Upload
sahala09
View
213
Download
0
Embed Size (px)
Citation preview
8/11/2019 Diabetic Retinopathy.doc
1/23
Chapter 30
Diabetic RetinopathyBrett J. RosenblattWilliam E. Benson
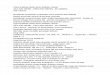
CLINICAL FINDIN!Diabetic retinopathy is "s"ally #i$i#e# into nonproli%erati$e #iabetic retinopathy &N'DR( an#proli%erati$e #iabetic retinopathy &'DR(.
EARL) N*N'R*LIFERA+I,E DIABE+IC RE+IN*'A+-)Altho"h microane"rysms are the %irst ophthalmoscopically #etectable chane in #iabeticretinopathy/ the earliest abnormalities seen histopatholoically are thicenin o% the capillarybasement membrane1/2an# pericyte #ropo"t.3/'ericytes are mesothelial cells that s"rro"n# an#s"pport the retinal capillary en#othelial cells. Normally there is one pericyte per en#othelial cell.In people 4ith #iabetes/ ho4e$er/ the pericytes #ie o%% an# are #ecrease# in n"mber &Fi. 1(.
+heir absence 4eaens the capillaries an# permits thin54alle# #ilatations/ calle#microane"rysms/ to #e$elop. Later/ en#othelial cells proli%erate an# lay #o4n layers o% basementmembrane material. Fibrin may acc"m"late 4ithin the microane"rysm alon 4ith erythrocytes/an# the l"men o% the microane"rysm may become occl"#e# &Fi. 2(. Initially/ mostmicroane"rysms are on the $eno"s si#e o% the capillaries/ b"t later they are seen on the arterialsi#e as 4ell. Clinically/ they appear as small re# #ots & Fi. 3(. Despite the m"ltiple layers o%basement membrane/ microane"rysms are permeable to 4ater an# lare molec"les/ allo4in thetrans"#ation o% %l"i# an# lipi# into the retina.
,ie4 Fi"re
Fi. 1 A. +rypsin #iest preparation o% early bacro"n#retinopathy. Normal retinal capillaries/ 4ith one pericyte &close#arro4s( per en#othelial cell &open arro4s(. B. Retinal capillary o%
a patient 4ith #iabetes 4ith necrotic pericytes &arro4s(. &Co"rtesyo% Dr. 6yron )ano%%(
,ie4 Fi"re
Fi. 2 +rypsin #iest preparation o% early bacro"n# retinopathy.Early microane"rysm &close# arro4(/ ane"rysm 4ith en#othelialproli%eration &open arro4(/ an# ane"rysm occl"#e# 4ith %ibrin&c"r$e# arro4(. &Co"rtesy o% Dr. 6yron )ano%%(
Fi. 3 A. Diabetic retinopathy 4ith m"ltiplemicroane"rysms/ #ot hemorrhaes/ an# earlyneo$asc"lari7ation o% the optic #isc &N,D(. Asmall blot hemorrhae is seen in%eriorly. B.Contin"e#. 6i#phase o% the %l"oresceinanioram. 'atent microane"rysms are seen ashyper%l"orescent #ots. Note that mostmicroane"rysms cannot be seenophthalmoscopically. +here is some enlaremento% the %o$eal a$asc"lar 7one beca"se o% some
http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F2-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F1-V3-308/11/2019 Diabetic Retinopathy.doc
2/23
,ie4 Fi"re occl"#e# capillaries. +emporally there is a larer7one o% capillary nonper%"sion. +he N,D isbeinnin to lea. C. Late phase o% the%l"orescein anioram sho4in #i%%"se leaae o%%l"orescein into the mac"la.
It is o%ten #i%%ic"lt to #istin"ish a small #ot hemorrhae %rom a microane"rysm byophthalmoscopy alone. *n %l"orescein anioraphy patent microane"rysms 4ill %ill 4ith #ye8"icly an# then lea/9"nlie a small #ot hemorrhae that 4ill bloc %l"orescence &see Fi. 3(.-o4e$er/ anioraphy cannot #istin"ish a hemorrhae %rom a microane"rysm %ille# 4ithclotte# bloo#. Beca"se %l"orescein passes easily tho"h them/ 4e "s"ally see many moremicroane"rysms on %l"orescein anioraphy than are apparent on e:amination.;
When the 4all o% a capillary or microane"rysm is thin/ it may r"pt"re/ i$in rise to anintraretinal hemorrhae. I% the hemorrhae is #eep &i.e./ in the inner n"clear layer or o"terple:i%orm layer(/ it "s"ally has a ro"n# or o$al shape &
8/11/2019 Diabetic Retinopathy.doc
3/23
,ie4 Fi"re
Fi. 9 A. Circinate retinopathy in%erotemporal to the centero% the mac"la. B. +he mi#phase o% the %l"orescein anioramsho4s a cl"ster o% microane"rysms in the center o% thecircinate rin. C. +he late phase o% the anioram sho4sleaae o% %l"orescein. D. *ptical coherence tomoram
centere# on the %o$ea o% an eye 4ith #iabetic mac"lar e#ema.+he area o% mare# retina thicenin contains n"mero"shypore%lecti$e cystoi# spaces &%ine arro4(. +he o"ter retinais limite# by the hyperre%lecti$e piment epithelial ban#&thic arro4(.
,ie4 Fi"re
Fi. ; A. Bacro"n# #iabetic retinopathy. B. +he mi#phaseo% the %l"orescein anioram sho4s m"ltiplemicroane"rysms. C. Late phase o% the anioram sho4scystoi# mac"lar e#ema.
I% the leaae o% %l"i# is se$ere eno"h/ lipi# may acc"m"late in the retina &see Fis. an# 9(.Aain/ the o"ter ple:i%orm layer is %irst to be a%%ecte#. In some cases/ lipi# is scattere# thro"hthe mac"la/ in others/ it acc"m"lates in a rin aro"n# a ro"p o% leain microane"rysms/ oraro"n# areas o% capillary nonper%"sion &see Fis. an# 9(. +his pattern is calle# circinateretinopathy.In a##ition to the retinal $asc"lar abnormalities/ the choriocapillaris may be in$ol$e# in N'DR.
Initially there is a thicenin o% the basement membrane.
?
Later/ a perio#ic aci#5!chi%% &'A!(positi$e material acc"m"lates/ 4hich impines on an# may occl"#e the l"men o% the choroi#alcapillaries in the posterior pole.
AD,ANCED N*N'R*LIFERA+I,E DIABE+IC RE+IN*'A+-)In a#$ance# N'DR/ sins o% increasin retinal hypo:ia appear/ incl"#in m"ltiple retinalhemorrhaes/ cotton54ool spots &Fi. (/ $eno"s bea#in an# loops &Fis. an# ?(/ intraretinalmicro$asc"lar abnormalities &IR6A( &see Fis. an# ?(/ an# lare areas o% capillarynonper%"sion.
,ie4 Fi"re
Fi. A. !e$erenonproli%erati$e retinopathy4ith $eno"s #ilatation an#
bea#in/ so%t e:"#ates/ an#intraretinal micro$asc"larabnormalities B. +he mi#phaseo% the anioram sho4s theintraretinal micro$asc"larabnormalities &IR6A( an#se$ere capillary nonper%"sion.
http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F7-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F6-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F5-V3-308/11/2019 Diabetic Retinopathy.doc
4/23
,ie4 Fi"re
Fi. ? ,eno"s loop &larearro4( an# intraretinalmicro$asc"lar abnormalities&IR6A small arro4(.
