Embed Size (px)
Citation preview

Chapter 15
DSN
Neurologic SystemKevin Dobi, MS, APRN
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.

Concept Overview
Intracranial regulation: Mechanisms that facilitate or impair neurologic
function.
Interrelationships: Brain requires oxygenation.
Respiratory and cardiovascular systems impacted by neurologic control.
Extensions of neurologic function: Sensory perception.
Tactile perception.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
2

Anatomy and Physiology
Nervous system controls body functions through voluntary and autonomic responses to external and internal stimuli.
Structural divisions of nervous system are: Central nervous system (CNS), which
consists of brain and spinal cord Peripheral nervous system (PNS) Autonomic nervous system (ANS)
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
3

Anatomy and Physiology: CNS: Protective Structures
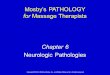
Skull protects brain. Foramen magnum is large oval opening at base of skull
in occipital bone. Spinal cord extends through from
medulla oblongata. Other foramina at base for entrance and exit of paired
cranial nerves and cerebral blood vessels. Meninges, three layers between skull and brain:
Dura mater, outer double layer. Arachnoid, middle meningeal
layer. Pia mater, inner meningeal layer.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
4

Anatomy and Physiology: CNS: Protective Structures (contd.)
Between arachnoid and pia mater is subarachnoid space where cerebrospinal fluid (CSF) circulates.
Falx cerebri, a fold of dura mater, separates two cerebral hemispheres.
Tentorium cerebelli, another fold of dura mater, supports temporal and occipital lobes and separates cerebral hemispheres from cerebellum.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
5

Anatomy and Physiology: CNS:Cerebrospinal Fluid
CSF is colorless, odorless fluid containing: Glucose, electrolytes, oxygen, water, carbon dioxide,
and leukocytes.
Circulates around brain and spinal cord. Provides cushion, maintains normal intracranial
pressure, nutrition, and removes metabolic wastes.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
6

Anatomy and Physiology: CNS:Cerebral Ventricular System
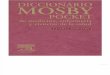
Cerebral ventricular system consists of four interconnecting ventricles producing and circulating CSF: Two lateral ventricles, one in each hemisphere. One ventricle adjacent to thalamus. One ventricle adjacent to brainstem.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
7
Anatomy and Physiology: CNS:CSF and Cerebral Ventricular System
CSF circulates from lateral ventricles through the interventricular foramen to third ventricle. Through aqueduct of Sylvius to fourth ventricle. Into cisterna magna, a small reservoir for CSF. To subarachnoid space up around brain and down
around spinal cord. Absorbed through arachnoid villi that extend into
subarachnoid space and returned to venous system.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
8

Anatomy and Physiology: Brain
Brain consists of cerebrum, diencephalon, cerebellum, and brainstem; is composed of: Gray matter (cell bodies). White matter (myelinated nerve fibers).
Carotid arteries supply most of blood to brain, and branch off into posterior cerebral, middle cerebral, and anterior cerebral arteries. Remaining blood flows through two vertebral arteries and
into posterior and anterior communicating arteries that supply blood through circle of Willis.
Blood leaves brain through venous sinuses that empty into jugular veins.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
9

Anatomy and Physiology: Brain – Cerebrum
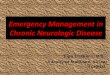
Cerebrum is largest part of brain consisting of two hemispheres, each divided into four lobes: Frontal lobe, parietal lobe, temporal lobe, and occipital lobe. Frontal lobe contains primary motor cortex and
functions related to voluntary motor activity. Broca’s area is located in left frontal lobe involved in
formulation of words. Frontal lobe also controls intellectual function,
awareness of self, personality, and autonomic responses related to emotion.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
10

Anatomy and Physiology: Brain – Cerebrum (contd.)
Cerebrum: Parietal lobe contains primary somesthetic (sensory) cortex that
receives sensory input such as position, touch, shape, and texture of objects.
Temporal lobe contains primary auditory cortex:
Wernicke’s area located in left temporal lobe, responsible for comprehension of spoken and written language.
Also interprets auditory, visual, and somatic sensory inputs that are stored in thought and memory.
Occipital lobe contains primary visual cortex, which receives and interprets visual information.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
11

Anatomy and Physiology: Brain – Diencephalon
Diencephalon is made up of thalamus, hypothalamus, epithalamus, and subthalamus. Thalamus is relay and integration station from spinal cord to cerebral
cortex and other parts of brain. Hypothalamus important in maintaining homeostasis.
Functions include regulation of body temperature, hunger, and thirst; formation of autonomic nervous system responses; and storage and secretion of hormones from pituitary gland.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
12

Anatomy and Physiology:Brain – Diencephalon (contd.)
Epithalamus contains pineal gland, which causes sleepiness and helps regulate some endocrine functions
Subthalamus is part of extrapyramidal system of autonomic nervous system and basal ganglia.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
13

