Embed Size (px)
Citation preview
AIR MAIL
INTE
RNATI
ONAL MAI
L
2016March
Field Trip Report 2016
The Philippines
School of Tropical Medicine and Glo
bal Health Nagasaki Universit
y
School of
Tropical Medicine and Global Health
Nagasaki University
The Philippines
Field Trip Report 2016
Contents
Map of the Philippines 2
Photos 3
Forewords 8
Abbreviation List 10
Overview of the Philippines 12
Overview of the Field Trip 14
Daily Field Reports
29th FebruaryDepartment of Health (DOH), Health Human Resource Development Bureau
18
1st March (AM)World Health Organization Regional Office for the Western Pacific (WHO / WPRO)
22
1st March (PM)Japan International Cooperation Agency (JICA) Philippines Office
24
2nd MarchSan Lazaro Hospital (SLH)
26
3rd March (AM)A.A. Zapa Health Center in Caloocan City, Manila
28
3rd March (PM)Research Institute of Tuberculosis / Japan Anti-Tuberculosis Association (RIT/JATA) Philippines, Inc.
30
4th March (AM)Research Institute for Tropical Medicine (RITM)
32
4th March (PM)Philippine Red Cross (PRC) Headquarters
34
7th MarchPhilippine Red Cross (PRC) Leyte Chapter
36
8th MarchInstitutions related to Project for Strengthening Maternal and Child Health Services in Eastern Visayas, Philippines (SMACHS-EV Project)
38
11th MarchWorld Health Organization Regional Office for the Western Pacific (WHO / WPRO)
40
Report of the Final Presentation
Report 44
Presentation Slides 49
Afterword 52
Editor’s Note 53
1
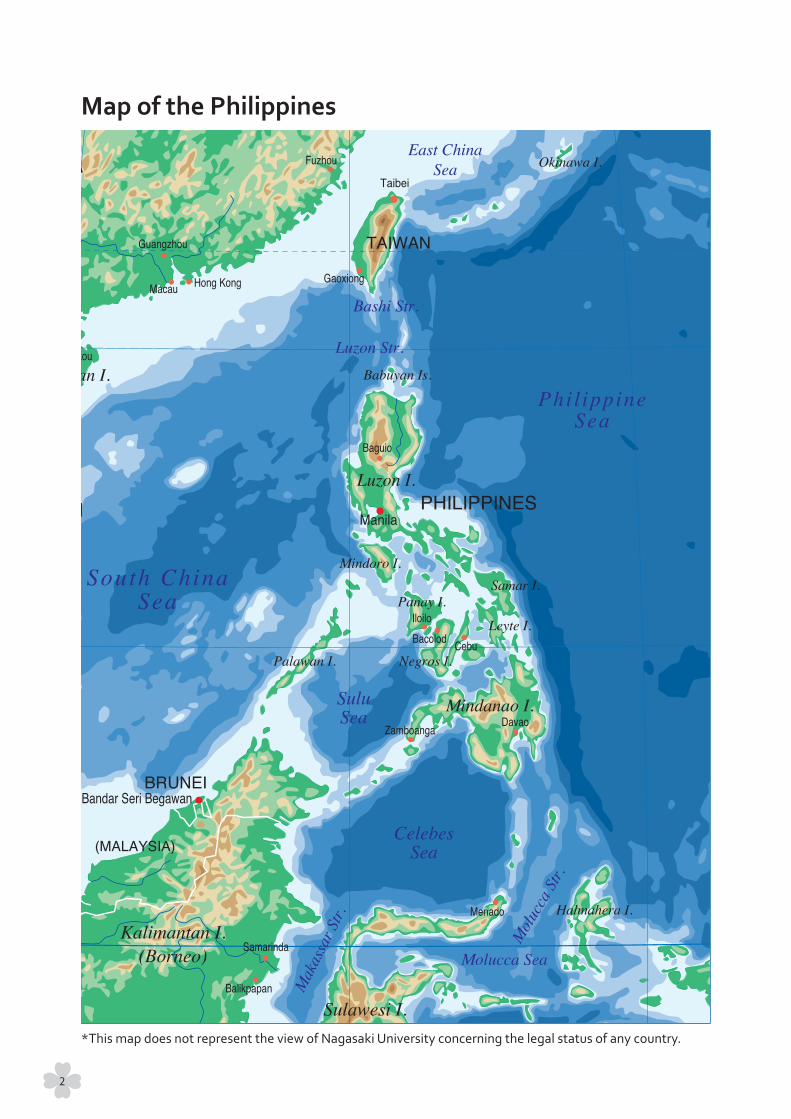
Map of the Philippines
*This map does not represent the view of Nagasaki University concerning the legal status of any country.
2
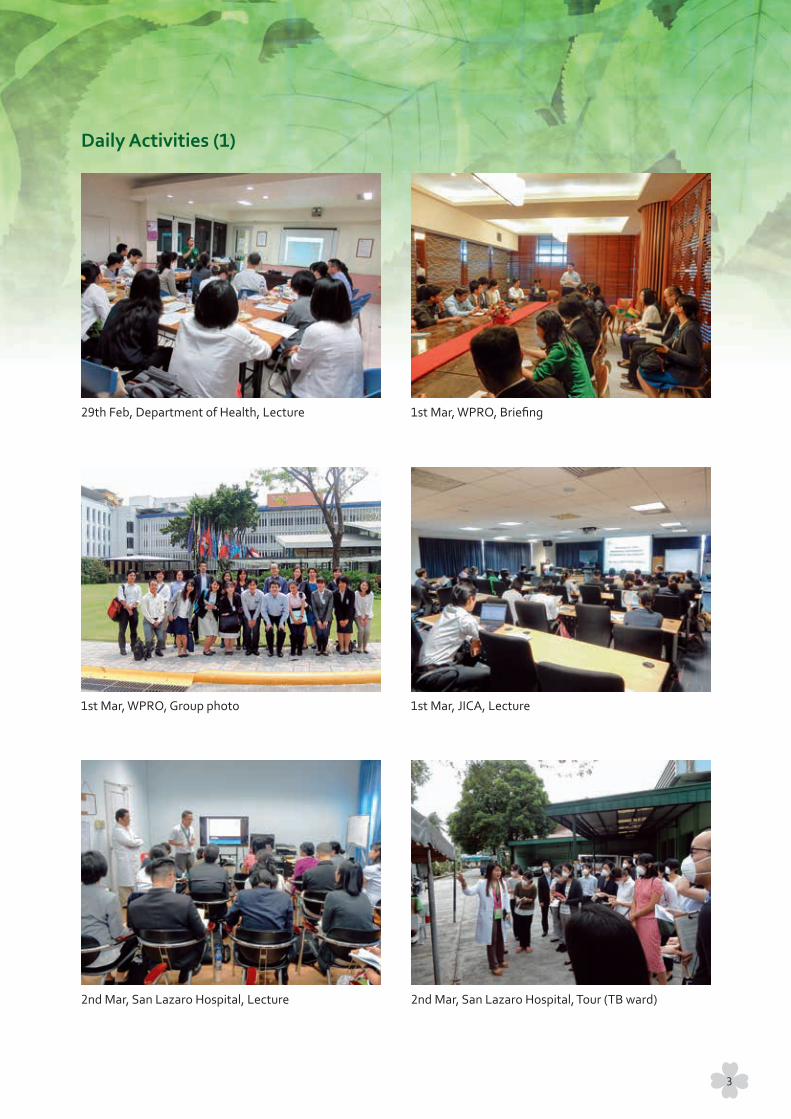
29th Feb, Department of Health, Lecture
Daily Activities (1)
1st Mar, WPRO, Group photo
2nd Mar, San Lazaro Hospital, Lecture
1st Mar, WPRO, Briefing
1st Mar, JICA, Lecture
2nd Mar, San Lazaro Hospital, Tour (TB ward)
3
3rd Mar, Caloocan City, Tour with barangay health workers
Daily Activities (2)
4th Mar, RITM, Laboratory tour
4th Mar, Red Cross Headquarters, Information and Technology Operation Center
3rd Mar, RIT / JATA Philippines, Inc., Lecture
4th Mar, Red Cross Headquarters, Lecture
4th Mar, Recap meeting
4

7th Mar, Red Cross in Leyte, Lecture
Daily Activities (3)
7th Mar, Red Cross in Leyte, Visiting WASH project site
8th Mar, JICA SMACHS-EV Project in Tolosa, Reception
7th Mar, Red Cross in Leyte, Lunch time
8th Mar, JICA SMACHS-EV Project in Tolosa, Visiting barangay health station
8th Mar, JICA SMACHS-EV Project in Dulag, Courtesy visit to the Mayor
5
8th Mar, Provincial health office, Leyte, Group photo
Daily Activities (4)
9th Mar, Preparation for final presentation
11th Mar, Final presentation, Reception
9th Mar, Preparation for final presentation
11th Mar, Final presentation at San Lazaro Hospital
11th Mar, Final presentation, Group photo after the presentation
6
Manila Intramuros
Casual Photos
Leyte Island
Food stand
On the way
Sightseeing in Leyte
Philippine cuisine
7

For everyone around the world “health” is irreplaceable. It is the same for our planet. How do we grasp
“health” as a “science” and respect “life” for the sustainable development of humans? In the 21st century,
globalization progresses rapidly in all fields and a variety of factors are mutually related creating complex
issues. To solve these global problems, it is essential to understand the current situation fully while continuing
to follow a specific direction with quick efficiency.
The School of Tropical Medicine and Global Health (TMGH) is intended to contribute to the fostering of
professionals in order to find solutions to global health problems alongside those from low-income countries
who must balance development with health issues. Though such talented people were lacking around the
world, particularly in Japan, large-scale graduate schools focused on public health and the institution of tropical
medicine were few in Japan.
In order to solve this problem, the Graduate School of International Health Development (Master course)
was established in 2008 at Nagasaki University. Here, in addition to classes that dealt with hygiene and public
health, comprehensive education regarding the natural environment, local situations, political circumstances,
economics, societies, and cultures was offered. Many of the young graduates from this School left for the field
and international organizations to work worldwide while others have been active in academia and research
institutes such as universities.
Changes in the world, however, occur more and more rapidly, especially in reference to “global health”.
When looking at the Ebola hemorrhagic fever in West Africa in 2014, then the example of the Middle East
Respiratory Syndrome (MERS) in South Korea that has finally subsided recently, one can’t help but think that
“the Earth is really connected”. Clearly, there is a need for a high degree of education and research in this field.
Therefore, in April 2015, TMGH was established as a new graduate school in Nagasaki University. TMGH aims
to further the development of high-level professionals in the field of global health. Our three courses, Tropical
Medicine (MTM), International Health Development (MPH), and Health Innovation (MSc) provide a variety of
learning experiences for each graduate student, motivating them to meet the requirements of research and
practice. In addition, in cooperation with the London School of Hygiene & Tropical Medicine which is leading
the world in global health studies, our School carries out education at a global level for students who are
internationally-oriented by using progressive instructions and integrating classroom education with in-field
practice.
The short-term field training in abroad during the first year of study for our MPH students is one of the key
subjects in our curriculum. Although my scientific background is biochemistry, I know field training is essential
for students in our School because I had a very valuable experience in Paraguay as a team leader for a JICA
project where I met many patients suffering from Chagas’ diseases and Leishmaniasis. This is why I have spent
much time studying parasites while attempting to discover and develop new drugs in order to help those in
need.
I hope that from this report you will have a better understanding of the activities and goals of TMGH.
Foreword
Kiyoshi KitaDean, School of Tropical Medicine and Global Health, Nagasaki University
8

