Embed Size (px)
Citation preview

結核病的診斷與治療
高醫附設醫院 感染內科
盧柏樑 醫師

結核病~三千年歷史的古老疾病 埃及時代 西元前 3700-1000年
土偶 木乃伊 (Nesperhan, priest of Amun)

Primary TB
Latent TB
Active TB
10%
有症狀
有傳染性
Latent TB
90%

Active TB disease
• Latent TB infection progresses to active TB in
– 感染後馬上發病 (primary progression)
– 5%感染後兩年內發病
– 5%感染兩年以後發病
• 90% 終身Latent TB
• Risk greater if cell-mediated immunity impaired

結 核 病 的 診 斷

空洞
結核菌吸入肺內引起感染,當細菌繁殖,體內白血球開始與結核菌戰鬥,病灶痊癒,殘餘結核菌轉變成潛伏者,但並未死亡。當身體抵抗力下降,潛伏的結核菌又開始繁殖,甚至可能產生空洞。
乾酪化病灶

Chest Radiograph
• Abnormalities often seen in apical
or posterior segments of upper
lobe or superior segments of
lower lobe
• May have unusual appearance in
HIV-positive persons
• Cannot confirm diagnosis of TB
Arrow points to cavity in
patient's right upper lobe.


檢體採集
• Obtain 3 sputum specimens for smear examination and culture
• Persons unable to cough up sputum, induce
sputum, bronchoscopy or gastric aspiration
• Follow infection control precautions during
specimen collection

Smear Examination
• Strongly consider TB in patients with smears
containing acid-fast bacilli (AFB)
• Results should be available within 24 hours of
specimen collection
• Presumptive diagnosis of TB

AFB smear
AFB (shown in red) are tubercle bacilli

What Does AFB Smear Tells Us?
IF positive, it is TB or NTM (Non-TB
Mycobacterium) infection.
If negative, no infection or infection but less
than 105 AFB/ml in the specimen
50% culture-positive are Smear-negative
Still it is the Most Widely Used Test Worldwide
And has had a Great Role in TB Diagnosis

1.A minimum of 100,000 tubercle bacilli per
millilitre of sputum are necessary to be seen on
microscopy.
2.Apparently only a few hundred bacilli per millilitre
of sputum are sufficient to be detected by culture.
BACTERIOLOGY

分支桿菌培養
傳統培養方法(固態培養基)需時四至八週
比鏡檢更敏感, 可偵測到10-100隻細菌/ml
敏感度: 80-85 %, 特異性 98 %
部分痰抹片陰性病人仍可因培養陽性獲致確診

Cultures
• Use to confirm diagnosis of TB
• Culture all specimens, even if smear negative
• Results in 4 to 14 days when liquid medium
systems used
Colonies of M. tuberculosis growing on media

Different Culture Media
The Old Way
Egg-base. LJ, Ogawa, and Others
Agar-base. Middlebrook.
BACTEC 12B Radiometric
BACTEC 460 has become a “GOLD Standard”
for culture and Susceptibility testing
The New Way
Non-radiometric liquid culture systems

快速檢驗
• Molecular method
• PCR
– In house
– FDA approved
• Antigen detection
• 抗原鑑定


Latent TB infection
• Tuberculin skin test usually positive at 2-10
weeks
• Tubercle bacilli may remain dormant but viable
for many years
• No symptoms of active TB disease
• Not infectious
• Usually no progression in 90% of persons

Administering the Tuberculin Skin Test
• Inject intradermally 0.1 ml of 5
TU PPD tuberculin
• Produce wheal 6 mm to 10 mm
in diameter
• Do not recap, bend, or break
needles, or remove needles from syringes
• Follow universal precautions for infection control

Reading the Tuberculin Skin Test
• Read reaction 48-72 hours after injection
• Measure only induration
• Record reaction in millimeters

