Embed Size (px)
Citation preview

Health Policy Post Affordable Care Act, Part 2: The Fundamentals of Reimbursement
CombinedSectionsMeeting2014
February 3‐6, 2014
Las Vegas, Nevada
www.aptahpa.org Section on Health Policy & Administration
of the American Physical Therapy Association
Speaker(s): Ira Gorman, PT, PhD
Janice Kuperstein, PT, PhD
Robert Sandstrom, PT, PhD
Session Type: Educational Sessions
Session Level: Basic
This information is the property of the author(s) and should not be copied or otherwise used without the
express written permission of the author(s).

Health Policy 102: Fundamentals of Reimbursement Post ACA
Ira Gorman, PT, PhD, MSPH
President, Health Policy and Administration Section, APTA
Assistant Professor Regis University
Janice Kuperstein, PT, PhD
Associate Professor and Chair, Department of Rehabilitation Sciences
University of Kentucky

Objectives At the conclusion of this session, the attendee will be able to: 1. Describe the classic reimbursement structures
used by third party payers to reimburse/pay for physical therapy services
2. Relate the insurance market reforms of the ACA that improved insurance eligibility for the U.S. population
3. Identify emerging provider structure changes responding to the changed reimbursement environment

Objectives Section 1
• Describe the classic reimbursement structures used by third party payers to reimburse/pay for physical therapy services including:
– Prospective vs. retrospective payment
– Fee for service
– Case rate structures
– Capitation
– Pay for Performance

Two Schools of Thought
You can’t always get what you want
but if you try sometimes
you just might find
you get what you need Mick Jagger
(Famous Health Care Economist and…)

Your debutante just knows what you need
But I know what you want.
Bob Dylan, 1966

Health Care - Financing vs Delivery
• Financing- payment for service
– Includes premium and payment
• Delivery- providing service/care
• Most countries financing and delivery is in the public sector
• In the US, can be private, public or mixed.
• Payment can be retrospective or prospective

4 Modes of Health Care Financing in US
• Out of pocket payment
• Individual private insurance
• Employment based group insurance
• Government- Social insurance model

Out of Pocket Payment

Out of Pocket Expenses
• Non Covered services- ABN Medicare
• Deductible
• Co-Insurance
• Co-Payment
• Regressive
– 12% of income of lowest quintile
– 1.2% of wealthiest 5%

Individual Private Insurance

Employer-based insurance

Government Financed Insurance

Health Care Financing-2006 SOURCE OF COVERAGE
(Percentage of Population)
Uninsured 16%
Individual Private Insurance 5%
Employment Based Private Ins 51%
Government Financing 28%
Medicare 13%
Medicaid 12%
TriCare/Champus/Military 3%

Health Care Financing-2006
– TYPE OF PAYMENT/ Source of Funds
• Out of Pocket 12%
• Individual Private Insurance 3%
• Employment based Private Ins 32%
• Other private funds 7%
• Government Financing 46% – Medicare 20%
– Medicaid (state & Fed) 13%
– Other Federal (VA, military) 7%
– Other State (SCHIP) 6%

Health Care 2011-2012 U.S. Census Bureau, Current Population Survey, 2012 and 2013 Annual Social and Economic
Supplements.
SOURCE OF COVERAGE (Duplicate coverage exists)
(Percentage of Population) 2011 2012
Any Private Plan 63.9% 63.9%
Employment Based Private Ins 55.1% 54.9%
Individual Private Insurance 9.8% 9.8%
Government Financing 32.2% 32.6%
Medicare 16.5% 15.7%
Medicaid 14.1% 16.4%
TriCare/CHAMPVA/Military 4.4% 4.4%
Uninsured 15.7% 15.4%

Insurance Products
• Indemnity
• PPO
• EPO
• HMO
• POS/ Open or managed choice
• Health Savings Account (HSA) with High Deductible Health Plan (HDHP)

Indemnity
• “Traditional” insurance plan
• Definition: to secure from loss or hurt
• Fixed cash amount or percentage paid to beneficiary (typically 80/20 coinsurance)
• May be per day, per procedure, per visit
• Patient responsible for balance > benefit
• Relatively easy to administer
• Increasingly rare in health care

Self Insurance
• Is Self “Funded” by employer
• Not self=individual
• Avoids risk and administrative charges
• Looks the same to employee/consumer
• Uses TPAs (Third party Administrator)
• Increasing trend in large and smaller employer groups ( Regis, UK, Coors, etc.)
• ERISA Exempt

