Embed Size (px)
Citation preview
Endocrine Disorders
Learning ObjectivesPituitary Adenoma
Acromegaly/gigantism
Cushing’s disease
Discuss epidemiology, causes, clinical manifestations, lab results, complications, treatment, and lifestyle modifications for both disease states
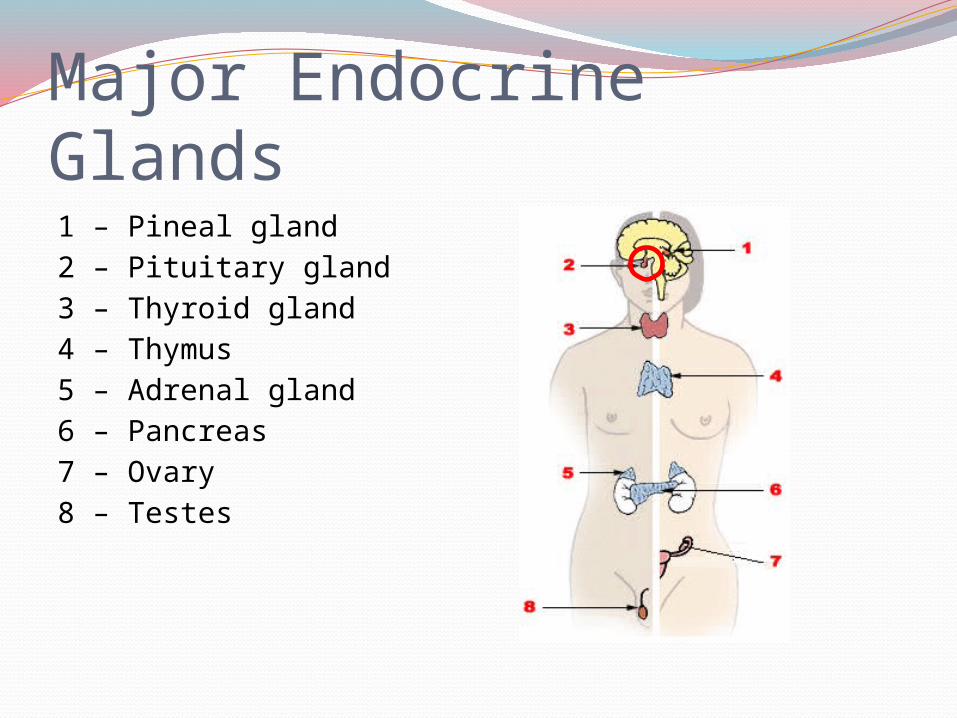
Major Endocrine Glands1 – Pineal gland2 – Pituitary gland3 – Thyroid gland4 – Thymus5 – Adrenal gland6 – Pancreas7 – Ovary 8 – Testes