不同結核病患接觸者皮膚結核菌素測驗結果
塗片培養均陽性*
塗片陰性培養陽性
非開放性病人
無接觸對照組
Group
tested
374
228
221
709
感染數
244
61
39
157
No. of person tested
檢查人數
世界衛生組織資料 1976
%
65.2
26.8
17.7
22.1
Reactors
*P<0.0001(差異具統計學意義)
10-14歲兒童
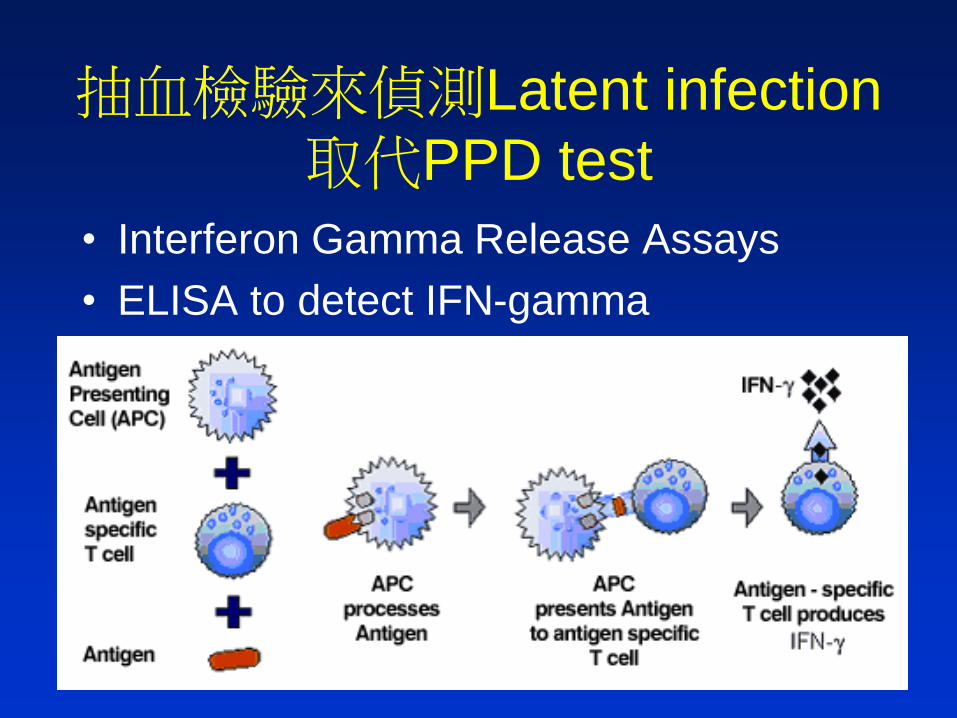
抽血檢驗來偵測Latent infection
取代PPD test
• Interferon Gamma Release Assays
• ELISA to detect IFN-gamma

Important!!!
Choose a right method!
• Active infection
– Acid fast stain
– Culture
– Molecular
detection
• In house PCR
• Genprobe
• Latent infection
– Tuberculin skin
test
g interfetron assay
– ELISPOT
– T SPOT

Hypocrites (460-
370 BC) and the
Kos School
• tuberculosis, or consumption.
• A morbid process characterized by
progressive debilitation, coughing,
hemoptysis, and suppurating lung
lesions.

The answer for a cure is in Nature
• The main goal of the doctor treating
tuberculosis was to avoid hindering
natural cures.
• Continual rest, a balanced diet, and
abstaining from anything in excess
including sex were considered crucial.
休養, 均衡飲食與禁慾

• Bloodletting to drain contaminated blood
from the infected lung,
• thoracic poultices,
• “sandacara” pollen (from Cupressaceae
plants),
• drinking wine to induce coughing and
suppurating from lung lesions,
• thoracentesis preformed with a sharp
knife to drain fluid from the lung.

In 1860, Hermann Brehmer from Germany
started the first center in Gobersdorf
• to cure tuberculosis by rest. • The mountain fresh air and over-feeding in
an establishment more like a luxury hotel than a hospital would strengthen the patient.

