Embed Size (px)
Citation preview

Cushing’s syndrome
Dr. Atallah Al-RuhailyDr. Atallah Al-Ruhaily
Consultant EndocrinologistConsultant Endocrinologist

Cushing’s syndrome
Dr. Atallah Al-RuhailyDr. Atallah Al-RuhailyConsultant EndocrinologistConsultant Endocrinologist

Cushing’s Syndrome DefinitionsDefinitions
Cushing’ Syndrome:Cushing’ Syndrome: A state of chronic glucocorticoid excess leading to A state of chronic glucocorticoid excess leading to
constellation of symptoms and signs of constellation of symptoms and signs of hypercortisolism regardless of the cause.hypercortisolism regardless of the cause.
Cushing’s Disease:Cushing’s Disease: The specific type of Cushing’s syndrome due to The specific type of Cushing’s syndrome due to
excessive ACTH secretion from a pituitary tumor. excessive ACTH secretion from a pituitary tumor.
Ectopic ACTH syndrome:Ectopic ACTH syndrome: type of Cushing’s syndrome due to ACTH secretion by type of Cushing’s syndrome due to ACTH secretion by
nonpituitary tumor.nonpituitary tumor.

Cushing’s Syndrome
The most common cause is The most common cause is iatrogeniciatrogenic due to due to chronic use of glucocorticoid.chronic use of glucocorticoid.
Regardless of etiology, all cases of Regardless of etiology, all cases of endogenousendogenous or or spontaneousspontaneous Cushing’s syndrome are due to Cushing’s syndrome are due to overproduction of cortisol by the adrenal glands.overproduction of cortisol by the adrenal glands.
Most endogenous types are due to Most endogenous types are due to Bilateral Bilateral Adrenal Hyperplasia Adrenal Hyperplasia due to ACTH secretion by due to ACTH secretion by pituitary adenoma. pituitary adenoma.
Incidence of pituitary-dependent adrenal Incidence of pituitary-dependent adrenal hyperplasia in women is 3 times that in men.hyperplasia in women is 3 times that in men.
The most frequent age of onset is 3The most frequent age of onset is 3rdrd to 4 to 4thth decade. decade.

Cushing’s syndrome: Differential DiagnosisACTH-dependent
pituitary adenoma (Cushing’s disease)
non-pituitary neoplasm (ectopic ACTH)
ACTH-independent
Iatrogenic (glucocorticoid, megestrol acetate)
Adrenal neoplasm (adenoma, carcinoma)
Nodular adrenal hyperplasia
• primary pigmented nodular adrenal disease.
• massive macronodular adrenonodular hyperplasia
• food-dependent (GIP-mediated)
Factitious

Tumors causing ectopic ACTH syndome
• small cell carcinoma of the lung (50% of ectopic ACTH cases).
• pancreatic islet cell tumors.
• carcinoid tumors (lung, thymus, gut, pancreas, ovary).
• medullary carcinoma of the thyroid.
• pheochromocytoma and related tumors.

Pathology of Cushing’s Syndrome 1/3Pathology of Cushing’s Syndrome 1/3
Anterior Pituitary GlandAnterior Pituitary Gland– Pituitary adenoma (> 90% of Cushing’s disease):Pituitary adenoma (> 90% of Cushing’s disease):
» Microadenoma (< 10 mm in diameter) 80-90%.Microadenoma (< 10 mm in diameter) 80-90%.» Macroadenoma (> 10 mm in diameter) & could be Macroadenoma (> 10 mm in diameter) & could be
invasive.invasive.» Mostly benign adenoma; rarely malignant.Mostly benign adenoma; rarely malignant.
– Pituitary Hyperplasia: Pituitary Hyperplasia: » Diffuse hyperplasia of corticotrophs cells are rare.Diffuse hyperplasia of corticotrophs cells are rare.» Due to excessive stimulation of pituitary by CRH.Due to excessive stimulation of pituitary by CRH.