Cotton54ool spots/ also re%erre# to as so%t e:"#ates/ are act"ally ner$e %iber layer in%arctions.+hey are 4hite/ %l"%%y5appearin lesions in the ner$e %iber layer that res"lt %rom occl"sion o%precapillary arterioles. Fl"orescein anioraphy con%irms the lac o% capillary per%"sion.6icroane"rysms %re8"ently s"rro"n# ol#er cotton54ool spots as 4ell as larer areas o% capillarynonper%"sion.,eno"s bea#in &see Fi. ( an# $eno"s loops &see Fi. ?( in#icates sl"ish retinal circ"lationan# are nearly al4ays a#acent to e:tensi$e areas o% capillary nonper%"sion. Focal $itreo"straction is tho"ht to contrib"te to their %ormation.Capillaries ne:t to areas o% nonper%"sion that#ilate an# %"nction as collaterals are re%erre# to as IR6A. +hey are %re8"ently #i%%ic"lt to#i%%erentiate %rom s"r%ace retinal neo$asc"lari7ation. Fl"orescein/ ho4e$er/ #oes not lea %rom
IR6A b"t leas pro%"sely %rom neo$asc"lari7ation &seeFi. (.+he Early +reatment Diabetic Retinopathy !t"#y &E+DR!(10%o"n# that IR6A/ m"ltiple retinalhemorrhaes/ $eno"s bea#in an# loops/ 4i#esprea# capillary nonper%"sion/ an# 4i#esprea#leaae on %l"orescein anioraphy are all sini%icant ris %actors %or the #e$elopment o%proli%erati$e retinopathy. Interestinly/ cotton54ool spots/ in the absence o% the other %in#ins/are not. Appro:imately 90 o% patients 4ith se$ere N'DR proress to proli%erati$e retinopathy4ith hih5ris characteristics isc"sse# later( 4ithin 1 year.11
'R*LIFERA+I,E DIABE+IC RE+IN*'A+-)'roli%erati$e $essels "s"ally arise %rom $eins an# o%ten bein as a collection o% %ine $essels.When they arise on or 4ithin 1 #isc #iameter o% the optic #isc they are re%erre# to asneo$asc"lari7ation o% the #isc &N,D( &Fi. (. When they arise %"rther than 1 #isc #iametera4ay/ they are calle# neo$asc"lari7ation else4here &N,E( &Fi. 10(. N,E nearly al4ays ro4sto4ar# an# into 7ones o% retinal capillary nonper%"sion/ b"t capillary nonper%"sion is nearlyal4ays more 4i#esprea# in eyes 4ith N,D than it is in N,E. 12 Interestinly/ it is seen moreo%ten in patients yo"ner than 0 compare# to ol#er patients 4ith #iabetes. 13
,ie4 Fi"re
Fi. A#$ance# neo$asc"lari7ation o% the #isc.
,ie4 Fi"re
Fi. 10 Neo$asc"lari7ation else4here &N,E(.
*nce the stim"l"s %or ro4th o% ne4 $essels is present the $essels ro4 alon the path o% leastresistance. +he absence o% the internal limitin membrane o$er the optic #isc co"l# e:plain theprocli$ity o% ne4 $essel ro4th at that location. Neo$asc"lari7ation ro4s rea#ily alonconnecti$e tiss"e sca%%ol#in s"ch as the posterior hyaloi#al %ace &Fi. 11(.
http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F10-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F9-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F8-V3-308/11/2019 Diabetic Retinopathy.doc
5/23
,ie4 Fi"re
Fi. 11 A"topsy eye. Neo$asc"lar stal a#herent to an# ro4in on the posteriorcortical $itreo"s 4hich has partially #etache#. &Co"rtesy o% Dr. 6yron )ano%%(
+he ne4 $essels/ initially nae#/ "s"ally proress thro"h a stae o% %"rther proli%eration 4ith
associate# connecti$e tiss"e %ormation. As 'DR proresses/ the %ibro"s component becomesmore prominent. Fibrotic tiss"e can be $asc"lar or a$asc"lar. +he %ibro$asc"lar $ariety is "s"ally%o"n# in association 4ith $essels e:ten#in into the $itreo"s ca$ity or 4ith abnormal ne4 $esselson the s"r%ace o% the retina or #isc. +he a$asc"lar $ariety "s"ally res"lts %rom orani7ation orthicenin o% the posterior hyaloi# %ace.'osterior $itreo"s #etachment in #iabetics is characteri7e# by a slo4/ o$erall shrinae o% theentire %orme# $itreo"s rather than by the %ormation o% ca$ities ca"se# by $itreo"s #estr"ction. 1
Da$is19has stresse# the role o% the contractin $itreo"s in the pro#"ction o% $itreo"s hemorrhae/retinal breas/ an# retinal #etachment. Neo$asc"lar $essels #o not
8/11/2019 Diabetic Retinopathy.doc
6/23
hemorrhaes are probably 8"ite rare. +iht s"binternal limitin membrane hemorrhaes are#anero"s bea"se they may proress to traction retinal #etachment.1?/1
,ie4 Fi"re
Fi. 12 !"binternal limitin membranehemorrhaes.
+4o types o% #iabetic retinal #etachments occ"r/ those that are ca"se# by traction alone&nonrhematoeno"s( &Fi. 1(/ an# those ca"se# by retinal brea %ormation &rhematoeno"s(&Fis. 19an# 1;(. Characteristics o% nonrhematoeno"s &traction( #etachment in 'DR incl"#ethe %ollo4inG &1( the #etache# retina is "s"ally con%ine# to the posterior %"n#"s an# in%re8"ently
e:ten#s more than t4o5thir#s o% the #istanc# to the e8"ator/ &2( it has a ta"t an# shiny s"r%ace/ &3(it is conca$e to4ar# the p"pil/ an# &( there is no shi%tin o% s"bretinal %l"i#.
,ie4 Fi"re
Fi. 1 +raction retinal #etachment. +he #etache# retina has a smoothnoncorr"ate# appearance an# is con$e: to4ar# the p"pil.
,ie4 Fi"re
Fi. 19 Combine# tractionHrhematoeno"s retinal #etachment. +he #etache#retina has a corr"ate# appearance an# is conca$e to4ar# the p"pil.
,ie4 Fi"re
Fi. 1; Ro"n# hole near %ibro"s proli%eration.
,itreo"s traction may also ca"se %ocal areas o% retinoschisis that may be #i%%ic"lt to #istin"ish%rom %"ll5thicness traction retinal #etachment. In retinoschisis the ele$ate# layer is thinner an#more transl"cent &Fi. 1(.
,ie4 Fi"re
Fi. 1 +raction retinoschisis nasal to the #isc &!tereo(. +here is a small inner
4all hole alon the $essel that lea$es the #isc at the 2 o>cloc position.
In combine# tractionHrhematoeno"s #etachment/ the bor#ers o% the ele$ate# retina "s"allye:ten# to the ora serrata the retinal s"r%ace is #"ll an# rayish an# "n#"lates beca"se o% retinalmobility ca"se# by shi%tin s"bretinal %l"i#. +he ca"sati$e retinal breas are "s"ally %o"n# in theposterior pole near areas o% %ibro$asc"lar proli%eration. +hey are o$al in shape an# appear to be
http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F17-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F16-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F15-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F14-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F12-V3-308/11/2019 Diabetic Retinopathy.doc
7/23
partly the res"lt o% tanential traction %rom the proli%erati$e tiss"e as 4ell as $itreo"s traction.Determinin the location o% retinal holes may be complicate# by many %actors/ partic"larly poor#ilation o% the p"pil/ lens opacity/ increase# $itreo"s t"rbi#ity/ $itreo"s hemorrhae/ intraretinalhemorrhae/ an# obsc"ration o% the breas by o$erlyin proli%erati$e tiss"e. *%ten they are onlylocate# #"rin $itrectomy s"rery.
RI! FAC+*R! *F DIABE+IC RE+IN*'A+-)D@RA+I*N *F DIABE+E!+he best pre#ictor o% #iabetic retinopathy is the #"ration o% the #isease. 21/22/23/2/29/2;/2/2?'atients4ho ha$e ha# type 1 or ins"lin5#epen#ent #iabetes mellit"s &IDD6( %or 9 years or less rarelysho4 any e$i#ence o% #iabetic retinopathy.2/2-o4e$er/ 2 o% those 4ho ha$e ha# #iabetes %or9 to 10 years an# 1 to 0 o% those 4ho ha$e ha# #iabetes %or loner than 10 years ha$e#iabetic retinopathy.30A%ter 20 to 30 years/ the inci#ence rises to 9 an# appro:imately one5thir# to one5hal% o% these patients ha$e 'DR.2
Determinin the role o% #"ratioo o% #iabetes as a pre#ictor o% retinopathy in type 2 or nonins"lin#epen#ent #iabetes mellit"s &NIDD6( is more #i%%ic"lt beca"se o% the "ncertainty o% the onset in
many patients. In some/ the #ianosis o% #iabetes is ma#e only a%ter retinopathy is #isco$ere#.With these limitations/ the best st"#ies are %rom Wisconsin an# Israel. )ano an# co54orers 30
%o"n# that the pre$alence o% nonproli%erati$e retinopathy 11 to 13 years a%ter the onset o% type 2#iabetes 4as 23. A%ter 1; or more years/ it 4as ;0. Ele$en or more years a%ter the onset/ 3o% the patients ha# proli%erati$e retinopathy. lein %o"n# that 10 years a%ter the #ianosis o% type2 #iabetes/ ; o% patients ha# retinopathy an# 10 ha# 'DR. +he ris 4as lo4est in patients4ho #i# not re8"ire ins"lin.31
AE *F +-E 'A+IEN+Altho"h the #"ration o% #iabetes is the most important #eterminant o% retinopathy/ the years thata patient has #iabetes be%ore the onset o% p"berty #o not co"nt aainst him or her. In other 4or#s/the ris o% retinopathy is ro"hly the same in t4o 29 year5ol# patients/ one o% 4hom #e$elope#type 1 at the ae o% ; an# the other o% 4hom #e$elope# it at ae 12 or 13.21/29/2?
