Embed Size (px)
Citation preview

Journal of Gastroenterology and Hepatology (1995) 10, 198-204
LIVER A N D BILIARY
Effects of nifedipine on hepatic venous pressure gradient and portal vein blood flow in patients with cirrhosis
KAZUHIRO OTA, HIROSHI SHIJO, HIROSHI KOKAWA, KATSUHIKO KUBARA, TETSUHIRO KIM, NOBUO AKIYOSHI, MASANORI YOKOYAMA AND MAKOTO OKUMURA
The First Department of Internal Medicine, School of Medicine, Fukuoka University, Fukuoka, Japan
Abstract We investigated the effects of nifedipine on splanchnic haemodynamics in 13 patients with cirrhosis and portal hypertension, and in 10 control subjects using hepatic venous catheterization and pulsed Doppler ultrasound. There were no significant changes in systemic or splanchnic haemodynamics in control patients. In contrast, systemic vasodilatation, evidenced by significant decreases in mean arterial pressure and systemic vascular resistance, was observed in patients 20 min after subllngual application of 10 mg nifedipine. Moreover, hepatic venous pressure gradient and portal vein blood flow significantly increased after nifedipine administration. There was a significant correlation between the percentage increases in portal vein blood flow and in hepatic venous pressure gradient. However, no correlation was found between the percentage change in cardiac output and that in portal vein blood flow. Thus the increase in portal vein blood flow appears to be related to splanchnic arterial vasodilatation by nifedipine. Consequently, nifedipine has deleterious effects on portal haemodynamics in patients with cirrhosis. As nifedipine may potentially increase the risk of variceal haemorrhage in patients with less advanced varices, this drug should be used with caution in patients with chronic liver disease.
Key words hepatic hernodynamics, liver cirrhosis, nifedipine, portal vein blood flow.
INTRODUCTION
Oesophageal variceal bleeding secondapy to portal hyper- tension is life-threatening in patients with cirrhosis of the liver. Prevention of variceal rebleeding is based mainly on endoscopic sclerotherapy' and pharmaadogic trea~nent.21~ Long-term oral beta-adrenergic antagonists and nitrates is the accepted therapy for preventing first or subsequent bleeding episode^.^^^ However, propranolol therapy reduces the fmal hepatic venous pressure gradient (HVPG) to 5 12 mmHg in only 12% of patients and nearly 40% show no reduction in HVPG.435 While nitrates are effective in acute situations, tolerance leading to refractoriness develops over the long-term. Moreover, recent investigations have demonstrated that nitrates decrease rend blood flow6 and impair oxygen uptake, resulting in tissue hyporria in patients with cirrhosis of the liver.'
Experimental studies have shown that calcium-channel blockers decrease intrahepatic resistance.* Potentially, calcium-channel blockers may decrease the HVPG in
patients with cirrhosis. However, the results of clinical mals of calcium-channel blockers for portal hypertension have been inconclu~ive.~~~ Carefully designed studies using verapamilg and nicardipine" demonstrated a lack of bene- ficial effects on portal pressure. To date, there are only a few studies concerning the effects of nifedipine on portal haemodynamics and the results are controver~ial."-'~ Therefore, we investigated the effects of nifedipine on portal haemodynamics in patients with cirrhosis of the liver.
SUBJECTS AND METHODS
Patients
The clinical Characteristics of the study patients with cirrhosis are shown in Table 1. There were 16 men and 7 women, aged 43-71 (60*8) years. All had histologically proven cirrhosis of the liver. The cause of the cirrhosis was related to hepatitis B v i rus in five, hepatitis C virus
Correspondence: Hiroshi Shijo, The First Department of Internal Medicine, School of Medicine, Fukuoka University, 45-
This study was presented in part at the 9th Biennial Sciendfic Meeting of The Asian Pacific Association for the Study of
Accepted for publication 4 July 1994.
1, 'I-chome Nanakuma, Jonan-ku, Fukuoka 814-01, Japan.
the Liver, Kuala Lumpur, 27-29 January, 1994.

