Embed Size (px)
Citation preview

Does Education Improve Health?Lessons Learned from Behavior Change
Interventions in Asia, Africa and Latin America
Kirk Dearden
Associate Professor
Department of Health Science
Brigham Young University
March 12, 2004

Organization of Presentation
1. My background
2. Discussion: “What is education?”
3. Discussion: “Does knowledge improve health?” (Group exercise)
4. If “education” doesn’t work, what does?
5. Principles of adult learning (Group exercise)
6. Institutionalizing impact assessment
Background
I’m a mixed breed!• Training in international health (UAB)• Helping improve health through behavior change
and applied research• ICDDR,B• Save the Children US
• SEEP Network• AIMS project
• JPHIEGO• Academy for Educational Development
• Brigham Young University

What is Education?
Where is the Knowledge that is lost in information?
Where is the wisdom that is lost in knowledge?
-- TS Eliot

What is Education?
• In the past, formal education techniques: “We teach the way we were taught”
• Communication was one way from “teacher” to “learner”- Empty Vessel Theory
• Assumption: “If people only knew the correct information, they would perform the correct behavior.” Therefore, giving information is enough.
• Education becomes a one-way mechanism for the transfer of information

Does Knowledge Improve Health?
Group Exercise: Fishes and Boulders
1. Divide into two groups• First group identifies barriers to reducing
Americans’ consumption of meat and fatty foods• What makes it difficult to reduce meat/fat
consumption?
• Second group identifies facilitators for reducing our consumption of meat and fatty foods
• What makes it easy to reduce meat/fat consumption?

Does Knowledge Improve Health?
2. Label boulders (barriers) depending on whether barriers are small, medium or large
3. Do the same for facilitators
4. Place barriers and facilitators in river
5. Two volunteers organize barriers and facilitators according to themes

Does Knowledge Improve Health?
• Knowing ≠ practice– Hygiene (Pinfold, 1999; Stanton et al, 1987; Curtis et al.,
1993)– ORS– HIV/AIDS and consistent condom use (Middlestadt et al.,
1996) Accepting information/adopting new behaviors are complex processes
– In 1601, James Lancaster showed that lemon juice prevents scurvy; 194 years later British Navy adopted policy of providing citrus fruits to all sailors
• Type of info affects whether or not we use it– scientific research less important than subjective
evaluations of near-peers (Rogers, 1995)• Individuals may not practice a behavior if the
innovation is difficult to understand/not “trialable”

Does Knowledge Improve Health?
So…• A lack of information may not be the (only)
challenge to changing behaviors