!)!+E6IC FAC+*R!Control o% Bloo# l"cose+he #eca#es5ol# contro$ersy rear#in 4hether or not intensi$e metabolic control pre$ents the#e$elopment or proression o% retinopathy 4as %inally lai# to rest by the Diabetes Control an#Complications +rial &DCC+( 31/32 an# the @nite# in#om 'rospecti$e Diabetes !t"#y&@'D!(.33 In the DCC+/ patients 4ho closely monitore# their bloo# l"cose an# 4ho 4eretreate# 4ith ins"lin at least three times per #ay by inection or by ins"lin p"mp 4ere compare# topatients treate# 4ith con$entional therapy. +he intensi$e5treatment ro"p ha# a ; re#"ction inthe rate o% #e$elopment o% any retinopathy an# an ?0 re#"ction in proression o% establishe#retinopathy. *phthalmoloists m"st be a4are that a%ter instit"tion o% strict control/ there is o%tenan initial 4orsenin o% preproli%erati$e retinopathy.3;/3/3?Fort"nately/ a%ter 2 years o% control/ thestrict5control ro"ps ha# the same or less retinopathy than ro"ps treate# con$entionally.3 +he@'D! 4as a ran#omi7e#/ controlle# clinical trial in$ol$in ne4ly #ianose# type 2 #iabetics.'atients 4ere ran#omly assine# to intensi$e lycemic control 4ith s"l%onyl"rea aents orins"lin or to con$entional control 4ith #iet. A%ter 12 years o% %ollo45"p/ proression o% #iabeticretinopathy in the intensi$e5control ro"p 4as re#"ce# by 21.3
8/11/2019 Diabetic Retinopathy.doc
8/23
+he bene%its o% rioro"s control o% bloo# l"cose #o not e:ten# to all eyes 4ith a#$ance#retinopathy. E$en patients 4ho are ma#e normolycemic by pancreatic transplantation contin"eto sho4 proression.0
Renal Disease6ost patients 4ith renal #isease/ as e$i#ence# by protein"ria/ ele$ate# bloo# "rea nitroen
&B@N(/ an# ele$ate# bloo# creatinine/ also ha$e retinopathy.2?/1/2/3
E$en patients 4ithmicroalb"min"ria are at hih ris o% ha$in retinopathy./9/;//?*n the other han#/ only 39 o%patients 4ith symptomatic retinopathy ha$e protein"ria/ ele$ate# B@N or ele$ate# creatinine.
!ystemic -ypertension+he literat"re in#icates that ele$ate# systolic bloo# press"re is a mo#erate ris %actor %or #iabeticretinopathy.2?/2/3/90*ther st"#ies ha$e %o"n#/ ho4e$er/ that 4hen patients 4ith nephropathy aree:cl"#e#/ bloo# press"re is not a stron ris %actor.91/92/93
+he -ypertension in Diabetes !t"#y &-D!(/ part o% the @'D!/ e$al"ate# the e%%ect bloo#press"re control on the proression o% #iabetic retinopathy. 'atients 4ho 4ere ept "n#er strictcontrol o% bloo# press"re & 190H?9 mm -( ha# a 3 ris re#"ction in micro$asc"lar chanescompare# to the con$entional bloo# press"re control ro"p & 1?0H109(.9For e$ery 105mm -
re#"ction in systolic bloo# press"re there 4as an associate# 13 re#"ction o% micro$asc"lar en#points. Lisinopril/ an aniotensin5con$ertin en7yme inhibitor/ has been sho4n in another st"#yto #ecrease by 90 the proression o% N'DR in normotensi$e type 1 #iabetics s"estin abene%it %or some antihypertensi$es in#epen#ent o% there bloo# press"re lo4erin e%%ect.99
'renancyWomen 4ith #iabetes 4ho bein a prenancy 4ith no retinopathy ha$e a 10 to 2; ris o%#e$elopin some N'DR.9;/9/9?+hose 4ho ha$e N'DR at the onset o% prenancy an# those 4hoha$e lo4 hemolobin or systemic hypertension ten# to sho4 accelerate# proression/ 4ithincrease# hemorrhaes/ cotton54ool spots an# mac"lar e#ema.9?/9/;0Fort"nately/ there is "s"allysome reression o% N'DR a%ter #eli$ery.;1/;2/;3
Women 4ho bein prenancy 4ith N'DR ha$e a 22 to 0 inci#ence o% proression to'DR.9?/;1/;+hose 4ith "ntreate# 'DR at the onset %re8"ently #o poorly "nless they are treate#4ith aressi$e panretinal photocoa"lation &'R'(/;9/;;b"t those 4ith pre$io"sly treate# 'DR"s"ally #o 4ell.+here is no #o"bt that 4omen 4ho maintain oo# metabolic control #"rin prenancy ha$e%e4er spontaneo"s abortions an# %e4er chil#ren 4ith birth #e%ects. ; +here%ore/ obstetriciansstri$e %or strict control. -o4e$er/ 4omen 4ho bein prenancy 4ith poorly controlle# #iabetes4ho are s"##enly bro"ht "n#er strict control %re8"ently ha$e se$ere #eterioration o% theirretinopathy an# #o not al4ays reco$er a%ter #eli$ery.9;/9/;2/;?It is probably best to ra#"ally brinthe bloo# l"cose "n#er control.RaceRetinopathy is more liely to be present in blacs than in 4hites.;6oreo$er/ blacs ha$e ahiher rate o% se$ere mac"lar e#ema an# o% blin#ness possibly beca"se o% a hiher inci#ence o%systemic hypertension.0 Contrary to these %in#ins/ the st"#y by Ar%in an# co54orers1
>s"este# that blacs ha# a slihtly slo4er rate o% proression than 4hites.Ciarette !moinCiarette smoin/ beca"se it increases bloo# carbon mono:i#e/ platelet areation/ an# ca"ses$asoconstriction/ miht be e:pecte# to accelerate #iabetic retinopathy b"t a lare st"#y recently%o"n# no e%%ect.2
!er"m Lipi#s
8/11/2019 Diabetic Retinopathy.doc
9/23
Ele$ate# ser"m cholesterol is a stron pre#ictor %or the rate o% $is"al loss. 'atients 4ith bothele$ate# cholesterol an# lo45#ensity lipoprotein &LDL( cholesterol are m"ch more liely to ha$e$ision loss associate# 4ith har# e:"#ates in the mac"la.3
'A+-*ENE!I!
+he %inal metabolic path4ay 4hich ca"ses #iabetic retinopathy is "nno4n. +here are se$eraltheories.ALD*!E RED@C+A!EAl#ose re#"ctase is an en7yme that con$erts s"ars/ 4hen present in hih concentration/ intoalcohols. For e:ample/ l"cose is con$erte# to sorbitol &an# later to %r"ctose by polyol#ehy#roenase( an# alactose is con$erte# to #"lcitol. Beca"se sorbitol/ #"lcitol/ an# %r"ctosecannot easily #i%%"se o"t o% cells/ their intracell"lar concentration increases. *smotic %orces #ra44ater into the cells res"ltin in electrolyte imbalance. +he res"ltant #amae to lens epithelialcells/ 4hich ha$e a hih concentration o% al#ose re#"ctase/ is responsible %or the cataracts seen inchil#ren 4ith alactosemia an# in animals 4ith e:perimental #iabetes mellit"s. Beca"se al#osere#"ctase is also %o"n# in hih concentration in retinal pericytes an# !ch4ann cells/ some
in$estiators s"est that #iabetic retinopathy an# ne"ropathy may be ca"se# by al#osere#"ctase5me#iate# #amae./9!tron s"pport %or this theory is that al#ose re#"ctase inhibitorsinhibit cataract %ormation/;permeability to small molec"les/capillary basement membranethicenin/?/ an# pericyte loss.?0 F"rthermore/ they impro$e ner$e con#"ction $elocity/?1/?2
#ecrease pain %rom peripheral ne"ropathy/?3 #ecrease protein"ria/? an# #ecrease $asc"larpermeability./?9
-o4e$er/ clinical trials ha$e th"s %ar %aile# to sho4 a re#"ction in the inci#ence o% #iabeticretinopathy or o% ne"ropathy by al#ose re#"ctase inhibitors/?/??possibly beca"se an e%%ecti$eal#ose re#"ctase inhibitor 4ith %e4 systemic si#e e%%ects has yet to be #e$elope#.?
