Embed Size (px)
Citation preview

Universidade Federal de São Paulo Pró-Reitoria de Extensão
1
Ata da reunião ordinária da Comissão de Residência Médica da UNIFESP
Aos dezesseis de maio de dois mil e doze, às oito horas na cidade de São Paulo, Rua 1
Pedro de Toledo n.º 781, Edifício Horácio Kneese de Melo, Anfiteatro Octávio Ribeiro 2
Rato, reuniu-se ordinariamente a Comissão de Residência Médica - COREME, sob a 3
coordenação do Professor Doutor Gilmar Fernandes do Prado, com a participação dos 4
membros da COREME. Presentes: Dra. Márcia Lika Yamamura; Dr. Alessandra Rolla; 5
Prof. Dr. Masashi Muneshika; Dra. Ana Laura A. Giraldes; Dr. Vinícius Fontanese Blum; 6
Dra. Daiane P. Guimarães; Dr. Flávio Augusto Vercillo Luisi; Dr. Carlos Haruo Arasaki ; 7
Prof. Dr. Sarhan Sydney Saad; Dr. Frederico Teixeira Barbosa; Profa. Dra. Maris Salete 8
Demuner; Dr. Alexandre Alberto Barros Duarte; Prof. Dr. Luiz Hirotoshi Ota; Dra. Erika 9
Rymkiewicz; Prof. Dr. Fausto Miranda Junior; Dra. Thais Ioshimoto; Dra. Katia Emi 10
Nakaema; Profa. Dra. Silmara da Costa Pereira Cestari; Prof. Dr. Orlando Ambrogini 11
Junior; Dra. Ana Cristina Fontenele Soares; Dra. Fernanda Teresa de Lima; Prof. Dr. 12
Eduardo Canteiro Cruz; Prof. Dr. Celso Francisco Hernandes Granato; Dra. Vanessa 13
Monteiro Sanvido; Dr. Ivaldo da Silva; Dr. Marcelo Marcos Piva Demarzo; Dra. Renata 14
Teixeira Ladeira; Dra. Cintia Camargo Dias; Prof. Dr. João Tomas de Abreu Carvalhaes; 15
Prof. Dr. Ítalo Craparo Soriano; Prof. Dr. Deusvenir de Souza Carvalho; Prof. Dr. Luiz 16
Celso Pereira Vilanova; Profa. Dra. Marair Gracio Ferreira Sartori; Dr. Pedro Venalle 17
Ferrari ; Prof. Dr. João Baptista Gomes dos Santos; Dr. Carlos Eduardo da Silveira 18
Franciozi; Prof. Dr. Adagmar Andriolo; Dr. Carlos Eduardo dos Santos Ferreira; Dra. 19
Renata Cavalcante Kuhn dos Santos; Dra. Maria Aparecida Gadiani Ferrarini; Profa. Dra. 20
Marina C. M. Barros; Dr. Humberto Bracco Neto; Dr. Meyer Izbicki; Profa. Dra. Ana 21
Cristina Chaves; Profa. Maria Conceição do Rosário; Dr. Henrique Carrete Júnior; Sra. 22
Andrea Puchnick; Dr. Rodrigo Souza Dias; Prof. Dr. Milton H. Miyoshi; Dr. Rodrigo 23
Perrella; e Dra. Maria Elizabeth M. Rezende. Ausentes: Dra. Beatriz Tavares Costa 24
Carvalho; Prof. Dr. Antônio Carlos de Camargo Carvalho; Prof. Dr. João Nelson Rodrigues 25
Branco; Dr. Nicolau Granado Segre; Prof. Dr. Onivaldo Cervantes; Prof. Dr. Alcides 26
Augusto Salzedas Netto; Prof. Dr. Luiz Eduardo Felipe Abla (Guará); Dra. Letícia Sandre 27

Universidade Federal de São Paulo Pró-Reitoria de Extensão
2
Vendrame; Dra. Angela Spinola e Castro; Prof. Dr. Otavio César Carvalho G. Baiocchi; 28
Dra. Josefina A P Braga; Prof. Dr. Ademir Baptista da Silva (Medicina do Tráfego); Prof. 29
Dr. Moisés Cohen; Profa. Dra. Therezinha Rosane Chamlian; Dr. Nilton Ferraro Oliveira; 30
Prof. Dr. Oscar Fernando Pavão dos Santos; Prof. Dr. José Osmar Medina Pestana; Dra. 31
Maria Fernanda Branco de Almeida; Profa. Dra. Shirley Shizue N. Pignatari; Prof. Dr. 32
Rimarcs Gomes Ferreira; Dr. Gilberto Petty da Silva; Dr. Ektor Tsuneo Onishi; e Prof. Dr. 33
Daniel Feldman. Ausência Justificada: Dra. Elaine Cristina Soares Martins, Prof. Dr. 34
João Aléssio Juliano Perfeito, Prof. Dr. João Roberto de Sá, Dr. Domingos Palma, Dra. 35
Fernanda Luisa Ceragioli Oliveira e Profa. Dra. Ilka Lopes Santoro. INFORMES: 1. Novos 36
membros da COREME: O Prof. Gilmar iniciou a sessão informando os membros que 37
justificaram ausência nesta Plenária e apresentando os novos integrantes da COREME 38
(anexo). Em seguida, o Prof. Gilmar abordou o 2. Cronograma do Processo Seletivo 2013 39
(Questões da prova até 18/05/2012), ressaltando algumas datas e dados pertinentes à 40
organização das provas teóricas e prática, bem como das entrevistas. O Prof. João 41
Tomas, Nefrologia Pediátrica, sugeriu que, ao invés de uma simples carta do Supervisor 42
do PRM de origem, que sejam estabelecidos critérios claros para a entrevista. A Profa. 43
Maris, Cirurgia Pediátrica/Unidades Afiliadas, acrescentou que qualquer documento que 44
se peça, venha, obrigatoriamente, com a assinatura (ciência) do Coordenador da 45
COREME de origem. O Prof. Sérgio, Cancerologia Pediátrica, solicitou que o Cronograma 46
do Processo Seletivo seja encaminhado por e-mail aos supervisores dos PRMs. O Prof. 47
Gilmar respondeu que o pedido será atendido. 3. Artigo “Avoiding Bournout”: A Dra. 48
Erika, Cirurgia Torácica, comentou o artigo (anexo). Falou sobre detalhes da pesquisa e 49
das inferências obtidas a partir do estudo. O Prof. Gilmar finalizou ressaltando um dado 50
apontado no artigo, também comentado pela Dra. Erika: uma parte dos pesquisados, 51
mesmo apresentado rotina de trabalho mais estressante que outros do grupo, 52
apresentavam-se em melhores condições de saúde, pois são cirurgiões com real 53
afinidade/vocação ao treinamento em cirurgia. O Prof. Haruo, Cirurgia do Aparelho 54
Digestivo, perguntou sobre a pertinência da apresentação do artigo na Plenária. O Prof. 55
Gilmar respondeu que se propõe à formação dos preceptores, quanto à afinidade dos 56
médicos em relação ao treinamento escolhido, e que os preceptores devem também 57
pensar na própria saúde, o que permite refletirem melhor sobre a saúde dos Médicos 58
Residentes (MR) que coordenam (“... Because of associations between personal health habits and 59

Universidade Federal de São Paulo Pró-Reitoria de Extensão
3
the care physicians provide their patients4–7, as well as the potential for poor health to result in premature 60
exit from practice, 3 hospitals, health maintenance organizations, academic medical centers, physician 61
societies, and officials responsible for promoting public health, should also consider howthey can help 62
surgeons maintain health and resilience...”. Vide Anexo, Grifado e com setas). 4. Psiquiatria da Infância 63
e da Adolescência: O Prof. Gilmar, respondendo ao solicitado pelos membros na última 64
plenária, informou que é válido (confirmado pela AMB) o Título de Especialista em 65
Psiquiatria apresentado por médica que cursou residência médica em Psiquiatria da 66
Infância e da Adolescência sem ter o pré-requisito de Residência Médica em Psiquiatria. 67
Lembrou que a COREME ainda aguarda posicionamento da Comissão Nacional de 68
Residência Médica (CNRM) quanto ao registro, para a referida médica, do certificado da 69
área de atuação cursada. 5. Vistoria no PRM de Acupuntura: O Prof. Gilmar fez um breve 70
comentário sobre os objetivos das vistorias internas e, em seguida, passou a palavra ao 71
Prof. Haruo, Cirurgia do Aparelho Digestivo, para falar dos trabalhos de vistoria no PRM 72
de Acupuntura. O Professor falou que a principal queixa dos médicos residentes do 73
programa diz respeito à infraestrutura (instalações, espaço físico etc). Acrescentou ainda 74
que é preciso aumentar a titulação de docentes na área. Em seguida, o Prof. Meyer, 75
Pneumonologia, comentou que o Projeto Pedagógico do Curso dá ênfase aos aspectos 76
da medicina chinesa, e que os MR do programa percebem que necessitam de maior 77
envolvimento com o diagnóstico clínico tradicional. O Dr. Vinícius, Coordenador das 78
Comissões de Vistorias, finalizou agradecendo o empenho dos vistoriadores (Dr Haruo – 79
Cirurgia do Aparelho Digestivo; Dr Meyer – Pneumologia; Dra Thais – 80
Neurologia/Cefaléia). O Prof. Gilmar aproveitou para comentar sobre Edital da CEREM-81
SP sobre seleção de vistoriadores. A Profa. Márcia falou do diferencial do PRM de 82
Acupuntura da UNIFESP em relação aos de outras instiuições, sendo exatamente o fato 83
de dar ênfase aos princípios da Medicina Chinesa que leva este PRM a ser bastante 84
concorrido. O Prof. Haruo sugeriu algumas alterações no formulário de vistorias, que 85
foram acatadas pelo Dr. Vinícius. 6. Pagamento de atividades referente ao Processo 86
Seletivo 2012: O Prof. Gilmar falou sobre os critérios de pagamento para servidores e 87
alertou para os prazos que, depois de esgotados, implicarão em não pagamento para os 88
que não os respeitaram. 7. Projeto Matriciamento: O Prof. Ivaldo deu detalhes sobre a 89
problemática envolvendo o pagamento de viagens para servidores participantes do 90
programa, o que tem impedido a formalização/finalização do contrato. O principal 91
problema, disse, é o teto para emissão de passagens estabelecido pelo Ministério do 92