The School of Tropical Medicine and Global Health (TMGH) at Nagasaki University was newly opened in October 2015. As a Master of Public Health (MPH) course at the School, International Health Development course welcomed 16 new students in its debut year, aiming to train them and their successors into health professionals who can contribute to solving global health problems. Through the very name of “International Health Development” we hope to convey our strong commitment to developing health-related status worldwide.
Entering into the 21st century, it has been made apparent that fundamental global health problems cannot be solved by relying on medicine and conventional public health alone. The promotion of problem-oriented education, research and practice, the integration of knowledge from development studies, international relations, development economics, area studies, social anthropology, pedagogy, environmental science, ecology, and many more aspects of our world are required. International Health Development, as an independent master program, is seeking to foster field-minded but sophisticated practitioners in global health.
The course’s two-year curriculum is characterized by the ‘short-term field training’ in developing countries during the first year and the ‘long-term field training’ conducted in the second year (5 month internship plus 3 month research). This report is a summary of the short-term field training which took place in the Republic of the Philippines from February 28th to March 12th, 2016. During these two weeks, students visited and observed field activities and sat in on lectures given by health professionals. Class discussions were held and a final presentation was also conducted. This experience was valuable for the students to prepare them for the long-term field training of their second year.
This year, the students were accompanied by Prof. Miho Sato (assistant professor) who was in charge of coordinating the entire trip, as well as Prof. Hisakazu Hiraoka (associate professor), Prof. Kota Yoshioka (assistant professor), and Mr. Masashi Teshima (second year student). They visited Manila and Leyte, observing and learning from various activities and organizations. This report has been compiled using the contents of the lectures held by the visited organizations, the students’ daily records, the summary presentation, and other materials gathered from the trip.
It is my hope that this report will be read by those who are actively working in, or are interested in, the area of international health. The commitment of the students to solving international health problems can be assessed through these reports and I would be greatly pleased if readers would be willing to share their feedback towards educational improvements of our School.
Finally, I would like to extend my profound thanks to all who provided valuable training opportunities to our students, including WHO/WPRO, JICA Philippines, San Lazaro Hospital, the Philippine Department of Health, RIT/JATA Philippines, Inc., Research Institute for Tropical Medicine, Philippine Red Cross, and more.
As a final note, please understand that the contents and data in this report were collected and described as a part of the students’ training and learning process. I would like to ask for your kind consideration if any of the information contained is inadequate or incomplete, and to please refrain from citing this report in any situation.
Foreword
Kazuhiko MojiDirector of International Health Development Course, School of Tropical Medicine and Global Health, Nagasaki University
9
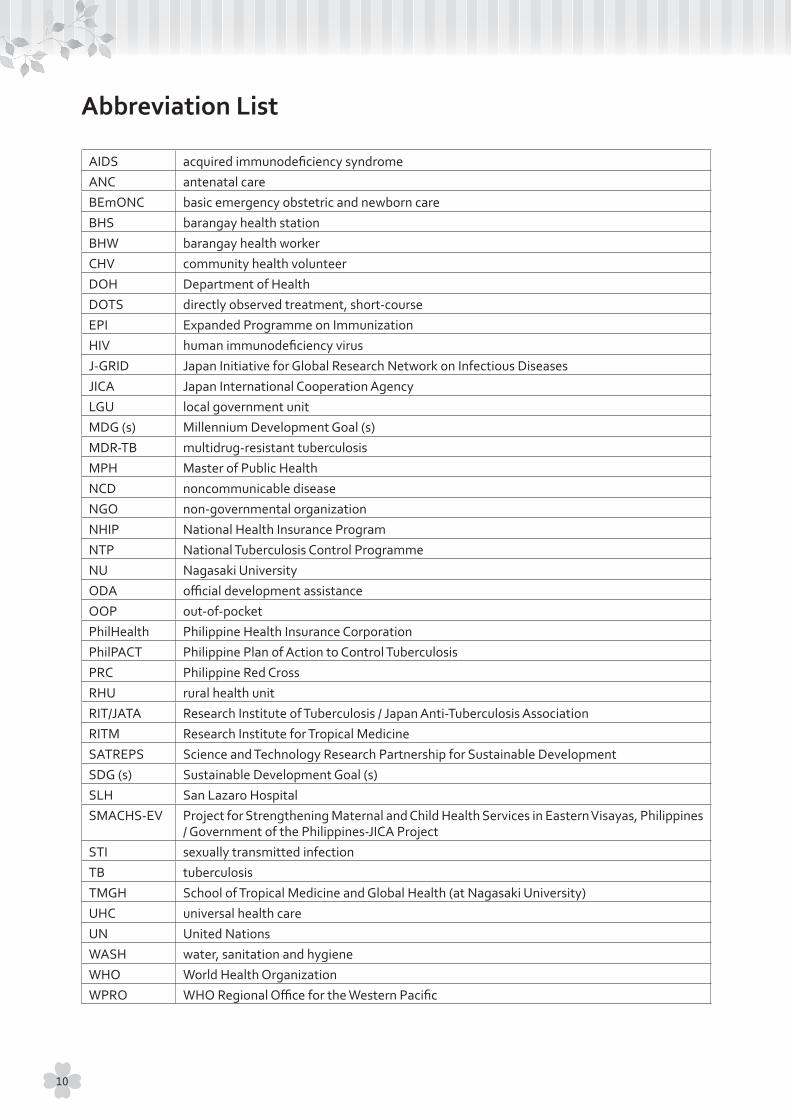
AIDS acquired immunodeficiency syndromeANC antenatal careBEmONC basic emergency obstetric and newborn careBHS barangay health stationBHW barangay health workerCHV community health volunteerDOH Department of HealthDOTS directly observed treatment, short-courseEPI Expanded Programme on ImmunizationHIV human immunodeficiency virusJ-GRID Japan Initiative for Global Research Network on Infectious DiseasesJICA Japan International Cooperation AgencyLGU local government unitMDG (s) Millennium Development Goal (s)MDR-TB multidrug-resistant tuberculosisMPH Master of Public HealthNCD noncommunicable diseaseNGO non-governmental organizationNHIP National Health Insurance ProgramNTP National Tuberculosis Control ProgrammeNU Nagasaki UniversityODA official development assistanceOOP out-of-pocketPhilHealth Philippine Health Insurance CorporationPhilPACT Philippine Plan of Action to Control TuberculosisPRC Philippine Red CrossRHU rural health unitRIT/JATA Research Institute of Tuberculosis / Japan Anti-Tuberculosis AssociationRITM Research Institute for Tropical MedicineSATREPS Science and Technology Research Partnership for Sustainable DevelopmentSDG (s) Sustainable Development Goal (s)SLH San Lazaro HospitalSMACHS-EV Project for Strengthening Maternal and Child Health Services in Eastern Visayas, Philippines
/ Government of the Philippines-JICA ProjectSTI sexually transmitted infectionTB tuberculosisTMGH School of Tropical Medicine and Global Health (at Nagasaki University)UHC universal health careUN United NationsWASH water, sanitation and hygieneWHO World Health OrganizationWPRO WHO Regional Office for the Western Pacific
Abbreviation List
10
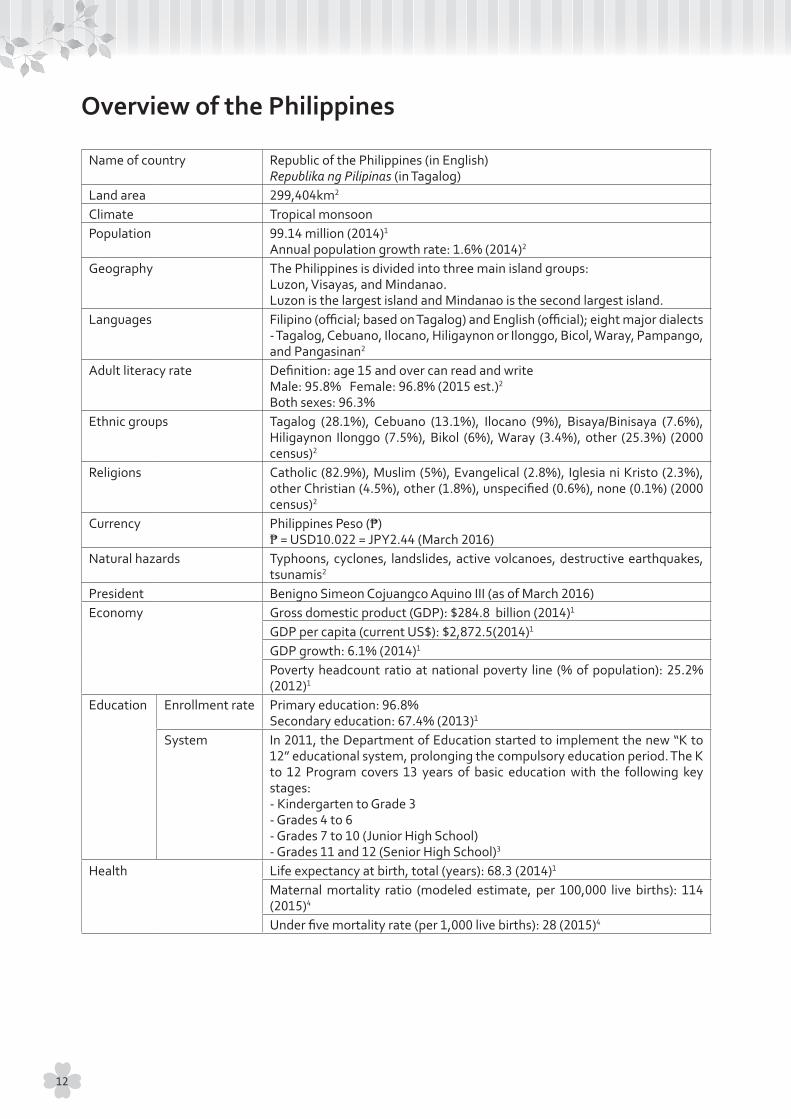
Name of country Republic of the Philippines (in English)Republika ng Pilipinas (in Tagalog)
Land area 299,404km2
Climate Tropical monsoonPopulation 99.14 million (2014)1
Annual population growth rate: 1.6% (2014)2
Geography The Philippines is divided into three main island groups:Luzon, Visayas, and Mindanao.Luzon is the largest island and Mindanao is the second largest island.
Languages Filipino (official; based on Tagalog) and English (official); eight major dialects - Tagalog, Cebuano, Ilocano, Hiligaynon or Ilonggo, Bicol, Waray, Pampango, and Pangasinan2
Adult literacy rate Definition: age 15 and over can read and writeMale: 95.8% Female: 96.8% (2015 est.)2
Both sexes: 96.3%Ethnic groups Tagalog (28.1%), Cebuano (13.1%), Ilocano (9%), Bisaya/Binisaya (7.6%),
Hiligaynon Ilonggo (7.5%), Bikol (6%), Waray (3.4%), other (25.3%) (2000 census)2
Religions Catholic (82.9%), Muslim (5%), Evangelical (2.8%), Iglesia ni Kristo (2.3%), other Christian (4.5%), other (1.8%), unspecified (0.6%), none (0.1%) (2000 census)2
Currency Philippines Peso (₱)₱ = USD10.022 = JPY2.44 (March 2016)
Natural hazards Typhoons, cyclones, landslides, active volcanoes, destructive earthquakes, tsunamis2
President Benigno Simeon Cojuangco Aquino III (as of March 2016)Economy Gross domestic product (GDP): $284.8 billion (2014)1
GDP per capita (current US$): $2,872.5(2014)1
GDP growth: 6.1% (2014)1
Poverty headcount ratio at national poverty line (% of population): 25.2% (2012)1
Education Enrollment rate Primary education: 96.8%Secondary education: 67.4% (2013)1
System In 2011, the Department of Education started to implement the new “K to 12” educational system, prolonging the compulsory education period. The K to 12 Program covers 13 years of basic education with the following key stages:- Kindergarten to Grade 3- Grades 4 to 6- Grades 7 to 10 (Junior High School)- Grades 11 and 12 (Senior High School)3
Health Life expectancy at birth, total (years): 68.3 (2014)1
Maternal mortality ratio (modeled estimate, per 100,000 live births): 114 (2015)4
Under five mortality rate (per 1,000 live births): 28 (2015)4
Overview of the Philippines
12
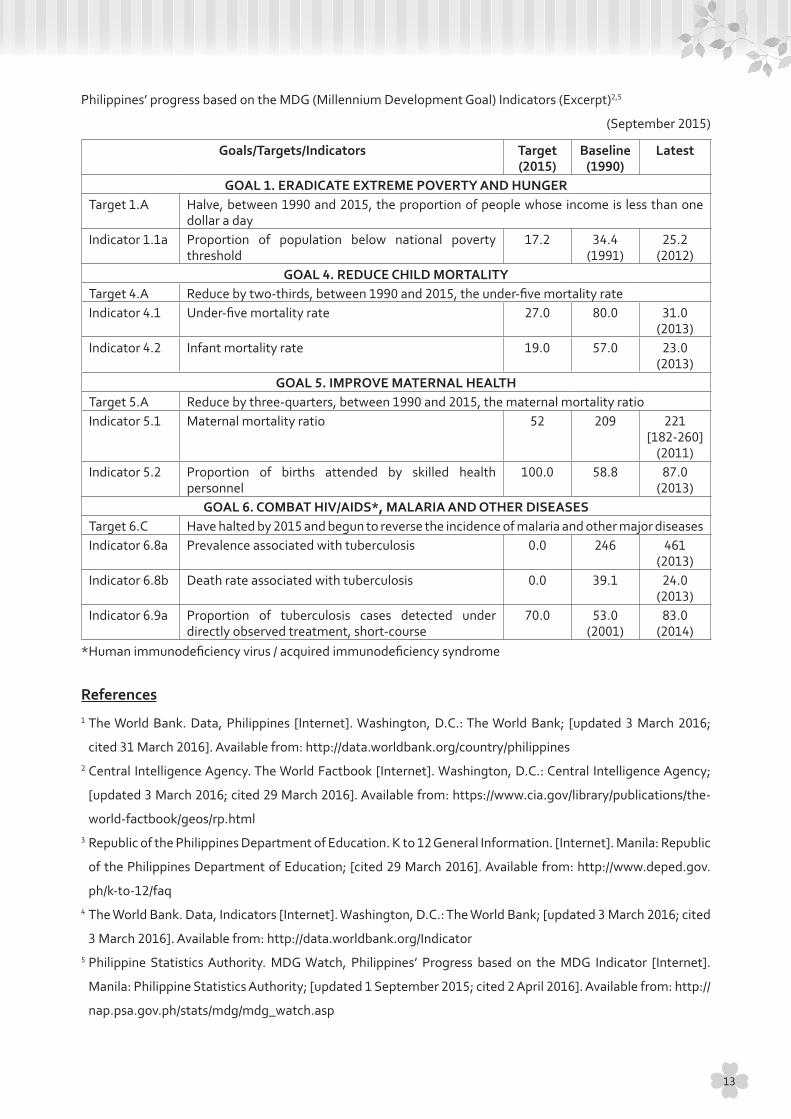
Philippines’ progress based on the MDG (Millennium Development Goal) Indicators (Excerpt)2,5
(September 2015)
Goals/Targets/Indicators Target(2015)
Baseline(1990)
Latest
GOAL 1. ERADICATE EXTREME POVERTY AND HUNGERTarget 1.A Halve, between 1990 and 2015, the proportion of people whose income is less than one
dollar a dayIndicator 1.1a Proportion of population below national poverty
threshold17.2 34.4
(1991)25.2
(2012)GOAL 4. REDUCE CHILD MORTALITY
Target 4.A Reduce by two-thirds, between 1990 and 2015, the under-five mortality rateIndicator 4.1 Under-five mortality rate 27.0 80.0 31.0
(2013)Indicator 4.2 Infant mortality rate 19.0 57.0 23.0
(2013)GOAL 5. IMPROVE MATERNAL HEALTH
Target 5.A Reduce by three-quarters, between 1990 and 2015, the maternal mortality ratioIndicator 5.1 Maternal mortality ratio 52 209 221
[182-260](2011)
Indicator 5.2 Proportion of births attended by skilled health personnel
100.0 58.8 87.0(2013)
GOAL 6. COMBAT HIV/AIDS*, MALARIA AND OTHER DISEASESTarget 6.C Have halted by 2015 and begun to reverse the incidence of malaria and other major diseasesIndicator 6.8a Prevalence associated with tuberculosis 0.0 246 461
(2013)Indicator 6.8b Death rate associated with tuberculosis 0.0 39.1 24.0
(2013)Indicator 6.9a Proportion of tuberculosis cases detected under
directly observed treatment, short-course70.0 53.0
(2001)83.0
(2014)*Human immunodeficiency virus / acquired immunodeficiency syndrome
References1 The World Bank. Data, Philippines [Internet]. Washington, D.C.: The World Bank; [updated 3 March 2016;
cited 31 March 2016]. Available from: http://data.worldbank.org/country/philippines2 Central Intelligence Agency. The World Factbook [Internet]. Washington, D.C.: Central Intelligence Agency;
[updated 3 March 2016; cited 29 March 2016]. Available from: https://www.cia.gov/library/publications/the-
world-factbook/geos/rp.html3 Republic of the Philippines Department of Education. K to 12 General Information. [Internet]. Manila: Republic
of the Philippines Department of Education; [cited 29 March 2016]. Available from: http://www.deped.gov.
ph/k-to-12/faq4 The World Bank. Data, Indicators [Internet]. Washington, D.C.: The World Bank; [updated 3 March 2016; cited
3 March 2016]. Available from: http://data.worldbank.org/Indicator5 Philippine Statistics Authority. MDG Watch, Philippines’ Progress based on the MDG Indicator [Internet].
Manila: Philippine Statistics Authority; [updated 1 September 2015; cited 2 April 2016]. Available from: http://
nap.psa.gov.ph/stats/mdg/mdg_watch.asp
13
1. Objectives
· To deepen students’ insight and to enhance their understanding on the importance of the practical
utilization of basic knowledge
· To motivate students to pursue global health practices through exposure to model health improvement
activities and research fields
2. Method
· From 28th February to 12th March, 2016, students visited several organizations:
❖ World Health Organization Regional Office for the Western Pacific (WHO/WPRO)
❖ Japan International Cooperation Agency (JICA) Philippines
❖ San Lazaro Hospital (SLH)
❖ Department of Health (DOH)
❖ Research Institute of Tuberculosis/ Japan Anti-Tuberculosis Association (RIT/JATA) Philippines,
Inc.
❖ Research Institute for Tropical Medicine (RITM)
❖ Philippines Red Cross (PRC)
❖ Others
· Students had an opportunity to sit in on lectures at each place, to attend a conference, and to discuss
health issues in the Philippines.
· Students gained experience regarding logistic management and developed necessary skills for activities
related to global health.
· Students acquired group discussion and facilitation skills by participating in daily recap meetings as well
as by making a final presentation.
· Students discussed their ideas regarding each facility they visited and wrote a report on what they
learned through this field trip.
3. Supporting Organization and People
Supervising Professors
Prof. Miho Sato Assistant Professor, Nagasaki University School of Tropical Medicine and Global Health
Prof. Kota Yoshioka Assistant Professor, Nagasaki University School of Tropical Medicine and Global Health
Prof. Hisakazu Hiraoka(Feb 28th to Mar 5th)
Associate Professor, Nagasaki University School of Tropical Medicine and Global Health
AccompanyingStudent
Mr. Masashi Teshima MPH course student (7th batch), Graduate School of International Health Development, Nagasaki University
Overview of the Field Trip
14
Supporting Organizations
Asian Health Institute (for preparatory lecture)JICA/ Japan International Cooperation Center (JICE) for the international students supported by the Japanese Grant Aid for Human Resource Development Scholarship (JDS)Japan Student Services Organization (JASSO)Student Support Department, Nagasaki University
4. Participating Students
▷ Nobuya Goto
▷ Satomi Ichino
▷ Aiko Inoue
▷ Khin Zar Wai
▷ Ryo Kobayashi
▷ Asuka Miyazaki
▷ Shoko Ogino
▷ Masanobu Ono
▷ Takuya Shizume
▷ Kumiko Takai
▷ Noriko Tamari
▷ Reiri Tsumura
▷ Meguru Yamamoto
▷ Erika Yoshimoto
▷ Yasue Yoshino
▷ Zar Lwin Hnin
5. Schedule of Trip
Date AM/PM Schedule28/Feb. SUN Flight from Fukuoka to Manila29/Feb. MON AM Cultural/historical program: Manila Intramuros
PM Department of Health1/Mar. TUE AM WHO/WPRO
The Tenth National TB Programme Managers Meeting in the Western Pacific Region
PM JICA Philippines Office2/Mar. WED AM/PM San Lazaro Hospital3/Mar. THU AM A.A. Zapa Health Center in Caloocan City
PM RIT/JATA Philippines, Inc.4/Mar. FRI AM Research Institute for Tropical Medicine
PM Philippine Red Cross Headquarters5/Mar. SAT Flight from Manila to Tacloban6/Mar. SUN AM/PM Cultural/historical program in Leyte7/Mar. MON AM/PM Philippine Red Cross Leyte Chapter8/Mar. TUE AM/PM JICA Project for Strengthening Maternal and Child Health Services in
Eastern Visayas (SMACHS-EV Project)DOH Regional Office 8Field sites (Dulag, Tolosa)Leyte Provincial Health OfficeLeyte Provincial Hospital
9/Mar. WED AM/PM Preparation for the final presentation10/Mar. THU Flight from Tacloban to Manila
PM Internal meeting/discussions11/Mar. FRI AM WHO/WPRO
PM Final presentation12/Mar. SAT Flight from Manila to Fukuoka
15
6. Persons met at visiting sites
Visiting sites Lecturers and CoordinatorsDOH ❖ Dr. Gloria Nenita Velasco, Medical Officer IV
❖ Dr. Juanita H. Fandiño, Human Resource Management Officer❖ Ms. Jocelyn T. Sosito, Senior Health Program Officer❖ Mr. Shogo Kanamori, JICA Health Advisor
WHO/WPRO ❖ Dr. Tomohiko Makino, Medical Officer❖ Dr. Nobuyuki Nishikiori, Coordinator❖ Ms. Mina Kashiwabara, Technical Officer❖ Dr. Aya Yajima, Technical Officer
JICA Philippines Office ❖ Ms. Eri Asada-Solleza, NGO Coordinator❖ Mr. Patrick Adams G.San Juan, Program Officer❖ Ms. Teresa Mendoza, Program Officer
SLH ❖ Dr. Carina H. Frayco❖ Dr. Rhona Fulgar❖ Dr. Lynsil Roy❖ Dr. Flora P. Marin❖ Dr. Marietta Solomte❖ Mr. Paul Solano
NU-SLH Collaborative Office
❖ Dr. Nobuo Saito
A. A. Zapa Health Center ❖ Dr. Panfilo B. Solano Jr., Medical OfficerRIT/JATA Philippines, Inc. ❖ Ms. Aurora G. Querri, Deputy Executive DirectorRITM ❖ Mr. Rex J. Centeno, Senior Science Research Specialist
❖ Mr. Neil Tristan M. Yabut, Science Research SpecialistRITM (Tohoku Team) ❖ Dr. Hitoshi Oshitani, SATREPS Chief Advisor, Professor, Tohoku University
Graduate School of Medicine❖ Dr. Raita Tamaki, SATREPS Expert, Assistant Professor❖ Mr. Ryosuke Kojima, SATREPS Coordinator, JICA❖ Dr. Mariko Saito, J-GRID Expert, Assistant Professor❖ Dr. Emiko Nakagawa, J-GRID Coordinator, Research Associate
PRC Headquarters ❖ Dr. Gwendolyn Pang, Secretary General❖ Ms. Norwina D. Eclarinal, Officer in Charge❖ Mr. Briccio L. Echo Jr., Emergency Field Hospital Officer❖ Mr. Alv Jordan V. Manansala, International Relations Officer❖ Ms. MayCarol Z. Layugan, Operations Center Manager
PRC Leyte Chapter ❖ Mr. Leo Haniff C. Ko, Field Operations Head❖ Ms. Ma Jessilou Marigo❖ Ms. Ethel Villodres❖ Mr. Hebert M Quijano
DOH Regional Office 8 ❖ Dr. Minerva P. Molon, Director IV, Regional Health Office8Leyte Provincial Health Office and Leyte Provincial Hospital
❖ Dr. Ofelia C. Absin, Officer in Charge, Chief of Leyte Provincial Hospital
JICA SMACHS - EV Project Office
❖ Ms. Chisaki Sato, Training/Project Coordinator❖ Ms. Lucila C. Loterte, Local Senior Project Coordinator❖ Ms. Esther Ruth Amable, Local Project Coordinator
Dulag MunicipalityRural Health Unit,Barangay Health Station
❖ Mr. Manuel Siaque, Mayor❖ Dr. Allan B. Alvarez, Municipal Health Officer
Tolosa MunicipalityRural Health Unit,Barangay Health Station
❖ Mr. Erwin C. Ocaña, Mayor❖ Dr. Ma. Aurora Lyn R. Benitez, Municipal Health Officer
16

