Embed Size (px)
Citation preview
요로종양병리 학습목표병리학교실 조 남훈
1. 방광 및 요로 상피세포의 조직학적 특징을
이해한다.
2. 방광암의 타종양과 차이점을 이해한다.2. 방광암의 타종양과 차이점을 이해한다.
3. 방광암의 육안 및 조직학적 유형 4가지를 이
해하고 각 유형별 가장 흔한 대표적인 유전
자 변이를 알아본다.
4. 방광암의 T0 개념을 포함한 병기를 이해하며
CIS의 진단방법을 알아본다.
Normal Histology
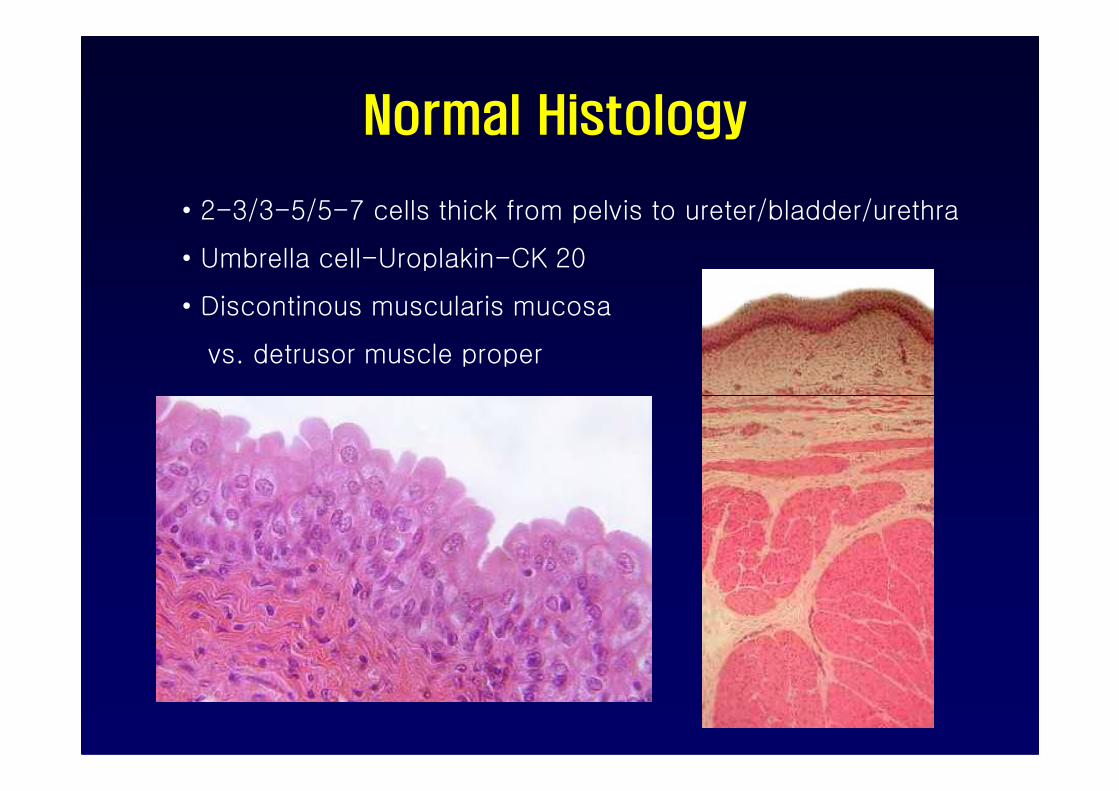
• 2-3/3-5/5-7 cells thick from pelvis to ureter/bladder/urethra
• Umbrella cell-Uroplakin-CK 20
• Discontinous muscularis mucosa
vs. detrusor muscle proper
Physiology and microanatomy of Normal Urotheliumto be characterized by Urine-Blood Barrier
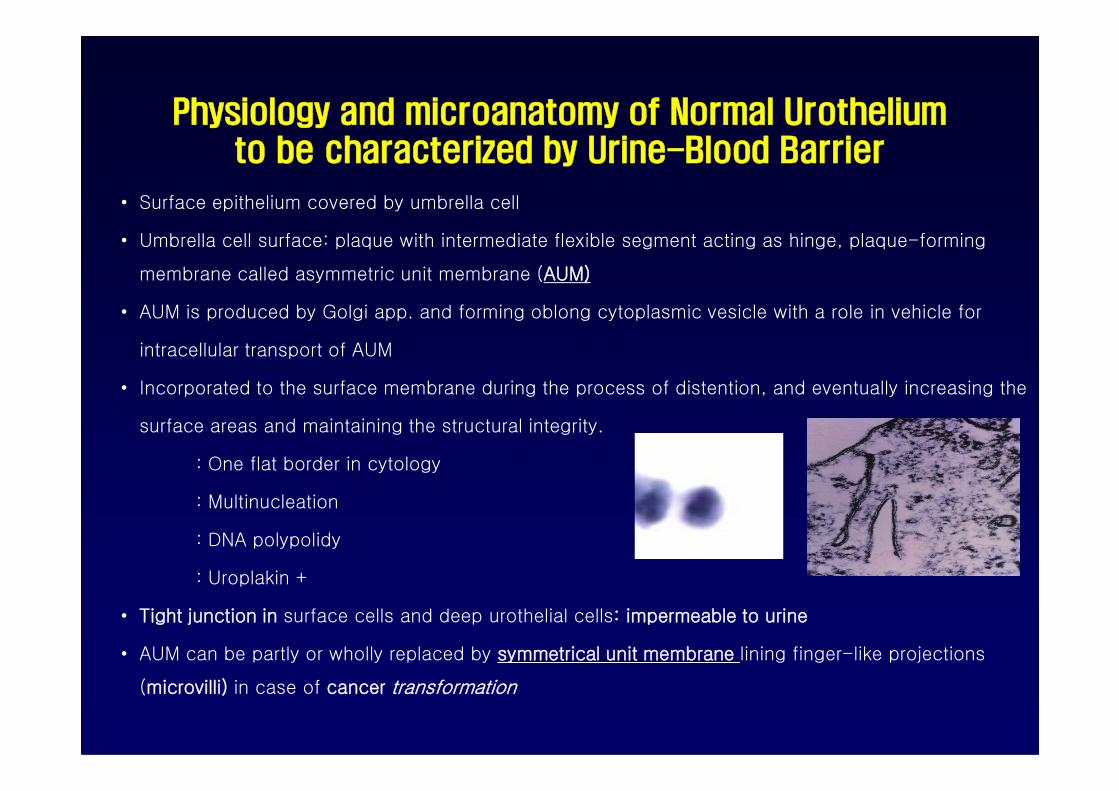
• Surface epithelium covered by umbrella cell
• Umbrella cell surface: plaque with intermediate flexible segment acting as hinge, plaque-forming
membrane called asymmetric unit membrane (AUM)
• AUM is produced by Golgi app. and forming oblong cytoplasmic vesicle with a role in vehicle for
intracellular transport of AUM
• Incorporated to the surface membrane during the process of distention, and eventually increasing the • Incorporated to the surface membrane during the process of distention, and eventually increasing the
surface areas and maintaining the structural integrity.