• Villemin, 1865, established that the disease
was infectious.
– An Army Doctor.
– Young solider in Barracks got TB.
– Rabbit experiment

Collapsing the lung
• In 1888, an Italian, Carlo Forlanini
preformed the first intentional
spontaneous pneumothorax using a
needle to puncture the pleual cavity and
then administering nitrogen.

結核病的治療: 1944年開始化學藥物治療, 之前只能依賴療養。 (1930~ Collapse therapy)
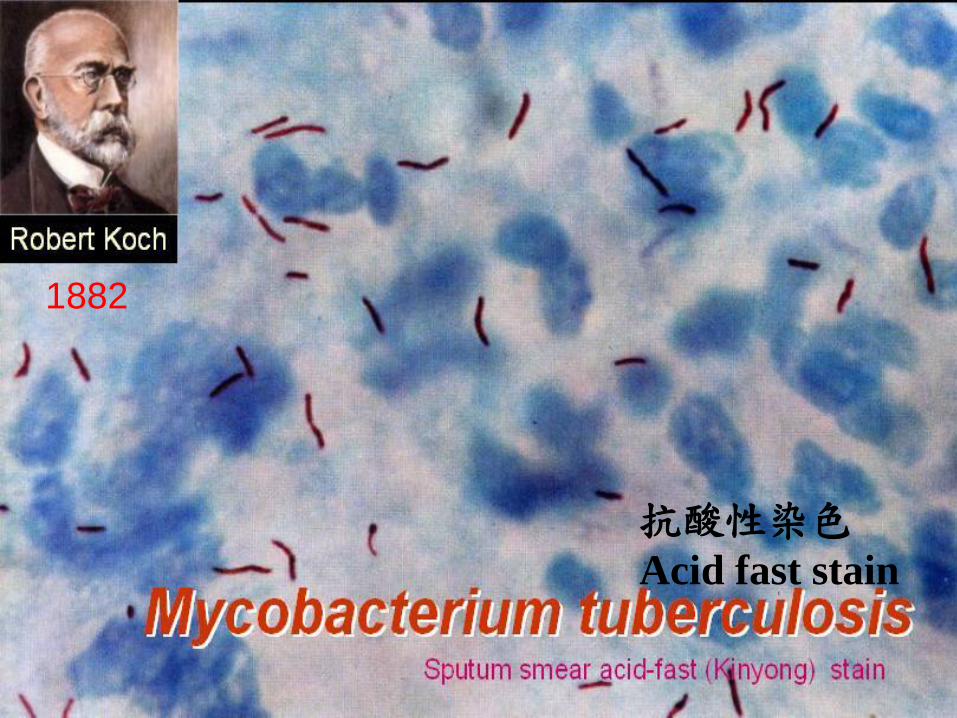
抗酸性染色
Acid fast stain
1882

結核菌
學名:Mycobacterium tuberculosis
1882年科霍發現結核菌
耐酸菌(acid-fast bacilli)
細胞壁富於脂質而會妨害色素通過, 因而不易染色, 一旦染色不易被強酸脫色, 故又稱耐酸菌
分裂速度慢(1次/20hrs)
潮濕陰暗處可存活 6-8 個月, 陽光直接照射 4-6
小時死亡, 煮沸5分鐘可殺死

TB治療的歷史
• X-rays used in the 1920’s to scan the
lungs for TB.
– 診斷
– 追蹤療效

空洞
結核菌吸入肺內引起感染,當細菌繁殖,體內白血球開始與結核菌戰鬥,病灶痊癒,殘餘結核菌轉變成潛伏者,但並未死亡。當身體抵抗力下降,潛伏的結核菌又開始繁殖,甚至可能產生空洞。
乾酪化病灶

土壤微生物學原理
• 賽爾曼·A·瓦克斯曼
(Selman
Waksman )
• 因發現鏈黴素,
Streptomycin和其他抗生素而獲得1952年的諾貝爾獎

結核病治療的里程碑
SM 1944 開始
治療進步但產生抗藥性
BMJ 1948 2:p769-782
PAS 1943 開始
# PAS + SM 避免了SM 抗藥性
# 確立TB 化學治療原則:多種藥物合併治療
INAH in 1951開始
兩階段治療的觀念
INH+PAS+SM
INH+PAS