Universidade Federal de São Paulo Pró-Reitoria de Extensão
4
Planejamento, impedindo que as passagens sejam emitidas pelo sistema comum. Falou 93
de detalhes do Projeto Matriciamento e esclareceu dúvidas dos presentes. 8. Ano 94
Opcional de Ginecologia e Obstetrícia: O Prof. Gilmar falou sobre os males entendidos 95
gerados pelas informações constantes no Edital do Processo Seletivo da Residência 96
Médica 2012, quanto à oferta de “ênfases” no Ano Opcional de Ginecologia e Obstetrícia. 97
O Prof. Gilmar informou aos presentes sobre os esclarecimentos prestados pela 98
COREME-UNIFESP à Comissão Nacional de Residência Médica. 9. Curso para 99
Preceptores: O Dr. Vinícius falou sobre como o curso está sendo organizado e, na 100
próxima plenária, trará a proposta já finalizada. ORDEM DO DIA: 1. Modelo de Avaliação: 101
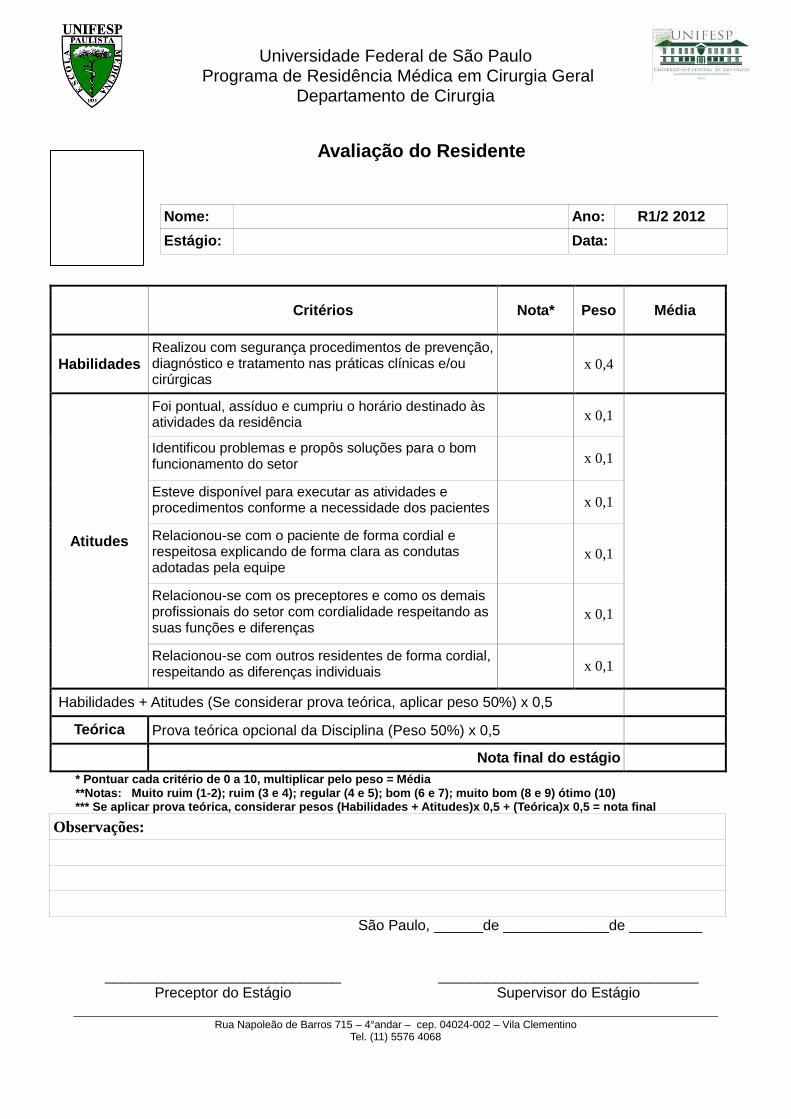
Com a palavra, o Dr. Frederico, Preceptor da Cirurgia Geral, falou sobre os estágios do 102
R1 e R2 do PRM. Comentou sobre detalhes da avaliação dos residentes, cujos resultados 103
são condensados em um formulário (modelo anexo) preenchido pelos preceptores do 104
PRM. As Professoras Dra. Marina, Pediatria, e Profa. Maris, Cirurgia Pediátrica, falaram 105
de procedimento similar desenvolvido por seus PRMs. O Prof. Gilmar ressaltou a 106
importância da avaliação e parabenizou o trabalho dos PRMs que se manifestaram. Em 107
seguida, houve discussão sobre a eficácia do modelo apresentado pelo Dr. Frederico, que 108
respondeu aos questionamentos dos presentes. Uma das críticas apresentadas diz 109
respeito às peculiaridades do estágio no Pronto Socorro, não contempladas pelo modelo. 110
O Prof. Ítalo, Neurocirurgia, acrescentou que várias das situações previstas no modelo de 111
avaliação apresentado pelo Dr. Frederico estão fora do centro cirúrgico e que, portanto, 112
podem ser avaliadas pelos chefes de cirurgia. O Prof. Gilmar finalizou sugerindo meios 113
de adequar o modelo de avaliação ao PS. A Profa. Maria da Conceição, Psiquiatria da 114
Infância e da Adolescência, reforçou elementos que devem ser adequados no modelo de 115
avaliação proposto pelo Dr. Frederico. 2. PRM de Medicina Física e Reabilitação – 116
Problema com residente matriculado sob nº. 59230: O Prof. Gilmar falou de detalhes do 117
caso, que abrangem, inclusive, supostas falta ética e outras transgressões. A Profa. Maria 118
da Conceição, Psiquiatria da Infância e da Adolescência, falou que é possível a existência 119
de outros casos e que a COREME deve prever como tratar médicos residentes com 120
problemas de convivência. Ao final da discussão, a plenária decidiu encaminhar o caso do 121
referido residente à Procuradoria Geral da UNIFESP e à Comissão de Ética Médica. 122
Encerrados os assuntos, o Prof. Gilmar encerrou a sessão e eu, Alessandra Aparecida da 123

Universidade Federal de São Paulo Pró-Reitoria de Extensão
5
Silva Menezes, lavrei a presente ata que será assinada pelo Coordenador da Comissão 124
de Residência Médica. 125
126
PROF. DR. GILMAR FERNANDES DO PRADO Coordenador da Comissão de Residência Médica – COREME
Escola Paulista de Medicina – EPM Universidade Federal de São Paulo - UNIFESP
ANEXOS:
- Artigo: “Avoiding Bournout”;
- Novos Membros da COREME;
- Cronograma do Processo Seletivo 2013
- Modelo de Formulário de Avaliação de Médico Residente – Cirurgia

