-
8/20/2019 C5. Chap10. Nouette-Gaulain
1/22
CURRENTOPINION Local anesthetic ‘in-situ’ toxicity
during peripheralnerve blocks: update on mechanismsand
prevention
Karine Nouette-Gaulaina,b, Xavier Capdevilac,d, and Rodrigue
Rossignol a
Purpose of review
Peripheral nerve blocks induce undesired side-effects linked to
the toxicity of local anesthetics on neuronand myocytes via
different cell targets. The effects of local anesthetics on these
targets are now well knownand summarized in this review.
Recent findings
Local anesthetic-induced local cell toxicity involved different
pathways leading to cell death, necrosis and
different factors closely associated with the clinical practice
modulated this toxicity. High concentration andprolonged duration
of local anesthetic administration are closely associated with
severe lesions.
Summary
Phenotypic analyses revealed that local anesthetics could induce
histological damage with lesions rangingfrom local to extreme in
skeletal muscle. Metabolic alterations were also described
involving sarcoplasmicreticulum and calcium dysregulation,
alteration of mitochondrial physiology and of
oxidativephosphorylation with associated overproduction of harmful
reactive oxygen species, typically leading toapoptosis or
necrosis.Biochemical and cell biology investigations now indicate
that local anesthetics interact with differentmolecular targets in
mammalian cells as respiratory chain complex I or the prosurvival
kinase Akt.Functional dysfunction in both muscle and neuron remains
to be investigated with caution in patients, aslocal anesthetic
toxicity remains under-evaluated. Likewise, the use of adapted
local anesthetics in patientswith particular diseases and
neuromuscular disorder could further reduce the risk of undesired
effect.
We need to improve our practice, and the optimization of our
clinical protocol could prevent from theseside-effects. Lastly,
experimental studies highlight the preventive effects of
antioxidant drugs or of recombinant human erythropoietin but
the pharmacokinetic feature of such strategies remain to
beevaluated.
Keywords
apoptosis, local anesthetic, local toxicity, muscle, neuron
INTRODUCTION
During peripheral nerve blocks, local anestheticspreads into
contact with the nerve, inhibits volt-
age-gated sodium channels, and prevents the propa-gation of
action potentials within the nervoussystem. Peripheral nerve blocks
performed with loc-al anesthetics improve postoperative analgesia
andrehabilitation in patients. However, local anes-thetics can
induce in-situ toxicity mediated by theirpleiotropic effects on
cell metabolism and tissueultrastructure in the neighborhood of
neuronsand muscle. In this review article we summarizedfirst the
reported iatrogenic events published indifferent clinical case
reports and we discuss theunderlying mechanisms of this toxicity
from the
analysis of different cell biology and biochemicalstudies. We
conclude with a discussion on suggestedpreventive approaches of
local anesthetic toxicity.
aUniversity Bordeaux, Maladies Rares, Génétique et
Métabolique(MRGM), bCHU de Bordeaux, Service d’Anesthésie
Réanimation 3,Pôle d’Anesthésie Réanimation, Bordeaux, cCHU de
Montpellier, Serviced’Anesthésie Réanimation A and dInserm
U1046, Bat Crastes de Paulet,Montpellier, France
Correspondence to Karine Nouette-Gaulain, Hôpital des
Enfants,Service d’Anesthésie Réanimation 3, Centre Hospitalier
Universitairede Bordeaux, Place Amélie Raba Léon, 33076 Bordeaux,
France. Tel:+33 5 56 79 56 10; fax: +33 5 56 79 56 61 96; e-mail:
[email protected]
Curr Opin Anesthesiol 2012, 25:589–595
DOI:10.1097/ACO.0b013e328357b9e2
0952-7907 2012 Wolters Kluwer Health | Lippincott
Williams & Wilkins www.co-anesthesiology.com
REVIEW
http://-/?-http://-/?-http://-/?-mailto:[email protected]:[email protected]:[email protected]:[email protected]://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
8/20/2019 C5. Chap10. Nouette-Gaulain
2/22
LOCAL ANESTHETIC-INDUCED
CYTOTOXICITY IN CLINICAL PRACTICE
Direct cytotoxicity of the local anesthetics wasdescribed in
both muscle and neuron. Local anes-thetic-induced myotoxicity is
well known after
cataract surgery and other intraocular procedures.Bupivacaine
induced persistent diplopia throughdirect damage to the extraocular
muscles, fromretrobulbar or peribulbar anesthesia [1,2].
Likewise,repeated bupivacaine injections (1.14 g of bupiva-caine
during 34-h period) through an interscalenecatheter after surgery
for capsular release of leftshoulder induced persistent pain over
the 3 post-operative months [3]. The muscle biopsy performedon
the 54th day revealed the coexistence of degen-erating and
regenerating muscle fibers with struc-tural evidences of myophagy
[3].
Apart from the muscle, local anesthetic-inducedperipheral nerve
injury is also rare (from 4 : 1000 to3 : 100 of transient
neurological deficit in intersca-lene block [4–6]) and can
even be observed inpatients after 6 months [7].
CELL ULTRASTRUCTURAL DAMAGES
INDUCED BY LOCAL ANESTHETICS
Microscopic analysis of myocyte and nerve showedthat local
anesthetics damaged cell ultrastructureand induced local
inflammatory reaction.
Alteration of myocyte ultrastructure and ofmitochondrial
architecture
Various local anesthetics were used in experimentalstudies to
investigate the mechanisms of necrosisand subsequent muscle
regeneration [8,9]. Highconcentration of bupivacaine (16
mg/kg) injecteddirectly in rat muscle induced myonecrosis, with
disjointed fibers, interstitial edema, and
infiltratingcells [9]. Likewise, an initial bolus (3– 5 mg/kg
bupi-vacaine or ropivacaine) followed by a continuousinfusion
(0.6–1 ml/kg during 6 h) of local anestheticcauses a widespread
interstitial and myoseptaledema, followed by disruption and
condensationof the myofilament, lytic degeneration of the
sarco-plasmic reticulum and of mitochondria, andpycnotic changes of
the nuclei in pig [10]. Likewise,rats treated with 2.5 mg/kg
bupivacaine presenteda wide spectrum of muscle and
mitochondrialabnormalities [11,12].
Alteration of neuron ultrastructure
Incubation of the axonal compartment with 40 mMlidocaine for 24
h induced axonal degeneration withretraction of distal neuritis and
fragmentationof neuritis [13]. Moreover, lidocaine,
ropivacaine,and bupivacaine reduced the number of neurons[14]. In
SH-SY5Y cells, 20min treatment with 10mMlidocaine induced
retraction of the cell extension[15]. Continuous infusions of
0.5–0.75% bupiva-caine for 72 h in the vicinity of the sciatic
nervesof rats induced severe wallerian degeneration, withvarying
degrees of disruption of the normal myelinarchitecture, formation
of myelin globules andvacuolization, and focal loss of myelin
staining[16
&&
]. Lastly, infusion of 600 mM lidocaine justoutside of the
perineurium was associated withswollen axons, macrophage
phagocytosis of degen-erated tissue, and epineurial and endoneurial
colla-gen [17].
IMPACT OF LOCAL ANESTHETICS ON
ENERGY METABOLISM
Local anesthetic-induced in-situ toxicity is medi-ated by
sarcoplasmic reticulum and mitochondria,closely linked, both
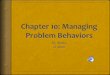
structurally and functionally[18]. Numerous effects coexist and
lead the neuronand the myocyte to apoptosis (Fig. 1).
Mobilization of intracellular calcium by localanesthetics
Local anesthetics interact with calcium homeostasisthrough their
effects on Ca2þ entry and on intra-cellular Ca2þ mobilization. In
skinned muscle fiber
KEY POINTS
Local anesthetics induce a large spectrum of muscleand
neuron ultrastructure abnormalities.
Local anesthetics induce an intracellular Ca2þ
mobilization and can change Ca2þ homeostasisthrough the
Ca2þ-influx pathway in both myocytes
and neurons.
Local anesthetics induce a reduction of themuscle
mitochondrial content and the kineticinhibition of oxidative
phosphorylationassociated with an overproduction of reactiveoxygen
species.
Local anesthetic-induced toxicity is time
andconcentration-dependent. Low concentration of localanesthetics
induces neuronal apoptosis and highconcentration of local
anesthetics leads to necroticcell death.
Toxicity prevention is based in clinical practice
on the determination of the minimum lowanesthetic concentration
for different peripheralblocks, the duration of the protocol, and
thetarget site in which the injection of local anestheticshould
occur.