,A!*'R*LIFERA+I,E FAC+*R!In 19/ 6ichaelson0%irst propose# that hypo:ic retina pro#"ces a syn#rome(/ ro4th hormone 4ass"specte# to play a ca"sati$e or at least an important s"pporti$e role in the #e$elopment an#
8/11/2019 Diabetic Retinopathy.doc
10/23
proression o% #iabetic $asc"lar complications. In the 190>s an# 1;0>s s"rical pit"itaryablation 4as consi#ere# by some to be an e%%ecti$e treatment %or #iabetic retinopathy/ b"t 4ashotly #ebate#. +he s"ccess o% 'R' en#e# the ar"ment. 6ore recently/ ro4th hormone#e%iciency 4as %o"n# to be some4hat protecti$e aainst retinopathy.100
'LA+ELE+! AND BL**D ,I!C*!I+)
!e$eral lines o% e$i#ence stronly s"est that platelet abnormalities in #iabetics may contrib"teto retinopathy.101+here are three steps in platelet coa"lationG initial a#hesion/ secretion/ an#%"rther areation. A#hesion re%ers to the propensity o% platelets/ ai#e# by $on Willebran#%actor &%actor ,III( to stic to basement membrane/ #amae# en#othelial cells/ an# collaen. 102Ithas been sho4n that the platelets in #iabetic patients are s cell membrane. Aracha#onic aci# is then con$#rte#thro"h se$eral prostalan#in interme#iaries to another prostalan#in/ thrombo:ane A2/ 4hich is
one o% the most potent $asoconstrictin an# platelet areatin aents no4n. As a bypro#"cto% these e$ents/ a#enosine #iphosphate &AD'(/ another platelet areatin aent/ is release#.Diabetic platelets are especially sensiti$e to thrombo:ane an# to other areatin aents s"ch asepinephrine.103/10 It has been post"late# that abnormal platelet a#hesion an# areation ca"ses%ocal capillary occl"sion an# %ocal areas o% ischemia in the retina/ 4hich in t"rn contrib"te to the#e$elopment o% #iabetic retinopathy.101-o4e$er/ it sho"l# be mentione# that 'DR has beenreporte# in patients 4ith se$ere platelet #ys%"nction.109
,ie4 Fi"re
Fi. 1? 'latelet a#hesion an# areation.
*+-ER -E6A+*L*IC ABN*R6ALI+IE!*ther hematoloic abnormalities seen in #iabetics are increase# bloo# $iscosity/10; increase#erythrocyte areation/10 an# #ecrease# erythrocyte #e%ormacility/10? all o% 4hich maycontrib"te to sl"ish circ"lation an# en#othelial #amae.'!)C-*'-)!ICAL AND ELEC+R*'-)!I*L*IC ABN*R6ALI+IE!'!)C-*'-)!ICAL ABN*R6ALI+IE!*ne o% the early symptoms o% #iabetic retinopathy is poor niht $ision ar a#aptation( an#poor reco$ery %rom briht lihts &photostress(.113/11/119/11;Also/ patients 4ith #iabetes/ e$en those4itho"t retinopathy/ are more liely to ha$e abnormal color $ision than are those 4itho"t
#iabetes matche# %or ae.11/11?/11/120 Bl"eyello4 #iscrimination is a%%ecte# earlier an# morese$erely than is re#reen #iscrimination. As retinopathy a#$ances/ color $ision #eteriorates.Contrast sensiti$ity may be abnormal in patients 4itho"t #iabetic retinopathy at a time that!nellen $is"al ac"ity is normal.121/122/123 *c"lar hypertension 4orsens both color $ision an#contrast sensiti$ity.12
ELEC+R*'-)!I*L*IC ABN*R6ALI+IE!*ne o% the earliest electrophysioloic aboormalities seen in patients 4ith #iabetes 4itho"tophthalmoscopically $isible retinopathy is #imin"tion o% the amplit"#e o% the oscillatory
http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F18-V3-308/11/2019 Diabetic Retinopathy.doc
11/23
potentials &*'>s( o% the electroretinoram at a time 4hen both the a5 an# b54a$es arenormal.129/12;/12/12?/12+his abnormality probably re%lects ischemia in the inner n"clear layer o% theretina. Diminishe# *'>s are a oo# pre#ictor o% proression o% retinopathy. 130As the se$erity o%#iabetic retinopathy increases/ the amplit"#e o% the b54a$e #ecreases.DIFFEREN+IAL DIAN*!I!
Con#itions that ha$e %eat"res similar to #iabetic retinopathy are ra#iation retinopathy/hypertensi$e retinopathy/ retinal $eno"s obstr"ction/ the oc"lar ischemic syn#rome/ anemia/le"emia/ Coats> #isease/ retinal telaniectasia/ an# sicle cell retinopathy.131
+REA+6EN+RED@C+I*N *F !)!+E6IC RI! FAC+*R!6e#ical +herapyA!'IRIN.Aspirin blocs the con$ersion o% aracha#onic aci# to prostalan#ins/ thereby inhibitin plateletsecretion an# areation &see Fi. 1?(. Beca"se o% its s"ccess in #ecreasin the inci#ence o%transient ischemic attacs &+IAs(/ clinicians theori7e# that it miht retar# the proression o%#iabetic retinopathy. +he Early +reatment Diabetic Retinopathy !t"#y %o"n# that ;90 m o%
aspirin #aily #i# not in%l"ence the proression o% retinopathy/ #i# not a%%ect $is"al ac"ity/ an# #i#not in%l"ence the inci#ence o% $itreo"s hemorrhaes.10*n the other han#/ another ro"p %o"n#that 0 m o% aspirin #aily alone or combine# 4ith 229 m o% #ipyri#amole &'ersantine(sini%icantly slo4e# the ann"al appearance o% ne4 microane"rysms/ b"t the st"#y 4as notcarrie# o"t lon eno"h to #emonstrate any clinical sini%icance.110
+ICL*'IDINE.+iclopi#ine &+icli#( inhibits AD'5in#"ce# platelet areation. !imilar to aspirin/ the e%%ect ispermanent %or the li%e o% a labele# platelet. It has been sho4n to #ecrease the ris o% stroe inpatients 4ith +IAs. *ne short5term st"#y sho4e# statistically sini%icant re#"ction in the#e$elopment o% #iabetic retinopathy.111
'EN+*KIF)LLINE.'ento:i%ylline &+rental( increases retinal capillary bloo# %lo4 $elocity probably by impro$inerythrocyte an# le"ocyte %le:ibility. It #ecreases bloo# $iscosity. +o #ate/ ho4e$er/ a clinicalbene%it has not been sho4n %or #iabetic retinopathy.112
'anretinal 'hotocoa"lationWhen 4ell5%oc"se#/ intense liht is absorbe# by pimente# cells &s"ch as erythrocytes orpiment epithelial cells(/ it is con$erte# to heat/ coa"latin the cells an# s"rro"n#in tiss"es.+he %irst photocoa"lator/ the :enon arc/ pro#"ce# an intense liht that 4as s"ccess%"l inobliteratin neo$asc"lari7ation that 4as either on the s"r%ace o% the retina or only slihtlyele$ate# &Fi. 1(. Clinicians tho"ht that eyes treate# 4ith :enon arc photocoa"lation ha#oo# reression o% retinopathy an# %e4er $itreo"s hemorrhaes than 4o"l# ha$e been e:pecte#ha# they not been treate#. -o4e$er/ :enon arc photocoa"lation ha# se$ere limitations. First/ theheat enerate# 4as o%ten ins"%%icient to obliterate hihly ele$ate# neo$asc"lari7ation. !econ#/neo$asc"lari7ation arisin %rom the optic ner$e co"l# not be #irectly treate# beca"se the intenseliht beam #amae# the optic ner$e. Finally/ in many cases/ all o% the neo$asc"lari7ation 4asinitially obliterate#/ b"t ne4 areas o% neo$asc"lari7ation later #e$elope#. For these reasons/ thelon5term res"lts o% photocoa"lation 4ere consi#ere# by many obser$ers to be no better than notreatment at all.
8/11/2019 Diabetic Retinopathy.doc
12/23
,ie4 Fi"re
Fi. 1 A. Neo$asc"lari7ation imme#iately a%ter :enon5arcphotocoa"lation. B. *ne year later. +he neo$asc"lari7ationelse4here &N,E( has been obliterate#.
+o pre$ent ne4 areas o% neo$asc"lari7ation/ se$eral ophthalmoloists bean to photocoa"latenot only neo$asc"lari7ation b"t all intraretinal hemorrhaes as 4ell &
8/11/2019 Diabetic Retinopathy.doc
13/23
TABLE 1. Results of the DRS at Three Years
VA less than 5/200 With PRP Without PRP
N,D 1H2 DD 4ith ,- .3 29.;N,D 1H2 DD 4Ho ,- ?.9 2;.2N,D 1H2 DD 4ith ,- 20.1 3;.
N,E 1H2 DD 4ith ,- .2 2.DR!/ Diabetic Retinopathy !t"#y DD/ #isc #iameters ,A/ $is"al ac"ity ,-/ $itreo"shemorrhae.