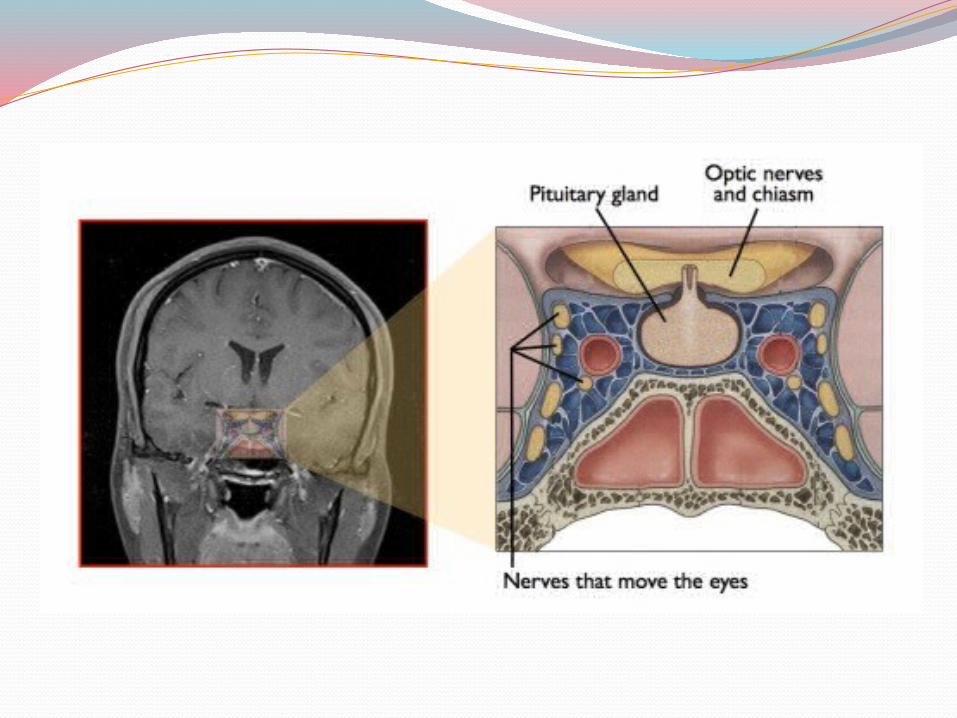
Pituitary adenomaA pituitary adenoma is an abnormal growth in
the pituitary gland. Problems occur when:
Overproduction of a certain hormone – Acromegaly and Cushing’s disease
Other pituitary cells growing larger and pressing on cells causing pituitary cells to not make as much hormone.
They can press on nearby structures in the brain such as the optic nerve
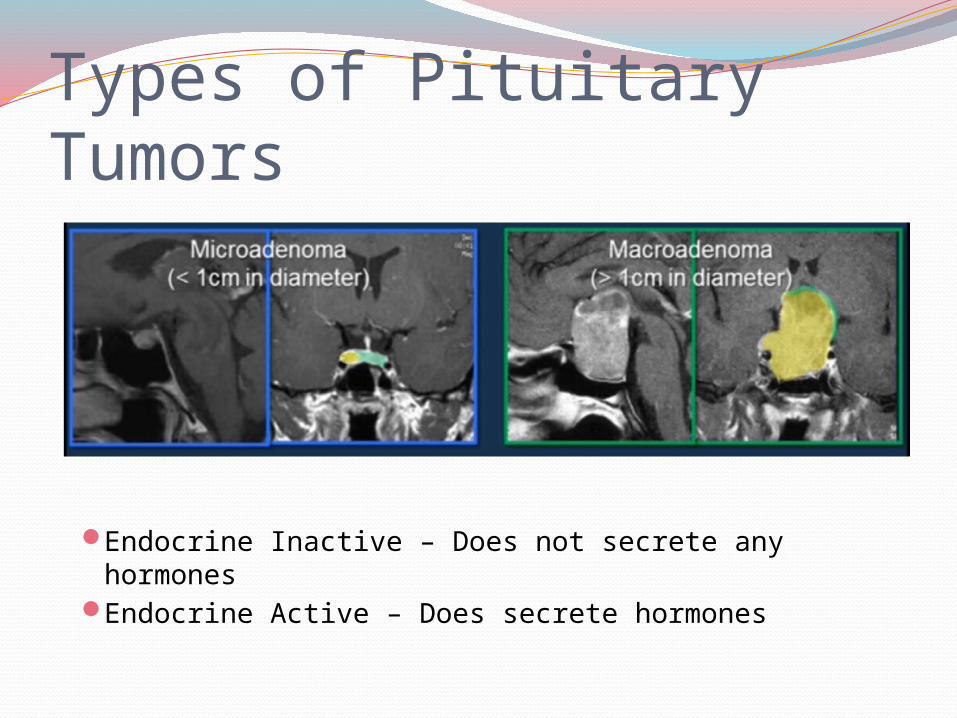
