Embed Size (px)
Citation preview
What’s new?
C More accurate assessment of left ventricular function is feasible
with 3D-TTE.
C Guidance by 3D TOE is increasingly required for percutaneous
INVESTIGATIONS
EchocardiographyMatthias Paul
Lindsay Smith
Mark Monaghan
(non-coronary) cardiac interventions (e.g. PFO-/ASD-closure,
trans-catheter aortic valve implantation).
AbstractEchocardiography e the investigation of the heart with ultrasound e is
the most frequently used cardiac imaging modality. Transthoracic echo-
cardiography is a powerful tool to evaluate the structure and function of
the heart. Further evaluation is possible with transoesophageal echocar-
diography. However, its higher resolution and image quality are accom-
panied by a small risk of complications. Stress echocardiography allows
identification of patients with significant coronary artery disease with
high sensitivity and specificity. The aim of this article is to outline the
information that echocardiography can provide and the clinical situa-
tions where it is indicated. Further advanced applications such as
contrast and three-dimensional echocardiography will also be
discussed.
Keywords contrast echocardiography; coronary artery disease; Doppler;
echocardiography; heart valve diseases; stress; three-dimensional;
transoesophageal; ventricular function
Echocardiography provides a wealth of information, and impor-
tantly, is a non-invasive technique which does not involve
radiation and is readily available at the bedside.
Basic ultrasound physics
Ultrasound waves transmitted into the body travel with
a distinct velocity and are reflected at interfaces between tissues
of different density (e.g. blood and myocardium). The time
these echoes require to return to the transducer is analyzed and
a two- or even three-dimensional image of a cross-section of the
heart can be generated. Ultrasound waves reflected by moving
structures such as red blood cells and myocardium cause
a frequency shift of the ultrasound (¼Doppler effect). This is
the basis of Doppler-echocardiography (colour, continuous and
pulsed-wave Doppler), which enables accurate
measurements of blood flow and myocardial tissue velocities
(Figures 1e3).
Matthias Paul MD is a Clinical Fellow of Cardiology at King’s College
Hospital, London, UK. Competing interests: none.
Lindsay Smith MD MRCP is a Research Fellow in Cardiology, King’s
College Hospital, London, UK. Competing interests: none.
Mark Monaghan PhD FRCP(Hon) FACC FESC is Director of Non-Invasive
Cardiology at King’s College Hospital, London, UK. Competing
interests: none.
MEDICINE 38:7 371
Transthoracic echocardiography (TTE)
A transthoracic study is usually performed by an experienced
sonographer or a trained doctor and takes approximately 40 min
for a full study. Optimal positioning of the patient is important
since the bony thorax and the lungs represent obstacles to the
ultrasound. While the patient is resting comfortably on his left
side, a set of standard views is acquired from the left parasternal,
apical, subcostal and suprasternal positions. Rotation and
angulation of the transducer enable different planes of the heart
to be visualized from a single position.
Left ventricular function
The commonest reason for requesting a TTE is evaluation of left
ventricular function. By scanning the left ventricle from different
views global systolic function can be qualitatively described as
normal, mildly, moderately and severely impaired. In order to
assess systolic function quantitatively, left ventricular area is
measured in two planes at end-systole and end-diastole, and
volumes and ejection fraction derived by applying Simpson’s
method. However, absolute numbers must be used carefully, as
the method is based on a number of assumptions. 3D echocar-
diography is more accurate and reproducible1,2 and may be
considered in patients where serial comparison is necessary (e.g.