FEATURE
Avoiding BurnoutThe Personal Health Habits and Wellness Practices of US Surgeons
Tait D. Shanafelt, MD,∗ Michael R. Oreskovich, MD,† Lotte N. Dyrbye, MD,∗ Daniel V. Satele,‡John B. Hanks, MD,§ Jeff A. Sloan, PhD,‡ and Charles M. Balch, MD¶
Objective: To evaluate the health habits, routine medical care practices, andpersonal wellness strategies of American surgeons and explore associationswith burnout and quality of life (QOL).Background: Burnout and low mental QOL are common among US surgeonsand seem to adversely affect quality of care, job satisfaction, career longevity,and risk of suicide. The self-care strategies and personal wellness promotionpractices used by surgeons to deal with the stress of practice are not wellexplored.Methods: Members of the American College of Surgeons were sent ananonymous, cross-sectional survey in October 2010. The survey includedself-assessment of health habits, routine medical care practices, and personalwellness strategies and standardized assessments of burnout and QOL.Results: Of 7197 participating surgeons, 3911 (55.0%) participated in aero-bic exercise and 2611 (36.3%) in muscle strengthening activities, in a patternconsistent with the Centers for Disease Control and Prevention recommen-dations. The overall and physical QOL scores were superior for surgeons’following the Centers for Disease Control and Prevention recommendations(all P < 0.0001). A total of 3311 (46.2%) participating surgeons had seentheir primary care provider in the last 12 months. Surgeons who had seentheir primary care provider in the last 12 months were more likely to be up todate with all age-appropriate health care screening and had superior overalland physical QOL scores (all P < 0.0001). Ratings of the importance of 16personal wellness promotion strategies differed for surgeons without burnout(all P < 0.0001). On multivariate analysis, surgeons placing greater emphasison finding meaning in work, focusing on what is important in life, maintaininga positive outlook, and embracing a philosophy that stresses work/life balancewere less likely to be burned out (all P < 0.0001). Although many factorsassociated with lower risk of burnout were also associated with achieving ahigh overall QOL, notable differences were observed, indicating surgeons’need to employ a broader repertoire of wellness promotion practices if theydesire to move beyond neutral and achieve high well-being.Conclusions: This study identifies specific measures surgeons can take todecrease burnout and improve their personal and professional QOL.
(Ann Surg 2012;255:625–633)
M aintaining a surgeon workforce adequate to meet societal needsrequires that both an adequate number of surgeons be trained
and premature exit from practice be prevented. Although evidencesuggests that physicians have healthier lifestyles and lower mortalitythan the general public,1,2 a 25-year single-institution cohort study
From the ∗Department of Medicine, Mayo Clinic, Rochester, MN; †Departmentof Psychiatry, University of Washington, Seattle, WA; ‡Department of HealthSciences Research, Mayo Clinic, Rochester, MN; §Department of Surgery,University of Virginia, Charlottesville, VA; and ¶Department of Surgery, Uni-versity of Texas Southwestern Medical Center, Dallas, TX.
Disclosure: Funding for this study was provided by the American College of Sur-geons and the Mayo Clinic Department of Medicine Program on PhysicianWell-Being.
Reprints: Tait Shanafelt, MD, Department of Medicine, Mayo Clinic, 200 FirstStreet, Rochester, MN 55905. E-mail: [email protected].
Copyright C© 2012 by Lippincott Williams & WilkinsISSN: 0003-4932/12/25504-0625DOI: 10.1097/SLA.0b013e31824b2fa0
suggested that 50% of US surgeons experience a major health is-sue by the age of 50 years and that the length of a surgeon’s careermay be influenced by personal health issues, exercise and preven-tive health patterns, and alcohol use/dependency.3 Other data suggestthat physicians’ personal health habits (eg, alcohol use, tobacco use,exercise habits) and whether or not they are themselves up to datewith recommended health screening may affect the medical care theyprovide to their own patients.4–7 Despite these facts underscoring theimportance of attention to surgeons’ personal health practices, littleis known about the health habits and routine medical care practicesof US surgeons.
In addition to the importance of maintaining their physicalhealth, surgeons face significant challenges due to practice-relatedstress. Studies suggest that burnout, depression, and a low mentalquality of life (QOL) are common among US surgeons.8–10 Furtherevidence indicates that surgeon burnout may affect quality of care,11
job satisfaction,8 intent-to-leave practice,12 and increase the risk ofsuicidal ideation among surgeons.13 Although some of the causesof burnout have been delineated,8,14–16 the self-care strategies andpersonal wellness promotion practices used by surgeons to deal withthe stress of practice are not well explored.
In this study, commissioned by the American College of Sur-geons (ACS) Committee on Physician Competency and Health, weevaluated the personal health habits, routine medical care practices,and personal wellness strategies of US surgeons and explored asso-ciations with surgeon burnout and QOL.
METHODS
ParticipantsStudy eligibility and survey administration process were iden-
tical to our 2008 ACS study.8 All surgeons who were members of theACS, had an e-mail address on file with the college, and permittedtheir e-mail to be used for correspondence with the college were el-igible for participation in the 2010 study. Participation was electiveand all responses were anonymous. The ACS Governor’s Committeeon Physician Competency and Health commissioned the study andinstitutional review board oversight for protection of human subjectswas provided by the Mayo Clinic institutional review board.
Data CollectionSurgeons were surveyed electronically in October 2010. A
cover letter stated that the purpose of the survey was to better un-derstand the factors that contribute to satisfaction among surgeons.Participants were not informed of any specific hypothesis of the study.The survey included approximately 70 questions about a wide range ofcharacteristics, including demographic information, practice charac-teristics, burnout, mental and physical QOL, symptoms of depression,and career satisfaction. Up to 3 follow-up e-mail messages remindedsurgeons to complete the survey.
Exercise and Personal Health HabitsTo evaluate surgeons’ aerobic exercise activities and muscle
strengthening activities relative to the Centers for Disease Control and
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Annals of Surgery � Volume 255, Number 4, April 2012 www.annalsofsurgery.com | 625

Shanafelt et al Annals of Surgery � Volume 255, Number 4, April 2012
Prevention (CDC) guidelines,17 surgeons were asked to indicate (i)the number of minutes per week they engaged in moderate-intensityexercise (eg, brisk walking, riding bike on level ground, pushinglawn mower, water aerobics), (ii) the number of minutes per weekthey engaged in vigorous-intensity exercise (eg, jogging or running,riding bike on hills, swimming laps, playing basketball), and (iii)the number of times they engaged in muscle-strength training thatworked all major muscle groups (legs, hips, back, abdomen, chest,shoulders, arms). The CDC recommends that adults participate in atleast 150 minutes per week of moderate-intensity exercise, at least 75minutes per week vigorous-intensity exercise, or an equivalent mix ofmoderate- and vigorous-intensity exercise (each minute of vigorousintense exercise equivalent to approximately 2 minutes of moderatelyintense exercise).17 In addition, the CDC recommends that adultsengage in muscle strengthening activities that work all major musclegroups at least 2 times per week.17
Routine Medical Care and HealthScreening Practices
Assessment of age-appropriate health screening (ie, choles-terol assessment, colon cancer screening, prostate cancer screening[men], Papanicolaou test screening [women], and mammography[women]) were based on the US Preventative Services Task Force(USPSTF) recommendations18 and were similar to the approachesused in previously published studies of physicians.2–4,19 Physicianswere also asked whether they currently had a primary care provider,when they had last seen a primary care provider, and when they hadlast seen a dentist, using an approach similar to previous surveys.20
Personal Wellness Promotion StrategiesIn addition to evaluating exercise and medical care/health
screening habits, we also assessed surgeons’ use of personal well-ness strategies to deal with stress of medical practice. Surgeons wereasked to rate the importance of 16 specific wellness strategies re-ported in previous studies of physicians.21–26 The strategies in thesequestions explored aspects of self-care, relationships, work attitudes,religious/spiritual practice, personal philosophies, mindfulness (eg,contemplative practices, reflecting writing), and approaches to pro-mote work-life balance integration. Surgeons were asked to rate thepersonal importance of each strategy with response options of “notimportant to me,” “minimally important,” “moderately important,”or “essential.” In addition to evaluating responses on this ordinalscale, answers were also transformed to a numeric score (not impor-tant to me = 0, minimally important = 1, moderately important =2, essential = 3) to allow a mean/median ratings and rank across allresponders.
Burnout and QOLStandardized survey tools were used to assess burnout,27 phys-
ical QOL and overall QOL.28–30 Although the 22-item MaslachBurnout Inventory (MBI) is the gold standard for the assessmentof burnout,27 its length (22 items) limits feasibility for use in longsurveys addressing multiple content areas. Because many burnoutstudies have focused on the presence of high levels of either emotionalexhaustion or depersonalization as the foundation of burnout amongphysicians,31–33 symptoms of burnout in this study were assessed us-ing 2 single-item measures adapted from the full MBI. Emotionalexhaustion was assessed by asking responders to rate how often theyfelt burned out from their work. Depersonalization was assessed byasking responders to rate how often they felt they had become morecallous toward people since they took their current job. Each questionwas answered on a 7-point Likert scale, with response options rang-ing from “never” to “daily.” Symptoms of high emotional exhaustion
were defined by a frequency of feeling burned out from work of at leastonce a week and symptoms of high depersonalization were defined bya frequency of feeling more callous toward people of at least once aweek. These single items have been shown to correlate strongly withthe emotional exhaustion and depersonalization domains of burnoutas measured by the full MBI in a sample of more than 10,000 medicalstudents, residents, and practicing physicians.34 The area under thereceiver operating characteristic curve for the emotional exhaustionand depersonalization single items relative to that of their respectivefull MBI domain score in previous studies were 0.94 and 0.93 andthe positive predictive values of the single-item thresholds for highlevels of emotional exhaustion and depersonalization were 88.2% and89.6%, respectively.34
QOL in a variety of domains was measured using single-itemlinear analog self-assessment items. Linear analog self-assessmentinstruments are widely used in QOL research21,35–37 and have beenextensively validated. Each QOL domain was assessed on a 0 to 10scale, with response anchors ranging from “As bad as it can be”(0) to “As good as it can be” (10). Population-based normative datasuggest that mean scores on QOL instruments for healthy individualsare generally above 70 when scaled to a 0 to 100 range (eg, ≥7 on0–10 scale).38,39 Consistent with this approach,40 we also exploredthe characteristics of individuals with QOL scores of 8 or higher toexplore features associated with achieving a high overall QOL.
Statistical AnalysisDescriptive statistics were used to characterize sample demo-
graphics. Comparisons between surgeons’ health habits and wellnessstrategies were tested using Wilcoxon-Mann-Whitney tests and Fisherexact tests. Such comparisons with approximately 5232 and 1925 sur-geons reporting in the 2 groups have 95% power to detect an averagedifference of less than 5% of the standard deviation, a very smalleffect size.41,42 Accordingly, the P values in this report are not asimportant as the observed effect sizes. Consistent with the scienceof QOL assessment,41 we a priori defined a 0.5 SD in QOL scoresas a clinically meaningful effect size.41,42 The multivariable asso-ciations among demographic characteristics, professional character-istics, health habits, and wellness strategies with burnout and careersatisfaction were assessed using logistic regression. Both forward andbackward elimination methods were used to select significant vari-ables for the models where the directionality of the modeling did notimpact the results. All analyses were done using SAS version 9 (SASInstitute Inc, Cary, NC) or R (R Foundation for Statistical Computing,Vienna, Austria; http://www.r-project.org.).
RESULTSAt the time of the survey, there were approximately 65,844
fellows and associate fellows in the ACS of whom 27,457 had ane-mail address on record with the college and permitted use of theire-mail address for correspondence. Of these 27,457, a correct e-mailaddress could be confirmed on the initial mailing for approximately91.3% (n = 25,073), and 7197 (28.7%) eventually returned surveys.
ParticipantsThe demographic and practice characteristics of the study par-
ticipants have been previously reported. Briefly, the median age ofresponders was 53 years and 6116 (85.4%) were men. Overall, 6527(90.7%) were married and 6384 (88.9%) had children. Participatingsurgeons had been in practice a median of 20 years, worked a me-dian of 60 hours per week, and were on call a median of 2 nightsper week. General surgery (n = 2737; 38.2%) was the most com-mon subspecialty area, but all surgical specialties were represented.A majority of responders were in private practice (n = 3723), with
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
626 | www.annalsofsurgery.com C© 2012 Lippincott Williams & Wilkins