Department of Health (DOH), Health Human Resource Development Bureau
Site Overview and Background
The DOH is the executive health department of
the Philippines government. It is responsible for
ensuring access to fundamental public health services
for all Filipinos through the provision of quality
healthcare, and the regulation of health providers,
services and products.1 The Philippines’ health care
service is decentralized; the country has 17 DOH
Regional Offices, 82 Provincial Health Offices, 38 City
Health Offices, and 865 Municipal Health Offices.2
Agenda
1. Philippines Health System
1-1. Health status and population transition
Health in the Philippines has improved dramatically
over the last two decades. According to data from
the MDGs, life expectancy at birth increased from
68.1 in 1999 to 71.8 in 2014 for women and 62.6 in
1990 to 64.9 in 2014 for men.3,4 During the MDG era,
under-five mortality rate and malaria infection
decreased significantly for past two decades,
however, tuberculosis (TB) is still a major burden in
the Philippines. Although maternal mortality ratio
has also been decreasing, it could not reach the MDG
targets.5
The Philippines total population boomed from
66.9 million in 1990 to 99.1 million in 2014.6 In recent
years, a demographic transition has also occurred in
that the proportion of children in the population has
gradually decreased when compared to those of
working-age and the elderly.7
1-2. Causes of death
According to the data on causes of death in 2010,
the most common causation was heart disease
(102,936 cases, 109.5 per 100,000 populations),
while TB (24,714 cases, 26.3 per 100,000 populations)
ranked sixth.8 The proportion of deaths caused by
noncommunicable diseases (NCDs) has increased
while that of infectious diseases has decreased.7
1-3. Overview of the health system
The health system of the Philippines consists of a
public sector and a private sector. The public sector’s
financing is based on taxes. In 1991, the health
service was delegated to the local governments.
Under the leadership of the DOH, local government
units (LGUs) became responsible as direct service
providers. As a result, this system led to the
fragmentation of health services in the Philippines.
For the private sector, a lot of actors including “for-
profit and non-profit” health providers such as clinics,
hospitals, health insurance service providers, health
products providers, and research and academic
institutions are taking part in the health system.
According to data in 2013, the number of private
hospitals accounted for 63% of the total number of
hospitals in the Philippines. Thus, in addition to
public hospitals, private hospitals also play an
important role in the country.9
1-4. PhilHealth and healthcare financing in the
Philippines
The proportion of out-of-pocket (OOP) health
expenditures in the Philippines has been relatively
high. This means that indigent people can easily fall
into financial difficulties just by paying for health
services. To improve this situation, the Philippine
Health Insurance Corporation (PhilHealth) was
established in 1995. The PhilHealth is a government-
owned and controlled corporation that deals with
29th February
18
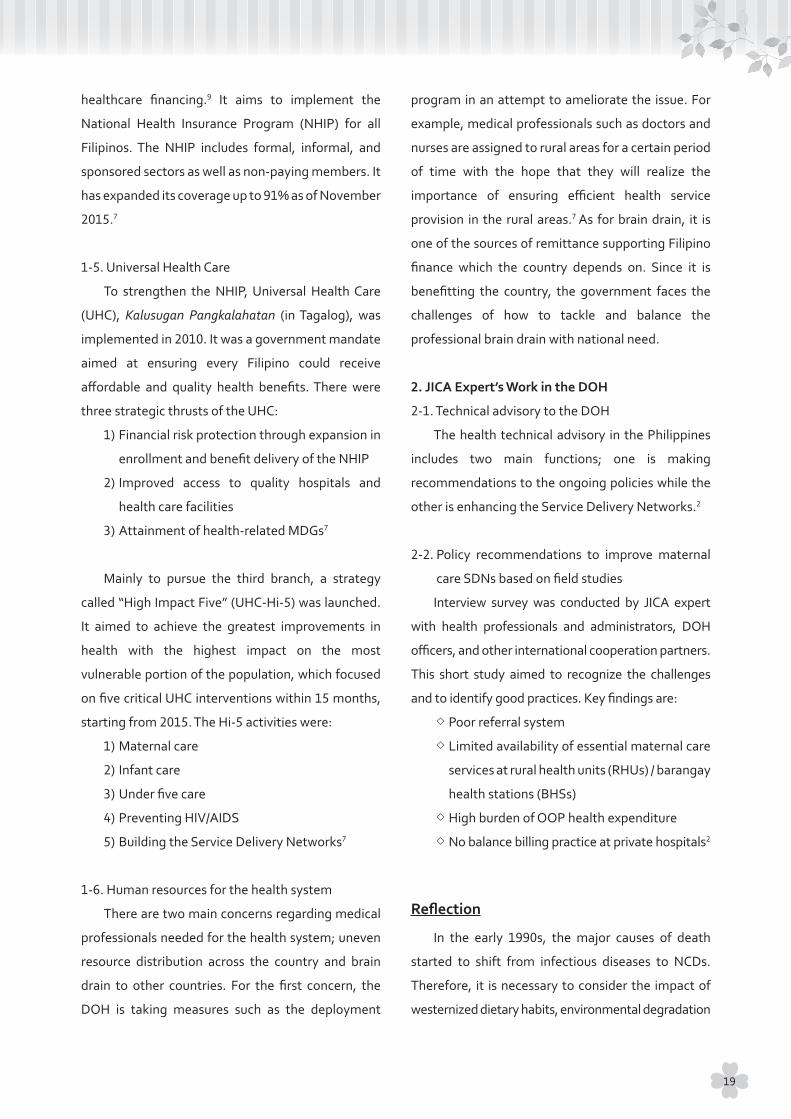
healthcare financing.9 It aims to implement the
National Health Insurance Program (NHIP) for all
Filipinos. The NHIP includes formal, informal, and
sponsored sectors as well as non-paying members. It
has expanded its coverage up to 91% as of November
2015.7
1-5. Universal Health Care
To strengthen the NHIP, Universal Health Care
(UHC), Kalusugan Pangkalahatan (in Tagalog), was
implemented in 2010. It was a government mandate
aimed at ensuring every Filipino could receive
affordable and quality health benefits. There were
three strategic thrusts of the UHC:
1) Financial risk protection through expansion in
enrollment and benefit delivery of the NHIP
2) Improved access to quality hospitals and
health care facilities
3) Attainment of health-related MDGs7
Mainly to pursue the third branch, a strategy
called “High Impact Five” (UHC-Hi-5) was launched.
It aimed to achieve the greatest improvements in
health with the highest impact on the most
vulnerable portion of the population, which focused
on five critical UHC interventions within 15 months,
starting from 2015. The Hi-5 activities were:
1) Maternal care
2) Infant care
3) Under five care
4) Preventing HIV/AIDS
5) Building the Service Delivery Networks7
1-6. Human resources for the health system
There are two main concerns regarding medical
professionals needed for the health system; uneven
resource distribution across the country and brain
drain to other countries. For the first concern, the
DOH is taking measures such as the deployment
program in an attempt to ameliorate the issue. For
example, medical professionals such as doctors and
nurses are assigned to rural areas for a certain period
of time with the hope that they will realize the
importance of ensuring efficient health service
provision in the rural areas.7 As for brain drain, it is
one of the sources of remittance supporting Filipino
finance which the country depends on. Since it is
benefitting the country, the government faces the
challenges of how to tackle and balance the
professional brain drain with national need.
2. JICA Expert’s Work in the DOH
2-1. Technical advisory to the DOH
The health technical advisory in the Philippines
includes two main functions; one is making
recommendations to the ongoing policies while the
other is enhancing the Service Delivery Networks.2
2-2. Policy recommendations to improve maternal
care SDNs based on field studies
Interview survey was conducted by JICA expert
with health professionals and administrators, DOH
officers, and other international cooperation partners.
This short study aimed to recognize the challenges
and to identify good practices. Key findings are:
❖ Poor referral system
❖ Limited availability of essential maternal care
services at rural health units (RHUs) / barangay
health stations (BHSs)
❖ High burden of OOP health expenditure
❖ No balance billing practice at private hospitals2
Reflection
In the early 1990s, the major causes of death
started to shift from infectious diseases to NCDs.
Therefore, it is necessary to consider the impact of
westernized dietary habits, environmental degradation
19