during potentially cardiotoxic chemotherapy or in patients where
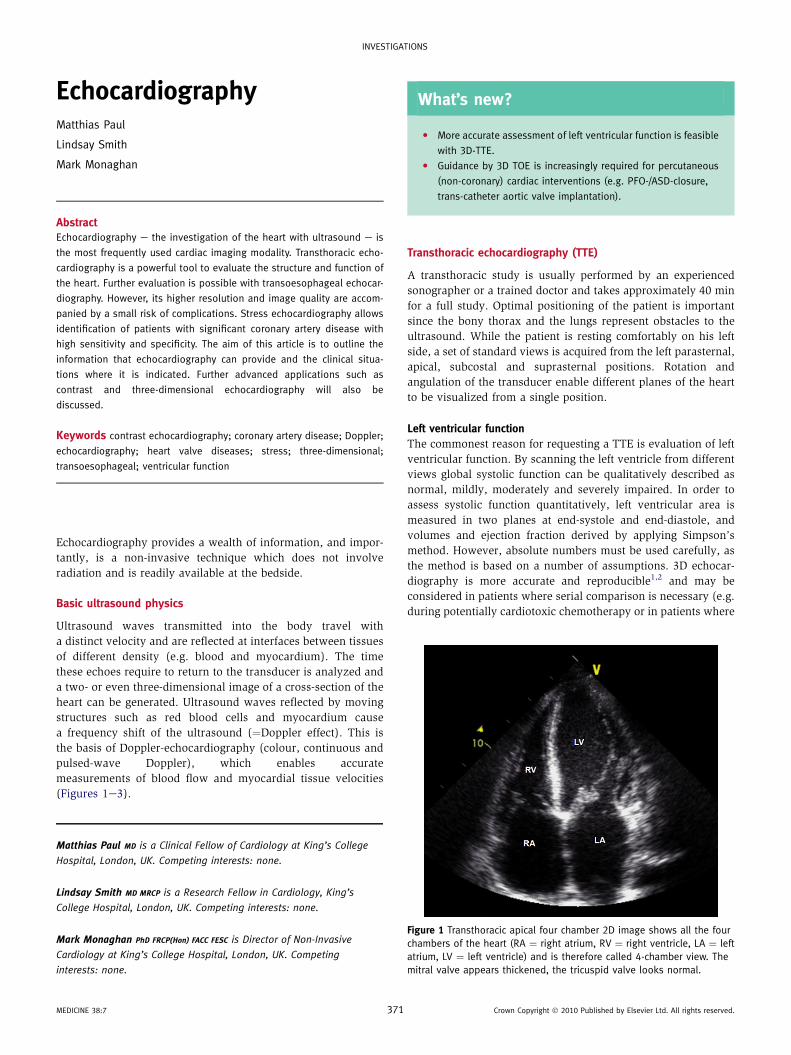
Figure 1 Transthoracic apical four chamber 2D image shows all the four
chambers of the heart (RA ¼ right atrium, RV ¼ right ventricle, LA ¼ left
atrium, LV ¼ left ventricle) and is therefore called 4-chamber view. The
mitral valve appears thickened, the tricuspid valve looks normal.
Crown Copyright � 2010 Published by Elsevier Ltd. All rights reserved.
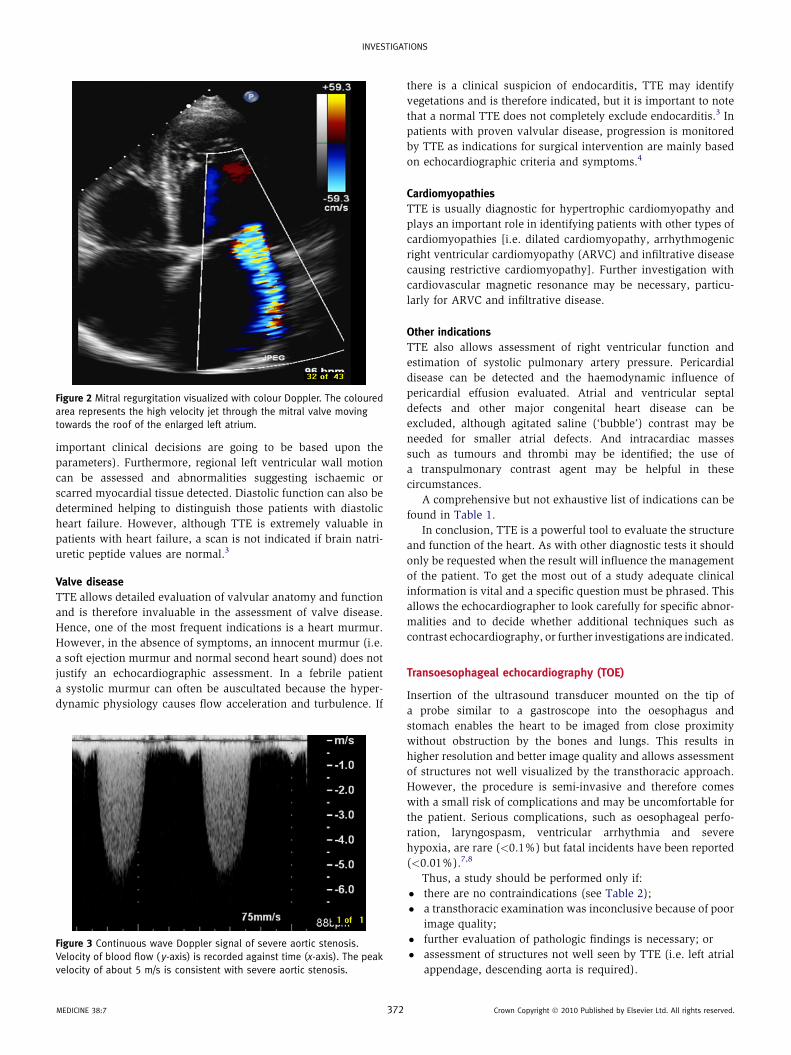
Figure 2 Mitral regurgitation visualized with colour Doppler. The coloured
area represents the high velocity jet through the mitral valve moving
towards the roof of the enlarged left atrium.
