 24 h with anti-IgE (dilution)"
% o
f con
trol h
ista
min
e"
Spontaneous release"0"
20"
40"
60"
80"
100"
105"107" 106"None"
Control
**"
***"***"***"
***"
***"
Threshold"
** p < 0.005"*** p < 0.0001"
Komiya A, et al."Int Arch A & I 2003."
Desensitization of basophils using subthreshold dose of anti-IgE Ab�

Desensitized basophils are morphologically the same�
Day 0� Day 1 non-desensitized�
Day 1 desensitized�
before stimutation�
after stimutation with high-dose anti-IgE Ab�
Komiya A, et al. Int Arch A & I 2003."
These results indicate:
Basophil desensitization can occur without degranulation in the presence of subthreshold anti-IgE Ab This process seems to: need a few hours require physiological medium disappear after a few days in the absence of Ab Precise mechanism(s) are unknown.�
High dose allergen
Ag!
Ag!
Ag!
Ag!
Ag!
Immediate activation�
Ag!
Basophils (& Mast cells)
Modified from : Suzukawa M, et al. Int Arch Allergy Immunol 143S:56,2007.
Ag!
Basophils (& Mast cells)
Desensitization limits cell activation
Very low dose allergen�
Ag!
Little or no activation�
Basophils (& Mast cells)
Modified from : Suzukawa M, et al. Int Arch Allergy Immunol 143S:56,2007.
High dose allergen High dose allergen
Ag!
Ag!
Ag!
Ag!
Ag!
Immediate activation�
Ag!
Basophils (& Mast cells)
IgE-mediated stimulation High low
Direct activation
Desensitization
Suppression
Desensitization and challenge test procedures may be explained by the interaction between the two phenomena
• Overview
• Trends in Japan
• Basis of desensitization procedure
• What needs to be kept in mind?�

Figure 1. Comparison of radioallergosorbent test and basophil activation test survival analysis during a follow-up period of 4 years.�
Blood tests may covert to negative after anaphylaxis to amoxicillin�
Fernández TD, et al. Allergy 64: 242, 2009. �
BAT: basophil activation test�
Figure 3. Comparison of the survival analysis in patients with (Group I) or without (Group II) skin tests during the study in both radioallergosorbent test (A) and basophil activation test (B). �
Skin test affects the results of blood test; consider the necessity of tests�
Fernández TD, et al. Allergy 64: 242, 2009. �
Antibiotics allergy: skin test threshold vs. usual dose �
g
pg
ng
µg
mg
usual dose, total �
usual dose per min �
intradermal test � threshold dose of intradermal test in patients with antibiotics anaphylaxis is variable
fg
initial dose for skin test �
skin prick test�
For patients with drug anaphylaxis �
Perform in vivo tests very carefully! �