Embed Size (px)
Citation preview

Fratura blow-out. Acesso retrosseptal sem sutura e reconstrução do assoalho orbitário com malha de titânio
José Augusto Gomes Pereira de Oliveira 1 Jorge Vicente Lopes da Silva 2
1) Postdoctoral Research Fellow em Cirurgia Ortognática pela University of Washington – USA. Pesquisador do Centro de Tecnologia da Informação Renato Archer.2) Doutor em Engenharia Química – UNICAMP. Chefe da Divisão de Tecnologias Tridimensionais do Centro de Tecnologia da Informação Renato Archer - Campinas - São Paulo.
Instituição: Centro de Tecnologia da Informação Renato Archer – CTI. Campinas / SP – Brasil.
Correspondência: José Augusto Gomes Pereira de Oliveira - Divisão de Tecnologias Tridimensionais (DT3D) do Centro de Tecnologia da Informação Renato Archer - CTI - MCTI - Rodovia Dom Pedro I (SP-65), Km 143,6 - Campinas / SP – Brasil - E-mail: [email protected] recebido em 06/05/2015; aceito para publicação em 23/09/2016; publicado online em 15/10/2016.Conflito de interesse: não há. Fonte de fomento: não há.
Relato de Caso
Blow-out fracture. Retroseptal approach with sutureless closure and reconstruction of the orbital floor using titanium mesh
Resumo
Introdução: Uma fratura blow-out orbitária é uma fratura do assoalho orbitário causada por um traumatismo rombo à órbita. As fraturas blow-out são geralmente causadas por objetos ovais ou arredondados com um diâmetro levemente maior do que o diâmetro orbitário, tais como uma bola de baseball ou de tênis. O mecanismo da fratura é controverso. As três teorias mais aceitas são: 1) a teoria da retropropulsão, teoria que propõe que a fratura é resultado de um aumento repentino da pressão intraorbitária quando o globo é empurrado posteriormente; 2) a teoria “buckling” estabelece que a fratura é secundária à força aplicada ao rebordo orbitário e transmitida aos ossos orbitários; 3) uma mistura das duas primeiras teorias. As fraturas blow-out podem causar vários problemas. Para manejar esses problemas, a reconstrução orbitária é mandatória. Vários acessos cirúrgicos e materiais são relatados na literatura. objetivo: Este relato de caso mostra o acesso retrosseptal sem sutura e reconstrução do assoalho orbitário com malha de titânio. Resultados: Os autores discutem os acessos pré e retrosseptais e as possíveis complicações pós-operatórias. Conclusões: Muitos pesquisadores concluíram que os implantes de malhas de titânio são uma opção confiável e simples para o reparo de assoalho orbitário rotineiro. Os autores consideram o acesso retrosseptal e o uso da malha de titânio como satisfatórios e confiáveis para a correção de fratura blow-out imediata em adultos.
Descritores: Fraturas Orbitárias; Telas Cirúrgicas; Zigoma.
AbstRACt
Introduction: An orbital blow-out fracture is a fracture of the orbital floor caused by blunt trauma to the orbit. Blow-out fractures are usually caused by round or oval object with a diameter slightly larger than the orbital diameter such as a baseball or tennis ball. The mechanism of fracture is controversial. The three most accepted theories are: 1) the “retropulsion” theory which proposes the fracture is a result of a sudden increase in intraorbital pressure when the globe is pushed posteriorly; 2) the “buckling” theory states that the fracture is secondary to the force applied to the orbital rim and transmitted to orbital bones; 3) a mixture of the first two teories. Blow-out fractures can cause several problems. To manage these problems, orbital reconstruction is mandatory. Various surgical approaches and materials are reported in the literature. objective: This case report shows a retroseptal approach with sutureless closure and reconstruction of the orbital floor using titanium mesh. Results: The authors discuss on pre and retroseptal approaches and potential postoperative complications. Conclusions: Many researchers have concluded that titanium mesh implants are a simple and reliable option for routine orbital floor repair. The authors consider the retroseptal approach and the use of titanium mesh as satisfactory and reliable for correction of immediate blow-out fracture in adults.