: One flat border in cytology
: Multinucleation
: DNA polypolidy
: Uroplakin +
• Tight junction in surface cells and deep urothelial cells: impermeable to urine
• AUM can be partly or wholly replaced by symmetrical unit membrane lining finger-like projections
(microvilli) in case of cancer transformation
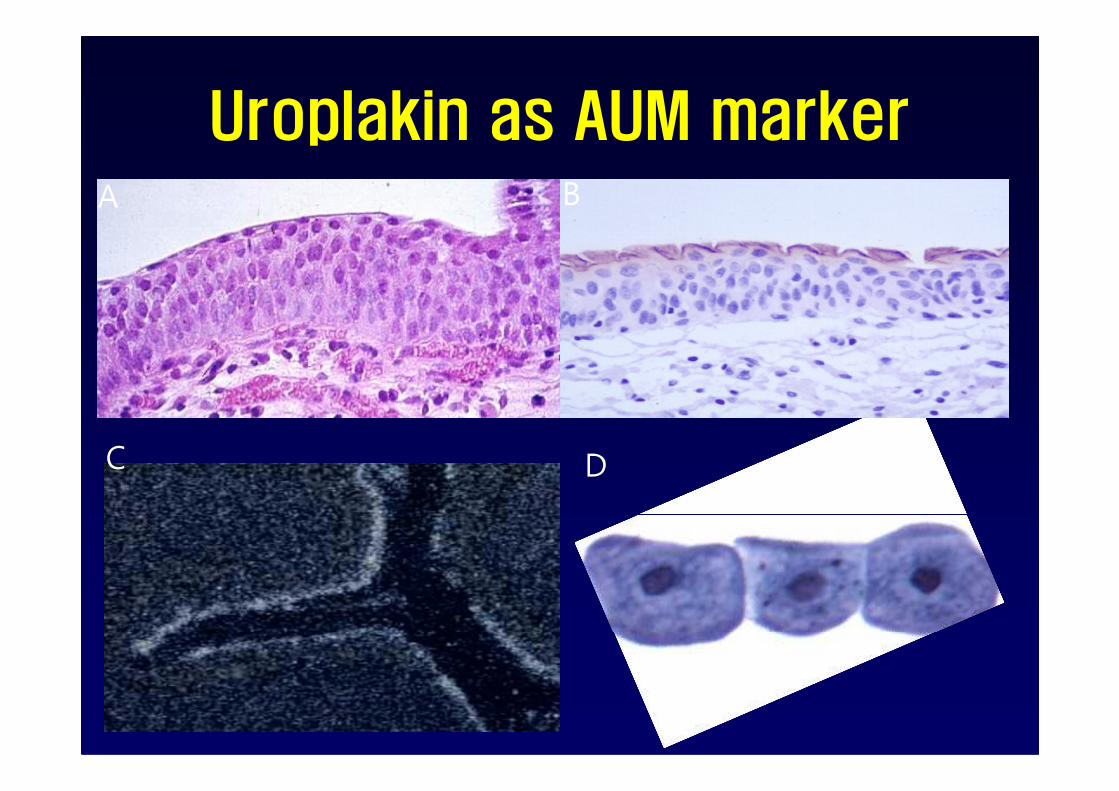
Uroplakin as AUM markerA B
C D

A B
C D E
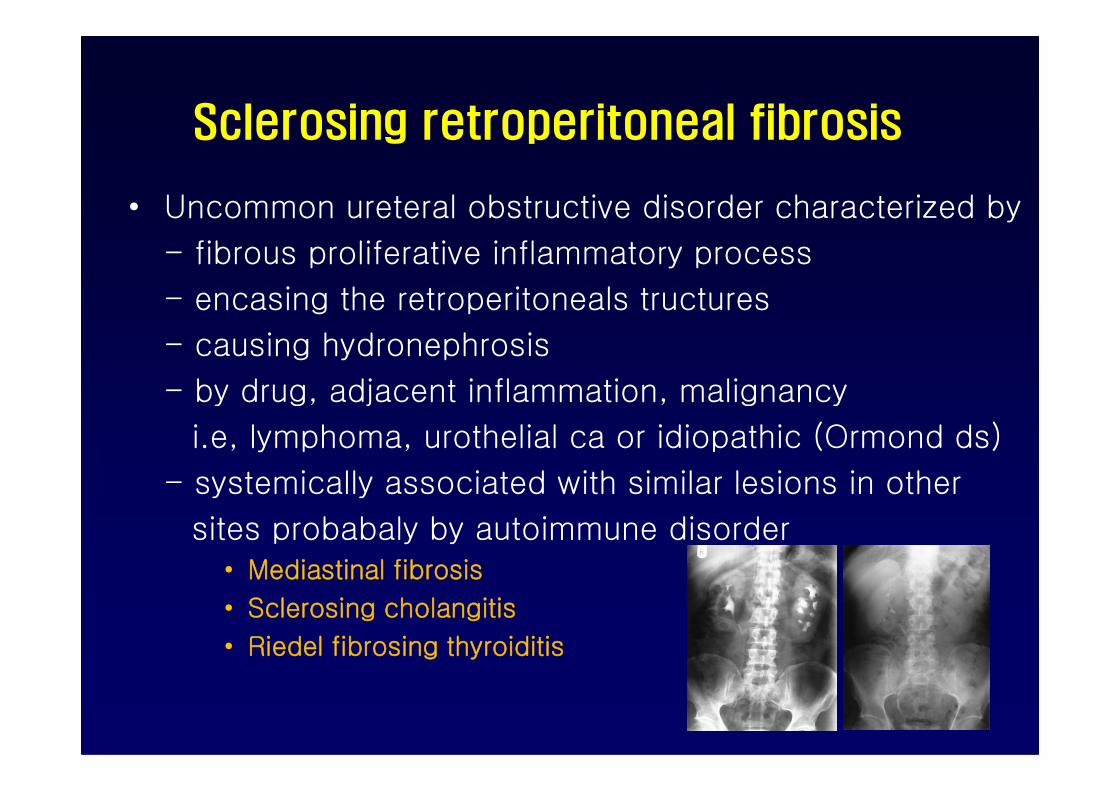
Sclerosing retroperitoneal fibrosis
• Uncommon ureteral obstructive disorder characterized by
- fibrous proliferative inflammatory process
- encasing the retroperitoneals tructures
- causing hydronephrosis
- by drug, adjacent inflammation, malignancy- by drug, adjacent inflammation, malignancy
i.e, lymphoma, urothelial ca or idiopathic (Ormond ds)
- systemically associated with similar lesions in other
sites probabaly by autoimmune disorder• Mediastinal fibrosis
• Sclerosing cholangitis
• Riedel fibrosing thyroiditis
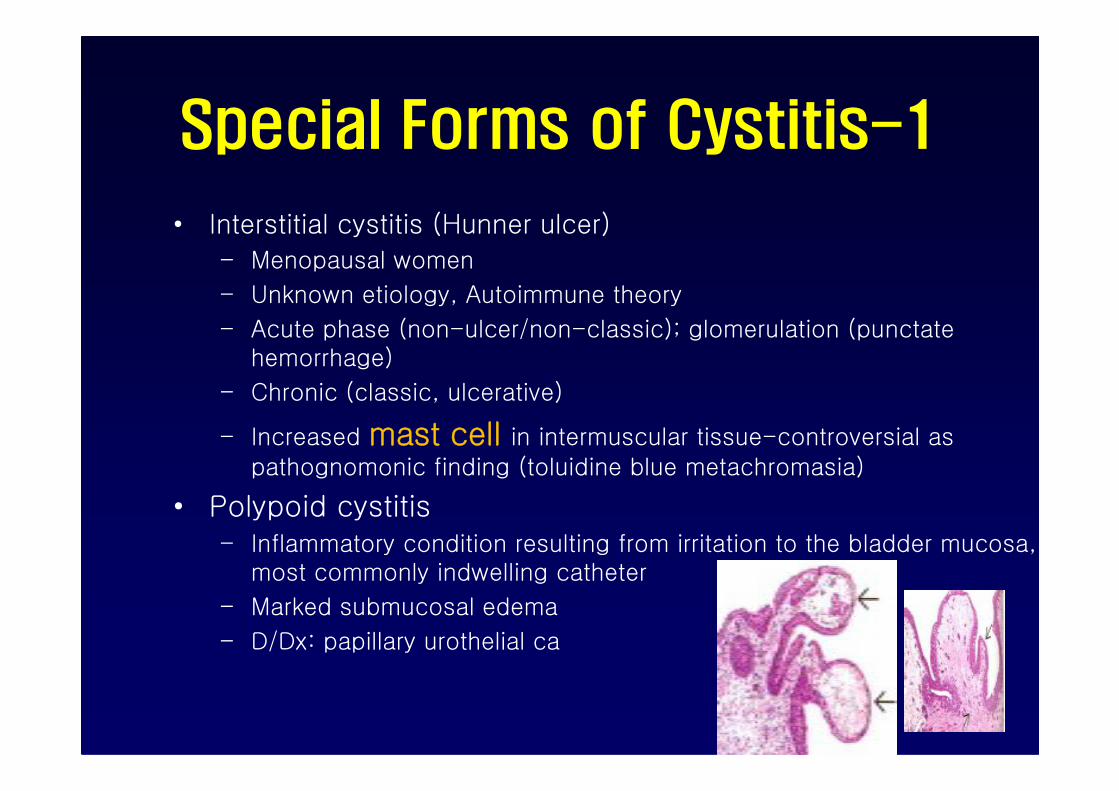