due to industrialization, and the widening economic
disparity. On the other hand, the number of patients
suffering from communicable diseases such as TB is
still high, which requires continuous efforts on a
public health approach, health promotion, and
health education.
The challenges relating to health professionals
such as uneven distribution of medical professionals
in the country and brain drain of medical professionals
to overseas are difficult to tackle, however, the
country’s deployment system has the potential to
make the situation better. Not only increasing the
number of medical students, but considering the
quality of education to retain students could be
another solution to these challenges.
Different perspectives can help further push
improvements in healthcare in the Philippines. By
sharing experiences in other developing countries
and Japan, the JICA experts push the DOH to broaden
its scope which can help to identify unrecognized
problems and discover new approaches to the
current situation.
References1 Republic of the Philippines Department of Health.
About us [Internet]. Manila: Republic of the
Philippines Department of Health; [cited 31 May
2016]. Available from:
http://www.doh.gov.ph/about-us
2 Overview of JICA Expert’s Work at Department of
Health, Philippines [unpublished lecture notes].
Japan International Cooperation Agency; notes
provided at lecture given 29 February 2016.
3 The World Bank. World DataBank, World Development
Indicators [Internet]. Washington, D.C.: The World
Bank; [cited 30 March 2016]. Available from:
http://databank.worldbank.org/data/reports.
aspx?source=2&country=&series=SP.DYN.LE00.
FE.IN&period=
4 The World Bank. World DataBank, World Development
Indicators [Internet]. Washington, D.C.: The World
Bank; [cited 30 March 2016]. Available from:
http://databank.worldbank.org/data/reports.
aspx?source=2&country=&series=SP.DYN.LE00.
MA.IN&period=
5 Republic of the Philippines Philippine Statistics
Authority. MDG Watch, Statistics at a glance of the
Philippines’ Progress based on the MDG indicators
[Internet]. Quezon City: Republic of the Philippines
Philippine Statistics Authority [cited 12 April 2016].
Available from:
http://www.nscb.gov.ph/stats/mdg/mdg_watch. asp
6 The World Bank. World DataBank, World Development
Indicators [Internet]. Washington, D.C.: The World
Bank; [cited 30 March 2016]. Available from:
http://databank.worldbank.org/data/reports.
a s p x? s o u r c e = 2 & c o u n t r y = & s e r i e s = S P. P O P.
TOTL&period=
7 The Philippine Health System [unpublished lecture
notes]. Department of Health; notes provided at
lecture given 29 February 2016.
8 Republic of the Philippines Department of Health
National Epidemiology Center. The 2010 Philippine
Health Statistics [Internet]. Manila: Republic of the
Philippines Department of Health National
Epidemiology Center; [cited 20 March 2016].
Available from:
http:/ /www.doh.gov.ph/sites/default/f i les/
publications/PHS2010_March13.compressed.pdf
20

9 Asia Pacific Observatory on Health Systems and
Policies. The Philippines Health System Review,
Health Systems in Transition Vol. 1 No.2 2011
[Internet]. Manila: World Health Organization
Representative Office Philippines; [cited 4 April
2016]. Available from:
http://www.wpro.who.int/philippines/areas/
health_systems/financing/philippines_health_
system_review.pdf
21

World Health Organization Regional Office for the Western Pacific (WHO / WPRO)
Site Overview and Background
WHO is an organization which deals with global
health issues as an United Nations (UN) agency. With
an initial membership of 61 countries, the number of
member states has more than tripled to 194 as of
March 2016.1,2 WHO has six regional offices and 149
country offices around the world.3 Countries are not
necessarily divided into regions based on their
geographical location. For example, Pakistan belongs
to the East Mediterranean region, although the
Southeast Asia regional office, located in New Delhi,
India, is the closest to the country.4 WPRO is one of
the regional offices of the WHO. It covers 37 countries
and areas and serves approximately 1.8 billion
people.5 WPRO consists of one head office located in
Manila, and 15 country offices in the region with 640
employees as of March 2016.6,7 Since the region
contains countries which vary greatly in regards to
development, from developing countries like
Cambodia and Lao People’s Democratic Republic to
developed countries like Australia and Japan, health
situations are different from country to country.5
Agenda
1. Briefing on WHO from Dr. Makino and Dr.
Nishikiori
Japan has been contributing to UN agencies
including WHO as a member state for around 60
years. The main roles for Japan as a developed
country are financial support and human resource
contribution.7 Financial support can be divided into
two aspects; assessed contribution and voluntary
contribution.7,8 Assessed contribution is mandatory for
all member states of the organization.8 Voluntary
contribution is additional contribution given by the
member states and others.7 Japan is the fifth highest
contributor in the organization.7 Considering the
amount of the annual budget contributed to the UN
system, Japan is one of the under-represented countries
in terms of human resources allocation in the system.7
2. Observing the Tenth National TB Programme
Managers Meeting in the Western Pacific Region
During the visit to the WPRO, there was a regional
TB conference. Experts from various organizations
and representatives from member states in the region
participated in the conference with several observers
in the room. The contents of the meeting in the
opening session consisted of an overview of the
agenda and a brief discussion based on lectures and
reports from participants. It was a closed conference
focusing its discussion on the “End TB Strategy”.
Reflection
WHO sets global goals and plays a vital role for
elevating the health of people around the world. It
faces challenges, however, in translating the global
agenda to local strategies. In the conference convened
by WPRO, participants actively discussed topics based
on not only the global situation but also their own
experiences and the situations in their home countries.
1st March (AM)
22
These processes can help draft necessary plans for the
region and to help shape a common understanding of
the magnitude of the existing problems that threaten
the health of the world. WHO exercises its convening
power to share and capture a diverse set of
perspectives and knowledge to find solutions to
overcome current health issues. Putting aside the
issues of political interest and financial contribution,
Japan has tremendous experience and expertise in
the public health field which can be disseminated,
applied, and replicated across the world.
References1 World Health Organization. WHO definition of Health
[Internet]. Geneva: World Health Organization; [cited
20 March 2016]. Available from:
http://www.who.int/about/definition/en/print.html
2 World Health Organization Representative Office
Philippines. About WHO in the Philippines,
Governance [Internet]. Manila: World Health
Organization Representative Office Philippines;
[cited 20 March 2016]. Available from:
http://www.wpro.who.int/philippines/about/story_
governance_in_WHO/en/
3 World Health Organization. WHO’s work with
countries, Where WHO works [Internet]. Geneva:
World Health Organization [cited 20 March 2016].
Available from:
http://www.who.int/country-cooperation/where-
who-works/en/
4 World Health Organization. About WHO, Regional
offices for East Mediterranean [Internet]. Geneva:
World Health Organization [cited 25 March 2016].
Available from:
http://www.who.int/about/regions/emro/en/
5 World Health Organization Western Pacific Region.
Countries and areas [Internet]. Manila: World
Health Organization Western Pacific Region; [cited
20 March 2016]. Available from:
http://www.wpro.who.int/countries/en/
6 World Health Organization Western Pacific Region.
WHO in the Western Pacific, Offices [Internet].
Manila: World Health Organization Western Pacific
Region; [cited 20 March 2016]. Available from:
http://www.wpro.who.int/about/offices/en/
7 Cooperation between WHO and Japan, 1. Financial
Contribution [in Japanese] [unpublished lecture
notes]. World Health Organization Western Pacific
Regional Office; notes provided at lecture given 1
March 2016.
8 World Health Organization. About WHO, Assessed
contribution [Internet]. Geneva: World Health
Organization; [cited 20 March 2016]. Available from:
http://www.who.int/about/finances-accountability/
funding/assessed-contributions/en/
23

Japan International Cooperation Agency (JICA) Philippines Office
Site Overview and Background
JICA conducts several projects including health
projects in the Philippines through technical
cooperation, yen loan, grant aid, and Japan Overseas
Cooperation Volunteers (JOCV). The Philippines is the
third largest recipient country of technical cooperation
by JICA.1,2 Moreover, in terms of total official
development assistance (ODA) by development
partner, Japan was the second largest donor in the
Philippines in 2014.2 The government of Japan
considers the following three points as priorities for its
ODA to the Philippines, which were formulated based
on discussions between the governments of the
Philippines and Japan:
1) Achieving sustainable economic growth through
further promotion of investment (transportation,
energy, infrastructure, governance, etc.)
2) Overcoming vulnerability and stabilizing
bases for human life and production (disaster,
environment, health, agriculture, etc.)
3) Peace and development in Mindanao2,3
Agenda
1. JICA’s Assistance to the Health Sector in the
Philippines
With a combination of hard and soft components,
the current technical cooperation mainly focuses on
maternal and child healthcare and infection control.
From 2006, the focused target areas have been the
Cordillera Administrative Region and the Eastern
Visayas Region.4 Steady progress can be seen in
these two areas.
Current ongoing JICA projects in these regions
include:
❖ JICA Expert on Health Sector (2013-2016)
❖ Project for Strengthening Maternal and Child
Health Services in Eastern Visayas (2010-2016)
❖ Grant Aid Program for Rehabilitation and
Recovery from Typhoon Yolanda* (2014-2017)
❖ Comprehensive Etiological and Epidemiological
Study on Acute Respiratory Infections in Children
(2011-2017)
❖ Project for Cordillera-wide Strengthening of
the Local Health System for Effective and
Efficient Delivery of Maternal and Child Health
Services (2012-2017)
❖ Capacity Development of Public-Private-
Partnership Project Formulation (2014-2016)4
* Typhoon Yolanda internationally known as Typhoon Haiyan.
2. JICA’s Assistance in Typhoon Haiyan Affected
Areas
Based on the Philippines’ national policies of
“Build Back Better” and “Faster and Safer”, JICA has
three objectives:
1) Re-establishment of safer communities
2) Recovery of people’s daily life
3) Restoration of local economy5
In alignment with the above objectives, one of
the interventions introduced was a tide embankment
project to protect communities from the risks of
being wiped out should there be a tidal surge.
Another innovation implemented was designing and
building schools in the Piloti style which lifts buildings
above the ground while still allowing water to flow
below them. This can not only minimize the impact
on the buildings caused by water pressure, but it can
also serve as an evacuation place and accommodate
people on the second floor in case of emergencies.
1st March (PM)
24

Reflection
As Japan is a natural disaster prone country, JICA
incorporates lessons learned from Japan’s disaster
experiences to design their projects in close
communication with the government of the Philippines.
Designing and creating a ‘Hazard Map’ is one good
example of technical support provided by JICA.
Engaging relevant stakeholders, including local
governments, the project focuses on community
capacity building by conducting emergency drills and
providing training to raise awareness of disaster
response and how to appropriately use tools such as
the Hazard Map in cases of emergency. Such efforts
were put into an effect when another typhoon hit the
Philippines the year following Typhoon Haiyan. This
time, the communities and the people were much
more prepared and were capable of protecting
themselves while minimizing damages. Through
disaster recovery, the government and local
communities have learned the importance of disaster
preparedness with proactive measures in place.
References1 Japan International Cooperation Agency. JICA
Supplement to the Annual Report 2015 [Internet].
Tokyo: Japan International Cooperation Agency;
November 2015 [cited 20 March 2016]. Available
from:
http://www.jica.go.jp/english/publications/reports/
annual/2015/c8h0vm00009q82bm-att/2015_
supplement_all.pdf
2 JICA Operations in the Philippines [unpublished
lecture notes]. Japan International Cooperation
Agency; notes provided at lecture given 1 March 2016.
3 Embassy of Japan in the Philippines. Country
Assistance Policy for the Republic of the Philippines
[Internet]. Tokyo: Ministry of Foreign Affairs of Japan;
April 2012 [cited 20 March 2016]. Available from:
http://www.ph.emb-japan.go.jp/bilateral/image/
oda%202010%20update/countryassistancepolicy.
4 JICA’s assistance to the Health Sector in the
Philippines [unpublished lecture notes]. Japan
International Cooperation Agency; notes provided
at lecture given 1 March 2016.
5 JICA’s assistance in Typhoon Yolanda affected areas
[unpublished lecture notes]. Japan International
Cooperation Agency; notes provided at lecture
given 1 March 2016.
25
San Lazaro Hospital (SLH)
Site Overview and Background
Founded in 1577, SLH is one of the special
tertiary hospitals of the DOH specializing in infectious
diseases with a 500 bed-capacity.
The purpose of the visit was to learn about the roles
and activities of SLH through briefings and a hospital
tour, with a focus on its hospital-based TB program.1
Agenda
1. General Information of SLH
1-1. Characteristics of the patients
The total number of admitted patients in 2015
was 11,087. Among inpatients, records showed that:
❖ Dengue fever/dengue hemorrhagic fever
(36%)
❖ Pulmonary TB (21%)
❖ TB meningitis (1%)
❖ Pneumonia (10%)
❖ HIV/AIDS (4%)
❖ Snake bite (3%)
❖ Tetanus (2%)
❖ Leptospirosis (1%)
❖ Rabies (1%)
❖ Measles (1%)
❖ Typhoid fever (<1%)
❖ Diphtheria (<1%)
❖ Others
Fatality rates for pulmonary TB and TB meningitis
were 34.5% and 41.5% respectively. The number of
patients, particularly those with dengue fever/dengue
hemorrhagic fever and leptospirosis, increased after
typhoons and during rainy seasons.2*
1-2. User fee
For the most part, patients are covered by the
PhilHealth. According to SLH criteria, the payments
depend on their income. As most patients at SLH are
classified to be in the low income group, they are not
required to pay.
1-3. Laboratories
SLH is a designated hospital which treats
infectious diseases such as Ebola, Middle East
Respiratory Syndrome (MERS), avian influenza, and
rabies. There are specialized rooms for treating
terminal rabies patients. It has various laboratories
to carry out diagnostic tests and research, including
the national reference laboratory for HIV/AIDS,
hepatitis, and sexually transmitted infections (STIs).2
1-4. Collaboration with Nagasaki University (NU)
SLH and NU have joint collaboration to further
2nd March
26