Regional anesthesia
590 www.co-anesthesiology.com Volume 25
Number 5 October 2012
http://-/?-http://-/?-
-
8/20/2019 C5. Chap10. Nouette-Gaulain
3/22
preparations, bupivacaine (5– 15 mM) induced Ca2þ
release from the sarcoplasmic reticulum by actingon the Ca2þ
release channel-ryanodine receptors
(RyR), and inhibits Ca2þ reuptake into the sarco-plasmic
reticulum, which is mainly regulated bysarcoplasmic reticulum Ca2þ
ATPase activity[19,20]. Bupivacaine might inhibit these receptorsby
direct binding, but this has never been demon-strated. Moreover,
the production of reactiveoxygen species (ROS) induced by 1.5 mM
bupiva-caine could modify oxidizable residues (cysteine,tyrosine)
of sarcoplasmic reticulum-associatedcalcium channels, such as RyR
(S-nitrosylation)and SR/ER Ca2þ ATPases (by tyrosine
nitration),causing their dysfunction and sarcoplasmic reticu-
lum calcium depletion [21,22]. After seven injec-tions of
levobupivacaine via a femoral nervecatheter, this regional
analgesia regimen induceda significant increase in the frequency of
Ca2þ sparks(caused by release of increment of Ca2þ via
sarco-plasmic reticulum) associated with a decrease insarcoplasmic
reticulum Ca2þ content [23].
On rat-isolated dorsal root ganglion, lidocaineinduced
intracellular Ca2þ mobilization with anincrease in intracellular
[Ca2þ] concentration andincreased [Ca2þ] influx through both plasma
mem-brane and intracellular store membrane [24].
Moreover, lidocaine (>0.5%) and bupivacaine(>0.125%)
caused an initial, short-lived, moderateincrease in
[Ca2þ]cytosolic [25]. After 60 min exposure
period, high concentrations of lidocaine (2.5%) orbupivacaine
(5%) caused a significant sustainedincrease in
[Ca2þ]cytosolic associated with cell deathin neurons. The
accumulation of Ca2þ inside the cellcould explain the
lidocaine-induced inhibition of axonal transport and the
decrease in the numberof particles in both anterograde and
retrogradedirections [26].
Inhibition of mitochondrial energymetabolism by local
anesthetics
Muscular and nervous tissues are particularly rich
inmitochondria and strongly rely on aerobic ATPproduction.
Inhibition of mitochondrial energyproduction involves different
mechanisms combin-ing the direct interaction between local
anestheticsand the respiratory chain localized in the
innermitochondria membrane, and the effects inducedby a prolonged
exposure over at least 24 h.
Local anesthetic-induced myotoxicity is nowwell established
[27–29]. Repeated injections of 0.25% bupivacaine
(1ml/kg via femoral nervecatheter) exhibited changes in
mitochondrial
CHOP
OXPHOS uncoupling
Mt network fragmentation
Mitophagy
ATP synthesis
ETC activity
∆Ψ
Cell survival Apoptosis
Akt, ERK
Reactive oygen
species
Caspase 3/7
Caspase 9
Cytochrome c
Ca2+
Bcl2
Nucleus
ER/RS
stress
Necrosis
FragmentationDNA
Transcription
p38 MAPK
FIGURE 1. Local anesthetics interact with many targets
leading mammalian cell to death by necrosis or apoptosis via
differentpathways. White arrows represent the inhibitor or the
activator effects of LA on the target. Ca 2þ, calcium; CHOP,
C/EBPhomologous protein; ETC, electron transport chain; LA, local
anesthetic; Mt, mitochondrial.
Local anesthetic in-situ toxicity Nouette-Gaulain et
al.
0952-7907 2012 Wolters Kluwer Health | Lippincott
Williams & Wilkins www.co-anesthesiology.com
591
-
8/20/2019 C5. Chap10. Nouette-Gaulain
4/22
structure with a significant inhibition of ATP pro-duction
(around 30–50%) in the psoas musclesurrounding the catheter. This
was explained bya reduction of the muscle mitochondrial con-tent
[30], and the kinetic inhibition of oxida-tive
phosphorylation [11,23]. Bupivacaine-inducedinhibition on
mitochondrial energy metabolism
includes various mechanisms: the specific inhi-bition of
mitochondrial respiratory chain complexI, oxidative phosphorylation
uncoupling, thespecific inhibition of the mitochondrial F1-F0
ATPsynthase, the decrease of mitochondrial membraneelectric
potential, the fragmentation of the mito-chondrial network, the
possible onset of mitoptosis,and the reduction of the respiratory
chain proteincontent, which can be observed for
long-lastingexposure to bupivacaine. Likewise, in the ND7 cellline
derived from rat dorsal root ganglion, the com-plete loss of
mitochondrial membrane potentialoccurred within 5 min after
exposure to 19mMlidocaine and a release of mitochondrial
cyto-chrome c to cytoplasm was observed within 2 h [31].
In a global approach, chronic effects of bupiva-caine iterative
injections via sciatic nerve catheter inrats were quantified using
P31 NMR [32
&
]. In thepresence of bupivacaine, the lack of difference
inelasticities of muscle energetics during contractionobtained in
treated rats in comparison with healthycontrol rats clearly showed
the absence of globaldysfunction in the control of muscle
contraction byenergy production. Yet, this work was performed
onhealthy animals and should be repeated on diseased
animals. In particular, the functional consequencesof local
anesthetic toxicity could be evaluated inmuscle fibers and neurons
of individuals or animalmodels suffering from metabolism
dysfunctionas diabetes, pure mitochondrial disease, or
evencancer.
An important feature of local anesthetic-induced cytotoxicity is
oxidative stress (elevatedlevels of ROS) [33]. After an 8-h
bupivacaineexposure, ROS production in bupivacaine-treatedmyotubes
was described in a dose-dependent man-ner [34]. Likewise, in
the human neuroblastoma cell
line SH-SY5Y, the intracellular ROS level peaked at3 h
after 1 mM bupivacaine treatment [35
&
]. ROSproduction can be amplified by the activation
of AMP-activated protein kinase pathway (AMPK) [36]upon
energy crisis as well as by P66shc [37].
Local anesthetic-decreased cell viability inneuron and in
myocyte
All local anesthetics but not tetrodotoxin caninduce a decrease
in cell viability in myotubesand in neuron from many minutes to a
few hours
of local anesthetic exposure [12,15]. This effectwas
explained by two mechanisms: apoptosis andnecrosis. At low
concentrations, all local anestheticsinduce apoptosis
[31,38]. On the contrary, at highconcentration, necrotic cell death
predominated[31,38,39].
Local anesthetic-induced apoptosis includes the
activation of caspases, p38 MAPK phosphorylation,Akt inhibition,
and sarcoplasmic reticulum/endo-plasmic reticulum stress. Apoptosis
is controlled bycaspases and 1 mM bupivacaine
treatment-causedcaspase 3/7 activation in SH-SY5Y. Local
anesthetictoxicity was also associated with cytochrome crelease in
ND7 cell line [31,39], caspase 9 activationin human Jurkat
cells and myotubes [34,39], poly(ADP-ribose)polymerase
(PARP) down-regulation(involved in DNA repair and genome
surveillance)in Schwann cell line and myotubes [34,40],
andDNA fragmentation [41]. As expected, the lack
of caspase 9, as well as overexpression of Bcl-2
protein(antiapoptotic protein), prevents caspase 3 acti-vation
[39]. These findings highlight the role
of mitochondrial pathway in local
anesthetic-inducedapoptosis.
Recent studies indicate that the p38 MAPK path-way might play a
central role in local anesthetic-induced cytotoxicity. The p38 MAPK
is involved inregulation of apoptosis, gene expression, mitosis,and
cell death. The direct neurotoxic effects of lidocaine,
ropivacaine, and bupivacaine leading tocell apoptosis are
associated with a phosphorylationof p38 MAPK and in c-Jun
N-terminal kinase (JNK)
in adult rat dorsal root ganglion neurons [14].
Theinhibition of p38 MAPK phosphorylation had noeffect on
bupivacaine-induced ROS production andmitochondria depolarization,
suggesting that mito-chondria injury could be upstream of
p38 MAPKphosphorylation [42
&
]. An inhibitor of caspase 1 and3 did not prevent selective
axonal injury, whereascaspase inhibition is neuroprotective in
dissociatedneuronal culture submitted to lidocaine treatment[13].
In conclusion, this suggests that the mechan-isms involved in cell
toxicity depend upon whetherthe entire neuron or only the axon is
submitted to
local anesthetic exposure.Another molecular target of Las
involved in
apoptosis inhibition is the kinase Akt which playsa pivotal role
in cell survival. Lidocaine and bupi-vacaine can induce Akt
inhibition, and in mouseC2C12 myoblast, a negative correlation
between thelevels of Akt activation and the degree of
localanesthetic-induced apoptosis was observed [43].Of
interest for the prevention of local anesthetictoxicity, the
activation of Akt phosphorylationcould protect from local
anesthetic-induced neurondamage [44].
Regional anesthesia
592 www.co-anesthesiology.com Volume 25
Number 5 October 2012
-
8/20/2019 C5. Chap10. Nouette-Gaulain
5/22
Lastly, the sarcoplasmic/endoplasmic reticulumstress could be
considered as a target of localanesthetics. Caspase 7 is involved
in endoplasmicreticulum stress-mediated apoptosis, as well
asexpression of the endoplasmic reticulum stressmarkers
X-box-binding protein 1 (XBP-1), activatingtranscription factor 6
(ATF-6), and C/EBP homo-
logous protein (CHOP). In myotubes, 8-h bupiva-caine treatment
induces CHOP expression (a keydownstream transcription factor in
sarcoplasmicreticulum stress-induced apoptosis) as well
asexpression of XBP-1 and ATF-6 (two transcriptionfactors that
control expression of CHOP) [34]. Block-ing ROS production during
bupivacaine treatmentin myotubes decreases CHOP expression and
inhi-bits expression of activated caspases.