Anatomy and Physiology: Brain – Basal Ganglia
Basal ganglia lies between cerebral cortex and midbrain, adjacent to diencephalon. Basal ganglia comprised of six ganglia: Putamen, caudate nucleus,
globus pallidus, thalamus, red nucleus, and substantia nigra. Function is balancing production of two neurotransmitters—
acetylcholine and dopamine—that create smooth, coordinated voluntary movement.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
14

Anatomy and Physiology: Brain – Brainstem
Brainstem is made up of midbrain, pons, and medulla oblongata.
Ten of twelve cranial nerves (CNs) originate from brainstem.
Midbrain functions to relay stimuli concerning muscle movement to other brain structures. Contains part of motor tract
pathways that control reflex motor movements in response to visual and auditory stimuli.
Oculomotor nerve (CN III) and trochlear nerve (CN IV) originate in midbrain.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
15

Anatomy and Physiology: Brain – Brainstem (contd.)
Brainstem: Pons relays impulses to brain centers and lower spinal
nerves. CNs that originate in the pons are trigeminal (CN V),
abducens (CN VI), facial (CN VII), and acoustic (CN VIII).
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
16

Anatomy and Physiology: Brain – Brainstem (contd.)
Brainstem: Medulla oblongata contains reflex centers for
controlling involuntary functions such as breathing, sneezing, swallowing, coughing, vomiting, and vasoconstriction.
Motor and sensory tracts from frontal and parietal lobes cross from one side to other in medulla; lesions on right side create abnormal movement and sensation on left side, and vice versa.
Cranial nerves originating in medulla are glossopharyngeal (CN IX), vagus (CN X), spinal accessory (CN XI), and hypoglossal (CN XII).
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
17

Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
18

Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
19

Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
20

Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
21

Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
22

Anatomy and Physiology: Brain – Cerebellum
Cerebellum separated from cerebral cortex by tentorium cerebelli.
Functions of cerebellum include coordinating movement, equilibrium, muscle tone, and proprioception. Each cerebellar hemisphere controls movement for
same (ipsilateral) side of body.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
23

Anatomy and Physiology: Brain – Spinal Cord
Spinal cord is continuation of medulla oblongata that begins at foramen magnum and ends at first and second lumbar (L1 and L2) vertebrae. At L1 and L2, spinal cord branches into lumbar and
sacral nerve roots termed cauda equina. Spinal cord consists of 31 segments, each giving rise to
a pair of spinal nerves. Nerve fibers, grouped into tracts, run through the
spinal cord transmitting sensory, motor, and autonomic impulses between brain and body.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
24

Anatomy and Physiology: Brain – Spinal Cord (contd.)
Spinal cord: Myelinated nerves form white matter of spinal cord and contain
ascending and descending tracts of nerve fibers. Descending or motor tracts carry impulses from frontal lobe to muscles
for voluntary movement and play a role in muscle tone and posture. Ascending or sensory tracts carry sensory information from body
through thalamus to parietal lobe.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
25

Anatomy and Physiology: Brain – Spinal Cord (contd.)
Spinal cord: Fasciculus gracilis travels within medial lemniscus in posterior (dorsal)
column carrying sensations of touch, deep pressure, vibration, position of joints, stereognosis, and two-point discrimination.
Lateral spinothalamic tract carries fibers for sensations of light touch, pressure, temperature, and pain.
Gray matter, which contains nerve cell bodies, arranged in a butterfly shape with anterior and posterior horns.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
26

Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
27

Anatomy and Physiology: Peripheral Nervous System
12 pairs of cranial nerves: Five pairs have only motor
fibers. Three pairs have only sensory
fibers. Four pairs have both motor and
sensory fibers.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
28

Anatomy and Physiology: Peripheral Nervous System –Spinal Nerves
Spinal nerves, 31 pairs, emerge from spinal cord: Cervical nerves: 8 pairs
First 7 exit above their corresponding vertebrae; remaining pair exit below corresponding vertebrae.
Thoracic nerves: 12 pairs Lumbar nerves: 5 pairs Sacral nerves: 5 pairs Coccygeal nerves: 1 pair
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
29

Anatomy and Physiology: Peripheral Nervous System –Spinal Nerves (contd.)
Spinal nerve pairs formed by union of efferent or motor (ventral) root and afferent or sensory (dorsal) root. Motor fibers carry impulses from frontal lobe through spinal cord to
muscles and glands; sensory fibers carry impulses from sensory receptors of body through spinal cord to parietal lobe.
Each pair of spinal nerves and its corresponding part of the spinal cord make up a spinal segment and innervate specific body segments.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
30
Anatomy and Physiology: Peripheral Nervous System –Spinal Nerves (contd.)
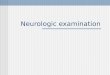
Spinal nerve pairs: Dorsal root of each spinal nerve supplies sensory innervation to a
specific area of skin known as a dermatome.
For example, if patient complains of pain with numbness and tingling across right knee, the nurse knows that fourth lumbar spinal segment is involved and perhaps compressed.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
31

Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
32
Anatomy and Physiology: Peripheral Nervous System – Reflex Arc
Reflex arcs tested by observing muscle movement in response to sensory stimuli. Deep tendon reflexes are responses to stimulation of tendon that
stretches neuromuscular spindles of muscle group.
Striking a deep tendon stimulates a sensory neuron that travels to spinal cord where it stimulates an interneuron, which stimulates a motor neuron to create movement.
Superficial reflexes tested similarly. Each reflex corresponds to a specific spinal segment.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
33

Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
34

Anatomy and Physiology: Autonomic Nervous System
Autonomic nervous system (ANS) regulates body’s internal environment in conjunction with endocrine system.
ANS has two components: Sympathetic nervous system Parasympathetic nervous
system
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
35

Anatomy and Physiology: Autonomic Nervous System – SNS
Sympathetic nervous system (SNS) arises from thoracolumbar segments of spinal cord and is activated during stress (the “fight-or-flight” response).
SNS actions include: Increasing blood pressure and heart rate. Vasoconstricting peripheral blood vessels. Inhibiting gastrointestinal peristalsis. Dilating bronchi.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
36

Anatomy and Physiology: Autonomic Nervous System – PNS
Parasympathetic nervous system (PNS) arises from craniosacral segments of spinal cord and controls vegetative function. “Helps out the SNS”
PNS actions associated with conserving energy such as: Decreasing heart rate and force of myocardial
contraction. Decreasing blood pressure and respiration. Stimulating gastrointestinal peristalsis.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
37

General Health History: Present Health Status
Have you noticed any changes in ability to move around or participate in usual activities?
Do you have any chronic diseases? High blood pressure? Myasthenia gravis? Multiple sclerosis?
What medications do you take? Are you taking medications as prescribed?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
38

General Health History: Past Medical History
Have you ever had injury to head or spinal cord? What changes have you experienced since injury?
Have you had surgery on brain, spinal cord, or nerves?
Have you ever had a stroke? What changes have you had as result of stroke?
Do you have a seizure disorder? How often? What do you do to prevent seizures?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
39

General Health History: Family History
In your family, has anyone ever had: A stroke?
Seizures?
Tumor in brain or spinal cord?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
40

General Health History: Personal and Psychosocial History
Have you had changes in your ability to perform personal care?
Do you drink alcohol? Have you ever used recreational drugs? Do you use seat belts?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
41

Problem-Based History: Headache
Describe your headaches. What do they feel like? Where? Last how long? How often?
Have you had any recent surgeries or medical procedures such as spinal anesthesia or lumbar puncture?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
42

Problem-Based History: Dizziness
What does it feel like when you are dizzy or lightheaded? Do you feel faint? How often do you experience this dizziness? What makes dizziness worse?
Have you ever had a sensation that room is spinning (objective vertigo), or that you are spinning (subjective vertigo)? Does this happen suddenly or gradually? What makes vertigo worse? What relieves vertigo?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
43

Problem-Based History: Seizures
Have you ever had a seizure? How often are you having seizures? When was your last seizure? What are they like? Do you become unconscious?
Do you have any warning signs before the seizure starts?
How do you feel after the seizure? Are you confused? Have a headache or aching muscles? Do you spend too much time sleeping?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
44

Problem-Based History: Seizures (contd.)
When patient loses consciousness during seizures, refer these questions to person who observed patient’s seizure: Describe the seizure movements that you observed. Did you notice any other signs such as a change in
color of the face or lips? Loss of consciousness (if so, how long)? Did the patient urinate or have a bowel movement
during the seizure? After the seizure, how long did it take the patient to get
back to normal?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
45

Problem-Based History: Seizures (contd.)
Are there any factors that start these seizures? Stress? Fatigue? Activity? Do you take actions to prevent hurting yourself during
seizures?
How have seizures affected your life? Your occupation? Do you wear any identification that indicates you have
seizures?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
46

Problem-Based History: Loss of Consciousness
When did you lose consciousness or feel you were not aware of surroundings? Did it occur suddenly? What happened just before? Other symptoms? Have diabetes mellitus, liver failure, or kidney failure?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
47

Problem-Based History: Changes in Movement
How long have you had a change in your mobility? Continuous or intermittent?
Noticed tremors or shaking of hands or face? When did they start? Do they seem worse when you are anxious or at rest? Are they worse when you focus on doing something
(intention)? What relieves tremors—rest, activity, or alcohol? Do they affect your performance of daily activities?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
48