Stages of Change Model
Pre-awareness
Aware
Contemplation
Intention
Trial
Adoption
Maintenance
Telling others
Persuade
Information
Encourage
Negotiate
Discuss benefits
Support
Praise
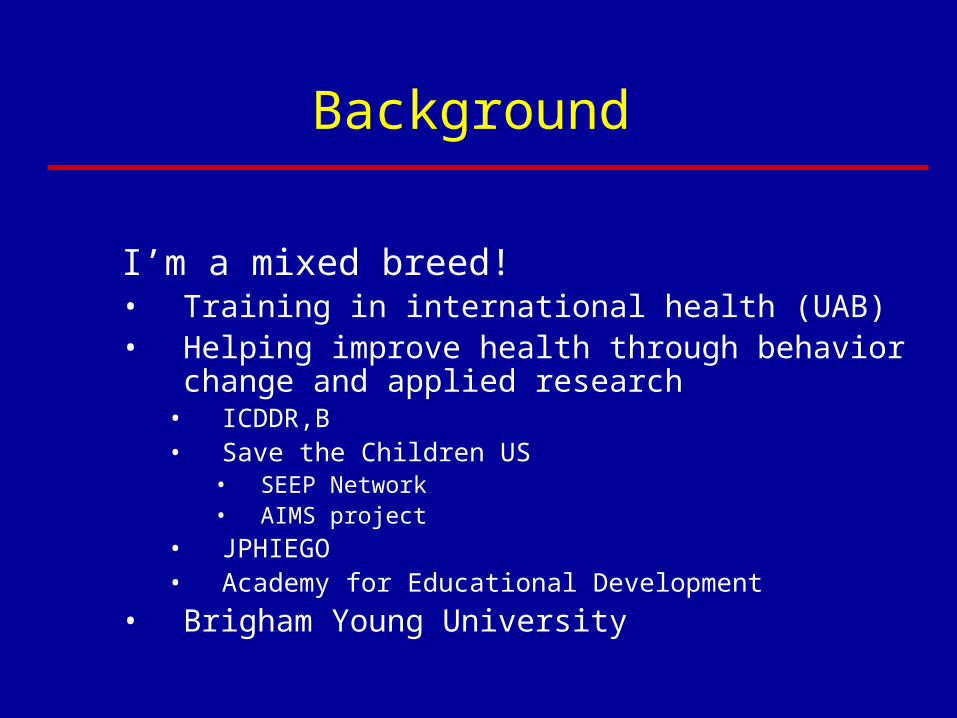
Steps
Pre-awareness
Awareness
Intention
State of individual/ community
Has not heard of the new practice
Has heard of the new practice
Intends to try the new practice
Appropriate Interventions
Provide informationDrama/fairs Community groupsRadioIndividual counselingMother-to-mother support groupsProvide more information and use persuasionGroupsOral and printed wordCounseling cardsMother to mother support groups
Identify benefits and help to overcome obstaclesHome visits; use of visualsGroup work/activities for family/community
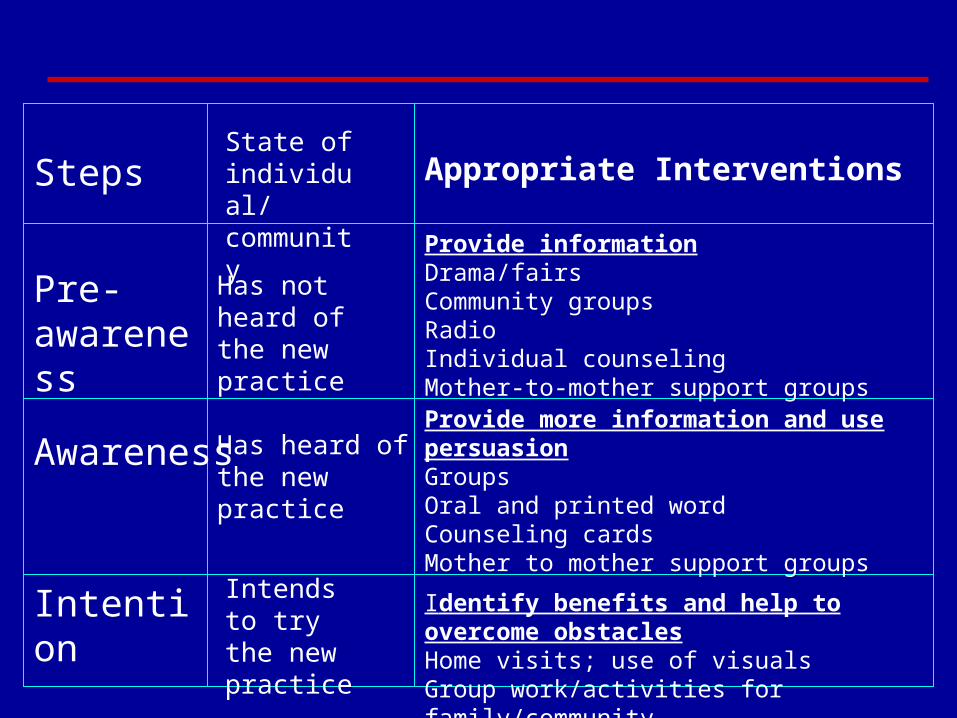
Trial of new practice
Adoption of new practice
Maintenance
Tell others
Tries the new practice to see if there are benefits
Sees the benefits; obstacles are not insurmountable; decides to adopt the new practice
Decides to continue
Believes in the new practice and wants to tell others
Reinforce the benefitsSupport the target mother Convince husband/mother-in-law to support motherCommunity members can provide supportHear messages on the radio
Reinforce the benefitsProvide support at all levelsPraise
Praise; reinforce the benefits; support
Provide situations/networking for sharingPraise; reinforce the benefits; supportfrom others