Limitations
All laboratory experiments were performed in thepresence of 1–
10 mM local anesthetic, for bothbupivacaine and lidocaine. This was
chosen tomimic the effects of direct local anesthetic exposureof
in-situ cell at clinically relevant concentration.Whereas such high
concentrations are systemati-cally discussed in the literature, we
know thatlipophilic local anesthetics accumulate in tissueand that
the real cell concentration remainsunknown. Thus, concentrations
commonly usedshould not be so far from clinical practice
[34].
Moreover, the cell model used for toxicityanalyses could play a
major role, and the results
must be interpreted according to the cell type. Forinstance, we
demonstrated that cell type (cancer cellor not) as well as
metabolic profile of cancer cellcould mitigate local
anesthetic-induced toxicity[45
&
]. Thus, the conclusions drawn from in-vitroexperiments based on
a cancer cell should be inter-preted with caution.
PREVENTION
Today, protective strategies based on optimizationof local
anesthetic protocol for regional analgesia
are proposed to prevent in-situ toxicity. Antioxidantdrugs or
new galenic local anesthetic remains in theinvestigation field and
many studies are still neededbefore clinical use.
Optimization of clinical protocol
All local anesthetics we daily use, induce Schwanncell and
myocyte toxicity in a time and concen-tration-dependent manner. The
severity of localanesthetic-induced in-situ toxicity increases
alongwith increase of the concentration and incubation
time of local anesthetics [12,39]. This
concernshistological damage as well as metabolism altera-tions
[12,25,31,46,47]. For clinicians, this requiresus to
determine the minimum low anestheticconcentration for different
peripheral blocks, theduration of the protocol, and to better
define thetarget site in which the injection of local
anesthetic
should occur [48]. Using ultrasound guidance
forperipheral nerve block contributes to the decreasein the volumes
of local anesthetic administered.Further studies will confirm or
not if this advantagewill be associated with a decrease in neural
or musclecell injuries.
Moreover, proper biochemical properties of local
anesthetics should be considered while assess-ing their toxicity.
Lidocaine has been describedespecially toxic for neurons when given
intrathe-cally [49–53], whereas bupivacaine have beenshown
to be the most toxic in myoblast [43,54]. Itseems likely that
the mechanism of injury is depend-ent not only on local anesthetics
and type of cell butalso on the pathway investigated. Thus, this
bio-chemical classification of toxicity does not appearclear in all
studies [13,15,55].
Finally, the importance of the cellular context,in particular
the energy state of the cell, coulddetermine in large part the
extent of local anesthetictoxicity. The mitochondrial inhibitory
effects makethe use of some local anesthetic particularly carefulin
patients with compromised energy production,such as observed in the
case of mitochondrial raredisorders, chronic hypoxia, diabetes, and
statin
treatment [27,56,57].
Perspectives
Antioxidant drugs prevent many dysfunctionsinduced by local
anesthetics. N-acetyl-l-cysteineprevents cell death, inhibition of
both complexesI and III activities [33],
sarcoplasmic/endoplasmicreticulum stress, activation of caspases 9,
3/7, andPARP degradation [34,40]. Resveratrol
mimicsN-acetyl-l-cysteine protection from bupivacaine-induced
in-situ toxicity [34]. Alpha-lipoic acid pre-
vents bupivacaine-decreased cell viability, Aktphosphorylation,
and apoptosis [58]. Recombinanthuman erythropoietin (5000
UI/kg/24 h) preventsthe inhibitory effects of bupivacaine on
mitochon-drial bioenergetics in rat and
bupivacaine-inducedreduction of mitochondrial membrane potentialand
fragmentation of mitochondria in human myo-blasts [12].
Other potential therapeutic strategy could beavailable:
dexamethasone prevents bupivacaineand lidocaine-decreased Akt
phosphorylation[44], nandrolone decanoate administration could
Local anesthetic in-situ toxicity Nouette-Gaulain et
al.
0952-7907 2012 Wolters Kluwer Health | Lippincott
Williams & Wilkins www.co-anesthesiology.com
593
-
8/20/2019 C5. Chap10. Nouette-Gaulain
6/22
enhance mouse muscle regeneration during therecovery from
bupivacaine-induced injury [59].
Lastly, suspension of liposomes and micro-particles with
prolonged local anesthetic releaseare tested in animals but
inflammatory reactionswere observed. Local anesthetic in liposomes
ismainly used for analgesia and not for anesthesia
because these new galenic forms could reduce theinitial burst of
local concentration. Moreover, therelease of bupivacaine could
occur over severaldays [60
&
,61]. Indeed, very low concentrationsof bupivacaine seem to be
myotoxic if the durationof exposure is sufficiently prolonged.
Furtherinvestigations are still requested before humanuse.
CONCLUSION
Regional anesthesia improves analgesia after sur-gery,
facilitates postoperative rehabilitation, andenhances patient
satisfaction. Thus, the peripheralnerve catheter is a gold standard
for postoperativeanalgesia and it should be systematically
proposedto the patient when indicated despite the riskof toxicity.
In-situ toxicity induces histologicaldamage, metabolic alteration
with cell death andapoptosis, and functional dysfunction in
bothmuscle and neuron. Improving our practice withthe optimization
of our clinical protocol couldprevent from these side-effects;
antioxidant useand suspension of liposomes releasing local
anes-thetics over several hours remain in perspective
area.
Acknowledgements
None.
Conflicts of interest
There are no conflicts of interest.
REFERENCES AND RECOMMENDED
READINGPapers of particular interest, published within the
annual period of review, havebeen highlighted as:& of special
interest&& of outstanding interestAdditional references
related to this topic can also be found in the CurrentWorld
Literature section in this issue (p. 635).
1. Gomez-Arnau JI, Yanguela J, Gonzalez A, et al.
Anaesthesia-related diplopiaafter cataract surgery. Br J
Anaesth 2003; 90:189–193.
2. Han SK, Kim JH, Hwang JM. Persistent diplopia after
retrobulbar anesthesia.J Cataract Refract Surg 2004;
30:1248–1253.
3. Hogan Q, Dotson R, Erickson S, et al.
Local anesthetic myotoxicity: a caseand review.
Anesthesiology 1994; 80:942–947.
4. Brull R, McCartney CJ, Chan VW, El-Beheiry H.
Neurological complicationsafterregional anesthesia: contemporary
estimates of risk.Anesth Analg2007;104:965–974.
5. Neal JM,BernardsCM, HadzicA, et al. ASRAPractice
Advisory on neurologiccomplications in regional anesthesiaand pain
medicine. Regional Anesth PainMed 2008; 33:404–415.
6. Barrington MJ, Watts SA, Gledhill SR, et al.
Preliminary results of theAustralasian Regional Anaesthesia
Collaboration: a prospectiveaudit of morethan 7000 peripheral nerve
and plexus blocks for neurologic and othercomplications. Regional
Anesth Pain Med 2009; 34:534–541.
7. Auroy Y, Benhamou D, Bargues L, et al.
Major complications of regionalanesthesia in France: The SOS
Regional Anesthesia Hotline Service.Anesthesiology 2002;
97:1274–1280.
8. Politi PK, Havaki S, Manta P, Lyritis G.
Bupivacaine-induced regeneration ofrat soleus muscle:
ultrastructural and immunohistochemical aspects. Ultra-structural
Pathol 2006; 30:461–469.
9. Duguez S, Feasson L, Denis C, Freyssenet D.
Mitochondrial biogenesis
during skeletal muscle regeneration. Am J Physiol Endocrinol
Metab 2002;282:E802–E809.10. Zink W, Seif C, Bohl
JR, et al. The acute myotoxic effects of bupivacaine
and
ropivacaine after continuous peripheral nerve blockades. Anesth
Analg 2003;97:1173–1179.
11. Nouette-Gaulain K, Dadure C, Morau D, et al.
Age-dependent bupivacaine-induced muscle toxicity during a
continuous peripheral nerve block in rat.Anesthesiology 2009;
111:1120–1127.
12. Nouette-Gaulain K, Bellance N, Prevost B, et
al. Erythropoietin protectsagainst local anesthetic
myotoxicity during continuous regional analgesia.Anesthesiology
2009; 110:648–659.
13. Lirk P, Haller I, Colvin HP, et al. In
vitro, lidocaine-induced axonal injury isprevented by peripheral
inhibition of the p38 mitogen-activated protein kinase,but not by
inhibiting caspase activity. Anesth Analg 2007; 105:1657–1664.
14. Lirk P, Haller I, Colvin HP, et al. In
vitro, inhibition of mitogen-activated proteinkinase pathways
protects against bupivacaine- and ropivacaine-inducedneurotoxicity.