Health Maintenance Organization
• HMO- coined by Paul Ellwood in 1971
• A form of health insurance that contracts with employers or other payers to provide health care services for members on a prepaid basis.
• HMOs are organizations that combine insurer and providers into one entity.
• Emphasis on preventive care
• Consumer has restricted choice of providers

HMO Act of 1973
• An organized system for providing health care in a geographic area
• An agreed upon set of basic and supplemental health maintenance and treatment services
• A voluntarily enrolled group of people
• A community rating

Preferred Provider Organization
• PPO- A system of health care delivery that provides a discounted fee structure in exchange for granting a provider “preferred” status in treating the group’s members. • Consumer enjoys higher level of coverage for
selection a preferred provider
• EPO- exclusive provider more restrictive greater discounts

Health Savings Account with High Deductible Health Plan
• 2014 -$3300 for individual, $6550 for families
• $1000 additional allowed if ≥ 55 years old
Contributions by individual and/or employer to a tax-advantaged account
• Annual deductible ≥ $1200 individual / $2500 families
Must be paired with a high-deductible insurance plan
• But what are the responsibilities and potential consequences
Individual directs and manages expenditures

<1%
1%
1%
1%
2%
3%
3%
3%
5%
5%
4%
7%
8%
10%
27%
46%
73%
16%
17%
19%
20%
20%
21%
20%
21%
25%
24%
27%
24%
29%
28%
31%
21%
16%
56%
55%
58%
60%
58%
57%
60%
61%
55%
54%
52%
46%
42%
39%
28%
26%
11%
9%
10%
8%
10%
12%
13%
13%
15%
15%
17%
18%
23%
21%
24%
14%
7%
19%
17%
13%
8%
8%
5%
4%
2012
2011
2010
2009
2008
2007
2006
2005
2004
2003
2002
2001
2000
1999
1996
1993
1988
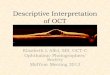
Conventional HMO PPO POS HDHP/SO
NOTE: Information was not obtained for POS plans in 1988. A portion of the change in plan type enrollment for 2005 is likely
attributable to incorporating more recent Census Bureau estimates of the number of state and local government workers and
removing federal workers from the weights. See the Survey Design and Methods section from the 2005 Kaiser/HRET Survey of
Employer-Sponsored Health Benefits for additional information.
SOURCE: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2012; KPMG Survey of Employer-Sponsored Health
Benefits, 1993, 1996; The Health Insurance Association of America (HIAA), 1988.
Distribution of Health Plan Enrollment for Covered Workers,
by Plan Type, 1988-2012

Units of Payment
• Fee for service - procedure
– may be discounted or scheduled
– UCR - usual doctors practice, customary community, reasonable by physicians in area
– RBRVS- labor, practice, liability=total units
• Per diem = per day/hospital , per visit/out
– bundling of services
– still at risk for number of days/visits
– can be used in outpatient programs

RBRVS
• Resource based relative value scale
• January 1, 1992- HCFA for CPT codes
• 3 components, vary by region
– work
– practice expense
– liability/ malpractice
• Reimbursement more accurate for amount of work and risk than previous UCR

Units of Payment II
• Episode of illness- DRG or case rate
• One fee independent of usage or intensity
– DRG- Diagnosis related group- 1983 PPS
– 492 DRGs with modifiers for exceptions
– Case rates for surgery and PT by Diagnosis

Units III - Capitation
• One payment for each patient per month independent of service or usage
• Unit is the patient or number of patients
• Per capita or “by the head”
• Two tiered or three tiered
• changes concept of risk


Units of Payment IV
• Salaried- unit is time
• Common in military, VA, mental health, teaching hospitals
• Staff model HMOs
• Global budget- unit is institution
– most aggregated and risk for hospital
– Kaiser, VA, Military

Risk Comparison
• Risk shifts to provider from payer with increase aggregation of payment
• Fee for service the least
• Capitation and global budget the most
• Risk versus quality


Pay for Performance
• A shift from payment based on VOLUME to payment based on OUTCOMES
• Examples
– Physician Quality Reporting System - PQRS
– Accountable Care Organizations – ACOs

Medicare Physician Quality Reporting System (PQRS)
• Linking Payment to Quality Outcomes
in Medicare: • The Centers for Medicare and Medicaid Services
finalized the use of the calendar year 2013 reporting
period to inform the 2015 payment adjustment.
• Eligible professionals, including physical therapists that
do not satisfactorily report data on quality measures for
the January 1, 2013-December 31, 2013 reporting
period, will be subject to the 1.5% adjustment in their fee
schedule amount in 2015

PQRS
• Physical therapists are eligible to participate in
11 different PQRS measures.
• To participate in PQRS using individual
measures an individual therapist must report on
a minimum of 3 measures for 50% of all
Medicare patients seen during the reporting
period if reporting via claims,
• or on a minimum of 3 measures for 80% of all
Medicare patients seen during the reporting
period if reporting via registry.