K. Ota et al. 199
Table 1 Clinical and biochemical data in the patients studied
Control Nifedipine ~ ~~
Sex (malelfemale) Age Atiology of cirrhosis
Hepatitis B virus Hepatitis C virus Primary biliary
cirrhosis Bilirubin (pnoVL) Albumin (g/L) Prothrombin rate (96)
classification (A/B) Child-Pugh
7/3 60*8
2 8
0 1 4 i 7 34i5 72 f 18
8/2
9/4 58 f 8
3 9
1 19f9 35 f 6 74 f 14
914
in 17 and primary biliary cirrhosis in one. Thus, all our patients had non-alcoholic cirrhosis. Severity of liver damage was graded according to the modified Child-Pugh ClassifiCati~n:'~ 17 patients were classitied as grade A and six as grade B. Oesophageal varices were found by endoscopic examination in all patients. None of the patients had a history of bleeding varices or prior surgical treatment for portal hypertension, and none had received vasoactive drugs such as beta-blockers or nitrates. All patients were informed of the scientific nature of the investigation and written consent was obtained. A group of 10 patients who were receiving placebo were used as controls. There were no significant difierences in clinical or biochemical data or hepatic function between control patients and those receiving nifedipine. The study protocol was approved by the Hospital Ethics Committee.
Haemodynamic measurement
Under local anaesthesia, a vessel dilator with a poly- propylene sheath was introduced into the lumen of the right femoral vein. A 7-F balloon-wedge pressure catheter (Goodtec Inc., Huntington Beach, CAY USA) was introduced into the right main hepatic vein and the hepatic venous wedge pressure and free-positioned pressure were measured. The correct wedge position of the catheter was confirmed with contrast medium. A Swan-Ganz catheter (Baxter Healthcare Inc., Irvine, CAY USA) was inserted into the pulmonary arterial trunk under fluoroscopic monitoring. The right atrial, pulmonary arterial and pul- monary wedge pressures were measured. All pressures were recorded with a multichannel recorder (Polygraph EP 1102, NEC San-Ai Inc., Tokyo, Japan), and pressure measurements were performed in triplicate on each patient. cardiac output (CO) was determined by the t h e d i l u t i o n method. During the procedure, arterial pressure was measured by an external sphygmomanometer (Dinamap, critikon. Inc., Tampa, FLY USA) and heart rate was determined by continuous elecuocardiogram monitoring. Haemodynamic calculations were performed according to the formulae below: Mean arterial pressure (MAP)(mmHg) = (systolic +
2 -diastoliC)/3
Systemic vascular resistance (SVR)(dyne-s.~m-~) = (MAP - right amal pressure).8O/CO
Pulmonary vascular resistance (dyne a s acm-') = (mean pulmonary arterial pressure - pulmonary capluary
wedge pressure).8O/CO HVPG (mmHg) = hepatic venous wedge pressure -
free hepatic venous pressure The cross-sectional area and blood flow of the portal
vein were measured using an ultrasonic duplex system composed of a real-time electronic B-mode scauner and a pulsed Doppler flow meter (SSA 270A/SDL-01AY Toshiba Corp., Tokyo, Japan). We used sector type probe for B-mode and pulsed Doppler scanning with a 5 mm of sample volume. The sample point was set at the portal vein trunk near the porta hepatis distal to the left gasmc vein. Flow velocity was calculated directly by the apparatus using the following formula.