Anesth Analg 2008; 106:1456–1464.
15. Perez-Castro R, Patel S, Garavito-Aguilar ZV,
et al. Cytotoxicity of localanesthetics in human neuronal
cells. Anesth Analg 2009; 108:997–1007.
16.
&&
Yang S, Abrahams MS, Hurn PD, et al. Local anesthetic
Schwann cell toxicityis time and concentration dependent. Regional
Anesth Pain Med 2011;36:444–451.
Local anesthetics induced Schawnn cell death in time and
concentration-depen-dent manner. Prolonged extraneural infusion of
bupivacaine results in nerve injury.17. Lirk P, Haller I,
Myers RR, et al. Mitigation of direct neurotoxic
effects of
lidocaine and amitriptyline by inhibition of p38
mitogen-activated proteinkinase in vitro and in vivo.
Anesthesiology 2006; 104:1266–1273.
18. de Brito OM, Scorrano L. An intimate liaison: spatial
organization of the endo-plasmic reticulum-mitochondria
relationship. EMBO J 2010; 29:2715– 2723.
19. Zink W, Graf BM, Sinner B, et al.
Differential effects of bupivacaineon intracellular Ca2þ
regulation: potential mechanisms of its myotoxicity.Anesthesiology
2002; 97:710–716.
20. Komai H, Lokuta AJ. Interaction of bupivacaine and
tetracaine with thesarcoplasmic reticulum Ca2þ release channel of
skeletal and cardiac muscles.Anesthesiology 1999; 90:835–843.
21. Viner RI, Ferrington DA, Williams TD, et al.
Protein modification duringbiological aging: selective
tyrosine nitration of the SERCA2a isoform of
the sarcoplasmic reticulum Ca2þ
-ATPase in skeletal muscle. Biochem J1999; 340:657–669.22.
Xu L, Eu JP,MeissnerG, Stamler JS. Activation ofthe cardiac
calcium release
channel (ryanodine receptor) by poly-S-nitrosylation. Science
1998;279:234–237.
23. Nouette-Gaulain K, Sirvent P, Canal-Raffin M,
et al. Effects of intermittentfemoral nerve injections of
bupivacaine, levobupivacaine, and ropivacaine onmitochondrial
energy metabolism and intracellular calcium homeostasis in ratpsoas
muscle. Anesthesiology 2007; 106:1026–1034.
24. Gold MS, Reichling DB, Hampl KF, et
al. Lidocaine toxicity in primary afferentneurons from the
rat. J Pharmacol Exp Therapeut 1998; 285:413–421.
25. Johnson ME, Saenz JA, DaSilva AD, et al.
Effect of local anesthetic onneuronal cytoplasmic calcium
and plasma membrane lysis (necrosis) in acell culture model.
Anesthesiology 2002; 97:1466–1476.
26. Kanai A, Hiruma H, Katakura T, et al.
Low-concentration lidocaine rapidlyinhibits axonal transport in
cultured mouse dorsal root ganglion neurons.Anesthesiology 2001;
95:675–680.
27. Nouette-Gaulain K, Jose C, Capdevila X, Rossignol R.
From analgesia tomyopathy: when local anesthetics impair the
mitochondrion. Int J BiochemCell Biol 2011; 43:14–19.
28. Nouette-Gaulain K, Quinart A, Letellier T, Sztark F.
La mitochondrie: rôles etimplications en anesthésie-réanimation.
Annales francaises d’anesthesie etde reanimation 2007;
26:319–333.
29. Zink W, Graf BM. Local anesthetic myotoxicity.
Regional Anesth Pain Med2004; 29:333–340.
30. Benard G, Faustin B, Passerieux E, et
al. Physiological diversity of mitochon-drial oxidative
phosphorylation. Am J Physiol Cell Physiol 2006;
291:C1172–C1182.
31. Johnson ME, Uhl CB, Spittler KH, et al.
Mitochondrial injury and caspaseactivation by the local
anesthetic lidocaine. Anesthesiology 2004;101:1184–1194.
32.
&
Arsac LM, Nouette-Gaulain K, Miraux S, et al. Acute
and chronic effects ofbupivacaine on muscle energetics during
contraction in vivo: a modularmetabolic control analysis. Biochem J
2012; 444:315–321.
Bupivacaine did notinduce a difference in elasticitiesand
suggests theabsence ofdysfunction in energetic control of muscle
contraction energetics.
Regional anesthesia
594 www.co-anesthesiology.com Volume 25
Number 5 October 2012
-
8/20/2019 C5. Chap10. Nouette-Gaulain
7/22
33. Cela O, Piccoli C, Scrima R, et
al. Bupivacaine uncouples the mitochondrialoxidative
phosphorylation, inhibits respiratory chain complexes I and III
andenhances ROS production: results of a study on cell cultures.
Mitochondrion2010; 10:487–496.
34. Galbes O, Bourret A, Nouette-Gaulain K, et al.
N-acetylcysteine protectsagainst bupivacaine-induced
myotoxicity caused by oxidative and sarcoplas-mic reticulum stress
in human skeletal myotubes. Anesthesiology 2010;113:560–569.
35.
&
Lu J, Xu SY,ZhangQG, LeiHY. Bupivacaine induces reactive
oxygenspeciesproduction via activation of the AMP-activated protein
kinase-dependentpathway. Pharmacology 2011; 87:121–129.
Bupivacaine induced cell apoptosis via the ROS production and
AMPK.36. Claret M, Smith MA, Batterham RL, et al.
AMPK is essential for energyhomeostasis regulation and
glucose sensing by POMC and AgRP neurons.J Clin Investig 2007;
117:2325–2336.
37. Marchi S, GiorgiC, Suski JM, et al.
Mitochondria-roscrosstalkin the control ofcell death and aging. J
Signal Transduction 2012; 2012:329635.
38. Werdehausen R, Fazeli S, Braun S, et al.
Apoptosis induction by differentlocal anaestheticsin a
neuroblastoma cell line. Br J Anaesth 2009; 103:711–718.
39. Werdehausen R, Braun S, Essmann F, et al.
Lidocaine induces apoptosisvia the mitochondrial pathway
independently of death receptor signaling.Anesthesiology 2007;
107:136–143.
40. Park CJ, Park SA, Yoon TG, et
al. Bupivacaine induces apoptosis via ROS inthe Schwann cell
line. J Dental Res 2005; 84:852–857.
41. Unami A, Shinohara Y, Ichikawa T, Baba Y. Biochemical
and microarrayanalyses of bupivacaine-induced apoptosis. J Toxicol
Sci 2003; 28:77–94.
42.
&
LuJ, XuSY,Zhang QG, et al. Bupivacaine induces apoptosis via
mitochondriaand p38 MAPK dependent pathways. Eur J Pharmacol 2011;
657:51–58.
Bupivacaine induced reactive oxygen species leading to
mitchondrial depolariza-
tion and the p38 MAPK activation.43. Maurice JM, Gan Y, Ma
FX, et al. Bupivacaine causes cytotoxicity in
mouse
C2C12 myoblast cells: involvement of ERK and Akt signaling
pathways. ActaPharmacol Sin 2010; 31:493–500.
44. Ma R, Wang X, Lu C, et al. Dexamethasone
attenuated bupivacaine-inducedneuron injury in vitro through a
threonine-serine protein kinase B-dependentmechanism. Neuroscience
2010; 167:329–342.
45.
&
Jose C, Bellance N, Chatelain EH, et al.
Antiproliferative activity of levobu-pivacaine and aminoimidazole
carboxamide ribonucleotide on human cancercells of variable
bioenergetic profile. Mitochondrion 2012; 12:100–109.
Effects of levobupivacaine were evaluated on human cancer cells.
Bioenergeticstate of cell determines in part the impact of
levopivacaine on cell viability.46. Nouette-Gaulain K,
Bringuier S, Canal-Raffin M, et al. Time course of
mito-
chondrial metabolism alterations to repeated injections of
bupivacaine in ratmuscle. Can J Anaesth 2010; 57:836–842.
47. Muguruma T, Sakura S, Saito Y. Epidural lidocaine
induces dose-dependentneurologic injury in rats. Anesth Analg 2006;
103:876–881.
48. Nakamura T, Popitz-Bergez F, Birknes J, Strichartz GR.
The critical role ofconcentration for lidocaine block of peripheral
nerve in vivo: studies offunction and drug uptake in the rat.
Anesthesiology 2003; 99:1189–1197.
49. KasabaT, Onizuka S, Takasaki M. Procaine andmepivacainehave
less toxicityin vitro than other clinically used local anesthetics.
Anesth Analg 2003;97:85–90.
50. Radwan IA, Saito S, Goto F. The neurotoxicityof local
anesthetics on growingneurons: a comparative study of lidocaine,
bupivacaine, mepivacaine, andropivacaine. Anesth Analg 2002;
94:319–324.
51.
Yamashita A, Matsumoto M, Matsumoto S, et al.