Types of Pituitary Tumors
Endocrine Inactive – Does not secrete any hormonesEndocrine Active – Does secrete hormones
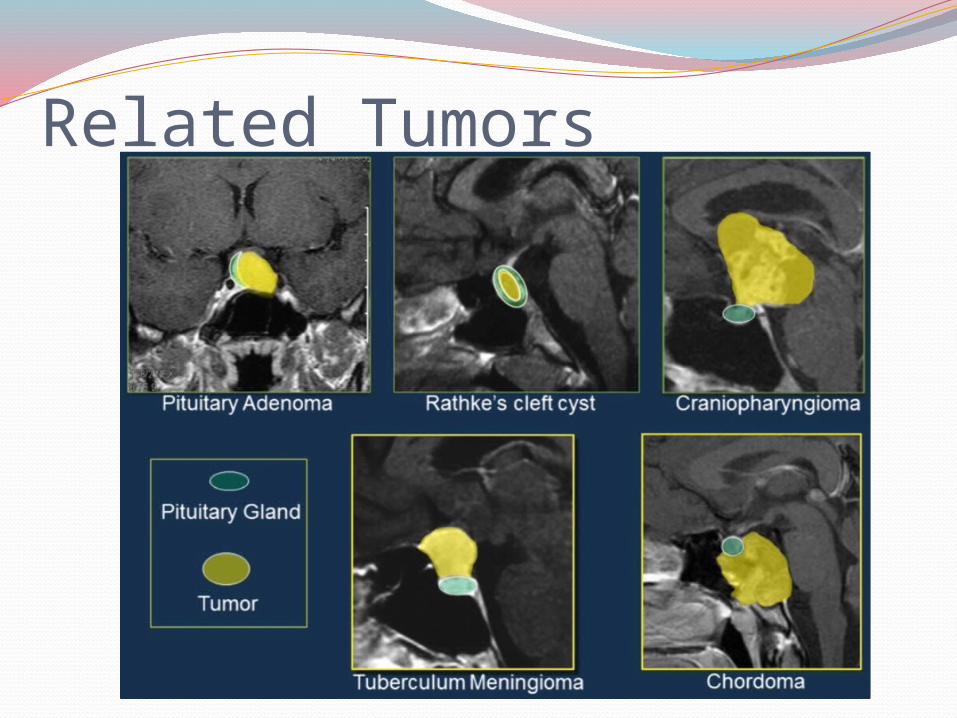
Related Tumors
Pituitary adenomaMass Effects:
Onset may be gradual due to tumor growth or sudden due to tumor bleeding (apoplexy)
Loss of peripheral vision, blurry visionFronto-orbital headacheHypopituitarism (pituitary gland failure)
Fatigue, weight gain, depression, decreased libido, impotence, infertility, loss of menses