promote research activities and clinical training of
both institutions.
2. TB Program in SLH
2-1. Outpatients
As a general routine, SLH offers directly observed
treatment, short-course (DOTS) which begins at 6
a.m. so that patients can receive treatment before
going to work.
Upon completion of DOTS, multidrug-resistant
tuberculosis (MDR-TB) patients are entitled to
receive a “reward” of 20,000 Philippine pesos as an
incentive, which is funded by the Global Fund. In
order to ensure that patients will complete the
treatment, the “reward” is distributed weekly (150
pesos/week) as an allowance. This motivates TB
patients to continue their treatment. At the same
time, the monitoring system keeps track of the
patients to prevent them from quitting their
treatment. If a patient fails to show up to receive
their medications, a hospital staff will visit their
house for a follow-up. SLH has a relationship with
LGUs to report and share information about the
progress and activities of the ongoing TB program.
TB education is provided to not only patients but
also their family members during waiting time, using
visual aids. Peer education is also carried out by
former TB patients.
2-2. Inpatients
Since family members stay with the patients to
take care of their daily needs, they have a higher risk of
becoming infected. Therefore, SLH provides them with
a TB screening test, vaccinations, and TB education.
The TB ward has difficulties in its bed-controlling
as some patients who are not required for further
admissions refuse to leave the hospital, because the
hospital provides them with free meals and more
comfortable accommodations than their homes.
Reflection
Currently the SLH TB program is sustained by
the Global Fund. Depending on such external funding
is not self-generating, thus, it is not promising in the
long-term run. A new framework or strategy that
engages the patients to be actively involved with
their treatment is necessary since the TB treatment
should be patient-oriented. This can be achieved by
fostering an enabling environment and ensuring
financial support for the patients.
References1 Department of Health, San Lazaro Hospital. San
Lazaro Hospital Today [Internet]. Manilla: Republic
of the Philippines Department of Health; [cited 28
May 2016]. Available from:
http://slh.doh.gov.ph/index.php/2-uncategorised/8-
san-lazaro-hospital-today
2 Nagasaki University SLH Project [unpublished
lecture notes]. SLH-Nagasaki Collaborative
research laboratory and office; notes provided at
lecture given 2 March 2016.* Data provided by Dr. Eumelia P. Salva, Department
of Epidemiology, San Lazaro Hospital
27
A.A. Zapa Health Center in Caloocan City, Manila
Site Overview and Background
The Caloocan area is a densely-populated area in
Manila. The A.A. Zapa Health Center is one of the
community clinics based in this area which provides
free healthcare.
The objective of this site visit was to understand
the role of barangay health worker (BHW) and how
the medical professionals at the health center handle
the challenges of a highly-populated community.
Agenda
1. The Role of the Community Health Center
Medical professionals stationed at the health
center include a doctor, nurses, midwives, and a
dentist. The BHWs are assigned to the health center.
As the objectives of the community health center are
to oversee and maintain the health of community
people, they provide clinical consultations, antenatal
care (ANC), and the measures to prevent and control
communicable diseases such as DOTS and
vaccinations. They also convene workshops on
family planning, nutrition, and hygiene promotion.
Aside from the services provided at the health center,
they also conduct home visits. In cases of emergency,
transportation to a referral hospital can be arranged
even during the night.
2. The Role of BHWs
According to the DOH, a BHW is a person who
has undergone training programs under any
accredited government and/or non-governmental
organization (NGO), and who voluntarily gives
primary healthcare services in a community after
having been accredited to function as such by the
local health board in accordance with the guidelines
promulgated by the DOH.1
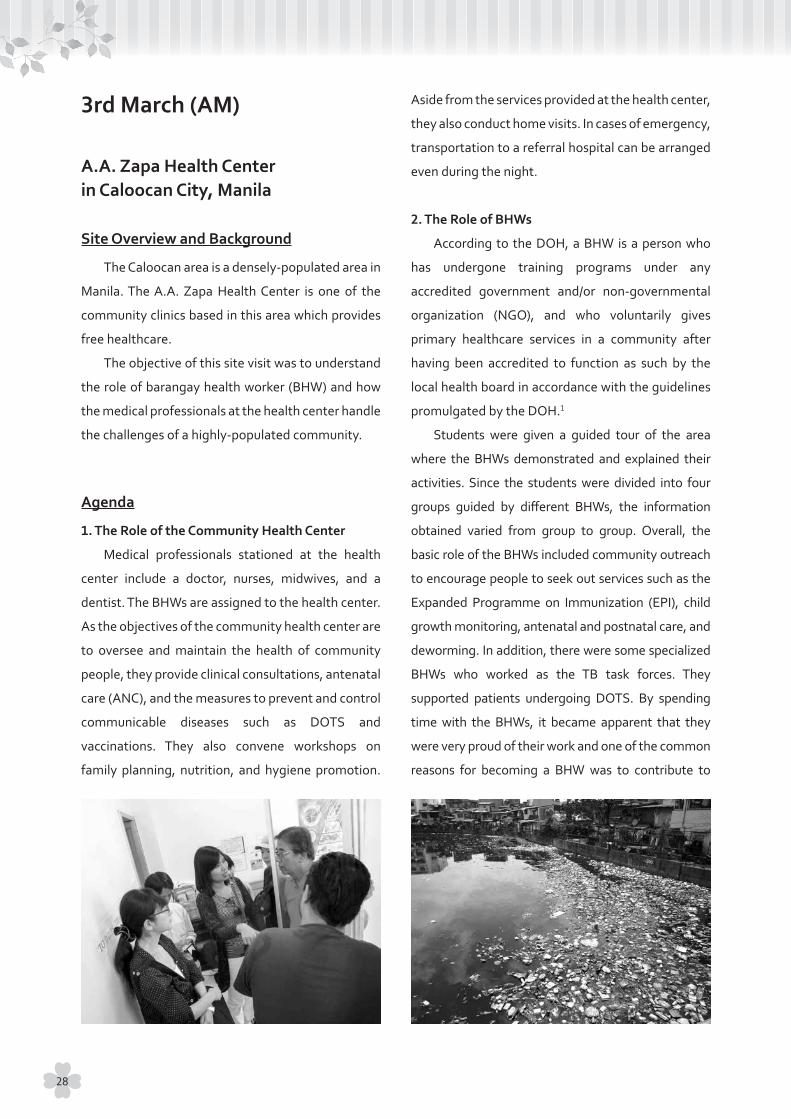
Students were given a guided tour of the area
where the BHWs demonstrated and explained their
activities. Since the students were divided into four
groups guided by different BHWs, the information
obtained varied from group to group. Overall, the
basic role of the BHWs included community outreach
to encourage people to seek out services such as the
Expanded Programme on Immunization (EPI), child
growth monitoring, antenatal and postnatal care, and
deworming. In addition, there were some specialized
BHWs who worked as the TB task forces. They
supported patients undergoing DOTS. By spending
time with the BHWs, it became apparent that they
were very proud of their work and one of the common
reasons for becoming a BHW was to contribute to
3rd March (AM)
28

their respective communities. According to them, the
availability of financial incentives does not affect
significantly in their motivation to dedicate themselves
to their communities.
3. Condition Observed in Caloocan Area
People in the area lived in densely-populated
buildings where animals and people were in close
proximity. Garbage could be seen scattered along
the sidewalks and floating in stagnant water.
Reflection
Given the insufficiency of health professionals in
the Philippines, efficient resource mobilization is
crucial in the local context. Thus, BHWs play
important roles in community health outside the
realm of health facilities. Under the resource-limited
circumstances, it is essential to foster BHWs who are
highly motivated and to ensure their level of
motivation is maintained. Based on the conversations
with the BHWs, it would appear that, financial
incentives are not crucial and may not be the main
factor for their motivation. Other reasons such as
religious belief, surrounding environment, identity
as Filipinos, etc. contribute more to their enthusiasm
for their work. However, in order to better understand
the driving forces of the BHWs, further investigations
and observations are required.
From the observations of the living conditions, it
would seem that sanitation and hygiene management
is needed urgently. To improve the living environment
of the community using people-centered approach,
not only the health sector but also other sectors
should be involved. In order to maximize the effect,
the main actors should be the residents themselves
who would be required to exhibit strong leadership to
implement changes.
Reference1 The Republic of the Philippines Department of
Health. What is Barangay Health Worker? [Internet].
Manila: The Republic of the Philippines Department
of Health; [cited 27 May 2016]. Available from:
http://www.doh.gov.ph/node/837
29

Research Institute of Tuberculosis / Japan Anti-Tuberculosis Association (RIT/JATA) Philippines, Inc.
Site Overview and Background
RIT/JATA Philippines, Inc. (hereafter RIT/JATA) is a
locally-based NGO established in 2008. Its headquarters
is located in Japan while the Philippine office is located
in Manila. Currently there are seven staff members
working there.1
The purpose of the visit was to learn about the
NGO’s activities supporting TB patients at the
community level and to learn about how the NGO
collaborates with the government, national
hospitals, and health centers to tackle TB issues in
the Philippines.
Agenda
In 2009, the National Center for Disease
Prevention and the Control of the DOH led to the
formulation of the 2010-2016 Philippine Plan of
Action to Control Tuberculosis (PhilPACT), which
aimed to achieve the related MDGs.1 According to
RIT/JATA’s presentation, its activities focus on four
strategies out of eight of the PhilPACT strategies:
1) To engage both public and private TB care
providers
2) To promote and strengthen positive behavior
of communities
3) To address MDR-TB, TB/HIV and the needs of
vulnerable populations
4) To certify and accredit TB care providers2
As for the specific activities, it offers multiple
trainings for medical officers to build up their abilities
such as basic TB DOTS training, infection control
training, basic direct sputum smear microscopy
training for medical technologist, appreciation
course for chest radiography, and interpersonal
communication counseling. Trainings on the
National Tuberculosis Control Programme (NTP) and
basic STI, HIV/AIDS education for community health
volunteers (CHVs) are also conducted. In order to
motivate CHVs, RIT/JATA continues to provide them
with training sessions as well as opportunities to
recognize their own contributions at CHV assemblies.
Aside from conducting trainings, RIT/JATA visits
target facilities regularly to monitor and evaluate the
actual implementation of the NTP. Peer education
organized by RIT/JATA also enhances former TB
patients to take an active role in supporting the
current TB patients.2
Its latest project is to build the capacity of
community based organizations to increase TB
reference cases to RHUs as well as to follow up with
patients currently undergoing treatment.2
Reflection
There are two important factors to sustaining an
NGO activities within a community. One is recognition
by the government. Being recognized by the
government allows NGOs to obtain funding to
continue their projects. In order to promote their
contributions to the society, monitoring and
evaluating their own projects is necessary. Meanwhile,
a lack of communication with the government may
result in the undervaluation of NGOs. Since RIT/JATA
has an opportunity to discuss on their activities with
the government only once a year, it seems that there
is room for more constructive dialogue between the
two parties. Recognition by the society as well as the
government generates satisfaction and confidence in
NGOs, which could be fundamental to their ownership.
Such ownership is essential to sustaining their
3rd March (PM)
30

activities.
The second factor is community involvement.
Through annual meetings, CHVs who are engaged in
NGO activities can be recognized and appreciated by
the society for their efforts, which then would
enforce their motivation and dedication. As for peer
education, recognized and highly motivated peer
educators may contribute to sustaining the activities
in their own communities. Peer educators strengthen
the treatment adherence of the current TB patients.
If these people in the community can take over the
activities even after the completion of a project, it
will be an ideal form of sustainability.
References1 Republic of the Philippines Department of Health.
Tuberculosis Control Program [Internet]. Manila:
Republic of the Philippines Department of Health;
[cited 25 April 2016]. Available from: http://www.
doh.gov.ph/national-tuberculosis-control-program
2 RIT/JATA Philippines, Inc.. Activities and
Accomplishments [unpublished lecture notes].
Research Institute of Tuberculosis / Japan Anti-
Tuberculosis Association Philippines; notes
provided at lecture given 3 March 2016.
31

Research Institute for Tropical Medicine (RITM)
Site Overview and Background
RITM was established in 1981 as a research
facility under the Philippines’ DOH. It was partially
funded by a grant aid from the government of Japan
for the establishment of the main building. Its
principle task is planning and implementing research
programs for infectious and/or tropical diseases. As
the principle research arm of the DOH, RITM
conducts multidisciplinary research and contributes
to the prevention and control of infectious and
tropical diseases with a special focus on public
health.1
The purpose of the visit was to understand the
RITM’s general tasks as well as its collaborative
project that has been implemented in cooperation
with Tohoku University.
Agenda
During the visit, two researchers explained their
ongoing research projects to the students. The
researches were under the Science and Technology
Research Partnership for Sustainable Development
(SATREPS)* program and the Japan Initiative for
Global Research Network on Infectious Diseases
(J-GRID)**. These are Japanese governmental
programs aimed to promote international joint
research in which both the recipient countries and the
Japanese research institutions work together based
on the social needs of the recipient countries.2 Their
research focused on infectious diseases in children
such as childhood pneumonia, acute gastroenteritis,
mosquito-borne infections, antimicrobial resistant
bacteria, etc. According to WHO, the Philippines is one
of the 15 countries that together account for 75% of
childhood pneumonia cases worldwide.3 Their research
is rooted in major health issues of the Philippines, and
the collaboration between the Philippines and the
Japanese researchers are realized at RITM.
A short laboratory tour was organized. Some
labs visited were a real-time PCR lab, a serology test
room, a vaccine-production room, etc. Hospital
service for communicable disease patients was on
the same premises.
* SATREPS is funded by AMED (Japan Agency for Medical Research and
Development) and JICA.
** J-GRID is funded by AMED.
Reflection
The main takeaway from the lecture was how
academia, government, and the health sector
actively collaborate with one another in the form of
joint research to find solutions for life-threatening
diseases in the Philippines and around the world. By
leveraging their core strengths, each sector works
toward the same goal of producing new interventions
while aiming to generate and scale up their
effectiveness. Since the research was result-driven in
nature, once a positive result has been produced and
presented, it could bring a multiplying effect to
further scale up research opportunities that would
be beneficial to the community and its people.
Putting a new intervention into practical use is the
main and foremost objective of conducting research,
however, in the current Sustainable Development
Goal (SDG) era, the prospective researches are
expected to expand their objectives to further
advance global health such as:
1) To use the research findings to influence the
policy-making process
4th March (AM)
32
2) To render the findings to the community for
the benefit of local people who were involved
in the research in some way
This was hinted at by the researchers during the
visit. In order to achieve the two objectives, creating
and adopting a two-way feedback framework across
various layers is important to further advance the
quality of future research conducted in the
Philippines.
References1 Research Institute for Tropical Medicine. About Us
[Internet]. Manila: Research Institute for Tropical
Medicine; [cited 26 May 2016]. Available from:
http://ritm.gov.ph/about-us/history-vision-mission/
2 Japan Science and Technology Agency. About
SATREPS [Internet]. Tokyo: Japan Science and
Technology Agency; [cited 24 April 2016]. Available
from:
http://www.jst.go.jp/global/english/about.html
3 World Health Organization Representative Office
Philippines. EWARN weekly summary, Focus on
Pneumonia [Internet]. Manila: World Health
Organization Representative Office Philippines;
February 2014 [cited 24 April 2016]. Available from:
http://www.wpro.who.int/philippines/typhoon_
haiyan/media/Pneumonia.pdf?ua=1
33