Special Forms of Cystitis-1
• Interstitial cystitis (Hunner ulcer)
– Menopausal women
– Unknown etiology, Autoimmune theory
– Acute phase (non-ulcer/non-classic); glomerulation (punctate hemorrhage)
– Chronic (classic, ulcerative)– Chronic (classic, ulcerative)
– Increased mast cell in intermuscular tissue-controversial as pathognomonic finding (toluidine blue metachromasia)
• Polypoid cystitis – Inflammatory condition resulting from irritation to the bladder mucosa,
most commonly indwelling catheter
– Marked submucosal edema
– D/Dx: papillary urothelial ca
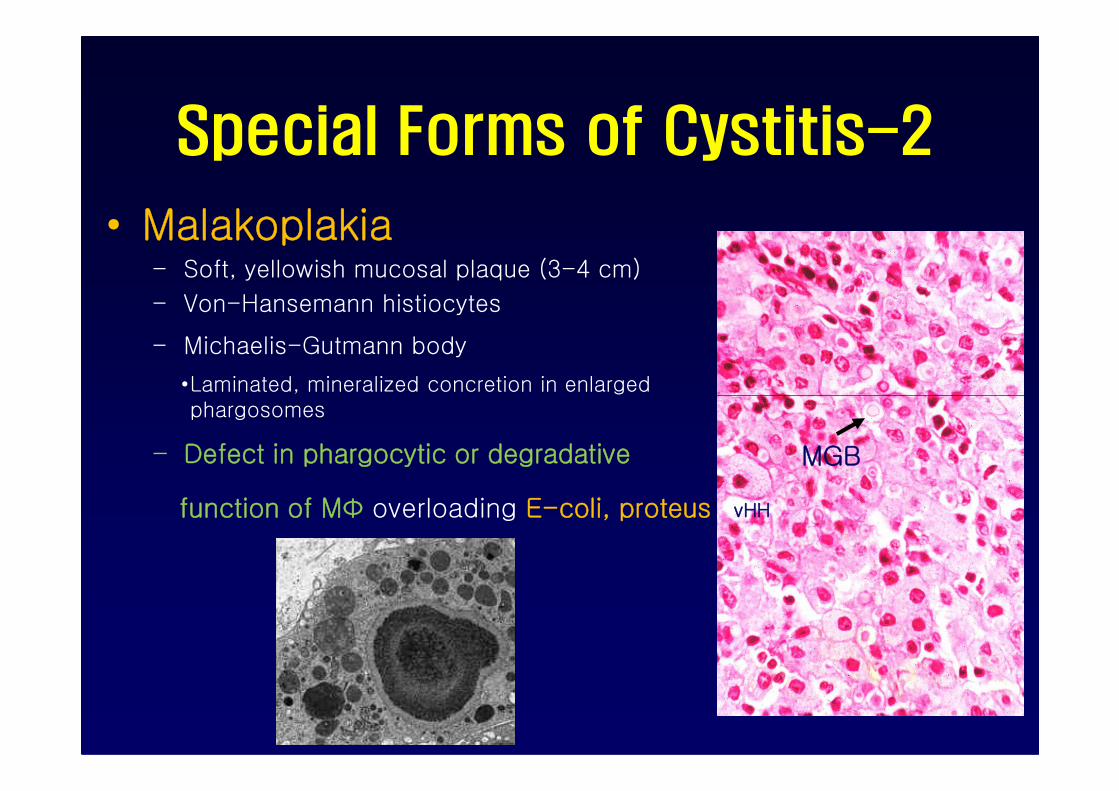
Special Forms of Cystitis-2
• Malakoplakia– Soft, yellowish mucosal plaque (3-4 cm)
– Von-Hansemann histiocytes
– Michaelis-Gutmann body
•Laminated, mineralized concretion in enlarged phargosomes
– Defect in phargocytic or degradative
function of MФ overloading E-coli, proteus
MGB
vHH

Metaplastic Lesions
1. Cystitis glandularis and (et) cysticaOften coexist
Intestinal metaplasia in case of goblet cells