Problem-Based History: Changes in Movement (contd.)
Have you felt sense of weakness in or difficulty moving parts of your body? Confined to one area or generalized? Associated with anything in particular (e.g., activity)? Does anything help to relieve weakness?
Do you have problems with coordination? Do you have difficulty keeping your balance when you
walk? Do you lean to one side or fall? Which direction? Do your legs suddenly give way?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
49

Problem-Based History: Changes in Sensation
Where are you experiencing numbness or tingling? How does it feel? Is it associated with any activity?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
50

Problem-Based History: Difficulty Swallowing (Dysphagia) How long have you had problems
swallowing? Do these problems involve liquids or solids? Both? Do you have excessive saliva or drooling? Do you cough or choke when trying to swallow?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
51

Problem-Based History: Difficulty Communicating (Aphasia/Dysphasia)
How long have you had problems speaking? Difficulty forming words or finding right words? Difficulty understanding
things said to you? Has handwriting changed? When did that begin? How long did it last?
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
52

Physical Examination
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
53

Examination: Routine Techniqueswith Normal Findings
Assess mental status and level of consciousness.
Evaluate speech for articulation and voice quality and conversation for comprehension.
Note cranial nerve functions (data about expected cranial nerve functions collected during interview). Assessing cranial nerves is not ordinarily performed
during routine examination, but when you suspect an abnormal finding of one or more of cranial nerves.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
54

Examination: Routine Techniques with Normal Findings (contd.)
Observe gait for balance and symmetry.
Evaluate extremities for muscle strength.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
55

Examination: Special Circumstances and Advanced Practice
Assess individual cranial nerves: Test nose for smell (olfactory nerve CN1). Test eyes (visual acuity optic nerve CN II) for visual
acuity using Snellen’s chart and an ophthalmoscopic examination of eyes.
Test eyes for peripheral vision. Observe eyes for extraocular muscle movement;
oculomotor (CN III), trochlear (CN IV), and abducens (CN VI) nerves are tested together because they control eye movement.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
56

Examination: Special Circumstances and Advanced Practice (contd.)
Assess individual cranial nerves: Observe eyes for pupillary size, shape, equality,
construction, and accommodation. Evaluate face for movement and sensation; evaluate the
trigeminal nerve (CN V) for facial movement and sensation. Test motor function by having patient
clench his or her teeth, then palpate temporal and masseter muscles for muscle mass and strength; there should be bilaterally strong muscle contractions.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
57

Examination: Special Circumstances and Advanced Practice (contd.)
Assess individual cranial nerves: Test ears for hearing and balance (CN VIII).
• Whisper test, Weber/Rinne. P.166-8 Test tongue for taste (CNs VII, IX).
• Sweet, salty (VII); sour, bitter (IX).• Not done unless problem reported.
Inspect oropharynx for gag reflex and soft palate movement (CNs IX, X).
• Touch posterior pharynx with tongue blade.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
58

Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
59

Examination: Special Circumstances and Advanced Practice (contd.)
Assess individual cranial nerves: Inspect tongue for movement, symmetry, strength,
absence of tumors (CN XII).
• Have patient protrude tongue, move toward nose, chin, side to side.
• Have patient press tongue against gloved finger.
Test shoulder and neck muscles for strength and movement (CN XI).
• Have patient shrug shoulders and turn head to side against hands.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
60

Examination: Special Circumstances and Advanced Practice (contd.)
Test cerebellar function for balance and coordination. Tests for balance:
Romberg test (patient standing)—feet together, arms at side, eyes open/closed.
Eyes closed, stand on one foot. Tandem walking. Hopping on one foot, then other. Knee bending. Walking on toes and heels.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
61

Examination: Special Circumstances and Advanced Practice (contd.)
Test cerebellar function for balance and coordination: Tests for coordination of upper extremity:
Rapid pronation/supination on thighs. Alternately touching nose with index
fingers (eyes closed). Touching each finger to thumb in
rapid sequence. Moving index finger between nose
and examiner finger. Tests for coordination of lower extremity:
Heel to shin of opposite leg.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
62

Examination: Special Circumstances and Advanced Practice (contd.)
Assess peripheral nerves. Assess for sensation:
Areas routinely assessed are the hands, lower arms, abdomen, lower legs, and feet.
Flex muscles, then resist against opposite force.
Dermatome map to identify spinal nerve providing sensation.
Monofilament for peripheral sensation for peripheral neuropathy.
Light touch with cotton tipped swab. Vibration using tuning fork on bony
prominence; feel vibration and when it stops.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
63

Examination: Special Circumstances and Advanced Practice (contd.)
Assess peripheral nerves Assess for sensation:
Kinesthetic sensation by moving finger and toe up and down.
Stereognosis by identification of familiar object in hand.
Two-point discrimination by touching parts of body simultaneously with two points—how many points felt?
Graphesthesia by identification of number and letter drawn on hand, back, other area.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
64