Endonasal Pituitary Adenoma Removalhttp://
www.youtube.com/watch?v=fY7p1bhg1P0&list=PLwWS6c78u0byN9EdQEIX772eV9ApAEigl&feature=player_detailpage#t=336
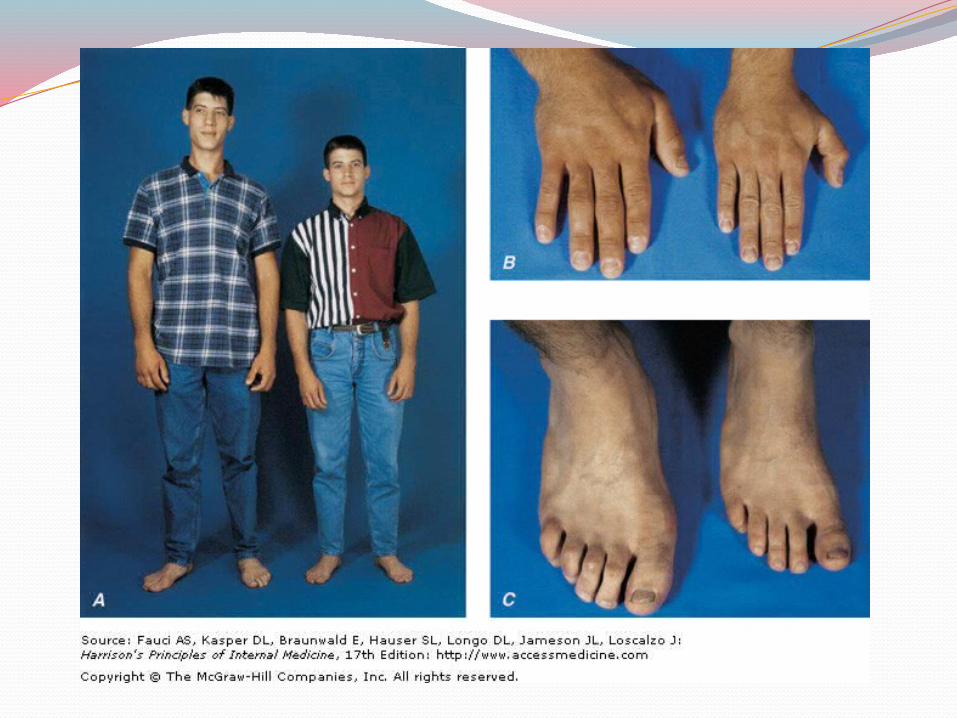
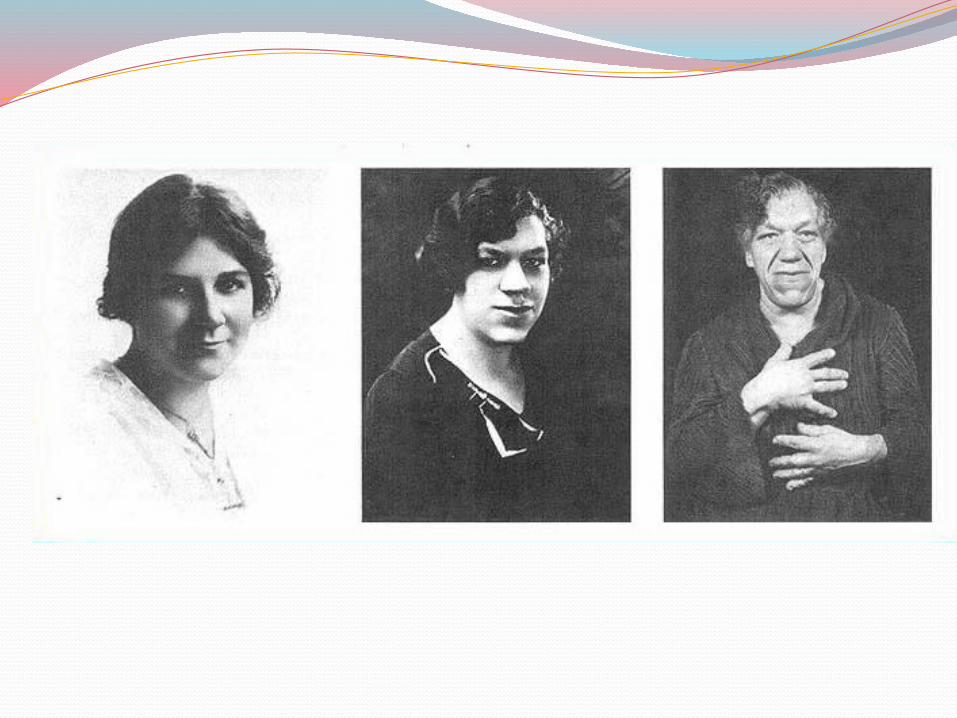
Acromegaly/gigantismOverview:
Caused by excessive and extended growth hormone secretion → ↑ IGF → causes growth changes
Due to a benign tumor in the anterior pituitary Timing is important!