A%ter 'R'/ retinal circ"lation is #e%initely impro$e#. +here is a better re"latory response tohypo:ia an# #ecrease# bloo# %lo4.13/1+he e:act mechanism by 4hich 'R' 4ors remains"nno4n. !ome in$estiators belie$e that 'R' #ecreases pro#"ction o% $asoproli%erati$e %actors%irst by eliminatin some o% the hypo:ic retina or by stim"latin the release o% anthanioenic%actors %rom the retinal piment epitheli"m.19An alternati$e hypothesis is that $essel #ilatationca"se# by chronic hypo:ia is the #irect stim"l"s %or en#othelial cell proli%eration an#neo$asc"lari7ation an# that 'R' 4ors by thinnin the retina. ,aso#ilatation is re#"ce# by
increase# #i%%"sion o% o:yen %rom the choroi#.
1;/1/1?/1
Another possibility is that 'R'#ecreases choroi#al circ"lation in the mi#periphery/ 4hich in t"rn sh"nts bloo# %lo4 centrally/&
8/11/2019 Diabetic Retinopathy.doc
14/23
'R' "ntil hih5ris characteristics #e$elope# ha# a $is"al ac"ity o% 9H200 or less compare# to2.9 o% eyes assine# to imme#iate 'R'. +he #i%%erence 4as neither clinically nor statisticallysini%icant. !o/ i% all eyes 4ith se$ere N'DR recei$e# 'R'/ many 4o"l# be treate# "nnecessarily.+hir#/ 'R' has sini%icant complications. 'R' o%ten ca"ses #ecrease# $is"al ac"ity by increasinmac"lar e#ema1;2/1;3/1;or by ca"sin mac"lar p"cer. Fort"nately/ the e#ema %re8"ently reresses
spontaneo"sly o$er ; months. +he $is"al %iel# is "s"ally mo#erately #ecrease#.113
Color $isionan# #ar a#aptation/ 4hich are o%ten alrea#y impaire#/ are also 4orsene# by 'R'.11/119/11;Finally/'DR is associate# 4ith an increase# ris o% myocar#ial in%arction an# increase# mortality.1;9
6any patients 4ill #ie be%ore they #e$elop complications o% the 'DR.'eripheral Retinal Cryotherapy'eripheral retinal cryotherapy &'RC( is "se# to treat eyes 4ith hih5ris characteristics an# 4ithme#ia too ha7y %or 'R'. Reporte# bene%its incl"#e resorption o% $itreo"s hemorrhaes an#reression o% N,D/ N,E/ an# N,I.1;;/1;/1;?/1;/10/11/12+he main complication is the #e$elopmentor acceleration o% traction retinal #etachment in 29 to 3? o% eyes.10/13 +here%ore/ thistreatment sho"l# be a$oi#e# in patients 4ith no4n traction retinal #etachment an# all patientsm"st be care%"lly monitore#. An alternati$e treatment in eyes 4ith ha7y me#ia is transscleral
#io#e laser photocoa"lation.+reatment o% 6ac"lar E#ema'at7 an# co54orers14ere the %irst to sho4 that %ocal aron laser photocoa"lation #ecreases orstabili7es mac"lar e#ema. Later/ the E+DR! con%irme# their res"lts. +he E+DR! #e%ine#clinically sini%icant mac"lar e#ema &C!6E( as &1( retinal thicenin in$ol$in the center o% themac"la/ &2( har# e:"#ates 4ithin 00 Mm o% the center o% the mac"la &i% they are associate# 4ithretinal thicenin(/ or &3( an area o% mac"lar e#ema reater than one #isc area 4hich is 4ithinone #isc #iameter o% the center o% the mac"la. +he treatment stratey 4as to treat all leainmicroane"rysms %arther than 900 Mm %rom the center o% the mac"la &Fi. 23( an# to place a ri#o% 100 to 200 M b"rns in areas o% #i%%"se capillary leaae an# in areas o% capillary nonper%"sion.A%ter 3 years o% %ollo45"p/ 19 o% eyes 4ith eyes 4ith C!6E ha# #o"blin o% the $is"al anleas oppose# to 32 o% nontreate# control eyes.19Recent s"bro"p analysis sho4e# that treatmentco"l# be #e%erre# in eyes in 4hich the center o% the %o$ea is not thicene# as lon as har#e:"#ates are not threatenin the center. -o4e$er/ s"ch eyes m"st be closely obser$e#.19
,ie4 Fi"re
Fi. 23 A. Fi%ty5t4o5year5ol# man 4ith clinically sini%icantmac"lar e#ema an# a partial circinate rin o% har# e:"#ates. B.6i#phase o% the %l"orescein anioram sho4s a cl"ster o%microane"rysms in the center o% the are a e#ema. C. Late phasesho4s se$ere leaae. D. !e$eral months a%ter treatment/ thee#ema is no loner present an# the $is"al ac"ity is 20H29.
+he E+DR! also sho4e# that 'R' is not part o% the treatment stratey o% C!6E. Eyes thatrecei$e# 'R' alon 4ith their %ocal treatment 4ere m"ch more liely to ha$e an imme#iate#ecrease in $is"al ac"ity than 4ere eyes that recei$e# %ocal treatment alone. 11 An alternati$etreatment to the E+DR! stratey is a ri# treatment &Fi. 2(.1;
http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F23-V3-308/11/2019 Diabetic Retinopathy.doc
15/23
,ie4 Fi"re
Fi. 2 A. +hirty5%i$e5year5ol# 4oman 4ith #i%%"se mac"lare#ema an# a $is"al ac"ity o% 20H;0. B. +he mi#phase o% theanioram sho4s #i%%"se mac"lar e#ema C. +he late phase sho4sse$ere leaae an# cystoi# mac"lar e#ema D. ri# treatment. E.+he mi#phase o% the anioram #one months later sho4s
minimal leaae. F. +he late phase also sho4s minimal leaae.+he $is"al ac"ity is 20H29.
'atients 4ith mac"lar e#ema 4ho ha$e the best pronosis %or impro$e# $ision ha$e circinate
retinopathy o% recent #"ration or %ocal/ 4ell5#e%ine# leain areas an# oo# capillary per%"sions"rro"n#in the a$asc"lar 7one o% the retina. 'atients 4ith an especially poor pronosis ha$e#ense lipi# e:"#ate in the center o% the %o$ea & Fi. 29(. *ther poor pronostic sins incl"#e#i%%"se e#ema 4ith m"ltiple leain areas/ capillary clos"re aro"n# the %o$ea &Fi. 2;(/ increase#bloo# press"re/ an# cystoi# mac"lar e#ema.1/1Ne$ertheless/ the E+DR! %o"n# that e$en eyes4ith these a#$erse %in#ins bene%ite# %rom treatment compare# to control eyes. 19+he "se o%intra$itreal steroi#s is also recei$in attention %or its potential role in the treatment o% persistent#iabetic e#ema. !mall "ncontrolle# series ha$e #emonstrate# #ramatic re#"ction o% mac"lathicness 4ith associate# impro$ement in $is"al %"nction.1?/1 Altho"h enco"rain/intra$itreal corticosteroi#s are associate# 4ith %re8"ent ele$ate# intraoc"lar press"re an#occasionally en#ophthalmitis.1?0/1?1
,ie4 Fi"re
Fi. 29 Circinate retinopathy 4ith lare har# e:"#ates pla8"e in the center o% themac"la.
,ie4 Fi"re
Fi. 2; Ischemic #iabetic mac"lopathy. Notice lare central areas o% capillarynonper%"sion s"rro"n#e# by microane"rysms.
,itrectomy techni8"es are also increasinly bein consi#ere# %or #iabetic e#ema manaement.Early reports %o"n# "p to 0 o% eyes "n#eroin $itrectomy %or the treatment o% e#emaassociate# 4ith a ta"t or thicene# posterior hyaloi# ha# $is"al impro$ement.1?2/1?3Recent larerseries con%irm the e%%icacy o% $itrectomy %or eyes 4ith abnormal hyaloi#mac"la inter%ace. 1?/1?9
+he s"ccess in this s"bro"p o% patients is pre#icte# by the hypothesis that tanential tractione:erte# by attache# $itreo"s contrib"tes to mac"lar e#ema.1?;
6ore mo#est res"lts ha$e been reporte# 4ith $itrectomy %or the treatment o% eyes 4ith attache#hyaloi# that 4ere not ta"t or thicene#. '"blishe# series report appro:imately one5hal% o% the
http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F26-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F25-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-F24-V3-308/11/2019 Diabetic Retinopathy.doc
16/23
eyes impro$e by only a line o% ac"ity.1?Interestinly mac"lar e#ema resol$e# in most o% theseeyes. *tani an# collea"es1??re$ie4e# se$en patients 4ith symmetric #iabetic e#ema 4itho"t anabnormally ta"t hyaloi# 4ho ha# one eye ran#omi7e# to $itrectomy. +hey "se# *C+ to#emonstrate an a$erae #ecrease in mac"lar thicness o% 393 Mm postoperati$ely compare# to a;0 Mm a$erae #ecrease in thicness in the %ello4 eyes.