INVESTIGATIONS
important clinical decisions are going to be based upon the
parameters). Furthermore, regional left ventricular wall motion
can be assessed and abnormalities suggesting ischaemic or
scarred myocardial tissue detected. Diastolic function can also be
determined helping to distinguish those patients with diastolic
heart failure. However, although TTE is extremely valuable in
patients with heart failure, a scan is not indicated if brain natri-
uretic peptide values are normal.3
Valve disease
TTE allows detailed evaluation of valvular anatomy and function
and is therefore invaluable in the assessment of valve disease.
Hence, one of the most frequent indications is a heart murmur.
However, in the absence of symptoms, an innocent murmur (i.e.
a soft ejection murmur and normal second heart sound) does not
justify an echocardiographic assessment. In a febrile patient
a systolic murmur can often be auscultated because the hyper-
dynamic physiology causes flow acceleration and turbulence. If
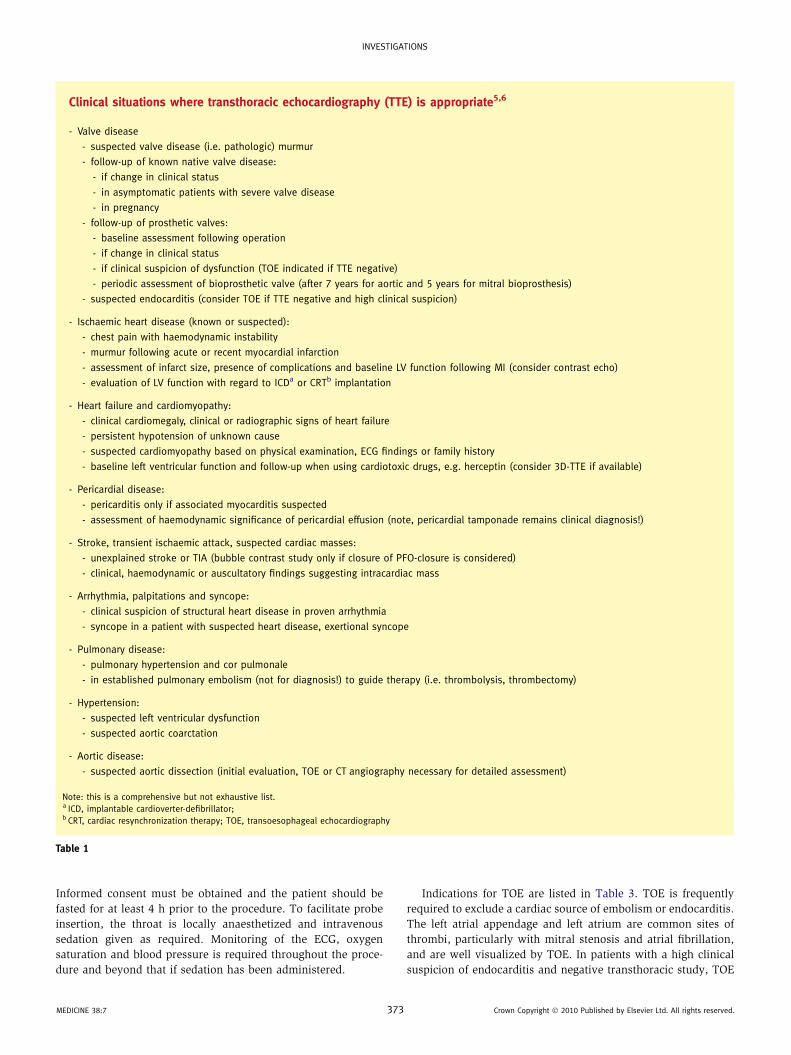
Figure 3 Continuous wave Doppler signal of severe aortic stenosis.