2013 PQRS Individual Measures
• Chronic Wound Care Measures (2)
• Diabetic Foot and Ankle Care Measures (2)
• Documentation of Current Medications Measure
• Falls measures (2)
• Outcome Assessment
• Pain Assessment Measure
• BMI
• Participation in Clinical Database Registry

2013 PQRS Group Measures
• Physical therapists are eligible to participate in
one group PQRS measure. To participate in
PQRS using the group measure an individual
therapist must report on all measures within the
group for a minimum of 20 unique Medicare
patients seen during the reporting period if
reporting via claims or registry
– Measure 148 Back Pain Initial Visit
– Measure 149 Back Pain Physical Exam
– Measure 150 Back Pain Advice for Normal Activities
– Measure 151 Back Pain Advice Against Bed Rest

Objectives Section 2
• Relate the insurance market reforms of the ACA that improved insurance eligibility for the U.S. population including
– Guaranteed issue of private insurance
– Individual mandate to purchase insurance
– Expansion of Medicaid
– American Health Benefit Exchanges
• Government subsidies to improve affordability

Patient Protection and Affordable Care Act (P.L. 111-148)
ACA Highlights (http://kaiserfamilyfoundation.files.wordpress.com/2011/04/
8061-021.pdf)
• Expanded access to coverage – Individual mandate
– Employer requirements
– Medicaid expansion
• Health Insurance Exchanges
• Essential Benefits Package

With Medicaid Expansion Without Medicaid
Expansion
Up to 100% of poverty Medicaid Unsubsidized
100-138% of poverty* Medicaid Exchange
138-400% of poverty Exchange Exchange
>400% of poverty Unsubsidized Unsubsidized
NOTES: Poverty Level is $11,170 for a single person and $23,050 for a family of four
*Medicaid eligibility cut off is 133% FPL, however 5% of income is disregarded, making the threshold 138% FPL
SOURCE: Kaiser Family Foundation
How People Get Covered

From Kaiser Family Foundation Webpage

ACA Highlights Continued
• Changes to private insurance
– MLR ≥ 85% or 80%
– No lifetime limits of coverage
– Guaranteed issue, no pre-existing condition exclusion, premium rating restrictions

ACA Highlights Continued
• Medicare – Create an Innovation Center within CMS to test, evaluate,
and expand different payment structures and methodologies to reduce expenditures while maintaining or improving quality of care.
– Reduce Medicare payments that would otherwise be made to hospitals by specified percentages to account for excess (preventable) hospital readmissions. (Effective October 1, 2012)
– Reduce Medicare payments for hospital-acquired conditions by 1%. (Effective fiscal year 2015

ACA Highlights Continued • Allow providers organized as accountable care
organizations (ACOs) that voluntarily meet quality thresholds to share in the cost savings they achieve for the Medicare program.
– To qualify as an ACO, organizations must agree to be accountable for the overall care of their Medicare beneficiaries, have adequate participation of primary care physicians, define processes to promote evidence-based medicine, report on quality and costs, and coordinate care

ACA Highlights Continued
• Establish a national Medicare pilot program to develop and evaluate paying a bundled payment for acute, inpatient hospital services, physician services, outpatient hospital services, and post-acute care services for an episode of care that begins three days prior to a hospitalization and spans 30 days following discharge.