v = F d C/wO 'COS(Y
where F d is the Doppler shift frequency, c is the velocity of ultrasound in tissues (1500 m/s) , Fo is the emitted ultrasonic wave frequency and (I is the angle approach between the ultrasonic beam and the longitudinal axis of the vessel. All measurements were performed with (Y being 55-60O. The 'mean velocity of flow' (Vmm) in this study was calculated directly by the apparatus. The flow volume (F) was calculated by the following formula:
F = V,,, - m2 40 (mL/min) where t represents the halfdiameter of the vessel. Patients were studied by one of the authors (K.O.), who obtained three consecutive measurements of flow velocity and vessel diameter from each patient. During the Doppler study, the operator was blinded to other haemodynamic variables and the kind of medication. The mean coefficient of vari- ation of portal flow was 9.4 f 3.0%. The specifications and methods of measurement have been described previously.15 The portal vascular resistance was calculated according to the modified equation of Moriyasu et al. l6 as follows: Portal vascular resistance = (WHVP - FHVP)/portal blood
flowhdyweight (mmHg -mL-l emin e k g )
Hepatic blood flow and indocyanine green clearance
The hepatic blood flow was estimated by the continuous indocyanine green (ICG) infusion method." In brief, after a single infusion of 25 mg of ICG, a constant infusion was started at the rate of 0.2 mg/min. After an equilibrium period of 40 min, four sets of blood samples were drawn from peripheral vein and hepatic vein over a 10 min period. Steady ICG levels and extraction above 0.1 were required for the calculation of hepatic blood flow. The intrinsic hepatic clearance of ICG was calculated according to the sinusoidal model. lo
Blood gas measurements
Heparinized arterial and mixcd venous blood samples were simultaneously withdrawn for immediate measurements of

200 Nifdiipine and hepatic haemodyMmics
Table 2 EEects of nifedipine on systemic haemodynamics in patients with cirrhosis
Mean arterial pressure ( d g ) Heart rate (beats/&)
Systemic vascular resistance (dyne - s - Cm') Right atrial pressure ( d g ) Pulmonary arterial pressure (mmHg) Pulmonary capillary wedge pressure (mmHg) Pulmonary vascular resistance (dyne * s Cms 1
cardiac output (L/&)
Control Baseline
94f 11 71 f 9 5.5 f 1.6 1337 f 403 7.6 f 2.2 16.8 f 3.5 10.9 f 3.1 92f36
2omin
92f 12 72f 12 5.5 f 1.5 1293 f 348 7.4 f 2.5 17.0 f 3.8 11.0 f 3.4 93 f 35
Nfedipine 20 min
97f9 88 f 9' 72f9 75k 10 6.5 f 1.0 6.5 f 1.6 1122 f 191 1009 f 218t 8.3 f 1.0 8.5 f 1.8 19.0 f 2.7 17.8 f 2.5 12.8 f 2.4 11.5 f 1.9 78 f 29 81 f 31
Baseline
oxygen tension, carbon dioxide tension, haemoglobin concentration and oxyhaemoglobin saturation using a blood gas analyser (Radiometer ABL-300 analyser, Copenhagen, Denmark). Arterial oxygen content, mixed venous oxygen content, arteriovenous oxygen Content Merence, oxygen transport, oxygen uptake and oxygen extraction ratio were calculated with the standard formula."
After the catheter was placed, the patients were allowed to rest for 30 min. Baseline measurements were then obtained, and nifedipine was administered sublinguaUy. Twenty minutes after the drug administration, the measurements were repeated to evaluate the effects of nifedipine. The Doppler study was performed immediately after the CO determinations. In all cases, p o d vein blood flow was measured within 5 min after CO measurements.
Statistics
The results are presented as mean f s.d. Paired two-tailed Student's t-tests were used for mean comparisons between two measurements. One-way ANOVA test was used to compare the percentage changes in haemodynamic measurements. Linear coefficients of Correlation were also used in the analysis of the resuIts. Results were considered statistically signifkmt at P < 0.05.
RESULTS Systemic haemodynamic data are summarized in Table 2. In patients receiving nifedipine, MAP (P < 0.01) and SVR (P < 0.02) decreased significantly. The other haemo- dynamic parameters showed no significant changes after nifedipine administration. In control patients, there were no significant changes in systemic haemodynamic parameters.
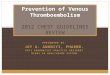
Splanchnic haemodynamic data are summarized in Table 3 and Fig. 1. In patients receiving nifedipine, the mean value of HVPG significantly increased from 15.4 f 5.3 to 18.1 f 5.8 mmHg (P< 0.01). There was also a significant increase in the mean value of hepatic venous wedge pressure and intrinsic clearance of ICG. Portal vein blood flow was hepatopetal in all 13 patients before and after nifedipine administration. There was a si&icant increase in portal vein blood flow from 689 f 159 to 816 f 193 mL/min (P < 0.01) after nifedipine adminis- tration. In control patients, there were no significant changes in splanchnic haemodynamic parameters.