If “Education” Doesn’t Work, What Does?
No single “right” answer
• Two behavior change strategies that have potential for MED:– Positive Deviance
– Negotiation

What is Positive Deviance (PD)?
• A behavior change strategy based on the uncommon, beneficial behaviors that some community members already practice. Applications:– Rehabilitation of malnourished children– Exclusive breastfeeding– Newborn care– Pregnancy outcomes– Condom use– Commercial sex workers– Conflict resolution

Positive Deviant: Risk vs. Outcome
Outcome Status
Good Not Good
Risk
Status
“Worse Off”PD
“Better Off”

Situation Analysis
• Community Norms (4-6 group discussions with mothers, fathers, mothers-in-law, etc.)
• Positive Deviance Inquiry (4-6 key informant interviews with PD families)

Identifying the PDs: Nutrition Case Study
• Census• Weigh all children < 36 months of age• Categorize them by family income
• So, PDs = well-nourished children from poor families.
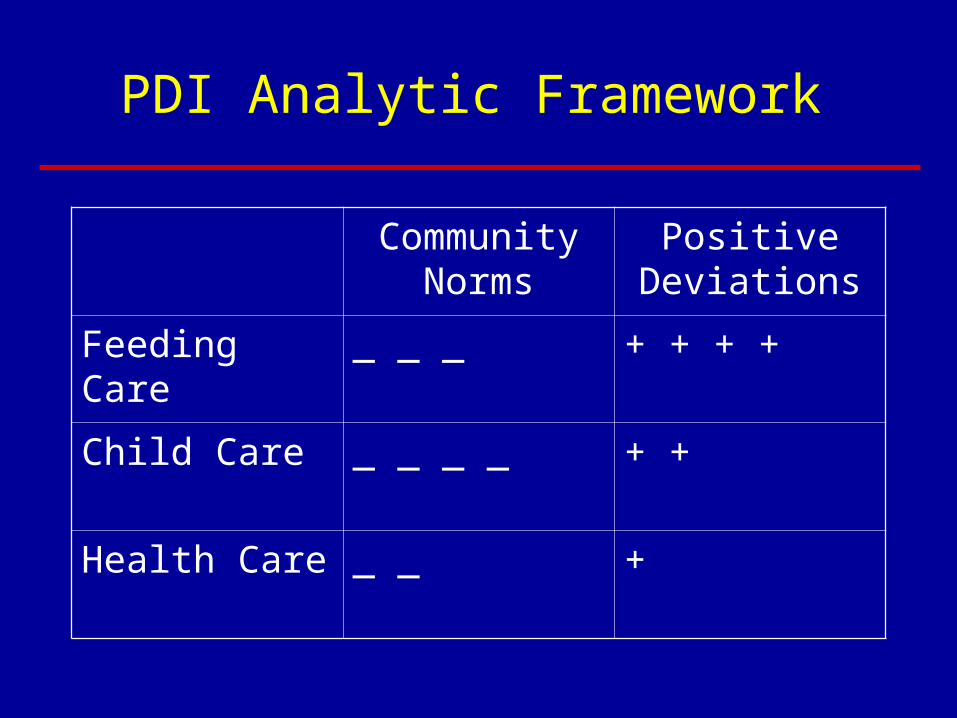
PDI Analytic Framework
Community Norms
Positive Deviations
Feeding Care _ _ _ + + + +
Child Care _ _ _ _ + +
Health Care _ _ +

What is the Impact of PD?
Study on sustainability of PD in Viet Nam conducted by Mackintosh et al. (2002), 3-4 years after SC implemented PD
• Older SC children who participated in PD pgms were better nourished than older control kids
• Younger sibs (never participated in PD pgms) were sig more likely than younger control kids to be better nourished– Also more likely to be fed more often and have hands
washed before meals

What is the Impact of PD?
• Recent results from a prospective, randomized community intervention trial in Viet Nam encouraging but less promising. For example:– No significant impact on growth overall– Younger, more malnourished children benefited in terms of
height (HAZ) and weight (WAZ) compared to younger, malnourished control children
– Magnitude of impacts is consistent with literature of efficacy trials, and better than effectiveness trials