ACA Highlights Continued
• Improving Quality / Health System Performance
– Support comparative effectiveness research by establishing a non-profit Patient-Centered Outcomes Research Institute to identify research priorities and conduct research that compares the clinical effectiveness of medical treatments = PCORI
– Create the Independence at Home demonstration program to provide high-need Medicare beneficiaries with primary care services in their home and allow participating teams of health professionals to share in any savings

ACA Highlights Continued
• Improving Quality / Health System Performance
– Establish a hospital value-based purchasing program in Medicare to pay hospitals based on performance on quality measures
– Extend PQRS
– Develop plans to implement value-based purchasing programs for skilled nursing facilities, home health agencies, and ambulatory surgical centers

ACA Highlights Continued
• Prevention and Wellness
– National strategy development supported by grant funding
– Evaluate and support (technical assistance and other resources) employer-based wellness programs
– Permit employers to offer employee rewards for participation (e.g. reduction in premiums, waiver of cost sharing)
– Eliminate cost-sharing for preventive services recommended by the U.S. Preventive Services Task Force

Triple Aim from IHI
• Improved experience of care
• Improved health of populations
• Reduced cost

THINK, PAIR, SHARE
Like them or not, identify
opportunities for physical therapy to
be involved in healthcare reform


Yes, have been
contacted about the
law 10%
No, have not been
contacted about the
law 90%
NOTE: Other, Don’t remember (VOL.), and Don’t know/Refused answers not shown for follow-up question. SOURCE: Kaiser Family Foundation Health Tracking Poll (conducted August 13-19, 2013)
One in Ten Say They’ve Been Contacted About Law
Percent who mentioned
Information about the law (general) 27%
Arguments against the law 11
Arguments in favor of the law 9
Did not listen/hung up 8
Called about a survey/asked me questions 6
Political arguments 4
Tried to sell me insurance 3
Heard from both sides: in favor and against 2
Have you been personally contacted by anyone about the health care law through a phone call, email, text message, or door to door visit, or not?
Among the 10% who say they have been contacted: What did that person want to tell you about the health care law? {open-end}

Medicaid Expansion
• Optional expansion of Medicaid eligibility to include non-elderly, non-disabled adults up to 138% (133% + 5%) of Federal Poverty Level
• Federal government will cover the costs for the newly eligible at 100% through 2016
– Gradually decreases to 90% by 2020
– “Grand experiment” or opportunity to improve health of this population to decrease cost

Federal Poverty Guidelines 2014
Family Size 100% FPL 62% FPL
1 $11,490 $7,124
2 $15,510 $9,616
3 $19,530 $12,109
4 $23,550 $14,601
Cutoff prior to ACA Expanded Medicaid in Kentucky

Medicaid http://www.hcfa.gov/medicaid
• Title XIX of SSA, July 30, 1965
• Federal/State welfare program
• Average split 57% Fed, 43% State (50-83%)

Eligibility Prior to ACA
• Parent, children and pregnant women with low income
• Persons receiving Supplemental Security Income (Older adults with low income, individuals with disabilities)
• Special eligibility for pregnant women with low income (185% FPL): PRESUMPTIVE ELIGIBILITY

Copyright © 2012 American Medical
Association. All rights reserved.
From:
Medicaid
Expansion
Under the
Affordable
Care Act
JAMA.
2013;309
(12):1219
-1219.
doi:10.10
01/jama.
2013.248
1

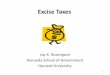
NOTES: Data are as of January 28, 2014. *AR and IA have approved waivers for Medicaid expansion; MI has an approved waiver for expansion and plans to implement in Apr. 2014; IN and PA have pending waivers for alternative Medicaid expansions; WI amended its Medicaid state plan and existing waiver to cover adults up to 100% FPL, but did not adopt the expansion. SOURCES: States implementing in 2014 and not moving forward at this time are based on data from CMS here States noted as “Open Debate” are based on KCMU analysis of State of the State Addresses, recent public statements made by the Governor, issuance of waiver proposals or passage of a Medicaid expansion bill in at least one chamber of the legislature.
Current Status of State Medicaid Expansion Decisions, 2014
WY
WI*
WV
WA
VA
VT
UT
TX
TN
SD
SC
RI
PA*
OR
OK
OH
ND
NC
NY
NM
NJ
NH
NV NE
MT
MO
MS
MN
MI*
MA
MD
ME
LA
KY KS
IA*
IN* IL
ID
HI
GA
FL
DC
DE
CT
CO
CA
AR* AZ
AK
AL
Implementing Expansion in 2014 (26 States including DC)
Open Debate (6 States)
Not Moving Forward at this Time (19 States)

Eligibility Post Expansion
Family Size 100% FPL 138% FPL
1 $11,490 $15,856
2 $15,510 $21,404
3 $19,530 $26,951
4 $23,550 $32,499

Medicaid Enrollees are Sicker and More Disabled Than the Privately-Insured
38%
26%
36%34%
25%28%
12% 13%
6%
12%10%
4%
Fair/Poor
Health
Physical &
Mental Chronic
Condition
Unable/Limited
Work Due to
Health
Fair/Poor
Health
Physical &
Mental Chronic
Condition
Unable/Limited
Work Due to
Health
Medicaid Privately Insured
Poor (<100% FPL)
Near Poor
(100-199% FPL)
Note: Adults 19-64.
SOURCE: KCMU analysis of MEPS 3-year pooled data, 2004-2006.