抗結核藥物
• First-line Anti-tuberculosis Drugs
– Isoniazid (INH)
– Rifampin (RMP)
– Pyrazinamide (PZA)
– Ethambutol (EMB)
初次治療常規用藥
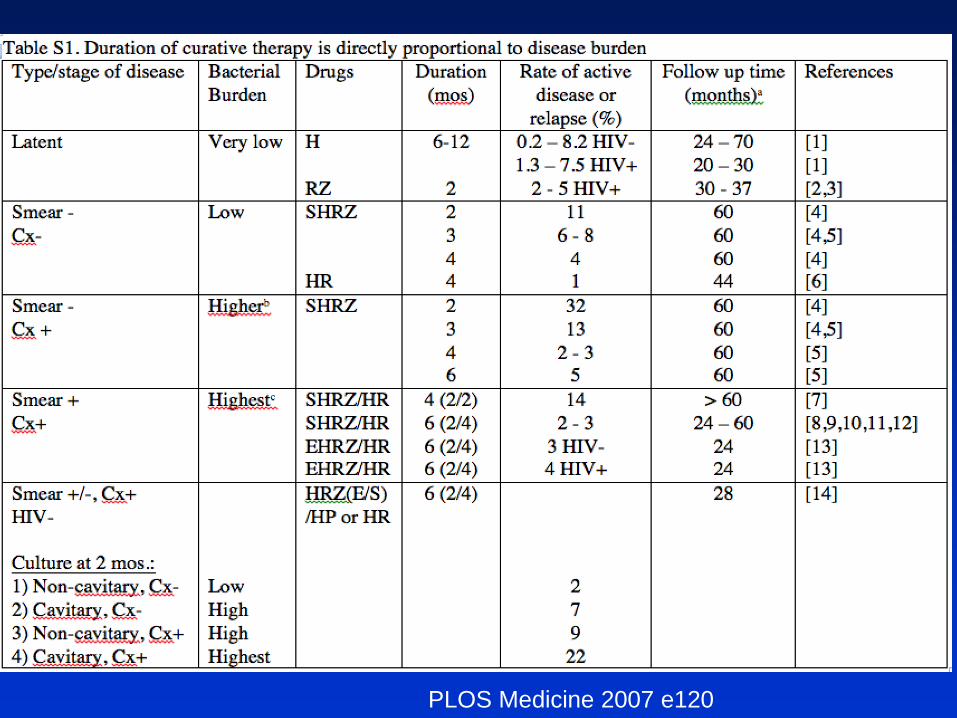
PLOS Medicine 2007 e120