2. Squamous metaplasia2. Squamous metaplasiaResponse to injury
Physiologically glycogenated vaginal-type of
squamous epithelium in woman at trigone-
no sq metaplasia
3. Nephrogenic metaplasia (adenoma)Papillary pattern lined by cuboidal cells and
tubular proliferation, ca mimicker
Epidemiology of Urothelial Ca
• Cigarette somking
• Industrial exposure– 2-naphthylamine
– 15-40 yrs after the first exposure
• Schistosoma haemoatobium
• Analgesics abuse
• long-term exposure to cyclophophamide– hemorrhagic cystitis
• Prior exposure of bladder to radiation
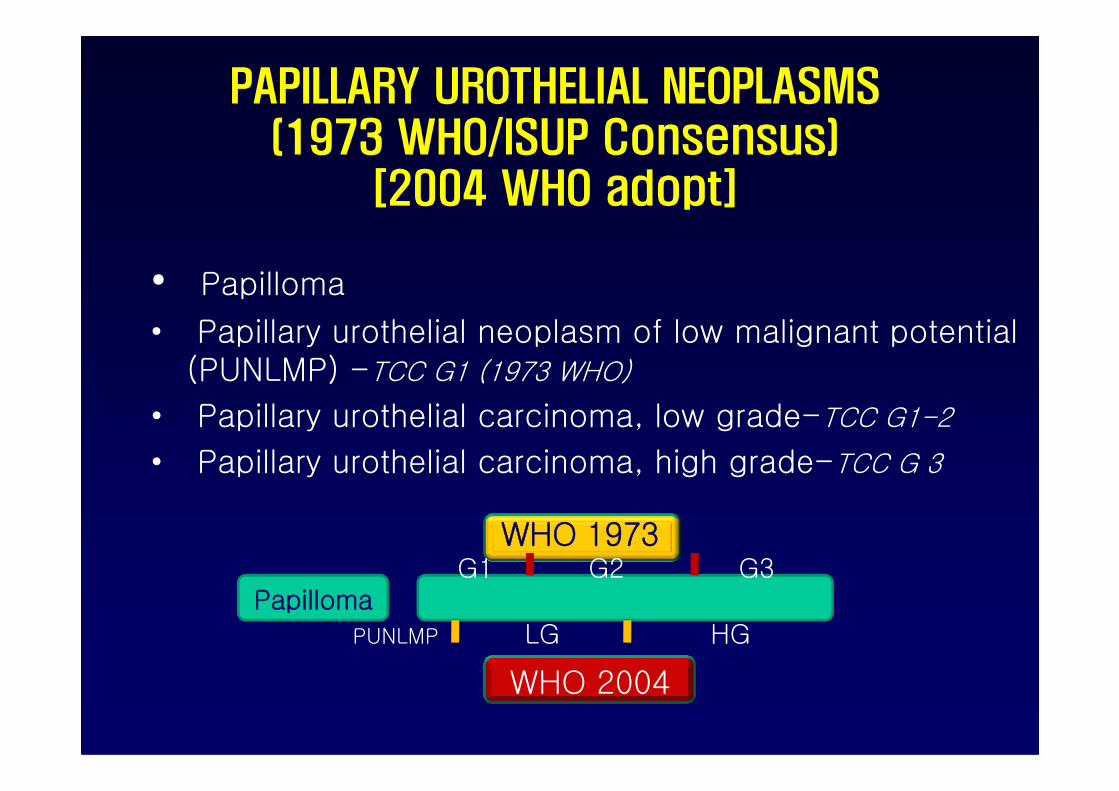
PAPILLARY UROTHELIAL NEOPLASMS(1973 WHO/ISUP Consensus)
[2004 WHO adopt]
• Papilloma
• Papillary urothelial neoplasm of low malignant potential (PUNLMP) -TCC G1 (1973 WHO)
• Papillary urothelial carcinoma, low grade-TCC G1-2
• Papillary urothelial carcinoma, high grade-TCC G 3
PapillomaG1 G2 G3
PUNLMP LG HG
WHO 1973
WHO 2004
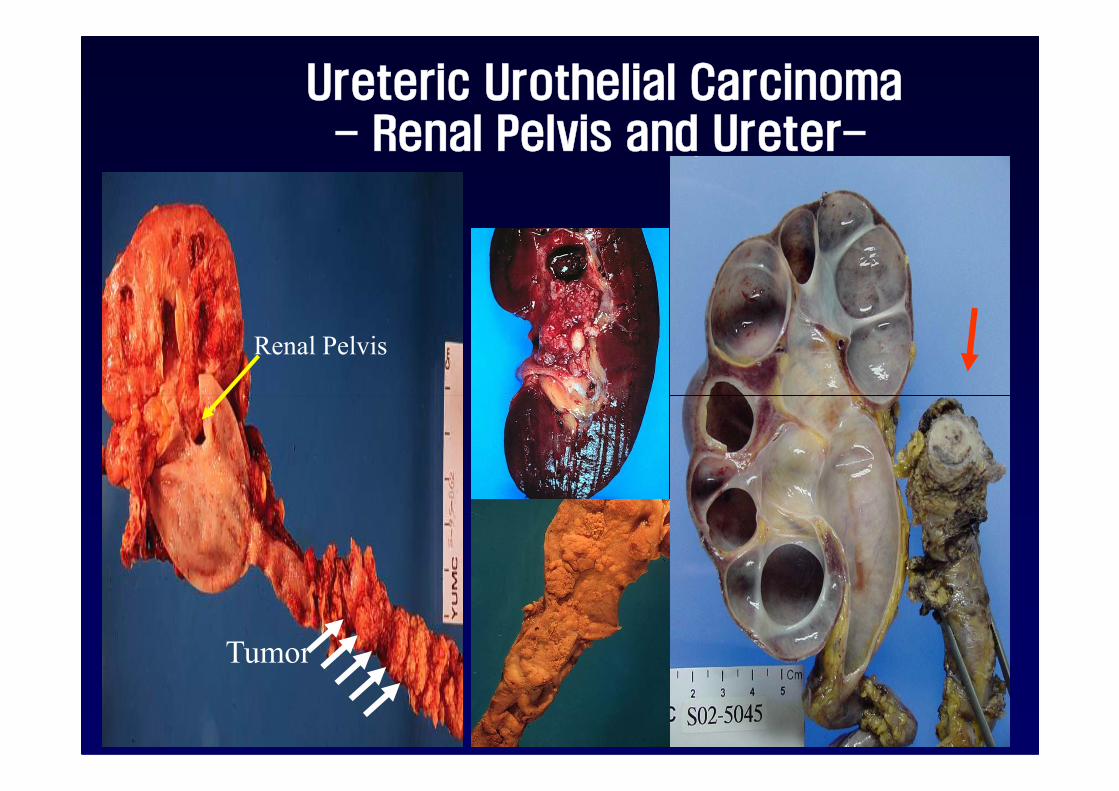