Examination: Special Circumstances and Advanced Practice (contd.)
Assess peripheral nerves Evaluate extremities for deep tendon reflexes:
Muscle contraction response to direct and indirect percussion of tendon.
Patient relaxed and lying or sitting down; 4+ scoring system.
Triceps reflex: Contraction of triceps muscle, extension of elbow.
Biceps reflex: Contraction of biceps muscle, flexion of elbow.
Brachioradial reflex: Pronation of forearm, flexion of elbow.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
65

Examination: Special Circumstances and Advanced Practice (contd.)
Assess peripheral nerves. Evaluate for deep tendon reflexes:
Patellar reflex: Contraction of quadriceps muscles, extension of lower leg.
Achilles tendon: Contraction of gastrocnemius muscle, plantar flexion of toes.
Plantar: Plantar flexion of toes using end of handle on reflex hammer, stroke lateral aspect of sole of foot from heel to ball, curving medially across the ball of the foot; expected findings should be plantar flexion of all toes.
Ankle clonus reflexes if reflexes are hyperactive: Sharply dorsiflex foot, maintain in flexion; should be no movement.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
66

Examination: Special Circumstances and Advanced Practice (contd.)
Evaluate superficial reflexes (little clinical significance for presence or absence): Abdominal reflexes by stroking abdomen away from
umbilicus. Cremasteric reflexes (men) by stroking upper, inner
thigh; testicle should rise slightly.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
67

Additional Assessment for Special Cases
Altered level of consciousness (LOC): Nurse can determine if the patient is alert
and oriented by the way questions are answered during interview.
Change in LOC is earliest and most sensitive indicator of alterations in cerebral function. Awareness is higher level function
controlled by reticular activating system.
Wakefulness is controlled by brainstem.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
68

Additional Assessment for Special Cases (contd.)
Altered LOC Assessing awareness:
Determined by orientation, memory, attention, calculation, recall, and language, as well as judgment, insight, and abstraction.
Awareness—mental status (orientation, memory, attention, calculation, recall, language, insight, abstraction).
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
69

Additional Assessment for Special Cases (contd.)
Altered LOC: If orientation is a concern during history, determine if
oriented to time, place, and person. Date and time is first orientation to
disappear. Only a problem if remains
disoriented after being reoriented. Place is second orientation to
disappear. Person is last orientation to disappear.
Orientation returns in opposite order in which is lost.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
70

Additional Assessment for Special Cases (contd.) Altered LOC:
Assessing arousal—modified assessment for unconscious individual who cannot participate. When interacting: Assume ability
to hear. Pupillary reaction: Hold eyelid open
when shining light. Inspect to observe respiratory pattern.
Cheyne-Stokes is alternating periods of apnea with hyperventilation (brainstem compression).
Central neurogenic hyperventilation is sustained hyperventilation (lesions of midbrain/pons).
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
71

Additional Assessment for Special Cases (contd.)
Altered LOC: Assessing arousal—modified assessment for unconscious individual
who cannot participate. Smell breath for alcohol.
Pupillary response: CN III oculomotor, which originates in midbrain.
Small, reactive pupils: Bilateral cerebral dysfunction.
Bilaterally dilated pupils: Overdose of hallucinogens or CNS stimulants; pressure in brainstem compressing CN III bilaterally.
Unilateral fixed and dilated pupil: Pressure on ipsilateral CN III.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
72

Additional Assessment for Special Cases (contd.)
When patient’s awareness cannot be assessed because unconscious, awakening is assessed. Glasgow Coma Scale: Assess LOC using 15-point scale. Assess for best response to eye opening, motor
response, and verbal response. Determine stimulation or pain required to elicit
response.
Only time acceptable to inflict pain on patient.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
73

Additional Assessment for Special Cases (contd.)
Assessing awakening: First stimulation is touch, normal voice tone. Shake patient on shoulder or leg; shout. Painful stimuli begin peripherally, move centrally.
Applied until patient responds in some way or for at least 15 seconds, but no more than 30 seconds.
Begin by depressing nail bed at cuticle with your fingernail or length of pen or pencil.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
74

Additional Assessment for Special Cases (contd.)
Assessing awakening: Squeeze trapezius muscle very hard. Push upward on supraorbital notch above eye.
Best motor response describes and assigns arbitrary number to level of movement. 5: Localization of pain: Moves to remove stimulus. 4: Attempt to withdraw from stimulus. 3: Abnormal flexion (decorticate). 2: Abnormal extension. 1: No response.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
75