Philippine Red Cross (PRC) Headquarters
Site Overview and Background
The PRC, a member of the International Red
Cross and Red Crescent Movement, was officially
established in 1947. It is committed to providing
quality life-saving services to protect the lives and
dignities of people with a focus on indigent Filipinos
in vulnerable situations.1 The PRC is composed of
individuals who devote their time and resources to
help others. Currently, they provide blood and
disaster-related activities, first aid, and health
promotion to uplift the conditions of the most
vulnerable groups in the country.
The main purpose of the visit was to learn about
the overall functions of the organization and their
health services in the Philippines.
Agenda
1. Orientation of PRC
The PRC is governed by 30 board members and
has 102 chapters nationwide. 80% of its manpower
comes from volunteers and more than 1,000 regular
staff across the country. It is funded by public
donations.2 The services offered by the PRC1 are:
1) Disaster management services
(including emergency response, early recovery,
and disaster risk management)
2) National blood services
3) Social services
4) Community health and nursing services
5) Safety services
6) Red Cross Youth
7) Red Cross 143
Other programs offered by the PRC include the
dissemination of the basics of International
Humanitarian Law, membership and fund drives,
and volunteer recruitment.2 The PRC follows the
slogan “A Red Cross that is always first, always ready,
always there” 3 for its activities and programs which
are supported by the Red Cross 143, formed to
strengthen the PRC activities at the community
level. It is composed of one leader and 43 members
who work to plan, prepare, practice, report, and
respond in communities.4
2. Health Service Orientation
The PRC implements their health services with
four key programs:
1) Community-based health program
2) Health response program
3) Training program
4) Organ donation program
The PRC performs these services across the
country and along with other branches of the
International Red Cross including the Japanese Red
Cross Society. The community-based health program
aims to give primary health care and teach about
water, sanitation and hygiene (WASH). The health
response program targets health and WASH during
disasters and emergencies. Training programs
include disaster nursing and home nursing. The PRC
coordinates the organ donation program with the
DOH to recruit donors and establish a donor registry
database in the National Health Quarter.5
3. Information and Technology Operation Center
The Information and Technology Operation Centre
operates as a monitoring and reporting center equipped
with a continuous monitoring system. Relevant
information is integrated into one system for maximum
utilization of its activities. Disaster affected areas,
4th March (PM)
34

hospitals, schools, and other related information can be
detected easily through this system. For example, the
latest information on the availability of ambulances
and blood for transfusion can be obtained promptly.
This facilitates the PRC to provide its assistance in a
timely manner through the operation center.
Reflection
The PRC is a well-organized and functioning
organization across the Philippines. It cooperates
and has established a strong partnership with the
government of the country. PRC volunteers are
highly motivated and passionate. The PRC conducts
disaster management training for locals and
professionals as well. Although all of the activities
are going well currently, a monitoring and evaluation
system is still important. An effective monitoring
and evaluation system is needed to assess the
effectiveness of each program. In addition,
harmonized collaboration with the government of
the Philippines is important to avoid duplication and
fragmentation in working areas. Evaluation should
be conducted by presenting the outcomes of
activities to assure their accountability. At the same
time, the organization can learn lessons from
assessing the process of their activities.
References1 Philippine Red Cross. About the Philippine Red
Cross [Internet]. Mandaluyong City: Philippine Red
Cross; [cited 11 April 2016]. Available from:
http://www.redcross.org.ph/about-the-philippine-
red-cross
2 Philippine Red Cross [unpublished lecture notes].
Philippine Red Cross Headquarters; notes provided
at lecture given 4 March 2016.
3 Philippine Red Cross. Philippine Red Cross
[Internet]. Mandaluyong City: Philippine Red Cross;
[cited 11 April 2016]. Available from:
www.redcross.org.ph
4 Philippine Red Cross. Red Cross 143 [Internet].
Mandaluyong City: Philippine Red Cross; [cited 11
April 2016]. Available from:
http://www.redcross.org.ph/get-involved/red-
cross-143
5 Health Services Orientation [unpublished lecture
notes]. Philippine Red Cross Headquarters; notes
provided at lecture given 4 March 2016.
35

Philippine Red Cross (PRC) Leyte Chapter
Site Overview and Background
The PRC has 102 chapters nationwide1 with the
Leyte chapter covering 25 municipalities and 300
barangays. During the Typhoon Haiyan response, it
collaborated with nine international partners including
the Japanese Red Cross Society,2 to conduct disaster
relief. The 180 staff and 300 volunteers who operated
during emergency operations for Typhoon Haiyan
were involved in shelter building, livelihood support,
health, education, and WASH. The places visited were
Barangay 107 (Santa Elena), the Cabalawan Health
Station, and Abango Elementary School which
showcased their achievements.
Agenda
1. Briefing on Haiyan Operations
1-1. Shelter
“Shelter Repair Assistance” aimed at distributing
materials and cash assistance to those whose houses
were damaged by the typhoon. In addition, another
program named “Core Shelter” provided permanent
housing to those who lost their houses entirely. As of
March 2016, 17,724 houses were repaired and 8,440
houses were newly built.2
1-2. Livelihoods
Activities to restore livelihoods were separated
into phases as listed below:
Phase 1:
Provision of conditional/unconditional cash grants
and monitoring
Phase 2:
Skills training for youth and support for enterprises
Phase 3:
Support for community-based enterprises
Phase 1 was implemented for emergencies and
phase 2 and 3 focused on recovery efforts of affected
areas.1
1-3. Health and Education
The PRC provided both hardware and software
support for disaster reconstruction. Reconstructions
of health facilities and schools had proceeded
smoothly and achieved 42% and 56% of the targets
respectively as of March 2016. The hardware support
was more easily accepted by the community people
because facility reconstructions were visible and
concrete. On the other hand, software support such
as health promotion received much less interests
from local communities.2
1-4. WASH
The main activities were rehabilitation and
construction of water facilities and community/
school-based WASH promotion.2
2. Site Visits
2-1. Barangay 107 Santa Elena: “Shelter” building
operational site
Although they were called “shelters”, the houses
provided by the PRC were permanent housings for
people who had lost their houses to Typhoon Haiyan.
The houses were a mix of concrete and wood, 4m ×
5m in size, and equipped with WASH facilities (water
tank and toilet). To ensure proper usage of WASH
facilities, promotional activities were also conducted
in the community to embed its practice. The barangay
reconstruction committee which was constituted by
residents of the community allocated housing
7th March
36
appropriately to the people, weighing socioeconomic
status and their capacity to re-establish their lives. The
PRC staff and Red Cross Volunteers (RCVs) monitored
the progress of the construction by visiting the sites
daily.
2-2. Barangay 97 Cabalawan: Health Station
The Cabalawan Health Station was rehabilitated
in August 2015 by the PRC in partnership with the
International Federation of Red Cross and Red
Crescent Societies (IFRC). Altogether, around 20
CHVs and/or RCVs were working regularly. The
medical staff, nurses, doctors, and midwives were
not stationed on the site every day, and the frequency
of their visits varied. The health services provided
were ANC, immunization, patient follow-ups, school-
based health education, etc.
2-3. Abango Elementary School: School-based
WASH activities
To promote and advance WASH activities among
pupils and their families, several initiatives were
implemented as a school program. For example,
peer-education, preparing a teacher’s guide, and
social dramas were carried out to educate children
on the importance of personal hygiene and the risks
associated with waterborne diseases. The toilets and
faucets on the school premises were designed not
only for school children but also as the designated
public facilities in case of emergencies.
Reflection
A long-term strategy that incorporates a vision
of health promotion from the very beginning of
disaster response is required. For example, in order
to help rebuild people’s lives, the PRC reconstructed
housing with an emphasis to adopt WASH activities
to promote good health. Health promotion is needed
as much as cash assistance in order to help enrich
people’s lives in disaster response. The PRC showed
good practice of school-based WASH activity. The
key elements for this success were how the PRC
managed to nourish and embed a sense of ownership
in the educational sector.
References1 Philippine Red Cross [unpublished lecture notes].
Philippine Red Cross Headquarters; notes provided
at lecture given 4 March 2016.
2 Haiyan Operations Update 2016 [unpublished
lecture notes]. Philippine Red Cross Leyte Chapter;
notes provided at lecture given 7 March 2016.
37

Institutions related to Project for Strengthening Maternal and Child Health Services in Eastern Visayas, Philippines (SMACHS-EV Project)
Site Overview and Background
The Project for Strengthening Maternal and
Child Health Services in Eastern Visayas, Philippines
(SMACHS-EV Project) is carried out in Leyte Province
(except Tacloban City) and Ormoc City. The purpose
of the visit was to learn how JICA was supporting and
working together with the local government in the
health sector to reduce maternal and neonatal
mortality in Eastern Visayas and how they
implemented the projects in the field.
Agenda
1. Overview of the SMACHS-EV Project
The SMACHS-EV Project (February 2010 - July
2016) is funded and technically assisted by JICA at
the request of the DOH to support ensuring safe
pregnancies, safe deliveries, and postpartum care
services in the targeted areas. In order to achieve the
national target of the MDG 5 as well as to reduce the
consistently high maternal mortality, the SMACHS-
EV Project was launched in collaboration with the
local government and JICA.
The main achievements of this project included:
1) Developed a strong monitoring system on
service quality of basic emergency obstetric
and newborn care (BEmONC) health facilities
2) Obtaining support and commitment from all
LGUs support on health
3) Strengthening the functionality of the
community health team1
2. Good Practice at the RHU and the BHS in Dulag
and Tolosa
Through the site visits, the roles and
responsibilities of the RHU and the BHS and how
they conduct their services in alignment with the
project were presented. At the RHU, progress and
achievements such as the coverage rate of ANC,
were displayed throughout the hospital in the form
of posters and brochures highlighting their efforts in
contributing to the well-being of pregnant women,
mothers, and babies. In the case of Dulag, the
municipal mayor had a strong interest in public
health which was a factor to further enhance the
achievements of this project. Working closely with
the RHU, the BHWs had a very important role in
overseeing the health of the people living in the
community. In Tolosa, students had a chance to meet
and talk with a group of the BHWs to explore how
they perceived their roles and the factors which
drove them to work as a BHW for a long period of
time. They all mentioned that they feel great
satisfaction from serving their communities and take
much pride in their work.
3. Leyte Provincial Health Office and Leyte
Provincial Hospital
The Leyte Provincial Hospital was severely
damaged by Typhoon Haiyan in 2013. Since they
received no aid from any organization for several
days, they suffered greatly after the typhoon.
Furthermore, in the following year, another large
typhoon hit the island and thus the reconstructed
hospital was again destroyed. The bitter experience
highlighted the importance of comprehensiveness in
the rapid assessment of disasters and the necessity
of sustainability for disaster preparedness.
8th March
38

Reflection
Maintaining motivation among health workers
across all levels of the system is extremely important
and a fundamental element that influences how well
the projects operate. Throughout the site visits, it
was clear that a sense of satisfaction and confidence
built by being recognized are essential factors to
enhance their motivation. This could trigger a higher
sense of responsibility and willingness to lead the
project on their own. In this sense, JICA emphasized
the effective utilization of national staff who knew
and were familiar with the situation in the local
context in order to build local ownership.
Furthermore, in order to avoid the projects from
becoming a one-time effort, it was essential to
engage relevant actors, including policy makers,
from the very beginning to foster and obtain their
commitment. This ensured that projects were not
only carried out but also the effects of the projects
were sustained even after they were completed.
Reference1 The Project for “Strengthening Maternal and Child
health Services in Eastern Visayas” (SMACHS EV)
[unpublished lecture notes]. Japan International
Cooperation Agency; notes provided at lecture
given 8 March 2016.
39
World Health Organization Regional Office for the Western Pacific (WHO / WPRO)
Site Overview and Background
Same as the report for 1st March. The roles of
WHO/WPRO were presented through three specific
initiatives on TB, tobacco, and filariasis.
Agenda
1. The Roles of WHO/WPRO
WHO has three core functions:
1) Normative guidance
2) Public service at regional level
3) Country support
WHO is responsible for developing health
guidelines based on evidence. In order to develop these
guidelines which can be applied across a vast spectrum
of situations, WHO sets up commissions to ensure that
the voices of various experts are incorporated. This
process takes about one to two years.
Once certain guidelines have been developed,
WHO supports each member state to adapt and
implement the guidelines and strategies. The
situations, however, vary country by country requiring
more specific factors to be considered and reflected
before the guidelines to be implemented. Thus, to
identify and help member states to overcome similar
challenges at a regional level, WPRO serves to develop
a regional framework for action.
2. The Challenges of the Health System through
an Example of MDR-TB
Drug-resistance is a result of failed treatment
caused by a weak health system. Consequently, it
can be said that MDR-TB is a man-made phenomenon.
In the Philippines, MDR-TB accounts for
approximately 4.0% of the total number of new TB
cases.1 There are many patients being treated in the
private sector. Due to the nature of the current Filipino
health system and the relationship between the DOH
and private sectors, the quality of the treatment
carried out by private hospitals are not fully captured
by the DOH. Therefore, the number of patients who
may be mistreated are unknown. It can be assumed
that those patients have a higher risk of suffering from
TB drug resistance. Unfortunately, the weak health
system has created a hotbed for MDR-TB.
Through the case of TB drug resistance, it is evident
that having a strong health system is fundamental to
controlling diseases, while many factors such as early
diagnosis, prevention, communication, advocacy, and
surveillance should also be considered. In the MDG era,
interventions were provided to reduce certain diseases.
In the SDG era, a good health system is needed to
control diseases sustainably.
11th March
40