Ureteric Urothelial Carcinoma- Renal Pelvis and Ureter-
Renal Pelvis
Tumor
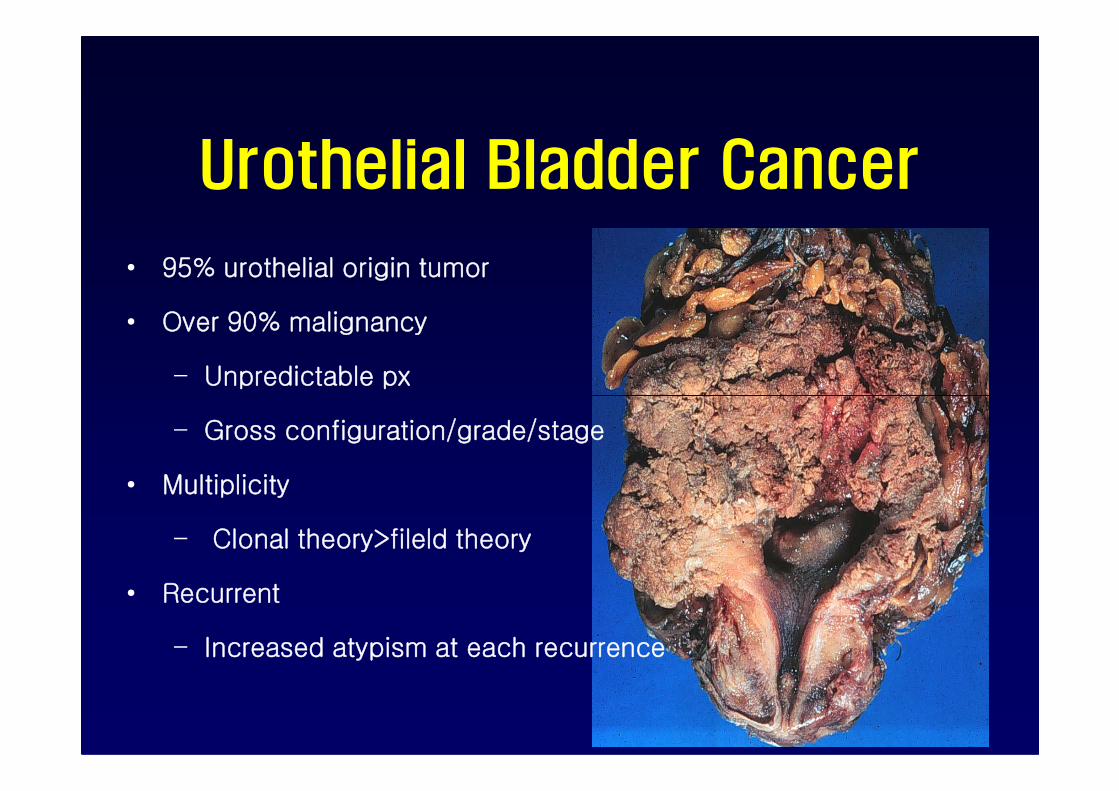
Urothelial Bladder Cancer
• 95% urothelial origin tumor
• Over 90% malignancy
– Unpredictable px
– Gross configuration/grade/stage
• Multiplicity
– Clonal theory>fileld theory
• Recurrent
– Increased atypism at each recurrence
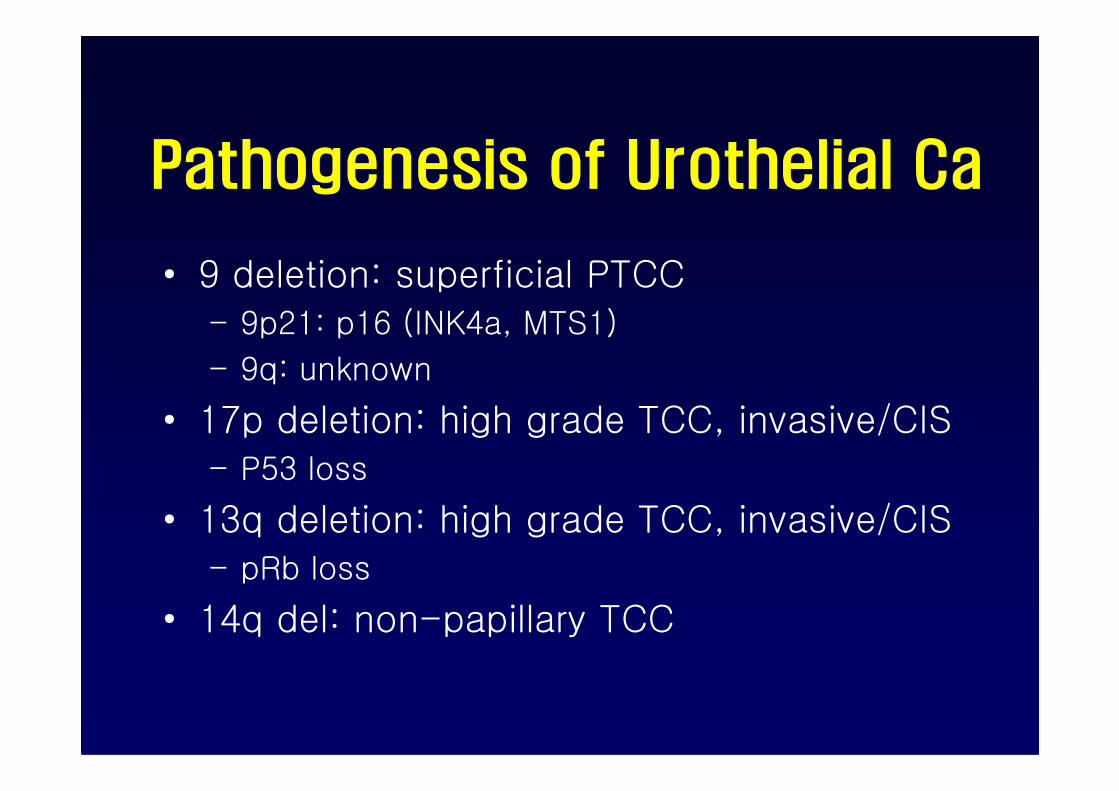
Pathogenesis of Urothelial Ca
• 9 deletion: superficial PTCC– 9p21: p16 (INK4a, MTS1)
– 9q: unknown
• 17p deletion: high grade TCC, invasive/CIS– P53 loss
• 13q deletion: high grade TCC, invasive/CIS– pRb loss
• 14q del: non-papillary TCC
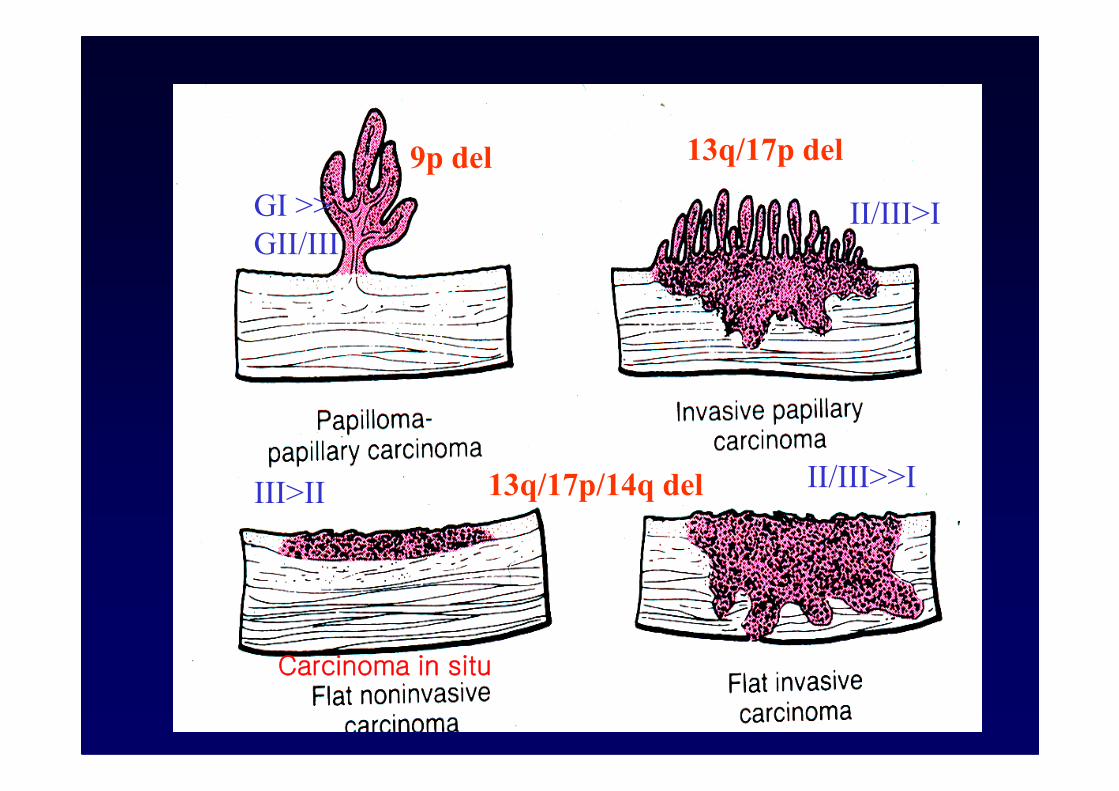
9p del 13q/17p del
GI >>
GII/III
II/III>I
13q/17p/14q delIII>IIII/III>>I
Carcinoma in situ
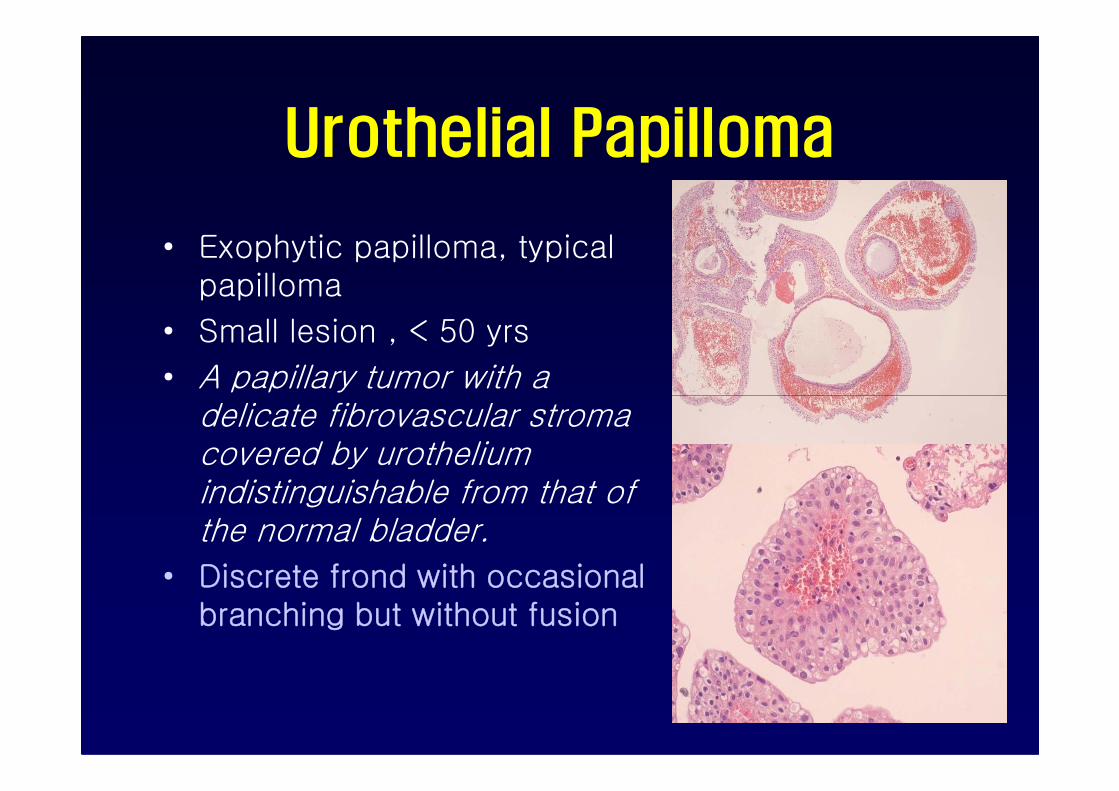
Urothelial Papilloma
• Exophytic papilloma, typical papilloma
• Small lesion , < 50 yrs
• A papillary tumor with a delicate fibrovascular stroma covered by urothelium indistinguishable from that of the normal bladder.