In s"mmary/ DR! an# the E+DR! concl"si$ely pro$e# that timely laser photocoa"lation o%#iabetic retinopathy can re#"ce se$ere $is"al loss by 9.1?!"ch treatment maes sense notonly %rom the h"manitarian point o% $ie4 b"t is e:tremely cost5e%%ecti$e as 4ell/ sa$inappro:imately 290 to 900 million per year by eepin patients o%% #isability an#4el%are.10/11/12 Ne$ertheless/ only hal% o% Americans 4ith #iabetes/ especially the poor an#minority pop"lation/ %ail to recei$e an ann"al #ilate# eye e:amination.13/1 +he AmericanDiabetes Association recommen#s that patients 4ith type 1 #iabetes sho"l# be screene# ann"allybeinnin 9 years a%ter the onset o% the #isease an# patients 4ith type 2 sho"l# be screene#imme#iately an# then ann"ally therea%ter.19 Alternati$es metho#s o% screenin 4henophthalmoloists are not a$ailable incl"#e the "se o% primary care physicians or #iitalphotoraphy 4ith remote imae interpretation. Altho"h primary care physicians commonly %ail
to #etect sini%icant retinopathy 4ith #irect ophthalmoscopy/ trainin sini%icantly impro$es theirability.?;/1;
,itrectomy in 'atients 4ith DiabetesRear#in this topic/ the rea#er sho"l# also cons"lt Chapter 9;/ ,ol"me ; %or #etails.202
,itrectomy/ intro#"ce# by Robert 6achemer/ plays a $ital role in the manaement o% se$erecomplications o% #iabetic retinopathy. +he maor in#ications are non5clearin $itreo"shemorrhae/ traction retinal #etachment/ an# combine# tractionHrhematoeno"s retinal#etachment. Less common in#ications are mac"lar e#ema 4ith a thicene# an# ta"t posteriorhyaloi#/203/20mac"lar heterotopia/ an# tiht preretinal mac"lar hemorrhae/1?/1
+o e$al"ate 4hether early $itrectomy &in the absence o% $itreo"s hemorrhae( miht impro$e the$is"al pronosis by eliminatin the possibility o% later traction mac"lar #etachment/ the DiabeticRetinopathy ,itrectomy !t"#y &DR,!( ran#omi7e# 30 eyes 4ith %lori# neo$asc"lari7ation an#$is"al ac"ity o% 10H200 or better to either early $itrectomy or to obser$ation. 209A%ter years o%%ollo45"p/ appro:imately 90 o% both ro"ps ha# 20H;0 or better an# appro:imately 20 o%each ro"p ha# liht perception or 4orse. +h"s/ the res"lts in#icate that s"ch patients probably#o not bene%it %rom early $itrectomy. +hey sho"l# be obser$e# closely so that $itrectomy/ 4henin#icate#/ can promptly be "n#ertaen.I% a patient has a $itreo"s hemorrhae se$ere eno"h to ca"se a $is"al ac"ity o% 9H200 or less/ thechances o% $is"al reco$ery 4ithin 1 year are only appro:imately 1.20;+he DR,! ran#omi7e#patients 4ho ha# a $is"al ac"ity o% 9H200 or less %or more than ; months into t4o ro"psG those4ho recei$e# an imme#iate $itrectomy an# those %or 4hom $itrectomy 4as #e%erre# %or ana##itional ; months.20Fi%teen percent o% those 4ho ha# a #e%erre# $itrectomy ha# a %inal $is"alac"ity o% 20H0 or better as oppose# to 29 o% those 4ho ha# an imme#iate $itrectomy. Inpatients 4ith type 1 #iabetes/ 12 o% those 4ho ha# a #e%erre# $itrectomy ha# a %inal $is"alac"ity o% 20H0 or better as oppose# to 3; o% those 4ho ha# an imme#iate $itrectomy. +hereason %or this #iscrepancy 4as tho"ht to be e:cessi$e ro4th o% %ibro$asc"lar proli%eration#"rin the 4aitin perio#. For this reason/ the DR,! concl"#e# that stron consi#eration sho"l#be i$en to imme#iate $itrectomy/ especially in type 1 #iabetics. &In type 2 #iabetics/ the %inal$is"al res"lts 4ere similar.( In most cases/ $itrectomy sho"l# be #e%erre# %or appro:imately ;months or loner i% the retina is attache# to i$e the patient a chance %or spontaneo"s clearin.
8/11/2019 Diabetic Retinopathy.doc
17/23
!ome patients 4ill ne$er nee# the s"rery/ b"t more importantly/ 29 o% the patients in theDR,! 4ho recei$e# an imme#iate $itrectomy ha# a %inal $is"al ac"ity o% NL'. 'atients 4ithbilateral $is"al loss beca"se o% $itreo"s hemorrhae/ 4ith chronically rec"rrin hemorrhae/ 4ithno history o% 'R'/ an# 4ith no4n traction retinal #etachment close to the mac"la are o%%ere#s"rery sooner. I% s"rery is #e%erre#/ "ltrasonoraphy sho"l# be per%orme# at re"lar inter$als
to mae s"re that traction retinal #etachment is not #e$elopin behin# the hemorrhae. +he oalso% s"rery are to release all anteriorposterior $itreo"s traction an# to per%orm a complete 'R' tore#"ce the inci#ence o% rec"rrent hemorrhae. F"rthermore/ the res"lts o% $itrectomy %ornonclearin $itreo"s hemorrhae are e:cellent &+able 2(.TABLE 2. !eral Visual Results
Benson Tho"#son20$ DRVS20%
20H2020H0 2 2 2920H9020H100 2 2 220H12020H300 1; 22 920H00CF ? 12 -65L' 12 13 10
NL' ; ; 29DR,!/ Diabetic Retinopathy ,itrectomy !t"#y. -65L'/ O NL'/ O.
In patients 4ho ha$e rec"rrent $itreo"s hemorrhae a%ter $itrectomy/ a simple o"tpatientairHli8"i# e:chane may restore $ision 4itho"t the nee# %or a repeat $itrectomy.20
+raction retinal #etachments are "s"ally a m"ch reater challene. In eneral/ "nless the mac"labecomes in$ol$e#/ obser$ation is the best therapy %or these patients beca"se/ in most cases/ the#etachment 4ill not proress into the mac"la.210+hese patients sho"l# be co"nsele# to cons"lttheir ophthalmoloist 4itho"t #elay sho"l# mac"lar $ision be s"##enly lost/ beca"se $itrectomyat that point becomes a relati$e emerency.202+he s"rical obecti$es are to clear the me#ia/ torelease all anteriorposterior traction/ to release tanential traction by c"ttin bri#es bet4eenareas o% traction #etachment or by #elamination/ an# to per%orm en#ophotocoa"lation to pre$entneo$asc"lari7ation o% the iris. +he pronosis is best in patients 4ith small areas o% traction. Analternati$e techni8"e is to remo$e the $itreo"s an# preretinal membranes by the
8/11/2019 Diabetic Retinopathy.doc
18/23
s"rery/ i% the lens is remo$e# #"rin s"rery/ an# i% there is %lori# N,D an# N,E. In eyes4itho"t these %actors/ the inci#ence o% neo$asc"lar la"coma is only abo"t 2.22; +hepathoenesis o% this complication is "nno4n. !ome in$estiators %eel that remo$al o% the$itreo"s allo4s $asoproli%erati$e %actors pro#"ce# in hypo:ic retina to #i%%"se %or4ar# to the iris.*thers %eel that the main problem is that o:yen #i%%"ses posteriorly %rom the anterior chamber
lo4erin its o:yen tension too %ar. Fort"nately/ i% an eye #oes not #e$elop r"beosis iri#is in the%irst to ; months a%ter $itrectomy/ it rarely 4ill #o so later.Another $ision5threatenin complication is neo$asc"lari7ation oriinatin %rom the anteriorretina an# e:ten#in alon the anterior hyaloi# to the posterior lens s"r%ace &anterior hyaloi#al%ibro$asc"lar proli%eration(.22
*+-ER *C@LAR C*6'LICA+I*N! *F DIABE+E! 6ELLI+@!C*RNEA!e$eral in$estiations ha$e %o"n# #ecrease# corneal sensiti$ity in patients 4ith#iabetes.22?/22/230/231+he se$erity o% the hypesthesia has been correlate# 4ith both the #"ration o%the #isease230an# the se$erity o% the retinopathy.22?/231
+he a#hesion bet4een the basement membrane o% the corneal epitheli"m an# the corneal stroma
is not as %irm as that %o"n# in normal corneas/ probably beca"se o% a #ecrease# n"mber o%hemi#esmosomes bet4een the stroma an# the epitheli"m. When the epitheli"m is scrape# %rom anormal cornea/ the bottom hal% o% the cells %ormin the basal layer are broen an# remainattache# to the basement membrane/ 4hich remains attache# to the stroma. In #iabetics/ theentire epitheli"m is remo$e# intact. -yperlycemia an# the al#ose re#"ctase path4ay probablyplay a maor role in epithelial abnormalities beca"se al#ose re#"ctase inhibitors acceleratehealin o% corn#al abrasions.232/233/23 A%ter $itrectomy/ rec"rrent corneal erosion/ striateeratopathy/ an# corneal e#ema are more common in patients 4ith #iabetess than in tose 4itho"t#iabetes. Altho"h it has been sho4n that the en#othelial cell #ensity is normal in #iabetics/ 239itis not yet no4n 4hether or not en#othelial cell"lar #ys%"nction contrib"tes to thesecomplications.LA@C*6ABecer23;%o"n# that in patients 4ith #iabetes there is a hiher inci#ence o% open5anle la"comaan# mare# ele$ation o% intraoc"lar press"re a%ter prolone# a#ministration o% topicalcorticosteroi#s than there is in patients 4itho"t #iabetes. 6oreo$er/ patients 4ith #iabetes aremore s"sceptible to $is"al %iel# loss than those 4ho #o not ha$e #iabetes.N,I is rarely associate# 4ith N'DR alone. It is "s"ally seen only in eyes 4ith 'DR. By the en#o% the %ollo45"p perio# o% the DR!/ +asman an# co54orers23%o"n# N,I in 3.? o% the patients4ho ha# not recei$e# 'R' as oppose# to 2.0 in those 4ho ha#. +h"s/ 'R' appears to ha$esome protecti$e $al"e aainst N,I. 'R' is also an e%%ecti$e treatment aainst establishe#N,I.23?/23/20Reression o% the iris $essels an# stabili7ation o% any areas o% anle clos"re an# o%intraoc"lar press"re ha$e been reporte# in ?0 o% cases treate#. I% the me#ia are clear/ 'R'sho"l# be per%orme# prior to any other treatment o% N,I/ e$en in a#$ance# cases. Jacobson an#associates23?reporte# s"ccess%"l res"lts as lon as the intraoc"lar press"re 4as less than 0 mm- an# there 4as less than 20 #erees o% anle clos"re. We ha$e seen reression an# permanentpress"re control in patients 4ith press"res as hih as ;0 mm -. I% the me#ia are too clo"#y %or'R'/ peripheral retinal cryoablation an# transscleral #io#e laser photocoa"lation are alternati$emeans o% treatment &see abo$e(.