What is Negotiation?
• Based on Trials of Improved Practices (TIPS)
• Focuses on 1-2 priority feeding behaviors that are small and do-able
• Usually occurs in the context of home visits

5 Steps of Negotiation
• ASK mother about the current feeding practices to identify problems
• RECOMMEND options to mother and help her select one she can try
• AGREE on a behavior that the mother will try
• REMIND mother of optimal practice and help her overcome obstacles
• Make an APPOINTMENT for a follow-up visit
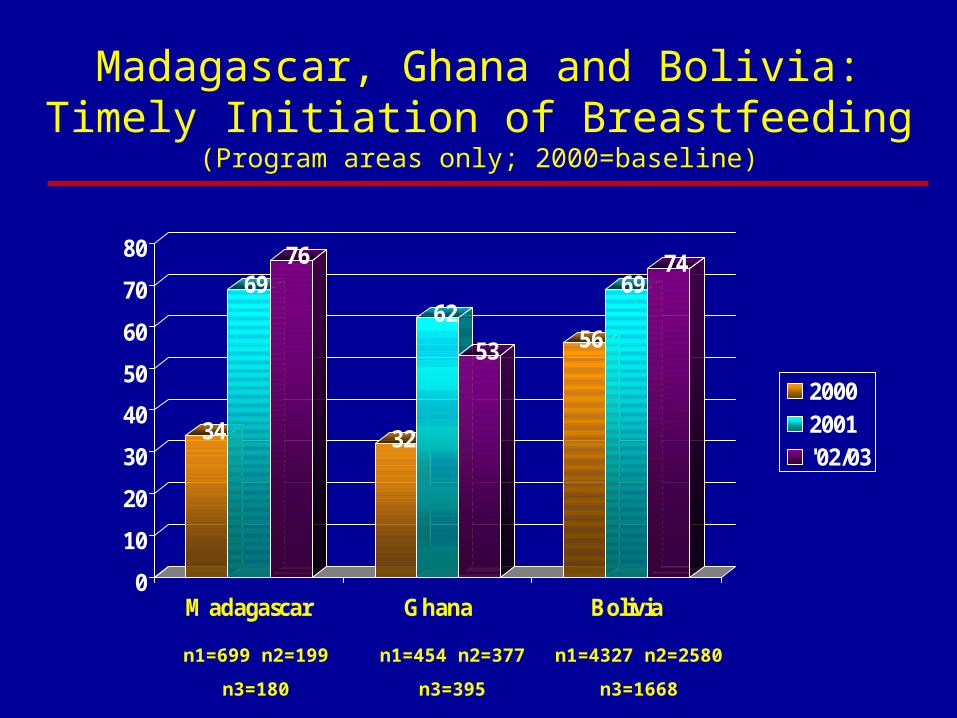
Madagascar, Ghana and Bolivia:Timely Initiation of Breastfeeding
(Program areas only; 2000=baseline)
34
6976
32
62
53 56
6974
0
10
20
30
40
50
60
70
80
Madagascar Ghana Bolivia
20002001'02/03
n1=699 n2=199
n3=180
n1=454 n2=377
n3=395
n1=4327 n2=2580
n3=1668
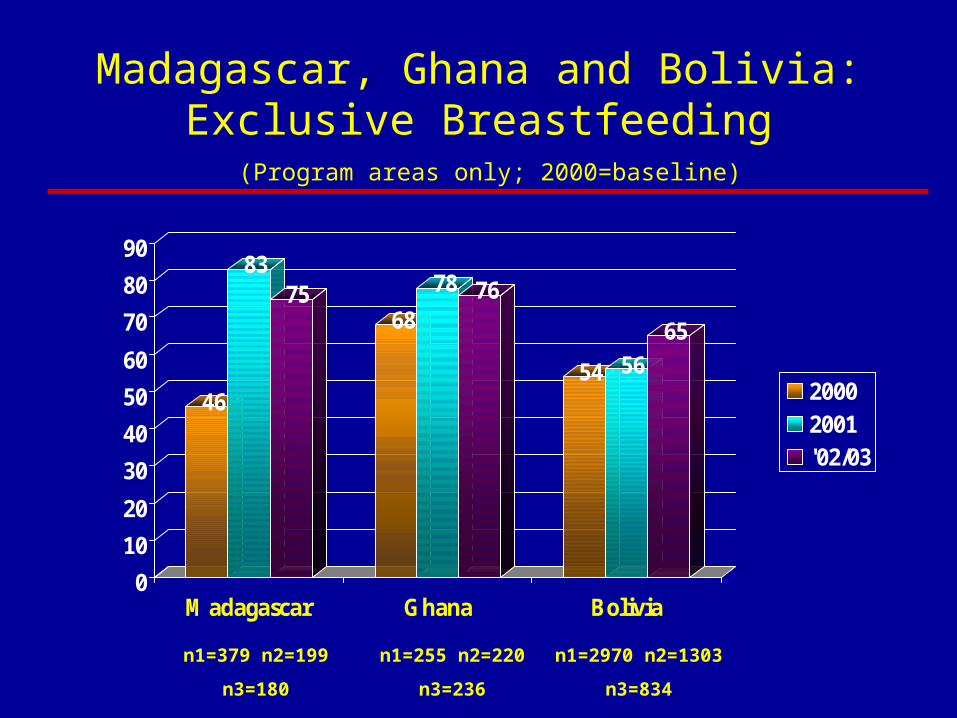
Madagascar, Ghana and Bolivia:Exclusive Breastfeeding
(Program areas only; 2000=baseline)
46
8375
68
78 76
54 56
65
0
10
20
30
40
50
60
70
80
90
Madagascar Ghana Bolivia
20002001'02/03
n1=379 n2=199
n3=180
n1=255 n2=220
n3=236
n1=2970 n2=1303
n3=834
Scale
Ghana Yr 2003 Coverage: > 3 million in 3 northern regions
Madagascar Yr 2002 Coverage: > 6 million in 23 districts
Bolivia Yr 2003 Coverage: 1 million in all 3 eco-regions