• Discrete frond with occasional branching but without fusion
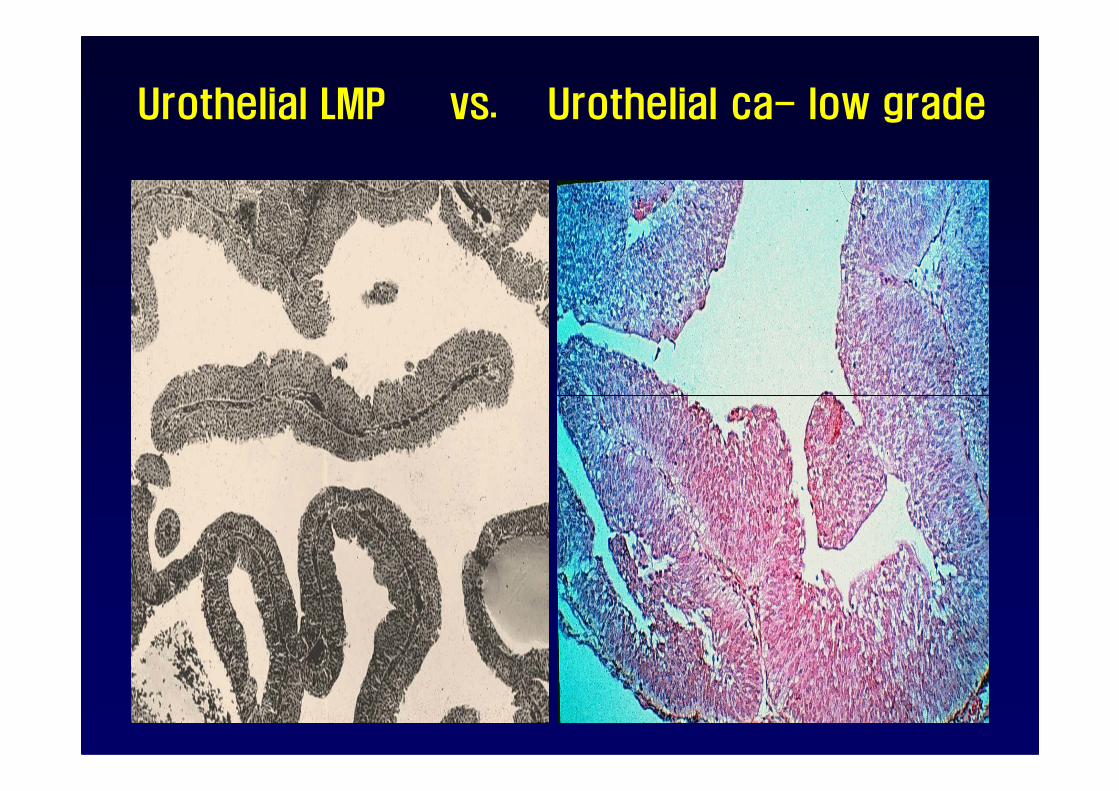
Urothelial LMP vs. Urothelial ca- low grade
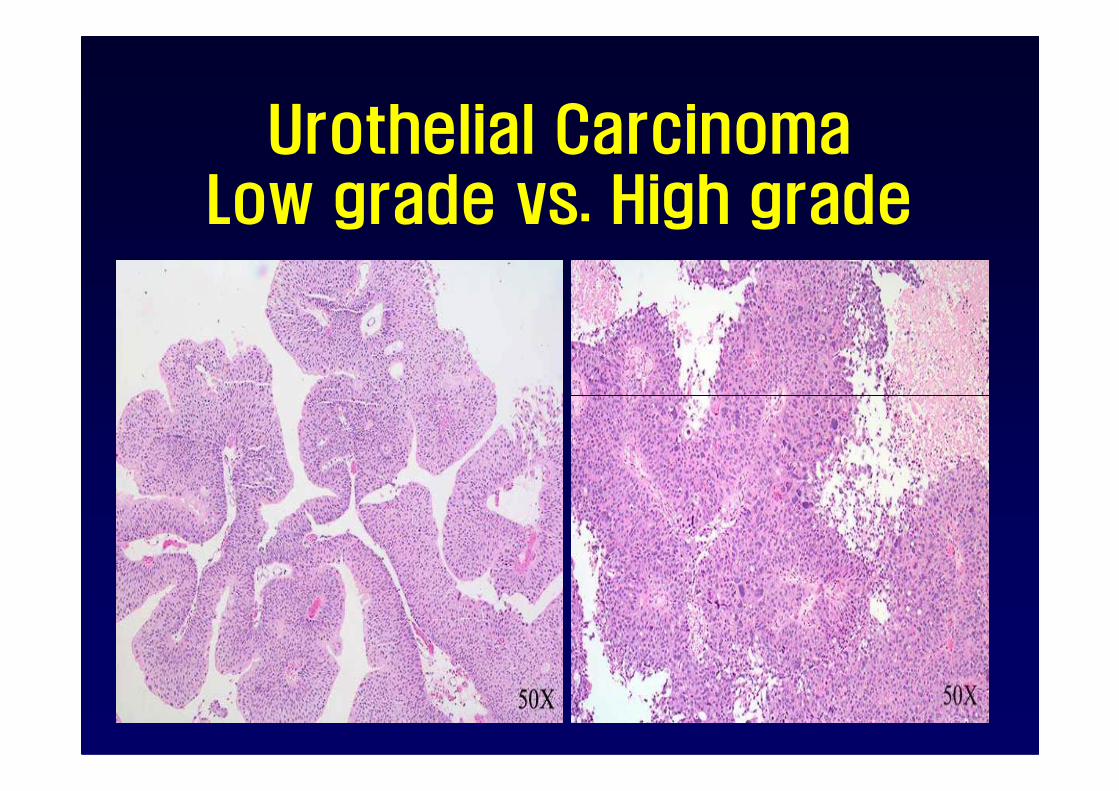
Urothelial CarcinomaLow grade vs. High grade
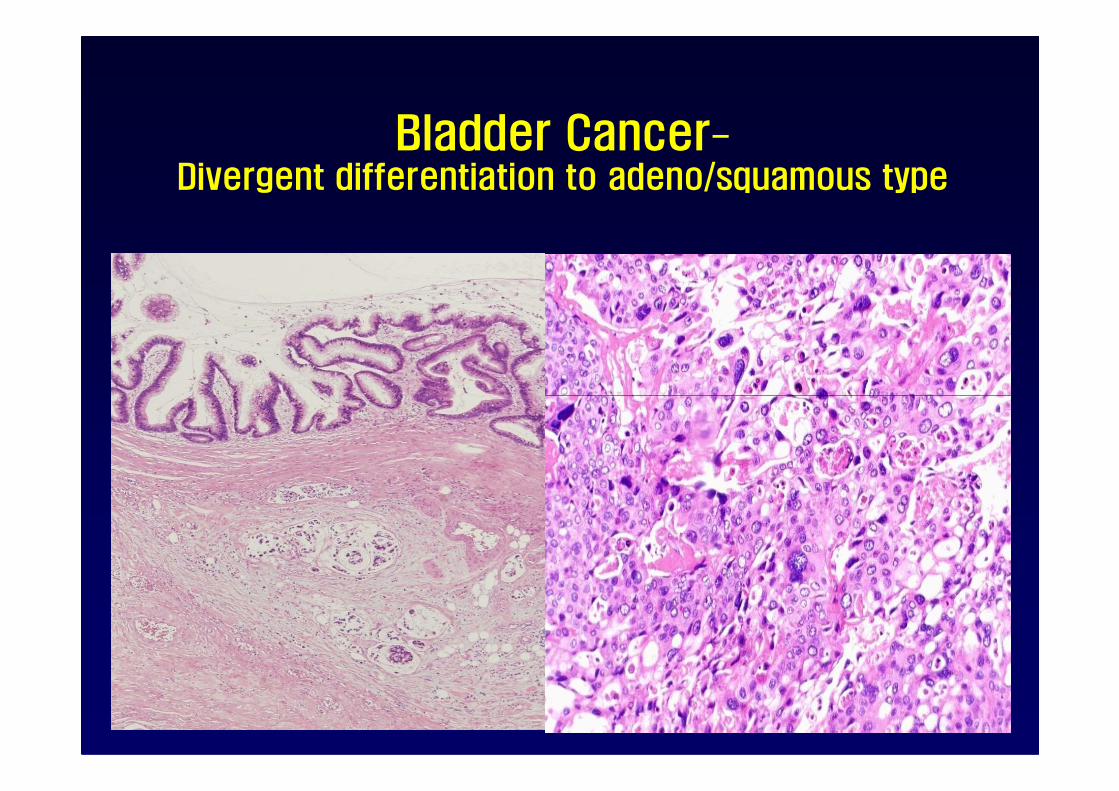
Bladder Cancer-Divergent differentiation to adeno/squamous type

Urothelial Carcinoma In SituNonpapillary Noninvasive TCC, Grade III
1-5% of CIS occurs in the absence of other pattern of cancer- primary CIS. If untreated, 50-75% of CIS progress to invasive ca.
Pagetoid CIS
Clinging CIS
Historical Overview of Urine Cytology• One of the first branch in medicine• Ancient era
– Soul substance to protect against evil– Rain-urine of god (deity)-exposure to rain is soul-healing.– Bathing for beauty and mouthwash for caries/ Cheese flavor, tobacco leaf, bakery leavening
• Hippocrates (Greek)– Foamy urine-serious and first invented biomarker – Colic, suppuration, hematuria: triad for urologic ds (stone, Tbc, cancer)
• Galen (Roman, AD 130-200)– Renal physiology and urine mechanism
• Avicenna (Persian, AD 980-1037)– Urinalysis (color, density, sediment, odor)-true biomarker