Key words: Orbital Fractures; Surgical Mesh; Zygoma.
Código 651
IntRoDuCtIon
An orbital blow-out fracture is a fracture of the orbital floor caused by blunt trauma to the orbit. Blow-out fractures are usually caused by round or oval object with a diameter slightly larger than the orbital diameter such as a baseball, snowball, tennis ball or fist. The mechanism of fracture is controversial. The three most accepted theories are: 1) the “retropulsion” theory which proposes the fracture is a result of a sudden increase in intraorbital pressure when the globe is pushed posteriorly; 2) the
“buckling” theory states that the fracture is secondary to the force causing the orbital rim to buckle and transmitting the force into the orbital bones; 3) a mixture of the first two teories.
One may expect medial wall fractures to be more common than orbital floor fractures as the medial wall is thinner; however, the reverse is true. Proponents of the “retropulsion” theory attribute this to the honeycomb structure of the ethmoid air cell septae, which support the lamina papyracea, thus allowing it to withstand the sudden rise in intraorbital hydraulic pressure better than
Rev. Bras. Cir. Cabeça Pescoço, v.45, nº 2, p. 59-62, Abril / Maio / Junho 2016 ––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––– 59
Fratura blow-out. Acesso retrosseptal sem sutura e reconstrução do assoalho orbitário com malha de titânio. Oliveira et al.
the orbital floor. Proponents of the “buckling” theory propose that the orbital floor is particularly vulnerable as the infraorbital canal further weakens the floor’s already delicate bony structure1.
Transconjunctival approach
When the repair of the fracture requires exposure of the orbital floor and rim (transconjunctival approach), both preseptal and retroseptal dissection planes have been described. This technique has proven be an excellent approach for the exposure of the orbital floor and inferior rim. The main advantage to this technique is the lack of visible scar. A recent review and study of this technique has demonstrated that this approach is indeed safe and effective in patients who have not undergone a previous transconjunctival incision2.
Choice of reconstruction material3
The unique and complex anatomy of the orbit, unless prebent plates are used, requires significant contouring of the implants to restore the proper anatomy.
The majority of cases require reconstruction of the orbital floor to support the globe position and restore the shape of the orbit. The reason for this is that the bony walls are comminuted and/or bone fragments are missing. Therefore, one is reconstructing missing bone rather than reducing bone fragments. This can be accomplished using various materials.
There is hardly any anatomic region in the human body that is so controversial in terms of appropriate material used for fracture repair: nonresorbable versus resorbable; autogenous/allogenous/xenogenous versus alloplastic material; non-prebent versus preformed (anatomical) plates; standard versus custom-made plates; nonporous versus porous material; noncoated versus coated plates.
Many surgeons recommend using materials that allow bending to an anatomical shape, that are radiopaque (to allow for intra or postoperative radiologic confirmation of placement), and stable over time.
Reconstruction of the dislocated orbital walls is demanding. Secondary changes to this contour are undesirable. This is why critical consideration of the use of resorbable materials is necessary.
There are different preferences of implant material depending on regional differences, variations in schools of teaching, and socio-economic factors. There is a paucity of evidence to support the ideal choice for an orbital implant. Modern imaging analysis offers a unique chance to quantitatively asses the surgical result and stability over the time. This can provide valuable information for future recommendation.
Titanium Meshes
Advantages: availability; stability; contouring (eased by the artificial sterile skull); adequate in large three-wall fractures (the pre-bent plate is limited to medial wall and orbital wall fractures only); radiopacity; spaces within the
mesh to allow dissipation of fluids; no donor site needed; tissue incorporation may occur.
Disadvantages: costs; possible sharp edges if not properly trimmed.