Gigantism before fusion of epiphyseal plates Acromegaly after fusion
“It’s not my fault being the biggest and the strongest. I don’t even exercise” – Fezzik, The Princess Bride
Acromegaly/GigantismCauses:
Proliferation of somatotroph cells in anterior pituitary Benign tumor
Increased GH stimulates increased IGF-1 in liver
IGF-1 causes growth of tissues and metabolic abnormalities
Acromegaly/GigantismEpidemiology:
Prevalence – 70/1,000,000Incidence – 3-4/1,000,000 per yearNeither disorder has strong genetic ties,
although some genetic diseases can predispose to gigantism Carney Complex, Multiple Endocrine Neoplasia
Acromegaly/GigantismClinical Manifestations:
Opthalmological Vision blurring
Pulmonary Sleep Apnea, Orthopnea
Dermatological Thickening of skin and hair Hyperhydrosis (sweating)
Muskuloskeletal Skeletal growth and thickening, especially hand and foot Widening of jaw and overbite Joint pain Abnormally heavy brow and prominent forehead Husky voice due to larynx thickening
Acromegaly/GigantismDiagnostic Testing:
IGF-1 levelsGrowth Hormone levels
Pulsatile secretion – one high value is not indicative Glucose tolerance test (glucose should suppress
GH)Brain MRI to visualize adenoma
Other Testing:Pituitary hormone levels to assess tumor effect
TSH, FSH, LH, ACTH, Prolactin
Acromegaly/GigantismComplications:
Cardiovascular Cardiomyopathy, CHF Valve dysfunction Arrhythmia Hypertension Atherosclerosis
Pulmonary Sleep apnea
Metabolic Impaired glucose tolerance Impaired lipid metabolism
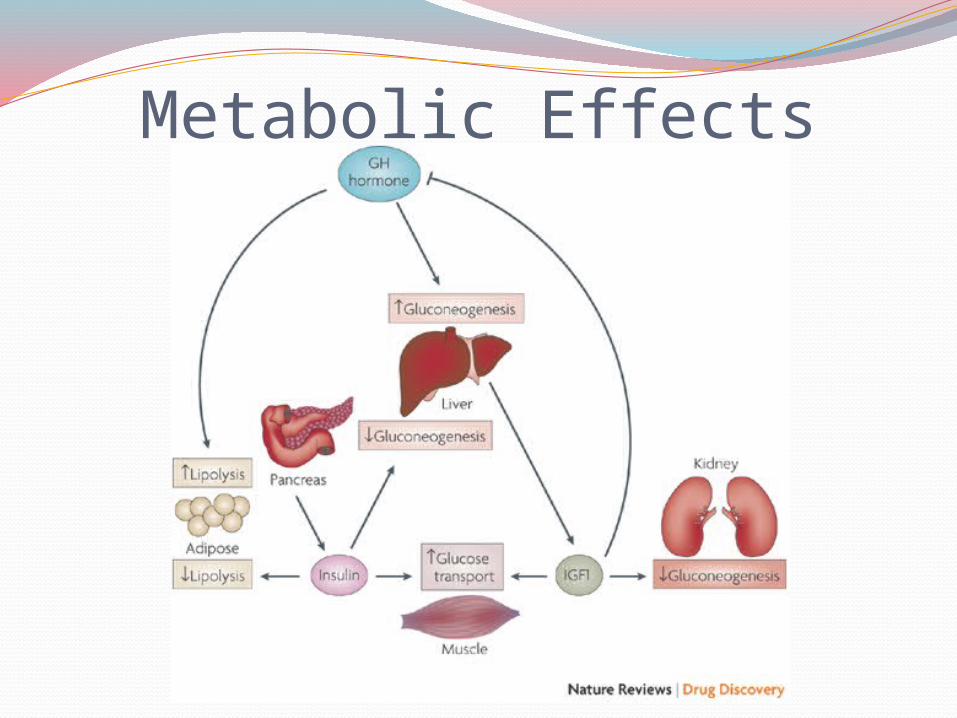
Metabolic Effects
Acromegaly/GigantismTreatment: Goal is to lower levels of IGF-1,
increase life expectancyPhysical TherapySurgery
Remove tumorMedication
Somatostatin analogues GH receptor antagonists Dopamine agonists
Radiation Therapy Gamma knife
Cushing’s DiseaseOverview
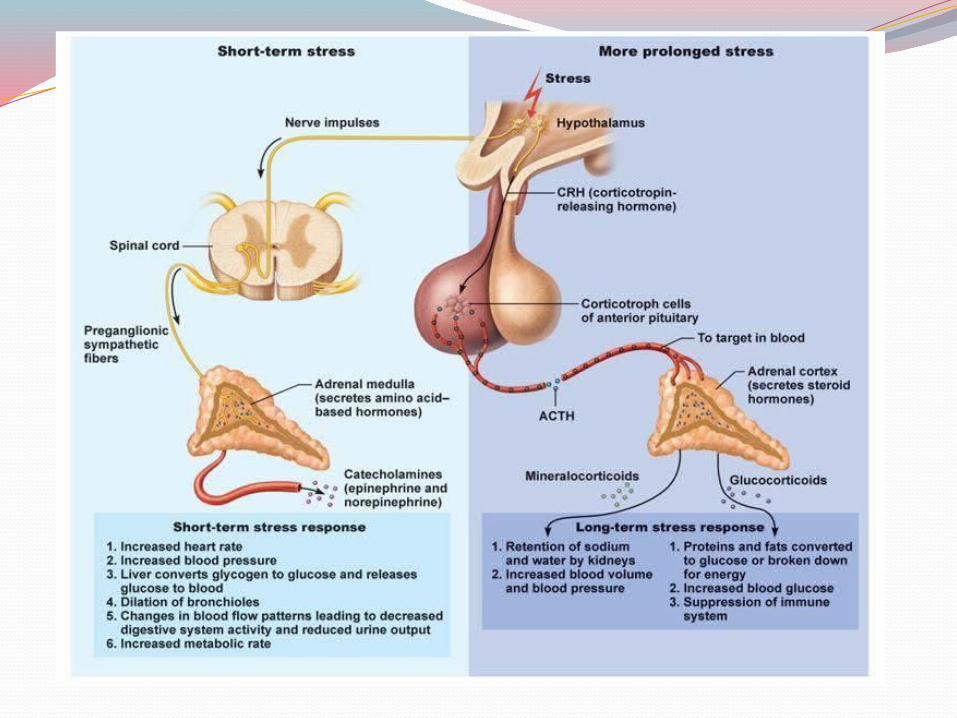