Additional Assessment for Special Cases (contd.) Meningeal irritation: Assessed when meningitis
suspected Kernig’s sign: Flexing one leg at hip and
knee, then extending knee: No pain indicates negative Kernig’s sign. If inflammation of meninges, patient
reports pain along vertebral column when leg is extended.
Brudzinski’s sign tested with patient supine. Patient’s neck flexed: Reports no pain or
resistance to neck flexion. Positive Brudzinski’s sign patient
passively flexes hip and knee in response to head flexion; reports pain along vertebral column.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
76

Age-Related Variations: Infants, Children, and Adolescents There are several differences in
assessment of system for infants and young children. Infants’ sensation and cranial nerves are assessed by
observation. Unique reflexes are assessed in infants. Children’s motor development is compared with
standardized tables of normal age and sequences of motor development.
Assessment of older children and adolescents follows same procedures and reveals similar expected findings.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
77

Age-Related Variations: Older Adults
Assessing neurologic system of an older adult usually follows same procedures as for younger adults.
Tests for balance and gait are often assessed for older adults to identify those at risk for falls.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
78

Disorders of the CNS: Multiple Sclerosis
Multiple sclerosis: Progressive demyelination of nerve fibers of brain and
spinal cord Autoimmune disorder initiated by virus attacks on
myelin at various sites of CNS
Symptoms vary depending on areas of central nervous system demyelinated: Symptoms: Fatigue, depression, paresthesias Signs: Clinical findings Signs and focal muscle weakness, ocular changes,
bowel, bladder, sexual dysfunction, gait instability, spasticity
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
79

Disorders of the CNS:Meningitis
Meningitis: Inflammation of meninges that surround brain and
spinal cord. Invasion of bacteria, viruses, fungi, parasites, or other
toxins. Bacterial meningitis most common; death results if not
treated promptly. Viral meningitis: Self-limiting infection with full
recovery.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
80

Disorders of the CNS:Meningitis (contd.)
Clinical findings: Meningitis: Symptoms: Severe headache, fever, and generalized
malaise. Signs: Stiff neck, and positive Brudzinski’s and Kernig’s
signs. LOC may decrease (drowsiness and reduced attention
span), may progress to stupor and coma. Confusion, agitation, and irritability may occur.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
81

Disorders of the CNS:Encephalitis
Encephalitis is inflammation of brain tissue and meninges. Caused by bacteria, viruses, fungi, and parasites; viral encephalitis
most common.
Clinical findings: Symptoms depend on invading organism and part of brain involved. Onset may be gradual or sudden with symptoms of headache, lethargy,
irritability, nausea, signs of fever, nuchal rigidity, and vomiting. May develop decreased consciousness, motor weakness, tremors,
seizures, aphasia, and positive Babinski’s sign over several days.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
82

Disorders of the CNS:Spinal Cord Injury
Spinal cord injury (SCI): Any traumatic disruption of spinal cord. Vertebral fractures or dislocations—car accidents,
sports injuries, and other violent impacts.
Injury to cervical spinal cord: Quadriplegia—injury to the thoracic or lumbar spinal cord—or paraplegia.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
83

Disorders of the CNS:SCI (contd.)
Clinical findings: SCI: Symptoms of complete spinal cord transection:
paresthesia or anesthesia. Signs: Paralysis below level of injury; loss of bowel and
bladder control. SCIs damage upper motor neurons causing spastic
paralysis. When injury incomplete, manifestations are variable
and correlates to location and extent of injury.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
84
Disorders of the CNS:Head Injury
Craniocerebral injury (head injury): Injury to scalp, skull, brain sufficient to alter normal
function. Open-head injuries result from fractures or penetrating
wounds. Closed-head injuries result from blunt head injury:
Cerebral concussion, contusion, laceration.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
85
Disorders of the CNS:Head Injury (contd.)
Clinical findings: Craniocerebral injury: Depend on severity of trauma and areas of brain
involved (LOC for a few minutes to several weeks) May have residual deficits in memory, cognition, and
motor or sensory abilities.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
86

Disorders of the CNS:Parkinson’s Disease
Parkinson’s disease: Develops slowly as brain’s dopamine-producing
neurons in substantia nigra of basal ganglia degenerate; second most common neurodegenerative disease after Alzheimer’s disease.
Clinical findings: Resting tremor, bradykinesia, and rigidity. Other manifestations: Masklike facies, trunk-forward
flexion, muscle weakness, shuffling gait, and finger pill-rolling tremor.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
87