Pathology of Cushing’s Syndrome 2/3Pathology of Cushing’s Syndrome 2/3
Adrenocortical HyperplasiaAdrenocortical Hyperplasia– Bilateral hyperplasia of adrenal cortex.Bilateral hyperplasia of adrenal cortex.– Results from chronic ACTH hypersecretion.Results from chronic ACTH hypersecretion.– There are 3 types of adrenocortical hyperplasia:There are 3 types of adrenocortical hyperplasia:
1.1. Simple Adrenocortical Hyperplasia (Cushing’s disease)Simple Adrenocortical Hyperplasia (Cushing’s disease)
2.2. Ectopic ACTH syndromeEctopic ACTH syndrome
3.3. Bilateral Nodular HyperplasiaBilateral Nodular HyperplasiaNodular enlargement of adrenal glands resulting from long-standing Nodular enlargement of adrenal glands resulting from long-standing ACTH hypersecretion (pituitary or nonpituitary).ACTH hypersecretion (pituitary or nonpituitary).
There are 2 types of Bilateral Nodular Hyperplasia: There are 2 types of Bilateral Nodular Hyperplasia:
A.A. Primary Pigmented Nodular Adrenocortical Disease, PPNAD)Primary Pigmented Nodular Adrenocortical Disease, PPNAD)
B.B. Massive Macronodular Adrenal Hyperplasia). Massive Macronodular Adrenal Hyperplasia).

Pathology of Cushing’s Syndrome 3/3Pathology of Cushing’s Syndrome 3/3
Adrenal TumorsAdrenal Tumors– Adrenal Adenomas:Adrenal Adenomas:
» Glucocorticoids-secreting adenomas.Glucocorticoids-secreting adenomas.
» Encapsulated; Encapsulated;
» weigh 10 – 70 gr.weigh 10 – 70 gr.
» Size: 1- 6 cm.Size: 1- 6 cm.
– Adrenal Carcinomas:Adrenal Carcinomas:» Usually weigh over 100 gr.; commonly palpable mass.Usually weigh over 100 gr.; commonly palpable mass.
» Encapsulated.Encapsulated.
» May invade local structures.May invade local structures.

CLINICAL SYMPTOMS AND SIGNS CLINICAL SYMPTOMS AND SIGNS OF CUSHING’S SYNDROMEOF CUSHING’S SYNDROME
General:General:– Central obesityCentral obesity– Proximal muscle weaknessProximal muscle weakness– HypertensionHypertension– HeadachesHeadaches– Psychiatric disordersPsychiatric disorders
Skin:Skin:– Wide(>1cm), purple striaeWide(>1cm), purple striae– Spontaneous echymosesSpontaneous echymoses– Facial plethoraFacial plethora– HyperpigmentationHyperpigmentation– AcneAcne– HirsutismHirsutism– Fungal skin infectionsFungal skin infections
Endocrine and Endocrine and Metabolic Metabolic Derangements:Derangements:– Hypokalemic alkalosisHypokalemic alkalosis– OsteopeniaOsteopenia– Delayed bone age in Delayed bone age in
childrenchildren– Menstrual disorders, Menstrual disorders,
decreased libido, impotencedecreased libido, impotence– Glucose intolerance, Glucose intolerance,
diabetes mellitusdiabetes mellitus– Kidney stonesKidney stones– PolyureaPolyurea

Clinical features of Cushing’s syndrome 1/2
General :
-Obesity 90%
-Hypertension 85%
Skin:
-plethora (70%)
-hirsutism (75%)
-striae (50%)
-acne (35%)
-bruising (35%)
Musculoskeletal:
-osteopenia (80%)
-weakness (65%)
Neuropsychiatric (85%):
-emotional lability
-euphoria
-depression
-psychosis

Clinical features of Cushing’s syndrome 2/2
Metabolic:
-glucose intolerance(75%)
-diabetes (20%)
-hyperlipidemia (70%)
-polyuria (30%)
-kidney stones (15%)
Gonadal dysfunction:
-menstrual disorders (70%)
-impotence, decreased libido(85%)

Cushing’ DiseaseCushing’ Disease
The most common type of endogenous The most common type of endogenous Cushing’s syndrome (70%).Cushing’s syndrome (70%).
Female : Male Ratio about 8 : 1Female : Male Ratio about 8 : 1
Incidence age ranges from childhood to 70 Incidence age ranges from childhood to 70 years. years.

Ectopic ACTH HypersecretionEctopic ACTH Hypersecretion
15-20% of ACTH-dependent Cushing’ syndrome.15-20% of ACTH-dependent Cushing’ syndrome.
Very high ACTH may result in severe hypercortisolism Very high ACTH may result in severe hypercortisolism with lack of classical features of Cushing’s syndrome.with lack of classical features of Cushing’s syndrome.
More common in men.More common in men.
Age incidence: 40-60 years. Age incidence: 40-60 years.