Essential Health Benefit (EHBs)
• Health plans that will be offered in the Marketplaces (and to newly eligible Medicaid recipients) must cover the following benefits:
• (1) ambulatory patient services; (2) emergency services; (3) hospitalization; (4) maternity and newborn care; (5) mental health and substance use disorder services, including behavioral health treatment; (6) prescription drugs; (7) rehabilitative and habilitative services and devices; (8) laboratory services; (9) preventative and wellness services and chronic disease management; and (10) pediatric services, including oral and vision care.

Provider Network Adequacy
• Reasonable access to sufficient
number of in-network HCPs
• If not in network, see APTA
resource Tips

Value-Based Purchasing
• Change in reimbursement mechanism from volume-based (more you do, more you earn) to value based (based on processes and outcomes of care).
• Advantages and disadvantages

Use Data with Five Whys • NH Compare or HH Compare
• Worse than peer groups in mobility
• WHY? What can PT do about it?
• Acute care hospital with high LOS in ICU • WHY? What can PT do about it?
• Inpatient Rehab Facility with long LOS • WHY? What can PT do about it?
• Primary care providers overwhelmed with
new patients seeking care • WHY? What can PT do about it?

Objectives Section 3
• Identify emerging provider structure changes responding to the changed reimbursement environment including
– Accountable Care Organizations (ACOs)
– Patient Centered Medical Homes(PCMHs)

ACO Definition
§ 3022 of the Affordable Act establishes a Shared Savings Program
• Group of health care providers accountable for the quality, cost, and overall care of the Medicare fee-for-service beneficiaries assigned to the organization
• Three Part Aim: 1. better care for individuals;
2. better health for populations; and
3. lower growth in expenditures
• Must meet specified quality performance standards to receive a share of any savings if the actual per capita expenditures of their assigned Medicare beneficiaries are a sufficient percentage below benchmark amounts set by CMS

Shared Savings • ACOs paid under current Medicare FFS payment
• Shared savings payments directly to the ACO
• CMS develops a benchmark for each ACO to assess
performance (estimate of FFS Part A and B costs if
provided absent ACO)
• Benchmark factors in patient characteristics and is
updated annually

Shared Savings
• ACOs must opt into one of two risk-sharing models, which will determine the percentage of savings that ACOs are eligible to receive: – One-Sided Risk Model—Savings are shared for the first
two years and then in the third year savings and losses are shared (50% of the savings are shared)
– Two-Sided Risk Model—Savings and losses are shared for all three years (60% of the savings
are shared)

PTs as Eligible Participants
• ACO participants – ACO professionals can contract and participate in ACOs but cannot form ACOs on own (PTs in private practice, physical therapy groups, Rehab Agencies, SNFs, HHAs)

ACO opportunities
• PTs as participants in ACOs can demonstrate to ACO professionals their value in improving care and decreasing costs
• Demonstrate to the public the knowledge, expertise and value of physical therapy as a component of integrated care with quality measures.
• Demonstrate the positive results of PTs as participants as evidenced by improved outcomes and increased shared savings for the ACO.

DISPELLING MYTHS
• APTA Resources are excellent
• Kaiser Family Foundation
• Commonwealth Fund

Patient Centered Medical Home

PCMH
• The medical home is intended to modernize
andbuild the practice infrastructure to support
high quality primary care, which the Institute
of Medicine(IOM) defines as “the provision of
integrated, accessible health care services by
clinicians who areaccountable for addressing
a large majority of personal health care
needs, developing a sustained partnership
with patients, and practicing in the context of
family and community” (IOM, 1978; IOM,
1996).

Features of PCMH
• Patient-centered: A partnership among practitioners, patients, and their families ensures that decisions respect patients’ wants, needs, and preferences, and that patients have the education and support they need to make decisions and participate in their own care.
• Comprehensive: A team of care providers is wholly accountable for a patient’s physical and mental health care needs, including prevention and wellness, acute care, and chronic care.