Velocity of blood flow ( y-axis) is recorded against time (x-axis). The peak
velocity of about 5 m/s is consistent with severe aortic stenosis.
MEDICINE 38:7 372
there is a clinical suspicion of endocarditis, TTE may identify
vegetations and is therefore indicated, but it is important to note
that a normal TTE does not completely exclude endocarditis.3 In
patients with proven valvular disease, progression is monitored
by TTE as indications for surgical intervention are mainly based
on echocardiographic criteria and symptoms.4
Cardiomyopathies
TTE is usually diagnostic for hypertrophic cardiomyopathy and
plays an important role in identifying patients with other types of
cardiomyopathies [i.e. dilated cardiomyopathy, arrhythmogenic
right ventricular cardiomyopathy (ARVC) and infiltrative disease
causing restrictive cardiomyopathy]. Further investigation with
cardiovascular magnetic resonance may be necessary, particu-
larly for ARVC and infiltrative disease.
Other indications
TTE also allows assessment of right ventricular function and
estimation of systolic pulmonary artery pressure. Pericardial
disease can be detected and the haemodynamic influence of
pericardial effusion evaluated. Atrial and ventricular septal
defects and other major congenital heart disease can be
excluded, although agitated saline (‘bubble’) contrast may be
needed for smaller atrial defects. And intracardiac masses
such as tumours and thrombi may be identified; the use of
a transpulmonary contrast agent may be helpful in these
circumstances.
A comprehensive but not exhaustive list of indications can be
found in Table 1.
In conclusion, TTE is a powerful tool to evaluate the structure
and function of the heart. As with other diagnostic tests it should
only be requested when the result will influence the management
of the patient. To get the most out of a study adequate clinical
information is vital and a specific question must be phrased. This
allows the echocardiographer to look carefully for specific abnor-
malities and to decide whether additional techniques such as
contrast echocardiography, or further investigations are indicated.
Transoesophageal echocardiography (TOE)
Insertion of the ultrasound transducer mounted on the tip of
a probe similar to a gastroscope into the oesophagus and
stomach enables the heart to be imaged from close proximity
without obstruction by the bones and lungs. This results in
higher resolution and better image quality and allows assessment
of structures not well visualized by the transthoracic approach.
However, the procedure is semi-invasive and therefore comes
with a small risk of complications and may be uncomfortable for
the patient. Serious complications, such as oesophageal perfo-
ration, laryngospasm, ventricular arrhythmia and severe
hypoxia, are rare (<0.1%) but fatal incidents have been reported
(<0.01%).7,8
Thus, a study should be performed only if:
� there are no contraindications (see Table 2);
� a transthoracic examination was inconclusive because of poor
image quality;
� further evaluation of pathologic findings is necessary; or
� assessment of structures not well seen by TTE (i.e. left atrial
appendage, descending aorta is required).
Crown Copyright � 2010 Published by Elsevier Ltd. All rights reserved.
Clinical situations where transthoracic echocardiography (TTE) is appropriate5,6
- Valve disease
- suspected valve disease (i.e. pathologic) murmur
- follow-up of known native valve disease:
- if change in clinical status
- in asymptomatic patients with severe valve disease
- in pregnancy
- follow-up of prosthetic valves:
- baseline assessment following operation
- if change in clinical status
- if clinical suspicion of dysfunction (TOE indicated if TTE negative)
- periodic assessment of bioprosthetic valve (after 7 years for aortic and 5 years for mitral bioprosthesis)
- suspected endocarditis (consider TOE if TTE negative and high clinical suspicion)
- Ischaemic heart disease (known or suspected):
- chest pain with haemodynamic instability
- murmur following acute or recent myocardial infarction
- assessment of infarct size, presence of complications and baseline LV function following MI (consider contrast echo)
- evaluation of LV function with regard to ICDa or CRTb implantation
- Heart failure and cardiomyopathy:
- clinical cardiomegaly, clinical or radiographic signs of heart failure
- persistent hypotension of unknown cause
- suspected cardiomyopathy based on physical examination, ECG findings or family history
- baseline left ventricular function and follow-up when using cardiotoxic drugs, e.g. herceptin (consider 3D-TTE if available)
- Pericardial disease:
- pericarditis only if associated myocarditis suspected
- assessment of haemodynamic significance of pericardial effusion (note, pericardial tamponade remains clinical diagnosis!)