Primary Adrenal TumorsPrimary Adrenal Tumors 10% of cases of Cushing’s syndrome.10% of cases of Cushing’s syndrome.
Most are benign adrenocortical adenomas.Most are benign adrenocortical adenomas.
Adrenocortical carcinomas are uncommon.Adrenocortical carcinomas are uncommon.
Both adenomas & carcinomas are more Both adenomas & carcinomas are more common in women.common in women.

Childhood Cushing’s SyndromeChildhood Cushing’s Syndrome Adrenal carcinoma is the commonest (51%) & Adrenal carcinoma is the commonest (51%) &
Adrenal adenoma (14%).Adrenal adenoma (14%).
More common in girls than in boys.More common in girls than in boys.
Most in age 1 – 8 years.Most in age 1 – 8 years.
Cushing’s disease more common in Cushing’s disease more common in adolescents (35%); most at age over 10 years.adolescents (35%); most at age over 10 years.

Routine Laboratory FindingsRoutine Laboratory Findings
High normal Hb, Htc & RBC.High normal Hb, Htc & RBC. WBC usually normal but lymphoctytes may be WBC usually normal but lymphoctytes may be
subnormal.subnormal. Eosinophils may be reduced.Eosinophils may be reduced. Electrolytes:Electrolytes:
Hypokalemia & alkalosis in marked steroid hypersecretion (ectopic ACTH).Hypokalemia & alkalosis in marked steroid hypersecretion (ectopic ACTH).
Impaired glucose tolerance or hyperglycemiaImpaired glucose tolerance or hyperglycemia Serum Calcium normal but hypercalciuria in 40%. Serum Calcium normal but hypercalciuria in 40%.

Features suggesting specific causesFeatures suggesting specific causes
Typifies classic clinical picture:Typifies classic clinical picture:– Female predominanceFemale predominance
– Onset age: 20 – 40 years.Onset age: 20 – 40 years.
– Slow progression over several years.Slow progression over several years.
Hyperpigmentation & hypokalemic alkalosis are rare.Hyperpigmentation & hypokalemic alkalosis are rare.
Androgenic manifestations are limited to acne & hirsutism.Androgenic manifestations are limited to acne & hirsutism.
Moderately increased cortisol & adrenal androgens. Moderately increased cortisol & adrenal androgens.
1. Cushing’s Disease

Features suggesting specific causesFeatures suggesting specific causes
Predominantly in males.Predominantly in males. Highest incidence at age 40 – 60 years.Highest incidence at age 40 – 60 years. Clinical manifestations are frequently limited to: weakness, Clinical manifestations are frequently limited to: weakness,
hyperpigmentation & glucose intolerance.hyperpigmentation & glucose intolerance. Primary tumor is usually apparent.Primary tumor is usually apparent. Hyperpigmentation, hypokalemia & alkalosis are common.Hyperpigmentation, hypokalemia & alkalosis are common. Weight loss & anemia are common.Weight loss & anemia are common. Hypercortisolism is of rapid onset.Hypercortisolism is of rapid onset. Steroid hypersecretion is frequently severe with equally Steroid hypersecretion is frequently severe with equally
elevated levels of glucocorticoids, androgens & DOC.elevated levels of glucocorticoids, androgens & DOC.
2. Ectopic ACTH Syndrome (Carcinoma)

Features suggesting specific causesFeatures suggesting specific causes
Slowly progressive course with typical features of Slowly progressive course with typical features of Cushing’s syndrome.Cushing’s syndrome.
Presentation may be identical to pituitary-dependent Presentation may be identical to pituitary-dependent Cushing’s disease & the responsible tumor may not be Cushing’s disease & the responsible tumor may not be apparent.apparent.
Hyperpigmentation, hypokalemic alkalosis & anemia are Hyperpigmentation, hypokalemic alkalosis & anemia are variably present. variably present.
3. Ectopic ACTH Syndrome (Benign Tumor)

Features suggesting specific causesFeatures suggesting specific causes
Usually the clinical picture of glucocorticoid excess alone.Usually the clinical picture of glucocorticoid excess alone.
Androgenic effects usually absent.Androgenic effects usually absent.
Gradual onset.Gradual onset.
Mild to moderate hypercortisolism.Mild to moderate hypercortisolism.
4. Adrenal Adenomas

Features suggesting specific causesFeatures suggesting specific causes
Rapid onset & rapid progression.Rapid onset & rapid progression.
Clinical picture of excessive glucocorticoids, androgens & Clinical picture of excessive glucocorticoids, androgens & mineralocorticoids secretion.mineralocorticoids secretion.
Marked elevation of cortisol & androgens.Marked elevation of cortisol & androgens.
Abdominal pain, palpable masses & metasteses in liver & lungs.Abdominal pain, palpable masses & metasteses in liver & lungs.
Hypokalemia is common.Hypokalemia is common.
5. Adrenal Carcinomas