PLOS Medicine 2007 e120

PLOS Medicine 2007 e120

若藥物敏感性試驗INH為抗藥
可不可以用INH
第五版


區分為初治或再治病人
• 新病人 (New case):不曾接受過抗結核藥治療或曾接受少於四週抗結核藥治療之病人。
• 再治病人(Retreatment case) – 復發 (Relapse):曾接受一個完整療程之抗結核藥治療並經
醫師宣告治癒而再次痰塗片或培養陽性之病人。
– 失落再治 (Treatment after default):中斷治療兩個月以上而再次痰塗片或培養陽性之病人。
– 失敗再治 (Treatment after failure):治療五個月後依然痰塗片或培養陽性的病人,或者治療前痰陰性、治療二個月後變成痰塗片或培養陽性的病人。
疾病管制局: 結核病診治指引
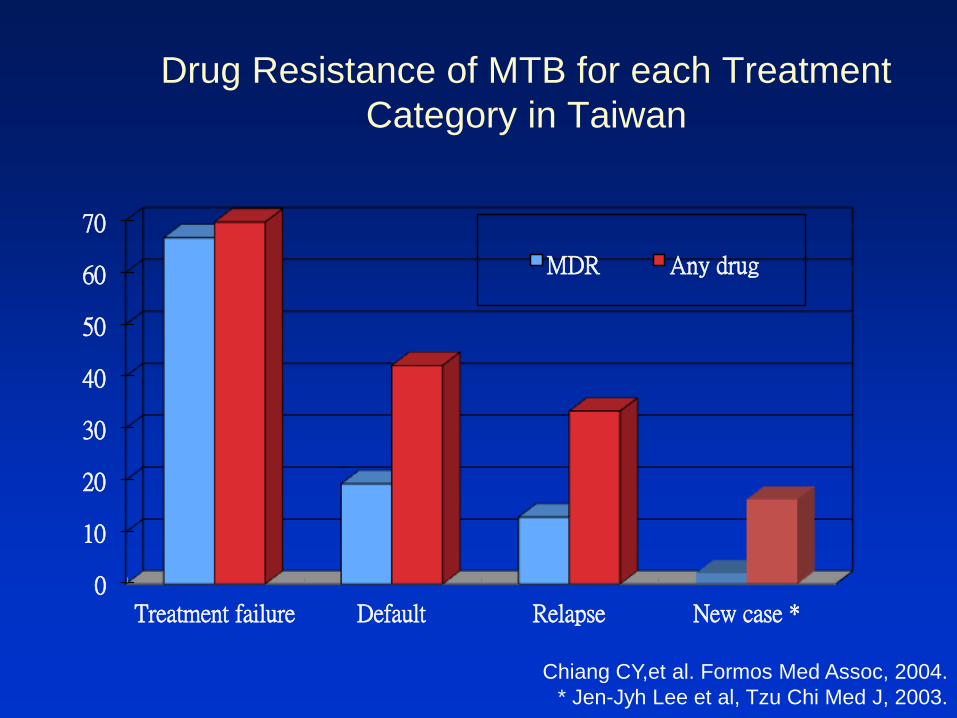
Drug Resistance of MTB for each Treatment
Category in Taiwan
0
10
20
30
40
50
60
70
Treatment failure Default Relapse New case *
MDR Any drug
Chiang CY,et al. Formos Med Assoc, 2004.
* Jen-Jyh Lee et al, Tzu Chi Med J, 2003.

結核病初次治療 *
• 標準治療
– 2HRZE/4HRE
– 每日一次口服
– 前 2 個月 INH+RMP+PZA+EMB
– 後 4 個月 INH+RMP+EMB
* 適用初治新案 (new case):不曾接受過抗結核藥治療或曾接受少於 4 週抗結核藥治療之病人。
如證實無 INH 或 RMP
抗藥, 則停用 EMB

•Rifater (each tab)
= INH 80mg
+ RMP 120mg
+ PZA 250mg
>=50kg 每日5錠
體重每減10kg 減1錠
Rifater (RFT) + EMB Rifinah (RFN) + EMB
•Rifinah300 (each tab)
= RMP 300mg + INH 150mg
•Rifinah150 (each tab)
= RMP 150mg + INH 100mg
>=50kg RFN300 每日2錠
<50kg RFN150 每日3錠
Fixed Drug Combination

若病人45kg, INH: 5*45=225, RIF: 10*45=450
3錠[RFN150] : INH 300, RIF 450
1錠[RFN150]+ 1錠[RFN300] : INH:250, RIF:450
也可 2.5錠INH 100*2.5=250, 3錠RIF 150*3=450
如果劑量過高, 容易副作用
若您是病人, 您會選哪種?

複方
• 病人接受度較高
• 沒有減少副作用, 甚至可能增加副作用
• 劑量上的困境
選高一點的劑量
有副作用再退回較低劑量
有助於減少抗藥性發生

指引

臨床指引的好處
• (1)增進品質並降低醫療錯誤
• (2)組織大量的資料
• (3)減少照護時的變數
• (4)排除浪費
• (5)改善對慢性病的處理
遵照指引, 病人就OK?

機器人醫生最遵守指引

送藥到手
服藥入口 嚥下再走
TB

同時四種藥 至少六個月
• 醫師, 假如吃結核病的藥有那麼多副作用, 您會願意吃嗎?
• 萬一有副作用,怎麼辦?