The effects of nifedipine on systemic and splanchnic haemodynamics are shown graphically in Fig. 2. The percentage increases in HWG and in portal vein blood flow were significantly greater than the percentage increase in CO. Moreover, there was a signifcant correlation
Table 3 Effects of nifedipine on splanchnic haemodynamics in patients with cirrhosis
control Nifedipine Baseline 2omin Baseline 20 min
Free hepatic venous pressure (mmHg) Hepatic venous wedge pressure (mmHg) Hepatic venous pressure gradient ( d g ) Hepatic blood flow (Wmin)' Intrinsic Clearance (L/min)+ Portal vein blood flow (mL/min) Portal vein blood velocity ( c d s ) Portal vein cross-sectional area (mm*) portal vascular resistance (mmHg mL-' - min kg)
8.5 f 2.0 22.4 * 4.9 l3.9k4.1 954f246 0.25 f 0.07 628 f 250 12.6 f 2.5 77.9 f 17.2 1.35 f 0.53
8.5 f 2.0 22.7 f 5.0 14.2 f 3.8 952 f 388 0.24 f 0.08 619 f 214 U.0 f 1.9 75.8 f 18.0 1.36 f 0.52
8.9 f 2.2 24.3 f 5.0 15.4 * 5.3 1043 f 390 0.21 f 0.02 689 f 159 17.3 f 4.1 70.9 f 21.5 1.38 f 0.6
8.1 f 2.8 26.2 * 5.17 18.1 * 5.8X 1391 f 7695 0.27 f 0.04t 816 f 193; 19.2 f 6.2 77.3 f 19.4 1.37 f 0.57
~
T h e data were obtained from 5 control patients and 7 patients with nifedipine group. tp < 0.05, Z P < 0.01, § P < 0.1 from baseline.

K. Om et al. 201
PcO.01 1200 A
c
m 0 R
- L
400 Before After
P<O,
~~ ~
Before After
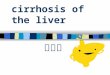
Figure 1 Changes in hepatic venous pressure gradient (a) and portal vein blood flow (b) in 13 patients receiving 10 mg of nifedi- pine. Horizontal bars indicate the mean values. Three patients with basal hepatic venous pressure gradient (HVPG) < 12 mmHg had relatively minor varices, such as small white varices, compared with the patients with basal HVPG 2 12 mmHg. There was a significant increase in the mean hepatic venous pressure gradient (P < 0.01) and the mean portal vein blood flow (P < 0.01) following nifedipine administration.
40
30
Y 20
F 10
A
fn a
fa J= 0 - 0 0
a -10 !!
-20
0) m C L
a R
MAP SVR CO HVPG PVF
PcO.01 I I Pc0.01 NS -
T
I T
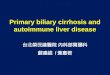
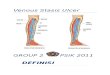
-30 I Figure 2 Percentage changes in MAP, SVR, cardiac output (CO), HVPG, and portal vein blood flow (PVF) in 13 patients receiving nifedipine. The percentage changes in PVF (+1!3%) and in HVPG (+20%) were signiihutly greater than the percentage changes in CO (+1%). One-way ANOVA test is used for the analyses.
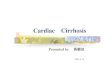
between the percentage increase in HVPG and that in portal vein blood flow (Fig. 3, P = 0.026, r = 0.61). However, there were no significant correlations between the percentage increase in CO and that in HVPG (r = 0.19) or that in portal vein blood flow (r = 0.13).
40
- $
a.
fn 20
30 > C
0 0 C m A=
a 0 a
.-
0 10
11-13 y=9.71+0.47~ a
R
- 1 0 L - - -20 0 20 40 60
Percentage changes in HVPG (%)
Figure 3 Correlation between percentage change in HVPG and percentage change in portal vein blood flow (PVF). There was a significant cornlation between the two parameters (P = 0.026)
The effects of nifedipine on pulmonary gas exchange, oxygen transport and oxygen utilization are shown in Table 4. There were no significant changes in arterial oxygen tension, arterial oxygen saturation or alveolar-arterial oxygen differences. Similarly, nifedipine administration also did not Sec t the oxygen transport or oxygen utilization by peripheral. tissues in patients with cirrhosis of the liver.