- Stroke, transient ischaemic attack, suspected cardiac masses:
- unexplained stroke or TIA (bubble contrast study only if closure of PFO-closure is considered)
- clinical, haemodynamic or auscultatory findings suggesting intracardiac mass
- Arrhythmia, palpitations and syncope:
- clinical suspicion of structural heart disease in proven arrhythmia
- syncope in a patient with suspected heart disease, exertional syncope
- Pulmonary disease:
- pulmonary hypertension and cor pulmonale
- in established pulmonary embolism (not for diagnosis!) to guide therapy (i.e. thrombolysis, thrombectomy)
- Hypertension:
- suspected left ventricular dysfunction
- suspected aortic coarctation
- Aortic disease:
- suspected aortic dissection (initial evaluation, TOE or CT angiography necessary for detailed assessment)
Note: this is a comprehensive but not exhaustive list.a ICD, implantable cardioverter-defibrillator;b CRT, cardiac resynchronization therapy; TOE, transoesophageal echocardiography
Table 1
INVESTIGATIONS
Informed consent must be obtained and the patient should be
fasted for at least 4 h prior to the procedure. To facilitate probe
insertion, the throat is locally anaesthetized and intravenous
sedation given as required. Monitoring of the ECG, oxygen
saturation and blood pressure is required throughout the proce-
dure and beyond that if sedation has been administered.
MEDICINE 38:7 373
Indications for TOE are listed in Table 3. TOE is frequently
required to exclude a cardiac source of embolism or endocarditis.
The left atrial appendage and left atrium are common sites of
thrombi, particularly with mitral stenosis and atrial fibrillation,
and are well visualized by TOE. In patients with a high clinical
suspicion of endocarditis and negative transthoracic study, TOE
Crown Copyright � 2010 Published by Elsevier Ltd. All rights reserved.
Contraindications for transoesophageal echocardiography
Absolute Oesophageal or pharyngeal obstruction or trauma
Gastrointestinal bleeding
Instability of cervical vertebrae
Uncooperative patient
Relative Oesophageal varices or diverticula
Cervical arthritis
Oropharyngeal distortion
Bleeding diathesis or overanticoagulation
Table 2
INVESTIGATIONS
allows smaller vegetations (1e2 mm) to be seen. TOE also has an
important role in assessing mitral valve disease to guide inter-
vention (valvuloplasty) and surgery (mitral valve repair versus
replacement). Finally, it allows assessment of the ascending
aorta, arch and descending aorta in cases of suspected dissection
and aneurysm.
Stress echocardiography
Stress echocardiography allows identification of patients with
significant coronary artery disease with high sensitivity and
specificity. Diagnostic accuracy is higher compared to conven-
tional exercise stress testing and similar to radionuclide stress
perfusion imaging.9 Stress can be achieved either by physical
exercise (treadmill or bicycle) or pharmacologically with dobut-
amine. Regional wall motion (thickening and excursion) is
assessed at rest and during stress. New regional wall motion
abnormalities or worsening of pre-existing ones suggest revers-
ible ischaemia indicating flow-limiting narrowing of coronary
Clinical situations where transoesophageal echocardi-ography is most appropriate (in general only after priortransthoracic echocardiography)6
Cardiac source of embolism (thrombus, tumour, PFO)
Infective endocarditis
C small vegetations (1e2 mm)
C complications (abscess, valve perforation)
Aortic pathology (dissection, aneurysm, atheroma)
Mitral valve disease
C to determine suitability for balloon valvuloplasty in mitral
stenosis or repair in regurgitation
Prosthetic valve evaluation (particularly mitral valve prosthesis)
Septal defects (particularly ASD and PFO)
Intra- and perioperative monitoring
Congenital heart disease
Guidance of percutaneous (non-coronary) cardiac interventions
Note: this is a comprehensive but not exhaustive list. PFO, patent foramen
ovale; ASD, atrial septal defect.