Annals of Surgery � Volume 255, Number 4, April 2012 Wellness Practices of US Surgeons
lesser numbers working in academic practice (n = 2108), at a vet-erans’ hospital (n = 161), in active military practice (n = 94), or inan “other” practice setting (n = 724). An additional 195 responders(2.8%) were retired or no longer in practice. With respect to burnout,symptoms of emotional exhaustion were reported at least weekly by1640 (22.9%) surgeons, whereas 1053 (14.9%) reported symptomsof depersonalization at least weekly. On the 0 to 10 Likert scale, themean overall QOL score was 7.3 (SD: 1.74), whereas the mean phys-ical QOL score was 6.9 (SD: 2.02) (population-based normative datasuggest that mean scores for healthy individuals are ≥7).38,39
Tobacco Use, Caffeine Use, and Exercise HabitsThe caffeine, tobacco, and exercise habits of participating sur-
geons are shown in Table 1. Only 1127 (15.8%) surgeons reportedany tobacco use in the last year, with 202 (2.8%) reporting daily use.In contrast, 6739 (94.1%) surgeons reported using caffeine in the lastyear, with 5367 (74.9%) reporting daily use.
Surgeons reported a median of 61 to 120 minutes of moderate-intensity exercise (eg, brisk walking, riding bike on level ground,pushing lawn mower, water aerobics) per week and a median of 31to 45 minutes of vigorous-intensity exercise per week (eg, joggingor running, riding bike on hills, swimming laps, playing basketball).Overall, the aerobic exercise activity of 3911 (55.0%) surgeons wasconsistent with the CDC recommendations. Surgeons engaged inmuscle strengthening activities working all major muscle groups amedian of 1 time per week, and 2611 (36.3%) surgeons engaged inmuscle strengthening activity consistent with the CDC recommenda-tions (eg, ≥2 times per week).
The mean overall (7.6 vs 7.1; P < 0.0001) and physical (7.5vs 6.1; P < 0.0001) QOL scores were superior for surgeons whoseaerobic exercise activity was consistent with the CDC recommenda-tions compared with those who exercised less than recommended.Similarly, the mean overall (7.6 vs 7.2; P < 0.0001) and physical (7.6vs 6.5; P < 0.0001) QOL scores of surgeons who engaged in musclestrengthening activities consistent with the CDC recommendationswere superior to those who did not follow the CDC recommenda-tions. Rates of burnout were also lower among surgeons whose ex-ercise habits were consistent with the CDC aerobic exercise (24.7%[963/3898] vs 29.5% [944/3197]; P < 0.0001) and muscle strengthtraining (24.6% [637/2593] vs 28.2% [1280/4542]; P = 0.0009) rec-ommendations.
Routine Medical Care and HealthScreening Practices
The routine medical care and health screening practices ofparticipating surgeons are shown in Table 2. Approximately two-thirds of surgeons (n = 4978; 69.8%) reported currently having aprimary care provider, and 3311 (46.2%) had seen their primary careprovider in the last 12 months. Surgeons were approximately twiceas likely to have seen a dentist in the last 12 months as a primarycare provider (77.7% vs 46.2%). The mean physical (7.06 vs 6.75;P < 0.0001) and overall (7.58 vs 7.23; P < 0.0001) QOL scores ofsurgeons who had seen a primary care provider in the last 12 monthswere superior to those who had not. Rates of burnout were also loweramong surgeons who had seen a primary care provider in the last 12months (23.7% [780/3295] vs 29.7% [1142/3845]; P < 0.0001).
With respect to those surgeons eligible for health screeningstudies recommended by the USPSTF, 6160 (88.7%) had undergonecholesterol evaluation in the last 5 years and 3768 (78.6%) had com-pleted age-appropriate screening for colon cancer. Among femalesurgeons, 847 (84.5%) had undergone cervical cancer screening (eg,Papanicolaou test) in the last 3 years and 675 of the 789 (85.6%)eligible for breast cancer screening had undergone mammography
TABLE 1. Tobacco Use, Caffeine Use, and Exercise Habits ofUS Surgeons
N (%)
Tobacco useMissing, n 42Never 6028 (84.3)Few times a year or less 528 (7.4)Once a month or less 108 (1.5)Few times a month 111 (1.6)Once a week 53 (0.7)Few times a week 125 (1.8)Daily 202 (2.8)
Caffeine useMissing, n 34Never 424 (5.9)Few times a year or less 239 (3.3)Once a month or less 134 (1.9)Few times a month 220 (3.1)Once a week 100 (1.4)Few times a week 679 (9.5)Daily 5367 (74.9)
Exercise habitsMinutes of moderately intense aerobic
exercise per week∗†Missing, n 44≤30 min 1773 (24.8)31–60 min 1660 (23.2)61–120 min 1702 (23.8)121–150 min 746 (10.4)>150 min 1272 (17.8)
Minutes of vigorous aerobic exercise perweek†‡
Missing, n 80<30 min 3387 (47.6)31–45 min 567 (8)46–60 min 594 (8.3)61–75 min 463 (6.5)76–90 min 378 (5.3)>90 min 1728 (24.3)
Surgeons compliant with CDC aerobicexercise recommendations§
3911 (55.0)
Episodes of muscle-strength training perweek†
Missing, n 33None 3267 (45.6)1 1286 (18)2 1265 (17.7)3 900 (12.6)≥4 446 (6.2)
Surgeons compliant with CDCmuscle-strength trainingrecommendations¶
2611 (36.5)
∗The CDC recommends 150 minutes per week. Moderately intense exercise: briskwalking, riding bike on level ground, pushing lawn mower, water aerobics, etc.
†CDC recommendations.17
‡CDC recommends ≥75 minutes per week. Vigorous intense exercise: jogging orrunning, riding bike on hills, swimming laps, playing basketball, etc.
§At the time of the survey, the CDC recommended that adults participate in ≥150minutes per week of moderately intense exercise, ≥75 minutes per week vigorous intenseexercise, or an equivalent mix of moderately intense and vigorous intense exercise (eachminute of vigorous intense exercise equivalent to approximately 2 minutes of moderatelyintense exercise).¶CDC recommendations are at least 2 times per week. Guidelines (and the question
asked of surgeons) specified muscle strength training work all major muscle groups: legs,hips, back, abdomen, chest, shoulders, arms.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2012 Lippincott Williams & Wilkins www.annalsofsurgery.com | 627

Shanafelt et al Annals of Surgery � Volume 255, Number 4, April 2012
TABLE 2. Routine Medical Care and Health ScreenPractice of US Surgeons
n (%)
Routine medical careHave a primary care provider 4978 (69.8)
Missing, n 68Last time saw primary care provider
Missing, n 26<1 yr 3311 (46.2)1–2 yrs 1653 (23.1)3–4 yrs 730 (10.2)5 yrs or more 907 (12.6)Never 570 (7.9)
Last time saw a dentistMissing, n 35<1 yr 5563 (77.7)1–2 yrs 925 (12.9)3–4 yrs 329 (4.6)5 yrs or more 333 (4.6)Never 12 (0.2)
Health screeningLast cholesterol check
Missing, n 62≤5 yrs 6160 (88.7)>5 yrs 783 (11.3)Not indicated, n∗ 192
Age-appropriate colon cancer screening†Missing, n 55Completed 3768 (78.6)Indicated but have not had 1027 (21.5)Not indicated‡ 2347
Papanicolaou test (women)≤3 yrs 847 (84.5)>3 yrs 155 (15.5)Not indicated, n§ 46
Mammogram (women)Within the last year 504 (63.9)>1 yr ago but < 2 yrs ago 171 (21.7)>2 yrs ago 114 (14.4)Not indicated, n¶ 252
Prostate examination (men)||Within the last year 2267 (41.1)>1 yr ago but <3 yrs ago 1252 (22.7)>3 yrs ago 915 (16.6)Never 1085 (19.7)
Prostate-specific antigen (men)||Within the last year 2701 (48.8)>1 yr ago but <3 yrs ago 974 (17.6)>3 yrs ago 359 (6.5)Never 1502 (27.1)
∗Men age <35 years; women age <45 years.†Colonoscopy within the last 10 years or other colon examination (eg, flexible
sigmoidoscopy, colon x-ray) within the last 5 years.‡Age <50 years.§Prior hysterectomy.¶Age <40 years; prior bilateral mastectomy.||Only assessed for men age ≥40 years; the USPSTF deems that there is “in-
sufficient evidence to assess the balance of benefits and harms of screening forprostate cancer” and that patients should understand this uncertainty before beingscreening.
in the last 2 years. Among men older than 40 years, 2267 (41.1%)had undergone digital rectal examination in the last year, and 3519(63.8%) had undergone digital rectal examination within the last 3years. Similarly, 2701 (48.8%) had undergone prostate-specific anti-gen screening in the last year, and 3675 (66.4%) had prostate-specificantigen screening within the last 3 years. It should be noted that theUSPSTF deems that there is “insufficient evidence to assess the bal-
ance of benefits and harms of screening for prostate cancer” and thatpatients should understand this uncertainty before screening. Accord-ingly, some (∼15.0%) of surgeons older than 40 years who had neverundergone either digital rectal examination or prostate-specific anti-gen screening may have chosen to forgo screening out of a consciousdecision rather than due to complacency.
Next, we assessed what proportion of surgeons was up todate with all age- and sex-appropriate health care screening guide-lines (eg, for women: cholesterol assessment, Papanicolaou test, age-appropriate mammography, age-appropriate colon cancer screening;for men: cholesterol assessment and age-appropriate colon cancerscreening). Digital rectal examination and prostate-specific antigenscreening were not included in this analysis. Collectively, 749 (71.7%)female surgeons and 4667 (76.8%) male surgeons were up to datewith all the age- and sex-appropriate health care screening guide-lines assessed. Surgeons who reported having seen their primary careprovider in the last 12 months were more likely to be up to date with allage- and sex-appropriate health care screening guidelines (2890/3273[88.3%] vs 2515/3832 [65.6%]; P < 0.0001). The mean overall (7.5vs 7.1; P < 0.0001) and physical (7.0 vs 6.6; P < 0.0001) QOL scoresof surgeons who were up to date with all age- and sex-appropriatehealth care screening guidelines were superior to those who were notup to date. Rates of burnout were lower among surgeons who wereup to date with all age- and sex-appropriate health care screeningguidelines (25.4% [1369/5396] vs 31.4% [534/1700]; P < 0.0001).
Personal Wellness Promotion StrategiesThe importance of various personal wellness promotion strate-
gies as rated by responding surgeons is shown in Table 3. On the basisof mean score, the highest rated coping strategies were (i) findingmeaning in work; (ii) protecting time away form work with spouse,family, and friends; and (iii) focusing on what is most important inlife. The lowest rated coping strategies were regular meetings with apsychologist/psychiatrist, reflective writing/journaling, and engagingin contemplative or mindfulness practices (eg, meditation, narrativemedicine, appreciative inquiry). The mean ratings of each of the cop-ing strategies were similar for male and female surgeons where nodifference in mean rating larger than 0.2 was observed by sex. Asso-ciations between personal wellness promotion strategies and burnoutare shown in Table 4. All personal wellness promotion strategies wererated more highly among surgeons without burnout, with the excep-tion of regular meetings with a psychologist/psychiatrist to discussstress and the delayed gratification strategy of “looking forward toretirement,” which were rated more highly by burned out surgeons(all P < 0.0001).
Multivariate Associations of Self-Care ActivitiesWith Burnout
We next explored associations between burnout and high over-all QOL and surgeons’ self-care activities, including their exer-cise habits (eg, compliance with CDC aerobic exercise and musclestrength training recommendations), routine medical care practices(saw primary care provider in last year, up to date all age-appropriatehealth care screening), and personal wellness promotion strategies(dichotomized as those rating each as “essential” vs those ratingless than “essential”). Basic demographic characteristics (age, sex,relationship status, children) and professional factors (subspecialty,years in practice, hours worked per week, number of nights on callper week) previously found to be associated with surgeon burnout inour 2008 study were included in the model.8
Factors independently associated with burnout on multivariateanalysis are shown in Table 5. Sex was the only demographic char-acteristic associated with burnout (lower risk for men). Professional
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
628 | www.annalsofsurgery.com C© 2012 Lippincott Williams & Wilkins