Diagnosis of Cushing’s SyndromeDiagnosis of Cushing’s Syndrome
Clinical suspicion.Clinical suspicion.
Biochemical diagnosis of hypercortisolism status.Biochemical diagnosis of hypercortisolism status.
Differential diagnosis for etiology of hypercortisolism Differential diagnosis for etiology of hypercortisolism (Biochemical & Imaging Tests).(Biochemical & Imaging Tests).
Stages of Evaluation

Diagnosis of Cushing’s SyndromeDiagnosis of Cushing’s Syndrome Biochemical diagnosis of hypercortisolism statusBiochemical diagnosis of hypercortisolism status
1.1. Dexamethasone suppression testDexamethasone suppression test2.2. 24 h Urine free cortisol24 h Urine free cortisol3.3. Diurnal rhythm of cortisol secretionDiurnal rhythm of cortisol secretion
Differential diagnosis of etiology of hypercortisolism Differential diagnosis of etiology of hypercortisolism (Biochemical & Imaging Tests).(Biochemical & Imaging Tests).
1.1. Plasma ACTHPlasma ACTH2.2. Pituitary MRIPituitary MRI3.3. High-dose Dexamethasone suppression testHigh-dose Dexamethasone suppression test4.4. Inferior Petrosal Sinus Sampling with CRH stimulationInferior Petrosal Sinus Sampling with CRH stimulation5.5. Localizing occult ectopic ACTHLocalizing occult ectopic ACTH6.6. Adrenal localizing proceduresAdrenal localizing procedures

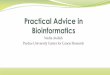
Diagnosis of Cushing’s syndromeDiagnosis of Cushing’s syndromeCushing’s syndrome suspected
Overnight 1mg Dexamethasone suppression test
High AM cortisol ( 3µg/dL) Low AM cortisol (< 3µg/dL)
Normal24-hour urine free cortisol
Normal
Repeat screening tests if highly suspected
Elevated
Hypercortisolism is confirmed
Needs differential diagnosis

Cushing’s syndrome established
<5 pg/mL >10 pg/mL
CT adrenals
Unilateral Mass Bilateral Enlargement
CRH test
Peak ACTH >20 pg/mL
Peak ACTH <10 pg/mL
Adrenal Surgery
MRI pituitary
AbnormalNormalIPSS
IPS/P>2.0IPS/P<1.8
Ectopic ACTH Pituitary Surgery
ACTH (by IRMA)

Problems in Diagnosis of Cushing’s SyndromeProblems in Diagnosis of Cushing’s Syndrome
Conditions:Conditions:1.1. DepressionDepression2.2. Alcoholism & withdrawal from alcohol intoxicationAlcoholism & withdrawal from alcohol intoxication3.3. Eating disorders (anorexia nervosa & bulimia)Eating disorders (anorexia nervosa & bulimia)
pseudo-Cushing’s syndromespseudo-Cushing’s syndromes

NON-CUSHING CAUSES OF NON-CUSHING CAUSES OF HYPERCORTISOLEMIAHYPERCORTISOLEMIA
Physical stressPhysical stressOperations, traumaOperations, traumaChronic exerciseChronic exerciseMalnutritionMalnutrition
Mental stress and psychiatric disordersMental stress and psychiatric disordersHospitalizationHospitalizationDrug and alcohol abuse and withdrawalDrug and alcohol abuse and withdrawalChronic depression (unipolar, bipolar)Chronic depression (unipolar, bipolar)Panic disorderPanic disorderAnorexia nervosaAnorexia nervosa
Metabolic abnormalitiesMetabolic abnormalitiesHypothalamic amenorrheaHypothalamic amenorrheaElevated cortisol-binding globulin (estrogen therapy, pregnancy, Elevated cortisol-binding globulin (estrogen therapy, pregnancy,
hyperthyroidism)hyperthyroidism)Glucocorticoid resistanceGlucocorticoid resistanceComplicated diabetes mellitusComplicated diabetes mellitus