A comparison of theneurotoxic effects on the spinal cord
of tetracaine, lidocaine, bupivacaine,and ropivacaine administered
intrathecally in rabbits. Anesth Analg 2003;97:512–519.
52. Malinovsky JM, Charles F, Baudrimont M, et al.
Intrathecal ropivacaine inrabbits: pharmacodynamicand
neurotoxicologic study. Anesthesiology 2002;97:429–435.
53. Sakura S, Kirihara Y, Muguruma T, et al.
The comparative neurotoxicity ofintrathecal lidocaine and
bupivacaine in rats. Anesth Analg 2005; 101:541–547.
54. Sztark F, Malgat M, Dabadie P, Mazat JP. Comparison
of the effectsof bupivacaine and ropivacaine on heart cell
mitochondrial bioenergetics.Anesthesiology 1998; 88:1340–1349.
55. Bouaziz H, Iohom G, Estebe JP, et al.
Effects of levobupivacaine andropivacaine on rat sciatic nerve
blood flow. Br J Anaesth 2005; 95:696–700.
56. Benard G, Trian T, Bellance N, et al.
Adaptative capacity of mitochondrialbiogenesis and of mitochondrial
dynamics in response to pathogenic respira-tory chain dysfunction.
Antioxidants Redox Signal 2012 (in press).
57. Nouette-Gaulain K, Forestier F, Malgat M, et
al. Effects of bupivacaine on
mitochondrial energymetabolism in heartof ratsfollowing exposure
to chronichypoxia. Anesthesiology 2002; 97:1507–1511.
58. Wang X, Zhang X, Cheng Y, et al.
Alpha-lipoic acid prevents bupivacaine-induced neuron injury in
vitro through a PI3K/Akt-dependent mechanism.Neurotoxicology 2010;
31:101–112.
59. White JP, Baltgalvis KA, Sato S, et al.
Effect of nandrolone decanoateadministration on recovery from
bupivacaine-induced muscle injury. J ApplPhysiol 2009;
107:1420–1430.
60.
&
Richard BM, Newton P, Ott LR, et al. The safety of
Exparel (R) (bupivacaineliposome injectable suspension)
administered by peripheral nerve block inrabbits and dogs. J Drug
Deliv 2012; 2012:962101.
Exparel is a sustained-releaseinjectionformulation of
bupivacaine.Exparel inducedminimal to mild granulomatous
inflammation around nerve roots.61. Padera R, Bellas E, Tse
JY, et al. Local myotoxicity from sustained release
of
bupivacaine from microparticles. Anesthesiology 2008;
108:921–928.
Local anesthetic in-situ toxicity Nouette-Gaulain et
al.
0952-7907 2012 Wolters Kluwer Health | Lippincott
Williams & Wilkins www.co-anesthesiology.com
595
-
8/20/2019 C5. Chap10. Nouette-Gaulain
8/22
Emulsions lipidiques intraveineuses : où en est-on ?
Karine Nouette-Gaulain1, Xavier Capdevila2, Florian Robin1,
Hélène Beloeil3
1. Laboratoire Maladies Rares: Génétique et Métabolisme (MRGM),
Université
Segalen Bordeaux 2, F-33076 Bordeaux, France; CHU Bordeaux,
Pôle
d’Anesthésie Réanimation, Centre François Xavier Michelet,
F-33076 Bordeaux
2. CHU Montpellier, Service d’Anesthésie Réanimation A
3. CHU Rennes, Pôle d’Anesthésie Réanimation
Les points essentiels
L’anesthésie régionale est en plein essor et le risque de
toxicité systémique augmente
avec le nombre des indications.
L’intérêt des émulsions lipidiques intraveineuses a été souligné
dans de nombreux cas
cliniques et études expérimentales. Une réduction du temps
nécessaire pour un retour
à un état hémodynamique stable et une amélioration du taux de
survie sont
classiquement décrits sur les modèles animaux. Le manque
d’études chez l’homme estresponsable du faible niveau de
preuve.
Le mécanisme d’action de l’interaction entre une émulsion
lipidique intraveineuse (ELI)
et un anesthésique local (AL) est mal connu, et est à l’origine
d’une controverse. Les
interactions ELI-AL pourraient être secondaires à un phénomène
de piège lipidique
intravasculaire mais également pourraient s’expliquer par des
modifications
métaboliques intracellulaires et par une modulation de l’action
de l’anesthésique localsur le canal sodique.
L’interaction entre une émulsion lipidique intraveineuse et un
anesthésique local
pourrait être modifiée par de fortes doses d’adrénaline, par une
hypoxie et une acidose.
Les émulsions lipidiques intraveineuses sont recommandées par
l’ASRA et par la SFAR
lors d’une réanimation d’un arrêt cardio-respiratoire induit par
un surdosage systémique
en anesthésique local.
-
8/20/2019 C5. Chap10. Nouette-Gaulain
9/22
Les émulsions lipidiques intraveineuses pourraient probablement
être utilisées lors d’un
surdosage en bêtabloquants, inhibiteurs calciques, amiodarone,
psychotropes. Le
risque lié à l’utilisation d’une émulsion lipidique
intraveineuse est peu décrit.
-
8/20/2019 C5. Chap10. Nouette-Gaulain
10/22
Les interactions entre les agents lipophiles et les émulsions
lipidiques intraveineuses
(ELI) sont connues depuis 1962 : la durée d’une anesthésie par
thiopental serait réduite
lors de l’administration d’une émulsion lipidique chez le rat
[1]. En 1998, l’équipe de
Guy Weinberg décrit les premières interactions entre la
bupivacaïne et les ELI [2].
Deux types de résultats sont obtenus :i) Après un prétraitement
par Intralipid ®
chez desrats, la dose toxique de bupivacaïne entrainant un
arrêt cardio-respiratoire est
significativement plus élevée que chez des rats contrôles
recevant uniquement du
sérum salé, ii) Lors d’un arrêt cardio-respiratoire induit par
une dose toxique de
bupivacaïne, le taux de mortalité des rats est significativement
plus faible s’ils reçoivent
une solution d’Intralipid ® lors de la réanimation. Suite à
ces résultats, de nombreux
travaux expérimentaux complémentaires ont exploré les mécanismes
d’action qui
pourraient expliquer ces phénomènes et la littérature a été
enrichie à partir de 2006 parla publication de nombreux cas
cliniques soulignant les effets bénéfiques des ELI [3].
Les ELI ont ainsi trouvé progressivement une indication dans le
traitement d’un
surdosage en anesthésique local (AL) puis dans les
recommandations internationales
[4, 5]. Mais, l’absence d’étude humaine randomisée et
l’hétérogénéité des résultats des
études expérimentales ont donné naissance à une controverse
concernant les effets
bénéfiques des interactions ELI-AL. Ces différents points seront
abordés
successivement dans cette revue.
1. Les mécanismes pouvant être impliqués dans l’interaction
ELI-AL
Suite aux effets d’une injection d’ELI sur la toxicité induite
par la bupivacaïne chez le
rat, ces résultats ont ensuite été retrouvés sur cœur isolé [6]
et sur des chiens au cours
d’une anesthésie générale [7]. Les mécanismes impliqués dans
cette prévention, voir
protection, ne sont pas clairement connus. Plusieurs hypothèses
sont décrites, parfois
complémentaires les unes des autres.
Pharmacocinétique des anesthésiques locaux
Avant d’aborder ces hypothèses, faisons un bref rappel sur la
pharmacocinétique des
AL. Les AL sont des molécules liposolubles, mais dont la
liposolubilité varie en fonction
de la molécule. Dans le sang, les AL sont globalement soient
liés à une protéïne
(l’albumine, l’alpha-1 glyco-protéine), soit libres et
responsables de la toxicité
systémique. Le métabolisme est essentiellement hépatique. Lors
d’une administration
-
8/20/2019 C5. Chap10. Nouette-Gaulain
11/22
intravasculaire accidentelle d’AL, l’AL va dans un premier temps
diffuser dans les
organes richement perfusés (le cœur, le cerveau), puis dans les
organes peu perfusés
tels la graisse[8].
L’hypothèse du piège lipidiqueL’interaction entre l’ELI et les
AL pourraient s’expliquer par la formation d’un piège
lipidique. En utilisant des méthodes de microcalorimétrie, le
type de liaison entre ELI et
AL serait probablement de nature entropique [9].
Sur cœur isolé de rat, l’administration d’ELI est associée une
récupération rapide de la
contraction cardiaque et à une diminution de la concentration
tissulaire de bupivacaïne
radio marquée [6]. Des études in vitro basée sur la
colorimétrie [10] et sur l’étude des
liaisons ELI-AL [9] sont en faveur de l’hypothèse du piège
lipidique. Suite à des étudesexpérimentales, la modélisation
pharmacocinétique d’une injection intravasculaire de
bupivacaïne suggère qu’une administration d’ELI diminue de 11%
la concentration
tissulaire de bupivacaïne dans le cœur 3 minutes après
l’injection d’ELI, et de 18%
dans le cerveau, 15 min après la fin de l’injection [8]. En
revanche, la concentration de
bupivacaïne dans le tissu adipeux augmenterait. Dans ce modèle,
l’injection d’ELI
s’accompagnerait d’une augmentation de la concentration
plasmatique totale de
bupivacaïne associée à une diminution de la concentration de la
fraction libre. Ces
résultats suggèrent une liaison des AL avec l’ELI. Tandis que le
délai de 3 minutes est
compatible avec l’hypothèse du piège lipidique et avec les
résultats décrits dans les cas
cliniques, le délai d’action de 15 minutes au niveau du cerveau
laisse supposer
l’implication d’autres phénomènes in vivo .