Principles of Adult Learning
Group Exercise: 3 Styles of Learning1. Read the description of the 3 distinct learning styles.
Underline what reminds you of yourself.
2. Read the 7 posted signs. Each describes your own preferences or blend of preferences.
3. Stand near the sign that best describes your learning style.
4. We will hear why you made that choice.
5. Analyze your own learning and teaching experiences.

Principles of Adult Learning
We already know that…• Education that revolves around information-sharing
is not likely to change behaviors nor improve health
What else do we know?• The way we teach influences how much others
remember and put into practice what they have learned (visual, auditory, kinesthetic)
– Respect, Affirmation, Relevance, Dialogue, Engagement, Immediacy, and Safety are all key elements of adult learning
• Freedom from Hunger as a model

Principles of Adult Learning
• Successful behavior change requires work at all levels (policy community)
• Scale and sustainability are achieved through partnerships with government and NGOs
• PD can facilitate a community “self-cure” today…(answers come from community) because there are accessible, culturally appropriate, sustainable behaviors already present within the community
• Negotiation eliminates barriers: women see benefits and try new practices– Women need to be supported by families/community
• Community wide saturation ensures a safe environment for new practices
• Using skills-based training ensures quick up-take by field workers

What are the Implications for Organizations Offering Microenterprise Services?
• We may need to re-examine assumptions about whether our educational efforts really change behaviors– Information alone is insufficient– Methods of teaching may be inadequate
• Our behavior change efforts need to be based on a more thorough understanding of why people behave the way they do– Formative research
• Positive Deviance and Negotiation hold considerable promise for changing health and other behaviors (including financial behaviors)

What are the Implications for Organizations Offering Microenterprise Services?
• Give greater attention to rigorous impact assessments that evaluate financial and social outcomes of microenterprise services
• What to evaluate (Habicht et al. 1999)?– Provision or utilization of services– Coverage – Impact
• Impact=effectiveness x sustainability x coverage– Cost (High Impact PVO Conference 1998)
• Focus on core principles of development work– Including gender equity

Impact Assessment
• Adequacy: did project meet criteria?– No control group
• Plausibility: program effect beyond external forces?– Control groups
• Probability: did program have an effect?– Randomization of Rx/Control
We need more:• Small operations research studies• Efficacy and effectiveness trials• Studies that truly incorporate quantitative/qualitative methods
– PLA/PRA to involve community members in all stages of the evaluation