Annals of Surgery � Volume 255, Number 4, April 2012 Wellness Practices of US Surgeons
TABLE 3. Personal Importance of Wellness Promotion Strategies as Rated by Surgeons
Not Important toMe (0),n (%)
MinimallyImportant (1),
n (%)
ModeratelyImportant (2),
n (%)Essential (3),
n (%) Mean Score∗ Rank
I find meaning in my work 46 (0.7) 347 (4.9) 2196 (30.9) 4521 (63.6) 2.6 1I protect time away from work with
my spouse, family, and friends108 (1.5) 564 (7.9) 2416 (34.0) 4011 (56.5) 2.5 2
I focus on what is most important tome in life
46 (0.7) 509 (7.2) 3076 (43.4) 3463 (48.8) 2.4 3
I try to take a positive outlook onthings
114 (1.6) 771 (10.8) 3113 (43.7) 3128 (43.9) 2.3 4
I take vacations 222 (3.1) 1168 (16.4) 2327 (32.7) 3397 (47.8) 2.3 5 (tie)I participate in recreation/
hobbies/exercise167 (2.4) 1076 (15.1) 2637 (37.1) 3233 (45.5) 2.3 5 (tie)
I talk with family, significant other,or friends about how I am feeling
324 (4.6) 1002 (14.1) 2569 (36.1) 3227 (45.3) 2.2 7
I have developed an approach/philosophy to dealing withpatients’ suffering and death
298 (4.2) 1019 (14.4) 3306 (46.8) 2448 (34.6) 2.1 8
I incorporate a life philosophystressing balance in my personaland professional life
468 (6.6) 1488 (21.0) 2904 (41.1) 2214 (31.3) 2.0 9
I look forward to retirement 1130 (16.0) 1877 (26.6) 2065 (29.3) 1986 (28.1) 1.7 10I discuss stressful aspects of work
with colleagues898 (12.7) 2079 (29.3) 2824 (39.8) 1289 (18.2) 1.6 11
I nurture the religious/spiritualaspects of myself
1495 (20.9) 1936 (27.1) 1900 (26.6) 1817 (25.4) 1.6 12
I am involved in nonpatient careactivities (eg, research, education,administration)
1527 (21.4) 1989 (27.9) 2319 (32.6) 1288 (18.1) 1.5 13
I engage in contemplative practicesor other mindfulness activitiessuch as meditation, narrativemedicine, or appreciative inquire,etc.
4500 (63.5) 1495 (21.1) 742 (10.5) 352 (5.0) 0.6 14
I engage in reflective writing or otherjournaling technique
4832 (68.6) 1400 (19.88) 546 (7.75) 264 (3.75) 0.5 15
I have regular meetings with apsychologist/psychiatrist todiscuss stress
6164 (86.6) 593 (8.33) 222 (3.12) 137 (1.93) 0.2 16
∗Scoring: not important to me = 0, minimally important = 1, moderately important = 2, essential = 3.
characteristics associated with a higher risk of burnout included areaof specialization (higher risk among urologists and ophthalmologists;lower risk among pediatric surgeons), hours worked per week, andnumber of nights on call per week. Higher ratings for several per-sonal wellness promotion strategies were associated with a lower riskof burnout after adjusting for other factors including finding mean-ing in work, taking a positive outlook, incorporating a philosophyof balance between personal and professional life, focusing on whatis most important in life, and taking vacations. Higher ratings forseveral other personal wellness promotion strategies were associatedwith a higher risk of burnout after adjusting for other factors includ-ing engaging in reflective writing/journaling, regular meetings with apsychologist/psychiatrist, nurturing religious/spiritual aspects of self,and discussing stressful aspects of work with colleagues. Surgeonswho had seen a primary care provider in the last 12 months were alsoat lower risk for burnout after adjusting for personal and professionalcharacteristics as well as wellness promotion strategies.
Factors independently associated with achieving a high overallQOL on multivariate analysis are shown in Table 6. Although manyof the factors associated with high overall QOL were similar to thefactors that seemed to protect against burnout, there were also notabledifferences. Shared factors included hours worked per week, nights
on call per week, and several personal wellness promotion strate-gies, including finding meaning in work, taking a positive outlook,incorporating a philosophy of balance between personal and profes-sional life, focusing on what is most important in life, and takingvacations. Factors unique to achieving high overall QOL includedcompliance with CDC aerobic exercise guidelines and higher ratingsfor several personal wellness promotion strategies including talkingwith family, significant other, or friends about feelings; protectingtime away from work with spouse/family/friends; and participatingin recreation/hobbies/exercise. Looking forward to retirement as anessential wellness strategy (a strategy of delayed gratification43) wasassociated with a lower likelihood of achieving high overall QOL.
DISCUSSIONAlthough recent studies have provided substantial insights into
surgeon distress, little is known about the personal health habits,routine medical care practices, or personal wellness strategies thatmay promote surgeon well-being. We are the first to simultane-ously evaluate the exercise habits, medical care/health screening prac-tices, and personal wellness strategies of a large sample of US sur-geons. Although many previous studies have explored whether physi-cians’ behaviors and health screening practices are consistent with
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2012 Lippincott Williams & Wilkins www.annalsofsurgery.com | 629