L’implication probable du métabolisme cellulaire
En 1961, Shipp et al . démontre que les lipides sont les
substrats énergétiques
essentiels pour le cardiomyocytes [11]. Les lipides sont
métabolisés via le cycle de la
béta-oxydation et vont fournir les substrats essentiels pour la
synthèse de l’ATP
mitochondrial.
Sur un modèle de rat in vivo et sur un cœur isolé de rat soumis
à un phénomène
d’ischémie-reperfusion, l’administration d’une ELI va diminuer
la taille de l’infarctus du
myocarde induite par l’ischémie, cet effet cytoprotecteur étant
significativement plus
important que celui induit par la cyclosporine A [12]. Ce
phénomène observé lors de la
-
8/20/2019 C5. Chap10. Nouette-Gaulain
12/22
reperfusion du myocarde est associé à l’activation de kinases
favorisant la
cytoprotection, telles la phosphorylation de l’Akt et de la
GSK-3béta.
Par opposition, les anesthésiques locaux à des fortes
concentrations interagissent
également avec le métabolisme mitochondrial en inhibant le
transport des acides gras à
chaîne longue, en diminuant le potentiel de membrane et la
synthèse d’ATPmitochondriale [13, 14].
En combinant les différents effets, la charge rapide en acide
gras apportée par
l’administration d’ELI pourrait compenser le blocage métabolique
induit par les AL.
Cette théorie a été suggérée par les travaux de l’équipe de
Stehr et al [15]. Sur cœur
isolé de rat, un apport supplémentaire en acide gras permettait
de réduire l’altération de
la fonction cardiaque induite par la bupivacaïne. Cette théorie
métabolique
mitochondriale vient d’être complétée par une étude évaluant
l’effet d’un blocagespécifique du métabolisme lipidique en
association à un surdosage en AL avec
administration d’ELI [16]. In vivo, un blocage spécifique du
métabolisme lipidique par
une concentration élevée de CVT-4325 lors d’un protocole
bupivacaïne(10mg/kg IV)-
ELI chez des rats induit un effondrement majeur de la fréquence
cardiaque, de la
fraction d’éjection et de la fraction de raccourcissement. Cela
suggère donc qu’un
prétraitement par CVT-4325 abolit l’effet d’une ELI et que le
métabolisme des acides
gras est impliqué dans l’interaction protectrice ELI-AL.
Mais d’autres voies de signalisation peuvent également être
impliquées.
L’administration d’ELI après une asystolie induite par une dose
toxique d’AL chez le rat
pourrait permettre de préserver le métabolisme calcique et
d’inhiber l’ouverture du PTP
[16]. De plus , les acides gras pourraient interférer sur
l’action des AL sur le canal
sodique [17]. Sur culture cellulaire (HEK-293 cells),
l’association acide gras-
bupivacaïne diminue significativement le bloc tonique et le bloc
phasique, par
comparaison au bloc induit par la bupivacaïne seule. Cet effet
direct sur le canal
sodique pourrait moduler également la toxicité induite par la
bupivacaïne et pourrait
contribuer à une protection cellulaire.
L’effet de l’ELI sur les paramètres hémodynamiques
Lors d’un surdosage toxique systémique d’AL, les signes
cardiovasculaires
couramment décrits sont les troubles de la conduction, les
troubles du rythme, se
compliquant d’une asystolie, une diminution de la fraction
d’éjection et de la fraction de
-
8/20/2019 C5. Chap10. Nouette-Gaulain
13/22
raccourcissement, un effondrement du débit cardiaque et des
résistances vasculaires
systémiques.
En absence d’AL, l’administration isolée d’ELI chez le rat
augmente significativement le
flux aortique et la pression artérielle par rapport à une
administration de sérum salé
isotonique.
En conclusion, les interactions ELI-AL pourraient être
secondaires à un phénomène de
piège lipidique intravasculaire mais également pourraient
s’expliquer par des
modifications métaboliques intracellulaires et une modulation de
l’action de l’AL sur le
canal sodique.
2. La controverse concernant les interactions entre des
émulsions lipidiques etles anesthésiques locaux
Les résultats controversés des études expérimentales
Tandis que les résultats sur les modèles murins, lapins ou
chiens sont assez
homogènes [18], les expérimentations réalisées chez le cochon ne
mettent pas en
évidence un effet bénéfique de l’interaction ELI-AL. Dans ce
dernier modèle, la liaison
ELI-AL n’est pas démontrée et aucune amélioration du taux de
survie n’est observée
chez les animaux recevant une ELI [19].
Chez le volontaire sain au cours d’une étude prospective
randomisée, une injection
intraveineuse de bupivacaïne 0,5 mg/kg a été réalisée en 20
minutes, suivie d’une
administration d’Intralipid ® 20% (bolus de
1,5ml/kg en 1min puis 29 min de perfusion
continue à 0,25ml/kg/min), le groupe contrôle recevait de la
bupivacaïne et du sérum
salé isotonique [20]. La valeur de la concentration plasmatique
de bupivacaïne (total et
libre) diminuait légèrement. Le seuil des concentrations
toxiques de la bupivacaïne
n’étant pas atteint, les mécanismes de protection ne sont
probablement pas saturés, et
la différence significative entre les traitements est donc
probablement difficile à mettre
en évidence.
Le rôle du terrain
-
8/20/2019 C5. Chap10. Nouette-Gaulain
14/22
La toxicité des anesthésiques locaux est majorée en cas
d’hypoxie et d’acidose. De
plus ces deux paramètres pourraient influencer l’action d’une
injection d’ELI. Ainsi,
l’injection d’ELI doit s’intégrer dans une stratégie de
réanimation avec injection d’agent
vaso-actif et des objectifs stricts.
Lors d’une asystolie induite par la bupivacaïne sur cœur isolé
de rat, larécupération de la fonction cardiaque initiale est
meilleure si l’organe bénéficie d’une
association adrénaline (0,15 mcg/kg) et ELI, plutôt que d’un
seul des deux traitements
[21]. En revanche, l’équipe de Guy Weinberg démontre qu’une
injection d’ELI a un effet
significativement meilleur que l’injection d’adrénaline (30
mcg/kg) au cours d’une
réanimation cardio-vasculaire chez le rat [22] . Ces résultats
discordants pourraient
s’expliquer par la différence de posologies d’adrénaline
utilisée et donc par l’effet use-
dependence démontré dans d’anciens travaux : les
posologies d’adrénaline utiliséesseraient au delà d’un certain
seuil, et donc trop élevées pour être bénéfiques. Cette
hypothèse a été confirmée dans une étude complémentaire où
différentes posologies
d’adrénaline (1-2,5-10 et 25 mcg/kg) ont été évaluées[23]. Chez
les rats, des doses
d’adrénaline supérieures à 10mcg/kg s’accompagnaient d’une
élévation des lactates,
d’une acidose sévère, rendant la réanimation plus complexe et
moins performante [23].
L’interaction ELI-AL semblerait modifiée en cas d’hypoxie. En
effet, dans les
deux études suivantes, des doses d’adrénaline entre 40 et 200
mcg/kg se révèlent plus
efficaces que l’ELI si une période d’hypoxie est appliquée à
l’animal. Ainsi, si l’injection
de 5 mg/kg de bupivacaïne 0,5% est suivie d’une période
d’hypoxie d’une à deux
minutes, le taux de survie des rats est meilleur dans le groupe
adrénaline-vasopressine
que dans le groupe ELI seule [24]. De même, sur un modèle de
lapin avec clampage de
la trachée lors d’une injection toxique de bupivacaïne, la
réanimation (ventilation,
massage cardiaque, adrénaline) d’un ACR est moins performante si
une ELI est
administrée chez l’animal, le groupe témoin recevant du sérum
salé [25].
Le pH pourrait également modifier l’interaction ELI-AL. Après
injection de
10mg/kg de bupivacaïne chez le porc, une réanimation est
réalisée avec ventilation,
massage cardiaque et adrénaline. Une injection d’ELI ou de sérum
salé isotonique est
ensuite réalisée. Dans les deux groupes, le taux de survie n’est
significativement
différent. En revanche, l’analyse des résultats révèle une
acidose majeure lors de la
réanimation des animaux, suggérant une interaction entre
l’acidose et l’administration
d’ELI possible [26].
-
8/20/2019 C5. Chap10. Nouette-Gaulain
15/22
L’ensemble de ces résultats suggère une titration des doses
d’adrénaline, des
objectifs de normoxie et normocapnie lors d’une réanimation
d’une asystolie induite par
les AL.