The extensive use of mesh for orbital reconstruction in traumatized orbits has been shown to be safe, with few problems due to infections and no problems with secondary displacement due to additional trauma, on condition of proper handling, contouring, and fixation of the mesh.
The purpose of this paper is to report on the surgical outcome of a patient undergoing orbital fracture repair without periosteal or conjunctival closure.
This work has been approved by the appropriate ethical committee related to the Federal University of Paraíba - Brazil - in which it was performed and that the patient gave informed consent to the work.
CAse RePoRt
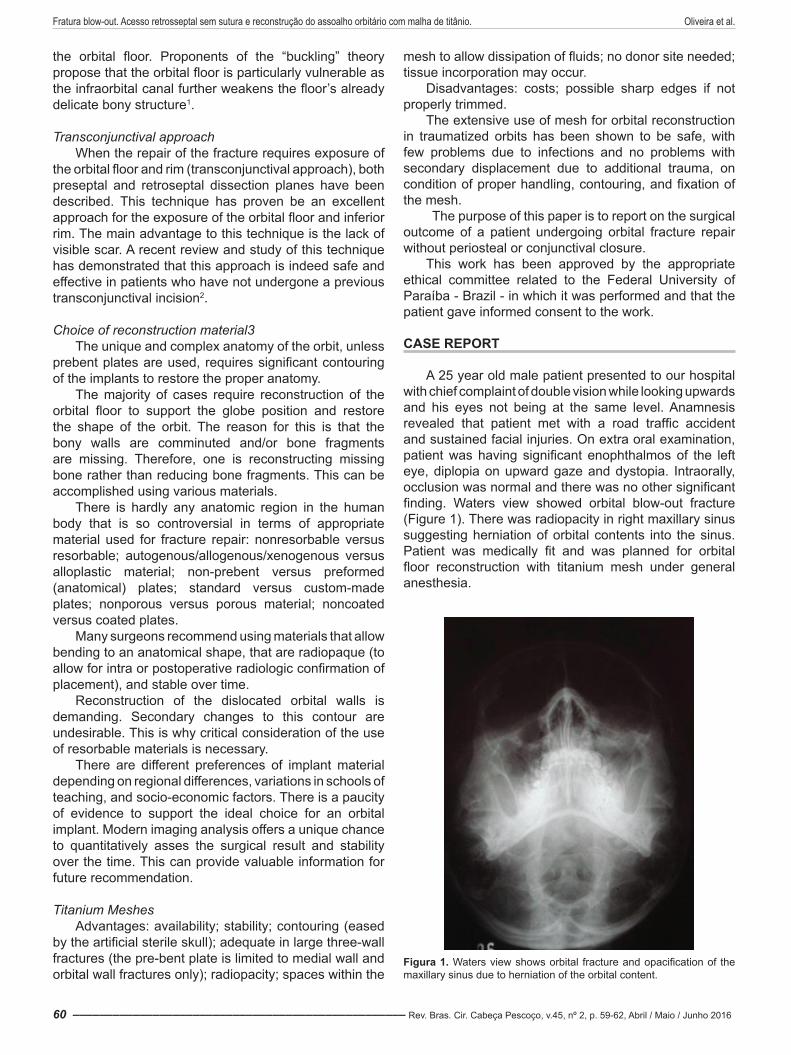
A 25 year old male patient presented to our hospital with chief complaint of double vision while looking upwards and his eyes not being at the same level. Anamnesis revealed that patient met with a road traffic accident and sustained facial injuries. On extra oral examination, patient was having significant enophthalmos of the left eye, diplopia on upward gaze and dystopia. Intraorally, occlusion was normal and there was no other significant finding. Waters view showed orbital blow-out fracture (Figure 1). There was radiopacity in right maxillary sinus suggesting herniation of orbital contents into the sinus. Patient was medically fit and was planned for orbital floor reconstruction with titanium mesh under general anesthesia.
Figura 1. Waters view shows orbital fracture and opacification of the maxillary sinus due to herniation of the orbital content.