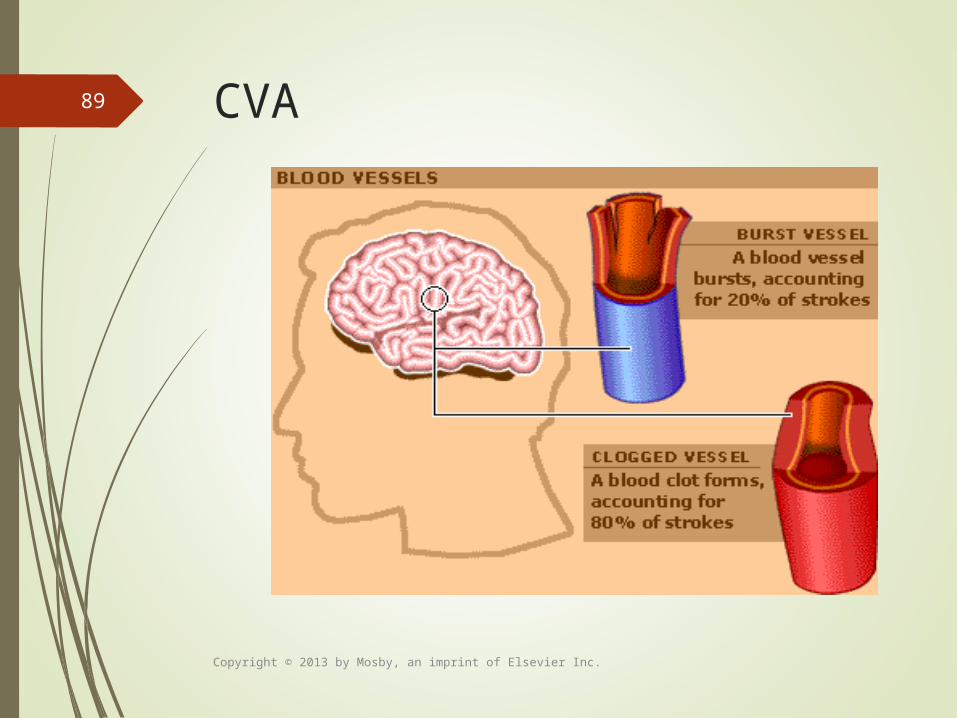
Disorders of the CNS:Cerebrovascular Accident
Cerebrovascular accident (CVA, stroke): When cerebral blood vessels
become occluded by thrombus or embolus, or when intracranial hemorrhage occurs, brain tissues become ischemic, resulting in CVA or stroke.
Hemorrhage can be caused by hypertension or a cerebral aneurysm (a weakened area in an artery that balloons out due to high pressure of blood).
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
88
CVA
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
89
CVA Warning Signs
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
90

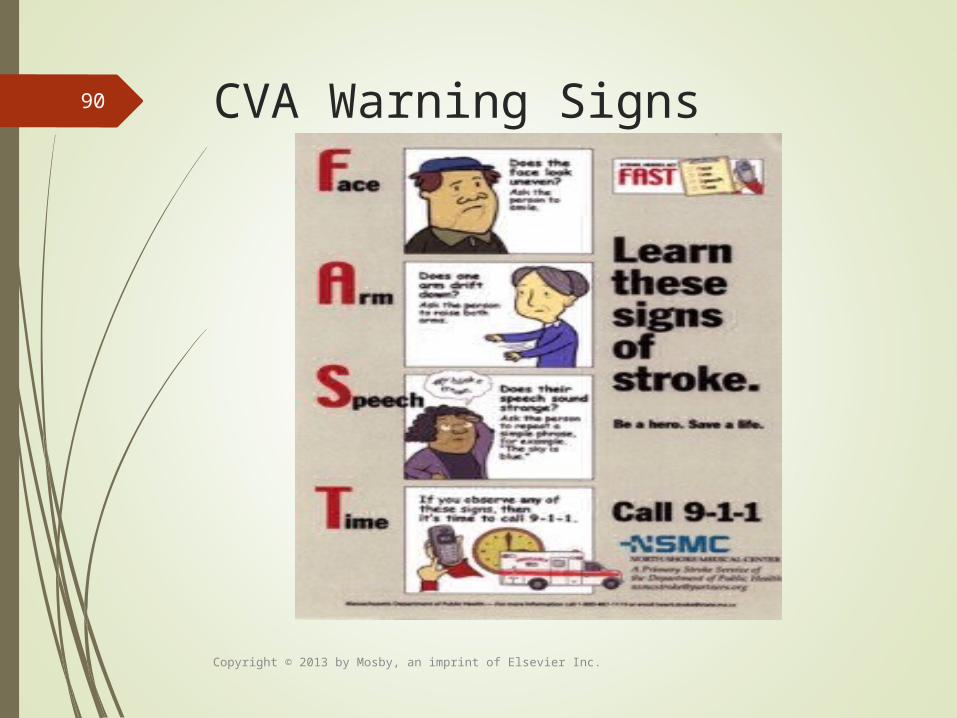
Disorders of the CNS: CVA (contd.)
Clinical findings: Signs and symptoms directly related to areas
of brain involved and extent of ischemia. Sudden unilateral numbness or weakness of
face, arm, or leg. Trouble walking, dizziness, or loss of balance. Sudden, severe headache with no known
cause. May be sudden confusion, difficulty
swallowing (dysphagia), difficulty speaking or understanding speech (aphasia), or partial loss of vision.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
91