PITFALLS IN THE INTERPRETATION OF THE 1-MG PITFALLS IN THE INTERPRETATION OF THE 1-MG OVERNIGHT DEXAMETHASONE SUPPRESSION TESTOVERNIGHT DEXAMETHASONE SUPPRESSION TEST
False-positive tests (I.e., lack of suppression)False-positive tests (I.e., lack of suppression)– Non-Cushing hypercortisolemiaNon-Cushing hypercortisolemia– ObesityObesity– StressStress– AlcoholismAlcoholism– Psychiatric illness (anorexia nervosa, depression, mania)Psychiatric illness (anorexia nervosa, depression, mania)– Elevated cortisol binding globulin (estrogen, pregnancy, hyperthyroidism)Elevated cortisol binding globulin (estrogen, pregnancy, hyperthyroidism)– Glucocorticoid resistanceGlucocorticoid resistance
Test-related artifactsTest-related artifacts– Laboratory error, assay interferenceLaboratory error, assay interference– insufficient dexamethasone delivery into the circulationinsufficient dexamethasone delivery into the circulation– NoncomplianceNoncompliance– Decreased absorptionDecreased absorption– Increased metabolism (drugs)Increased metabolism (drugs)
False-negative testsFalse-negative tests– chronic renal failure (creatinine clearance < 15 mL/min)chronic renal failure (creatinine clearance < 15 mL/min)– Hypometabolism of dexamethasone (e.g., liver failure)Hypometabolism of dexamethasone (e.g., liver failure)

Problems in Diagnosis of Cushing’s SyndromeProblems in Diagnosis of Cushing’s Syndrome
Similarities in biochemical features of Cushing’s syndrome:Similarities in biochemical features of Cushing’s syndrome:
1.1. Elevation of urine free cortisolElevation of urine free cortisol
2.2. Disruption of the normal diurnal pattern of cortisol secretionDisruption of the normal diurnal pattern of cortisol secretion
3.3. Lack of suppression of cortisol after overnight 1 mg Lack of suppression of cortisol after overnight 1 mg dexamethasone suppression testdexamethasone suppression test
pseudo-Cushing’s syndromespseudo-Cushing’s syndromes

Problems in Diagnosis of Cushing’s SyndromeProblems in Diagnosis of Cushing’s Syndrome
Distinguishing Tools:Distinguishing Tools:1.1. History & physical examinationHistory & physical examination2.2. Repeating screening testsRepeating screening tests3.3. Dexamethasone suppression test followed by CRH Dexamethasone suppression test followed by CRH
stimulation & measurement of plasma cortisol.stimulation & measurement of plasma cortisol.
pseudo-Cushing’s syndromespseudo-Cushing’s syndromes

Treatment of Cushing’s SyndromeTreatment of Cushing’s Syndrome
1.1. Pituitary microsurgeryPituitary microsurgery– Transphenoidal hypophysectomyTransphenoidal hypophysectomy
– Transfrontal hypophysectomy Transfrontal hypophysectomy
2.2. RadiotherapyRadiotherapy– Conventional irradiation (not recommended)Conventional irradiation (not recommended)
– Heavy particles irradiationHeavy particles irradiation
– Gamma-knife radiosurgeryGamma-knife radiosurgery
– Implantation of radioactive seeds (gold & ytrium)Implantation of radioactive seeds (gold & ytrium)
3.3. Medical TherapyMedical Therapy– KetoconanzoleKetoconanzole
– AminoglutethimideAminoglutethimide
– Mitotane (adrenolytic drug)Mitotane (adrenolytic drug)
Cushing’s syndromesCushing’s syndromes

Treatment of Cushing’s SyndromeTreatment of Cushing’s Syndrome
1.1. Ectopic ACTH syndromesEctopic ACTH syndromes
2.2. Adrenal AdenomasAdrenal Adenomas
3.3. Adrenal CarcinomasAdrenal Carcinomas
4.4. Nodular Adrenal HyperplasiaNodular Adrenal Hyperplasia
Other types of Cushing’s syndromesOther types of Cushing’s syndromes

Prognosis of Cushing’s SyndromePrognosis of Cushing’s Syndrome
1.1. Cushing’s DiseaseCushing’s Disease2.2. Ectopic ACTH syndromesEctopic ACTH syndromes3.3. Adrenal AdenomasAdrenal Adenomas4.4. Adrenal CarcinomasAdrenal Carcinomas5.5. Nodular Adrenal HyperplasiaNodular Adrenal Hyperplasia

Other Adrenal DisordersOther Adrenal Disorders
Not covered in this lecture and need Not covered in this lecture and need to be studied: to be studied: Pheochromocytoma Pheochromocytoma HyperaldoteronismHyperaldoteronism Syndomes of congenital adrenal Syndomes of congenital adrenal
hyperplasia (CAH).hyperplasia (CAH). HirsutismHirsutism VirilizationVirilization