Features of PCMH • Coordinated: Care is organized across all elements of the
broader health care system, including specialty care, hospitals, home health care, community services and supports.
• Accessible: Patients are able to access services with shorter waiting times, "after hours" care, 24/7 electronic or telephone access, and strong communication through health IT innovations.
• Committed to quality and safety: Clinicians and staff enhance quality improvement through the use of health IT and other tools to ensure that patients and families make informed decisions about their health.

Pillars of the PCMH
Heath
Information
Technology
Primary Care Modified from the
Family Physician
Foundation

Performance
Measurement
Culture of
Improvement
Reliable
Systems
• Quality measures should be
based in strong clinical
evidence
• You can’t improve what you
don’t measure
• Starts with a culture of
improvement
• Ensure quality
improvement initiatives
are not punitive; should not
discourage physicians from
caring for patients
• Develop reliable systems
to collect information
Quality
Measures

Personalized Care Convenient Access Care Coordination
• Patients want convenient
access to information,
communication, and care
• Patients want to access
to care when they are ill
• Patients are engaged in their
own care and want to share
in decision-making
• Patients want increased
ability to access information
• Patients want coordinated
care
• Patients want new
approaches to care: group
visits and on-line services
Patient
Experience Quality
Measures

Practice
Organization
Personnel Management Clinical Systems
• Every team member
understands the important
role they play in delivering
efficient care and is
empowered to make
suggestions for
improvement
• Lab testing
• Prescriptions
• Patient Registries
Financial Management
• All staff are aware of the
most effective ways to
deliver care
• National policies support the
investment of resources into
primary care practices that
are effective and efficient
Quality
Measures
Patient
Experience

Business & Clinical
Process Automation
Connectivity &
Communication
Evidence-Based
Medicine Support
Clinical Data Analysis
& Representation
• Patient reminders
• Patient notification for
new information
• Reminders for
recommended care or
health maintenance
• Makes patient registries
possible
• Can quickly pull clinical
data for quality analysis
• Can enhance business
processes
• Enhances care
coordination by
improving information
flow with other
physicians, practices,
and providers
• Improves patient -
provider communication
• Point-of-care learning
(e.g., Up-to-Date)
• Clinical decision support
(e.g., Epocrates)
Practice
Organization
Quality
Measures
Patient
Experience
Health
Information
Technology



Opportunities for PTs and PTAs in PCMHs
• As part of PCMH – Opportunity to join a practice
• As providers for PCMH – Opportunity to be physical therapy provider of choice
based on
• Outcomes
• Communication
• Patient satisfaction
• Access


Physical Therapy Classification and Payment System (PTCPS)
• The model will recognize the clinical reasoning and decision making by the physical therapist's evaluative process in addition to the planned interventions.
• The model will facilitate and promote the use and reporting of quality measures, electronic health records, and participation in national registries to provide essential data to improve the model over time.
• The model will promote and encourage accurate reporting and appropriate payment of services and significantly reduce inappropriate use, waste, and fraud.
• This model will take extensive education of physical therapists, other health care organizations and professionals, policymakers, governmental agencies, payers, and accrediting and licensing bodies.

PTCPS Continued
• The model assumes patient/client management is a continuum of care involving patient interaction across multiple episodes of care for specified physical therapist-directed care.
• Initially, the model will focus on payment for physical therapy services furnished in outpatient settings.
• The payment model will be designed so that it would be feasible in the future to adapt for use as a payment methodology for physical therapy services furnished in all settings.

PTCPS Continued
• The model assumes that on each visit the physical therapist should interact with the patient and qualified health care personnel involved in the visit and determine based on the patient's acuity and the planned interventions the appropriate use of qualified personnel.
• The model will incorporate the World Health Organization's (WHO) International Classification of Function (ICF) framework to the extent possible and applicable.
• There will continue to be the ability to separately report services outside of the model.
• The model assumes documentation shall include clinical reasoning and support the medically necessary services

Evaluation Based on Clinical Complexity of the Evaluation
Clinical Considerations and
Complexity
of the Examination
Evaluation
Level of Evaluation
Limited/Problem-focused 1
Moderate/Detailed 2
Significant/Comprehensive 3
.

The Visit/Session Based Examination (Patient Severity) and Intervention (Intensity of Visit)
Patient Severity at the Time of the Visit
Intensity of
the Visit
Limited Moderate Significant
Limited 4 5 6
Moderate 7 8 9
Significant 10 11 12

HPA Award & Global Health Reception
Wednesday, February 5, 2014 8:00 pm – 10:00 pm
Light fare and cocktails
HPA The Catalyst is the Section on Health Policy & Administration of APTA