Disorders of the CNS:Alzheimer’s Disease
Alzheimer’s disease: Incurable, degenerative neurologic disorder; begins
with decline in memory.
Most common cause of dementia in Western countries.
Cause unknown; theories suggest genetic tendency, environmental toxins, altered neurotransmitter function, autoimmune reaction, or slow virus.
Patients with history of small strokes have tendency to develop Alzheimer disease; stroke-prevention measures may reduce risk of developing disease.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
92

Disorders of the CNS:Alzheimer’s Disease (contd.)
Clinical findings: Alzheimer’s disease: Three stages of Alzheimer’s disease have been described:
Early stage lasts 2 to 4 years when patient’s memory begins to fail, such as forgetting names and misplacing items.
Second stage lasts from 2 to 12 years when patient experiences progressive memory loss and has difficulty with activities of daily living; language skills deteriorate and patient becomes disoriented and confused.
During final stage, patient requires total care and is unable to communicate.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
93

Disorders of Cranial Nerves:Trigeminal Neuralgia Trigeminal neuralgia:
Trigeminal neuralgia (tic douloureux)—intense paroxysmal pain (1 or all 3 branches of CN V).
Etiology is unknown but trauma to face or head or infection of teeth or jaw are contributing factors.
Many can identify trigger points: Small areas on cheek, lip, gum, forehead that initiate pain.
Clinical findings: Abrupt, intense unilateral pain along tissue innervated
by trigeminal nerve; lasts few seconds.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
94

Disorders of Cranial Nerves:Bell’s Palsy Bell’s palsy:
Acute unilateral paralysis of facial nerve. 80% of patients recover fully after few weeks or
months.
Clinical findings: History of pain behind ear or face few hours or days
before paralysis. Affected side: Eye does not close, forehead does not
wrinkle; patient is unable to whistle or smile.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
95

Disorders of Peripheral Nerves:Myasthenia Gravis
Myasthenia gravis: Neuromuscular disease with abnormal weakness of
voluntary muscles; improves with rest and anticholinesterase drugs.
Acetylcholine (Ach) receptor sites destroyed, so fewer receptor sites available to initiate muscle contraction, muscle weakness.
Some cases associated with tumors of thymus gland. Three types: Ocular (eyes); bulbar (swallowing),
generalized (skeletal muscles). Most common in younger women and older men.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
96

Disorders of Peripheral Nerves:Myasthenia Gravis (contd.)
Clinical findings: Ocular myasthenia: Weakness of muscles of eye (ptosis
and diplopia). Bulbar myasthenia: Aspiration of saliva and fluids
(impaired swallowing). Generalized myasthenia: Weakness of face, limbs,
trunk, including muscles of breathing.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
97

Disorders of Peripheral Nerves:Guillain-Barré Syndrome
Guillain-Barré syndrome: Widespread demyelinization of nerves of peripheral
nervous system (PNS). Motor component of peripheral nerves; believed to be
caused by cell-mediated autoimmune response to viral infection.
Respiratory or gastrointestinal viral infection weeks before onset.
80% to 90% recover with few or no residual deficits; however, patients may die if respiratory depression develops rapidly.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
98

Disorders of Peripheral Nerves:Guillain-Barré Syndrome (contd.) Clinical findings:
Ascending paralysis begins with weakness and paresthesia in lower extremities, and ascends to upper extremities and face.
Descending variation: Facial, glossopharyngeal, vagus, hypoglossal CNs downward to hand; can reach feet.
Deep tendon reflexes absent. If paralysis of thorax, respiratory depression may
result.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
99

Question 1
A patient suffered a head injury, and the neurologist notes a deficit in cerebellar function. As the nurse performs the neurologic assessment, which finding indicates a deficit in cerebellar function?
The patient is unable to count by serial sevens in reverse order.When doing the heel-shin exercise (patient supine), the patient’s heel overshoots shin and oscillates. The patient is unable to identify a paper clip (altered stereognosis).The right patellar deep tendon reflex is diminished.
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
100

Question 2
Three days after a camping trip, a patient is in the hospital with a severe headache and photophobia. The nurse performed a test for Kernig’s sign and documented the results as negative. What best explains this action?
The Kernig’s sign assesses for level of consciousness. A negative finding indicates that the patient is alert and oriented to person, place, and time.The symptoms reported could be a sign of peripheral nervous system damage.The symptoms reported could be a sign of meningeal irritation.The Kernig’s sign is a good test of a patient’s ability to withstand deep tendon reflex assessments.Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
101

The End
Copyright © 2013 by Mosby, an imprint of Elsevier Inc.
102