8/11/2019 Diabetic Retinopathy.doc
19/23
I% the anle is completely seale# an# there is reasonable $is"al potential/ a 6olteno or other t"besh"nt o%%ers the best chance %or preser$in $ision.21 Cyclocryo#estr"cti$e proce#"res o%tenres"lt in phthisis.LEN!Beca"se the lens in patients 4ith #iabetes has m"ltiple biochemical abnormalities/22the ris o%
cataract is 2 to times reater in than in patients 4itho"t #iabetes23/2/29/2;/2
an# may be 19 to29 times reater in patients 4ith #iabetes "n#er 0 years o% ae.2?F"rthermore/ the occ"rrenceo% cataract is a pre#ictor o% increase# mortality.22
'atients 4ith #iabetes mellit"s 4ho ha$e no retinopathy ha$e e:cellent res"lts %rom cataracts"rery/ 4ith 0 to 9 ha$in a %inal $is"al ac"ity o% 20H0 or better/ b"t/ chronic cystoi#mac"lar e#ema is appro:imately 1 times more common in patients 4ith #iabetes than in those4itho"t.2/290/291In patients 4ith mil# to mo#erate N'DR 4itho"t mac"lar e#ema/ appro:imately0 to ?0 attain 20H0 o"tcomes are sini%icantly 4orse in eyes 4ith more se$ereretinopathy.292/293/29Ris %actors %or proression an# 4orse $ision incl"#e an ol#er ae/ 299 poorlycemic control/292poor renal %"nction/ an# most sini%icant preoperati$e mac"lar e#ema. Inmany eyes the e#ema is sel%5limite# an# beha$es clinically lie postcataract C6E %ocal laser
sho"l# be #elaye# 4hen #i%%erentiation bet4een #iabetic e#ema cannot be ma#e. +he maority o%eyes 4ith C6E 4ill impro$e in ; months.29;
+he most #rea#e# anterior complication is N,I. It 4as hope# that mo#ern s"rery that lea$es anintact posterior caps"le 4o"l# protect the eye %rom neo$asc"lari7ation o% the iris/ by re#"cin the#i%%"sion o% $asoproli%erati$e %actors into the anterior chamber b"t se$eral st"#ies ha$e sho4nthat it #oes not. Eyes o% patients 4ith #iabetes more %re8"ently #e$elop sini%icant posteriorcaps"lar opaci%ication29 %ort"nately caps"lotomy #oes not seem to increase the ris o% anteriorsement neo$asc"lari7ation.2*ther anterior sement complications that are more common inpatients 4ith #iabetes than in those 4itho"t are p"pillary bloc/ posterior synechiae/ pimente#precipitates on the implant/ an# se$ere iritis.290
'osterior complications incl"#e mac"lar e#ema an# ischemia/299/29;/29? proli%erati$eretinopathy/2/29$itreo"s hemorrhae/ an# traction retinal #etachment.291/29?/2;0In patients 4ithacti$e N'DR an# no preoperati$e mac"lar e#ema/ as many as 90 to 9 4ill #e$elop it an#30 4ill #e$elop 'DR. Appro:imately ? 4ill #e$elop N,-. I% mac"lar e#ema is present priorto the s"rery/ it nearly al4ays 4orsens. *nly appro:imately 90 4ill ha$e a %inal $is"al ac"ityo% 20H0 or better. +he ris o% the #e$elopment o% or proression o% mac"lar e#ema is nearly#o"ble# in patients 4ho are ol#er than ;3 years o% ae.2;Clearly/ ca"tion m"st be obser$e#4hen consi#erin cataract s"rery in patients 4ho ha$e #iabetic retinopathy.Cataract s"rery in patients 4ith acti$e 'DR o%ten res"lts in still poorer postoperati$e $is"alo"tcome beca"se o% the hih ris o% both anterior2;2an# posterior sement complications. In oneseries/ no patient 4ith acti$e 'DR or ''DR achie$e# better than 20H?0. Anteriorly/ %ibrino"s"$eitis is seen in more than 90 o% patients 4ith acti$e 'DR. 6ost e:perts recommen#aressi$e preoperati$e 'R'.29?/2;?