Caused by an extended increase in levels of ACTH, stimulating the adrenal glands to produce too much cortisol (a glucocorticoid)
Caused by a benign pituitary tumor“Stress hormone” – Affects many organ
systems, leading to metabolic, cardiovascular, and immune dysfunction
Cushing’s DiseaseCauses:
All symptoms caused by prolonged exposure to high levels of cortisol
Cushing’s Syndrome includes many causes most commonly iatrogenic ACTH-independent
Cushing’s Disease is caused by pituitary adenoma ACTH-dependent
Cushing’s DiseaseEpidemiology:
Prevalence – 13/1,000,000Incidence – 2/1,000,000 per year8x more common in women than menMost common in ages 20-40 years

Cushing’s DiseaseClinical Manifestation
Cushing’s DiseaseDiagnostic Testing:
Urinary Free Cortisol Not specific unless 3x normal values
Dexamethasone suppression test Negative feedback test – should be negative in
pituitary adenomaACTH levels
Determine if adrenal or pituitary problemOvernight Cortisol levels
Cortisol levels should fall throughout the day, lowest overnight
MRI to visualize tumor
Cushing’s DiseaseComplications:
Demineralization of bones causing osteoporosis May progress to bone pain and even osteonecrosis
Generalized and sometimes extensive muscle weakness Often unable to rise from chair unassisted
Cardiac hypertrophy, hypertension May lead to CHF if untreated
Renal insufficiency Renal stones due to excretion of calcium
Cushing’s DiseaseTreatment: goal is to restore hormone balance
and reverse Cushing’s SyndromeSurgery
Removal of pituitary adenoma Removal of adrenal glands in refractory disease
Medication Cortisol synthesis inhibitors (Ketoconazole) Glucocorticoid type II receptor antagonist (Mifepristone)
Radiation Gamma knife
Lifestyle modification High protein diet for those with muscle wasting Regular exercise Clean and inspect all wounds

Any Questions?