Shanafelt et al Annals of Surgery � Volume 255, Number 4, April 2012
TABLE 4. Burnout and Wellness Promotion Strategies
Burned Out∗ No Burnout∗N = 1925 N = 5232 P
I find meaning in my work. 2.3 2.7 <0.0001I protect time away from work with my spouse, family,
and friends.2.4 2.5 <0.0001
I focus on what is most important to me in life. 2.2 2.5 <0.0001I try to take a positive outlook on things. 2.0 2.4 <0.0001I take vacations. 2.1 2.3 <0.0001I participate in recreation/hobbies/exercise. 2.1 2.3 <0.0001I talk with family, significant other, or friends about how
I am feeling.2.1 2.3 <0.0001
I have developed an approach/philosophy to dealingwith patients’ suffering and death.
2.0 2.2 <0.0001
I incorporate a life philosophy stressing balance in mypersonal and professional life.
1.7 2.1 <0.0001
I look forward to retirement. 2.1 1.5 <0.0001I discuss stressful aspects of work with colleagues. 1.5 1.7 <0.0001I nurture the religious/spiritual aspects of myself. 1.4 1.6 <0.0001I am involved in nonpatient care activities (eg, research,
education, administration).1.2 1.6 <0.0001
I engage in contemplative practices or othermindfulness activities such as meditation, narrativemedicine, or appreciative inquire, etc.
0.5 0.6 0.0063
I engage in reflective writing or other journalingtechnique.
0.4 0.5 0.0006
I have regular meetings with a psychologist/psychiatristto discuss stress.
0.3 0.2 <0.0001
∗Mean rating.
TABLE 5. Factors Independently Associated With Burnout
Independent Factor∗ Odds Ratio (95% CI)† P
Male 0.707 (0.588–0.849) 0.0002Hours worked per week (for each additional hour) 1.018 (1.014–1.023) <0.0001Nights on call per week (for each additional night) 1.087 (1.055–1.121) <0.0001Specialty‡
Pediatric surgery 0.607 (0.400–0.921) 0.0190Urology 1.752 (1.293–2.374) 0.0003Ophthalmology 1.726 (1.104–2.700) 0.0168Has seen primary care provider in last 12 months 0.827 (0.726–0.942) 0.0043
Wellness strategies§Find meaning in my work 0.445 (0.387–0.512) <0.0001Take a positive outlook 0.596 (0.515–0.691) <0.0001Incorporate a philosophy of stressing work-life balance 0.633 (0.536–0.748) <0.0001Focus on what is most important in life 0.806 (0.697–0.932) 0.0031Take vacations 0.857 (0.749–0.982) 0.0259Nurture religious/spiritual aspects of self 1.189 (1.017–1.390) 0.0294Discuss stressful aspects of work with colleagues 1.319 (1.104–1.575) 0.0023Regular meetings with psychiatrist 2.244 (1.460–3.449) 0.0002Engage in reflective writing/journaling 3.865 (3.375–4.425) <0.0001
∗Factors in model: age, sex, relationship status, children, subspecialty, years in practice, hours worked per week, number of nights oncall per week, compliant with CDC aerobic exercise recommendations, compliant with CDC muscle strength training recommendations,saw primary care provider in last year, up to date all age-appropriate health care screening, rated importance of each wellness promotionstrategy.
†OR > 1 indicate a higher risk of burnout; OR <1 indicate a lower risk of burnout.‡Compared to general surgery.§Rate this strategy “essential” as compared to less than essential.
published guidelines and/or relate to how physicians’ counsel theirpatients, to our knowledge, none have explored how these practicesrelate to physicians’ QOL or degree of burnout. The aerobic exercisehabits of approximately 50% of US surgeons were consistent withthe CDC guidelines; however, only approximately one-third partic-ipated in muscle strength training consistent with CDC guidelines.
The physical QOL scores of surgeons whose exercise and/or strengthtraining habits were consistent with the CDC recommendations weremore than 0.5 SD higher than those who did not follow the guidelines(a clinically significant difference).41,42 Although approximately 70%of surgeons reported having a primary care provider, less than halfhad seen their provider in the last 12 months and more than 20% had
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
630 | www.annalsofsurgery.com C© 2012 Lippincott Williams & Wilkins

Annals of Surgery � Volume 255, Number 4, April 2012 Wellness Practices of US Surgeons
TABLE 6. Model of Independent Factors Related to High Overall QOL∗
Independent Factors† Odds Ratio (95% CI)‡ P
Married (vs single) 1.736 (1.409–2.139) <0.0001Hours worked per week (each additional hour) 0.983 (0.979–0.986) <0.0001Nights on call per week (each additional night) 0.924 (0.899–0.950) <0.0001Years in practice (each additional year) 1.020 (1.014–1.026) <0.0001CDC compliant with aerobic exercise guidelines (vs not) 1.250 (1.104–1.414) 0.0004Wellness strategies§
Take a positive outlook on things 1.772 (1.560–2.014) <0.0001Incorporate a life philosophy stressing balance 1.578 (1.365–1.823) <0.0001Find meaning in work 1.523 (1.339–1.732) <0.0001Focus on what is most important in life 1.442 (1.266–1.642) <0.0001Take vacations 1.368 (1.201–1.558) <0.0001Participate in recreation/hobbies/exercise 1.246 (1.088–1.428) 0.0015Talk with family/spouse/friends about feelings 1.244 (1.101–1.405) 0.0004Protect time away from work with spouse/family/friends 1.198 (1.051–1.365) 0.0068Regular meetings with psychiatrist to discuss stress 0.460 (0.298–0.710) 0.0004Looking forward to retirement 0.376 (0.329–0.429) <0.0001
∗Overall QOL score ≥8 out of 10 (see methods).†Factors in model: age, sex, relationship status, children, sub-specialty, years in practice, hours worked per
week, # nights on call per week, compliant with CDC aerobic exercise recommendations, compliant with CDCmuscle strength training recommendations, saw primary care provider in last year, up to date all age-appropriatehealth care screening, rated importance of each wellness promotion strategy.
‡OR > 1 indicated a higher likelihood of having high overall QOL; OR < 1 indicate a likelihood of havinghigh overall QOL.
§Rate this strategy “essential” as compared to less than essential.
not seen a primary care provider in the last 4 years. Surgeons whohad seen their primary care provider in the last 12 months were morelikely to be up to date with all age- and sex-appropriate health screen-ing guidelines and again had higher overall and physical QOL scores.These observations suggest that following the CDC guidelines foraerobic exercise and muscle strength training, seeing a primary careprovider regularly, and keeping up to date receiving routine preven-tive care may be tangible and concrete ways for surgeons to promoteboth physical and overall QOL. Because 45% to 65% of surgeonseither did not follow the CDC guidelines or did not see a primarycare provider in the last 12 months, they also identify potentiallyunderutilized strategies for US surgeons explore as part of efforts toimprove their QOL.
Another unique aspect of our study is exploration of sur-geons’ personal wellness promotion strategies. Consistent with previ-ous qualitative studies,23,24,26 meaning in work, protecting time awayfrom work for relationships, and focusing on what is most importantin life were the strategies rated essential by the largest proportionof surgeons. The hierarchical rating of wellness strategies in thislarge sample of US surgeons was strikingly similar to a similar studyof US oncologists21; however, oncologists rated “developing an ap-proach/philosophy to dealing with patients’ suffering and death” morehighly than surgeons (tied with meaning in work as the number onewellness strategy for oncologist as compared with being the eighthrated strategy by surgeons). This observation suggests that althoughmany critical wellness strategies may be shared across specialties,others may have greater importance for physicians in certain disci-plines with unique challenges (eg, frequent exposure to death andsuffering associated with medical oncology).
It also should be noted that the personal strategies beneficialto one person may not be helpful to another. For example, while onesurgeon may find mindfulness-based activities particularly helpful,25
other surgeons may find greater value in other strategies. The resultsshown in Table 4 should be viewed as a description of which strate-gies are viewed as most helpful for a large population of surgeonsrather than as a recipe that all surgeons must follow. This descriptionmay provide ideas for individual surgeons regarding new strategies of
wellness promotion that their colleagues find useful but which theymay have personally neglected. In addition, the multivariate analysisexploring which wellness promotion strategies were associated withlower rates of burnout identifies specific strategies that, although notnecessarily widely used, may be particularly effective. For example“incorporating a philosophy stressing work-life balance” was reportedas an essential wellness promotion strategy by only one third of sur-geons but those who used this strategy were approximately 40% lesslikely to be burned out on multivariate analysis. Five specific wellnesspromotion strategies were associated with a lower risk of burnout onmultivariate analysis. The fact that only 31% to 64% of respondingsurgeons rated each of these strategies “essential” suggests broaderuse of these strategies among other surgeons may prove helpful for re-ducing burnout. Although rating some wellness promotion strategiesas “essential” was associated with a higher risk of burnout, cautionmust be used in interpreting these associations. Because the resultsare cross sectional, it is plausible that some of these strategies arenot necessarily dysfunctional approaches that contribute to burnoutbut rather are approaches more likely to be employed after distressdevelops (eg, regular meetings with a psychologist/psychiatrist). Itis possible, however, that over reliance on other strategies, such as“discuss stressful aspect of work with colleagues” (ie, which could re-sult in excessive complaining/focusing on negative aspects of work),could be detrimental. It should also be noted that seeing a primarycare provider within the last 12 months was associated with a lowerrisk of burnout after controlling for other factors in multivariatemodeling.
Although many of the factors that seemed to protect againstburnout were also factors associated with achieving a high over-all QOL, notable differences were observed. For example, althoughnot associated with a lower risk of burnout, compliance with theCDC guidelines for aerobic exercise, greater emphasis on recre-ation/hobbies/exercise, and wellness strategies that emphasized per-sonal relationships (eg, talking with family, significant other, orfriends about feelings and protecting time away from work withspouse/family/friends) exhibited large and strong associations withhigh overall QOL. These observations emphasize that the absence of
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2012 Lippincott Williams & Wilkins www.annalsofsurgery.com | 631