• Brian (1637)- urine examination alone in the absence of patient (Pisse-prophet)• Hooke (1665)-crystal figure in “Micrographia”• Rees (1836)- scientific urinalysis description in textbook
• Lambl (1856)-first documents on urothelial ca in urine cytology (On cancer of bladder)– 6 bladder tumors, 1 uterine ca to bladder, 1 papilloma in a girl, 2 inflammation
• Beale (1864)- urine cell type description • Papanicolaou (1945)-”urine cytologic evaluation of cancer” published in Science
– True + 88.8%, true – 60%
• Stewart (1942)-Carcinoma in situ (Dr. J. Ewing’s urine)• Koss-integrate urine cytology
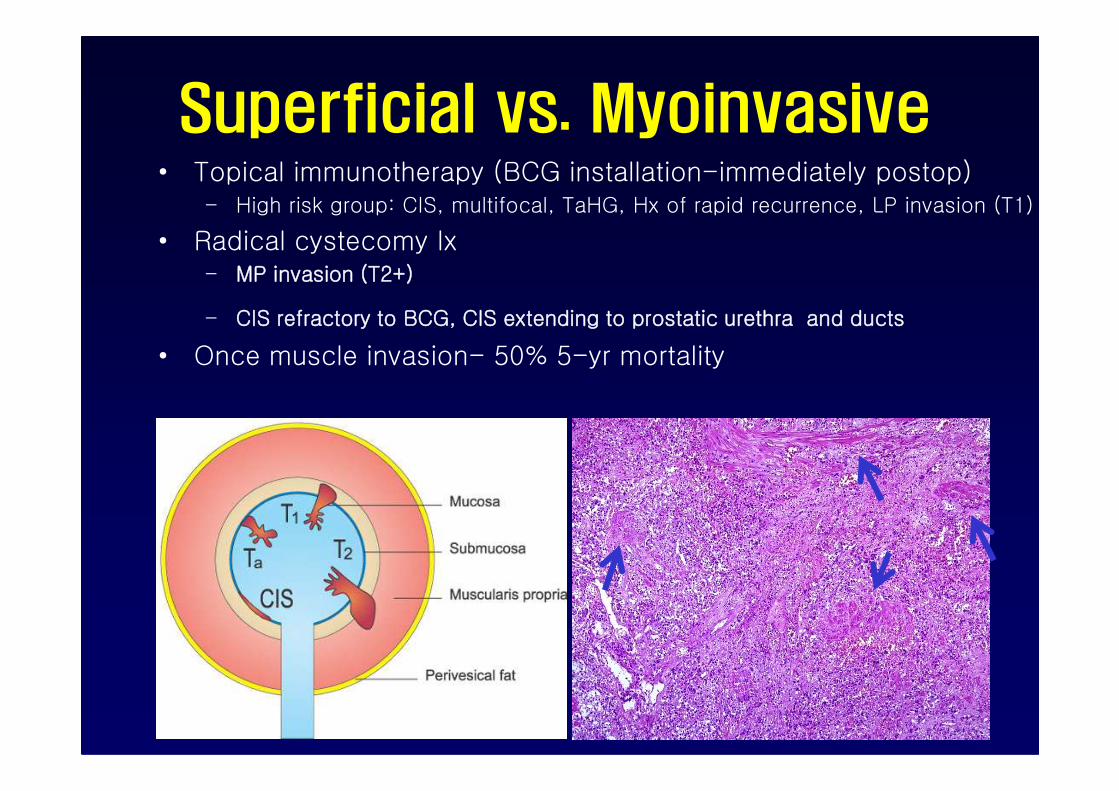
Superficial vs. Myoinvasive• Topical immunotherapy (BCG installation-immediately postop)
– High risk group: CIS, multifocal, TaHG, Hx of rapid recurrence, LP invasion (T1)
• Radical cystecomy Ix– MP invasion (T2+)
– CIS refractory to BCG, CIS extending to prostatic urethra and ducts
• Once muscle invasion- 50% 5-yr mortality
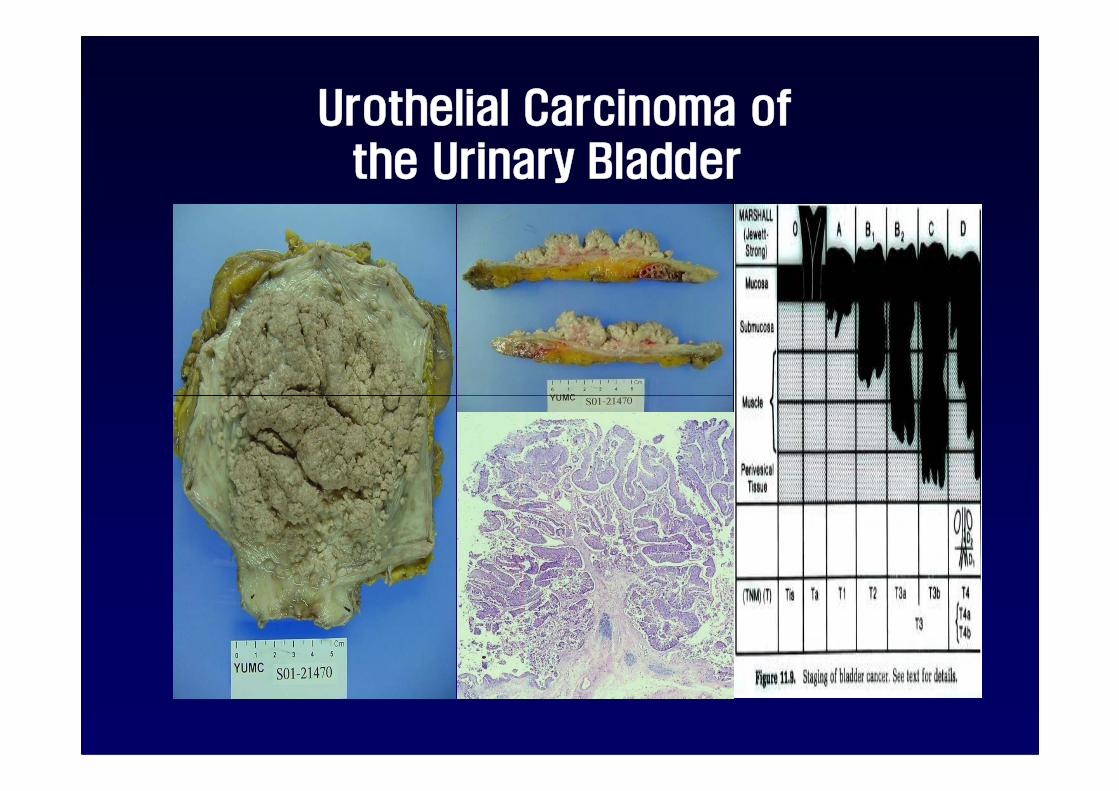
Urothelial Carcinoma of the Urinary Bladder
Recurrence vs. Progression
• Recurrence
– Subsequent tumor at different sites from the original lesions