DISCUSSION To date, there has been no agreement on the effects of nifedipine on portal haemodynamics in patients with

202 Nifediipine and hepatic h d y m m k s
Table 4 Effects of nifedipine on pulmonary gas exchange and oxygem transport, oxygen utilization in 13 patients with cirrhosis
Control Nifedipine Baseline 20 min BaSeline 20 min
~~ ~~ ~
Arterial 0 2 tension (mmHg) Arterial 02 content (mL/dL) Alveolar-arterial O2 dif€exnce ( d g ) Mixed venous 02 tension (mmHg) Mixed venous 02 content (mL/dL.) Arteriovenous 0 2 content difference (mL/dL) 02 transport ( m ~ -mid - m-') 02 uptake (mL - m i d em-') 02 extraction fraction ( W )
83f7 15.2 f 3.3 17f6 43f3 12.4 f 3.1 2.7 f 0.6 689 f 174 124 f 40 18.2 f 3.8
~~
84f7 15.2 f 3.4 17*8 40f3 12.7 f 3.3 2.6 f 0.3 692 f 177 118 f 24 17.4 k 3.6
89 * 16 16.5 f 2.0 21 rt 13 38 f 5 13.2 * 2.2 3.3 f 0.7 659 f 113 128 f 34 20.3 f 5.4
92f23 16.4 f 2.2 22 * 12 39*4 13.2 f 2.2 3.2 f 0.6 658 k 154 122 f 16 19.8 f 4.6
cirrhosis. Some reports have stated that nifedipine had no significant effect on hepatic haemodynamic~.'~,'~ However, Koshy et d. reported possible deleterious effects of nifedipine on hepatic haemodynamics.'I Since all of these studies have analysed only a small number of patients, the controversy over haemodynamic results may be due to type 2 errors. Additionally, all the previous studies did not evaluate the changes in portal vein blood flow. While some studies evaluated the changes in effective hepatic blood flow, this represents the sum of hepatic arterial flow and portal blood flow. We believe that portal vein blood flow is a direct and more reliable index of the portal haemodynamic changes following nifedipine administration. For these reasons, we evaluated the effects of nifedipine on both HVPG and portal vein blood flow in patients with cirrhosis.
In the present study, MAP and SVR sigaificantly decreased after nifedipine. These haemodynamic changes denote the central haemodynamic effects of nifedipine and these results are consistent with those of prior
In our study, CO and heart rate did not change after nifedipine administration findings contradicting the results of previous reports in which nifedipine was administered to patients with cirrh~sis. '~-~~ The differing results seem to be attributable to the Merences in the study design. We measured haemodynamic parameters before and 20 min after administration of nifedipine. As the maximum haemodynamic effect of nifedipine is obtained 3-60 min after sublingual administration,'8 present results appear to denote the early hypotensive phase which was followed by reflex tachycardia and CO increase. Indeed, an interval of several minutes between hypotensive response and reflex tachycardia was noted in cirrhosis undergoing intravenous nicardipine infusion.'O Abnormalities of sympathetic nervous activity in cirrhosis may contribute to the blunted tachycardia re~ponse.'~
In the present study, the baseline HVPG values were relatively low in several patients. Since all our patients had non-alcoholic cirrhosis, HVPG may underestimate the portal pressure due to the presinusoidal component.20 Following nifedipine administration, the mean value of HVPG rose significantly after nifedipine administration. Individual haemodynamic data showed that none of the patients with basal HVPG 212 mmHg experienced a
decrease in HVPG to 5 12 mmHg after receiving nifedipine. Moreover, two of three patients with basal HVPG <l2 mmHg experienced an increase in HVPG to > 12 mmHg after receiving nifedipine. It is generally believed that a value of HVPG 2 I2 mmHg is a signdkant risk factor for variceal bleeding and the aim of pharmacological treatment of portal hypertension is to reduce HVPG to < I2 mmHg.' Therefore, the present results suggest that long-term administration of nifedipine may potentially increase the risk of variceal bleedmg.
The mechanism of HVPG increase following nifedipine administration remains unclear. In the present study, there was a positive correlation between the percentage changes in HVPG and those in portal blood flow. These results revealed a direct interrelationship between the portal venous inflow and HVPG. Koshy et al. observed an increase in HVPG following nifedipine administration in patients with alcoholic cirrhosis." They presumed that increased HVPG may be related to the increase in portal vein blood flow via increased CO. But they did not evaluate the serial changes in portal blood flow. In the present study, the increase in CO was only 1%, while the increase in portal blood flow was 19%. Thus, there was no correlation between the percentage changes in CO and the portal blood flow nor HVPG. These results imply that the increase in portal blood flow is not a direct effect of the augmentation in CO. Nifedipine attenuates the splanchnic reflex vasoconstriction in response to systemic hypotension. As the percentage change in portal blood flow is more pronounced than the percentage change in CO, splanchnic arterial vasodilatation appears to be one of the si@icant contributors to the increase in portal blood flow. The effects of nifedipine on portal blood flow have not been reported
calciumchannel blockers are shown to have a direct vasodilatory effect on portal venous system in animal experiment.8 In the present study, there was no sigmfkant change in portal vascular resistance after nifedipine administration. The reason for the lack of effect on portal vascular tone remains unclear. Since nifedipine affects the arterial resistance vessels more intensely than the venous capacitance vessels, the dose of nifedipine may be inadequate to obtain significant effects on portal vein.'* Additionally, abnormalities of vasoactive substance in
previously.