Shanafelt et al Annals of Surgery � Volume 255, Number 4, April 2012
distress (eg, not being burned out) is not the same thing as achiev-ing high QOL/satisfaction and suggest physicians need to employ abroader repertoire of wellness promotion practices if they desire tomove beyond neutral and achieve high well-being.44
Although this study is the first, to our knowledge, to exploreimplications for QOL and burnout, the routine medical care andhealth screening practices of the surgeons in our sample are similarto those found in previous studies of physicians. In 2000, Gross andcolleagues,20 reported on the routine health care practices of morethan 900 alumni of the Johns Hopkins’ School of Medicine whohad graduated between 1948 and 1964. Roughly one-third of thesephysicians had no regular source of medical care, with surgeonsamong those less likely to have a regular source of care.20 Theseresults are relatively similar to our 2010 findings, which indicatethat approximately 30% of US surgeons do not have a primary careprovider. The proportion of US surgeons who had actually seen aprimary care provider in the last 1 (46.2%) or 2 years (69.3%) inour study is also nearly identical to the frequencies observed in anational sample of Canadian physicians conducted in 2007–2008.19
The proportion of surgeons up to date with cholesterol, colon cancer,cervical cancer, and breast cancer screening in our study is remarkablysimilar to those reported approximately 10 to 20 years ago.2,20 Similarto the findings of Gross and colleagues,20 surgeons who had a primarycare provider were more likely to be up to date with age- and sex-appropriate health care screening.
Given the declining ratio of general surgeons to the populationand the projected decrease of surgeons in the workforce over the next10 to 20 years,45,46 continued attention to surgeon burnout and itsassociation with intent-to-leave practice12 is critical. Although thisstudy is focused on the personal health and wellness practices of in-dividual surgeons, organizational efforts to promote surgeon healthare also needed. Ideally, the process of surgeon training should helpequip future surgeons with the habits and skills necessary to sus-tain them through the course of their career that prepare them forthe personal and professional challenges they will face.3 Because ofassociations between personal health habits and the care physiciansprovide their patients4–7, as well as the potential for poor health toresult in premature exit from practice,3 hospitals, health maintenanceorganizations, academic medical centers, physician societies, and of-ficials responsible for promoting public health, should also considerhow they can help surgeons maintain health and resilience. Additionalstudies are needed to evaluate the ability of programs supported bythese groups to promote surgeon health, where the findings of thisstudy provide information regarding some of the components suchprograms should contain (eg, exercise, routine medical care, effortsto promote meaning in work).
Our study is subject to a number of limitations. First, exer-cise habits and medical care/health screening practices were assessedby self-report. Although consistent with the approach used in nu-merous prior studies of physicians,2,4–7,19,20 how accurately this ap-proach assesses actual behaviors is unknown. Second, we are unableto determine whether the associations between exercise habits, med-ical care/health screening practices, and personal wellness strategiesand burnout/QOL are causally related or the potential direction ofthe effects in this cross-sectional study. Third, although similar toother national survey studies of physicians,9–11,47 our response rateof 28.7% is lower than that of physician surveys in general.48 Al-though this increases the possibility of response bias, several studiesfailed to identify significant differences between responding and non-responding physicians in cross-sectional studies.49 The fact that ratesof compliance with recommended health screening and use of routinemedical care among the participating surgeons were nearly identicalto those observed in other samples of physicians2,3,19,20 suggests thatthe participating surgeons are likely representative.
In conclusion, this study identifies specific measures asso-ciated with lower rates of burnout and improved QOL among USsurgeons. These measures include (1) increasing weekly aerobic ex-ercise and weight training to recommended levels, (2) annual visitsto their primary care provider, and (3) age-appropriate preventativetesting. It is unknown whether these measures are simply character-istics of surgeons who place a greater emphasis on self-care (andhence indirectly related) or if they represent direct ways to reduceburnout and improve QOL. Regardless, they represent the types oftangible behaviors that indicate that a surgeon values his or her per-sonal needs and health, and such a distinction may be consideredcircular. In addition to exercise habits and routine medical care prac-tices, incorporating wellness strategies that include finding meaningin work, focusing on what is important in life, maintaining a posi-tive outlook and attitude toward professional life, and embracing aphilosophy that stresses work-life balance may decrease the risk forburnout and improve professional and personal QOL. These personalstrategies, along with attention to the previously identified character-istics of work load (eg, hours worked, nights on call),8,14 specialtychoice,8 method of compensation,8 medical errors,11 medical mal-practice suits,50 and work–home conflicts,16 provide strategies forsurgeons to reduce burnout and promote QOL.
REFERENCES1. Frank E, Biola H, Burnett CA. Mortality rates and causes among U.S. physi-
cians. Am J Prev Med. 2000;19:155–159.2. Frank E, Brogan DJ, Mokdad AH, et al. Health-related behaviors of
women physicians vs other women in the United States. Arch Intern Med.1998;158:342–348.
3. Harms BA, Heise CP, Gould JC, et al. A 25-year single institution analysis ofhealth, practice, and fate of general surgeons. Ann Surg. 2005;242:520–526.Discussion 526–529.
4. Schwartz JS, Lewis CE, Clancy C, et al. Internists’ practices in health promo-tion and disease prevention. A survey. Ann Intern Med. 1991;114:46–53.
5. Frank E, Rothenberg R, Lewis C, et al. Correlates of physicians’ prevention-related practices. Findings from the Women Physicians’ Health Study. ArchFam Med. 2000;9:359–367.
6. Lewis CE, Clancy C, Leake B, et al. The counseling practices of internists.Ann Intern Med. 1991;114:54–58.
7. Frank E, Segura C, Shen H, et al. Predictors of Canadian physicians’ preventioncounseling practices. Can J Public Health. 2010;101:390–395.
8. Shanafelt TD, Balch CM, Bechamps GJ, et al. Burnout and career satisfactionamong American surgeons. Ann Surg. 2009;250:463–471.
9. Kuerer HM, Eberlein TJ, Pollock RE, et al. Career satisfaction, practice pat-terns and burnout among surgical oncologists: report on the quality of life ofmembers of the Society of Surgical Oncology. Ann Surg Oncol. 2007;14:3043–3053.
10. Yost W, Eshelman A, Raoufi M, et al. A national study of burnout amongAmerican transplant surgeons. Transplant Proc. 2005;37:1399–1401.
11. Shanafelt TD, Balch C, Bechamps G, et al. Burnout and medical errors amongAmerican surgeons. Ann Surg. 2010;251:995–1000.
12. Shanafelt T, Sloan J, Satele D, et al. Why do surgeons consider leaving practice?J Am Coll Surg. 2011;212:421–422.
13. Shanafelt TD, Balch C, Dyrbye LN, et al. Suicidal ideation among Americansurgeons. Arch Surg. 2011;146:54–62.
14. Balch CM, Shanafelt TD, Dyrbye L, et al. Surgeon distress as calibrated byhours worked and nights on call. J Am Coll Surg. 2010;211:609–619.
15. Dyrbye LN, Shanafelt TD, Balch CM, et al. Physicians married or partneredto physicians: a comparative study in the American College of Surgeons. J AmColl Surg. 2010;211:663–671.
16. Dyrbye LN, Shanafelt TD, Balch CM, et al. Relationship between work-homeconflicts and burnout among American surgeons: a comparison by sex. ArchSurg. 2011;146:211–217.
17. Centers for Disease Control and Prevention. Physical activity for everyone.Available at: www.cdc.gov/physicalactivity/everyone/guidelines/adults.html#aerobic. Accessed February 17, 2012.
18. Agency for Healthcare Research and Quality. U.S. Preventive Services TaskForce. Available at: http://www.ahrq.gov/clinic/uspstfix.htm. Accessed Febru-ary 17, 2012.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
632 | www.annalsofsurgery.com C© 2012 Lippincott Williams & Wilkins

Annals of Surgery � Volume 255, Number 4, April 2012 Wellness Practices of US Surgeons
19. Frank E, Segura C. Health practices of Canadian physicians. Can Fam Physi-cian. 2009;55:810.e7–811.e7.
20. Gross CP, Mead LA, Ford DE, et al. Physician, heal thyself? Regular source ofcare and use of preventive health services among physicians. Arch Intern Med.2000;160:3209–3214.
21. Shanafelt T, Novotny P, Johnson ME, et al. The well-being and personal well-ness promotion practices of medical oncologists in the North Central CancerTreatment Group. Oncology (Karger). 2005;68:23–32.
22. Swetz KM, Harrington SE, Matsuyama RK, et al. Strategies for avoidingburnout in hospice and palliative medicine: peer advice for physicians onachieving longevity and fulfillment. J Palliat Med. 2009;12:773–777.
23. Quill TE, Williamson PR. Healthy approaches to physician stress. Arch InternMed. 1990;150:1857–1861.
24. Lyckholm L. Avoiding stress and burnout in cancer care. Words of wisdomfrom fellow oncologists. Oncology (Williston Park). 2007;21:269.
25. Krasner MS, Epstein RM, Quill TE, et al. A continuing education program inmindful communication: effects on primary care physician burnout, empathy,and attitudes. J Am Med Assoc. 2009;302:1284–1293.
26. Weiner EL, Swain GR, Wolf B, et al. A qualitative study of physicians’ ownwellness-promotion practices. West J Med. 2001;174:19–23.
27. Maslach C, Jackson S, Leiter M. Maslach Burnout Inventory Manual. 3rd ed.Palo Alto, CA: Consulting Psychologists Press; 1996.
28. Ware J, Kosinski M, Turner-Bowker D, et al. How to Score Version 2 of theSF-12 Health Survey. Lincoln, RI: Quality Metric Incorporated; 2002.
29. Whooley MA, Avins AL, Miranda J, et al. Case-finding instruments for depres-sion. Two questions are as good as many. J Gen Intern Med. 1997;12:439–445.
30. Ware J, Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey:construction of scales and preliminary tests of reliability and validity. MedCare. 1996;34:220–233.
31. Thomas NK. Resident burnout. J Am Med Assoc. 2004;292:2880–2889.32. Shanafelt TD, Bradley KA, Wipf JE, et al. Burnout and self-reported pa-
tient care in an internal medicine residency program. Ann Intern Med.2002;136:358–367.
33. Rosen IM, Gimotty PA, Shea JA, et al. Evolution of sleep quantity, sleepdeprivation, mood disturbances, empathy, and burnout among interns. AcadMed. 2006;81:82–85.
34. West CP, Dyrbye LN, Sloan JA, et al. Single item measures of emotionalexhaustion and depersonalization are useful for assessing burnout in medicalprofessionals. J Gen Intern Med. 2009;24:1318–1321.
35. West CP, Tan AD, Habermann TM, et al. Association of resident fatigue anddistress with perceived medical errors. J Am Med Assoc. 2009;302:1294–1300.
36. Gudex C, Dolan P, Kind P, et al. Health state valuations from the general publicusing the visual analogue scale. Qual Life Res. 1996;5:521–531.
37. Spitzer WO, Dobson AJ, Hall J, et al. Measuring the quality of life of cancer pa-tients: a concise QL-index for use by physicians. J Chronic Dis. 1981;34:585–597.
38. Ware JE, Kosinski M, Keller SD, eds. The SF-36 Physical and Mental HealthSummary Scales: A Manual for User’s of Version 1. 2nd ed. Lincoln, RI:QualityMetric Incorporated; 2001.
39. Cella D, Zagari MJ, Vandoros C, et al. Epoetin alfa treatment results in clinicallysignificant improvements in quality of life in anemic cancer patients whenreferenced to the general population. J Clin Oncol. 2003;21:366–373.
40. Shanafelt TD. Finding meaning, balance, and personal satisfaction in the prac-tice of oncology. J Support Oncol. 2005;3:157–162, 164.
41. Sloan JA, Cella D, Hays RD. Clinical significance of patient-reported question-naire data: another step toward consensus. J Clin Epidemiol. 2005;58:1217–1219.
42. Sloan JA. Assessing the minimally clinically significant difference: scientificconsiderations, challenges and solutions. Copd. 2005;2:57–62.
43. Shanafelt T, Chung H, White H, Lyckholm LJ. Shaping your career to maximizepersonal satisfaction in the practice of oncology. J Clin Oncol. 2006;24:4020–4026.
44. Shanafelt T, Sloan J, Habermann T. The Well-Being of Physicians. Am J Med.2003;I114:513–517.
45. Poley S, Belsky D, Gaul K, et al. Longitudinal trends in the U.S. surgicalworkforce, 1981–2006. Bull Am Coll Surg. 2009;94:27–31.
46. Lynge DC, Larson EH, Thompson MJ, et al. A longitudinal analysis ofthe general surgery workforce in the United States, 1981–2005. Arch Surg.2008;143:345–350. Discussion 351.
47. Guntupalli KK, Fromm RE, Jr. Burnout in the internist–intensivist. IntensiveCare Med. 1996;22:625–630.
48. Asch D, Jedrziewski M, Christakis N. Response rates to mail surveys publishedin medical journals. J Clin Epidemiol. 1997;50:1129–1136.
49. Kellerman S, Herold J. Physician response to surveys. A review of the literature.Am J Prev Med. 2001;20:61–71.
50. Balch CH, Oreskovich MR, Dyrbye L, et al. Personal consequences ofmalpractice lawsuits on American surgeons. J Am Coll Surg. 2011;213:657–667.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
C© 2012 Lippincott Williams & Wilkins www.annalsofsurgery.com | 633