Table 3
MEDICINE 38:7 374
arteries. Thus, stress echocardiography not only reveals signifi-
cant coronary artery disease but can also identify the affected
coronary territory and guide intervention.
As inotropic stress is required for both exercise and dobut-
amine stress echo, beta-blockers must be omitted 48e72 h before
the stress test in order to achieve significant stress and to
improve sensitivity.
Furthermore, stress echocardiography is used to determine if
there is viable myocardium after myocardial infarction, which
would potentially benefit from revascularization.
Contrast echocardiography
Use of contrast in echocardiography can improve image quality
markedly and allow detection of concealed abnormalities.
The simplest form of contrast can be produced manually by
agitating saline between two syringes connected to a three-way
tap. The air bubbles produced opacify the right side of the
heart but are too large to pass through the pulmonary capillaries.
Thus, any bubbles appearing on the left side of the heart indicate
a shunt, usually an atrial septal defect (ASD) or a patent foramen
ovale (PFO). Bubble contrast TTE is frequently used after
a stroke or transient ischaemic attack (TIA) since a PFO may
represent a gateway for emboli from the venous system to the
brain. However, this test should only be requested if PFO closure
is to be considered (Figure 4).
Commercially produced contrast agents are available and
consist of high-molecular weight gas filled microbubbles
approximately the size of red blood cells which are therefore able
to cross the pulmonary capillaries. These enhance endocardial
border definition of both ventricles and can reveal intraventric-
ular thrombus and apical hypertrophy. Furthermore, trans-
pulmonary contrast agents are widely used in stress
echocardiography when image quality is suboptimal or to assess
myocardial perfusion.10e12
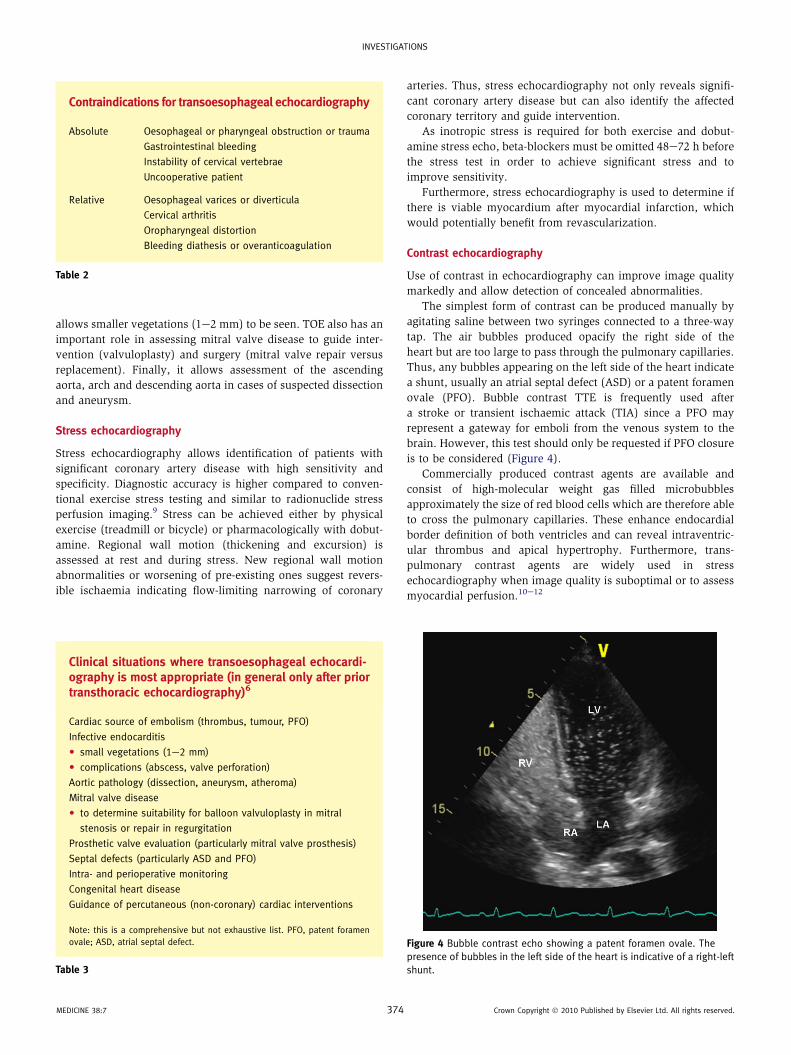
Figure 4 Bubble contrast echo showing a patent foramen ovale. The
presence of bubbles in the left side of the heart is indicative of a right-left
shunt.