– New tumor or shedding/implantation of the original tumor cells
– Recurrence-free survival factors
• Size, multifocality, stage, grade, prior recurrence rate, a/w CIS• Size, multifocality, stage, grade, prior recurrence rate, a/w CIS
– 98% of 10-yr survival in LG UC vs. 40% survival in HG UC
• Progression
– Staging progression (no applied on grading progression: recurrence)
– Progression-free survival factors
• grade
• presence of lamina propria (pT1 stage)
• associated carcinoma in situ
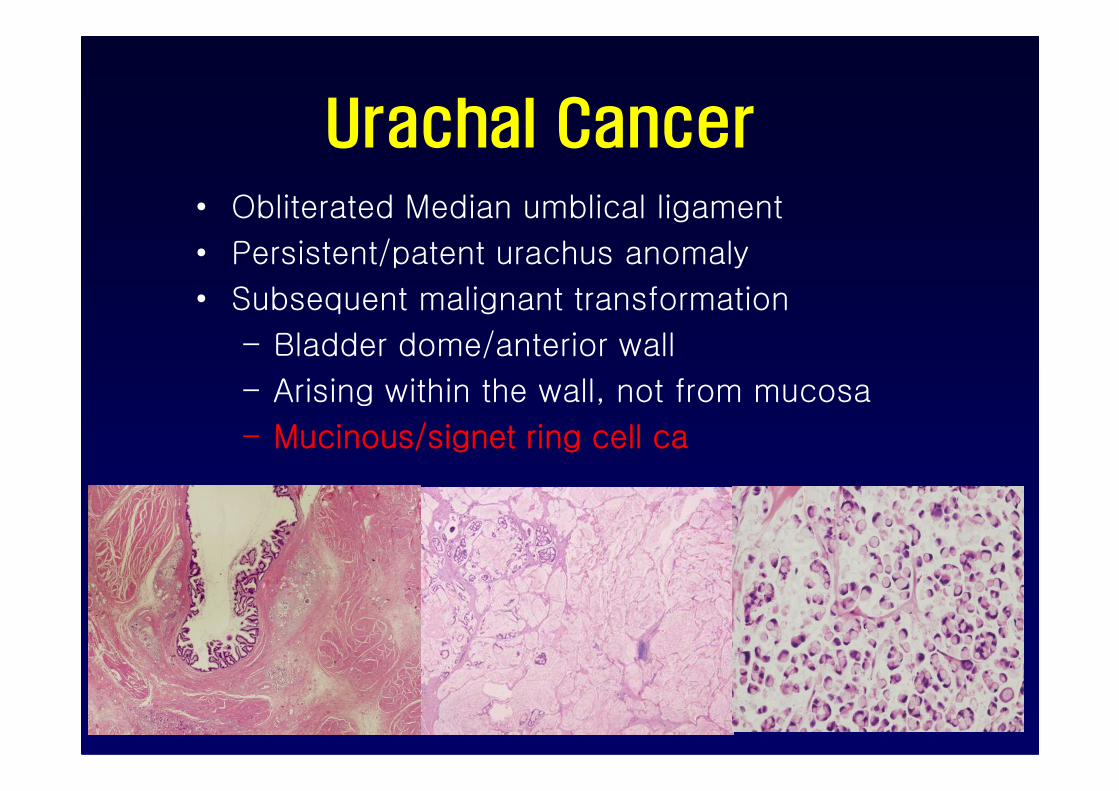
Urachal Cancer• Obliterated Median umblical ligament
• Persistent/patent urachus anomaly
• Subsequent malignant transformation
– Bladder dome/anterior wall
– Arising within the wall, not from mucosa– Arising within the wall, not from mucosa
– Mucinous/signet ring cell ca

Bladder calculi and trabeculation-outlet obstruction





















![2008 vesetumor- Kar di Zolt n [ r sv dett] · Vese térfoglaló folyamatainak életkor szerinti megoszlása • Újszülött – hydronephrosis 64 % – cystás vesebetegségek 18](https://img.pdfslide.tips/doc/110x75/5e128ad227919451aa0aab7c/2008-vesetumor-kar-di-zolt-n-r-sv-dett-vese-trfoglal-folyamatainak-letkor.jpg)