COREME-UNIFESP/2012
Alergia e Imunologia Pediátrica Dra. Beatriz Tavares Costa Carvalho (Supervisora)
Cirurgia Cardiovascular Dr. Nelson Américo Hossne Jr. (Preceptor) e Dr. Guilherme Flora Vargas (Suplente).
Cirurgia PediátricaDra. Elaine Cristina Soares Martins (Preceptora) e Dr. Alexandre Alberto Barros Duarte
(Suplente).
Endocrinologia PediátricaDra. Angela Spinola e Castro (Supervisora), Dra. Fabiola Sgrignoli Garcia (Preceptora ) e Dra.
Adriana Siviero Miachon ( Suplente).
Gastroenterologia Pediátrica Dra. Vera Lucia Sdepanian (Supervisora) e Dra. Ana Cristina Fontenele Soares (Preceptora).
Hematologia e Hemoterapia PediátricaDra. Josefina A P Braga (Supervisora), Dra. Andrea Angel (Preceptora ) e Dra. Mary Hokozono
( Suplente).
Infectologia Pediátrica Profa. Dra. Maria Aparecida Gadiani Ferrarini (Supervisora).
Medicina do AdolescenteDra. Sheila Rejane Niskier (Supervisora), Dra. Maria Sylvia de Souza Vitale (Preceptora ) e Dra.
Flavia Calanca da Silva ( Suplente).
Medicina Intensiva PediátricaDr. Nilton Ferraro Oliveira (Supervisor), Dr. Nivaldo de Souza (Preceptor ) e Dr. Renato Lopes
de Souza ( Suplente).
Nefrologia Pediátrica Prof. Dr. João Tomas de Abreu Carvalhaes (Supervisor).
Neonatologia Dra. Maria Fernanda Branco de Almeida (Supervisora).
Nutrologia Pediátrica Dr. Domingos Palma (Supervisor) e Dra. Fernanda Luisa Ceragioli Oliveira (Preceptora ).
Pediatria Ano OpcionalDra. Alzira Rosa Esteves (Supervisora), Dr. Humberto Bracco Neto (Preceptor ) e Dra. Cecilia
Micheletti ( Suplente).
Pneumologia Dr. Flávio Arbex (Preceptor).
Pneumologia PediátricaDr. Gilberto Petty da Silva (Supervisor), Dra. Beatriz Neuhaus Barbisan (Preceptora ) e Dr.
Carlos Roberto Bazzo ( Suplente).
Reumatologia Dr. Marcelo Pavan Paiva (Preceptor).
Reumatologia Pediátrica Prof. Dr. Claudio Arnaldo Len (Supervisor),
Novos Membros - COREME-UNIFESP/2012

Universidade Federal de São Paulo UNIFESP
Comissão de Exames de Residência Médica COEXREM
Rua Pedro de Toledo, 650 - 2°andar - Vila Clementino - São Paulo - SP - CEP 04039-002
Tel.: 5576-4717 Opção 04 [email protected]
Cronograma de Processo Seletivo para Residência Médica – 2013
Data Competência Evento
18/05/2012 UNIFESP Entrega dos Critérios e respectivos Pesos das Entrevistas.
31/05/2012 UNIFESP Entrega de Questões teóricas e práticas pelos Departamentos.
Até 03/09 UNIFESP Publicação do extrato do Edital
04 a 05/09 UNIFESP Recebimento de recursos referentes ao Edital
24/09 a 24/10/2012 UNIFESP Período de Inscrições.
25/09 UNIFESP Pedido de redução/isenção de taxa.
até UNIFESP Revisão das Provas.
01/11/2012 Instituição Aplicadora
Divulgação dos locais de prova, mediante o número de inscrição, no site da Instituição Aplicadora.
04/11/2012 (manha) Instituição Aplicadora
Aplicação das Provas.
05/11/2012 Instituição Aplicadora
Divulgação das Provas e Gabarito da Prova de Múltipla Escolha.
06 e 07/11/2012 UNIFESP Recebimento de recursos.
08/11/2012 UNIFESP Análise dos recursos relativos ao Gabarito da Prova de Múltipla Escolha.
05 a 09/11/2012 Instituição/ UNIFESP
Análise de amostragem e Conclusão do Gabarito Definitivo à Instituição Aplicadora.
19/11 (tarde) Aplicadora Divulgação das notas da 1ªFase
21 a 22/11 UNIFESP Recebimento de pedido de vista de prova.
23/11 (manhã) UNIFESP Vista de Provas ( das 8h às 10h) e prazo de recurso (das 8:00h às 16:00h)
28/11/2012 (tarde) Aplicadora Divulgação do resultado da 1ªFase após análise de recursos / Convocação dos classificados para a 2ªFase / Convocação para Entrevista
07/12/2012 UNIFESP Aplicação da Prova Prática - Acesso Direto.
07/12/2012 (tarde) UNIFESP Envio das Provas dissertativas de Psicologia e Clínica para correção.
08/12/2012 (Manhã) UNIFESP Aplicação da Prova Prática – G.O.
08/12/2012 (Tarde) UNIFESP Aplicação da Prova Prática – Especialidades Clínicas
10/12/2012 Correção das Provas dissertativas de Psicologia e Clínica.
11/12/2012 UNIFESP Envio da planilhas de entrevista para os programas
12 a 14/12/2012 Instituição Aplicadora
Entrevistas e retorno com as notas.
18/12/2012 UNIFESP Analise pré-homologação pela comissão
19/12/2012 UNIFESP Convocação dos Depto com notas erradas
20/12 UNIFESP Homologação
21/12 Instituição Aplicadora
Publicação do resultado final e convocação para matricula.
21/12 a 28/12 UNIFESP Confirmação de Interesse na vaga
15, 16 e 17/01/2013 UNIFESP Matrícula dos aprovados em 1ª chamada.
a partir de 25/01/2013 UNIFESP Matrícula dos aprovados em chamadas adicionais.
OBS.: Os eventuais atrasos no cronograma, por uma das partes, dará a outra, o direto de compensar em
igual período.
Universidade Federal de São Paulo Programa de Residência Médica em Cirurgia Geral
Departamento de Cirurgia
Rua Napoleão de Barros 715 – 4°andar – cep. 04024-002 – Vila Clementino Tel. (11) 5576 4068
Avaliação do Residente
Nome: Ano: R1/2 2012
Estágio: Data:
Critérios Nota* Peso Média
Habilidades Realizou com segurança procedimentos de prevenção, diagnóstico e tratamento nas práticas clínicas e/ou cirúrgicas
x 0,4
Atitudes
Foi pontual, assíduo e cumpriu o horário destinado às atividades da residência
x 0,1
Identificou problemas e propôs soluções para o bom funcionamento do setor x 0,1
Esteve disponível para executar as atividades e procedimentos conforme a necessidade dos pacientes x 0,1
Relacionou-se com o paciente de forma cordial e respeitosa explicando de forma clara as condutas adotadas pela equipe
x 0,1
Relacionou-se com os preceptores e como os demais profissionais do setor com cordialidade respeitando as suas funções e diferenças
x 0,1
Relacionou-se com outros residentes de forma cordial, respeitando as diferenças individuais x 0,1
Habilidades + Atitudes (Se considerar prova teórica, aplicar peso 50%) x 0,5
Teórica Prova teórica opcional da Disciplina (Peso 50%) x 0,5
Nota final do estágio
* Pontuar cada critério de 0 a 10, multiplicar pelo peso = Média **Notas: Muito ruim (1-2); ruim (3 e 4); regular (4 e 5); bom (6 e 7); muito bom (8 e 9) ótimo (10) *** Se aplicar prova teórica, considerar pesos (Habilidades + Atitudes)x 0,5 + (Teórica)x 0,5 = nota final
Observações:
São Paulo, ______de _____________de _________
_____________________________
Preceptor do Estágio
________________________________ Supervisor do Estágio





