60 –––––––––––––––––––––––––––––––––––––––––––––––––– Rev. Bras. Cir. Cabeça Pescoço, v.45, nº 2, p. 59-62, Abril / Maio / Junho 2016
Fratura blow-out. Acesso retrosseptal sem sutura e reconstrução do assoalho orbitário com malha de titânio. Oliveira et al.
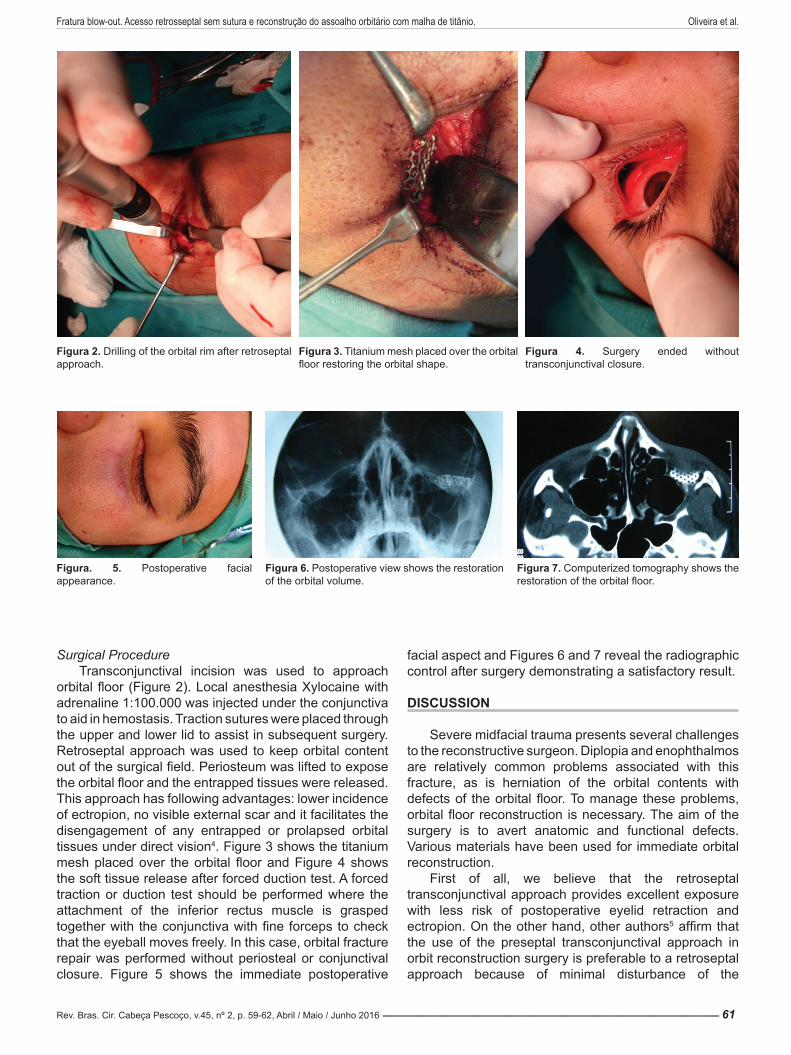
Surgical ProcedureTransconjunctival incision was used to approach
orbital floor (Figure 2). Local anesthesia Xylocaine with adrenaline 1:100.000 was injected under the conjunctiva to aid in hemostasis. Traction sutures were placed through the upper and lower lid to assist in subsequent surgery. Retroseptal approach was used to keep orbital content out of the surgical field. Periosteum was lifted to expose the orbital floor and the entrapped tissues were released. This approach has following advantages: lower incidence of ectropion, no visible external scar and it facilitates the disengagement of any entrapped or prolapsed orbital tissues under direct vision4. Figure 3 shows the titanium mesh placed over the orbital floor and Figure 4 shows the soft tissue release after forced duction test. A forced traction or duction test should be performed where the attachment of the inferior rectus muscle is grasped together with the conjunctiva with fine forceps to check that the eyeball moves freely. In this case, orbital fracture repair was performed without periosteal or conjunctival closure. Figure 5 shows the immediate postoperative
facial aspect and Figures 6 and 7 reveal the radiographic control after surgery demonstrating a satisfactory result.