3. Tobacco Free Initiative
Tobacco has killed 100 million people in the 20th
century. If the current trend continues, tobacco could
kill up to one billion in the 21st century unless urgent
action is taken. The Western Pacific Region holds the
greatest number of smokers, 430 million, which is about
one-third of the world’s smokers.2 In this region, two
people die each minute from a tobacco-related disease.
About 600,000 people die prematurely each year
as a result of exposure to second-hand smoke. It is
estimated that 50% of all children in this region are
regularly exposed to second-hand smoke at home
and in public places.
The WHO Framework Convention on Tobacco
Control (WHO-FCTC) is the most powerful tool to
reverse the tobacco epidemic. As a priority on the public
health agenda, WHO-FCTC establishes tobacco control
measures such as demand-reduction through high
taxation, supply-reduction, and suggesting alternative
crops to grow for tobacco farmers.3 Other activities
include global tobacco surveillance and monitoring,
developing prevention strategies to protect people
from tobacco and its smoke (e.g. smoke-free laws and
initiatives using mobile phones to provide cessation
services),4 and enforcing bans on tobacco advertising.
Among these measures, data indicates that
raising taxes on tobacco is the most cost effective
measure. A 10% increase in tobacco prices decreases
about 4% consumption in high-income countries
and about 8% in low and middle-income countries.5
Furthermore, there is a need to regulate the use of
electronic cigarettes, water pipe tobacco, etc.
4. Global Programme to Eliminate Lymphatic
Filariasis (GPELF)
The GPELF was launched in 2000.6 According to
WHO, in 2014 alone, 139 million people were reached
with ivermectin through GPELF in 18 sub-Saharan
African countries and 109 million people were
treated globally with ivermectin for onchocerciasis.7
Currently, 73 countries are considered endemic
for lymphatic filariasis (LF).8 The GPELF’s goal is to
eliminate LF by 2020, and its strategies are to stop
the spread of infection and to alleviate the suffering
of affected populations.8 The three steps being taken
to reach this goal are:
1) Mapping
2) Mass drug administration (MDA)
3) Surveillance6
The role for each level of the GPELF is as follows:
❖ WHO sets policy strategies
❖ Donors offer financial support
❖ The health departments and ministries
implement programs
❖ NGOs offer support in the field while academia
provides evidence
Through this approach, various actors collaborate
to eliminate LF. As for the Philippines, it has 100%
geographical coverage of the MDA.9
Reflection
There were three main findings from the lectures.
Firstly, the role of WHO is like a conductor of an
orchestra. It assembles member states, academia,
civil societies, and private sectors and drive them to
work towards a common goal. By collaborating and
complementing the strengths of each actor, WHO
aims to develop a global agenda and strategies that
could feed into the advancement of global health.
Secondly, all three initiatives mentioned in the
agenda above emphasized the importance of
strengthening a strong and stable health system.
Focusing only on specific health issues is not enough,
there is a definite need to view the health system in its
entirety. By taking a closer look, the root causes and
41

core solutions of particular health issues can be found.
Lastly, knowledge itself is insufficient. The skills
to think logically and comprehensively using
obtained knowledge to understand the scope of the
problem and the factors behind them are even more
important. This way of constructive thinking is
essential when developing any health strategies in
the field of global health.
References1 World Health Organization. Tuberculosis (TB), The
Philippines [Internet]. Geneva: World Health
Organization; [cited 15 April 2016]. Available from:
http://www.who.int/tb/publications/2009/airborne/
philippines/en/
2 World Health Organization Western Pacific Region.
Health Information and Intelligence Platform,
Tobacco Control [Internet]. Manila: World Health
Organization Western Pacific Region; [cited 12
April 2016]. Available from:
http://hiip.wpro.who.int/portal/Dashboards/
Tobaccocontrol.aspx
3 World Health Organization. Tobacco Free Initiative
(TFI), Tobacco control economics [Internet].
Geneva: World Health Organization; [cited 15
April2016]. Available from:
http://www.who.int/tobacco/economics/background/
en/index2.html
4 World Health Organization. Tobacco Free Initiative
(TFI), Checking your mobile phone for messages just
became good for you [Internet]. Geneva: World Health
Organization; [cited 22 April 2016]. Available from:
http://www.who.int/tobacco/communications/
highlights/mhealthleem/en/
5 World Health Organization. WHO global health days,
World No Tobacco Day - 31 May 2014 [Internet].
Geneva: World Health Organization; [cited 15 April
2016]. Available from:
http://www.who.int/campaigns/no-tobacco-
day/2014/event/en/
6 World Health Organization. Lymphatic filariasis,
Global Programme to Eliminate Lymphatic Filariasis
[Internet]. Geneva: World Health Organization;
[cited 10 April 2016]. Available from:
http://www.who.int/lymphatic_filariasis/disease/en/
7 World Health Organization. Neglected tropical
diseases, WHO welcomes Nobel Prize in Physiology
or Medicine 2015 for discoveries of drugs against
tropical diseases [Internet]. Geneva: World Health
Organization; [cited 10 April2016]. Available from:
http://www.who.int/neglected_diseases/news/
nobel_prize_2015/en/
8 World Health Organization. Lymphatic filariasis
[Internet]. Geneva: World Health Organization;
[updated February 2016; cited 10 April 2016].
Available from:
http://www.who.int/mediacentre/factsheets/fs102/en/
9 Global Programme to Eliminate Lymphatic Filariasis
(GPELF) [unpublished lecture notes]. World Health
Organization Western Pacific Region; notes
provided at lecture given 11 March 2016.
42
3. Presentation
Introduction
The theme of the presentation was “Sustainability”.
The Philippines has been steadily developing its
health status but there are still certain challenges
that need to be improved. Based on this context, we
realized the importance of sustainability in the global
health as we conducted our field trip. This diagram
summarizes our learnings.
Sustainability in global health is supported by
these five pillars:
❖ Preparedness
❖ Human resources
❖ Partnership
❖ Ownership
❖ Finance
The pillars are standing on the local context,
such as the culture, values, perspectives, etc. of local
communities.
Preparedness
Preparedness is important for supporting the
sustainability of disaster and disease management.
Some examples of counter disaster preparations can
1. Presentation Overview
2. Guests
DOH: Ms. Jocelyn T. Sosito
JICA: Mr. Shogo Kanamori
RITM: Mr. Ryosuke Kojima
SLH: Dr. Carina H. Frayco, Dr. Flora P. Marin, 5 Medical students
WHO Country Office in the Philippines: Dr. Kohei Toda
NU-SLH Collaborative Office: Dr. Nobuo Saito
Report of the Final Presentation
Title Presentation of the Field Trip to the Philippines
Place NU-SLH Collaborative Office in San Lazaro Hospital
Date 11 March 2016
Program 14:00-14:30
14:30-15:10
15:10-15:30
15:30-16:00
Opening
Presentation
Q&A / Comments from the guests
Reception
44

include residents practicing evacuation drills regularly
and participating in the making of hazard maps,
volunteers being trained in first-aids, and nurses being
trained for disaster care management. Adding to
these “soft” components of preparation, examples of
“hard” components include; reconstruction and
rehabilitation of disaster-resistant facilities, and also
building infrastructure such as public transportation
system to reduce traffic jams in cases when urgent
evacuation and emergency assistance are needed.
Information is a key to preparedness. Therefore,
it is advisable to disseminate lessons learned from
past disaster experiences and have a network among
related organizations through everyday operation to
share information and work together smoothly in
case of emergencies.
We noted some examples of preparations in
disease management from our field trip, which
included building WASH facilities, offering WASH
promotion, and awarding best practices. When it
comes to specific diseases such as TB, practicing and
promoting DOTS, and improving techniques of chest
radiography were also used. RITM offered their
research findings such as new methods for treating
local diseases as prevention measures. Health
insurance could also be a factor to promote resilience
against the future diseases.
From these learnings, we found that prevention,
resilience, dissemination of information, and training
as the four key components of “preparedness,”
which creates a state of being ready for unpredictable
future disasters and diseases that can affect the
sustainability of global health.
Human Resources
According to the WHO Health Systems Building
Blocks,1 health workforce is one of the most
important blocks of the health systems. Yet, as
WPRO pointed out, many countries in the Western
Pacific Region including the Philippines continue to
struggle to address the need for more health
professionals to meet health challenges.2 Through
visiting several sites including the DOH, WPRO, SLH,
local communities and meeting with various health
works across different levels, two issues were
highlighted as the core challenges of the current
Filipino health workforce situation.
Firstly, there are quantity and quality issues:
“how to secure necessary number for work force”
(quantity), and “how to enhance the quality of
medical professionals and health workers” (quality).
To address the issue of quantity, the Philippines must
tap into the country’s most valuable resource, the
people, and mobilize them into the health sector
through a mass recruitment. When doing so, they
should carefully consider ways to emphasize the
core characteristic of their people and apply the
Filipino “helping each other” spirit to full potential
beyond the framework of the BHWs. A hook to
attract people to commit to the medical/health
sector is essential. What are the values for the Filipino
people to engage in this sector? This is something
the national and local governments, as well as the
private sector should think seriously about and
define well in order to secure a robust health
workforce. A majority of the BHWs are currently
women and it would be beneficial to recruit more
men to encourage male participation. There are
gender specific health issues and more male BHWs
are needed to support the vulnerable male population
at a community level.
Secondly, to tackle the issue of quality, it is vital
to implement necessary measures to elevate both
the skills and motivation of health workers along
with the people in the communities. Capacity
building programs such as skill trainings and
educational trainings must be considered to improve
the quality of the workers and minimize the gap
45