不能說白色謊言的年代
• 以往,醫師可以視情況”安撫病人”….?
• 現在,如果未說明藥物副作用是有錯的,
法官可依此判刑
• 現在, 開藥不符合指引也可能會為醫師引來災害

醫學是科學 也是藝術
• 醫護人員: 犯罪率最高?
• 臨床上, 以對病人最佳的方式幫助病人
– 不會百分百依照指引

治療效果評估
• 門診評估症狀及病人服藥順從性:
– 治療第1個月至少應回診2次,以後每月至少1次。
• 結核菌檢查
– 痰抹片耐酸菌鏡檢及結核菌培養:
• 每個月至少檢查1次,直到連續2個月培養陰性;
• 治療滿6個月時再檢查1次。
– 菌種鑑定:
• 每次培養陽性均應作菌種鑑定。
• 藥物敏感性試驗:
– 第1次培養陽性的菌株,
– 治療滿3個月後仍培養陽性的菌株。
疾病管制局: 結核病診治指引, 2006 第二版

治療效果評估 • 胸部X光檢查:
– 至少在治療滿2個月,及治療滿6個月時作胸部X光檢查。
-3

When to suspect MDR-TB?
Chavez AM, Blank R, Smith Fawzi MC, et al. Identifying early treatment failure on Category I therapy for pulmonary tuberculosis in Lima Ciudad, Peru. Int J Tuberc Lung Dis 2004; 8: 52-8.

Standards for Treatment
• Patients who have positive smears during the fifth month of treatment should be considered as treatment failures and have therapy modified appropriately.
• 治療第五個月仍痰陽性, 很可能治療失敗
• 需區分NTM非結核分枝桿菌之可能性

治療前評估 *
Never treat multidurg-resistant TB
(MDR-TB) without expert consultation
TB Case
標準初次
治療 照會專業醫師
Y
N
過去治療史
新案
•Return after default
•Relapse
•Failure
•Chronic case
WHO. Treatement of tuberculosis, 3nd ed. 2003. WHO/CDS/TB 2003.313
* 依過去治療史分類
初治 再治
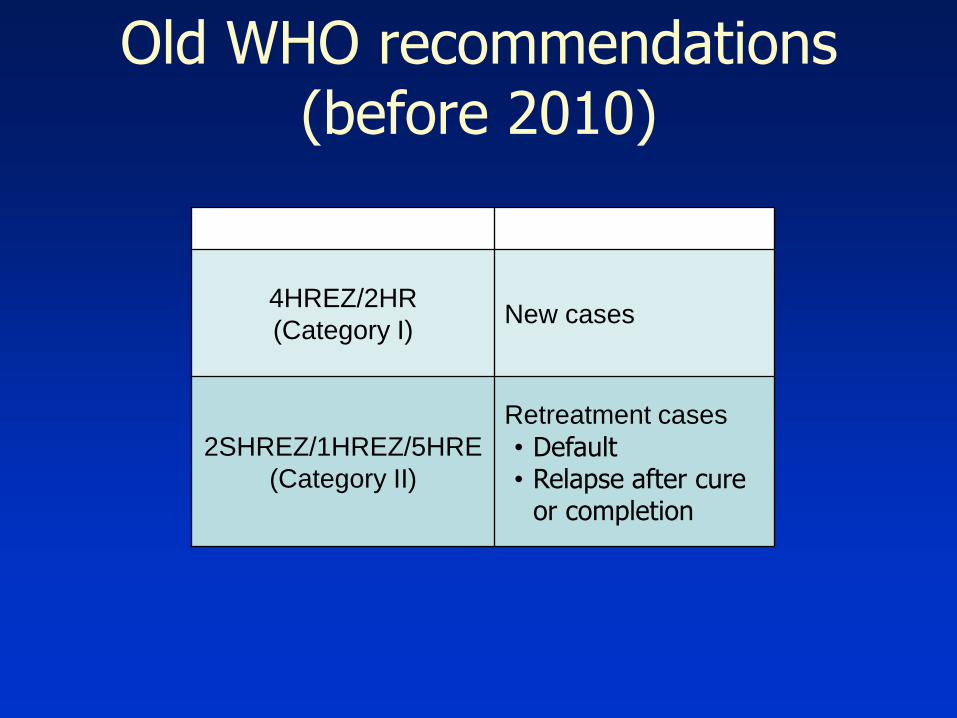
Old WHO recommendations (before 2010)
Regimen Indications
4HREZ/2HR
(Category I) New cases
2SHREZ/1HREZ/5HRE
(Category II)
Retreatment cases
• Default • Relapse after cure
or completion