DIsCussIon
Severe midfacial trauma presents several challenges to the reconstructive surgeon. Diplopia and enophthalmos are relatively common problems associated with this fracture, as is herniation of the orbital contents with defects of the orbital floor. To manage these problems, orbital floor reconstruction is necessary. The aim of the surgery is to avert anatomic and functional defects. Various materials have been used for immediate orbital reconstruction.
First of all, we believe that the retroseptal transconjunctival approach provides excellent exposure with less risk of postoperative eyelid retraction and ectropion. On the other hand, other authors5 affirm that the use of the preseptal transconjunctival approach in orbit reconstruction surgery is preferable to a retroseptal approach because of minimal disturbance of the
Figura 2. Drilling of the orbital rim after retroseptal approach.
Figura 3. Titanium mesh placed over the orbital floor restoring the orbital shape.
Figura 4. Surgery ended without transconjunctival closure.
Figura. 5. Postoperative facial appearance.
Figura 6. Postoperative view shows the restoration of the orbital volume.
Figura 7. Computerized tomography shows the restoration of the orbital floor.
Rev. Bras. Cir. Cabeça Pescoço, v.45, nº 2, p. 59-62, Abril / Maio / Junho 2016 ––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––– 61

Fratura blow-out. Acesso retrosseptal sem sutura e reconstrução do assoalho orbitário com malha de titânio. Oliveira et al.
intraorbital connective tissue framework in as much as the anatomic optimal dissection line also results in a lower complication rate.
In relation to titanium meshes, several authors have demonstrated the safety and effectiveness of titanium in orbital reconstruction. One question posed by clinicians is what happens to large pieces of titanium in communication with the paranasal sinuses or nasal-oral-pharyngeal area. This question becomes increasingly relevant as titanium is used to reconstruct extensive defects for which the destruction of bony architecture requires the placement of mesh in proximity to these areas. There is a study that provides evidence of titanium’s compatibility with soft tissue. The mesh underwent progressive incorporation with soft tissue that was then resurfaced by indigenous cells, including respiratory epithelia and goblet cells. This phenomenon occurred despite communication with the nasal-oral-pharyngeal area and paranasal sinuses6.
Titanium meshes are thin, stiff and easy to contour. They are easily stabilized, maintain their shape, and have the unique ability to compensate for volume without the potential for resorption. When titanium meshes were introduced, it was generally believed that they needed no removal, since titanium is a highly biocompatible material. However, it has been shown that both titanium and aluminium are released from titanium implants into the adjacent structures and even into regional lymph nodes. The clinical relevance of this release is not yet known. In our personal experience, we believe that these potential clinical problems are irrelevant in long-term outcomes.
It has been suggested that in pediatric surgery in the 20 areas of bony resorption and deposition, metallic fixation plates should be removed due to plate displacement and to restriction of growth. There are further disadvantages with titanium implants in orbital wall reconstruction. These include the risk of extrusion due to dehiscence of covering soft tissue and the risk of infection. There is also a theoretical risk of injury to the tissues of the orbital apex from any subsequent blow to the orbit. Because of the mesh structure, the orbital implant is difficult to remove. Concordantly, we perform bioabsorbable systems in pediatric surgery as routine. Moreover, in our understanding the mentioned risks are feasable and should be considered especially for adults who play radical sports.
Titanium implants have been used to span large defects in the internal orbit to provide a platform for bone graft support. Many researchers have concluded that titanium mesh implants are a simple and reliable option for routine orbital floor repair7.