between those who are skilled and satisfied with
their work and those who are unskilled and
unsatisfied. Thus, in order to tackle current
challenges and to further strengthen the existing
human resource framework, we have identified the
following four components as necessary measures:
1) Knowledge-sharing
2) Coordination
3) Monitoring and evaluation
4) Motivation
Active knowledge-sharing and coordination
among the health workers across different levels will
generate a smooth and transparent flow of
information and knowledge which will help to create
an environment where relevant information
dissemination is possible, thus allowing professional
skills to be enhanced through the exchange of
experiences and best practices. To maintain workers’
motivation and quality of their work, a monitoring
and evaluation system to regularly evaluate their
performances and progress is fundamental. The
system should be standardized and act as an enforcer
for the health workers to fully maximize their
potential as a skilled professional. If each component
can function and integrated effectively, we believe
the Filipino health workforce management will be on
the optimal track to sustainability.
Partnership and Ownership
Here, the term “partnership” is used interchangeable
with “coordination”, “collaboration”, “cooperation”,
and “relationship.” The importance of partnerships
among stakeholders at each level was recognized
through the field trip. For example, at the regional
level of the TB program, WPRO takes the leadership
role in its covering region while the countries of the
region cooperate to tackle the TB problem. There are
also vertical and horizontal collaborations at the
national and community levels respectively. An
example of vertical collaboration at the national
level is the referral system between SLH and BHS. In
terms of the horizontal collaboration at the
community level, local NGOs and BHS have meetings
to share information about their activities. Engaging
multiple stakeholders runs the risks of duplication
and fragmentation of service delivery, but if these
stakeholders are aligned as partners such risks can
be prevented and it can magnify the scope of their
services. Good coordination among the organizations
and activities lead to a positive outcome of the
projects and it motivates people to manage their
problems by themselves. Moreover, the communities
will be empowered and a sense of ownership will
grow within themselves.
Finance
The PhilHealth is a government-owned and
controlled corporation that deals with healthcare
financing.3 It aims to implement the NHIP for all
Fillipinos. A part of its revenue is covered by sin tax,
which is a taxation on tobacco and alcohol products.4
The PhilHealth allows patients to receive free
healthcare and reduces economic burden on them,
however, when we consider the sustainability of the
system, high dependency on sin tax is not
recommended. If the sin tax amount influences the
availability of health care provision, this might affect
the health status of financially vulnerable populations
as well as taxpayers. Therefore, the more people
consume tobacco and alcohol, the more money goes
to the government and the PhilHealth for health
care provisions. This results in a situation where the
poor can receive free healthcare and become
healthier while the taxpayers continue their bad
habits and become unhealthy. In conclusion, high
dependency on sin tax creates a situation where one
population’s health status is compensated by
deteriorating the other population’s health. For
46
long-term operations of the health insurance system,
a more sustainable way to cover the expenses is
needed.
Conclusion
The five pillars: preparedness, human resources,
partnership, ownership, and finance are the key
concepts supporting the sustainability of the health
system in the Philippines. We should not forget,
however, that the base of these pillars is the local
context of the country. Through the observations at
the sites visited and our discussions, we learned how
each institution operates and strives to contribute to
achieving sustainable development of the health
sector in the country. By making use of the lessons
learned in the country, we, the MPH candidates, are
strongly motivated to take an active part in
contributing to the advancement and development
of the global agenda.
4. Questions and Answers, Comments from
the Guests
Questions and Answers
Q. How can we sustain programs that tackle health
related issues?
A. Community empowerment is important. Since
Filipinos are very active and kind, they have the
potential to achieve this. One of the examples
that we learned through the field trip was training
local people to detect TB suspicious cases. Sin tax
is one source of securing financial budget to tackle
health relate issues.
Q. How can we solve problems of human resources?
A. One of the solutions could include the younger
generation. To involve the young people, more
information should be disseminated to them.
Comments
· Connections among the governments at the
national, provincial, and municipal levels are
important.
· It is important to keep in mind questions such as
“when can we say that a country has recovered
from a disaster?” and “how should we determine
when to withdraw aid?” when considering about
external aid.
· The framework for sustainability might not be for
the case of the Philippines. It might be more
suitable for less developed countries.
5. Reflection
Throughout the field trip, all students were
required to not just learn about the health issues in
the Philippines, but to take part in the discussions,
and to be a leader and facilitator at each occasion. At
the very end of our trip, we prepared a final
47
presentation as a compilation of what we have
learned. The following steps were taken by the
students to organize the presentation:
1) Sharing the objectives of the presentation
2) Discussing the overall framework of the
presentation
3) Brainstorming the keywords of our findings
4) Drafting the presentation concept based on
identified keywords to develop the pillar
model
This “concept-based” procedure enabled us to
sum up our learnings from various institutions
dealing with different health issues into several
common key word. Through the process of preparing
for this presentation, our perspectives were broaden,
which allowed us to think more about various
approaches to global health issues.
Lastly, we would like to express our deepest
gratitude to everyone who supported our field trip.
References1 World Health Organization Western Pacific Region.
Health services development, The WHO Health
Systems Framework [Internet]. Manila: World
Health Organization Western Pacific Region; [cited
10 March 2016]. Available from:
http://www.wpro.who.int/health_services/health_
systems_framework/en/
2 World Health Organization Western Pacific Region.
Human resources for health [Internet]. Manila:
World Health Organization Western Pacific Region;
[cited 10 March 2016]. Available from:
http://www.wpro.who.int/hrh/en/
3 Asia Pacific Observatory on Health Systems and
Policies. The Philippines Health System Review,
Health Systems in Transition Vol. 1 No.2 2011
[Internet]. Manila: World Health Organization
Representative Office Philippines; [cited 4 April
2016]. Available from:
http://www.wpro.who.int/philippines/areas/
health_systems/financing/philippines_health_
system_review.pdf
4 World Health Organization. “Sin Tax” expands
health coverage in the Philippines [Internet].
Geneva: World Health Organization; May 2015
[cited 10 March 2016]. Available from:
h t t p : / / w w w . w h o . i n t / f e a t u r e s / 2 0 1 5 / n c d -
philippines/en/
48
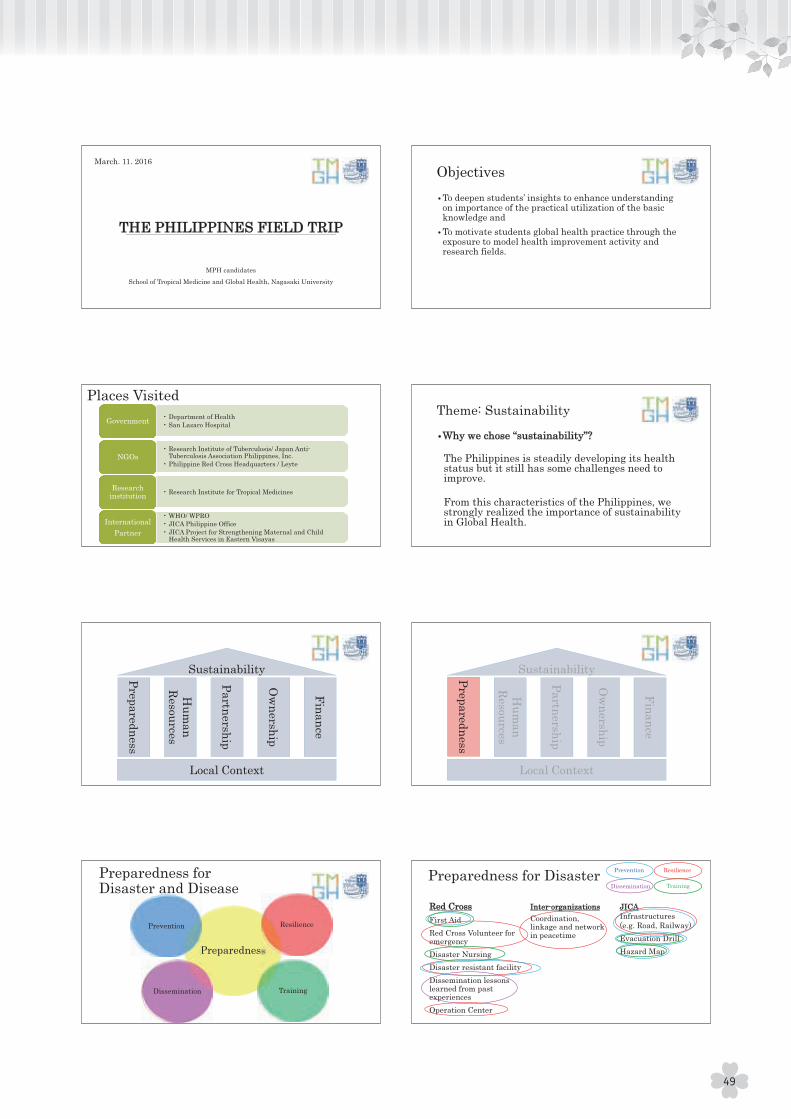
49
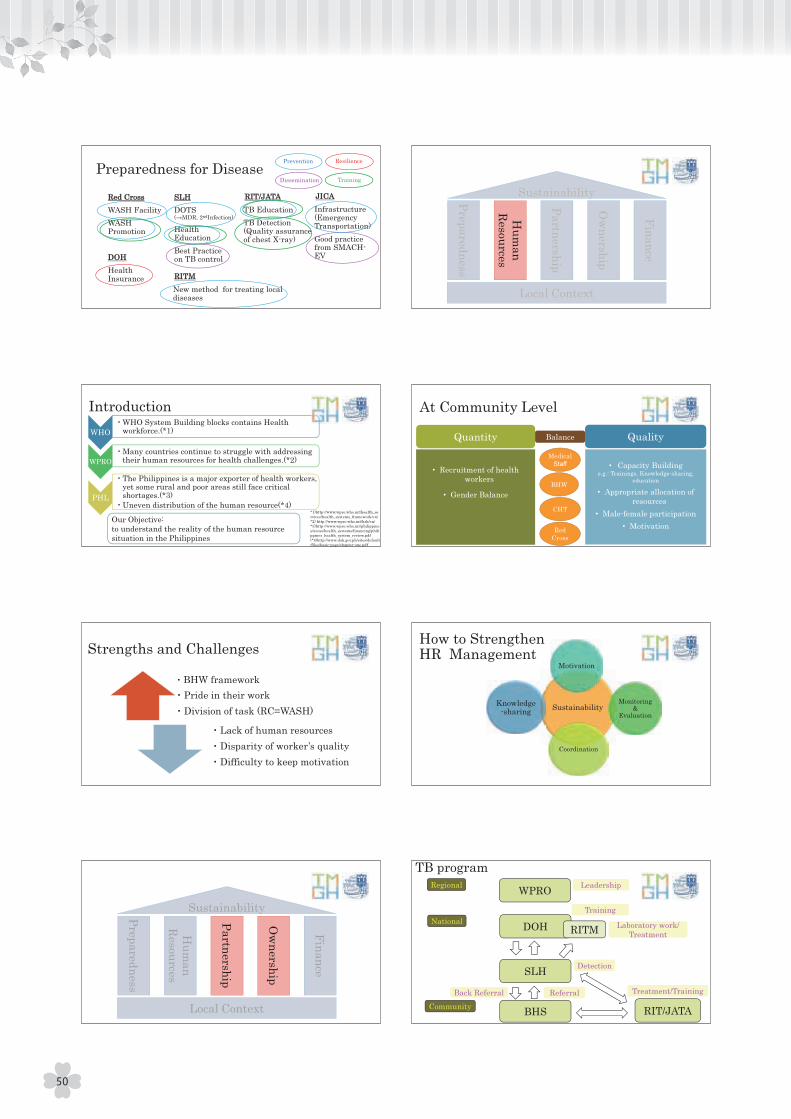
50
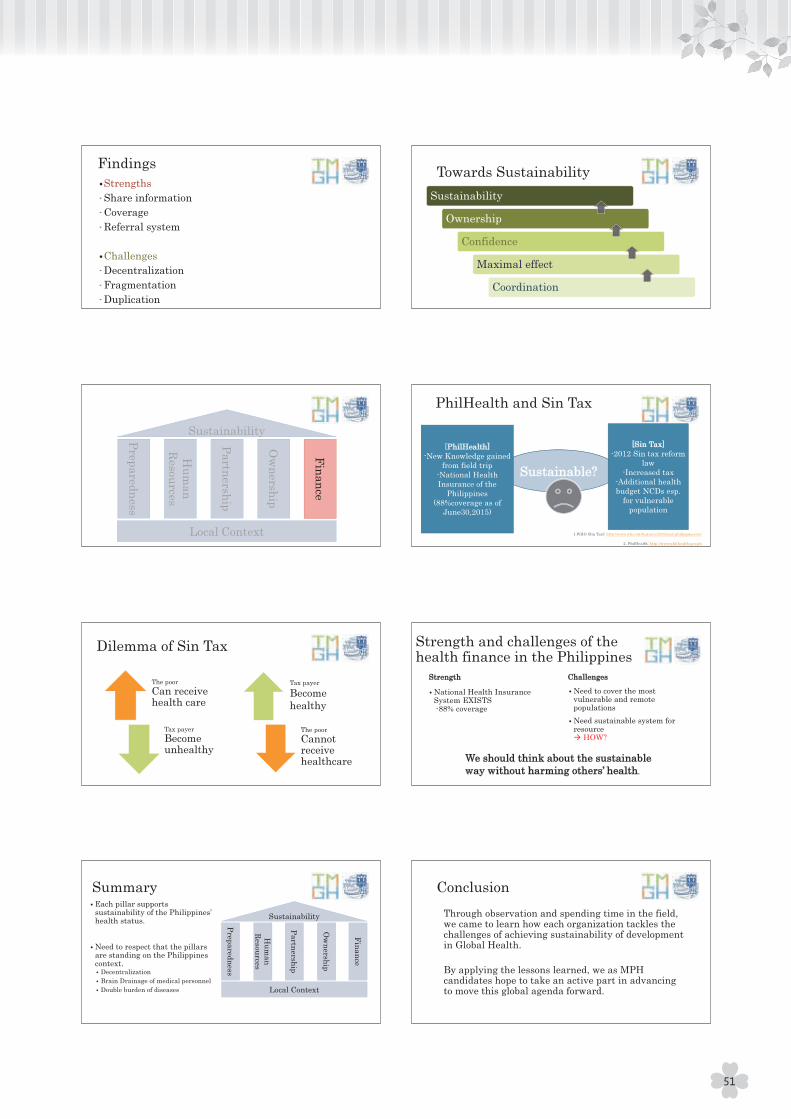
51

The short-term field training trip has been a part of the International Health Development course since the
inception of the School of International Health Development in 2008. At the time, the destination was
Bangladesh, however, this was changed in academic year 2015/2016 to the Philippines due to security concerns
in Bangladesh. In addition to the destination, the field trip’s program had a series of changes from previous
years. We were a large party of 20 individuals including accompanying faculty members, which was twice the
size of previous trips. Furthermore, the language of instruction was English in compliance with the rest of the
coursework at the School of Tropical Medicine and Global Health (TMGH). In essence, both students and faculty
had to navigate through new arrangements during the field trip this year.
The objectives of the field trip, as mentioned earlier in this report, are for students to deepen their insights,
to enhance their understanding on the importance of the practical utilization of basic knowledge, and to
motivate students to global health practice through exposure to model health improvement activities and
research fields. While faculty members design and make arrangements for the site visits, it is the students who
are in charge of running daily activities under the supervision of the accompanying faculty members. For this
year’s field trip, students formed four working groups to facilitate preparation as well as implementation of
planned activities. In addition, as a daily routine, each student was assigned to perform certain tasks according
to the daily schedule, such as team leader/sub-leader of the day, note taker, and someone to arrange transport,
etc. Through performing these tasks students were expected to strengthen their skills such as facilitation, time
management, stress management, leadership, and followership from the group work.
“How could we have used the limited time more efficiently?”
“Did I do a good job as team leader/facilitator?”
“What were better ways to engage more people in the discussions?”
“Why did I feel so frustrated regarding something that usually does not bother me?”
I believe these questions came across the minds of many students during and/or after the field trip. I hope
that each student will keep their individual reflections in mind and apply them towards their forthcoming
internship and/or future endeavors.
The field trip program is assisted by a number of individuals every year. In particular, I would like to
acknowledge the individuals listed in the beginning of this report for having spent the time and effort for the
benefit of the Nagasaki TMGH students.
The field trip program is a one-credit, requisite coursework for the MPH students at Nagasaki University.
This year, each student was financially supported by one of the following organizations: Japan Student Services
Organization (JASSO), Japan International Cooperation Agency (JICA)/Japan International Cooperation Center
(JICE), and the Student Support Department, Nagasaki University. I would like to extend our sincere gratitude
to these organizations in helping the students participate in the field trip program.
Afterword
Miho SatoAssistant Professor, School of Tropical Medicine and Global Health, Nagasaki University
52

On the way back from Caloocan City to our hotel in the Malate district in Manila, our bus passed the place
where the notorious landfill called Smokey Mountain used to be. Soon after the view of the mega city of Manila
came into the picture with dozens of high-rise buildings towered behind thousands of poor housings spread
rampantly like weeds in a neglected garden. The scene seemed very symbolic illustrating the discrepancy
existing in the Philippines which we experienced during this two-week field trip.
As we had opportunities to visit many sites and see various dimensions of the Philippines’ health system, it
was challenging to capture the core essence of each site and we consumed a great amount of time and effort
consolidating different perspectives and takeaways of 16 students into one report. Yet, through this process,
we, the five of us in the editorial team realized that this time was needed to recap and to really process what we
observed and learned during the field trip. As we deepened our understanding, we felt how fortunate we were
to have our experiences in the Philippines. A fellow student said that “by hearing the opinion directly from local
people and observing the health situation in both urban and rural areas with my own eyes, I could deepen my
insights and develop my knowledge from textbooks to more applicable one”. This resonates well with us in
thinking that we would not be able to understand a reality in any given context unless we observe and pay
attention to details of different aspects of a health system. As the MPH candidates, we are expected to have the
eyes, ears, and minds to question the current situations and to willingly explore the solutions to even those that
are undetected problems of the people.
We would like to take this moment to thank all the people who have supported us in the field trip and during
the making of this report. At a point, we felt it was not possible that this report will see the light of day! A big
thank also goes out to all the fellow students who made this trip a memorable one in every sense(!) and helped
us put this report together. And, last but not least, let’s give ourselves well-deserved pats on our back for
completing this journey of endless nights of learning, exhaustion, agony, and friendship. We own ourselves a
big party to celebrate the launch of this publication!
Sincerely,
Kumiko Takai
Meguru Yamamoto
Reiri Tsumura
Ryo Kobayashi
Satomi Ichino
Editor’s Note
53

Field Trip Report 2016, The Philippines
Published by School of Tropical Medicine and Global Health, Nagasaki University
Edited by Kumiko Takai, Meguru Yamamoto, Reiri Tsumura, Ryo Kobayashi, Satomi Ichino
Photographs edited by Noriko Tamari, Asuka Miyazaki
Cover design by Aiko Inoue, Takuya Shizume
References checked by Shoko Ogino, Erika Yoshimoto, Khin Zar Wai, Masanobu Ono, Nobuya Goto,
Yasue Yoshino, Zar Lwin Hnin
English proofread by Mengya Li (Academic support staff at TMGH)
Supervised by Hisakazu Hiraoka, Miho Sato
© 2016 by School of Tropical Medicine and Global Health, Nagasaki University
All rights reserved.
First printing on 20 July 2016
Printed by IN-TEX Co. Ltd. Nagasaki, Japan
School of Tropical Medicine and Global Health
Nagasaki University
1-12-4 Sakamoto, Nagasaki City
852-8523, Japan
Tel: +81(0)95 819 7583
http://www.tmgh.nagasaki-u.ac.jp/?lang=en
1-12-4 Sakamoto,Nagasaki City 852-8523,JAPANTel:+81(0)95 819 7583 Fax:+81(0)95 819 7892http://www.tmgh.nagasaki-u.ac.jp/?lang=en





