K. Ota et al. 203
cirrhosis may interfere with the haemodynamic effects of nifedipine.
The intrinsic clearance of indocyanhe green sigmkantly increased and the estimated hepatic blood flow tended to increase following nifedipine administration. As previously reported,” estimation of intrinsic clearance according to sinusoidal perfusion model of hepatic elimination was used to express the metabolic activity of hepatocytes, present results indicate that nifedipine actually improved the hepatic function. Similar results have been observed in patients with cirrhosis after administration of nicardipine. lo
Other authors have suggested that patients with hepa- tic failure have impaired oxygen utilization in spite of in- creased oxygen tran~port.”.~’ Thus, the cirrhotic patient has subclinical tissue hypoxia.I7 Because vasoactive drugs interfere with pulmonary gas exchange and oxygen utilization in patients with cirrhosi~,’*~*~~~ vasodilators pose a potential risk of exacerbating the tissue hypoxia. Indeed, nitrate has been shown to aggravate tissue hypoxia via reduction in oxygen transport in patients with cirrho~is.~ The second aim of this study was to elucidate whether nifedipine affects pulmonary gas exchange and tissue oxygenation in patients with cirrhosis. Our results showed no sigmfkant changes in pulmonary gas exchange and tissue oxygenation. These results may be due to the fact that nifedipine, contrary to nitrate, does not attenuate effects on CO and pulmonary gas exchange. As pulmonary arterial pressure and pulmonary vascular resistance did not change following nifedipine administration, insignifcant pulmonary vasodilatation may account for the lack of changes in arterial oxygenation.
Finally, we realize that portal vein blood velocity in our nifedipine group was considerably high, as compared with the previous rep0rt.2~ In our nifedipine group, two patients with recanalized para-umbilical vein experienced extremely high baseline blood velocity (23.2 cm/s, 24.0 c d s , respectively), and the mean value of the remain- ing 11 patients was 15.8 + 3.1 c d s . Large individual vari- ability seemed to be the main factor for high portal vein blood velocity. However, all statistical results were similar when the remainding 11 patients were separately analysed. Further, since the majority of our patients were Child- Pugh class A, a dominant population with less advanced cirrhosis may also contribute to high portal vein blood velocity.
In conclusion, we found slgnifcant increases in hepa- tic venous pressure gradient and portal vein blood flow after nifedipine administration. The increase in portal vein blood flow appeared to be related to splanchnic arterial vasodilatation by nifedipine. Consequently, nifedipine may increase the risk of variceal haemorrhage in patients with less advanced varices. We conclude that nifedipine should be used with caution in patients with chronic liver disease.
REFERENCES
1. KOKAWA H., SHIJO H., KUBARA K. er al. Long-term risk factors for bleeding after first course of endoscopic injection
sclerotherapy: A Univariate and multivariate analysis. Am. 3. Gastroenterol. 1993; 88: 1206-11.
2. TERES J., BOSCH J., BORDAS J. M. et al. Propranolol versus sclerotherapy in preventing variceal rebleeding: A randomized controlled trial. Gastroenterology 1993; 105: 1508-14.
3. GARCIA-PAGAN J. C., FEU F., NAVASA M. et al. Long-term hemodynamic effects of isosorbide 5-mononitrate in patients with cirrhosis and portal hypertension. 3. Hepatol. 1990, 11:
4. GARCIA-TSAO G., GROSZMANN R. J., FISHER R. L., CONN H. O., A ~ R B U R Y C. E. & GLICKMANN M. Portal pressure, presence of gastroesophageal varices and variceal bleeding. Hepatology 1985; 5: 419-24.
influencing the portal pressure response to propranolol administration in patients with cirrhosis. Hepatology 1991; 14: 133A.
6. SALMERON J. N., ARBOL R. D., GINES A. et al. Renal effects of acute isosorbide-5-mononitrate administration in cirrhosis. Hepatology 1993; 17: 800-6.