Propriétés biochimiques des ELI et AL : quel rôle
?Schématiquement, les ELI sont composées d’acides gras à chaîne
longue (exemple
Intralipid ® ) ou d’un mélange chaîne longue et chaîne
intermédiaire (exemple
Medialipid ® ). Les propriétés liposolubles sont
différentes pour chaque AL. Des études in
vitro ont évalué l’interaction ELI-AL en fonction des propriétés
de chaque solution. En
présence d’une solution tampon, la solubilité et la capacité de
liaison d’une solution
d’acides gras à chaîne longue sont significativement meilleures
que celles d’une
solution comprenant un mélange d’acide gras à chaîne longue et
intermédiaire [9]. Enrevanche, en présence de sérum humain, une ELI
composée d’un mélange d’acides
gras à chaîne longue et intermédiaire paraitrait plus
performante pour séquestrer les
AL[27]. Il paraît donc difficile de conclure au vu des résultats
très divergents de ces
études in vitro. Testée chez le rat, cette hypothèse serait en
faveur d’une ELI composée
uniquement d’acides gras à chaîne longue : le taux de rats
survivant à une réanimation
classique est supérieur dans le groupe
Intralipid ® que dans le groupe recevant une
ELI
composée d’un mélange acides gras à chaîne longue et
intermédiaire [28]. Chez le
cochon, les deux ELI (Intralipid ® et un
mélange acides gras à chaîne longue et
intermédiaire) permettaient une meilleure récupération des
paramètres cardiaques et
hémodynamiques que dans le groupe sérum salé isotonique, mais le
manque de
puissance de l’étude ne permet pas de mettre en évidence une
différence significative
entre les ELI [29].
3. Place des émulsions lipidiques dans les recommandations
professionnelles
lors d’un surdosage systémique en anesthésique local
Anesthésiques Locaux et risque de toxicité systémique
L’administration locale d’AL peut se compliquer d’une injection
directe vasculaire ou
d’une diffusion vasculaire passive, les deux cas conduisant à un
surdosage toxique
systémique d’AL. Ces surdosages sont caractérisés par des signes
neurologiques et/ou
cardiaques dont les cas les plus sévères conduisent à des
convulsions, un coma et/ou
un arrêt cardio-respiratoire.
-
8/20/2019 C5. Chap10. Nouette-Gaulain
16/22
Aujourd’hui, une quarantaine de cas cliniques publiés souligne
l’effet bénéfique d’une
administration d’ELI lors de la survenue d’un surdosage en AL,
tels que la bupivacaïne
et la ropivacaïne, chez la plupart des patients. Dans le premier
cas clinique publié en
2006, un homme de 58 ans avait bénéficié d’un bloc
interscalénique avec mépivacaïne
et bupivacaïne [3]. A la fin du bloc, le patient a présenté des
signes neurologiquesgraves puis un arrêt cardio-respiratoire. Après
20 minutes de réanimation et la
persistance d’une instabilité hémodynamique, l’administration de
100 ml d’Intralipid ®
20% a été suivie par une amélioration très rapide des paramètres
hémodynamiques et
électriques, le patient ne présentant par la suite aucune
complication neurologique. Ces
résultats ont été décrits chez les adultes, mais également chez
des enfants, dès la
période néonatale [30]. Très schématiquement, lors d’une
réanimation standard
survenant après un surdosage en AL, tandis que le patient est
massé avec injectiond’adrénaline, oxygéné et ventilé,
l’administration complémentaire d’ELI s’accompagne
le plus souvent d’une amélioration des signes cliniques dans un
délai rapide d’environ 5
à 10 minutes.
Nous devons cependant rester vigilants sur les relations de
causes à effets car : i) une
sous-estimation du nombre d’échecs de la thérapie par ILE ne
peut pas être exclues, ii)
les études prospectives et randomisées sur ce sujet ne sont pas
possibles
Les Recommandations internationales
Ainsi depuis plusieurs années, l’ « American Society of Regional
Anesthesia and Pain
Medicine » a publié une check list à suivre en cas
d’arrêt cardio-respiratoire induit par
une injection toxique d’AL. Cinq points sont clairement
identifiés en 2012 [4] :
Appel à l’aide
Démarche initiale
o Gestion des voies aériennes et ventilation avec 100%
d’oxygène
o Prise en charge des troubles neurologiques graves : les
benzodiazépines
en premier lieu, et ne pas injecter de propofol
o Organiser la possibilité d’une CEC
Prise en charge de l’asystolie
o Massage cardiaque prolongé
o Eviter la vasopressine, les inhibiteurs calciques, les
béta-bloquants, ou
d’autres anesthésiques locaux
o Titration des doses d’adrénaline (
-
8/20/2019 C5. Chap10. Nouette-Gaulain
17/22
Traitement par ELI (20%)
o Bolus initial de 1,5 ml/kg IV en 1 minute
o Perfusion continue de 0,25 ml/kg/min
o Répéter le bolus une ou deux fois en cas de collapsus
cardiovasculaire
persistanto Perfusion continue au moins 10 min après le
retour à un équilibre
hémodynamique satisfaisant
o Eviter de dépasser la dose maximale de 10ml/kg au cours
des 30
premières minutes
Déclaration de l’événement indésirable grave sur le
site
http://www.lipidrescue.org/
Finalement, les auteurs proposent une surveillance prolongée
supérieure à 12 heures,
justifiée par un risque de récidive à l’arrêt de
l’ELI.
Les recommandations disponibles sur le site de la SFAR
(http://www.sfar.org/accueil/article/340/toxicite-systemique-aigue-des-anesthesiques-
locaux) diffèrent en quelques points, dont le recours non
indispensable à la perfusion
continue et la durée de surveillance réduite à 6 heures.
4. Risques et perspectives
Perspectives
Aujourd’hui, la littérature a été enrichie de cas cliniques au
cours desquels l’ELI a été
utilisée pour antagoniser des surdosages d’autres agents
liposolubles [31]. Ainsi, les
ELI ont été utilisées en cas de surdosages en bêtabloquants, en
amiodarone, en
inhibiteurs calciques, en psychotropes. Mais la description des
interactions ELI-agents
liposolubles a les mêmes limites que celles décrites avec les AL
: peu d’études sur
modèle animal, essentiellement des cas cliniques. De plus, se
pose le problème du
patient qui arrive aux urgences pour une prise médicamenteuse
dont la nature n’est pas
connue : existe t’il un risque à administrer une ELI ?
Risques liés à une perfusion d’ELI
-
8/20/2019 C5. Chap10. Nouette-Gaulain
18/22
En cas de surdosage systémique en AL, il est recommandé d’éviter
de dépasser la
dose maximale de 10ml/kg au cours des 30 premières minutes.
Cette recommandation
peut s’expliquer sur les arguments suivants. Sur modèle animal,
la perfusion d’ELI lors
d’un arrêt cardio-respiratoire induit par un surdosage en AL va
majorer la
vasoconstriction et l’hyperlactatémie induite par l’adrénaline
[23]. Lors d’uneantagonisation d’un surdosage en amiodarone avec
une ELI, une coloration cutanée
rouge est parfois décrite. Lors d’injection de grand volume
d’ELI chez le rat, une
élévation des triglycérides est observée au cours des 48
premières heures, associée à
une élévation de l’amylase et des ASAT [32]. Ces résultats
biologiques sont décrits
dans certains cas cliniques [5]. En histologie chez le rat, une
administration de 60 à
80ml/kg en 30 minutes d’ELI s’accompagne de lésions
histologiques au niveau des
poumons (infiltration de neutrophiles et microhémorragies
intra-alvéolaires) et du foie(stéatose micro vasculaire) [32]. Si
nous gardons en tête que le facteur de conversion
théorique des doses d’ELI entre le rat et l’homme recommandée
par la FDA est de 6, il
est justifié de ne pas dépasser la dose maximale de 10ml/kg au
cours des 30 premières
minutes [12].
5. Conclusion
Au vu des données issues des études expérimentales et des cas
cliniques, les ELI font
aujourd’hui partie des recommandations à suivre lors d’un arrêt
cardio-respiratoire
induit par un surdosage systémique en anesthésique local. Les
ELI ne doivent pas être
substituées aux autres moyens de réanimation, mais sont un
élément supplémentaire.
Des études expérimentales complémentaires et un registre de cas
cliniques permettront
probablement de mieux caractériser l’interaction ELI-AL et de
mieux connaître les
éléments qui aujourd’hui amènent parfois à des controverses. De
même, des travaux
complémentaires permettront de mieux définir la place des ELI au
cours de surdosages
avec d’autres agents liposolubles.
-
8/20/2019 C5. Chap10. Nouette-Gaulain
19/22
Références bibliographiques
1. Russell RL, Westfall, B.A. Alleviation of barbiturate
depression. Anesthesia
Analgesia 1962; 41:582-5.2. Weinberg GL, VadeBoncouer T,
Ramaraju GA, Garcia-Amaro MF, Cwik MJ.