Crown Copyright � 2010 Published by Elsevier Ltd. All rights reserved.
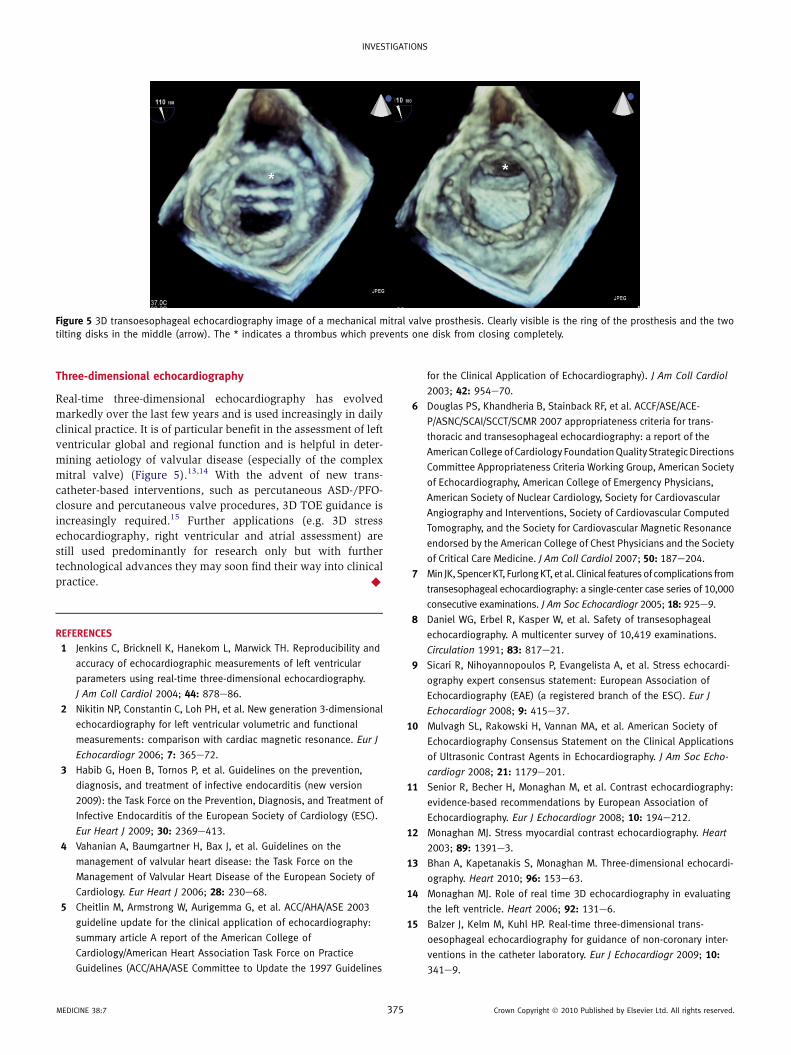
Figure 5 3D transoesophageal echocardiography image of a mechanical mitral valve prosthesis. Clearly visible is the ring of the prosthesis and the two
tilting disks in the middle (arrow). The * indicates a thrombus which prevents one disk from closing completely.
INVESTIGATIONS
Three-dimensional echocardiography
Real-time three-dimensional echocardiography has evolved
markedly over the last few years and is used increasingly in daily
clinical practice. It is of particular benefit in the assessment of left
ventricular global and regional function and is helpful in deter-
mining aetiology of valvular disease (especially of the complex
mitral valve) (Figure 5).13,14 With the advent of new trans-
catheter-based interventions, such as percutaneous ASD-/PFO-
closure and percutaneous valve procedures, 3D TOE guidance is
increasingly required.15 Further applications (e.g. 3D stress
echocardiography, right ventricular and atrial assessment) are
still used predominantly for research only but with further
technological advances they may soon find their way into clinical
practice. A
REFERENCES
1 Jenkins C, Bricknell K, Hanekom L, Marwick TH. Reproducibility and
accuracy of echocardiographic measurements of left ventricular
parameters using real-time three-dimensional echocardiography.