7. MOREAU R., LEE S. S., HANDENGUE A., OZIER Y., SICOT C. & LEBREC D. Relationship between oxygen transport and oxygen uptake in patients with cirrhosis: Effects of vasoactive
8. BLEI A. T. Vasodilator therapy of portal hypertension: Focus on the liver. Hepatology 1989; 9 8969.
9. NAVASA M., BOSCH J., REICHEN J. et al. Effects of vera- pamil on hepatic and systemic hemodynamics in patients with cirrhosis and portal hypertension. Hepatology 1988; 8: 850-4.
10. IWAO T., TOYONAGA A., IKEGAMI M. et al. Nicardipine infusion improved hepatic function but failed to reduce hepatic venous pressure gradient in patients with cirrhosis. Am. 3. Gastroenterol. 1992; 07; 326-31.
11. KOSHY A., HADENGUE A., LEE S. S., JIRON M. & LEBREC D. Possible deleterious hemodynamic effect of nifedipine on portal hypertension in patients with cirrhosis. Clin. Phannacol.
12. LAY C. S., TSAI Y. G., KONG C. W. er al. Lack of effects of nifedipine on hepatic hernodynamics in patients with HBsAg-positive cirrhosis. Liver 1987; 7: 223-7.
13. STRAUMAN N. A., GYR K., KIOWSKI W., BRUENDLER H. & STALDER G. A. Hemodynamic effects of nifedipine on hepatic venous pressure gradient in patients with portal hypertension. Hepatogastroenterology 1986; 33: 101-4.
14. PUGH R. N. H., MURRAY-LYON I. M., DAWSON J. L., PIETRONI M. C. & WILLIAMS R. Transection of oesophagus for bleeding oesophageal varices. Br. 3. Surg. 1973; 60: 646-9.
15. SABBA C., WELTIN G. G., CICCHE~TI D. V. et al. Observer variability in echo-Doppler measurements of portal flow in cirrhotic patients and normal volunteers. Ganroenterology
16. MORIYASU F., NISHIDA O., BAN N. et al. Measurement of portal vascular resistance in patients with portal hyper- tension. Gastroenterology 1986; 90: 710-17.
17. MOREAU R., LEE S. S., SOUPISON T., ROCHE-SICOT J. & SICOT C. Abnormal tissue oxygenation in patients with cirrhosis and liver failure.3. Hepard. 1%8; 7 98-105.
18. MCALLISTER R. G. JR. Kinetics and dynamics of nifedipine after oral and sublingual doses. Am. J. Med. 1986; 81 (Suppl.
189-95.
5. PEREIRA O., GARCIA-PAGEN J. C., FEU F. et d. Factors
drugs. Hepatology 1989; 9 427-32.
T h . 1987; 42: 295-8.
1990; 98: 1603- 11.
6A): 2-5.

204 Nifedip'ne and hepatic haemodymics
19. I~NDRICKSE M. T. & TRIGER D. R. Peripheral and cardio- vascular autonomic impairment in chronic liver disease: prevalence and relation to hepatic function. j . Hepatol. 1992; 16 177-83.
20. POMIER-LAYRARGUES G., KUSIELEWICZ D., WILLIAMS B. et al. Presinusoidal portal hypertension in non-alcoholic cirrhosis. Hepatology 1985; 5 46-18.
21. BIHARI D., GIMSON A. E. S., LINDRIDGE J. & WILLIAMS R. Lactic acidosis in fulminamt hepatic failure: Some aspects of pathogenesis and prognosis. J . Hepatol. 1985; 1: 405-16.
22. AGUSTI A. G. N., ROCA J., Bosw J., GARCIA-PAGAN J. C.,
WAGNER P. D. & RODRIGUEZ-ROISIN R. Effects of propran- 0101 on arterial oxygenation and oxygen transport to tissues inpatients with cirrhosis. Am. Rev. Re@+. Dis. 1990, 142: 305-10.
23. SHIJO H., SASAKI H., MIYAJIMA Y. & OKUMURA M. Prosta- glandin Fz0 and indomethacin on hepatogenic pulmonary angiodyspksia: Effects on pulmonary hernodynamics and gas exchange. Chest 1991; 100: 873-5.
24. OHNISHI K., SAITO M., NAKAYAMA T. er al. Portal venous hernodynamics in chronic liver disease: Effects of posture change and exercise. Radiology 1985; 155: 757-61.