*'+IC NE@R*'A+-)As #emonstrate# by increase# latency an# #ecrease# amplit"#e o% the $is"al e$oe# potential/many patients 4ith #iabetes 4itho"t retinopathy ha$e s"bclinical optic ne"ropathy.2;/20 Ina##ition/ patients 4ith #iabetes can #e$elop t4o types o% ac"te optic ne"ropathy. +he %irst/anterior ischemic optic ne"ropathy &AI*N( is i#entical to that seen in patients 4itho"t #iabetes.+he patients report a s"##en #ecrease in $is"al ac"ity or a s"##en $is"al %iel# loss.21/22/23+hemain oc"lar %in#in is a
8/11/2019 Diabetic Retinopathy.doc
20/23
8/11/2019 Diabetic Retinopathy.doc
21/23
?. Far>s +/ !yl$ester ,/ Archer DG An electron microscopic st"#y o% the choriocapillaries an#Br"ch>s membrane in #iabetic retinopathy. +rans *phthalmol !oc @ 0G;9/ 1. -ersh '!/ reen WR/ +homs JJ,G +ractional $eno"s loops in #iabetic retinopathy. Am J*phthalmol 2G;;1/ 1?110. Early +reatment Diabetic Retinopathy !t"#y Research ro"pG F"n#"s photoraphic ris
%actors %or proression o% #iabetic retinopathy. *phthalmoloy ?G?23/ 1111. Early +reatment Diabetic Retinopathy !t"#y Research ro"pG Early 'hotocoa"lation %or#iabetic retinopathy. E+DR! Report N"mber . *phthalmoloy ?G;;/ 1112. !him"7" / obayashi )/ 6"raoa G 6i#peripheral %"n#"s in$ol$ement in #iabeticretinopathy. *phthalmoloy ??G;01/ 1?113. ,alsania '/ Warram J-/ Ran# LI/ et alG Di%%erent #eterminants o% neo$asc"lari7ation on theoptic #isc an# on the retina in patients 4ith se$ere nonproli%erati$e #iabetic retinopathy. Arch*phthalmol 111G202/ 131. Foos R)/ reier AE/ Fors:the AB/ et alG 'osterior $itreo"s #etachment in #iabetic s"bects.*phthalmoloy ?G122/ 1?019. Da$is 6DG ,itreo"s contraction in proli%erati$e #iabetic retinopathy. Arch *phthalmol
G1/ 1;91;. An#erson BJrG Acti$ity an# #iabetic $itreo"s hemorrhae. *phthalmoloy ?G13/ 1?01. +asman WG Diabetic $itreo"s hemorrhae an# its relationship to hypolycemia. 6o# 'rob*phthalmol 20G13/ 11?. Ralsay RC/ nobloch W-/ Cantrill -LG +imin o% $itrectomy %or acti$e proli%erati$e#iabetic retinopathy. *phthalmoloy 3G2?3/ 1?;1. *>-anley '/ Canny CLBG Diabetic #ense premac"lar hemorrhae. A possible in#ication %orprompt $itrectomy. *phthalmoloy 2G90/ 1?920. Bresnic -/ -aiht B/ #e,enecia G Retinal 4rinlin an# mac"lar heterotopia in #iabeticretinopathy. Arch *phthalmol G1?0/ 121. ostraaba JN/ Dorman J!/ *rchar# +J/ et alG Contrib"tion o% #iabetes #"ration be%orep"berty to #e$elopment o% micro$asc"lar complications in IDD6 s"bects. Diabetes Care12G;?;/ 1?22. lein R/ lein BE/ !yrala !E/ et alG Wisconsin epi#emioloic st"#y o% #iabeticretinopathy. In Frie#man EA/ L>Esperance FA/ e#s. Diabetic Renal5Retinal !yn#rome. Ne4)orG r"ne P !tratton/ 1?1G2123. lein R/ lein BE/ 6oss !E/ Da$is 6D/ De6ets DL. +he Wisconsin epi#emioloic st"#yo% #iabetes retinopathy. III. 're$alence an# ris o% #iabetic retinopathy 4hen ae o% #ianosis is30 or more years. Arch *phthalmol 102G92/ 1?2. !olie AG *c"lar complications in ins"lin treate# #iabetes mellit"s. *phthalmoloica.1?1;3G1;29. 'almber '/ !mith 6/ Waltman !/ et alG +he nat"ral history o% retinopathy in ins"lin5#epen#ent "$enile5onset #iabetes. *phthalmoloy ??G;13/ 1?12;. D4yer 6!/ 6elton LJ/ Ballar# DL/ et alG Inci#ence o% #iabetic retinopathy an# blin#nessG Apop"lation5base# st"#y in Rochester/ 6inoesota. Diabetes Care ?G31;/ 1?92. lein R/ lein BEG Epi#emioloy o% proli%erati$e #iabetic retinopathy. Diabetes Care19G1?9/ 122?. lein R/ Da$is 6D/ 6oss !E/ et alG +he Wisconsin epi#emioloic st"#y o% #iabeticretinopathyG a comparison o% retinopathy in yo"ner an# ol#er onset #iabetic persons. In ,ranic
http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R27-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R26-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R25-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R24-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R23-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R22-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R21-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R20-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R19-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R18-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R17-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R16-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R15-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R14-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R13-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R12-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R11-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R10-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R9-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R8-V3-308/11/2019 Diabetic Retinopathy.doc
22/23
6/ -ollenber C/ !teiner / e#s. Comparison o% +ype I an# +ype II Diabetes. Ne4 )orG'len"m/ 1?9G3213292. lein R/ lein BE/ 6oss !E/ et alG +he Wisconsin Epi#emioloic !t"#y o% #iabeticretinopathy. KI,. +en5:ear inch#ence an# proression o% #iabetic retinopathy. Arch *phthalmol112G121/ 1
30. )ano L/ ol#bo"rt @/ 6ichaelson IC/ et alG 're$alence an# 195year inci#ence o% retinopathyan# associate# characteristics in mi##le5ae# an# el#erly #iabetic men. Br J *phthalmol ;G9/1?331. Diabetes Control an# Complications +rial Research ro"pG +he e%%ect o% intensi$e #iabetestreatment on the proression o% #iabetic retinopathy in ins"lin5#epen#ent #iabetes mellit"s. Arch*phthalmol 113G3;/ 1932. Diabetes Control an# Complications +rial Research ro"p. +he e%%ect o% intensi$e treatmento% #iabetes on the #e$elopment an# proression o% lon5term complications in ins"lin5#epen#ent#iabetes mellit"s. N Enl J 6e# 32G/ 1333. @nite# in#om 'rospecti$e Diabetes !t"#y ro"pG Intensi$e bloo#5l"cose control 4iths"lphonyl"reas or ins"lin compare# 4ith con$entional treatment an# ris o% complications in
patients 4ith type 2 #iabetes &@'D! 33(. Lancet 392G?3/ 1?3. ray A/ Raio" 6/ 6c"ire A/ et alG Cost e%%ecti$eness o% an intensi$e bloo# l"cosecontrol policy in patients 4ith type 2 #iabetesG economic analysis alonsi#e ran#omise#controlle# trial &@'D! 1(. @nite# in#om 'rospecti$e Diabetes !t"#y ro"p. B6J320G133/ 200039. Brinchmann5-ansen */ Dahl5Jorens#n / !an#$i L/ et alG Bloo# l"cose concentrationsan# proression o% #iabetic retinopathyG the se$en year res"lts o% the *slo st"#y. B6J 30G1/123;. La4son '6/ Champion 6C/ Canny C/ et alG Contin"o"s s"bc"taneo"s ins"lin in%"sion&C!II( #oes not pre$ent proression o% proli%erati$e an# preproli%erati$e retinopathy. Br J*phthalmol ;;G;2/ 1?23. Brinchmann5-ansen */ Dami5Jorensen / -anssen F/ et alG E%%ects o% intensi%ie# ins"lintreatment on $ario"s lesions o% #iabetic retinopathy. Am J *phthalmol 100G;/ 1?93?. $anBalleooie E/ -ooymans J6/ +immerman Q/ et alG Rapi# #eterioration o% #iabeticretinopathy #"rin treatment 4ith contin"o"s s"bc"taneo"s ins"lin in%"sion. Diabetes CareG23;/ 1?3. R*C Collaborati$e !t"#y ro"pG Diabetic retinopathy a%ter t4o years o% intensi%ie# ins"lintreatment. JA6A 2;0G3/ 1??0. Ramsay RC/ oet7 FC/ !"therlan# DER/ et alG 'roression o% #iabetic retinopathy a%terpancreas transplantation %or ins"lin5#epen#ent #iabetes mellit"s. Ne4 Enl J 6e# 31?G20?/ 1??
1. Cha$ers B6/ 6a"er !6/ Ramsay RC/ et alG Relationship bet4een retinal an# lomer"larlesions in IDD6 patieots. Diabetes 3G1/ 12. *rchar# +J/ Dorman J!/ 6aser RE/ et alG Factors associate# 4ith a$oi#ance o% se$erecomplications a%ter 29 yr o% IDD6. Diabetes Care 13G1/ 103. 'ar$in -5-G Impact o% bloo# press"re an# antihypertensi$e treatment on incipient an# o$ertnephropathy/ retinopathy/ an# en#othelial permeability in #iabetes mellit"s. Diabetes Care1G2;0/ 11. Jernel# B/ Al$ere 'G 'rotein"ria an# bloo# l"cose le$els in a pop"lation 4ith #iabeticretinopathy. Am J *phthalmol 10G2?3/ 1?
http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R44-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R43-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R42-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R41-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R40-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R39-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R38-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R37-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R36-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R35-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R34-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R33-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R32-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R31-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R30-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R29-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R28-V3-308/11/2019 Diabetic Retinopathy.doc
23/23
9. 6oensen CE/ ,istr"p J/ Ehlers NG 6icroalb"min"ria pre#icts proli%erati$e #iabeticretinopathy. Lancet 1G1912/ 1?9;. lein R/ lein BE/ 6oss !E/ et alG +he Wisconsin epi#emioloic st"#y o% #iabeticretinopathy. II. 're$alence an# ris o% #iabetic retinopathy 4hen ae is less than 30 years. Arch*phthalmol 102G920/ 1?
. Nelson R/ Wol%e JA/ -orton 6B/ et alG 'roli%erati$e retinopathy in NIDD6. Diabetes3?G39/ 1??. Cr"icshans J/ Ritter LL/ lein R/ et alG +he Association o% 6icroalb"min"ria 4ithDiabetic Retinopathy. *phthalmoloy. 100G?;2/ 13. Fel#man JN/ -irsch !R/ Beyer 66G 're$alence o% #iabetic nephropathy at time o% treatment%or #iabetic retinopathy. In Frie#man EA/ L>Esperance FA/ e#s. Diabetic Renal5Retinal!yn#rome. Ne4 )orG r"ne P !tratton/ 1?2G2090
http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R49-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R48-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R47-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R46-V3-30http://c/Program%20Files/Duane's%20Ophthalmology%20on%20DVD-ROM%202009/ophthalmology/body/01_clinical_ophth/B01222986-DA1-DB3-DC1-C30.html#to-R45-V3-30