J Am Coll Cardiol 2004; 44: 878e86.
2 Nikitin NP, Constantin C, Loh PH, et al. New generation 3-dimensional
echocardiography for left ventricular volumetric and functional
measurements: comparison with cardiac magnetic resonance. Eur J
Echocardiogr 2006; 7: 365e72.
3 Habib G, Hoen B, Tornos P, et al. Guidelines on the prevention,
diagnosis, and treatment of infective endocarditis (new version
2009): the Task Force on the Prevention, Diagnosis, and Treatment of
Infective Endocarditis of the European Society of Cardiology (ESC).
Eur Heart J 2009; 30: 2369e413.
4 Vahanian A, Baumgartner H, Bax J, et al. Guidelines on the
management of valvular heart disease: the Task Force on the
Management of Valvular Heart Disease of the European Society of
Cardiology. Eur Heart J 2006; 28: 230e68.
5 Cheitlin M, Armstrong W, Aurigemma G, et al. ACC/AHA/ASE 2003
guideline update for the clinical application of echocardiography:
summary article A report of the American College of
Cardiology/American Heart Association Task Force on Practice
Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines
MEDICINE 38:7 375
for the Clinical Application of Echocardiography). J Am Coll Cardiol
2003; 42: 954e70.
6 Douglas PS, Khandheria B, Stainback RF, et al. ACCF/ASE/ACE-
P/ASNC/SCAI/SCCT/SCMR 2007 appropriateness criteria for trans-
thoracic and transesophageal echocardiography: a report of the
AmericanCollegeof Cardiology FoundationQuality StrategicDirections
Committee Appropriateness Criteria Working Group, American Society
of Echocardiography, American College of Emergency Physicians,
American Society of Nuclear Cardiology, Society for Cardiovascular
Angiography and Interventions, Society of Cardiovascular Computed
Tomography, and the Society for Cardiovascular Magnetic Resonance
endorsed by the American College of Chest Physicians and the Society
of Critical Care Medicine. J Am Coll Cardiol 2007; 50: 187e204.
7 Min JK,SpencerKT, FurlongKT, et al. Clinical featuresof complications from
transesophageal echocardiography: a single-center case series of 10,000
consecutive examinations. J Am Soc Echocardiogr 2005; 18: 925e9.
8 Daniel WG, Erbel R, Kasper W, et al. Safety of transesophageal
echocardiography. A multicenter survey of 10,419 examinations.
Circulation 1991; 83: 817e21.
9 Sicari R, Nihoyannopoulos P, Evangelista A, et al. Stress echocardi-
ography expert consensus statement: European Association of
Echocardiography (EAE) (a registered branch of the ESC). Eur J
Echocardiogr 2008; 9: 415e37.
10 Mulvagh SL, Rakowski H, Vannan MA, et al. American Society of
Echocardiography Consensus Statement on the Clinical Applications
of Ultrasonic Contrast Agents in Echocardiography. J Am Soc Echo-
cardiogr 2008; 21: 1179e201.
11 Senior R, Becher H, Monaghan M, et al. Contrast echocardiography:
evidence-based recommendations by European Association of
Echocardiography. Eur J Echocardiogr 2008; 10: 194e212.
12 Monaghan MJ. Stress myocardial contrast echocardiography. Heart
2003; 89: 1391e3.
13 Bhan A, Kapetanakis S, Monaghan M. Three-dimensional echocardi-
ography. Heart 2010; 96: 153e63.
14 Monaghan MJ. Role of real time 3D echocardiography in evaluating
the left ventricle. Heart 2006; 92: 131e6.
15 Balzer J, Kelm M, Kuhl HP. Real-time three-dimensional trans-
oesophageal echocardiography for guidance of non-coronary inter-
ventions in the catheter laboratory. Eur J Echocardiogr 2009; 10:
341e9.
Crown Copyright � 2010 Published by Elsevier Ltd. All rights reserved.




