MDR-TB in Category I treatment failure
1. Becerra MC et al. Int J Tuberc Lung Dis. 2000; 4(2): 108-14.
2. Fitzwater SP et al. Clin Inf Dis 2010; 51(4):371–37.
3. Quy HT et al. Int J Tuberc Lung Dis 2003; 7: 631-636.
4. Gler MT et al. Int J Tuberc Lung Dis 2011; 15: 652-656.
Study Country
Proportion of MDR-
TB in Category I
treatment failure
Becerra et al.1 Peru 94%
Fitzwater et al.2 Peru 100%
Quy et al.3 Vietnam 80%
Gler et al.4 Philippines 83%

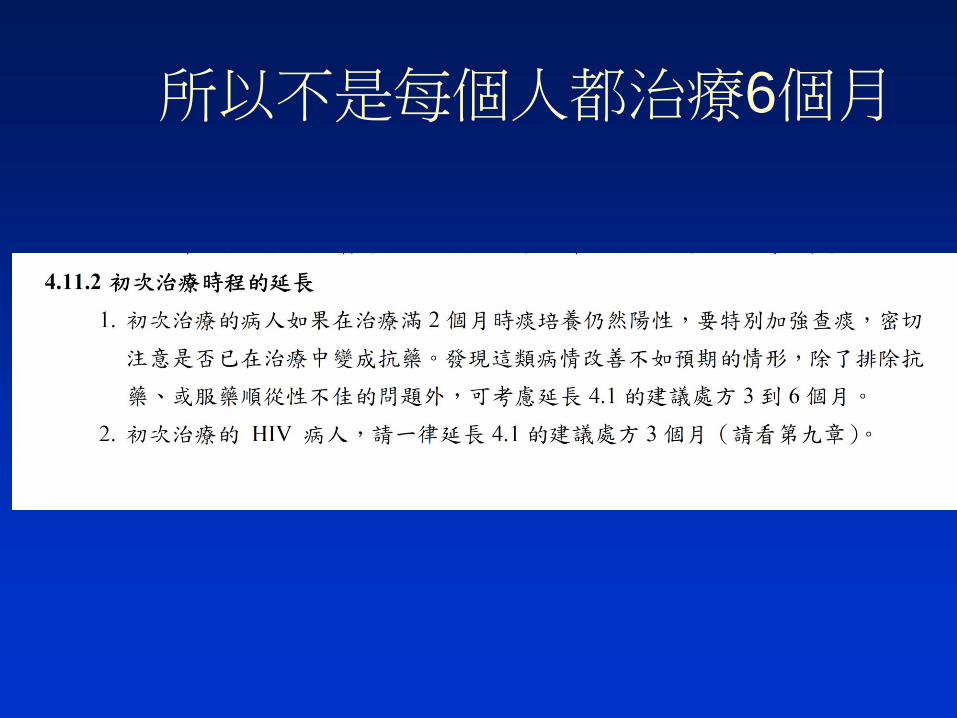
所以不是每個人都治療6個月


肺外結核要治療更久
• 九個月
• 12個月
• 必要時 超過12個月……

完成治療
• 痰陰 (塗片及培養)
• 症狀改善
• 胸部X光改善
• 服藥期滿
謝謝 請指教
• 多種有效的抗結核藥物合併使用
• 藥物須按規服用
• 治療期間須夠長





