Pretreatment or resuscitation with a lipid infusion shifts the
dose-response to
bupivacaine-induced asystole in rats. Anesthesiology 1998;
88:1071-5.
3. Rosenblatt MA, Abel M, Fischer GW, Itzkovich CJ, Eisenkraft
JB. Successful use
of a 20% lipid emulsion to resuscitate a patient after a
presumed bupivacaine-related
cardiac arrest. Anesthesiology 2006; 105:217-8.
4. Neal JM, Mulroy MF, Weinberg GL. American Society of Regional
Anesthesiaand Pain Medicine checklist for managing local anesthetic
systemic toxicity: 2012
version. Reg Anesth Pain Med 2012; 37:16-8.
5. Weinberg GL. Lipid emulsion infusion: resuscitation for local
anesthetic and other
drug overdose. Anesthesiology 2012; 117:180-7.
6. Weinberg GL, Ripper R, Murphy P, Edelman LB, Hoffman W,
Strichartz G,
Feinstein DL. Lipid infusion accelerates removal of bupivacaine
and recovery from
bupivacaine toxicity in the isolated rat heart. Reg Anesth Pain
Med 2006; 31:296-303.
7. Weinberg G, Ripper R, Feinstein DL, Hoffman W. Lipid emulsion
infusion
rescues dogs from bupivacaine-induced cardiac toxicity. Reg
Anesth Pain Med 2003;
28:198-202.
8. Kuo I, Akpa BS. Validity of the lipid sink as a mechanism for
the reversal of local
anesthetic systemic toxicity: a physiologically based
pharmacokinetic model study.
Anesthesiology 2013; 118:1350-61.
9. Mazoit JX, Le Guen R, Beloeil H, Benhamou D. Binding of
long-lasting local
anesthetics to lipid emulsions. Anesthesiology 2009;
110:380-6.
10. Papadopoulou A, Willers JW, Samuels TL, Uncles DR. The use
of dye
surrogates to illustrate local anesthetic drug sequestration by
lipid emulsion: a visual
demonstration of the lipid sink effect. Reg Anesth Pain Med
2012; 37:183-7.
11. Shipp JO, LH; Challoner,D. Fatty acid and glucose metabolism
in the perfused
heart. Nature 1961; 189:1018-9.
-
8/20/2019 C5. Chap10. Nouette-Gaulain
20/22
12. Fettiplace MR, Ripper R, Lis K, Lin B, Lang J, Zider B, Wang
J, Rubinstein I,
Weinberg G. Rapid Cardiotonic Effects of Lipid Emulsion
Infusion*. Crit Care Med
2013; 41:e156-e62.
13. Nouette-Gaulain K, Bellance N, Prevost B, Passerieux E,
Pertuiset C, Galbes O,
Smolkova K, Masson F, Miraux S, Delage JP, Letellier T,
Rossignol R, Capdevila X,Sztark F. Erythropoietin protects against
local anesthetic myotoxicity during continuous
regional analgesia. Anesthesiology 2009; 110:648-59.
14. Nouette-Gaulain K, Forestier F, Malgat M, Marthan R, Mazat
JP, Sztark F.
Effects of bupivacaine on mitochondrial energy metabolism in
heart of rats following
exposure to chronic hypoxia. Anesthesiology 2002;
97:1507-11.
15. Stehr SN, Ziegeler JC, Pexa A, Oertel R, Deussen A, Koch T,
Hubler M. The
effects of lipid infusion on myocardial function and
bioenergetics in l-bupivacaine toxicityin the isolated rat heart.
Anesth Analg 2007; 104:186-92.
16. Partownavid P, Umar S, Li J, Rahman S, Eghbali M. Fatty-acid
oxidation and
calcium homeostasis are involved in the rescue of
bupivacaine-induced cardiotoxicity by
lipid emulsion in rats. Crit Care Med 2012; 40:2431-7.
17. Mottram AR, Valdivia CR, Makielski JC. Fatty acids
antagonize bupivacaine-
induced I(Na) blockade. Clin Toxicol (Phila) 2011;
49:729-33.
18. Jamaty C, Bailey B, Larocque A, Notebaert E, Sanogo K,
Chauny JM. Lipid
emulsions in the treatment of acute poisoning: a systematic
review of human and
animal studies. Clin Toxicol (Phila) 2010; 48:1-27.
19. Litonius ES, Niiya T, Neuvonen PJ, Rosenberg PH. Intravenous
lipid emulsion
only minimally influences bupivacaine and mepivacaine
distribution in plasma and does
not enhance recovery from intoxication in pigs. Anesth Analg
2012; 114:901-6.
20. Litonius E, Tarkkila P, Neuvonen PJ, Rosenberg PH. Effect of
intravenous lipid
emulsion on bupivacaine plasma concentration in humans.
Anaesthesia 2012; 67:600-
5.
21. Liu L, Xia Y, Chen Y, Wang Q, Shi T, Wang F, Small RH, Xu X.
The comparative
effects of lipid, epinephrine, and their combination in the
reversal of bupivacaine-
induced asystole in the isolated rat heart. Anesth Analg 2012;
114:886-93.
22. Weinberg GL, Di Gregorio G, Ripper R, Kelly K, Massad M,
Edelman L, Schwartz
D, Shah N, Zheng S, Feinstein DL. Resuscitation with lipid
versus epinephrine in a rat
model of bupivacaine overdose. Anesthesiology 2008;
108:907-13.
-
8/20/2019 C5. Chap10. Nouette-Gaulain
21/22
23. Hiller DB, Gregorio GD, Ripper R, Kelly K, Massad M, Edelman
L, Edelman G,
Feinstein DL, Weinberg GL. Epinephrine impairs lipid
resuscitation from bupivacaine
overdose: a threshold effect. Anesthesiology 2009;
111:498-505.
24. Mayr VD, Mitterschiffthaler L, Neurauter A, Gritsch C,
Wenzel V, Muller T,
Luckner G, Lindner KH, Strohmenger HU. A comparison of the
combination ofepinephrine and vasopressin with lipid emulsion in a
porcine model of asphyxial cardiac
arrest after intravenous injection of bupivacaine. Anesth Analg
2008; 106:1566-71,
table of contents.
25. Harvey M, Cave G, Kazemi A. Intralipid infusion diminishes
return of
spontaneous circulation after hypoxic cardiac arrest in rabbits.
Anesth Analg 2009;
108:1163-8.
26. Hicks SD, Salcido DD, Logue ES, Suffoletto BP, Empey PE,
Poloyac SM, MillerDR, Callaway CW, Menegazzi JJ. Lipid emulsion
combined with epinephrine and
vasopressin does not improve survival in a swine model of
bupivacaine-induced cardiac
arrest. Anesthesiology 2009; 111:138-46.
27. Ruan W, French D, Wong A, Drasner K, Wu AH. A mixed (long-
and medium-
chain) triglyceride lipid emulsion extracts local anesthetic
from human serum in vitro
more effectively than a long-chain emulsion. Anesthesiology
2012; 116:334-9.
28. Li Z, Xia Y, Dong X, Chen H, Xia F, Wang X, Dong H, Jin Z,
Ding X, Papadimos
TJ, Xu X. Lipid resuscitation of bupivacaine toxicity:
long-chain triglyceride emulsion
provides benefits over long- and medium-chain triglyceride
emulsion. Anesthesiology
2011; 115:1219-28.
29. Candela D, Louart G, Bousquet PJ, Muller L, Nguyen M, Boyer
JC, Peray PA,
Goret L, Ripart J, Lefrant JY, de La Coussaye JE. Reversal of
bupivacaine-induced
cardiac electrophysiologic changes by two lipid emulsions in
anesthetized and
mechanically ventilated piglets. Anesth Analg 2010;
110:1473-9.
30. Shah S, Gopalakrishnan S, Apuya J, Shah S, Martin T. Use of
Intralipid in an
infant with impending cardiovascular collapse due to local
anesthetic toxicity. J Anesth
2009; 23:439-41.
31. Rothschild L, Bern S, Oswald S, Weinberg G. Intravenous
lipid emulsion in
clinical toxicology. Scand J Trauma Resusc Emerg Med 2010;
18:51.
32. Hiller DB, Di Gregorio G, Kelly K, Ripper R, Edelman L,
Boumendjel R, Drasner
K, Weinberg GL. Safety of high volume lipid emulsion infusion: a
first approximation of
LD50 in rats. Reg Anesth Pain Med 2010; 35:140-4.
-
8/20/2019 C5. Chap10. Nouette-Gaulain
22/22


![10-chap10-Applet.ppt [호환 모드] - djeong.kunsan.ac.krdjeong.kunsan.ac.kr/.../10-chap10-Applet.pdf · Dongwon Jeong, djeong@kunsan.ac.kr 3 / 16 IT COOKBOOK 웹브라우저를통한애플릿실행과정](https://img.pdfslide.tips/doc/110x75/5a8316b37f8b9a0c748e8e70/10-chap10-djeongkunsanackrdjeongkunsanackr10-chap10-appletpdfdongwon.jpg)