Post-Operative Management2
The patient’s vision should be monitored in the immediate post-operative phase, whilst still in the recovery room and over the next few hours. Functional tests, in particular, for diplopia and mobility, should be
performed once the swelling has subsided using standard ophthalmological procedures. Radiological assessment (CT) is not required if functional findings are normal.
ComplicationsOperative complications of the transconjunctival
inferior fornix approach are related in the literature such as: cicatricial entropion, lower eyelid retraction, canthal dehiscence, lower eyelid avulsion, canalicular laceration, buttonhole laceration of the lower eyelid, conjunctival chemosis, and lacrimal sac laceration. Attention to anatomic landmarks and sound surgical execution will prevent these complications in most patients8.
The most severe complication that may occur during or following surgery is the loss of vision caused by damage to the optic nerve, e.g. by intrusion of bone fragments into the dorsal orbital conus. Extra-ocular muscles and the nerves innervating them are subject to damage especially in the region of the anterior orbital floor as a result of traumatic detachment of the peri-orbita or massive fragment displacement during reduction2.
In our opinion, a meticulous surgical technique prevents potential problems and postoperative complications. The authors consider the retroseptal approach and the use of titanium mesh as satisfactory and reliable for correction of immediate blow-out fracture in adults.
ReFeRenCes
1. Pubblicato da David Spizzichino. Neuroradiology on the net. A isointense on T1 – Blog. Orbital blow out fracture. http://neuroradiologyonthenet.blogspot.com.br/2009/01/orbital-blow-out-fracture.html. Acess: May 9, 2012.2. Oral & Maxillo-Facial Surgery. Facial Trauma, Zygomatic Arch Fractures. http://oralmaxillo-facialsurgery.blogspot.com.br/search?q=facial+trauma+zygomatic +complex. Acess: May 9, 2012.3. Cornelius CP, Gellrich N, Hillerup S, Kusumoto K. AO Foundation. Midface Orbital floor fracture – Orbital Reconstruction. https://www2.aofoundation.org/wps/portal/surgery?showPage=redfix&bone=CMF&segment=Midface&classification=92-Orbit,%20Orbital%20floor%20fracture&treatment=&method=Open%20treatment&implant-s t y p e = O r b i t a l % 2 0 r e c o n s t r u c t i o n & a p p r o a c h = & r e d f i x _url=&Language=e n. Access: May 8, 2012.4. Dendukuri G, Mohan AP, Sukhvinder B. NACD. National Academy of Dentistry. Secondary Correction Of Orbital Deformity Using Iliac Crest Bone Graf. thttp://www.nacd.in/ijda/volume-02-issue-01/32-secondary-correction-of-orbital-deformity-using-iliac-crest-bone-graft. Access: May 8, 2012.5. Baumann A, Ewers R. Use of the preseptal transconjunctival approach in orbit reconstruction surgery. J Oral Maxillofac Surg 59(3):287-291; discussion 291-2 11243611 Cit:19, 2001.6. Schubert W, Gear AJ, Lee C, Hilger PA, Haus E, Migliori MR, Mann DA, Benjamin CI. Incorporation of titanium mesh in orbital and midface reconstruction. Plast Reconstr Surg. 15;110(4):1022-1030; discussion 1031-2, 2002.7. Kontio R. Reconstruction of Orbital Wall Fracture. An experimental and clinical study. http://ethesis.helsinki.fi/julkaisut/laa/hamma/vk/kontio/reconstr.pdf. Academic dissertation. Helsinki University, 2005. Access: May 7, 2012.8. CT Westfall, JW Shore, WR Nunery, JJ Hawes, MJ Yaremchuck. Operative complications of the transconjunctival inferior fornix approach. Ophthalmology 98 (10):1525-1528 1961638 Cit:31, 1991.
62 –––––––––––––––––––––––––––––––––––––––––––––––––– Rev. Bras. Cir. Cabeça Pescoço, v.45, nº 2, p. 59-62, Abril / Maio / Junho 2016